4/15/2016
1
In-Stent Restenosis: The Tail IS Wagging the Dog
Michael S. Conte MDDivision of Vascular and Endovascular Surgery
UCSF Heart and Vascular CenterUCSF Vascular Symposium 2016
Disclosures
•NONE
IF YOU WERE A PAD PATIENT:What is the minimum efficacy threshold you would accept for an invasive treatment strategy for life-style limiting claudication?
1. >50% likelihood of improvement for at least one year
2. >50% likelihood of improvement for at least two years
3. >50% likelihood of improvement for at least three years
PAYOR Restenosis: The Continuing Challenge for Peripheral Vascular Intervention
• Most severe in the infrainguinalvessels
• Limited Current Strategies– Cutting balloons– Covered stents– Brachytherapy– Atherectomy– Drug-eluting stents, balloons
• Promising data in early studies– Gene and cell-based therapies
• Remains the greatest unmet need in Vascular Intervention

4/15/2016
2
Risk Factors for Restenosis
• Female gender• Long-segment disease (>15 cm)• Small caliber artery (≤5 mm)• Extensive calcification • Stent fracture• Poor runoff• Systemic inflammation (e.g. elevated hsCRP)• Diabetes (?)
Strongest Predictors of Endovascular Treatment
Failure in PAD
• POOR SELECTION
• OVERUTILIZATION OF INTERVENTIONS-ESPECIALLY IN CLAUDICATION
TASC A-Endo Rx of choice
TASC D- Surgery Rx of choice
TASC B- Endo preferred
TASC C- Surgery preferred
Relevant in 2015??
Needed to address current limitations– Atherosclerotic burden, calcification– High rates of restenosis– High prevalence of permanent implants; challenges of ISR
Evolution of Balloon Angioplasty for PVI– Improve lumen gain– Reduce dissection– Reduce Restenosis rates
Improvements in stents for femoropopliteal disease– Drug elution to reduce restenosis– Woven nitinol design to increase flexibility and reduce
fracture in highly mobile vessels
Improving Technology for PVI

4/15/2016
3
no control
no contol
p=.0001
p=.84
p=.01
p=.377
p=.028
p=.01
p=.035
p=.01
p=.227
p=.491
no contol
p=.001
0 20 40 60 80 100 120
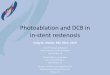
Durability I
Durability II
Resilient
Super
ABSOLUTE
FAST
ASTRON
**Thunder
**Fempac
**PACIFIER
**SIROCCO I
**SIROCCO II
STRIDES
Zilver PTX
BMS
DCB
DES
ControlIntervention
Improving Technology for SFA Disease
Lesions in the Regulatory Trials Generally <10 cm (TASC A/B)
Options for TASC C/D SFA Disease
Estimated 2-yr Patency (%)
POBA
PTA+ BMS (or DES)
Atherectomy +/- adjunct
Endoluminal stent graft
Fem-Pop Bypass GraftingVein (AK or BK)
Prosthetic (AK)
Prosthetic (BK)
20-30
30-60
30-50
40-60
70-80
65-80
40-60
CLAUDICATION MATH for Bilateral TASC C/D Disease:
Endo patency 1st limb at 2 years= 0.4-0.6Endo patency 2nd limb at 2 years = 0.4-0.6
Likelihood of Clinical Success at 2 years:Probability of anatomic success in two legs= 0.16-0.36
�150mm FP lesions�50% SES failure
at 1 yr
J Vasc Surg 2012;55:1001-7.

4/15/2016
4
Armstrong Ej et al Cath Cardiovasc Interv 2013; 82:1168-74
In-Stent Restenosis: The Ongoing Challenge for Vascular Intervention
4% 6%9%
8% 10% 10%12%
17%
10%
18%
23%21% 23% 19% 21%
26%
27%
28%
0%
10%
20%
30%
40%
50%
2003 2004 2005 2006 2007 2008 2009 2010 2011
Critical Limb Ischemia
Claudication
22%
29% 29% 30% 31%
38%
43%
38%
Proportion of all LEB (N=3,504) performed as secondary procedures, By indication and year
72% increase, p<.001
RESTENOSIS IS THE NEW VASCULAR EPIDEMIC
Growing impact of restenosis on the surgical treatm ent of peripheral arterial disease. Jones D et al; JAHA 2013
Impact of Treatment Failure on Surgical Options in PAD
• Many advocate “endovascular first” treatment strategieso Presumed harmless as long as bypass targets
remain intact
o Stakes may increase with each PVI
• However, prior work has suggested that bypass following a failed prior peripheral endovascular intervention (PVI) is associated with poorer outcomeso BASIL trial, Bradbury AW, et al, J Vasc Surg, 2010o Nolan BW, et al, J Vasc Surg, 2011
o Simons JP, et al, J Vasc Surg, 2012
Growing impact of restenosis on the surgical treatm ent of peripheral arterial disease. Jones D et al; JAHA 2013
Propensity score adjustment included approximately 20 patient-level, anatomic and surgical variables
The difference in outcomes is increasing with observation time

4/15/2016
5
What are the potential explanations for inferior bypass outcomes after
PVI failure?• Systemic Factors (i.e. Bad Patient)
• Being a poor surgical candidate associates with “pushing the envelope” in PVI
• Change in DANA to more distal target
• Embolization of runoff vessels in calf and foot
• Target artery inflammation/injury from catheter and wire manipulations
• Delay in effective revascularization for CLI–further tissue loss, infection worsens limb stage
End of nitinolstent
Fem-tib for limb salvage after failed full metal jacket for claudication(fortunately, did OK)
Was a “bridge burned”? Would 100 of these bypass grafts do as well as 100 fem-pop BPGs?
Is treatment failure worse than the natural progression of disease?
Everything we do has the potential for negative, unintended consequences
Those who don’t manage those consequences may lack full perspective

4/15/2016
6
In treating lifestyle limiting claudication, shared decision-making should include honest discussions about the durability of the intervention and the likelihood of sustained functional improvement, as well as the possible negative sequelae of treatment failure
Vascular SpecialistsIndustry Professional Societies
Evidence-Based Practice in PAD?
We are going to have to become MORE SELECTIVE about who we treat, and how
we treat them, to demonstrate EFFECTIVENESS and VALUE
[Fewer Procedures, Better Outcomes]
Recommended