Indolent forms of T-cell
lymphomas
Philippe Gaulard
Département de Pathologie & Inserm U955
Hôpital Henri Mondor, Créteil, France
XXVI Congreso National de la Sociedad Espanola de Anatomica Patologica,
Cadiz, may 22-24, 2013


Indolent forms of PTCL
- More questions than answers -
What does « indolent » means?
?

Gisselbrecht et al. Blood, 1998 International T-cell lymphoma project,
J Clin Oncol, 2008
The most common PTCL entities are
aggressive!
• Poor efficacy of conventional therapies in most entities
• Yet, limited improvement in the survival of PTCL patients during the last 20 years

• Limited understanding of the pathogenesis of PTCL…
• Difficult recognition (lack of stringent diagnostic marker)
From “low grade” B-cell lymphomas to specific
entities with adapted therapeutic strategies
The exemple of MALT Lymphoma
Zucca et al. J Clin Oncol 2013

Postulated cell of origin
Translocations Other genetic alterations
Main pathways
T- LGL (NK)
T (more rarely T or NK
STAT3 mut
Apoptosis (Fas-FasL), JAK-STAT
ALCL, ALK+ T (Th2?) t(2;5) or t(2;X) (ALK)
JAK-STAT
ALCL, ALK- (subset)
T (Th2?)
t(6;?) ot t(6;7) (IRF4,DUSP22,..)
AITL T (CD4, TFH) TET2, IDH2, DNMT3 mut +3, +5,….
PDGFR
PTCL,NOS T (CD4>CD8), a subset TFH, rarely T
t(5;9), ITK-SYK, TP63 or other p53-rel genes?
Multiple (del 9p,…)
PDGFRSYK, ….
NK/T, nasal-type
NK (more rarely T or T
del6q21-q25) PRDM1,HACE1, AIM1, .. JAK3 mut
PDGFRJAK-STAT EBV
Hepatosplenic (HSTL)
T (more rarely T
Iso 7q(q10) (?) SYK
Enteropathy-type
T (more rarely T
+9q (9q33) (?), trisomy 1p
PTCLs: genetics is limited !
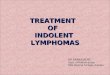
T- and NK-cell lymphomas
Leukemic/diss. nodal extra-nodal prolymphocytic angioimmunoblastic extranodal NK/T nasal-type
T-LGL leukemia peripheral, nos enteropathy-associated
Indolent NK LPD hepatosplenic ( )
Aggressive NK Leuk ALCL, ALK -
ATL/L (HTLV-1) ALCL, ALK + mycosis
Systemic EBV+ LPD Sezary syndrome
Hydroa vaccineforme-like primary cut. CD30+ LPD
subcutaneous panniculitis-like
primary cut.
primary cut aggressive CD8+
primary cut small/medium CD4+
Updated WHO classification (2008)

« Indolent » forms of PTCL
• Entities that are usually indolent: - T-LGL (NK) - Hydroa vaccifiniforme-like - Cutaneous CD30+ T-LPD - ALCL, ALK negative, adjacent to breast implants (seroma-assoiated) - Primary cut small/medium CD4+ TCL (TFH) - CD8+ T-cell LPD (cutaneous, Gastrointestinal,..?) - NK-cell enteropathy
• Entities that are commonly aggressive, however variably indolent: - any entity (?) - more specifically: ° ATLL (smouldering/chronic forms) ° SPTCL ° PTCL-F/AITL (?) ° ALK+ ALCL limited to the skin (?)
• # early lesions (RCD,…): toward the recognition of a premalignant stage in (some) PTCL entities

Indolent Clonal T(NK)-cell
lymphoproliferative diseases
• Not always early in the sense they do not always transform
• Look morphologically malignant, but have a good behaviour, without therapy
• Best examples: - T-LGL, - Lymphomatoid papulosis - Cut small/medium CD4+ lymphoma - NK-cell enteropathy - Hydroa vacciniforme-like LPD,…
• Clinically, important to recognize
How to distinguish from “clonal expansion of T cells” in benign
situations ?

T- CELL LARGE GRANULAR LYMPHOCYTIC (LGL) LEUKEMIA
• indolent disorder
• Peristent increased number of LGLs (>0.5x109/L, >6 mo) - CD3+, CD8+,TCR +, CD57+, CD16+, CD56- - Clonal TCR gene rearrangement
• adults, frequently asymptomatic
• neutropenia ------> recurrent infections, anemia
• frequent serologic abnormalities (RF++, ANA,..)
• moderate splenomegaly (50%)

T- CELL LARGE GRANULAR LYMPHOCYTE (LGL) LEUKEMIA
• Blood smears (++): « small » lymphocytes with azurophilic granules
• Flow cytometry (+++): incl. KIRs expression for NK,
• Genotype
• Bone marrow smears & histology when LGL count <0.5x109/L - « lymphocytic » infiltration * diffuse interstitial +/- sinuses, small clusters of CD8+/TIA1+/GrB+ cells - + reactive nodules - + “maturation arrest” of myeloid series [spleen: red pulp (cords +/- sinuses), liver: sinusoids] (°) Morice WG et al. Blood 2002;99:268; Costes V et al. Br J Hematol, 2002 Lamy Th & Loughran TP. Blood 2011

• A 68 year-old woman, Pneumonia • Hb 10.9 g/dl, WBC: 2.1 g/dl (neutrophils 19%, lympho : 75% with 45% LGLs) • Mild splenomegaly, no hepatomegaly, no lymphadenopathy • BM biopsy scored as normal

CD57
Gr B CD8
CD20
• By flow and IHC: CD3+, CD5+, CD2+, CD7+ , CD4-/CD8+, CD57+, CD56-, GrB+, TCR +
• Clonal rearragement of genes

Clusters of cytotoxic CD8+, Granzyme B+ CD3+ T cells
E Poullot, P Tas, P Gaulard & T Lamy. In press
CD3
Gr B CD8
Bone marrow biopsy usually not required !

Gr B
CD3
Splenectomy usually not required !
• Disease entity, limited to mature clonal proliferations of « small » LGL, with indolent clinical presentation
• Cell lineage: most often T (CD8+, CD57+), more rarely T ; all with restricted expression of KIRs
• Cases with NK-cell phenotype & genotype referred as “Chronic NK LPD” in the 2008 WHO classification
• Proliferation of activated cytotoxic T lymphocytes (CTLs) of unknown antigen specificity : setting of sustained immune stimulation?
• Alteration of the Fas-Fas ligand pathway (blockade of Fas-dependent apoptosis), which could result in: - autoimmune manifestations - lymphoproliferative syndome
• Constitutive activation of STAT3 resulting from somatic STAT3 mutations in 30-40% of both NK and T forms of the disease
STAT3 mut: a novel biomarker unifying T- and NK- cell LGL Leukemia
Koskela et al. NEJM 2012; Jarez et al. Blood 2012
Teramo et al. Blood 2013; Ragala et al. Blood 2013

Algorithm of the diagnosis of LGL leukemia. Adapted from E Poullot, P Tas, P Gaulard & T Lamy. Oncopathol In press

T : CD 3+, CD 3/TCR+, TCR genes
rearranged
«activated cytotoxic T cells»
NK : CD 3s -, CD 3/TCR -
no rearrangement of TCR
genes
T-LGL
leukemia
Aggressive NK-
cell leukemia
Chronic
NK-LPD-
LGL
leukemia
Both cell subsets mediate «non-MHC» restricted cytotoxicity
EBV, del 6q… ?
LGL
Extranodal NK/T
nasal-type

LGL Leukemia HSTL
CD3

Hydroa vacciniforme-like lymphoma of childhood
Quintanilla-Martinez L, Kimura H, Jaffe ES WHO 2008
• Epidemiology: - Mainly children and adolescents from Asia and Native Americans from Central and South America and Mexico. • Etiology: - mainly neoplastic CD8+T-cells and rarely NK-cells (CD56+) - Some show hypersensitivity to mosquito
bites - defective cytotoxic immune response to EBV-infection as a potential cause • Clinical features: - initially a papulovesicular eruption - subsequently ulceration and scarring - commonly sun-exposed skin - seasonal variation
Hydroa vacciniforme-like lymphoma of childhood
Courtesy Prof L Quintanilla-Martinez

Morphology: • Neoplastic cells small to medium in size without significant atypia • Infiltration of the Epidermis to the subcutis • Angiocentricity and angioinvasion
Prognosis: - The clinical course is variable,
- recurrent skin lesions up to 10-15 years, - progression to systemic disease can occur
Quintanilla-Martinez L, Kimura H, Jaffe ES WHO 2008
Hydroa vacciniforme-like lymphoma of childhood
Courtesy Prof L Quintanilla-Martinez

CD3 TIA1 CD8
CD4 CD30 EBER
Courtesy Prof L Quintanilla-Martinez
Hydroa vacciniforme-like lymphoma of childhood
Cytotoxic (GrB+, perf+), most often CD8+ & CD56-, clonal
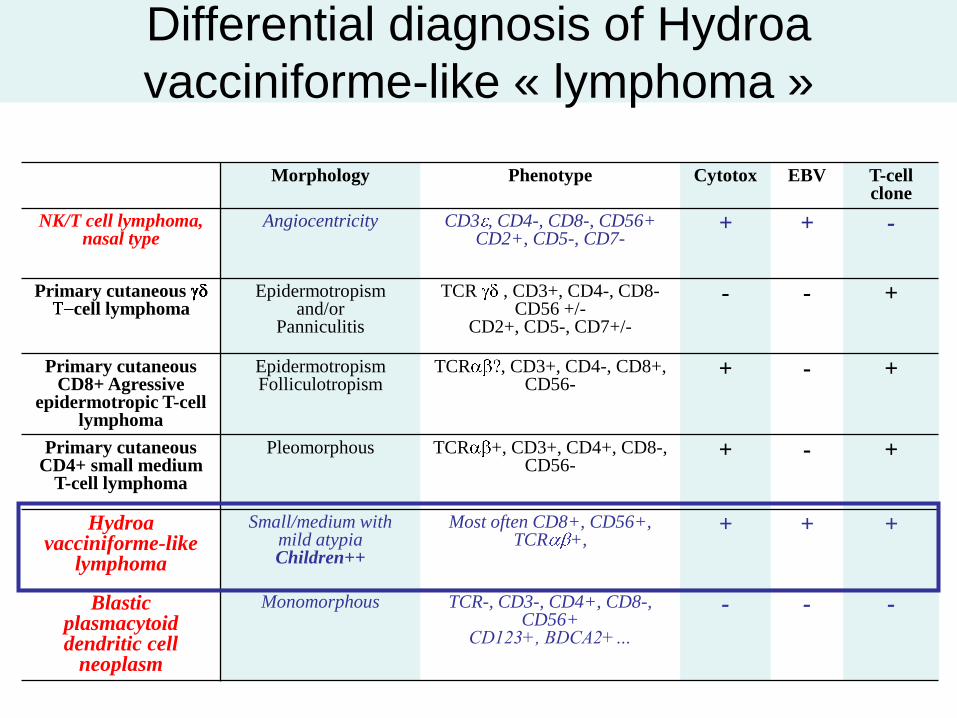
Differential diagnosis of Hydroa
vacciniforme-like « lymphoma »
Morphology Phenotype Cytotox EBV T-cell clone
NK/T cell lymphoma, nasal type
Angiocentricity CD3 , CD4-, CD8-, CD56+ CD2+, CD5-, CD7-
+ + -
Primary cutaneous cell lymphoma
Epidermotropism and/or
Panniculitis
TCR , CD3+, CD4-, CD8- CD56 +/-
CD2+, CD5-, CD7+/-
- - +
Primary cutaneous CD8+ Agressive
epidermotropic T-cell lymphoma
Epidermotropism Folliculotropism
TCR , CD3+, CD4-, CD8+, CD56-
+ - +
Primary cutaneous CD4+ small medium
T-cell lymphoma
Pleomorphous TCR +, CD3+, CD4+, CD8-, CD56-
+ - +
Hydroa vacciniforme-like
lymphoma
Small/medium with mild atypia Children++
Most often CD8+, CD56+, TCR +,
+ + +
Blastic plasmacytoid dendritic cell
neoplasm
Monomorphous TCR-, CD3-, CD4+, CD8-, CD56+
CD123+, BDCA2+…
- - -
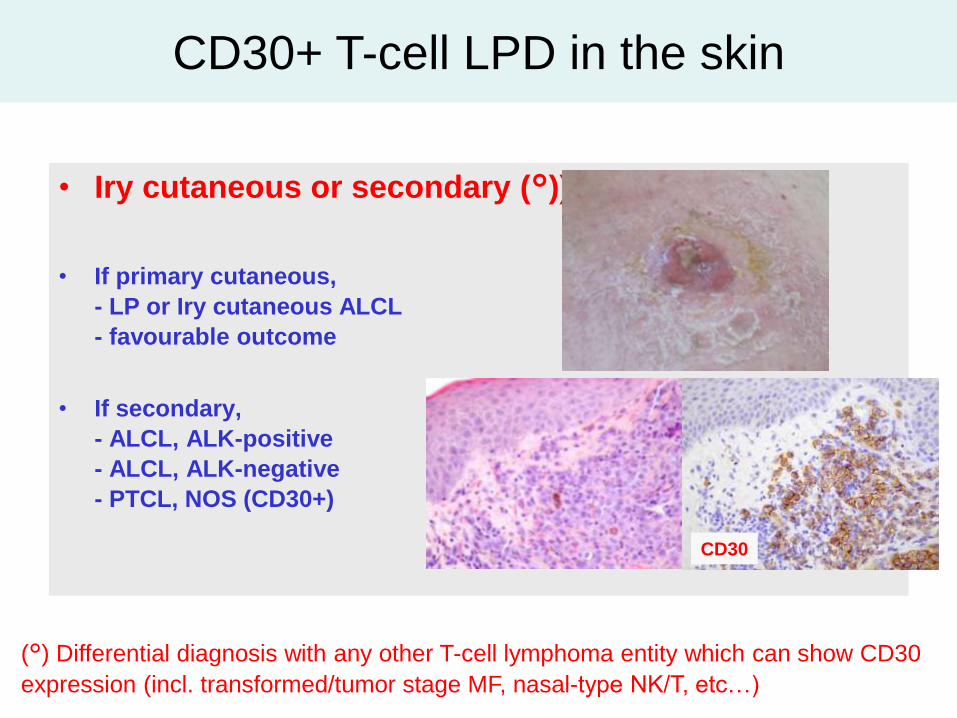
• Iry cutaneous or secondary (°))?
• If primary cutaneous,
- LP or Iry cutaneous ALCL
- favourable outcome
• If secondary,
- ALCL, ALK-positive
- ALCL, ALK-negative
- PTCL, NOS (CD30+)
(°) Differential diagnosis with any other T-cell lymphoma entity which can show CD30
expression (incl. transformed/tumor stage MF, nasal-type NK/T, etc…)
CD30
CD30+ T-cell LPD in the skin
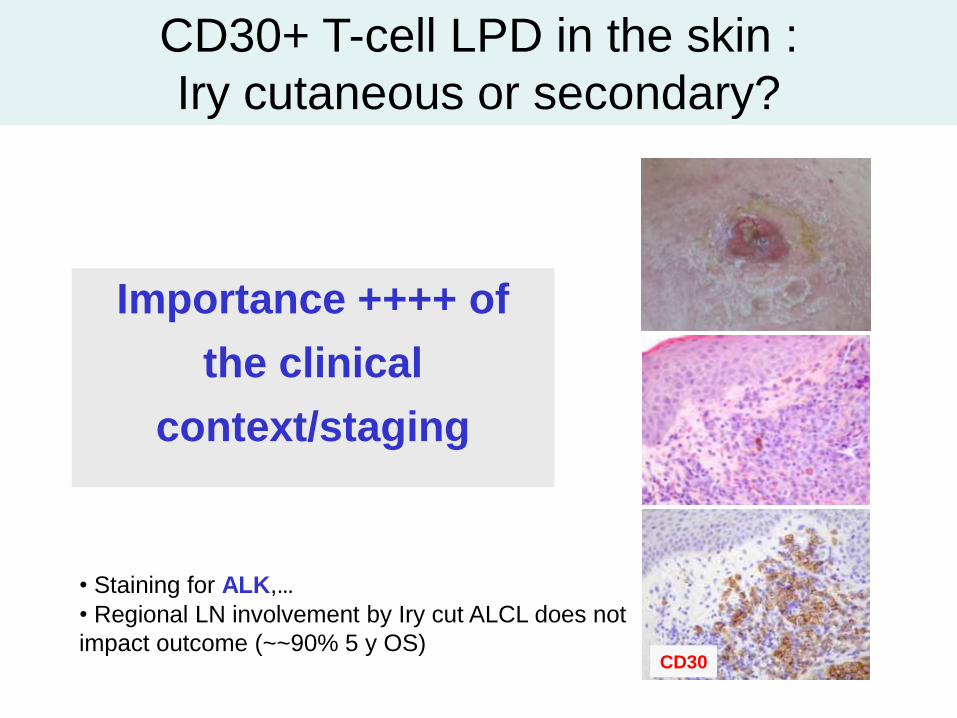
Importance ++++ of
the clinical
context/staging
• Staining for ALK,…
• Regional LN involvement by Iry cut ALCL does not
impact outcome (~~90% 5 y OS) CD30
CD30+ T-cell LPD in the skin :
Iry cutaneous or secondary?

Case A Dogan, EAHP, Uppsala, 2010
ANAPLASTIC LARGE LYMPHOMA, ALK- and breast
implants (« seroma-associated primary ALK-negative
ALCL adjacent to breast implants »)
Kim B et al. Plast Reconstr Surg 2011
CD30 TIA1

• A 61 year-old woman, injured with knifes in 1970, several breast implants since 1980 • 01/2012, large mass + seroma (adjacent to the implant) : biopsies

?

CD30
PAX5
CD8
GrB
CD30+, CD15-, EMA+/- , ALK1- CD20-, CD79a-, PAX5-, CD3-, CD2+, CD5-, CD7-, CD4-, CD8+, TIA1+, GrB+, CD56-, EBV - T-cell clone (PCR )
• « seroma-associated » primary ALK-negative ALCL adjacent to breast implants - atypical presentation with a tumour mass - morphology « Hodgkin-like »
• treatment : 6x CHOP (large mass, 8x12 cm)
• Persistent CR since june 2012

BCA-1=CXCL13
CXCR5 CXCL13 BCL-6 Il6R IL21 CD84 CD40L CD200/OX2 ICOS PD1
TFH
AITL (de Leval et al. Blood 2007)
PTCL-F (Huang et al. AJSP 2009)
Iry cut CD4+ small /medium
pleomorphic
T-cell lymphoma (Rodriguez Pinilla et al. AJSP 2009)
T-cell lymphomas expressing TFH markers ?
Primary cutaneous CD4+ small/medium-sized pleomorphic
T-cell lymphoma

Primary cutaneous CD4+ small/medium sized pleomorphic T-cell
lymphoma
CXCL13 PD1
Rodriguez Pinilla SM, et al. Am J Surg Pathol. 2009;33(1):81-90
Provisional entity of the 2008 WHO classification, most likely identical to cutaneous
« Pseudo-T cell lymphomas » described previously (Cetinozman F et al. Am J Surg Pathol 2012;36)
Diagnostic usefulness of TFH markers in skin
biopsies (PD1, CXCL13,..)
• AITL : common expression (PD1, CXCL13)
• Iry cutaneous CD4+ small/medium-sized PTCL :
common expression (PD1, CXCL13)
• Mycosis fungoides : occasional expression of
PD1, more rarely CXCL13
• Sézary cells
– Common expression of PD1 in both blood and skin Cetinözman F, et al. Am J Surg Pathol 2011
– CXCL13? Picchio MC, et al. Cancer Res 2008;68:7137–46

Indolent CD8+ cutaneous T-cell
lymphoproliferation (ear-type)
Patient 3: nodules of both ears
Petrella T et al. Am J Surg Pathol 2007; 31 Beltraminelli et al., JCP, 2009; Li et al., Histopathology, 2009; Suchak et al., JCP, 2009
Géraud et al., BJD, 201; Swick at al., JCP, 2011; Zeng et al, JCP, 2012
Coutesy, T Petrella

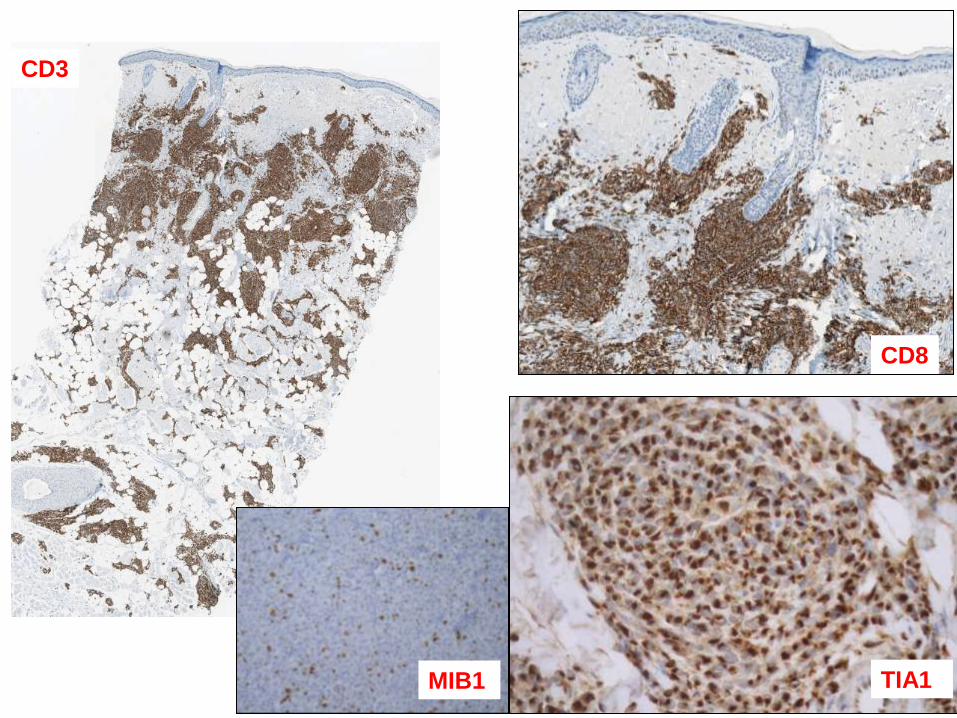
CD3
CD8
TIA1 MIB1
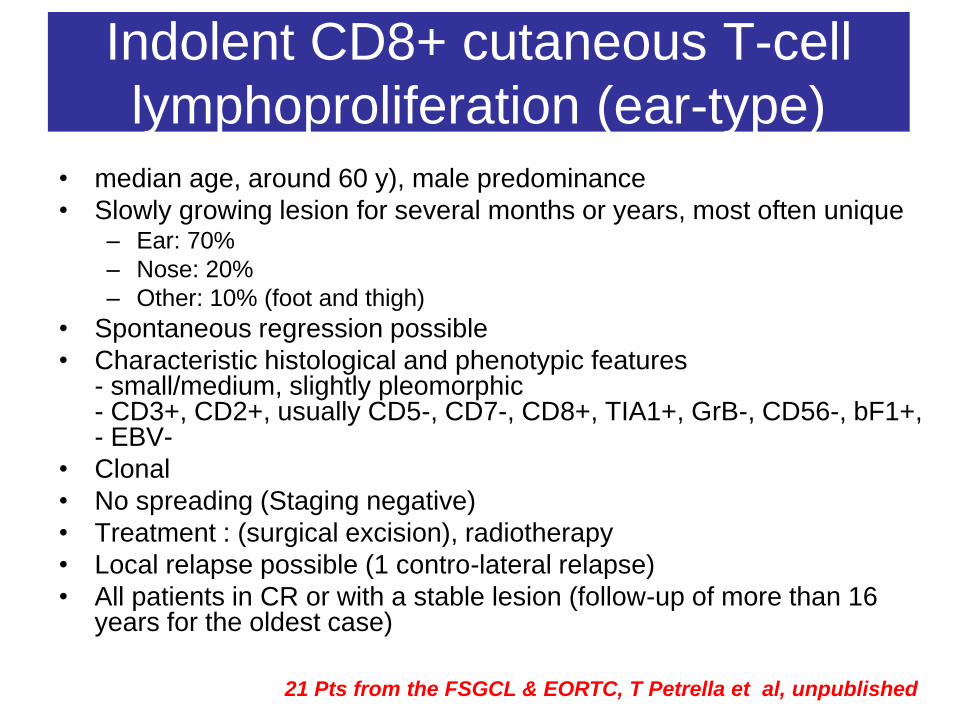
• median age, around 60 y), male predominance
• Slowly growing lesion for several months or years, most often unique – Ear: 70%
– Nose: 20%
– Other: 10% (foot and thigh)
• Spontaneous regression possible
• Characteristic histological and phenotypic features - small/medium, slightly pleomorphic - CD3+, CD2+, usually CD5-, CD7-, CD8+, TIA1+, GrB-, CD56-, bF1+, - EBV-
• Clonal
• No spreading (Staging negative)
• Treatment : (surgical excision), radiotherapy
• Local relapse possible (1 contro-lateral relapse)
• All patients in CR or with a stable lesion (follow-up of more than 16 years for the oldest case)
21 patients (FSGCL and EORTC CL groups) Indolent CD8+ cutaneous T-cell
lymphoproliferation (ear-type)
21 Pts from the FSGCL & EORTC, T Petrella et al, unpublished

Yet, this lesion doesn’t fit into any category of the WHO
nor EORTC classifications
• Is it a real low grade lymphoma or pseudolymphoma? - histologically it looks like a lymphoma (atypical cells,
clonality, loss of antigens, relapses)
- clinically it is not a lymphoma (localized disease, good
outcome
• Why this ear tropism (+ nose)? - Is there a local trigger agent (infectious, chemical, physical) ?
• Genetic abnormalities?
• How to designate this lesion? - This lesion must not be confused with more aggressive
lymphomas
Yet, the term “Indolent CD8+ cutaneous lymphoid proliferation (ear-
type)” seems to be appropriate?
Indolent CD8+ cutaneous T-cell
lymphoproliferation (ear-type) - more questions than answers -
• 7 patients - histologically it is a lymphoma (atypical cells, clonality, loss of
antigens, relapses)
- clinically it is not a lymphoma (localized disease, good
outcome
• Why this ear tropism (+ nose)? - Is there a local trigger agent (infectious, chemical, physical) ?
• Genetic abnormalities?
• How to designate this lesion? - This lesion must not be confused with more aggressive
lymphomas
Similar Indolent CD8+ T-cell
lymphoproliferation may occur in the GI tract (Dr Perry et al. EAHP Lisbonne 2012, Abstract LYS017)

ileon
colon
• A 31 year-old man, presenting without chonic diarrhea, without B symptoms • Multiple polypoid lesions (ileon, colon) at endocopy • Clinical staging & laboratory tests: normal

CD3 CD20
CD8 TiA1
• Immunophenotype : CD20-, CD2+, CD3+, CD5+, CD7+, CD4-, CD8+, CD56-,
CD30-, TiA1+, GrB-, proliferative index <10% (Ki67), EBERs negative
• T cell clone.
PTCL, NOS????
Or…

Conclusion
• This patient was given polychemotherpy for PTCL,NOS
(CHOP, DHAOX) without CR; therapay was stopped a year
ago: patient well but with persistent non evolutive lesions
(same pathological features)
• 6 others similar cases reported by Dr Perry
• Unknown physiopathology: continuous stimulation by
an unknown antigen inducing a clonal T-cell response ???
• Similarities with:
- NK-cell enteropathy: a benign NK-cell lymphoproliferative
disease mimicking intestinal lymphoma (Mansoor et al,
Blood 2011)
- Cutaneous indolent CD8+ lymphoproliferation of the ears
(Petrella et al, AmJSurgPath 2007)
How should we call this indolent clonal T-cell
lymphoproliferative disease?
Indolent CD8+ T-cell lymphoproliferative disorder of
the GI tract (Dr Perry et al. EAHP Lisbonne 2012, Abstract LYS017)

CD3 CD56
8 patients, 27-68 yo
Asymptomatic or variable
abdominal symtoms
Single or multiple GI sites
Endoscopy: superficial +/-
ulcerated lesions
No enteropathy
CD3+, CD5-, CD4-/CD8-,
CD56+, GrB+, EBV-, TCR
polyclonal
Alive WD 22 to 120 months
after diagnosis (5/8 untreated)
Mansoor et al. Blood 2011
NK-cell enteropathy
« Indolent » forms of PTCL
• Entities that are usually indolent: - T-LGL (NK) - Hydroa vaccifiniforme-like - Cutaneous CD30+ T-LPD - ALCL, ALK negatif adjacent to breast implants (seroma) - Primary cut small/medium CD4+ TCL (TFH) - CD8+ T-cell LPD (cutaneous, Gastrointestinal,..?) - NK-cell enteropathy
• Entities that are commonly aggressive, however variably indolent: - any entity (?) - more specifically: ° ATLL (smouldering/chronic forms) ° SPTCL ° PTCL-F/AITL (?) ° ALK+ ALCL limited to the skin (?)
• # early lesions (RCD,…): toward the recognition of a premalignant stage in (some) PTCL entities
Adult T-cell leukaemia/lymphoma
(HTLV1+) (ATLL)
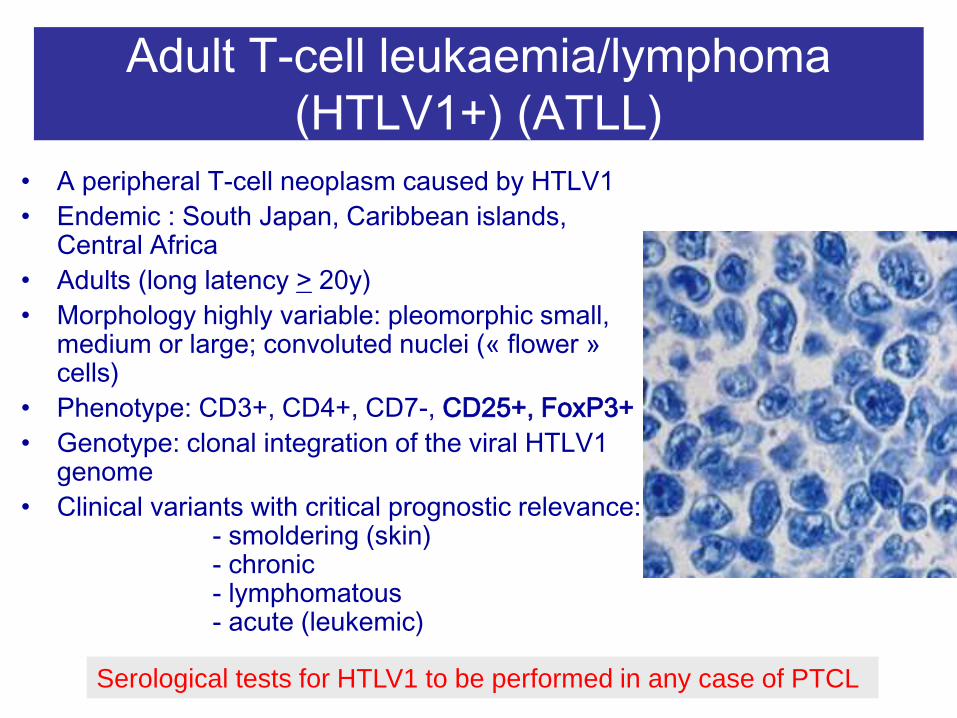
• A peripheral T-cell neoplasm caused by HTLV1
• Endemic : South Japan, Caribbean islands, Central Africa
• Adults (long latency > 20y)
• Morphology highly variable: pleomorphic small, medium or large; convoluted nuclei (« flower » cells)
• Phenotype: CD3+, CD4+, CD7-, CD25+, FoxP3+
• Genotype: clonal integration of the viral HTLV1 genome
• Clinical variants with critical prognostic relevance: - smoldering (skin) - chronic - lymphomatous - acute (leukemic)
Serological tests for HTLV1 to be performed in any case of PTCL

Frequency Skin involvement
Non-cutaneous
sites
Lymphocytosis
5 year OS
Acute 65% Common (50%)
Spleen, liver,LN,…
Yes 5%
Lymphoma 30% Common Adenopathies,.. No 5%
Chronic <5% Common Adenopathies Liver, lung,…
Rare 27%
Smoldering <5% Constant …. No 62%
Leucémie/lymphome T de l’adulte (HTLV-1) Adult T-cell leukaemia/lymphoma (HTLV1+)
(ATLL)
•Overall, the skin is the most common extralymphatic site of involvement (>50%)
•Diagnostic importance of skin biopsy specially in chronic & smoldering variants

Leucémie/lymphome T de l’adulte (HTLV-1)
Forme indolente…
CD25 (IL2®)
Adult T-cell leukaemia/lymphoma (HTLV1+) (ATLL)
Pathological features

ALK-postive ALCL limited to the skin:
some cases with indolent outcome, at
least in children?
Oschlies et al. Haematologica 2013
« In these 6 pediatric cases of ALK+ ALCL, therapy confined to local measures
was sufficient to induce cure. »

Angioimmunoblastic
T-cell lymphoma
AITL
PTCL-F
TFH
Subset of CD4+
cutaneous T-cell
lymphomas
Follicular variant of PTCL,NOS : a subgroup with variable outcome, most likely related to AITL?
PTCL, NOS
With TFH
phenotype
(« TFH-like »)

Is the group of so-called « follicular PTCL » an “early”
TFH-derived PTCL and is it related to AITL?
De Leval et al. AJSP, 2002
M Qubaja et al. Hum Pathol 2008
CM Bacon et al. Br J Haematol 2008
Y-L Huang et al. AJSP, 2009
PD1 PD1

Follicular variant of PTCL, NOS ?
• Nodular growth pattern
– may mimick follicular
lymphoma
– small/medium sized T cells
• CD4+ Bcl6+ CD10 +/-,
• Expression of TFH markers
(CXCL13+, PD1+, ICOS+)
• t(5;9) translocation (SYK-ITK
fusion) in a subset of cases
• Relationship to AITL?
de Leval L et al. AJSP 2001; Streubel B et al. Leukemia 2006; Bacon C et al. Br J
Haematol 2008; Qubaja M et al. Human Pathol 2008; Huang L et al. AJSP 2009
CD3
Pt 23: t(5;9) positive
PTCL,NOS with follicular pattern (follicular
variant)

1998:
• 62 y old man
• B symptoms
• Cervical ADP
• Skin rash
• Hyper glob, Coombs test+
1998
2006
2007
The spectrum of AITL might be wider than expected
PD1
PD1
PD1
M Qubaja et al. Hum Pathol 2008
Y-L Huang et al. AJSP, 2009

Clonality # Malignancy
Some (rare) «PTCL» entities
with indolent behaviour
- terminology?
- need to be recognized
- mostly extranodal
(cutaneous or mucosa)
Cytotoxic (CD8+/NK) T-cell
LPD in the skin or GI tract: a
novel subgroup/entity?
Uncover the oncogenic
pathways
Disease subgroups in other
entities ?

Recognition needed !
ILSG, 1996
R Delarue et al. Blood 2013 Kluin-Nelemans et al. NEJM 2012
The exemple
of MCL
R-CHOP/R-DHAP + ASCT
• In addition, indolent forms of MCL are recognized !
Recommended



![Indolent T- and NK-cell lymphoproliferative disorders of ... · extranodal site of occurrence of non-Hodgkin lymphomas [1]. Most GI lymphomas are of B-cell lineage, and T-cell lymphomas](https://img.pdfslide.us/doc/110x75/5f93d293a1c10d3ed34c6b11/indolent-t-and-nk-cell-lymphoproliferative-disorders-of-extranodal-site-of.jpg)