Informatics and Risk Management
David W. Bates, MD, MScDavid W. Bates, MD, MScMedical Director of Clinical and Quality Analysis, Medical Director of Clinical and Quality Analysis,
Partners HealthcarePartners HealthcareChief, Division of General Medicine, Brigham and Chief, Division of General Medicine, Brigham and
WomenWomen’’s Hospitals Hospital
Hong Kong, Spring 2006

OverviewNature/scope of safetyNature/scope of safety
CostsCostsImpact/potential of ISImpact/potential of ISReportingReportingRole of leadershipRole of leadershipConclusionsConclusions

Leadership and IT
Leadership is the capacity to hold a shared vision of Leadership is the capacity to hold a shared vision of that we wish to create.that we wish to create.
–– Peter Peter SengeSenge

Relationship between Risk Management and Safety
True underlying goal to improve safetyTrue underlying goal to improve safetyMany safety problems present low risk for Many safety problems present low risk for organizationsorganizations
Thus, not complete overlap between managing Thus, not complete overlap between managing risk and improving safetyrisk and improving safety
But two are sufficiently close to be considered But two are sufficiently close to be considered togethertogether
Generally, improving safety will lower riskGenerally, improving safety will lower risk

IOM I: To Err Is HumanReport targets hospital errors: Mistakes killing Report targets hospital errors: Mistakes killing thousands every year thousands every year 11/30/9911/30/99
Medical errors kill 44,000Medical errors kill 44,000--98,000 people per year98,000 people per year““More people die from medical errors each year than from More people die from medical errors each year than from suicides, highway accidents, breast cancer, or AIDSsuicides, highway accidents, breast cancer, or AIDS””
““These stunningly high rates of medical errors These stunningly high rates of medical errors --resulting in deaths, permanent disability, and resulting in deaths, permanent disability, and unnecessary suffering unnecessary suffering -- are simply unacceptable are simply unacceptable in a system that promises to first in a system that promises to first ‘‘do no harm.do no harm.’”’”
William RichardsonWilliam Richardson

The Chasm Report
““Indeed, between the health care that we now have, Indeed, between the health care that we now have, and the health care we could have, lies not just a and the health care we could have, lies not just a gap, but a chasm.gap, but a chasm.”” Crossing the Quality Chasm: A Crossing the Quality Chasm: A New Health System for the 21New Health System for the 21stst CenturyCentury

Safety and Systems
““Every system is perfectly Every system is perfectly designed to achieve exactly the designed to achieve exactly the results it gets.results it gets.””
Donald Berwick
“Safety is a systems property.”
Chasm Report


Handwriting example

Rates of Adverse Events3.7% of hospitalizations in New York3.7% of hospitalizations in New York
58% preventable58% preventable2.8% Colorado2.8% Colorado--UtahUtah16.6% in Quality in Australian Health Care study16.6% in Quality in Australian Health Care study10.8% in UK pilot study (Vincent)10.8% in UK pilot study (Vincent)
Half preventableHalf preventable1/3 resulted in moderate or greater disability or death1/3 resulted in moderate or greater disability or death

Types of Complications
OverallOverallAdv. drug events 19%Adv. drug events 19%Wound infections 14%Wound infections 14%Technical Technical complcnscomplcns 13%13%
Almost half were associated Almost half were associated with a surgical procedurewith a surgical procedure
NonNon--OperativeOperativeAdv drug events 37%Adv drug events 37%Diagnostic mishaps 15%Diagnostic mishaps 15%Therapeutic mishaps 14%Therapeutic mishaps 14%ProcedureProcedure--related 13%related 13%Falls 5%Falls 5%

Costs to the SystemQAHCSQAHCS
8% of hospital bed days8% of hospital bed days$4.7 billion/year$4.7 billion/year
UKUK8.5 days/adverse event8.5 days/adverse eventCosts to NHS 1 billion pounds/yearCosts to NHS 1 billion pounds/year
USUSCosts of ADEs in hospitals $2 billion/yearCosts of ADEs in hospitals $2 billion/yearAll drugAll drug--related problems $177.4 billion/year!related problems $177.4 billion/year!
Limited data from other areas all suggest similar Limited data from other areas all suggest similar

Systems Improvement and IT in Healthcare
Systems shouldSystems shouldMake errors less likelyMake errors less likelyCatch those that do occurCatch those that do occur
Current systems communicate poorlyCurrent systems communicate poorlyHealth care spends little on ITHealth care spends little on IT
Implementation is challenging, turnover highImplementation is challenging, turnover highWriting a large check doesnWriting a large check doesn’’t guarantee successt guarantee success

Reengineering Medicine:The Role of IS
Could be changed by providing external aidsCould be changed by providing external aidsLinking medical knowledge and patientLinking medical knowledge and patient--specific dataspecific dataIdentifying optionsIdentifying options
Without such tools, expertsWithout such tools, expertsMake errorsMake errorsOverlook available knowledgeOverlook available knowledgeDonDon’’t sufficiently account for uniqueness of patientst sufficiently account for uniqueness of patients
Weed LL, Weed L, Federation Bulletin, 1994

Ways IT Can Improve Safety
Prevent errors and adverse eventsPrevent errors and adverse eventsFacilitating a more rapid response after an Facilitating a more rapid response after an adverse event has occurredadverse event has occurredTracking and providing feedback about adverse Tracking and providing feedback about adverse eventsevents

Main Strategies for Preventing Errors and AEs Using IT
Tools to improve communicationTools to improve communicationMaking knowledge more readily accessibleMaking knowledge more readily accessibleRequiring key pieces of informationRequiring key pieces of informationAssisting with calculationsAssisting with calculationsPerforming checks in real timePerforming checks in real timeAssisting with monitoringAssisting with monitoringProviding decision supportProviding decision support
Bates and Gawande, NEJM 2003

Specific IT Applications
Computerized physician order entryComputerized physician order entrySmart pumpsSmart pumpsSmart monitoringSmart monitoringComputerized notification about critical test resultsComputerized notification about critical test resultsComputerized ADE monitoringComputerized ADE monitoringTracking abnormal test resultsTracking abnormal test resultsElectronic health record (outpatient)Electronic health record (outpatient)
Includes computerized prescribingIncludes computerized prescribing

IS and Adverse Events in Hospitals
Adverse drug eventsAdverse drug eventsNosocomial infectionsNosocomial infectionsAsynchronous eventsAsynchronous eventsCoverageCoverage--related eventsrelated events

Computerized Physician Order Entry
Single most powerful intervention for improving Single most powerful intervention for improving medication safety to datemedication safety to dateOver 80% reduction in medication error rateOver 80% reduction in medication error rateNeed to have associated decision support if want Need to have associated decision support if want to see high level of benefitto see high level of benefit

NEPHROS studyEffect of realEffect of real--time decision support for patients time decision support for patients
with renal insufficiencywith renal insufficiencyOf 17,828 patients, 42% had some degree of Of 17,828 patients, 42% had some degree of renal insufficiencyrenal insufficiency
IntervInterv ControlControlDoseDose 67%67% 54%54%FrequencyFrequency 59%59% 35%35%
LOS 0.5 days shorter LOS 0.5 days shorter Chertow et al, JAMA 2001

Guided Prescription for Geriatric Inpatients
Elderly patients frequently get dosages that are too Elderly patients frequently get dosages that are too high, especially initial dosageshigh, especially initial dosagesPerformed RCT of decision support around dosing Performed RCT of decision support around dosing for psychoactive drugsfor psychoactive drugsWas associated with:Was associated with:
More frequent recommended dose (29% vs. 19%)More frequent recommended dose (29% vs. 19%)Lower fall rate (2.8 vs. 6.4 falls/1000 pt days)Lower fall rate (2.8 vs. 6.4 falls/1000 pt days)Lower frequency of 10Lower frequency of 10--fold overdose (2.8% vs. 5%)fold overdose (2.8% vs. 5%)No difference in mental status change, LOSNo difference in mental status change, LOS
Clearly beneficial to suggest starting with lower Clearly beneficial to suggest starting with lower dosage but more room for improvementdosage but more room for improvement
Peterson, Arch Intern Med, 2005

How to Prioritize?ROI of inpatient CPOE evaluatedROI of inpatient CPOE evaluatedCumulative net savings were $16.7 million over 10 years, Cumulative net savings were $16.7 million over 10 years, and net operating $9.5 millionand net operating $9.5 millionLeading contributorsLeading contributors
Renal dosing guidanceRenal dosing guidanceTools to help nursesTools to help nursesSpecific drug guidanceSpecific drug guidanceAdverse drug event preventionAdverse drug event prevention
Kaushal, JAMIA 2006

Bar-codingTechnology is inexpensiveTechnology is inexpensiveWill help in:Will help in:
Matching medication orders and drug productsMatching medication orders and drug productsMedications dispensed/administeredMedications dispensed/administeredIdentifying correct patientIdentifying correct patient
Will knowWill knowWhat/how much/who/whenWhat/how much/who/when
Few published data so far, but experience in other Few published data so far, but experience in other industries suggest important benefitindustries suggest important benefit
Doing controlled trial nowDoing controlled trial nowSubstantial benefit even with barSubstantial benefit even with bar--coding in pharmacycoding in pharmacy


Impact of “Smart” IV PumpsFew administration errors get caughtFew administration errors get caught
Yet intravenous errors can be especially dangerous Yet intravenous errors can be especially dangerous CaseCase
Heparin bolus dose of 4000 units, followed by an Heparin bolus dose of 4000 units, followed by an infusion of 890 units/hrinfusion of 890 units/hr
4000 unit bolus dose was given appropriately4000 unit bolus dose was given appropriatelyBut nurse misinterpreted the order and programmed the But nurse misinterpreted the order and programmed the infusion device to deliver 4000 U/hour, not 890 U/hourinfusion device to deliver 4000 U/hour, not 890 U/hour
Smart pump alerted nurseSmart pump alerted nurseEarly dataEarly data——2 such errors/day in 4002 such errors/day in 400--bed hospitalbed hospital
ISMP Newsletter Feb 6, 2002

Take-Away Messages ofControlled Trial
Serious IV med errors were frequent and could be Serious IV med errors were frequent and could be detected using smart pumpsdetected using smart pumpsHowever, no impact on the serious med error or However, no impact on the serious med error or preventable ADE rate was foundpreventable ADE rate was found
Likely because of poor complianceLikely because of poor complianceBehavioral and technologic factors must be addressed Behavioral and technologic factors must be addressed if smart pumps are to achieve their potential for if smart pumps are to achieve their potential for improving medication safety improving medication safety
Rothschild et al, Crit Care Med 2005

System-Provider Communication:ADE Computer Monitor
Goal: to identify possible ADEs and communicate Goal: to identify possible ADEs and communicate the info to cliniciansthe info to cliniciansMakes safety more ingrained into pharmacy culture Makes safety more ingrained into pharmacy culture and workflow and workflow Rule is a preRule is a pre--determined set of criteriadetermined set of criteria
E.g E.g AminoglycosideAminoglycoside and rise in creatinineand rise in creatinineWhen criteria met, an alert is generated to the When criteria met, an alert is generated to the pharmacistpharmacistPharmacist contacts MD to make a changePharmacist contacts MD to make a changeInterventions are trackedInterventions are trackedNet savings: $900,000/yearNet savings: $900,000/year

“Smart” Monitoring
Monitoring is inherently boringMonitoring is inherently boringComputers can do better than peopleComputers can do better than peoplePeople are better than computers at evaluating People are better than computers at evaluating importance of signalsimportance of signals
““SmartSmart”” monitoring will have huge impactmonitoring will have huge impactICUsICUsGeneral care unitsGeneral care unitsHomeHome

Nosocomial Infections
Timely preoperative antibioticsTimely preoperative antibioticsMajor reduction in postMajor reduction in post--surgical infection ratesurgical infection rate
ComputerComputer--assisted antibiotic managementassisted antibiotic managementIn intervention period, those who always got In intervention period, those who always got recommended rx vs. not:recommended rx vs. not:
Lower Lower antiinfectiveantiinfective costs ($102 vs. $427)costs ($102 vs. $427)Total hospital costs ($26,315 vs. $44,865)Total hospital costs ($26,315 vs. $44,865)LOS (10.0 vs. 16.7 days)LOS (10.0 vs. 16.7 days)
Evans RS, NEJM 1998

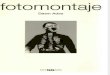
Event Monitor Architecture
Rule editor
Knowledge base
Inference engine(decisions)
Applications (new data)Applications (new data)Applications (new data)
Patient database
Annun-ciators
page, email, write to file,
[real time message]
Coverage List

RCT to Improve Response to Critical Labs
Mean time to rx 11% shorter Mean time to rx 11% shorter For events not meeting labFor events not meeting lab’’s calling criteria (half of s calling criteria (half of events), 21% shorterevents), 21% shorter
Nearly identical for events meeting criteriaNearly identical for events meeting criteriaMean time to resolution 29% shorterMean time to resolution 29% shorterMortality was 7% in intervention group, 13% control Mortality was 7% in intervention group, 13% control group (p=0.19)group (p=0.19)95% physicians pleased to be paged95% physicians pleased to be paged
Kuperman, JAMIA 2000

Coverage-Related Events
Before data showed patients being crossBefore data showed patients being cross--covered covered at 5at 5--fold excess risk of adverse eventfold excess risk of adverse eventAfter computerized After computerized signoutsignout introduction, no introduction, no excess riskexcess risk
Included medicationsIncluded medicationsSimple from informatics perspective but major Simple from informatics perspective but major benefitbenefit
Petersen, Jt Comm Jl

Other Non-IT Inpatient Approaches
IT not only way to improve safety by any meansIT not only way to improve safety by any means66% reduction in preventable ordering ADEs 66% reduction in preventable ordering ADEs with pharmacist participation in ICU roundswith pharmacist participation in ICU rounds
Leape, JAMA, 2000Leape, JAMA, 2000
Building a culture of safety is extremely Building a culture of safety is extremely importantimportant

Outside the Hospital: Problem Areas in which IT Can Help
PrescribingPrescribingMonitoringMonitoringFollowing up important abnormalitiesFollowing up important abnormalities
Results ManagerResults Manager

Prescribing and Monitoring
PrescribingPrescribing——no RCT yet, but results forthcoming soonno RCT yet, but results forthcoming soonObservational data show high error rates in outpatient Observational data show high error rates in outpatient prescriptionsprescriptions
MonitoringMonitoringFew patients on amiodarone receive appropriate Few patients on amiodarone receive appropriate monitoringmonitoring
StelfoxStelfox, 2003, 2003Only about half of patients on thyroid supplement Only about half of patients on thyroid supplement received appropriate monitoringreceived appropriate monitoring
StelfoxStelfox, 2003, 2003

Dilbert

Evidence of Need for Better Lab Follow-up: Ambulatory Area
RMF dataRMF data1/4 of diagnosis1/4 of diagnosis--related malpractice cases were related malpractice cases were attributable to failures in the followattributable to failures in the follow--up system.up system.
AMQUIP dataAMQUIP dataAfter an abnormal mammogram, 37.4% of women After an abnormal mammogram, 37.4% of women did not complete a repeat mammogram within the did not complete a repeat mammogram within the timetime--frame suggested by the radiologistframe suggested by the radiologist
National U.S. dataNational U.S. data35% of patients with abnormal pap smear are lost 35% of patients with abnormal pap smear are lost to followto follow--upup

Results Manager Home Page



Current Status
Trial to assess impact nearly completedTrial to assess impact nearly completedProviders really like the applicationProviders really like the application
Has been hard to keep the operational Has been hard to keep the operational leadership from allowing them to useleadership from allowing them to use
Should improve safety/decrease riskShould improve safety/decrease risk

ReportingMain tool now used to identify adverse eventsMain tool now used to identify adverse events
Yet spontaneous reporting detects only Yet spontaneous reporting detects only about 5% of eventsabout 5% of eventsComputerized detection works much betterComputerized detection works much betterCurrently comparing what yield is from Currently comparing what yield is from spontaneous reporting, executive spontaneous reporting, executive walkroundswalkrounds, claims, claims
Future is computerized detectionFuture is computerized detection

Organized effort to buy rightOrganized effort to buy rightPurchasing principles that strongly reward Purchasing principles that strongly reward higher provider valuehigher provider valuePurchaser accountabilityPurchaser accountabilityPush via plans or directlyPush via plans or directly
Create a Business Case for ProviderCreate a Business Case for ProviderssEmphasize tangible safety leapsEmphasize tangible safety leaps
Mobilize Consumers and PatientsMobilize Consumers and Patients
Leapfrog Purchaser Strategy

Initial Safety ‘Leap’ SummaryAn Rx for RxAn Rx for Rx
Computer Physician Order Entry (CPOE)Computer Physician Order Entry (CPOE)Up to 88% serious drug errors preventedUp to 88% serious drug errors prevented
Practice Makes PerfectPractice Makes PerfectEvidenceEvidence--based Hospital Referral (EHR)based Hospital Referral (EHR)> 20% mortality reduction for 7 complex treatments> 20% mortality reduction for 7 complex treatments
Sick People Need Special Care Sick People Need Special Care ICU Daytime Staffing with CCM Trained M.D.ICU Daytime Staffing with CCM Trained M.D.> 10% mortality reduction> 10% mortality reduction

What are the Three Leaps Worth?
Annual Gain Projected by Dartmouth:Annual Gain Projected by Dartmouth:↓↓ 522,000 serious med errors522,000 serious med errors↓↓ 5858,300 deaths,300 deaths↓↓ 5858,300 X disabilities,300 X disabilities
(if fully implemented in U.S. urban hospitals)(if fully implemented in U.S. urban hospitals)

WHO World Alliance For Patient Safety:Agenda of Research Priorities
To produce an agenda of research priorities for To produce an agenda of research priorities for patient safety research worldwidepatient safety research worldwide
Stratified by development levelStratified by development levelProduce inventory of methodologies used in Produce inventory of methodologies used in patient safety researchpatient safety researchBuild infrastructure for research networks Build infrastructure for research networks across culturesacross culturesFoster research in developing countriesFoster research in developing countries

Signature Initiatives6 network6 network--wide initiativeswide initiativesOne focuses on ITOne focuses on IT
Inpatient CPOEInpatient CPOEOutpatient EHROutpatient EHR
Another on safetyAnother on safetyStandardizing medicationStandardizing medication--related decision supportrelated decision supportImplementing proactive tools to look for ADEs, Implementing proactive tools to look for ADEs, implementing standard webimplementing standard web--based reportedbased reportedMaking more uniform decisions about administrationMaking more uniform decisions about administrationStandardizing information exchanged at transfersStandardizing information exchanged at transfers

Future Potential of IT
Huge, hard to estimateHuge, hard to estimateVery large improvement with medication errorsVery large improvement with medication errors
With surgical errors wonWith surgical errors won’’t be as bigt be as bigYet communication is keyYet communication is key
For many types of errors in outpatient setting For many types of errors in outpatient setting such as monitoring will be enormoussuch as monitoring will be enormous
Bottom line: current systems far from Bottom line: current systems far from FedexFedex level of level of accountability, need IT to get thereaccountability, need IT to get there

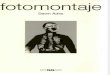
Do First Investment
Don’t Bother
Low
High
Impact
HighCost
CPOE
Bar-coding
Smart pumps
Automated ADE monitoring
Dedicated ICUPharmacist
Pocket drug reference
Preprinted order forms
Medication trainingLimiting
abbreviationsDrug-food interactions
Remove concentrated electrolytes
Intervention database
Unit dose dispensing

What Leadership Can DoCreate a Create a ““systemssystems”” climateclimatePush for systems changes that workPush for systems changes that work
Physician order entryPhysician order entryBarBar--codingcodingChanging pharmacist rolesChanging pharmacist roles? Smart pumps? Smart pumpsComputerized surveillanceComputerized surveillance
Support effective onSupport effective on--going monitoringgoing monitoringPatient safety teamPatient safety teamComputerized surveillanceComputerized surveillance

Inpatient Medication System of the Future
Providers write orders on computerized systems, get Providers write orders on computerized systems, get feedbackfeedback
FaceFace--toto--face counterface counter--detailing for complex problemsdetailing for complex problemsOrders sent directly to pharmacy (review)Orders sent directly to pharmacy (review)Simple orders filled using automationSimple orders filled using automationPointPoint--ofof--care delivery devices linked with ordercare delivery devices linked with order--entry systems dispense medicationsentry systems dispense medicationsAll drugs, patients, personnel barAll drugs, patients, personnel bar--codedcoded
Computerized MAR records what given, whenComputerized MAR records what given, whenAdministration via Administration via ““smartsmart”” devicesdevices
Routine electronic surveillance for ADEs in placeRoutine electronic surveillance for ADEs in place

ConclusionsHealthcare today is inefficient, errorHealthcare today is inefficient, error--prone, prone, of variable qualityof variable qualityIT can substantially improve care by:IT can substantially improve care by:
Bringing decision support to point of careBringing decision support to point of careImproving communicationImproving communicationClosing Closing ““openopen--looploop”” systemssystemsAllowing routine quality measurementAllowing routine quality measurement

Recommended