INITIATIVES THAT CREATE ADDITIONAL REVENUE FOR HEALTH CARE IN JAMAICA
THE NATIONAL HEALTH FUND
Eva Lewis-FullerPublic Health Consultant
Jamaica W.I.

•Achieved independence from Britain – 1962
•Total population: 2,751,300
•Life expectancy at birth (years): Total: 73 - Male: 71years; Female: 76 years•An ageing population with 11% over 60 years•Main causes of death:
- Cardiovascular diseases- Malignant neoplasm (cancers)- Diabetes- Trauma/violence

The Health Care System• Emerged as a centralized health care system out of the
era of slavery. • 1997 - Decentralized into 4 Regions: i)South East,
ii)Southern, iii)Western, iv)North East. • 24 hospitals operating at 3 levels: A, B, C• 350 primary health care centres operating at 5 levels:
Types 1, 2, 3, 4, 5• Government-funded health care from general taxes• Health workers/providers are paid negotiated/
standardized salaries through temporary or permanent appointments or contracts

PRIVATE HEALTH CARE• Provides 60% of primary health care
services• Provides about 15% of secondary/tertiary
services in 6 private hospitals• 18% of population covered with private
health insurance• Few government/private partnership in
health care - e.g. diagnostic services


Population (2007): 2.78 millionPopulation (2007): 2.78 million
GDP per capita @ PPP (2006): US$ GDP per capita @ PPP (2006): US$ 46004600
Smoking prevalence: 15%Smoking prevalence: 15%

CARICOMCaribbean Regional Integration Efforts
Jamaica
Trinidad & Tobago Barbados Dominica
Grenada
Belize
Antigua & Barbuda
SurinameThe BahamasGuyanaHaitiMontserrat
St Kitts & Nevis
St Vincent & the Grenadines
St Lucia

Overview of Functions of Health Care Systems
Source: Murray c. and Frenk S. (1999) A WHO Framework for Health System Performance Assessment


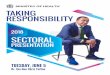
Tobacco Taxation – Potential for increased revenue
Tax Revenue
Tax Rate %
0 20 40 60 80 100
The Laffer Curve
Optimal

• Value Added Tax/General Consumption Tax
• Special Consumption Tax – Specific *
• Import Duty
• Standard Compliance Fee
• Customs User Fee
• Cost Insurance and Freight
• Environmental Levy
* SCTS increased from $2.30 to $6.00 per stick of cigarette
• Excise Duty
• Additional Stamp Duty
• Special Consumption Tax ad valorem
Changes in Taxation, 2008Amendment to the GCT Act, resulted in changes in the tax structure

Taxes and Charges Collected from Cigarettes
Tax Type 2007 2008 2012/2013 Financial Year
Tariff 7,328,281.10 6,336,712.79
Additional Stamp duty
21,614,500.02 14,241,230.51
General Consumption Tax
495,772,884.29 699,341,204.16
Special Consumption Tax (AVD)
6,669.15 22,724.62
Special Consumption Tax
1,967,274,560.00 3,609,399,500.00
Environmental Levy 1.414,116.51 2,527,629.84
Excise 561,753,177.06 200,121,711.86
Standards Compliance Fee
1,493,707.06 1,516,577.71
Customs User Fee 9,948,309.46 10,081,004.60
TOTAL 3,066,606,204.65 4,543,588,296.09 1,250,776,784.71

TOBACCO TAXATION – JAMAICA 2007• Share of tobacco-specific taxes in the prices of pack of cigarette:• Excise specific tax .........15.8%• Excise ad-valorem tax....14.5%• Import duties on pack ....23.9%TOTAL TOBACCO-SPECIFIC TAXES IN PRICE = 54.2%
2008Increase in Special consumption tax to produce $2.88 billionTobacco-specific taxation in retail price = 57%2009SCT on cigarettes increased from $6,000 per 1,000 sticks to $8,500
to produce a revenue of $1.84 Billion. Tobacco-specific taxation in retail price= approx. 60%

A clear negative relationship between the A clear negative relationship between the real price of cigarettes and consumption in real price of cigarettes and consumption in
JamaicaJamaica
14

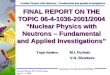
Impact of a 10 per cent increase in cigarette tax, given Impact of a 10 per cent increase in cigarette tax, given different price elasticities of demand (and an initial tax different price elasticities of demand (and an initial tax
burden of 52 per cent)burden of 52 per cent)Price Price
elasticitelasticityy
% change in % change in consumptionconsumption
% change in % change in government government
revenuerevenue
0.00.0 0.000.00 10.0010.00
-0.1-0.1 -0.52-0.52 9.439.43
-0.2-0.2 -1.04-1.04 8.868.86
-0.3-0.3 -1.56-1.56 8.288.28
-0.4-0.4 -2.08-2.08 7.717.71
-0.5-0.5 -2.60-2.60 7.147.14
-0.6-0.6 -3.12-3.12 6.576.57
-0.7-0.7 -3.64-3.64 6.006.00
-0.8-0.8 -4.16-4.16 5.425.42
-0.9-0.9 -4.68-4.68 4.854.85
-1.0-1.0 -5.20-5.20 4.284.28
-1.1-1.1 -5.72-5.72 3.713.71
-1.2-1.2 -6.24-6.24 3.143.14
-1.3-1.3 -6.76-6.76 2.562.56
For all realistic (and even For all realistic (and even unrealistic) price elasticities unrealistic) price elasticities of demand an increase in of demand an increase in the excise taxthe excise tax
(1)(1)decreases consumptiondecreases consumption
(2)(2)increases government increases government revenuerevenue
15

Brought about by The National Health Fund Act, April 1, 2003.

Areas to be presented:
1. NHF’s MANDATE
2. REVENUE SOURCES & PERFORMANCE
3. EXPENDITURE 2004 – 2011
4. FINANCIAL SUSTAINABILITY ISSUES
5. CONCLUSION
THE NATIONAL HEALTH FUND
17

To provide prescribed health benefits to all residents of Jamaica
To provide greater access to medical treatment and preventative care for specified diseases and specified conditions
To secure improvement in the productivity of residents by reducing time lost on the job due to health care problems
NHF’s MANDATE

To reduce the Island’s disease burden through health promotion and prevention programmes
To provide support to health services and promote and encourage the utilization of primary health care services
To improve the quality of life of the populationTo make pharmaceutical and medical supplies
accessible and available to government owned health facilities
NHF’s MANDATE

NHF’s mandate is achieved through:NHF Benefits Division
• Individual Benefits - provide direct assistance to patients with specific conditions, the elderly under the Jamaica Drug for the Elderly Programme (JADEP), for persons of all ages with chronic diseases.
• Institutional Benefits - provide assistance to the public and private healthcare system
• Public Information - provides direct assistance through education and information.
NHF Pharmaceutical Division• Wholesale pharmaceuticals mainly to Regional Health Authorities (RHA). Will
be fully responsible for pharmaceutical services as of 2014.
• Drug Serv: Provides retail sale of pharmaceuticals at affordable prices
through Drug Serv Pharmacies strategically located.
THE BENEFITS OF THE NHF

REVENUE SOURCESNHF’s revenue stream is comprised of:
NHF Benefits Division• Tobacco Tax• SCT• Payroll Tax (from National Insurance deductions)
NHF Pharmaceutical Division • Sale of Pharmaceuticals mainly to Regional Health Authorities
(RHA)
Drug Serv• Provides retail sale of pharmaceuticals at affordable prices
through Drug Serv.A broadened revenue base will go a far way in ensuring that the NHF is better
able to achieve its objectives now and in the longer term as financial sustainability is strengthened.

FUNDING 2009/2010 to presentThe NHF is financed by three sources of funding:1) 20% of SCT charged on the importation of tobacco related products.2) A Payroll Deduction collected by the National Insurance Fund (1% of 5% (20%) of NIS Collected).3)5% of the Special Consumption Tax collected.
Note that in April 2009 the tax structure on Tobacco was changed; the changes were as follows for 2009/2010:NHF’s entitlement from SCT on Tobacco was reduced from 23% to 20%; however, the specific tax rate was increased from $6,000.00 to $8,500.00 per thousand sticks of cigarettes.
22

TOBACCO TAX 2003 to 2008 – 23% Excise Revenue declined between
2005-20082008-2009 - Tax structure
revised as follows: 23% Excise eliminated. SCT increased from $2,300 to
$6,000 per thousand sticks with NHF entitled to 20% of this SCT.
2009-2010 – increase in specific tax from $6,000 to $8,500 per thousand sticks of cigarettes

5% SCT Since April 2003 – 5% of Special
Consumption Tax Collected Increase in revenue from this
source is due to increase in the price of the products on which SCT is charged; petrol and alcohol in particular.
Effective April 27, 2009 SCT on petrol was increased by $8.75 per litre; based on Section 9(c) of the NHF Act, NHF is entitled to 5% of this additional SCT, however this is in dispute with the MOF.

PAYROLL TAX Since Oct. 2003 (1% of 5% of
NIS collected).Presently accounts for 41% of
NHF’s revenue.Revenue from Payroll Tax
declined in 2009/10 when compared to 2008/09; this is due to: Unemployment increasing Reduction in compliance by
employer. There was an increase in
2010/11, this is due to an increase in the NIS threshold from $500k to $1m.

26

27

Health care expenditure will continue to consume a greater share of revenue as utilization pattern increases.
In order to achieve a high level of efficiency and quality delivery of services, further expenditure in technological development will be warranted.
Demographic factors such as ageing population will impact utilization patterns.
EXPENDITURE

29

INCOME & EXPENDITURE

• Financial sustainability from NHF’s perspective refers to the ability of NHF to collect sufficient financial resources and to manage these resources effectively to realise our mandate over the long term and to allow us to promote quality and efficiency in service delivery and improvement in
administrative and technical processes
NHF’s FINANCIAL SUSTAINABILITY

Declining revenues from established sources of funding
Impediments to revenue outcomes e.g due to illegal activities such as counterfeit cigarettes and alcohol
Harsh economic climate may force collection agencies to withhold fund due to NHF to meet their immediate financial needs
Changes in Government Policy (eg. The pending policy that will require government owned entities to remit a minimum of 5 – 10 % of surplus to the Consolidated Fund.)
THREATS TO NHF’S SUSTAINABILITY

• The NHF is an important source is revenues for the Ministry of Health. • Based on our current level of funding, the NHFshould continue to be sustainable in themedium term, assuming no additional demands. • As effective health promotion measures achieves the goals of reducing prevalence of
illnesses and deaths caused by lifestyle habits such as tobacco smoking and excessive alcohol, other sources of funding will have to be found for the NHF in the future
If, however, benefits are to be added, it mustbe done incrementally and there must be atleast a commensurate increase in revenue. The sustainability of the NHF must bestrengthened so that we will continue toeffectively reduce the burden of health care inJamaica.
CONCLUSION

THE HEALTH EQUATION
Health = Constant (nutrient consumption x education x healthy lifestyle x child care x sanitation x appropriate health technology x .....etc etc.....
Remember ...whatever is done to one side of the equation should be done to the other.

END
THANK YOU
35
Recommended