“MAKING A LAUNCH STRATEGY FOR A NEW BRAND OF AN EMERGING
COMPANY IN THE INTERNATIONAL AND DOMESTIC MARKET” by Diptarup Biswas
Dissertation submitted to the Rajiv Gandhi University Of Health Science, Karnataka, Bangalore In partial fulfillment of the requirements for the degree of MASTER OF PHARMACY IN PHARMACEUTICAL MARKETING AND MANAGEMENT Under the guidance of Dr.V Kusum Devi (H.O.D) Department of Pharmaceutical Marketing and Management Al – Ameen College of Pharmacy Bangalore – 560027 March 2010
COPYRIGHT
Declaration by the Candidate
I here by declare that the Rajiv Gandhi University of Health Sciences,
Karnataka shall have the rights to preserve, use and disseminate this
dissertation / thesis in print or electronic format for academic / research
purpose.
Date: March 2010
Place: Bangalore
DIPTARUP BISWAS
© Rajiv Gandhi University of Health Sciences, Karnataka
ii
Declaration by the Candidate
I hereby declare that this dissertation/ thesis entitled “Making a launch
strategy for a new brand of an emerging company in the international
and domestic market” is a bonafide work carried out by me under the kind
guidance of Dr. V Kusum Devi, (H.O.D) Department of Pharmaceutical
Marketing and Management, Al-Ameen College of Pharmacy, Bangalore
Date: March 2010
Place: Bangalore
DIPTARUP BISWAS
iii
CERTIFICATE BY THE GUIDE This is to certify that the dissertation entitled
“MAKING A LAUNCH STRATEGY FOR A NEW BRAND OF AN EMERGING COMPANY IN THE INTERNATIONAL AND DOMESTIC MARKET” is a bonafide research work done by
DIPTARUP BISWAS
In partial fulfillment of the requirement for the degree of
Master of Pharmacy in Pharmaceutical Marketing and Management
Date : March 2010 Place: Bangalore
Signature of the Guide
Dr. V Kusum Devi HOD
Dept. of Pharmaceutical Marketing and Management
iv
CERTIFICATE OF CO-GUIDE
This is to certify that the dissertation entitled “Making a launch strategy for a
new brand of an emerging company in the international and domestic
market” is a bonafide research work carried out by Diptarup Biswas under the
co-guidance of Dr. Anjan Roy.
Dr. Anjan Roy
Managing Director
R L FINE CHEM
v
ENDORSEMENT BY THE HOD, PRINCIPAL/HEAD OF THE INSTITUTION
This is to certify that the dissertation entitled Making a launch strategy for a
new brand of an emerging company in the international and domestic
market” is a bonafide research work carried out by Diptarup Biswas under the
guidance of Dr.V Kusum Devi (HOD)
Department of Pharmaceutical marketing and management, Al-Ameen College of Pharmacy, Bangalore Dr. V Kusum Devi HOD Dept. Pharmaceutical Marketing and Management Al-Ameen College of Pharmacy Bangalore 560027
Prof. B.G Shivananda Principal Al-Ameen College of Pharmacy Bangalore 560027
Date : March 2010 Place : Bangalore
Date : March 2010 Place : Bangalore
vi
ACKNOWLEDGEMENT
As I begin to reflect on to the magnitude of this project, I am reminded of the
kindness, support and affection rendered to me by selfless people to whom I am grateful.
I am indebted to my esteemed guide Dr. V Kusum Devi, HOD, Department of
Pharmaceutical marketing and management, for her valuable guidance, her advice and
constant encouragement, which saw me through the course of my research work.
I extended my sincere gratitude to Mr. Ashoke Bhattacharya (Vice President, R
L Fine Che)., Mr. Pawan K. Ghai (Marketing Head, RL Fine Chemicals), Mr Anjan
Ray (Managing Director, R L Fine Chem), Mr. P V Prasad (General manager, Centum
Pvt. Ltd), Dr. Asha N, Mr. Indu Sankar (Asst. Manager, International Procurement,
Manipal) for providing me valuable help and guidance through out my academic period
here.
I am thankful to “Almighty” and my “Guru-dev” for showering their grace and
blessing on me and helping me to overcome every obstacle I faced till now in my life.
I am blessed indeed to have such supportive, caring, and loving Parents, and it is
to them that I dedicate this thesis.
vii
I also want to thank my late Grand father, Choto pisi and Pisay-mosai, Mejo pisi
and Pisay mosai, Chanu pisi, Mala kakimuni, Jethu and Jemma for their support and
blessings.
I would be failing in my duty, if I do not express my heartfelt thanks to my
dearest friends, Gayatri, Siddharth, Rohit, Pasa, Chinmaya, Pankaj, Amitava, Trishna,
Snigdha, Sourab, Deena, Priyanka, Shruti, Suman, my juniors Pradipta, Saptarshi,
Soumoditta, Jaydeep, Chandana, Shubojit and seniors Aditya bhai, Viswas bhai, Sardul
bhai for their immense love, help, encouragement and support and without which I may
not have completed this work successfully.
I am also indebted to all the Cardiologists, MD Internal medicine, General
practitioners and Pharmacists/Chemists across Bangalore and Kolkata, who
participated in the primary market research and provided their comments and views that
laid the foundation of this work.
And lastly I would like to thank all those who have directly or indirectly helped
me getting through this project successfully.
Date: March 2010
Place: Bangalore Diptarup Biswas
viii
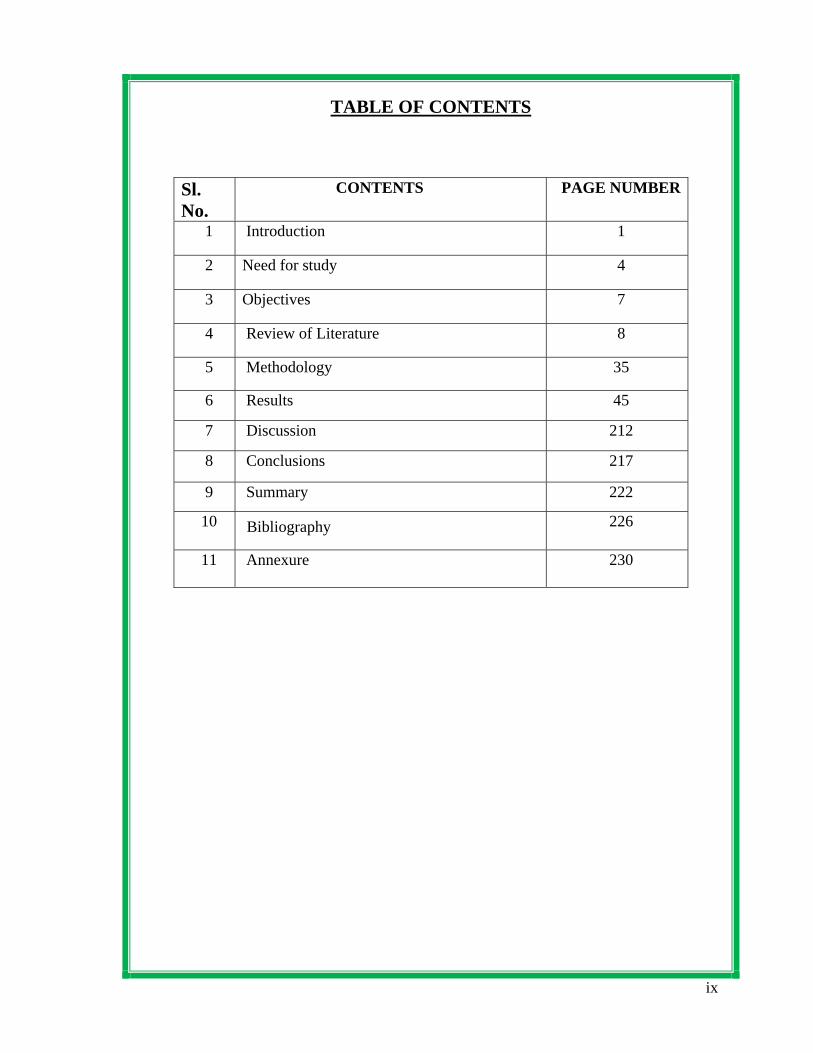
TABLE OF CONTENTS
ix
Sl. No.
CONTENTS PAGE NUMBER
1 Introduction 1
2 Need for study 4
3 Objectives 7
4 Review of Literature 8
5 Methodology 35
6 Results 45
7 Discussion 212
8 Conclusions 217
9 Summary 222
10 Bibliography 226
11 Annexure 230
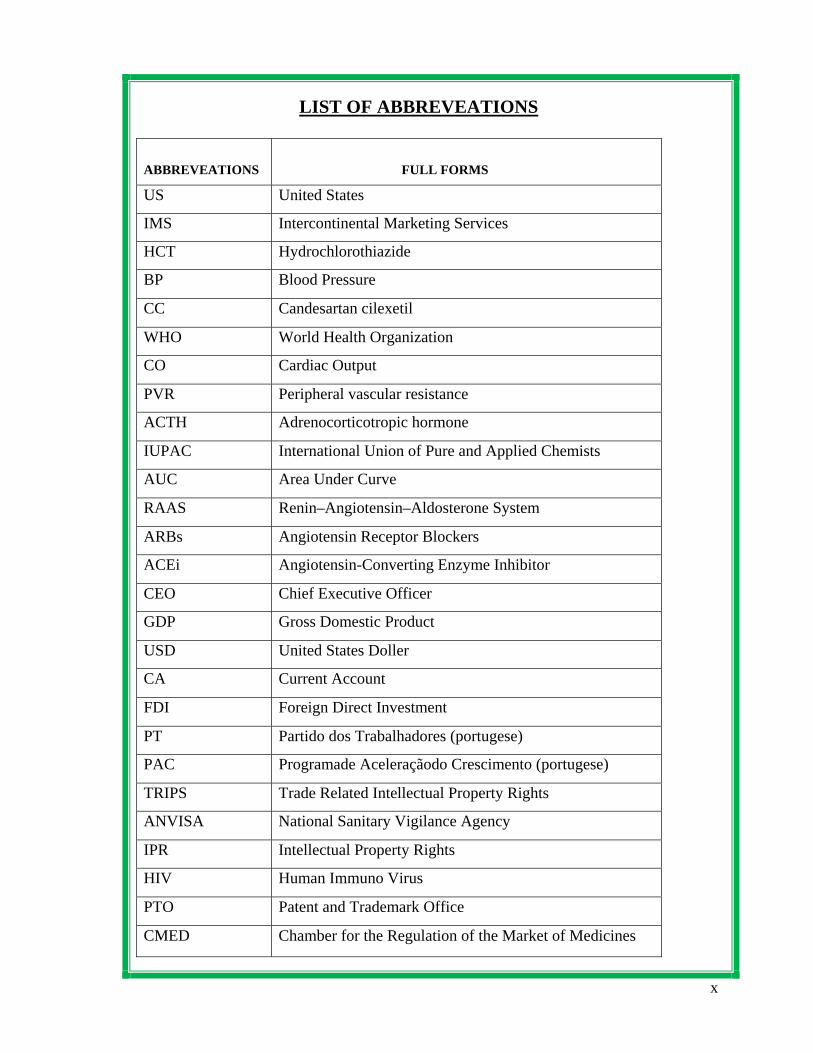
LIST OF ABBREVEATIONS
x
ABBREVEATIONS
FULL FORMS
US United States
IMS Intercontinental Marketing Services
HCT Hydrochlorothiazide
BP Blood Pressure
CC Candesartan cilexetil
WHO World Health Organization
CO Cardiac Output
PVR Peripheral vascular resistance
ACTH Adrenocorticotropic hormone
IUPAC International Union of Pure and Applied Chemists
AUC Area Under Curve
RAAS Renin–Angiotensin–Aldosterone System
ARBs Angiotensin Receptor Blockers
ACEi Angiotensin-Converting Enzyme Inhibitor
CEO Chief Executive Officer
GDP Gross Domestic Product
USD United States Doller
CA Current Account
FDI Foreign Direct Investment
PT Partido dos Trabalhadores (portugese)
PAC Programade Aceleraçãodo Crescimento (portugese)
TRIPS Trade Related Intellectual Property Rights
ANVISA National Sanitary Vigilance Agency
IPR Intellectual Property Rights
HIV Human Immuno Virus
PTO Patent and Trademark Office
CMED Chamber for the Regulation of the Market of Medicines
xi
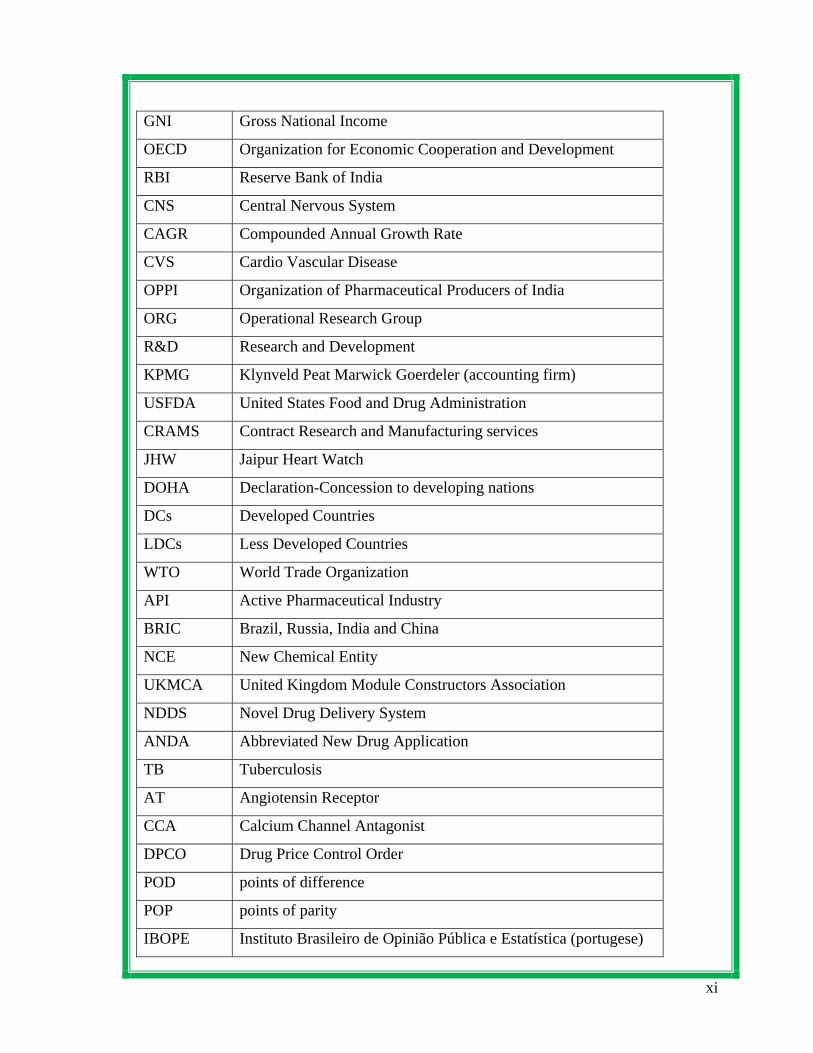
GNI Gross National Income
OECD Organization for Economic Cooperation and Development
RBI Reserve Bank of India
CNS Central Nervous System
CAGR Compounded Annual Growth Rate
CVS Cardio Vascular Disease
OPPI Organization of Pharmaceutical Producers of India
ORG Operational Research Group
R&D Research and Development
KPMG Klynveld Peat Marwick Goerdeler (accounting firm)
USFDA United States Food and Drug Administration
CRAMS Contract Research and Manufacturing services
JHW Jaipur Heart Watch
DOHA Declaration-Concession to developing nations
DCs Developed Countries
LDCs Less Developed Countries
WTO World Trade Organization
API Active Pharmaceutical Industry
BRIC Brazil, Russia, India and China
NCE New Chemical Entity
UKMCA United Kingdom Module Constructors Association
NDDS Novel Drug Delivery System
ANDA Abbreviated New Drug Application
TB Tuberculosis
AT Angiotensin Receptor
CCA Calcium Channel Antagonist
DPCO Drug Price Control Order
POD points of difference
POP points of parity
IBOPE Instituto Brasileiro de Opinião Pública e Estatística (portugese)
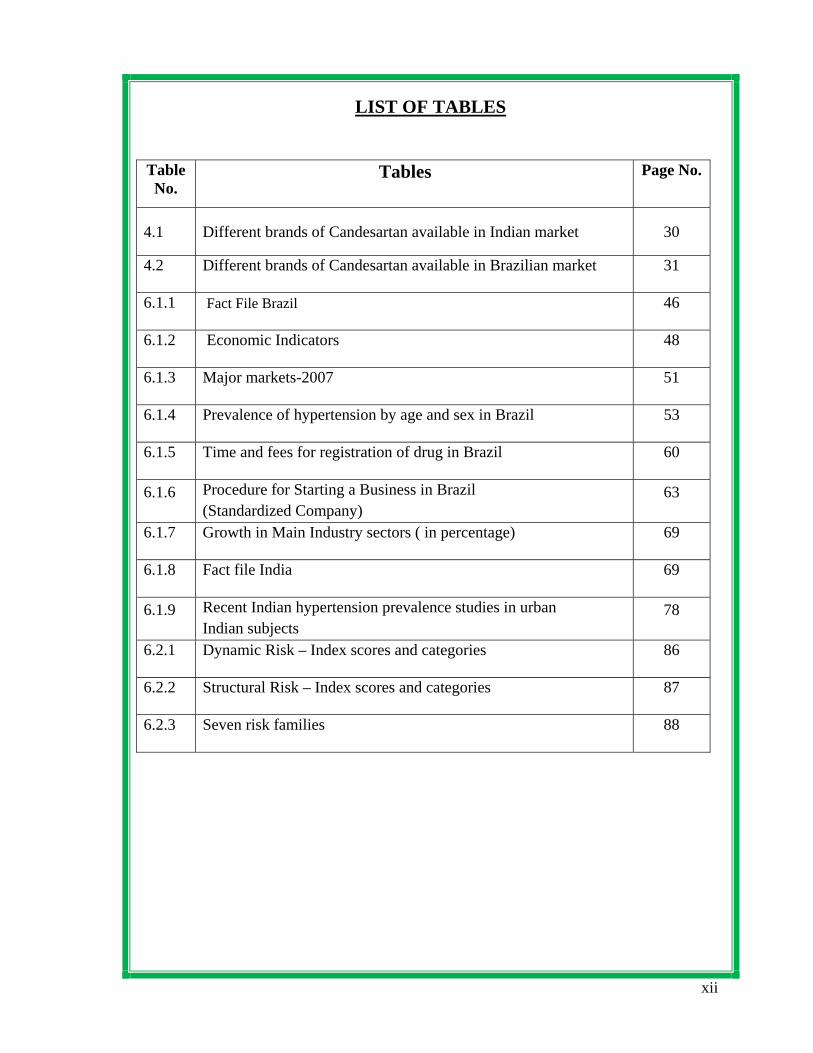
LIST OF TABLES
Table No.
Tables Page No.
4.1 Different brands of Candesartan available in Indian market 30
4.2 Different brands of Candesartan available in Brazilian market 31
6.1.1 Fact File Brazil 46
6.1.2 Economic Indicators 48
6.1.3 Major markets-2007 51
6.1.4 Prevalence of hypertension by age and sex in Brazil 53
6.1.5 Time and fees for registration of drug in Brazil 60
6.1.6 Procedure for Starting a Business in Brazil (Standardized Company)
63
6.1.7 Growth in Main Industry sectors ( in percentage) 69
6.1.8 Fact file India 69
6.1.9 Recent Indian hypertension prevalence studies in urban Indian subjects
78
6.2.1 Dynamic Risk – Index scores and categories 86
6.2.2 Structural Risk – Index scores and categories 87
6.2.3 Seven risk families 88
xii
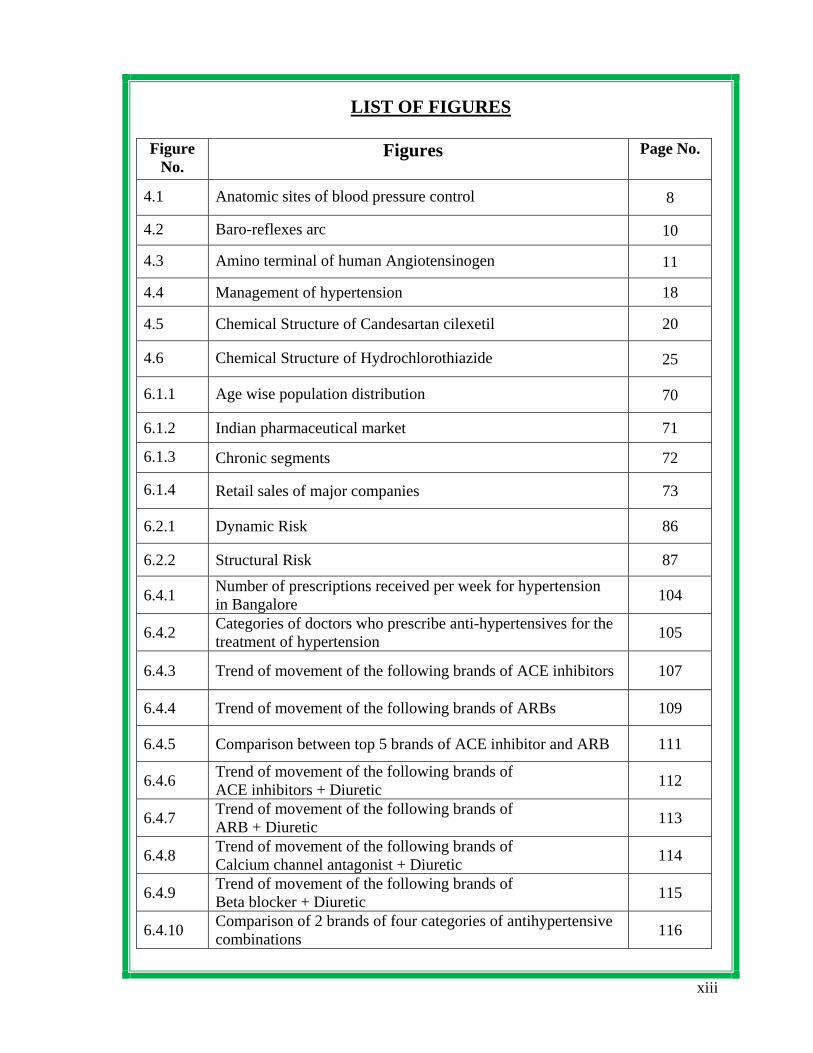
LIST OF FIGURES
xiii
Figure No.
Figures Page No.
4.1 Anatomic sites of blood pressure control 8
4.2 Baro-reflexes arc 10
4.3 Amino terminal of human Angiotensinogen 11
4.4 Management of hypertension 18
4.5 Chemical Structure of Candesartan cilexetil 20
4.6 Chemical Structure of Hydrochlorothiazide 25
6.1.1 Age wise population distribution 70
6.1.2 Indian pharmaceutical market 71
6.1.3 Chronic segments 72
6.1.4 Retail sales of major companies 73
6.2.1 Dynamic Risk 86
6.2.2 Structural Risk 87
6.4.1 Number of prescriptions received per week for hypertension in Bangalore 104
6.4.2 Categories of doctors who prescribe anti-hypertensives for the treatment of hypertension 105
6.4.3 Trend of movement of the following brands of ACE inhibitors 107
6.4.4 Trend of movement of the following brands of ARBs 109
6.4.5 Comparison between top 5 brands of ACE inhibitor and ARB 111
6.4.6 Trend of movement of the following brands of ACE inhibitors + Diuretic 112
6.4.7 Trend of movement of the following brands of ARB + Diuretic 113
6.4.8 Trend of movement of the following brands of Calcium channel antagonist + Diuretic 114
6.4.9 Trend of movement of the following brands of Beta blocker + Diuretic 115
6.4.10 Comparison of 2 brands of four categories of antihypertensive combinations 116
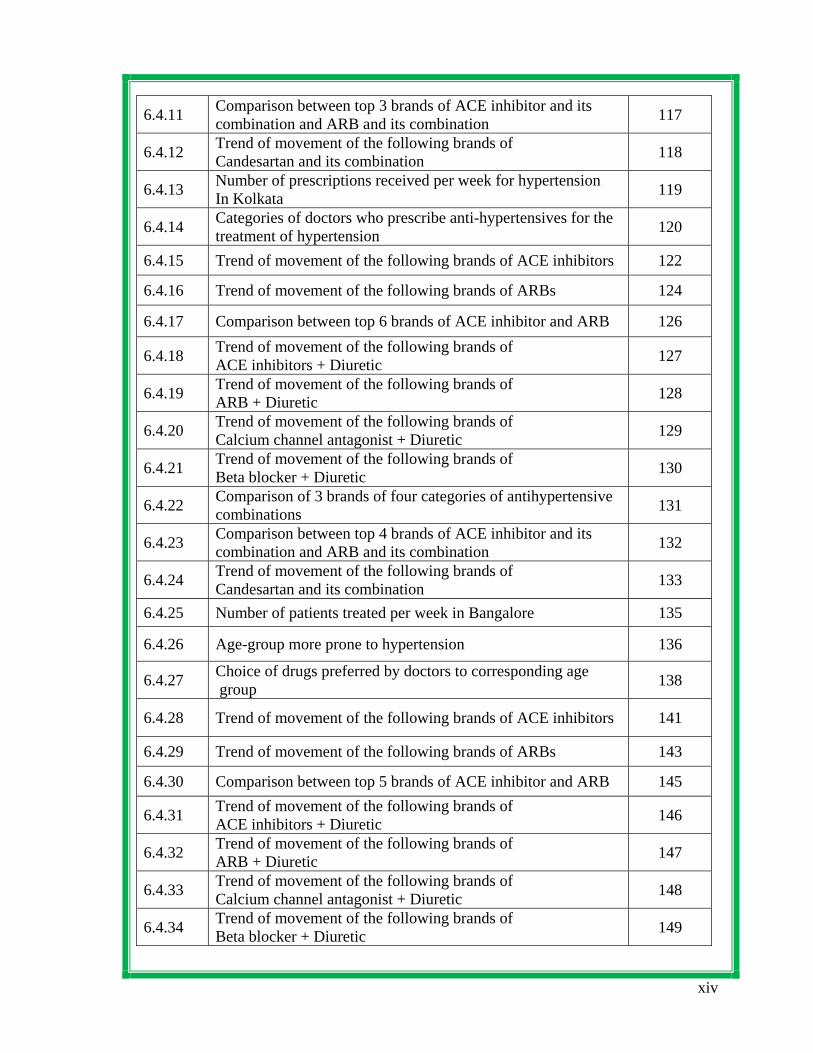
xiv
6.4.11 Comparison between top 3 brands of ACE inhibitor and its combination and ARB and its combination 117
6.4.12 Trend of movement of the following brands of Candesartan and its combination 118
6.4.13 Number of prescriptions received per week for hypertension In Kolkata 119
6.4.14 Categories of doctors who prescribe anti-hypertensives for the treatment of hypertension 120
6.4.15 Trend of movement of the following brands of ACE inhibitors 122
6.4.16 Trend of movement of the following brands of ARBs 124
6.4.17 Comparison between top 6 brands of ACE inhibitor and ARB 126
6.4.18 Trend of movement of the following brands of ACE inhibitors + Diuretic 127
6.4.19 Trend of movement of the following brands of ARB + Diuretic 128
6.4.20 Trend of movement of the following brands of Calcium channel antagonist + Diuretic 129
6.4.21 Trend of movement of the following brands of Beta blocker + Diuretic 130
6.4.22 Comparison of 3 brands of four categories of antihypertensive combinations 131
6.4.23 Comparison between top 4 brands of ACE inhibitor and its combination and ARB and its combination 132
6.4.24 Trend of movement of the following brands of Candesartan and its combination 133
6.4.25 Number of patients treated per week in Bangalore 135
6.4.26 Age-group more prone to hypertension 136
6.4.27 Choice of drugs preferred by doctors to corresponding age group 138
6.4.28 Trend of movement of the following brands of ACE inhibitors 141
6.4.29 Trend of movement of the following brands of ARBs 143
6.4.30 Comparison between top 5 brands of ACE inhibitor and ARB 145
6.4.31 Trend of movement of the following brands of ACE inhibitors + Diuretic 146
6.4.32 Trend of movement of the following brands of ARB + Diuretic 147
6.4.33 Trend of movement of the following brands of Calcium channel antagonist + Diuretic 148
6.4.34 Trend of movement of the following brands of Beta blocker + Diuretic 149

6.4.35
Comparison between top 3 brands of ACE inhibitors + Diuretic ARB + Diuretic, Calcium channel antagonist + Diuretic and Beta blocker + Diuretic
150
6.4.36 Awareness of the molecule Candesartan among different specialities of doctors 151
6.4.37 Awareness of the molecule Candesartan cilexetil among different specialities of doctors 152
6.4.38 Awareness of the molecule Candesartan cilexetil with hydrochlorothiazide among different specialities of doctors 153
6.4.39 Single factor the doctors expect to support the brand 154
6.4.40 Number of patients treated per week in Kolkata 156
6.4.41 Age-group more prone to hypertension 157
6.4.42 Choice of drugs preferred by doctors to corresponding age group 158
6.4.43 Trend of movement of the following brands of ACE inhibitors 161
6.4.44 Trend of movement of the following brands of ARBs 163
6.4.45 Comparison between top 6 brands of ACE inhibitor and ARB 165
6.4.46 Trend of movement of the following brands of ACE inhibitors + Diuretic 166
6.4.47 Trend of movement of the following brands of ARB + Diuretic 167
6.4.48 Trend of movement of the following brands of Calcium channel antagonist + Diuretic 168
6.4.49 Trend of movement of the following brands of Beta blocker + Diuretic 169
6.4.50 Comparison between top 3 brands of ACE inhibitors + Diuretic ARB + Diuretic, Calcium channel antagonist + Diuretic and Beta blocker + Diuretic
170
6.4.51 Awareness of the molecule Candesartan among different specialities of doctors 171
6.4.52 Awareness of the molecule Candesartan cilexetil among different specialities of doctors 172
6.4.53 Awareness of the molecule Candesartan cilexetil with hydrochlorothiazide among different specialities of doctors 173
6.4.54 Single factor the doctors expect to support the brand 174
6.7.1 Components of marketing activities 190
xv
Introduction
DEPARTMENT OF PHARMAEUTICAL MARKETING AND MANAGEMENT Page 1
1. Introduction
Emerging from a highly protected economy and an insulated business environment,
many companies in India have come a long way in their quest to become global
players. Indian companies have started to venture into the global business arena by
acquisition, joint venturing and direct investment. Although the opportunities for
companies to enter and compete in foreign market are significant, the risks can also
be high.(1)
Among these companies, pharmaceutical organizations in India are also
competing in the global market. There are several factors which are responsible for
drawing more and more companies into the international arena:
• The company discovers that some foreign markets present higher profit
opportunities than the domestic market.
• The company needs a large customer base to achieve economies of scale
• The company wants to reduce its dependence on any one market
• Global firms offering better products can attack the company’s domestic
market.
• The company might want to counterattack these competitors in their home
markets.(1)
Introduction
DEPARTMENT OF PHARMAEUTICAL MARKETING AND MANAG
The Chartered Institute of Marketing Defines marketing as the “Management
process responsible for identifying, anticipating and satisfying customer
requirements profitably”. Thus marketing involves: n
Focusing on the needs and wants of customers
Identifying the best method of satisfying those needs a
Orienting the company towards the process of providin
Meeting organizational objectives(2)
Achieving product success is difficult. Projects like these
development for a number of reasons. Sometimes available
meet desired performance specifications or a desired price p
firm’s strategy changes, rendering the product on longer inte
beats the firm to the market or sometimes the development te
marketing or management in commercializing the product.
either strategic or development process factors or some com
most important aspects to manage effectively in the process
stages and the proficiencies of both the technological and ma
within them.( 3)
The key difference between domestic marketing and marke
scale is the multi-dimensionality and complexity of the many
a company may operate in.(4)
Introductio
EMENT Page 2
nd wants
g that satisfaction
are abandoned during
technology is unable to
oint. At other times, a
resting, or a competitor
am is unable to interest
Product can fail due to
bination of two. So the
are the predevelopment
rketing-related activities
ting on an international
foreign country markets
Introduction
DEPARTMENT OF PHARMAEUTICAL MARKETING AND MANAGEMENT Page 3
Developing a new product and launching in the market is time and resource
consuming, as great care must be taken to ensure the best decisions are made before
the product reaches channel members and final consumers.
Therefore to launch a new product in the domestic and international market, some
important aspects such as analysis of targeted country, risks, cultural aspects,
competitors, company financial status should be extensively analyzed. The proposed
study involves the consideration of all the relevant aspects for the launch of a new
brand of a combination product that is Candesartan cilexetil with Hydrochlorothiazide
in domestic and international markets. It involves the development of tactics, plans
and strategies which helps to introduce the proposed new brand successfully.
Candesartan cilexetil with hydrochlorothiazide belonging to the therapeutic category
antihypertensives will be introduced in the market by formulating an effective launch
strategy.
• This project proposes to assist the company to develop a preliminary strategy
plan for introducing the new product into the market. The plan consists of
three part, such as
• The first part describes the target market’s size, structure and behavior; the
planned product positioning; and the sales, market share and profit goals
sought in the first few years
• The second part outlines the planned price, distribution strategy, and
marketing budget for the first year
Introduction
DEPARTMENT OF PHARMAEUTICAL MARKETING AND MANAGEMENT Page 4
The third part of the marketing-strategy plan describes the long-run sales and profit
goals and marketing mix strategy over time.(1)
When launching new products in today’s competitive market, it is critical to develop
innovative launch strategies that differentiate a company’s new brand and position it
for maximum growth. Without aggressive tactics, a company risks in missing a
window of opportunity for achieving optimal results from the launch. The
development, evaluation and implementation of launch strategies are essential for a
successful product launch.
Thereby a launch strategy for a product includes the development of strategy that
is externally oriented, proactive, timely, implementable and appropriate for a long
time horizon.(5)

Introduction
DEPARTMENT OF PHARMAEUTICAL MARKETING AND MANAGEMENT Page 5
Objectives
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 8
3. OBJECTIVES
The study covers the following objectives:
1. To study the epidemiology of hypertension
2. Study of the anti-hypertensive drugs market with special reference to
Candesartan cilexetil with Hydrochlorthiazide
3. To find out the prescription trends for the treatment of Hypertension.
4. Preparation of the launch strategy for a new brand of Candesartan cilexetil
with Hydrochlorthiazide
Need for study
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 5
2. NEED FOR STUDY
The global pharmaceutical market was valued at US$ 712 billion in 2007. Major
markets can be broadly classified into mature markets and emerging markets
depending upon the nature of the market growth. The market growth accelerates in the
seven pharma emerging markets are China, Brazil, Mexico, South Korea, India,
Turkey and Russia. In these markets there is significantly greater access to both
generic and innovative medicines as primary care improves and becomes available in
rural areas. Ongoing economic growth in the developing world will continue to shift
the focus from infectious diseases to cardiovascular, diabetes and other chronic
illnesses.
From the source of IMS health audit 2007 world wide, Angiotensin-II antagonists
ranked 8th, amounting to a global sales of US$ 19.4 billion with a growth of 13.6%
within the top leading therapeutic segments.
The angiotensin II receptor blocker candesartan cilexetil and the diuretic
hydrochlorothiazide (HCT) is a combination introduced by Astrazeneca. It is used to
treat high blood pressure (hypertension) when one medicine (monotherapy) is not
sufficiently effective. The combination of two medicines that have different ways of
working (modes of action) and leads to a greater lowering of blood pressure in more
people than with either medicine used alone. The following studies supports the
greater efficacy and cost effectiveness of the product:
The clinical studies carried out by the company proved that the drug reduces
blood pressure and proportion of patients with normalized BP was greater with
Candesartan-HCT 16/12.5 mg than with Losartan-HCT 50/12.5 mg.(6)
Need for study
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 6
Another study which was carried out to compare the antihypertensive effect
and tolerability of a once-daily combination of candesartan cilexetil, and the
diuretic hydrochlorothiazide (HCT), with a combination of lisinopril and HCT
in patients with primary hypertension. The results proved that the
combinations of candesartan cilexetil/HCT once daily, and lisinopril/HCT,
once daily, had similar antihypertensive efficacy in patients, but candesartan
cilexetil/HCT was significantly better tolerated than lisinopril/HCT.(7)
The use of candesartan cilexetil as part of antihypertensive therapy in elderly
patients with elevated blood pressure was deemed to be cost effective in a
Swedish analysis, primarily resulting from a reduced risk of nonfatal stroke.(8)
The antihypertensive efficacy and tolerability of combination therapy with
candesartan cilexetil, 16 mg plus hydrochlorothiazide (CC/HCT), 12.5 mg was
compared with that of amlodipine , in a multicentre, double-blind, randomised,
parallel-group study in patients with mild-to-moderate essential hypertension
inadequately controlled by monotherapy.. In conclusion, CC/HCTZ and
amlodipine were equally effective in reducing BP in hypertensive patients not
controlled by monotherapy, but CC/HCT was much better tolerated.(9)
From the above mentioned data it is quite clear that the molecule Candesartan
cilexetil with Hydrochlorthiazide is a potent drug having superiority over other drug
in the same and different categories of antihypertensives and also economical and
safe.
Now developing a competitively advantaged product requires: input from customers
on unmet needs, input from marketing as to what the competition is doing to address
Need for study
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 7
the need, input from manufacturing about what the firm can currently build to satisfy
the need, input from R&D about new ways of potentially addressing the need and
input from finance about costs. Which finally leads to successful new product
development fulfilling the requirements of profit, market share and customer
satisfaction.(4)
Candesartan cilexetil with hydrochlorothiazide belongs to the therapeutic category of
antihypertensives will be introduced in the market by formulating an effective launch
strategy in the domestic and Brazilian market.
The apparent reasons for selecting Brazilian and Indian market is due to their market
growth of 13.4% and 13% respectively which is higher in comparison to other major
pharmaceutical markets, such as North America, Europe and Japan according to IMS
health report. The driving force behind the growth is the rising consumption levels in
both the countries.
This project proposes to assist the company to develop a preliminary strategy plan for
introducing the new product into the market.
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 9
4. REVIEW OF LITERATURE
The Concept of Hypertension (10)
According to WHO, Hypertension is the state of body in which systolic BP is 150
mmHg or more & diastolic BP is 95 mmHg or more.
Hypertension can be classified either essential (primary) or secondary.
Secondary hypertension indicates that the high blood pressure is a result of (i.e.,
secondary to) another condition, such as kidney disease or tumors
(pheochromocytoma and paraganglioma). Persistent hypertension is one of the risk
factors for strokes, heart attacks, heart failure and arterial aneurysm, and is a leading
cause of chronic renal failure.
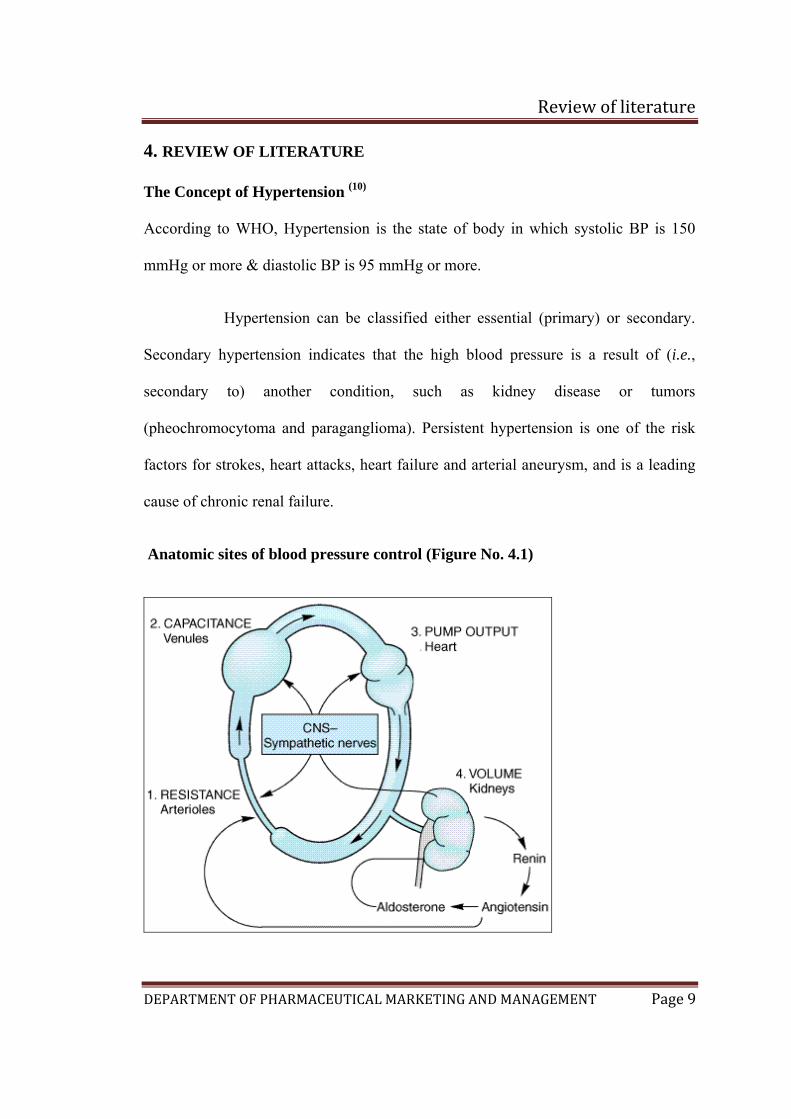
Anatomic sites of blood pressure control (Figure No. 4.1)
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 10
According to the hydraulic equation, arterial blood pressure (BP) is directly
proportionate to the product of the blood flow (cardiac output, CO) and the resistance
to passage of blood through precapillary arterioles (peripheral vascular resistance,
PVR): Physiologically, in both normal and hypertensive individuals, blood pressure is
maintained by moment-to-moment regulation of cardiac output and peripheral
vascular resistance, exerted at three anatomic sites (Figure 4.1): arterioles,
postcapillary venules (capacitance vessels), and heart. A fourth anatomic control site,
the kidney, contributes to maintenance of blood pressure by regulating the volume of
intravascular fluid. Baroreflexes, mediated by autonomic nerves, act in combination
with humoral mechanisms, including the renin-angiotensin-aldosterone system, to
coordinate function at these four control sites and to maintain normal blood pressure.
Finally, local release of hormones from vascular endothelium may also be involved in
the regulation of vascular resistance
Blood pressure in a hypertensive patient is controlled by the same mechanisms that
are operative in normotensive subjects. Regulation of blood pressure in hypertensive
patients differs from healthy patients in that the baroreceptors and the renal blood
volume-pressure control systems appear to be "set" at a higher level of blood
pressure. All antihypertensive drugs act by interfering with these normal mechanisms.
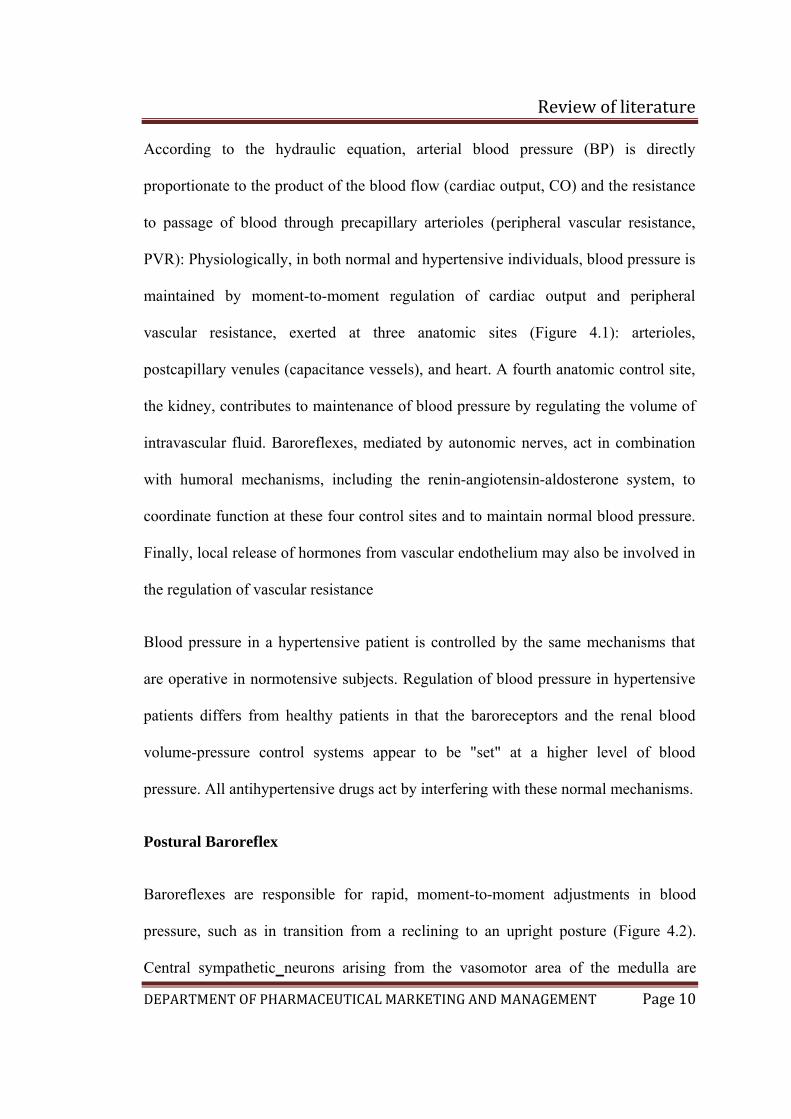
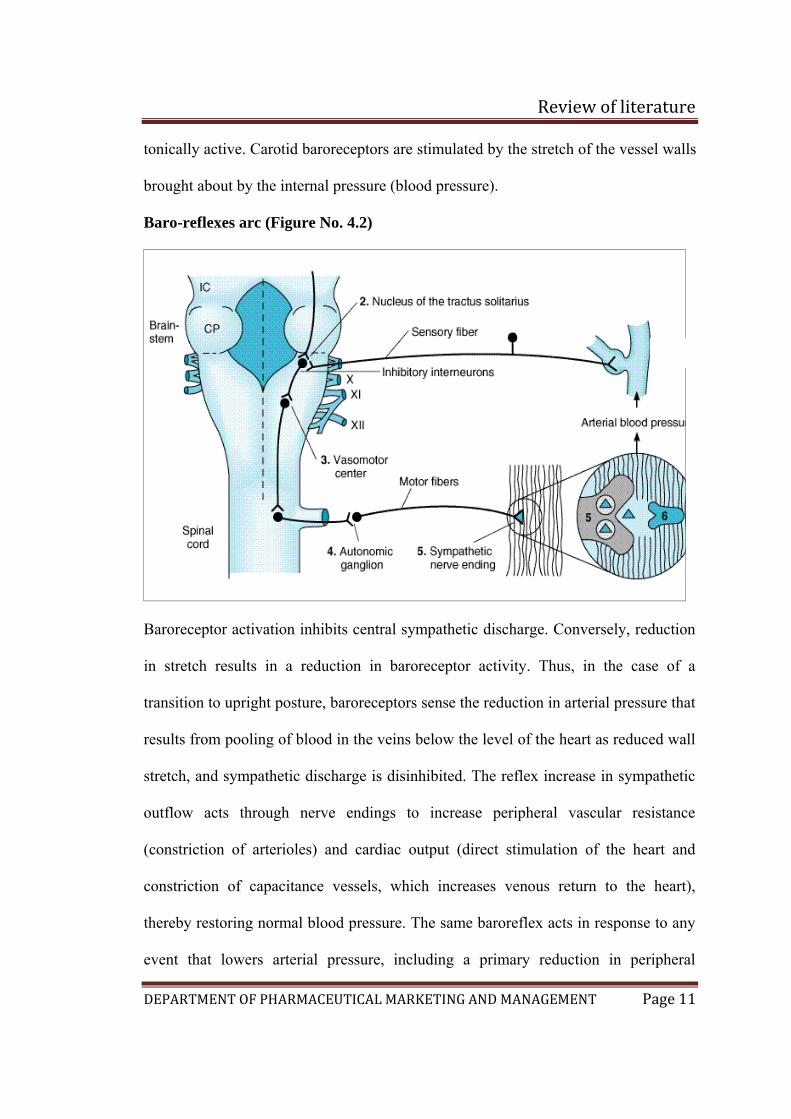
Postural Baroreflex
Baroreflexes are responsible for rapid, moment-to-moment adjustments in blood
pressure, such as in transition from a reclining to an upright posture (Figure 4.2).
Central sympathetic neurons arising from the vasomotor area of the medulla are
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 11
tonically active. Carotid baroreceptors are stimulated by the stretch of the vessel walls
brought about by the internal pressure (blood pressure).
Baro-reflexes arc (Figure No. 4.2)
Baroreceptor activation inhibits central sympathetic discharge. Conversely, reduction
in stretch results in a reduction in baroreceptor activity. Thus, in the case of a
transition to upright posture, baroreceptors sense the reduction in arterial pressure that
results from pooling of blood in the veins below the level of the heart as reduced wall
stretch, and sympathetic discharge is disinhibited. The reflex increase in sympathetic
outflow acts through nerve endings to increase peripheral vascular resistance
(constriction of arterioles) and cardiac output (direct stimulation of the heart and
constriction of capacitance vessels, which increases venous return to the heart),
thereby restoring normal blood pressure. The same baroreflex acts in response to any
event that lowers arterial pressure, including a primary reduction in peripheral
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 12
vascular resistance (eg, caused by a vasodilating agent) or a reduction in intravascular
volume (e.g, due to hemorrhage or to loss of salt and water via the kidney).
Renal Response to Decreased Blood Pressure
By controlling blood volume, the kidney is primarily responsible for long-term blood
pressure control. A reduction in renal perfusion pressure causes intrarenal
redistribution of blood flow and increased reabsorption of salt and water. In addition,
decreased pressure in renal arterioles as well as sympathetic neural activity (via -
adrenoceptors) stimulates production of renin, which increases production of
angiotensin II (see Figure 11–1). Angiotensin II causes (1) direct constriction of
resistance vessels and (2) stimulation of aldosterone synthesis in the adrenal cortex,
which increases renal sodium absorption and intravascular blood volume. Vasopressin
released from the posterior pituitary gland also plays a role in maintenance of blood
pressure through its ability to regulate water reabsorption by the kidney.
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 13
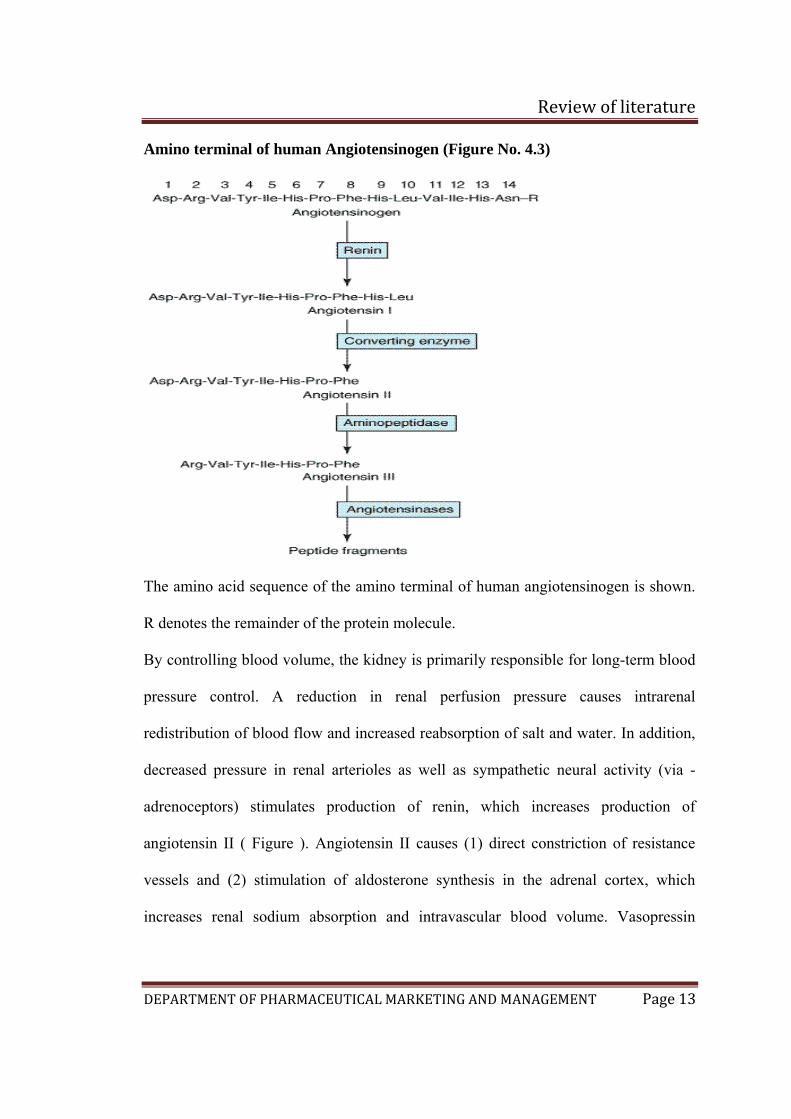
Amino terminal of human Angiotensinogen (Figure No. 4.3)
The amino acid sequence of the amino terminal of human angiotensinogen is shown.
R denotes the remainder of the protein molecule.
By controlling blood volume, the kidney is primarily responsible for long-term blood
pressure control. A reduction in renal perfusion pressure causes intrarenal
redistribution of blood flow and increased reabsorption of salt and water. In addition,
decreased pressure in renal arterioles as well as sympathetic neural activity (via -
adrenoceptors) stimulates production of renin, which increases production of
angiotensin II ( Figure ). Angiotensin II causes (1) direct constriction of resistance
vessels and (2) stimulation of aldosterone synthesis in the adrenal cortex, which
increases renal sodium absorption and intravascular blood volume. Vasopressin
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 14
released from the posterior pituitary gland also plays a role in maintenance of blood
pressure through its ability to regulate water reabsorption by the kidney
Angiotensin
Angiotensin II inhibits renin secretion. The inhibition, which results from a direct
action of the peptide on the juxtaglomerular cells, forms the basis of a short-loop
negative feedback mechanism controlling renin secretion. Interruption of this
feedback with inhibitors of the renin-angiotensin system (see below) results in
stimulation of renin secretion.
Pharmacologic Alteration of Renin Release
The release of renin is altered by a wide variety of pharmacologic agents. Renin
release is stimulated by vasodilators (hydralazine, minoxidil, nitroprusside), β-
adrenoceptor agonists (isoproterenol), -adrenoceptor antagonists, phosphodiesterase
inhibitors (theophylline, milrinone,rolipram), and most diuretics and anesthetics. This
stimulation can be accounted for by the control mechanisms just described. Drugs that
inhibit renin release are discussed below in the section on inhibition of the renin-
angiotensin system.
Angiotensinogen
Angiotensinogen is the circulating protein substrate from which renin cleaves
angiotensin I. It is synthesized in the liver. Human angiotensinogen is a glycoprotein
with a molecular weight of approximately 57,000. The 14 amino acids at the amino
terminal of the molecule are shown in (Figure 4.3). In humans, the concentration of
angiotensinogen in the circulation is less than the Km of the renin-angiotensinogen
reaction and is therefore an important determinant of the rate of formation of
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 15
angiotensin. The production of angiotensinogen is increased by corticosteroids,
estrogens, thyroid hormones, and angiotensin II. It is also elevated during pregnancy
and in women taking estrogen-containing oral contraceptives. The increased plasma
angiotensinogen concentration is thought to contribute to the hypertension that may
occur in these situations. There is also evidence for a genetic linkage between the
angiotensinogen gene and essential hypertension..
Angiotensin I
Although angiotensin I contains the peptide sequences necessary for all of the actions
of the reninangiotensin system, it has little or no biologic activity. Instead, it must be
converted to angiotensin II by converting enzyme. Angiotensin I may also be acted on
by plasma or tissue aminopeptidases to form [des-Asp1]angiotensin I; this in turn is
converted to [des-Asp1]angiotensin II (commonly known as angiotensin III) by
converting enzyme.
Converting Enzyme (Peptidyl Dipeptidase , Kininase II)
Converting enzyme is a dipeptidyl carboxypeptidase that catalyzes the cleavage of
dipeptides from the carboxyl terminal of certain peptides. Its most important
substrates are angiotensin I, which it converts to angiotensin II, and bradykinin, which
it inactivates. It also cleaves enkephalins and substance P, but the physiologic
significance of these effects has not been established. The action of converting
enzyme is prevented by a penultimate prolyl residue, and angiotensin II is therefore
not hydrolyzed by converting enzyme. Converting enzyme is distributed widely in the
body. In most tissues, converting enzyme is located on the luminal surface of vascular
endothelial cells and is thus in close contact with the circulation.
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 16
Angiotensinase
Angiotensin II, which has a plasma half-life of 15–60 seconds, is removed rapidly
from the
circulation by a variety of peptidases collectively referred to as angiotensinase. It is
metabolized during passage through most vascular beds (a notable exception being
the lung). Most metabolites
of angiotensin II are biologically inactive, but the initial product of aminopeptidase
action—[des- Asp1]angiotensin II—retains considerable biologic activity.
Actions of Angiotensin II
Angiotensin II exerts important actions at several sites in the body, including vascular
smoothmuscle, adrenal cortex, kidney, and brain. Through these actions, the renin-
angiotensin system plays a key role in the regulation of fluid and electrolyte balance
and arterial blood pressure. Excessive activity of the renin-angiotensin system can
result in hypertension and disorders of fluid and electrolyte homeostasis.
Blood Pressure
Angiotensin II is a very potent pressor agent—on a molar basis, approximately 40
times more potent than norepinephrine. The pressor response to intravenous
angiotensin II is rapid in onset (10– 15 seconds) and sustained during long-term
infusions of the peptide. A large component of the pressor response to intravenous
angiotensin II is due to direct contraction
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 17
of vascular—especially arteriolar—smooth muscle. In addition, however, angiotensin
II can also increase blood pressure through actions on the brain and autonomic
nervous system. The pressor response to angiotensin is usually accompanied by little
or no reflex bradycardia because the peptide acts on the brain to reset the baroreceptor
reflex control of heart rate to a higher pressure. Angiotensin II also interacts with the
autonomic nervous system. It stimulates autonomic ganglia, increases the release of
epinephrine and norepinephrine from the adrenal medulla, and—what is most
important—facilitates sympathetic transmission by an action at adrenergic nerve
terminals. The latter effect involves both increased release and reduced reuptake of
norepinephrine. Angiotensin II also has a less important direct positive inotropic
action on the heart.
Adrenal Cortex
Angiotensin II acts directly on the zona glomerulosa of the adrenal cortex to stimulate
aldosterone biosynthesis. At higher concentrations, angiotensin II also stimulates
glucocorticoid biosynthesis.
Kidney
Angiotensin II acts on the kidney to cause renal vasoconstriction, increase proximal
tubular sodium reabsorption, and inhibit the secretion of renin.
Central Nervous System
In addition to its central effects on blood pressure, angiotensin II acts on the central
nervous system to stimulate drinking (dipsogenic effect) and increase the secretion of
vasopressin and adrenocorticotropic hormone (ACTH). The physiologic significance

Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 18
of the effects of angiotensin II on drinking and pituitary hormone secretion is not
known
Primary hypertension(11)
The cause of essential hypertension is unknown but a number of factors are related to
its development. These are as under:
Genetic factors: The evidences in support are the familial aggregation,
occurrence of hypertension in twins, epidemiologic data, experimental animal
studies and identification of hypertension susceptibility gene (angiotensinogen
gene)
Racial and environmental factors: A number of environmental factor have
been implicated in the development of hypertension including salt intake,
obesity, skilled occupation, higher living standards and patients in high stress.
Risk factors modifying the course of essential hypertension : These are, age,
sex, atherosclerosis and others (smoking, excess alcohol intake, diabetes
mellitus etc).
The pathogenetic mechanism in essential hypertension is explained by many
theories…..
1. High plasma level of catecholamines
2. Increase in blood volume
3. Increased cardiac output
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 19
4. Low renin essential hypertension due to altered responsiveness to renin release
5. High renin essential hypertension due to decresed adrenal responsiveness to
angiotensin ll
Secondary hypertension(11)
Renal hypertension: Hypertension produced by renal diseases is called renal
hypertension, which can again be subdivided into 2 groups:
a) Renal vascular hypertension
b) Renal parenchymal hypertension can be due to activation of renin-
angiotensin system, sodium and water retension, or release of
vasodepressor materials
Endocrine hypertension: A number of hormonal secretions may produce
secondary hypertension. These are due to diseased condition in adrenal gland,
parathyroid gland and oral contraceptives
Coarctation of aorta can cause hypertension
Neurogenic: psychogenic, polyneuritis, increased intracranial pressure etc are
uncommon causes of secondary hypertension
Another way of classifying hypertension is as follows….
Normal – (Systolic 90-120, diastolic 60-80)
Pre-hypertension – (Systolic 120-139, diastolic 80-99)
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 20
Hypertension Mild, Stage 1 - (Systolic 140-159 or diastolic 90-99)
Hypertension Moderate, Stage 2 - (Systolic 160 - 179 diastolic 100 – 109)
Hypertension Severe, Stage 3 - (Systolic 180 - 209 or diastolic 110 – 119)
Hypertension Very Severe, Stage 4 - (Systolic > or = 210 or diastolic > or =
120)
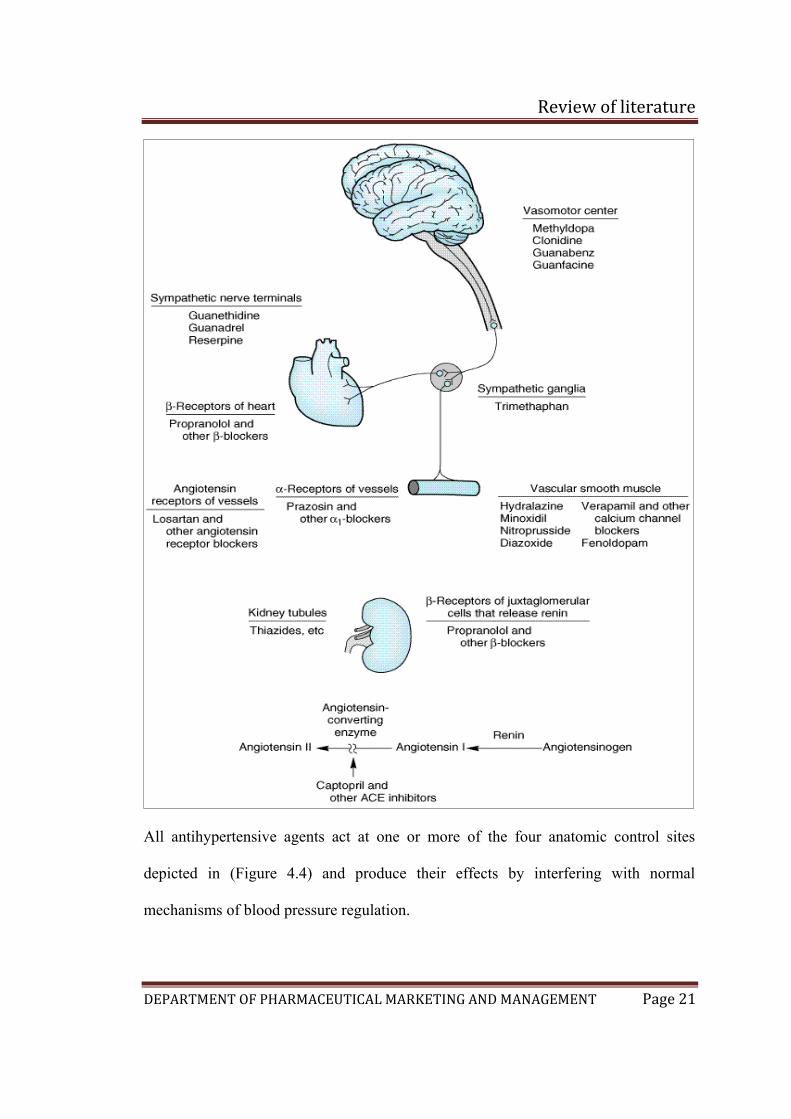
Management Of Hypertension (10) (Figure No. 4.4)
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 21
All antihypertensive agents act at one or more of the four anatomic control sites
depicted in (Figure 4.4) and produce their effects by interfering with normal
mechanisms of blood pressure regulation.
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 22
A useful classification of these agents categorizes them according to the principal
regulatory site or mechanism on which they act (Figure4.4). Because of their common
mechanisms of action, drugs within each category tend to produce a similar spectrum
of toxicities. The categories include the following:
(1) Diuretics, which lower blood pressure by depleting the body of sodium and
reducing blood volume and perhaps by other mechanisms.
(2) Sympathoplegic agents, which lower blood pressure by reducing peripheral
vascular
resistance, inhibiting cardiac function, and increasing venous pooling in capacitance
vessels.
(The latter two effects reduce cardiac output.) These agents are further subdivided
according to their putative sites of action in the sympathetic reflex arc.
(3) Direct vasodilators, which reduce pressure by relaxing vascular smooth muscle,
thus
dilating resistance vessels and—to varying degrees—increasing capacitance as well.
(4) Agents that block production or action of angiotensin and thereby reduce
peripheral
vascular resistance and (potentially) blood volume.
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 23
CANDESARTAN CILEXETIL/ HYDROCHLOROTHIAZIDE (12)
Candesartan cilexetil:
Candesartan is a nonpeptide angiotensin II blocker used as an antihypertensive.
Commercially cilexetil (cyclohexyl 1-hydroxyethyl carbonate) ester form is available.
Candesartan cilexetil is the prodrug which is separated into the active candesartan and
ester by reacting with a molecule of water.
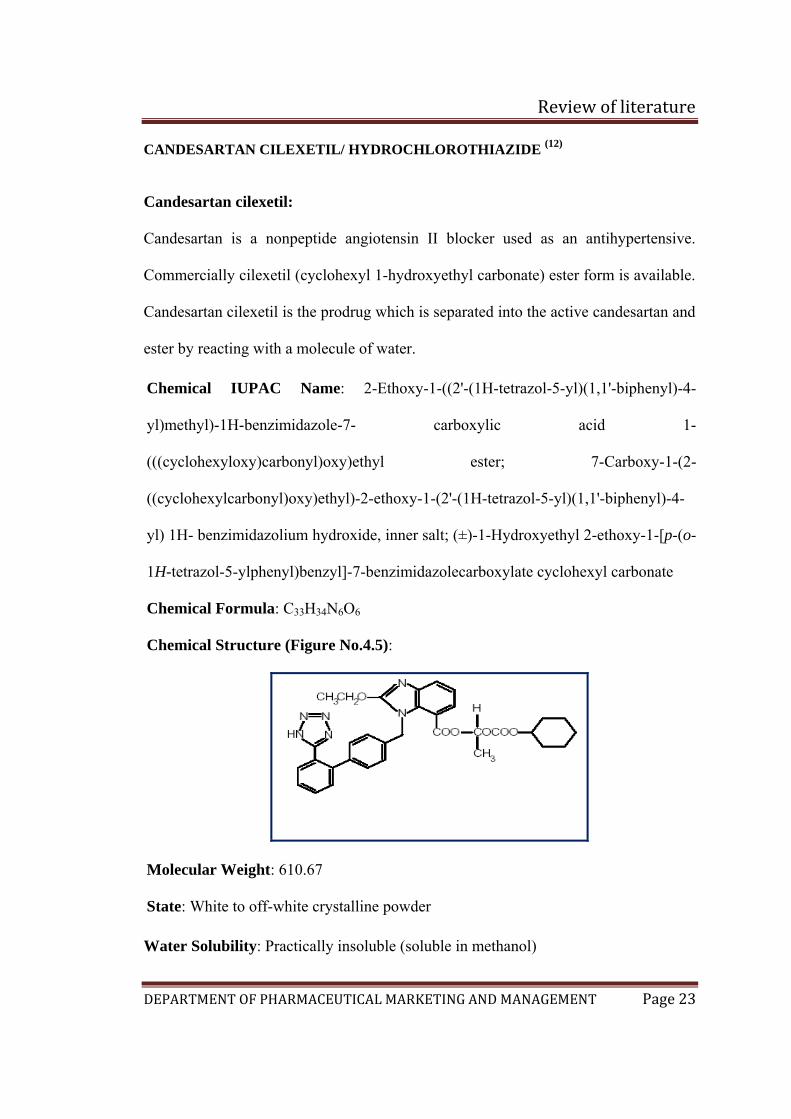
Chemical IUPAC Name: 2-Ethoxy-1-((2'-(1H-tetrazol-5-yl)(1,1'-biphenyl)-4-
yl)methyl)-1H-benzimidazole-7- carboxylic acid 1-
(((cyclohexyloxy)carbonyl)oxy)ethyl ester; 7-Carboxy-1-(2-
((cyclohexylcarbonyl)oxy)ethyl)-2-ethoxy-1-(2'-(1H-tetrazol-5-yl)(1,1'-biphenyl)-4-
yl) 1H- benzimidazolium hydroxide, inner salt; (±)-1-Hydroxyethyl 2-ethoxy-1-[p-(o-
1H-tetrazol-5-ylphenyl)benzyl]-7-benzimidazolecarboxylate cyclohexyl carbonate
Chemical Formula: C33H34N6O6
Chemical Structure (Figure No.4.5):
Molecular Weight: 610.67
State: White to off-white crystalline powder
Water Solubility: Practically insoluble (soluble in methanol)
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 24
Half Life: Approximately 9 hours.
Melting point: 157 - 160 C
• Candesartan works by blocking the action of a hormone (a natural chemical
carried in the blood) called angiotensin II:
• It stops angiotensin II attaching itself (binding) to sites (called receptors)
found on cells in the body.
• In the body Angiotensin II causes blood vessels to become narrowed
(constricted) and in the kidney, it causes less urine to be produced so salt and
water are retained in the body. These actions may be part of the cause of high
blood pressure.
• If angiotensin II can’t bind to the receptors because of the action of
candesartan, the blood vessels relax and widen and blood pressure decreases.
Dose: The usual recommended starting dose of candesartan 16 mg once daily when it
is used as monotherapy in patients who are not volume depleted. Patients requiring
further reduction in blood pressure should be titrated to candesartan 32 mg. ( )
Pharmacokinetics: General
Candesartan cilexetil is rapidly and completely bioactivated by ester hydrolysis
during absorption from the gastrointestinal tract to candesartan, a selective AT1
subtype angiotensin II receptor antagonist. Candesartan is mainly excreted unchanged
in urine and feces (via bile). It undergoes minor hepatic metabolism by O-
demethylation to an inactive metabolite. The elimation half-life of candesartan is
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 25
approximately 9hours. After single and repeated administration, the pharmacokinetics
of candesartan are linier for oral doses upto 32 mg of candesartan cilexetil.
Candesartan and its inactive metabolite do not accumulate in serum upon repeated
once-daily dosing. Following administration of candesartan cilexetil, the absolute
bioavailability of candesartan was estimated to be 15%. After tablet ingestion, the
peak serum concentration (Cmax) is reached after 3 to 4 hours. Food with a high fat
content does not affect the bioavailability of candesartan after candesartan cilexetil
administration.
Metabolism and excretion:
Total plasma clearance of candesartan is 0.37 ml/min/kg, with a renal clearance of
0.19 ml/min/kg. when candesartan is administered orally, about 26% of the dose is
excreted unchanged in urine.
Distribution:
The volume of distribution of candesartan is 0.13L/kg. candesartan is highly bound to
plasma proteins (>99%) and does not penetrate red blood cells. The protein binding is
constant at candesartan plasma concentrations well above the range achieved with
recommended doses.
Special populations:
The pharmacokinetics of Candesartan have been studied in the elderly (≥65years).
The plasma concentration of Candesartan was higher in the elderly (Cmax was
approximately 50% higher, and AUC was approximately 80% higher) compared to
younger subjects administered the same dose. The pharmacokinetics of Candesartan
were linear in the elderly, and Candesartan and its inactive metabolite did not
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 26
accumulate in the serum of these subjects upon repeated, once-daily administration.
No initial dosage adjustment is necessary.
Gender:
There is no difference in the pharmacokinetics of Candesartan between male and
female subjects.
Pharmacodynamics:
Candesartan Cilexetil inhibits the pressor effects of angiotensin II infusion in a dose-
dependent manner. After 1 week of once-daily dosing with 8mg Candesartan cilexetil,
the pressor effect was inhibited by approximately 90% at peak with approximately
50% inhibition persisting for 24 hours.
Warnings:
Drug that act directly on the rennin-angiotensin system can cause fetal and neonatal
morbidity and death when administered to pregnant women. Post-marketing
experience has identified reports of fetal and neonatal toxicity in babies born to
women treated with Candesartan cilexetil during pregnancy. The use of drugs that act
directly on the rennin-angiotensisn system during the second and third trimesters of
pregnancy has been associated with fetal and neonatal injury, including hypotension,
neonatal skull hypoplasia, anuria, reversible or irreversible renal failure and death.
Oligohydramnios has been reported, presumably resulting from decreased fetal renal
functions.
Hypotension in volume and salt depleted patients:
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 27
Based on adverse events reported from all clinical trials, excessive reduction of blood
pressure was rarely seen in patients with uncomplicated hypertension treated with
candesartan cilexetil and hydrochlorothiazide. Initiation of antihypertensive therapy
amy cause symptomatic hypotension in patients with intravascular volume or sodium
depletion. These conditions should be corrected prior to administration of the drug.
Adverse reactions:
These include hypotension, hyperkalemia, and reduced renal function, including that
associated with bilateral renal artery stenosis and stenosis in the artery of a solitary
kidney. Hypotension is most likely to occur in patients in whom the blood pressure is
highly dependent on angiotensin II, including those with volume depletion (e.g., with
diuretics), renovascular hypertension, cardiac failure, and cirrhosis; in such patients
initiation of treatment with low doses and attention to blood volume is essential.
Hyperkalemia may occur in conjunction with other factors that alter K+ homeostasis,
such as renal insufficiency, ingestion of excess K+, and the use of drugs that promote
K+ retention.
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 28
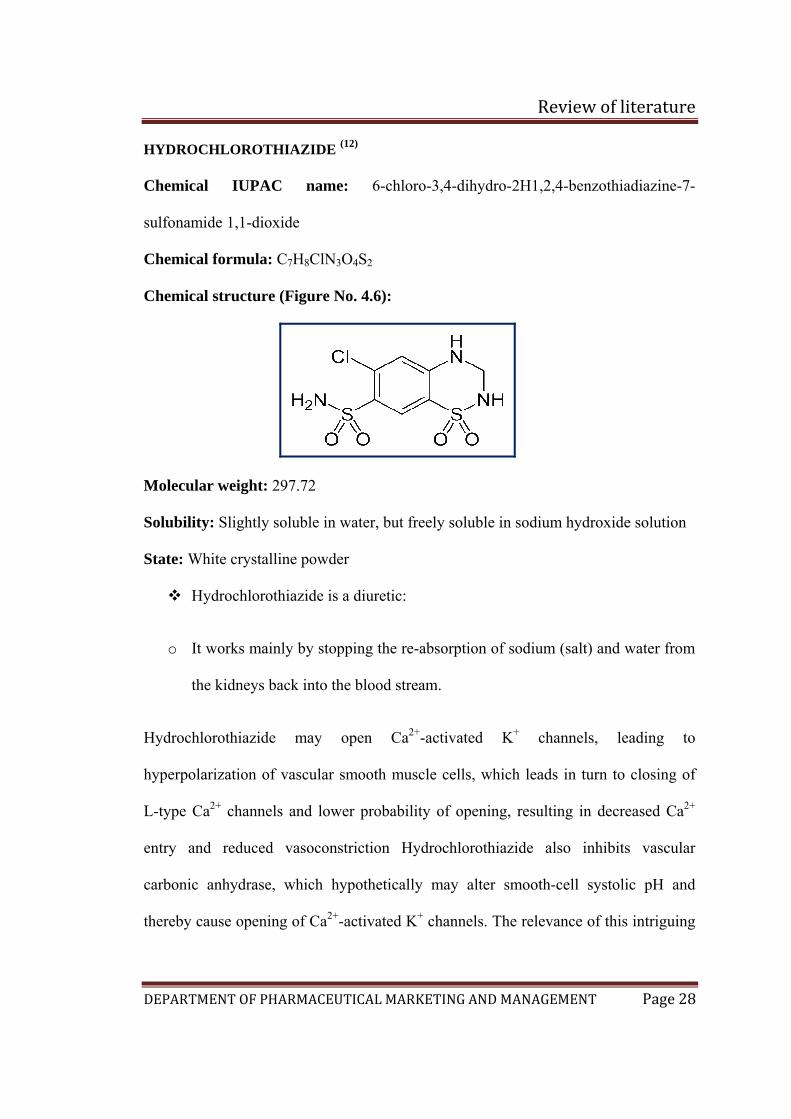
HYDROCHLOROTHIAZIDE (12)
Chemical IUPAC name: 6-chloro-3,4-dihydro-2H1,2,4-benzothiadiazine-7-
sulfonamide 1,1-dioxide
Chemical formula: C7H8ClN3O4S2
Chemical structure (Figure No. 4.6):
Molecular weight: 297.72
Solubility: Slightly soluble in water, but freely soluble in sodium hydroxide solution
State: White crystalline powder
Hydrochlorothiazide is a diuretic:
o It works mainly by stopping the re-absorption of sodium (salt) and water from
the kidneys back into the blood stream.
Hydrochlorothiazide may open Ca2+-activated K+ channels, leading to
hyperpolarization of vascular smooth muscle cells, which leads in turn to closing of
L-type Ca2+ channels and lower probability of opening, resulting in decreased Ca2+
entry and reduced vasoconstriction Hydrochlorothiazide also inhibits vascular
carbonic anhydrase, which hypothetically may alter smooth-cell systolic pH and
thereby cause opening of Ca2+-activated K+ channels. The relevance of this intriguing
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 29
finding to the observed antihypertensive effects of thiazides is speculative. These
effects lower the blood pressure
Dose: It is effective in doses of 12.5 to 50 mg once daily.
Pharmacokinetics: General
When plasma levels have been followed for at least 24 hours, the plasma half-life has
been observed to vary between 5.6 and 14.8 hours
Metabolism and Excretion:
Hydrochlorothiazide is not metabolized but is eliminated rapidly by kidney. At least
61% of the oral dose is eliminated within 24 hours.
Distribution:
It crosses the placental barrier but not the blood brain barrier and is excreted in breast
milk.
Pharmacodynamics:
After oral administration of hydrochlorothiazide, dieresis begins within 2 hours, peak
in about 4 hours and last about 6 to 12 hours.
Warnings:
Thiazide diuretics should be used with caution in patients with impaired hepatic
function or progressive liver disease, since minor alterations of fluid and electrolyte
balance may precipitate hepatic coma. Hypersensitivity reactions to
hydrochlorthiazide may occur in patients with or without a history of allergy or
bronchial asthma, but are more likely in patients with such a history. Thiazide
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 30
diuretics have been reported to cause exacerbation or activation of systemic lupus
erythematous.
Adverse reactions:
Erectile dysfunction is a troublesome adverse effect of the thiazide-class diuretics,
and physicians should inquire specifically regarding its occurrence in conjunction
with treatment with these drugs. Gout may be a consequence of the hyperuricemia
induced by these diuretics. The occurrence of either of these adverse effects is a
reason for considering alternative approaches to therapy. However, precipitation of
acute gout is relatively uncommon with low doses of diuretics. Hydrochlorothiazide
may cause rapidly developing, severe hyponatremia in some patients. Thiazides
inhibit renal Ca2+ excretion, occasionally leading to hypercalcemia; although
generally mild, this can be more severe in patients subject to hypercalcemia, such as
those with primary hyperparathyroidism. The thiazide-induced decreased Ca2+
excretion may be used therapeutically in patients with osteoporosis or hypercalciuria.
Clinical trials (12)
Of 12 controlled clinical trials involving 4588 patients, 5 were double-blinded,
placebo controlled and evaluated the hypertensive effects of single entities vs the
combination. these 5 trials, of 8 to 12 weeks duration, randomized 3037 hypertensive
patients. does ranged from 2 to 32 mg Candesartan cilexetil and from 6.25 to 25 mg
Hydrochlorthiazide administered once daily in various combinations. the combination
of Candesartan cilexetil with Hydrochlorthiazide resulted in placebo-adjusted
decreases in sitting systolic and diastolic blood pressure of 14 – 18/8 – 11 mm Hg at
doses of 16 – 12.5 mg and 32 – 12.5 mg. The combination of Candesartan cilextil and
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 31
Hydrochlorthiazide 32 – 25 mg resulted in placebo adjusted decreases in sitting
systolic and diastolic blood pressure of 16- 19 /9 – 11 mm Hg. The placebo corrected
trough to peak ratio was evaluated in a study of Candesartan cilexetil
Hydrochlorthiazide 32 - 12.5 mg and was 88%.
Most of the antihypertensive effect of the combination was seen in 1 to 2 weeks with
the full effect observed within 4 weeks.in long term studies of upto 1 year, the blood
pressure lowering effect of the combination was maintained. the antihypertensive
effect was similar regardless of age or gender, and overall response to the
combination was similar in black and non-black patients.
Men and women, aged 20–80 years, during treatment with any kind of
antihypertensive monotherapy for at least 4 weeks were randomised to treatment with
Candesartan cilexetil (Candes)-Hydrochlorthiazide (HCT) or Los-HCT once daily for
12 weeks. Efficacy analysis was performed according to intention to treat. The
reduction in BP was independent of previous antihypertensive agent, gender and age
of the patient. It was concluded conclude that the combination Candes-HCT reduced
blood pressure effectively and was well tolerated. BP was normalised in 61% of these
patients who had insufficient response to previous monotherapy. The reduction in
blood pressure and proportion of patients with normalized BP was greater with
Candes-HCT 16/12.5 mg than with Los-HCT 50/12.5 mg.(13)
Monotherapy with an antihypertensive agent is likely to achieve a desirable lowering
of blood pressure in about 50% of patients. The aim of this study was to compare the
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 32
antihypertensive effect and tolerability of a once-daily combination of the angiotensin
II type 1 (AT1) receptor blocker candesartan cilexetil, and the diuretic
hydrochlorothiazide (HCT), with a combination of the angiotensin-converting
enzyme inhibitor, lisinopril and HCT in patients with primary hypertension. The
study included men and women, 20-80 years of age, with sitting diastolic blood
pressure of 95-114 mm Hg. After a run-in period of 2 weeks on any antihypertensive
monotherapy, 355 patients were randomized to double-blind treatment with either a
combination of candesartan cilexetil/HCT or a combination of lisinopril/HCT The
combinations of candesartan cilexetil/HCT once daily, and lisinopril/HCT, once daily,
had similar antihypertensive efficacy in patients with mild to moderate hypertension
during the 26-week treatment period, candesartan cilexetil/HCT was significantly
better tolerated than lisinopril/HCT.(6)
The primary objective of the study was to assess the bioequivalence of one
candesartan cilexetil/hydrochlorothiazide (HCT) 32/25 mg tablet and two candesartan
cilexetil/HCT 16/12.5 mg tablets after single dose administration. The secondary
objective of the study was to assess the pharmacokinetics of candesartan cilexetil 32
mg and HCT 25 mg after single dose administration of the fixed combination tablet
and after each monocomponent (ie one candesartan cilexetil tablet 32 mg tablet and
two HCT 12.5 mg tablets). According to the group-sequential design, 53 healthy male
and female subjects, aged between18 and 59 years, with female subjects comprising
at least 20% per treatment group, were enrolled in the first step, to ensure completion
by at least 48 subjects. A total of 48 subjects completed the study. Single dose
administration of candesartan cilexetil and hydrochlorothiazide was well tolerated,
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 33
and no new safety issues were identified during the study regardless of the
administration schedule. Headache and dizziness were the most frequently observed
adverse events (AE). No deaths, serious adverse events, or adverse events classified
as "other significant AEs" occurred during the study. No subject discontinued study
treatments due to an AE. There were no clinically relevant changes in laboratory
safety variables or physical examinations. An expected blood pressure lowering effect
was observed reaching mean minimum SBP and DBP values at around 8 hours after
dosing of 32 mg candesartan cilexetil, ie, after one candesartan cilexetil/HCT 32/25
mg tablet, after two candesartan cilexetil/HCT16/12.5 mg tablets or after one
candesartan cilexetil 32mg tablet. This blood pressure lowering effect was less
evident after treatment with two HCT 12.5 mg tablets.(10)
The angiotensin II receptor blocker candesartan cilexetil and the diuretic
hydrochlorothiazide is a combination introduced by Astrazeneca. It is used to treat
high blood pressure (hypertension) when one medicine (monotherapy) is not
sufficiently effective. The combination of two medicines that have different ways of
working (modes of action) and leads to a greater lowering of blood pressure in more
people than with either medicine used alone.(7)
Hypertension treatment and control is largely unsatisfactory when guideline-defined
blood pressure goal achievement and maintenance are considered. Patient- and
physician-related factors leading to non-adherence interfere in this respect with the
efficacy, tolerability, and convenient use of pharmacological treatment options.
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 34
Blockers of the renin–angiotensin system (RAS) are an important component of
antihypertensive combination therapy. Thiazide-type diuretics are usually added to
increase the blood pressure lowering efficacy. Fixed drug–drug combinations of both
principles like candesartan/hydrochlorothiazide (HCT) are highly effective in
lowering blood pressure while providing improved compliance, a good tolerability,
and largely neutral metabolic profile. Comparative studies with losartan/HCT have
consistently shown a higher clinical efficacy with the candesartan/HCT combination.
Data on the reduction of cardiovascular endpoints with fixed dose combinations of
antihypertensive drugs are however scarce, as are the data for candesartan/HCT. But
many trials have tested candesartan versus a non-RAS blocking comparator based on
a standard therapy including thiazide diuretics. The indications tested were heart
failure and stroke and particular emphasis was put on elderly patients or those with
diabetes. In patients with heart failure, for example, the fixed dose combination might
be applied in patients in whom individual titration resulted in a dose of 32 mg
candesartan and 25 mg HCT which can then be combined into one tablet to increase
compliance with treatment. Also in patients with stroke the fixed dose combination
might be used in patients in whom maintenance therapy with both components is
considered. Taken together candesartan/HCT assist both physicians and patients in
achieving long-term blood pressure goal achievement and maintenance. (13)
Therapeutic interventions that block the renin–angiotensin–aldosterone system
(RAAS) have an important role in slowing the progression of cardiovascular risk
factors to established cardiovascular diseases. In recent years, angiotensin receptor
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 35
blockers (ARBs) have emerged as effective and well-tolerated alternatives to an
angiotensin-converting enzyme inhibitor (ACEi) for RAAS blockade. The ARB
candesartan was initially established as an effective once-daily antihypertensive
treatment, providing 24 h blood pressure (BP) control with a trough:peak ratio close
to 100%.
Compared with other ARBs, candesartan demonstrates the strongest binding affinity
to the angiotensin II type 1 receptor. Clinical trials have demonstrated that
candesartan is well tolerated in combination with diuretics or calcium channel
blockers (CCBs), making it a suitable treatment option for patients whose
hypertension is not adequately controlled by monotherapy. Subsequently, candesartan
became the only ARB licensed in the UK to treat patients with CHF and left
ventricular ejection fraction ≤ 40% as add-on therapy to an ACEi or when an ACEi is
not tolerated. Studies in patients with symptomatic HF have indicated that candesartan
treatment was associated with significant relative risk reductions in cardiovascular
mortality and hospitalisation due to CHF. (14 )
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 36
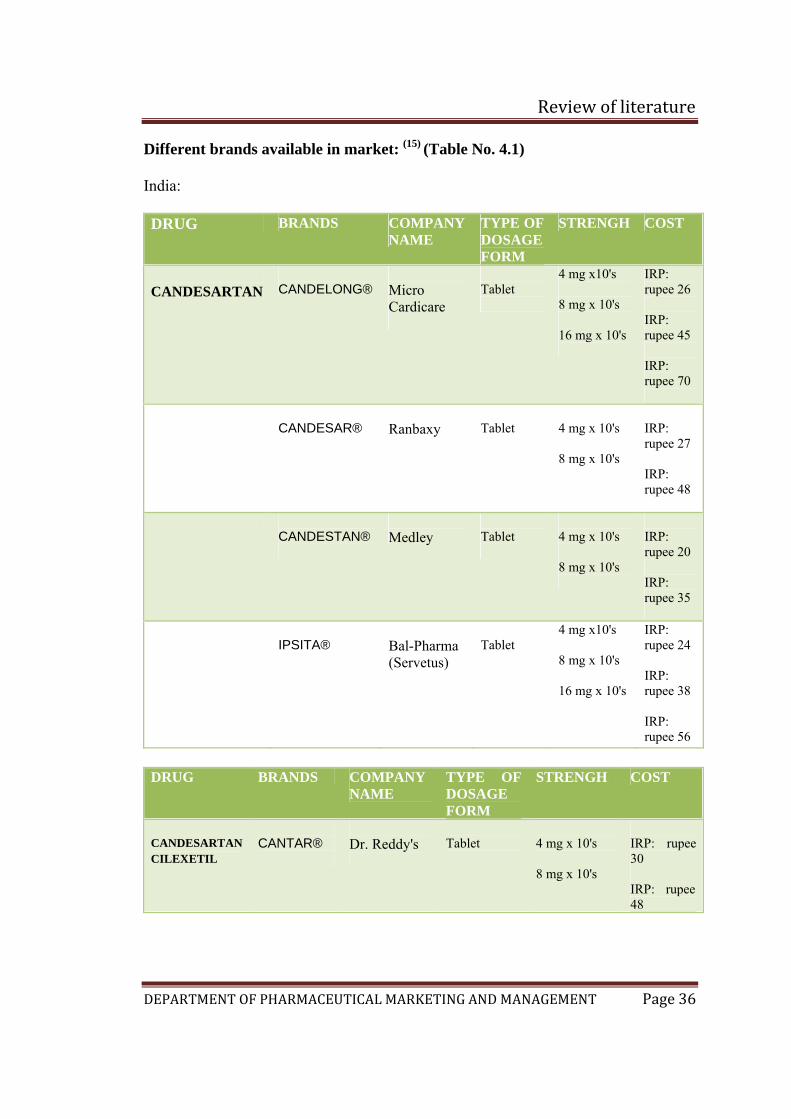
Different brands available in market: (15) (Table No. 4.1)
India:
DRUG BRANDS COMPANY NAME
TYPE OF DOSAGE FORM
STRENGH COST
CANDESARTAN
CANDELONG®
Micro Cardicare
Tablet
4 mg x10's 8 mg x 10's 16 mg x 10's
IRP: rupee 26 IRP: rupee 45 IRP: rupee 70
CANDESAR®
Ranbaxy
Tablet
4 mg x 10's 8 mg x 10's
IRP: rupee 27 IRP: rupee 48
CANDESTAN®
Medley
Tablet
4 mg x 10's 8 mg x 10's
IRP: rupee 20 IRP: rupee 35
IPSITA®
Bal-Pharma (Servetus)
Tablet
4 mg x10's 8 mg x 10's 16 mg x 10's
IRP: rupee 24 IRP: rupee 38 IRP: rupee 56
DRUG BRANDS COMPANY
NAME TYPE OF DOSAGE FORM
STRENGH COST
CANDESARTAN CILEXETIL
CANTAR®
Dr. Reddy's
Tablet
4 mg x 10's 8 mg x 10's
IRP: rupee 30 IRP: rupee 48
Review of literature
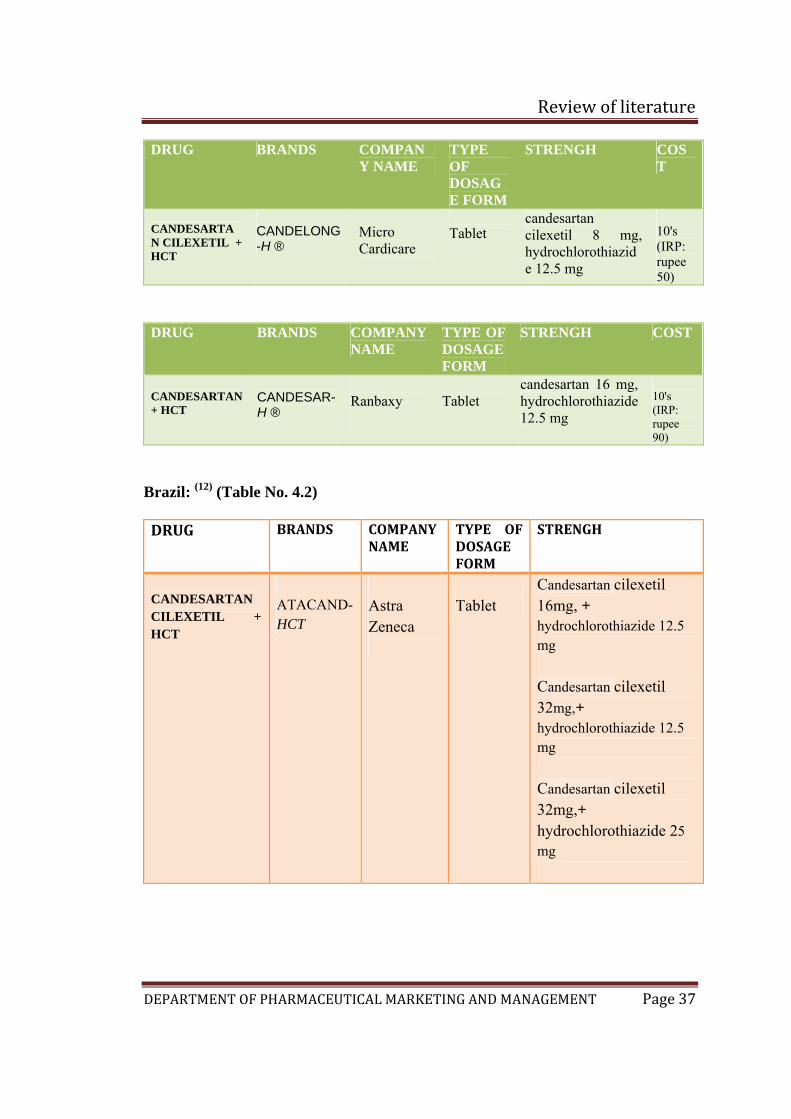
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 37
DRUG BRANDS COMPANY NAME
TYPE OF DOSAGE FORM
STRENGH COST
CANDESARTAN CILEXETIL + HCT
CANDELONG-H ®
Micro Cardicare
Tablet
candesartan cilexetil 8 mg, hydrochlorothiazide 12.5 mg
10's (IRP: rupee 50)
DRUG BRANDS COMPANY NAME
TYPE OF DOSAGE FORM
STRENGH COST
CANDESARTAN + HCT
CANDESAR-H ®
Ranbaxy
Tablet
candesartan 16 mg, hydrochlorothiazide 12.5 mg
10's (IRP: rupee 90)
Brazil: (12) (Table No. 4.2)
DRUG BRANDS COMPANY NAME
TYPE OF DOSAGE FORM
STRENGH
CANDESARTAN CILEXETIL + HCT
ATACAND- HCT
Astra Zeneca
Tablet
Candesartan cilexetil 16mg, + hydrochlorothiazide 12.5 mg Candesartan cilexetil 32mg,+ hydrochlorothiazide 12.5 mg Candesartan cilexetil 32mg,+ hydrochlorothiazide 25 mg
Review of literature
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 38
Market potential:
According to World Health Organisation (WHO) the mortality from cardiovascular
disease by the year 2020 in low to middle income countries will exceed deaths from
infectious and parasitic disease in all regions except sub-Saharan Africa, where
hypertension is a major risk factor. (16) Where in India also high blood pressure is a
major risk factor and better control can lead to prevention of 300,000 of 1.5 million
annual deaths from cardiovascular disease. (17)
Thus the market potential (in terms of prevalence) is huge. Recently, the JNC 7 (the
Seventh report of the Joint National Committee on Prevention, detection, evaluation,
and treatment of High Blood pressure) has defined blood pressure 120/80 mmHg to
139/89 mmHg as "Pre-hypertension.“ Pre-hypertension is not a disease category;
rather, it is a designation chosen to identify individuals at high risk of developing
hypertension. Hence, strategies devised to increase awareness can help in gaining
footholds in the latent potential market also.
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 38
5. METHODOLOGY
Source of Data:
The source for market research will include:
• Primary source: Primary data will be obtained from the identified respondents
by the administration of questionnaire following informed consent
Inclusion criteria:
a) Doctors who are cardiologist, general physician and general practitioners.
b) Registered pharmacists who are at retail outlets and hospitals
Exclusion criteria:
a) Doctors who do not belong to the specialties mentioned above and who
practice in Ayurvedic , Homeopathy, Unani etc are not included in the study
b) Pharmacist who are not registered and trainees are not included in the study
• Secondary source:
a) Journals
b) Trade and business journals
c) Internationals magazine
d) Textbook of pharmaceutical marketing and international marketing
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 39
e) Internet
f) Pharma pulse
g) Pharma biz
Method of collection of data:
Preliminary communication with doctors and pharmacists through personal
interview to get consent to participate in the survey
Sample size:
1. Doctors:
a) 50 Cardiologists
b) 25 General physicians
c) 25 General practitioners
2. Pharmacist:
a) 100 registered pharmacists
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 40
AL -AMEEN COLLEGE OF PHARMACY, BANGALORE-27
DEPARTMENT OF PHARMA MARKETING AND MANAGEMENT
QUESTIONNAIRE FOR DOCTOR
Q.1. How many patients with hypertension do you treat on average per week?
A. MALES:
a) Less than 10 (b) 11 to 15 (c) 16 to 20 (d) 21 to 30 (e) more than 30
B. FEMALES:
a) Less than 10 (b) 11 to 15 (c) 16 to 20 (d) 21 to 30 (e) more than 30
Q.2. Which age-group of patients are more prone to hypertension?
Sex of patient
Age group of patients in years
Female
Less than 35
36 to 45
46 to 55
More than 55
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 41
Male
Less than 35
36 to 45
46 to 55
More than 55
Q.3. Does the age of patient play a role while deciding upon the drug of choice?
(a) Yes (b) No
If yes please select the appropriate drug of choice to the corresponding age group.
Age – group in years
Drug of choice
Less than35
36 to 45
46 to 55
More than 55
Beta blockers
Alfa blockers
Calcium channel antagonists
ACE inhibitors
Angiotensin II antagonist
Diuretics
Central and peripheral sympatholytics
Direct vasodilators
Calcium channel antagonists + Diuretic
Beta blockers + Calcium channel antagonists
Calcium channel antagonists +
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 42
ACE inhibitors Diuretic + ACE inhibitors
Calcium channel antagonists + Angiotensin II antagonist
Angiotensin II antagonist + Diuretic
Alfa blockers + Diuretic
Angiotensin II antagonist + ACE inhibitors
Beta blockers + Diuretic
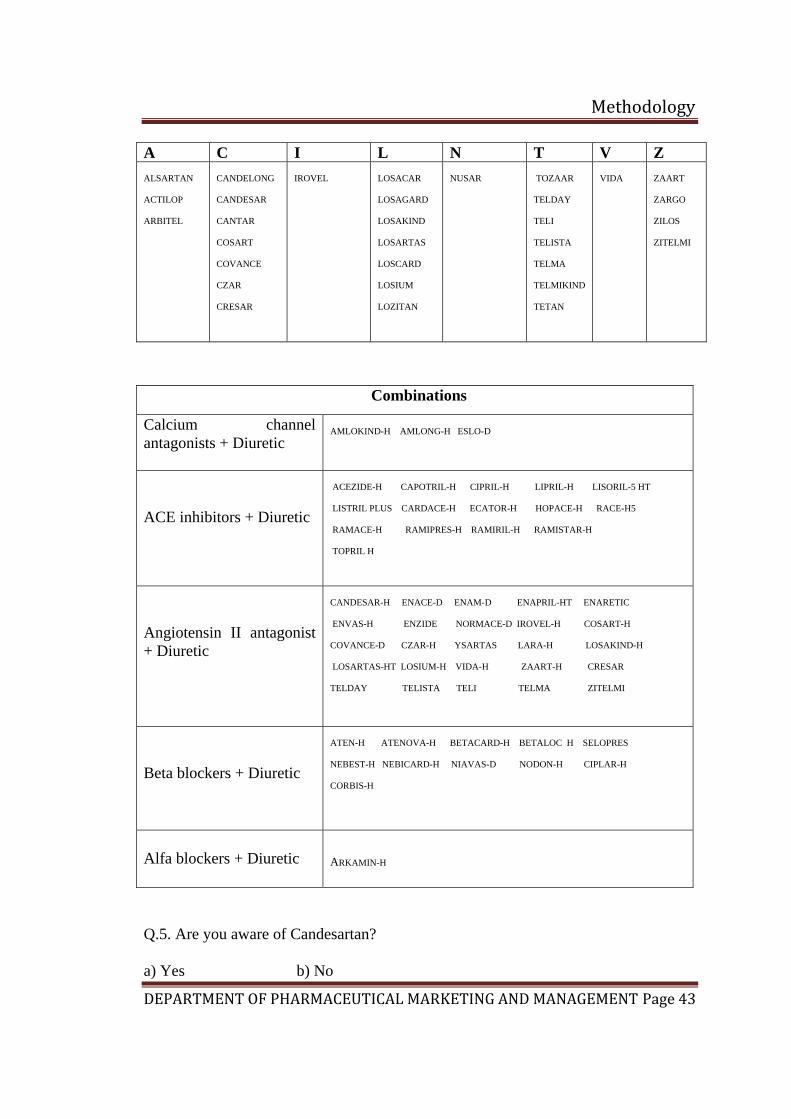
Q.4. Select the brand of your choice with respect to the following classes of drugs in
the treatment of hypertension
ACE inhibitors A B C D E F I L M ACETEN ACEBITOR ACINOPRIL
BQL BIOPRIL
CANVAS CIPRIL CARDACE CARDIOPRIL CORPRIL
DILVAS
ENACE ENAMATE ENAPRIL ENLACARD ENVAS ECATOR
FOSINACE FOVAS
INVORIL
LUPINACE LINVAS LIPRIL LISCARD LISITEC LISORIL LISOTEC LISTRIL
MINIPRIL MYOACE
P R S Z
PRILACE PREFACE
R-CORD RACE RAMACE RAMIHART RAMIL RAMIPRES RAMIRIL RAMISTAR
SCLERACE SERVACE
ZESTRIL ZIPRIL ZIRAM
Angiotensin II receptor antagonists
Methodology
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 43
A C I L N T V Z ALSARTAN ACTILOP ARBITEL
CANDELONG CANDESAR CANTAR COSART COVANCE CZAR CRESAR
IROVEL
LOSACAR LOSAGARD LOSAKIND LOSARTAS LOSCARD LOSIUM LOZITAN
NUSAR
TOZAAR TELDAY TELI TELISTA TELMA TELMIKIND TETAN
VIDA
ZAART ZARGO ZILOS ZITELMI
Combinations
Calcium channel antagonists + Diuretic
AMLOKIND-H AMLONG-H ESLO-D
ACE inhibitors + Diuretic
ACEZIDE-H CAPOTRIL-H CIPRIL-H LIPRIL-H LISORIL-5 HT LISTRIL PLUS CARDACE-H ECATOR-H HOPACE-H RACE-H5 RAMACE-H RAMIPRES-H RAMIRIL-H RAMISTAR-H TOPRIL H
Angiotensin II antagonist + Diuretic
CANDESAR-H ENACE-D ENAM-D ENAPRIL-HT ENARETIC ENVAS-H ENZIDE NORMACE-D IROVEL-H COSART-H COVANCE-D CZAR-H YSARTAS LARA-H LOSAKIND-H LOSARTAS-HT LOSIUM-H VIDA-H ZAART-H CRESAR TELDAY TELISTA TELI TELMA ZITELMI
Beta blockers + Diuretic
ATEN-H ATENOVA-H BETACARD-H BETALOC H SELOPRES NEBEST-H NEBICARD-H NIAVAS-D NODON-H CIPLAR-H CORBIS-H
Alfa blockers + Diuretic
ARKAMIN-H
Q.5. Are you aware of Candesartan?
a) Yes b) No
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 44
Please give opinion
………………………………………………………………………………………
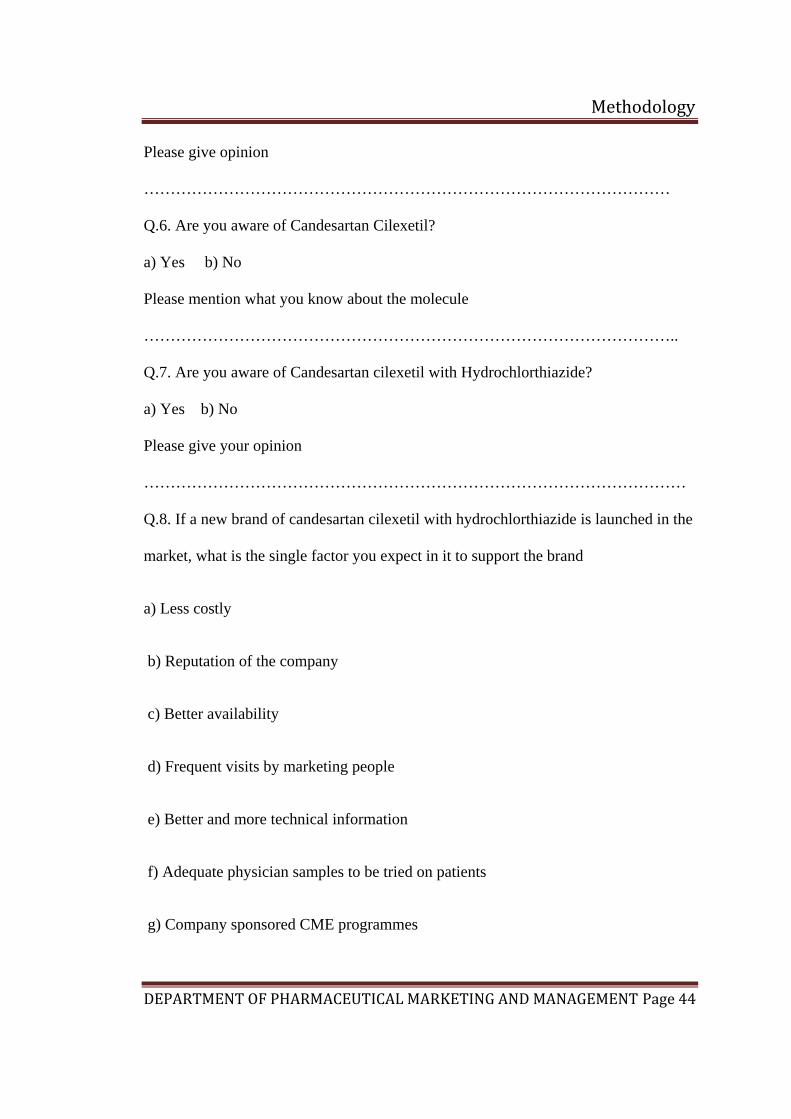
Q.6. Are you aware of Candesartan Cilexetil?
a) Yes b) No
Please mention what you know about the molecule
………………………………………………………………………………………..
Q.7. Are you aware of Candesartan cilexetil with Hydrochlorthiazide?
a) Yes b) No
Please give your opinion
…………………………………………………………………………………………
Q.8. If a new brand of candesartan cilexetil with hydrochlorthiazide is launched in the
market, what is the single factor you expect in it to support the brand
a) Less costly
b) Reputation of the company
c) Better availability
d) Frequent visits by marketing people
e) Better and more technical information
f) Adequate physician samples to be tried on patients
g) Company sponsored CME programmes
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 45
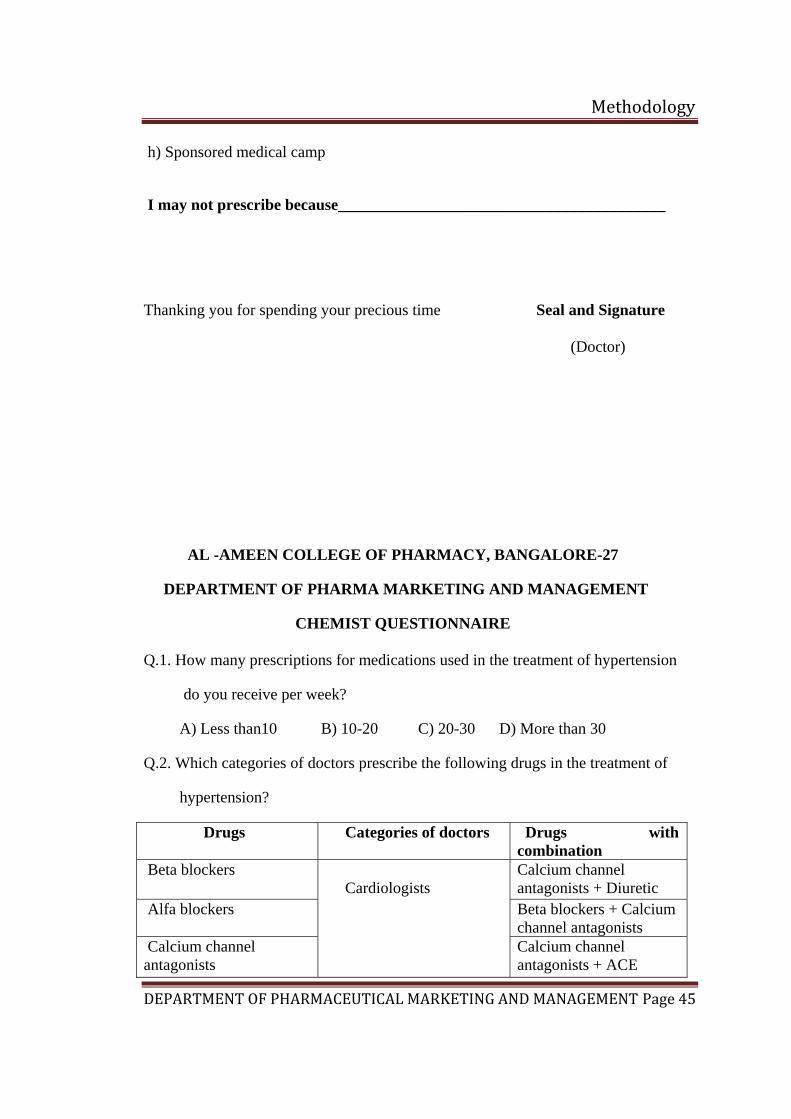
h) Sponsored medical camp
I may not prescribe because_________________________________________
Thanking you for spending your precious time Seal and Signature
(Doctor)
AL -AMEEN COLLEGE OF PHARMACY, BANGALORE-27
DEPARTMENT OF PHARMA MARKETING AND MANAGEMENT
CHEMIST QUESTIONNAIRE
Q.1. How many prescriptions for medications used in the treatment of hypertension
do you receive per week?
A) Less than10 B) 10-20 C) 20-30 D) More than 30
Q.2. Which categories of doctors prescribe the following drugs in the treatment of
hypertension?
Drugs Categories of doctors Drugs with combination
Beta blockers Calcium channel antagonists + Diuretic
Alfa blockers Beta blockers + Calcium channel antagonists
Calcium channel antagonists
Cardiologists
Calcium channel antagonists + ACE
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 46
inhibitors
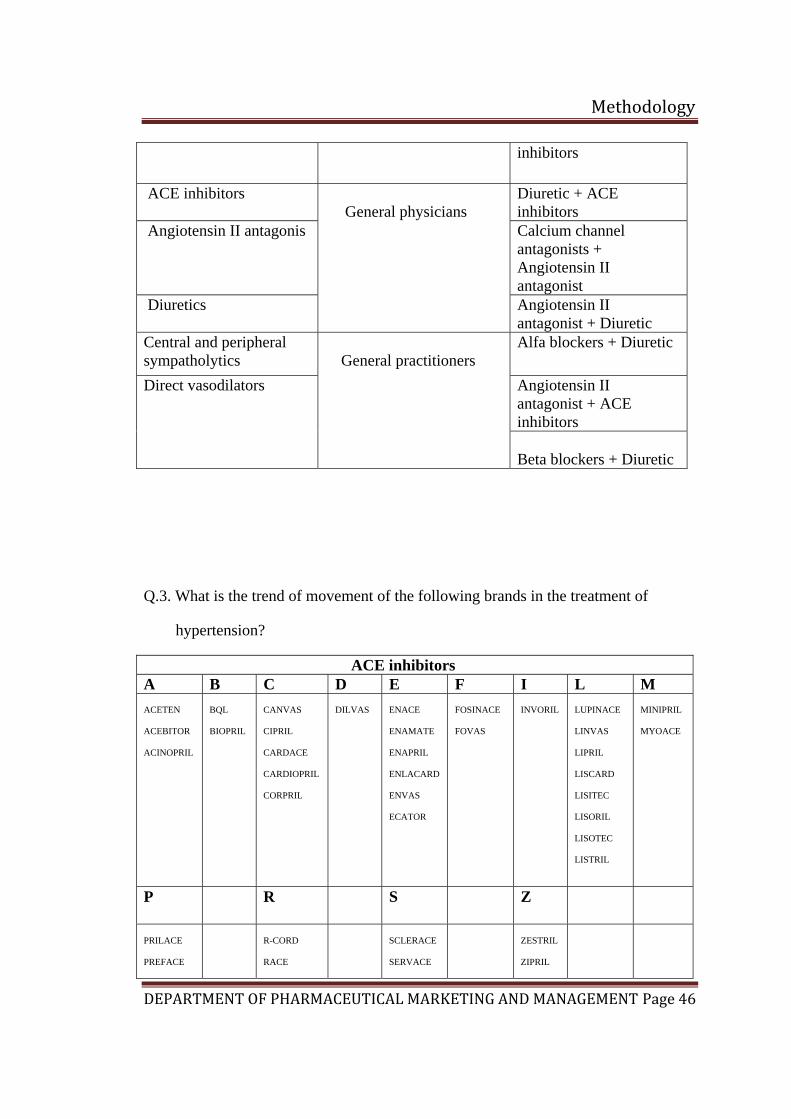
ACE inhibitors Diuretic + ACE inhibitors
Angiotensin II antagonis Calcium channel antagonists + Angiotensin II antagonist
Diuretics
General physicians
Angiotensin II antagonist + Diuretic
Central and peripheral sympatholytics
Alfa blockers + Diuretic
Angiotensin II antagonist + ACE inhibitors
Direct vasodilators
General practitioners
Beta blockers + Diuretic
Q.3. What is the trend of movement of the following brands in the treatment of
hypertension?
ACE inhibitors A B C D E F I L M ACETEN ACEBITOR ACINOPRIL
BQL BIOPRIL
CANVAS CIPRIL CARDACE CARDIOPRIL CORPRIL
DILVAS
ENACE ENAMATE ENAPRIL ENLACARD ENVAS ECATOR
FOSINACE FOVAS
INVORIL
LUPINACE LINVAS LIPRIL LISCARD LISITEC LISORIL LISOTEC LISTRIL
MINIPRIL MYOACE
P R S Z
PRILACE PREFACE
R-CORD RACE
SCLERACE SERVACE
ZESTRIL ZIPRIL
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 47
RAMACE RAMIHART RAMIL RAMIPRES RAMIRIL RAMISTAR
ZIRAM
Angiotensin II receptor antagonists A C I L N T V Z ALSARTAN ACTILOP ARBITEL
CANDELONG CANDESAR CANTAR COSART COVANCE CZAR CRESAR
IPSITA IROVEL
LOSACAR LOSAGARD LOSAKIND LOSARTAS LOSCARD LOSIUM LOZITAN
NUSAR
TOZAAR TELDAY TELI TELISTA TELMA TELMIKIND TETAN
VIDA
ZAART ZARGO ZILOS ZITELMI
Combinations
Calcium channel antagonists + Diuretic
AMLOKIND-H AMLONG-H ESLO-D
ACE inhibitors + Diuretic
ACEZIDE-H CAPOTRIL-H CIPRIL-H LIPRIL-H LISORIL-5 HT LISTRIL PLUS CARDACE-H ECATOR-H HOPACE-H RACE-H5 RAMACE-H RAMIPRES-H RAMIRIL-H RAMISTAR-H TOPRIL H
Angiotensin II antagonist + Diuretic
CANDESAR-H ENACE-D ENAM-D ENAPRIL-HT ENARETIC ENVAS-H ENZIDE NORMACE-D IROVEL-H COSART-H COVANCE-D CZAR-H YSARTAS LARA-H LOSAKIND-H LOSARTAS-HT LOSIUM-H VIDA-H ZAART-H CRESAR TELDAY TELISTA TELI TELMA ZITELMI
Methodology
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 48
Beta blockers + Diuretic
ATEN-H ATENOVA-H BETACARD-H BETALOC H SELOPRES NEBEST-H NEBICARD-H NIAVAS-D NODON-H CIPLAR-H CORBIS-H
Alfa blockers + Diuretic
ARKAMIN-H
Q.4. Which is/are the fastest moving brand(s) of candesartan and its combination?
Drug Drug + diuretic CANDELONG CANDESAR CANTAR IPSITA
CANDESAR-H
Date : Thank You
Place : Seal and Signature
Chemist/pharmacist
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 38
6. RESULTS
6.1 Country analysis: (Secondary data)
Brazil (18)(19)(20)(23)
Brazil became an independent nation in 1822 after three centuries under the rule of
Portugal. It has pursued industrial and agricultural growth and development exploiting
vast natural resources and a large labor pool. Today, it is South America's leading
economic power and a regional leader. Being the largest and most populous country
in South America, Brazil continues to feel the pressure from highly unequal income
distribution. Brazil is located in the eastern part of South America, bordering the
Atlantic Ocean, spreading across 8,511,965 sq km. It shares common borders with
every South American country except Chile and Ecuador. Brazilian climate can be
described as tropical, but temperate in southern part. It is rich with natural resources
like bauxite, gold, iron ore, manganese, nickel, phosphates, platinum, tin, uranium,
petroleum, hydropower and timber.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 39
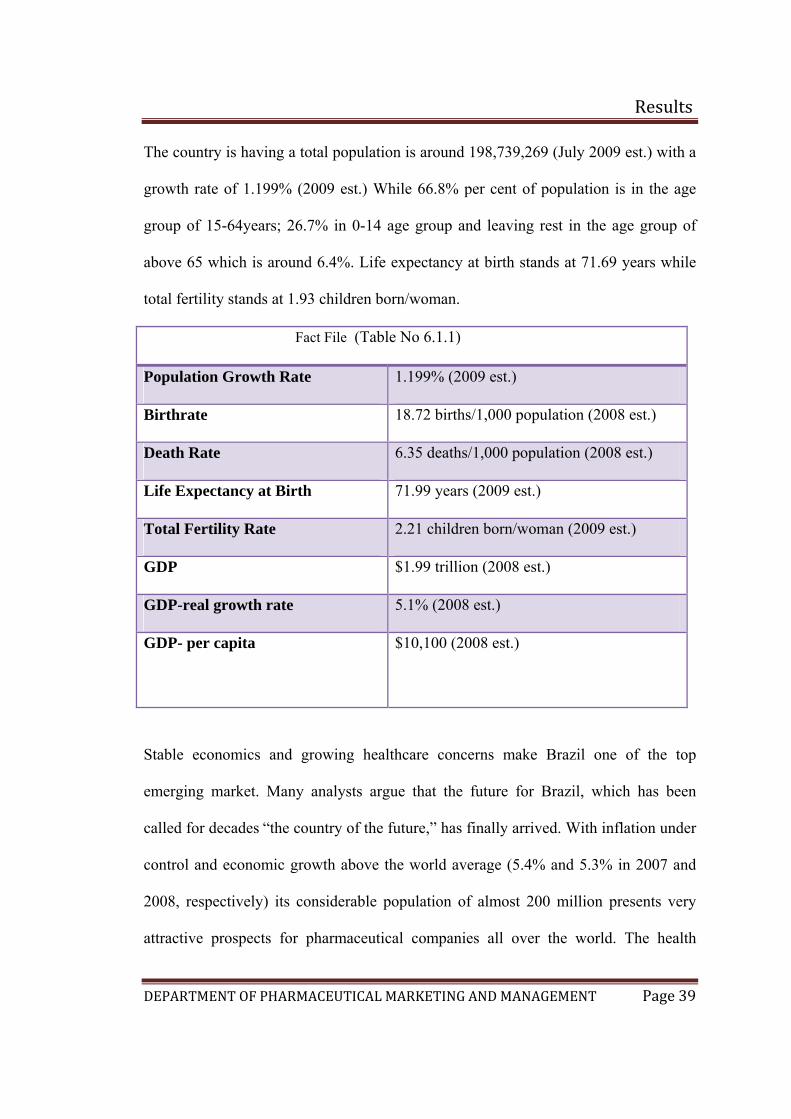
The country is having a total population is around 198,739,269 (July 2009 est.) with a
growth rate of 1.199% (2009 est.) While 66.8% per cent of population is in the age
group of 15-64years; 26.7% in 0-14 age group and leaving rest in the age group of
above 65 which is around 6.4%. Life expectancy at birth stands at 71.69 years while
total fertility stands at 1.93 children born/woman.
Fact File (Table No 6.1.1)
Population Growth Rate 1.199% (2009 est.)
Birthrate 18.72 births/1,000 population (2008 est.)
Death Rate 6.35 deaths/1,000 population (2008 est.)
Life Expectancy at Birth 71.99 years (2009 est.)
Total Fertility Rate 2.21 children born/woman (2009 est.)
GDP $1.99 trillion (2008 est.)
GDP-real growth rate 5.1% (2008 est.)
GDP- per capita $10,100 (2008 est.)
Stable economics and growing healthcare concerns make Brazil one of the top
emerging market. Many analysts argue that the future for Brazil, which has been
called for decades “the country of the future,” has finally arrived. With inflation under
control and economic growth above the world average (5.4% and 5.3% in 2007 and
2008, respectively) its considerable population of almost 200 million presents very
attractive prospects for pharmaceutical companies all over the world. The health
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 40
sector as a whole represents 8% of the Brazilian GDP, around US$80 billion per year.
Government purchases represent 50% of the market for medical equipments, and
more than 90% of the vaccines and 25% of all drugs (Brazilian Ministry of Health).
On the foreign trade side, Brazilian products totaled more than US$961 million in
exports in 2008, a 29% increase from 2007. The main export markets are Venezuela
(14%), Argentina (13%) and the USA (12%). On the other hand, imports amounted to
US$ 4.28 billion, an increase of 21% year over year, coming mainly from the USA
(19%), Germany and Switzerland (13% each). For example, all 450 tons of
amoxicillin (antibiotics) consumed per year are imported.
External Sector:
The Lula administration has used the last few years of solid global demand, surging
commodity prices and elevated liquidity to lower external indebtedness, smooth its
debt maturity profile, and improve currency and interest rate dynamics. Massive
capital inflows have allowed foreign exchange reserves to grow to around USD
236.1bn (equivalent to more than a year worth of imports) and Brazil has become a
net international creditor for the first time in its history. On the downside, we expect
the Current Account will balance to end the year in negative territory. We estimate the
CA deficit will amount to around 1.8% of GDP this year, but it will continue to be
covered by FDI, even under the current tight global financial conditions.
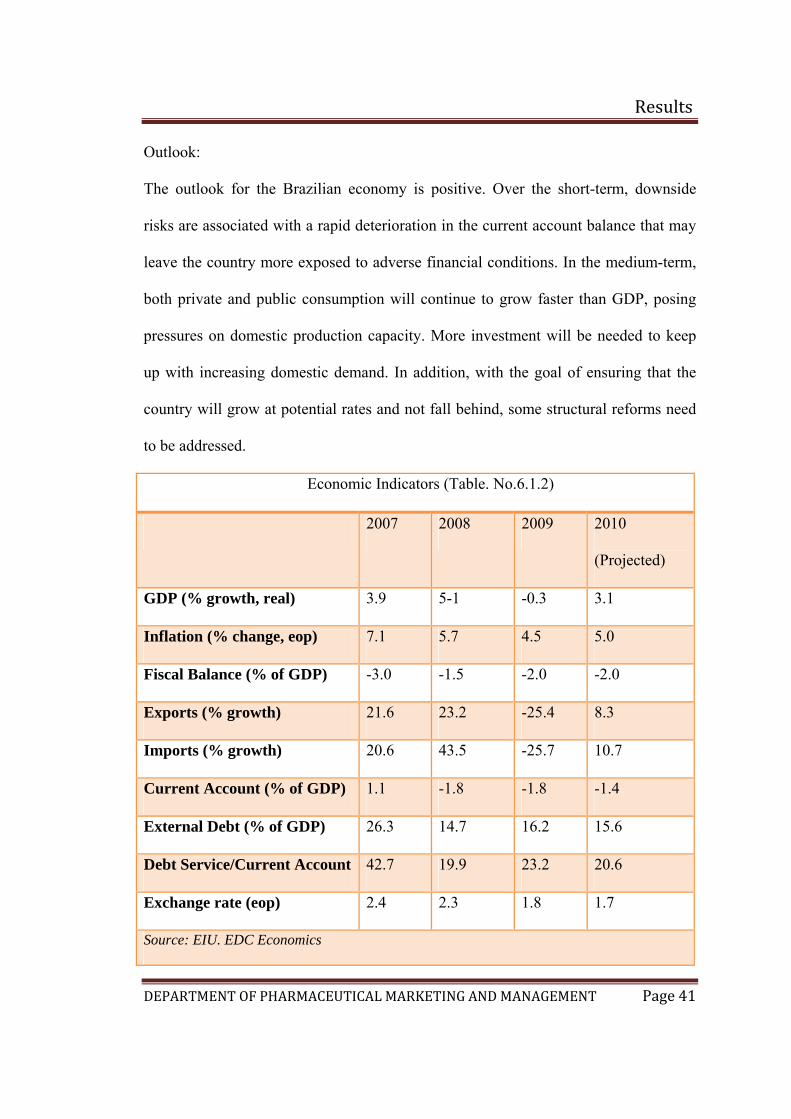
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 41
Outlook:
The outlook for the Brazilian economy is positive. Over the short-term, downside
risks are associated with a rapid deterioration in the current account balance that may
leave the country more exposed to adverse financial conditions. In the medium-term,
both private and public consumption will continue to grow faster than GDP, posing
pressures on domestic production capacity. More investment will be needed to keep
up with increasing domestic demand. In addition, with the goal of ensuring that the
country will grow at potential rates and not fall behind, some structural reforms need
to be addressed.
Economic Indicators (Table. No.6.1.2)
2007 2008 2009 2010
(Projected)
GDP (% growth, real) 3.9 5-1 -0.3 3.1
Inflation (% change, eop) 7.1 5.7 4.5 5.0
Fiscal Balance (% of GDP) -3.0 -1.5 -2.0 -2.0
Exports (% growth) 21.6 23.2 -25.4 8.3
Imports (% growth) 20.6 43.5 -25.7 10.7
Current Account (% of GDP) 1.1 -1.8 -1.8 -1.4
External Debt (% of GDP) 26.3 14.7 16.2 15.6
Debt Service/Current Account 42.7 19.9 23.2 20.6
Exchange rate (eop) 2.4 2.3 1.8 1.7
Source: EIU. EDC Economics
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 42
Market Spotlight: The economy has gone out of recession in the second quarter.
• Both equity market and the currency are showing signs of recovery.
• The Central Bank is expected to hold rates for the rest of the year.
• The country has recently signed bilateral agreements with China for USD15bn
and is reviewing proposals for a new regulatory framework for the recently
discovered deepwater oil and gas reserves.
• The three rating agencies now rate the Brazil investment grade
• The government has announced a new 2% tax on foreign investment on equity
and bonds.
General Political Environment:
Brazilian politics are characterized by a fractiousness that mirrors the country’s
diverse socioeconomic make-up. Relations are generally difficult between the
executive and the legislature, as well as between federal and state governments. In
addition, a tradition of switching parties has made party politics and political strength
in Congress fluid. In 2007 the Supreme Court barred members of Congress from
party-hopping; this will likely forge stronger party loyalty over time.
For now political progress requires constant horse-trading that slows the passage of
reforms, including those widely considered necessary to maintain fiscal sustainability
and to accelerate growth to a level that will move Brazil forward. A difficult
balancing between promoting business and making progress on social issues
undermines the government’s ability to meet expectations on all fronts.
Populist president Luiz Inácio Lula da Silva (Lula) won a second term in October
2006 and has fashioned an 11-party Partido dos Trabalhadores (PT) -led coalition.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 43
Lula’s greatest challenge for 2009 and 2010 will be to construct an electoral coalition
out of the current government in preparation for elections in October 2010. He will
seek to ensure that Brazil’s next President is also from the PT and committed to his
policies. He has chosen to back a solid PT performer, Lula’s task is made more
difficult by the economic crisis and his administration’s priority is tackling the
negative effects of the global economic slowdown, including a slowing of important
flows of FDI and rising unemployment rates. Lula’s administration is focussing on its
expansionary "growth acceleration" programme of public investment (Programade
Aceleraçãodo Crescimento, or PAC).
Although Brazil’s ratings for control of corruption are improving, corruption is an
ongoing concern. It is more visible now than in the past because of increased
transparency and willingness to prosecute. Lula has skillfully remained at arm’s
length of the various corruption scandals that have touched many of his close allies as
well as his PT party.
Investment Environment:
Lula is a poster child for the moderate left in Latin America, promoting policies that
strengthen the investment environment. This said, Lula advocates for both
government participation in the economy and respect for investors’ contractual rights;
he actively promotes public-private partnerships, not privatizations, to attract private
capital. This approach functions as a moderate disincentive to investment. Despite
significant progress in the liberalization of the foreign exchange regime, important
residual controls remain. Foreign currency bank accounts (such as in USD) are not
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 44
permitted in Brazil. Regulatory agencies are weak and the bureaucracy is
cumbersome. According to the World Bank’s 2008 Doing Business survey,
procedural requirements to start a business in Brazil take 152 days against a regional
average of 60.7 days. The judicial system is generally regarded as fair, but is
considered slow and complex.
Political Outlook:
A mix of moderate nationalism and neo-liberal economic policies will likely continue
to underpin Lula’s policy program, striking a balance between the interests of the
country’s various stakeholders. However, for the foreseeable future the
administration’s energies are expected to be directed to the management of oil policy
and the 2010 elections. On the international front, Lula will pursue his diplomatic
campaign to promote Brazil as the region’s leader and a key player on the world
stage.
Pharmaceutical market scenario:
Emerging pharmaceutical markets in Western Europe, the US and Japan are mature.
The top 10 key pharmaceutical markets accounts for majority of sales amounting to
US$529.5 billion. The seven emerging markets such as China, Brazil, Mexico, South
Korea, India, Turkey and Russia has a growth by 12-13% (US$ 85-90 billion) in
2008.
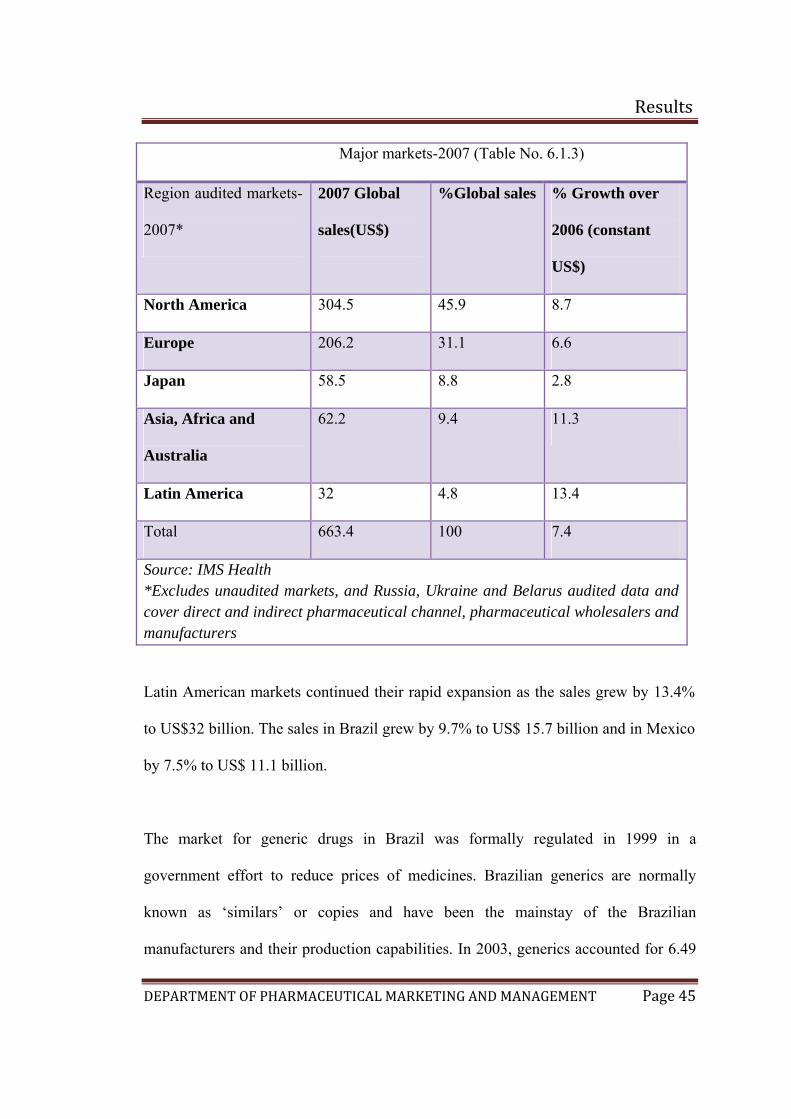
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 45
Major markets-2007 (Table No. 6.1.3)
Region audited markets-
2007*
2007 Global
sales(US$)
%Global sales % Growth over
2006 (constant
US$)
North America 304.5 45.9 8.7
Europe 206.2 31.1 6.6
Japan 58.5 8.8 2.8
Asia, Africa and
Australia
62.2 9.4 11.3
Latin America 32 4.8 13.4
Total 663.4 100 7.4
Source: IMS Health *Excludes unaudited markets, and Russia, Ukraine and Belarus audited data and cover direct and indirect pharmaceutical channel, pharmaceutical wholesalers and manufacturers
Latin American markets continued their rapid expansion as the sales grew by 13.4%
to US$32 billion. The sales in Brazil grew by 9.7% to US$ 15.7 billion and in Mexico
by 7.5% to US$ 11.1 billion.
The market for generic drugs in Brazil was formally regulated in 1999 in a
government effort to reduce prices of medicines. Brazilian generics are normally
known as ‘similars’ or copies and have been the mainstay of the Brazilian
manufacturers and their production capabilities. In 2003, generics accounted for 6.49
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 46
per cent of the total pharmaceutical market in Brazil at ex-manufacturers prices. The
generic market in year 2008 was around US$ 2.3 billion and use to cover 19.1% of the
total pharmaceutical market. Public awareness of generic alternatives is clearly
growing and the sector is also likely to remain attractive to foreign players.
Due to the depreciation of Brazil’s currency against the US dollar, the Brazilian
pharmaceutical market has fallen in dollar values in 2009. Controlled drug prices are
increasing below inflational levels and demand is contained by a falling economic
growth projected in 2009. For the industry, price controls are not directly linked to
consumption levels. In fact, between 1997 and 2008, the pharmaceutical market by
volume increased significantly only in 2004.
The pharmacy sector in dollar values performed exceptionally well in 2008, but the
sector is starting to register slower growth in the first quarter of 2009. Generic
medicines continue to grow at a higher rate than overall pharmacy sales, and are
expected to represent 20% of the sector by volume in 2010. Foreign participation in
the generic sector has increased.(10)
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 47
Epidemiology of hypertension in Brazil (16 )(21)
Cardiovascular diseases are the leading cause of premature death in industrialized
countries and the World Health Organization (WHO) predicts that by the year 2020
the mortality from cardiovascular disease in low- to middle-income countries will
exceed deaths in all regions except sub-Saharan Africa. A study carried out in 2004
describes the prevalence of hypertension in an urban adult population in north east
Brazil and identifies the most common risk factors, and explores differences in
prevalence rates and risk factors in different socioeconomic areas within the urban
study area.
The prevalence of hypertension (31.8%) in this population is similar to reports from
other developing countries using similar diagnostic criteria. It has been reported that
hypertension affects up to 40% of the adult Brazilian population and is higher in the
urban areas. Most studies however come from the prosperous southern part of the
country. Catanduva (Sao Paulo state), for example (a municipality with high
socioeconomic profile), had a prevalence of 32%, Bambui reported 45% in adults and
Pelotas 20%. In contrast, a small study of the Xavante Indians in rural central Brazil
described a prevalence of 5% in males and 8% in females. Prevalence of hypertension
by age and sex was mentioned in the table below
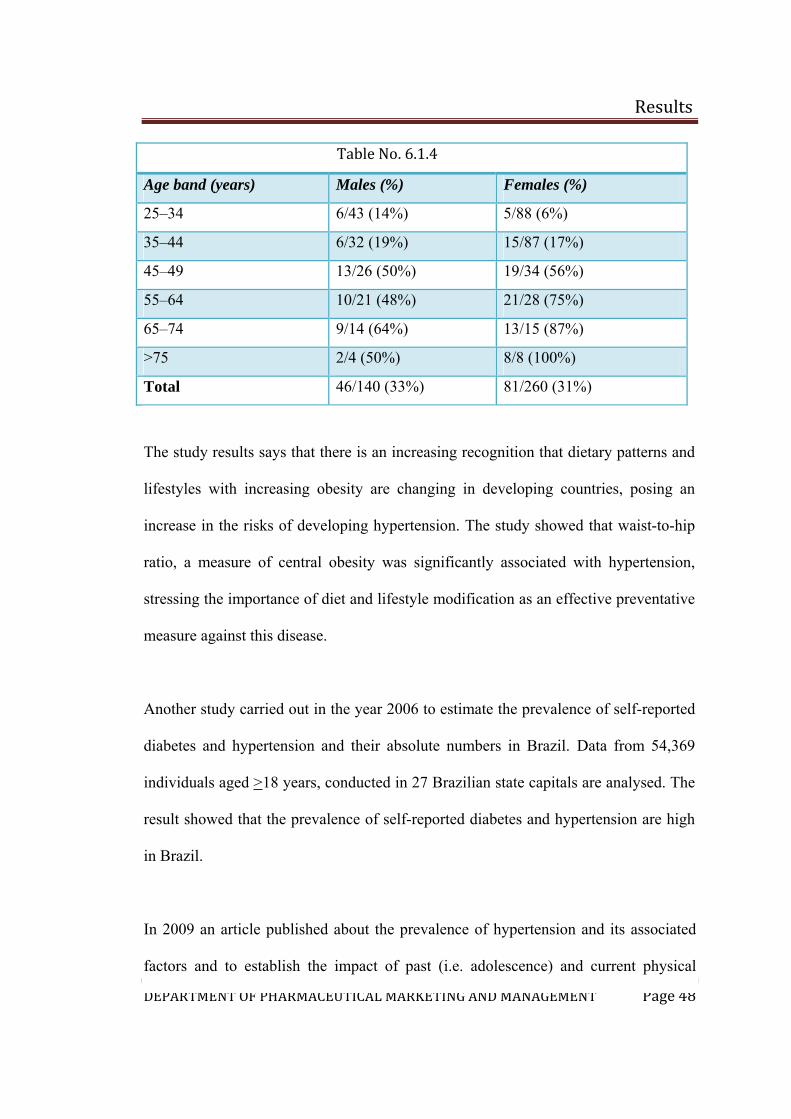
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 48
Table No. 6.1.4
Age band (years) Males (%) Females (%)
25–34 6/43 (14%) 5/88 (6%)
35–44 6/32 (19%) 15/87 (17%)
45–49 13/26 (50%) 19/34 (56%)
55–64 10/21 (48%) 21/28 (75%)
65–74 9/14 (64%) 13/15 (87%)
>75 2/4 (50%) 8/8 (100%)
Total 46/140 (33%) 81/260 (31%)
The study results says that there is an increasing recognition that dietary patterns and
lifestyles with increasing obesity are changing in developing countries, posing an
increase in the risks of developing hypertension. The study showed that waist-to-hip
ratio, a measure of central obesity was significantly associated with hypertension,
stressing the importance of diet and lifestyle modification as an effective preventative
measure against this disease.
Another study carried out in the year 2006 to estimate the prevalence of self-reported
diabetes and hypertension and their absolute numbers in Brazil. Data from 54,369
individuals aged >18 years, conducted in 27 Brazilian state capitals are analysed. The
result showed that the prevalence of self-reported diabetes and hypertension are high
in Brazil.
In 2009 an article published about the prevalence of hypertension and its associated
factors and to establish the impact of past (i.e. adolescence) and current physical
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 49
activity on hypertension. The report says prevalence of hypertension is high among
Brazilians and markedly different among population subgroups. There was no robust
evidence of association between adolescence physical activity practice and
hypertension in later life.
The Pharmaceutical Intellectual Property (IP) Environment in Brazil:
Brazil's industrial property law (Law 9,279/1996) became effective in May 1997.
Concerns continue about a provision in Brazil’s industrial property law that disallows
importation as a means of satisfying the requirement that a patent be “worked” in
Brazil. Law 10,196 (2001) includes some problematic provisions, including a
requirement that Health Ministry approval be obtained prior to the issuance of a
pharmaceutical patent. This raises concerns with respect to Article 27 of the TRIPS
Agreement, and U.S. officials have raised this concern with their Brazilian
counterparts.
Brazil is one of the largest markets for pharmaceutical products in the world, with one
pharmacy for every 3,300 inhabitants, which is almost twice the number
recommended by the World Health Organization (WHO). The market has the
potential to double and reach more than $ 15 billion. This could be a dream scenario
for the pharmaceutical industry, but several hindrances stand in the way. The industry
is fighting battles against a few domestic laboratories and against ANVISA, (National
Sanitary Vigilance Agency), an agency of the Brazilian Ministry of Health.
Patent applications filed in Brazil on or after May 15, 1997, including PCT
applications having a later international filing date, fully benefit from the new law,
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 50
particularly concerning the patentability of pharmaceutical products and processes
and the 20-year patent term. According to article. 68 of the new law, a patent is
subject to a compulsory license upon request by a third party if (i) the patentee
exercises patent rights in an abusive manner or (ii) by means of the patent the patentee
practices abuse of economic power that is proven under the terms of the law by an
administrative or court decision. A patent will also be subject to a compulsory license
if (iii) the invention is not effectively worked in Brazil or (iv) if commercialization
does not meet the needs of the market.
There still lot of flaws in the IPR issues which are contradictory in nature. Such as
,there has been an urgency to negotiate the prices of life-saving drugs with health
authorities from those countries rather than face the imminent granting of compulsory
licenses of their patents. The policies adopted by the Brazilian government in May
2007, that the government issued the first compulsory license on the grounds of public
interest after negotiations with patent owner Merck when price reduction of the HIV
drug Efavirenz fell through. This was without doubt the most severe penalty the
Brazilian government has applied.
The Brazilian government approved two laws (9,787) of February 10 1999, which
regulates provisions on generic drugs, and Law 10,603 of December 17 2002, which
protects confidential data and information submitted for obtaining approval of
agrochemical, veterinary and pharmaceutical products.
A further concern of the pharmaceutical companies is that Brazil’s Regulatory Law
10,603 of December 17 2002 exempts regulatory officers from responsibility in
granting sanitary registrations to third parties that cover patented drugs. In some
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 51
countries, such as the US, the regulatory officer will check the Orange Book listing to
determine whether the granting of a registration on a drug to a third party will infringe
prior patent rights.(12)
It should be clear that the lack of a dynamic and modern IP system will block
substantial investment and divert it to other developing countries whose laws and
policies favor patent rights. Ironically, Brazil’s market potential as a net taker of
investments is widely acknowledged.
The backlog of patent applications pending substantive examination at the Brazilian
Patent and Trademark Office (PTO) is alarming. The simple reason is the inadequate
number of patent examiners – approximately 200 – responsible for examining all of
the technological areas. The result is a seven to eight year delay for a pharmaceutical
patent application to issue.
High tax rates and price control:
In addition to the high tax rate applied to pharmaceuticals in Brazil, which, at present,
amounts to 35% of the end price of the medicines, the pharmaceutical industry faces
another major problem with the pricing of its products. Since the enactment of Law
10,742/2003, the price of any medicine must be approved prior to its launch in the
market. After this readjustments are only granted on an annual basis by the Brazilian
Chamber for the Regulation of the Market of Medicines (CMED).
Influencing advertising:
Another concern of pharmaceutical companies doing business in Brazil relates to the
advertising of their products. For more than 24 years there was no official control
over advertising of pharmaceutical products. In November 2000 ANVISA
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 52
implemented rigorous rules through Resolution RDC 102. A survey carried out by
IBOPE Monitor compared the first trimesters of the years 2000 through 2007, and
found that pharmaceutical industry investment in publicity had grown almost 70%
over the past three years, as opposed to 33,6% growth in publicity in general.(12)
Multiple trade marks:
Another concern for the pharmaceutical companies is ANVISA’s prohibition to the
effect that a given company cannot sell the same substance under two different marks.
This prohibition appeared in an internal ANVISA note issued in August 2004, and
was later confirmed by an ANVISA Committee. It states that the same pharmaceutical
company cannot own more than one registration covering the same product in the
same presentation identified by different trade marks. According to the internal
instruction, the legal basis for this prohibition is Article 124, Item XX, of Law
9,279/96, which happens to be the Brazilian Patent and Trade Mark Law.
It is clear to trade mark attorneys that ANVISA has misinterpreted the provision.
What the Patent and Trade Mark Law prohibits is the “duplication of trade marks in
the name of a single owner for the same product, unless they are displayed in a
sufficiently distinctive form”. As in foreign laws, the purpose of this provision is to
prevent trade mark owners from duplicating trade marks in an attempt to circumvent
cancellation proceedings on the grounds of non-use. ANVISA has not only
misinterpreted the provisions of the Trade Mark Law, but is also applying the Law
when it is not within its jurisdiction to do so.
Conflict between marks:
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 53
Prior to 2005, whenever there was a conflict between two product names (marks),
ANVISA would give priority to that which identified the product that was first
submitted for registration before ANVISA, even over a previously applied-for or even
registered trade mark for a product which was submitted to ANVISA at a later date.
Surprisingly, however, since June 2005 ANVISA has been recognizing the rights of
trade mark owners and applicants over the rights of the companies which have merely
applied for a product registration, even when the product was registered with
ANVISA at a date earlier than that of the filing of the application or registration at the
Brazilian PTO.
The decision to empower ANVISA with the approval of pharmaceutical patents does
not make sense. It will serve to stimulate conflict between PTO examiners and
ANVISA’s authorities. In addition, the legitimacy of several of ANVISA’s actions
should be challenged on the basis of being unconstitutional.(12)
Drug registration in Brazil
Product registration in Brazil is a lengthy task. Only companies with local operations
have standing to apply for registration of medical products. Depending on the product,
the registration may be valid from two to five years and can be renewed continuously
for the same period. In the case of pharmaceutical drugs, one must inform the active
and inactive ingredients. Instructions, directions, cautions, labels, brochures, and
pertinent information about the products must be translated into Portuguese. The
product registration process often takes more than one year. If the process takes
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 54
longer than three months, importers and producers are allowed to use a protocol
number provided by the Brazilian authorities to distribute their products in Brazil.
The only countries that offer incentives for the registration of generics/copies/similars
are Argentina, Brazil and Chile. These three countries discount the registration
application fee for generic drugs and in addition Brazil offers a shorter evaluation
time for generic and similar products. The cost of registering a product is $27,000 as
on March, 2005. According to the Brazilian legislation, the production,
manufacturing, imports, exports and sales of any medical, pharmaceuticals and
cosmetics products can only be handled by authorized companies, registered with the
ANVISA - National Sanitary Vigilance Agency, an agency of the Brazilian Ministry
of Health. Manufacturers have to disclose to the local authorities, through their agents
(local distributors), the quantitative and qualitative formula of their products, which
should be patented in Brazil before the product is introduced into the market, and at
the time of registration. This has to be described on the registration document.
Time & Fees
The length of time taken to approve drugs in each country is different. All countries in
Latin America, except Brazil, Chile and Cuba have shorter drug approval time than
more developed countries, such as Australia (17 months), countries in European
Union (14-30 months), Canada (17 months) and USA (14 months). The cost of
registering a product is low in Latin America. While Chile offer higher fees for the
registration of generics and similars than for the registration of a new product; Brazil
offer incentives for the registration of generics/copies/similars and discount the
registration application fee for generic drugs.
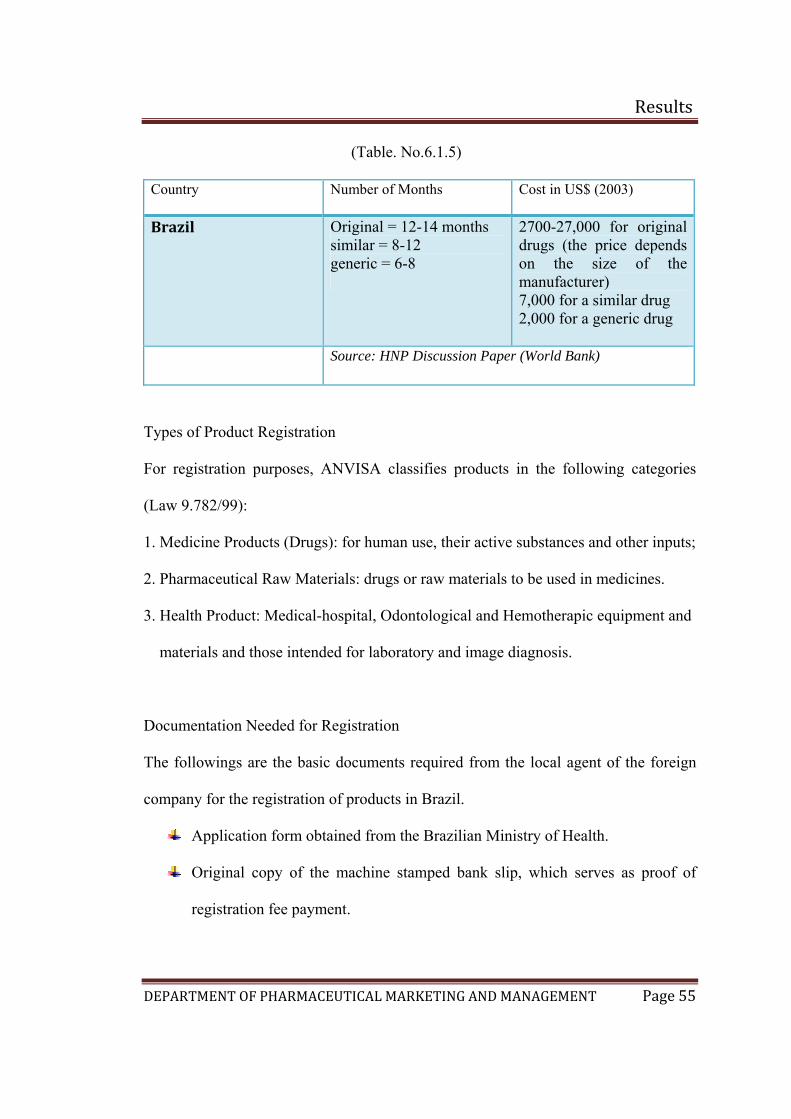
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 55
(Table. No.6.1.5)
Country Number of Months Cost in US$ (2003)
Brazil Original = 12-14 months similar = 8-12 generic = 6-8
2700-27,000 for original drugs (the price depends on the size of the manufacturer) 7,000 for a similar drug 2,000 for a generic drug
Source: HNP Discussion Paper (World Bank)
Types of Product Registration
For registration purposes, ANVISA classifies products in the following categories
(Law 9.782/99):
1. Medicine Products (Drugs): for human use, their active substances and other inputs;
2. Pharmaceutical Raw Materials: drugs or raw materials to be used in medicines.
3. Health Product: Medical-hospital, Odontological and Hemotherapic equipment and
materials and those intended for laboratory and image diagnosis.
Documentation Needed for Registration
The followings are the basic documents required from the local agent of the foreign
company for the registration of products in Brazil.
Application form obtained from the Brazilian Ministry of Health.
Original copy of the machine stamped bank slip, which serves as proof of
registration fee payment.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 56
Trade Permit ("Alvará de Funcionamento") issued by the State authority to the
manufacturer's distributor.
Same type of document ("Autorização de Funcionamento"), issued by the
Federal authority to the manufacturer's distributor.
Document showing the technical responsibility of the distributor/
manufacturer, issued by the certification entity.
Technical Report on the product, informing the components of the formula,
instructions, directions, cautions, etc.
Label sample, brochures, pertinent information about the products, all
translated into Portuguese;
For products not clearly mentioned in the Brazilian law, it is mandatory to
provide information about their utilization in order to demonstrate its efficacy
and safety;
Copy of the registration granted to the products at the country of origin (or
copy of the Free Sale Certificate);
Copy of legal document, by which the manufacturer authorizes its distributor
to trade and distribute the products.
If a medical equipment, all documents showing product safety, country of
origin, detailed (exploded view) of the equipment’s inner parts and user
manual, have to be presented for registration.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 57
Registration of Company in Brazil
Setting up new companies is relatively easy and inexpensive in Brazil. There are four
steps to launch business viz. procedures required to establish a business, the
associated time and cost, and the minimum capital requirement. Entrepreneurs can
expect to go through 17 steps to launch a business over 152 days on average, at a cost
equal to 11.7 per cent of gross national income (GNI) per capita. There is no
minimum deposit requirement to obtain a business registration number, compared
with the regional average of 28.9 per cent of GNI and OECD average of 44.1 per cent
of GNI.
A company should go for registration if any of the following parameters exists:
It is a limited liability company
It operates in the country’s most populous city
The business is 100 per cent domestically owned and has five owners, none of
whom is a legal entity
It has a start-up capital of 10 times income per capita at the end of 2003, paid
in cash
It leases the commercial plant and offices and is not a proprietor of real estate
It does not qualify for investment incentives or any special benefits
The business has up to 50 employees one month after the commencement of
operations, all of them nationals
The turnover is at least 100 times income per capita, and
The business has a company deed 10 pages long.
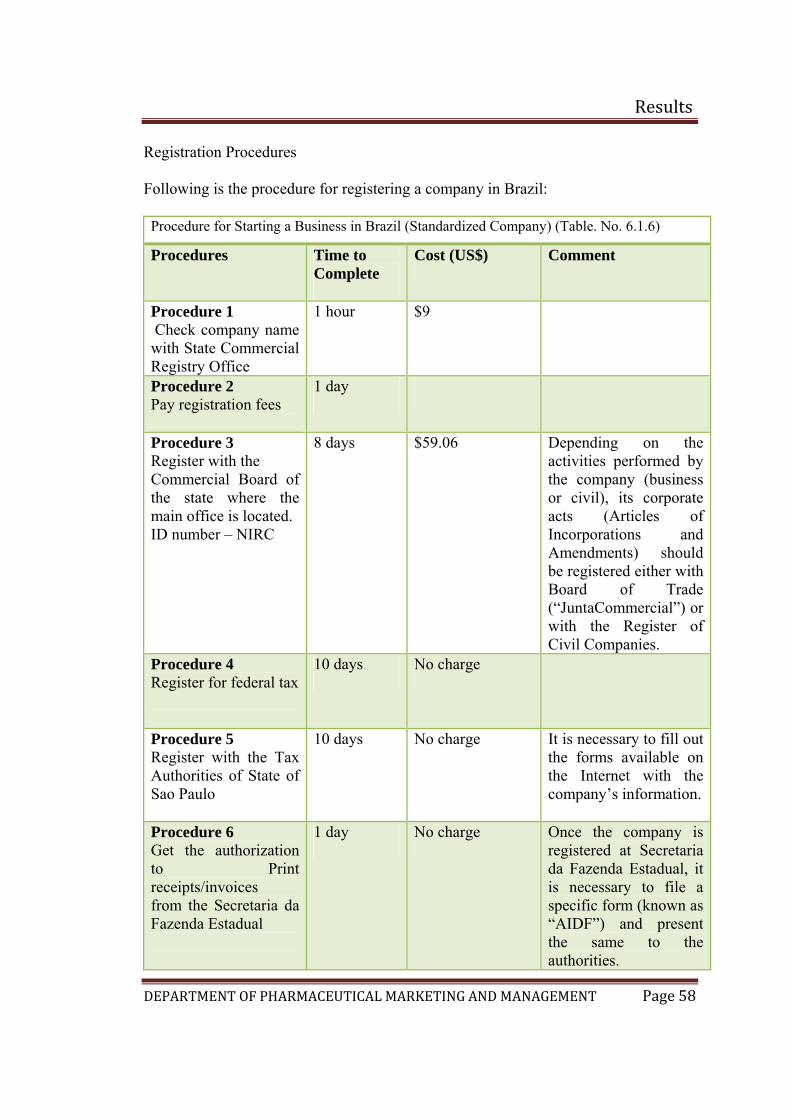
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 58
Registration Procedures
Following is the procedure for registering a company in Brazil:
Procedure for Starting a Business in Brazil (Standardized Company) (Table. No. 6.1.6)
Procedures Time to Complete
Cost (US$) Comment
Procedure 1 Check company name with State Commercial Registry Office
1 hour $9
Procedure 2 Pay registration fees
1 day
Procedure 3 Register with the Commercial Board of the state where the main office is located. ID number – NIRC
8 days $59.06 Depending on the activities performed by the company (business or civil), its corporate acts (Articles of Incorporations and Amendments) should be registered either with Board of Trade (“JuntaCommercial”) or with the Register of Civil Companies.
Procedure 4 Register for federal tax
10 days No charge
Procedure 5 Register with the Tax Authorities of State of Sao Paulo
10 days No charge It is necessary to fill out the forms available on the Internet with the company’s information.
Procedure 6 Get the authorization to Print receipts/invoices from the Secretaria da Fazenda Estadual
1 day No charge Once the company is registered at Secretaria da Fazenda Estadual, it is necessary to file a specific form (known as “AIDF”) and present the same to the authorities.
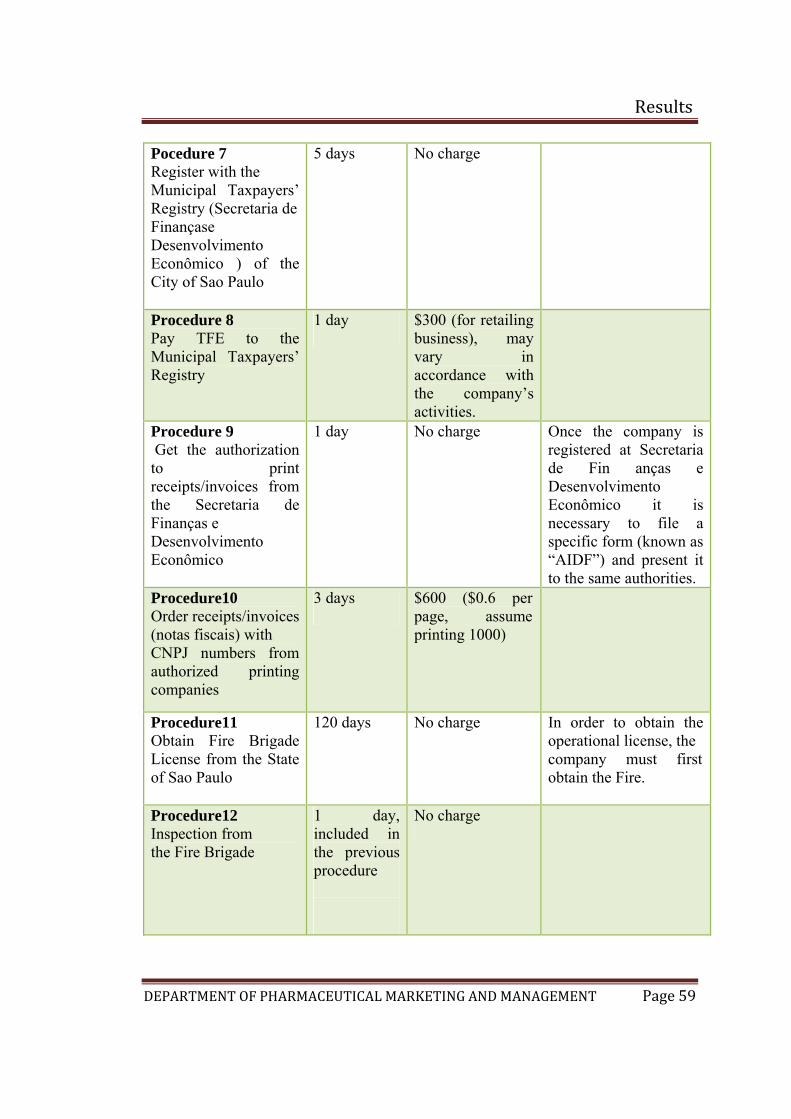
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 59
Pocedure 7 Register with the Municipal Taxpayers’ Registry (Secretaria de Finançase Desenvolvimento Econômico ) of the City of Sao Paulo
5 days No charge
Procedure 8 Pay TFE to the Municipal Taxpayers’ Registry
1 day $300 (for retailing business), may vary in accordance with the company’s activities.
Procedure 9 Get the authorization to print receipts/invoices from the Secretaria de Finanças e Desenvolvimento Econômico
1 day No charge Once the company is registered at Secretaria de Fin anças e Desenvolvimento Econômico it is necessary to file a specific form (known as “AIDF”) and present it to the same authorities.
Procedure10 Order receipts/invoices (notas fiscais) with CNPJ numbers from authorized printing companies
3 days $600 ($0.6 per page, assume printing 1000)
Procedure11 Obtain Fire Brigade License from the State of Sao Paulo
120 days No charge In order to obtain the operational license, the company must first obtain the Fire.
Procedure12 Inspection from the Fire Brigade
1 day, included in the previous procedure
No charge
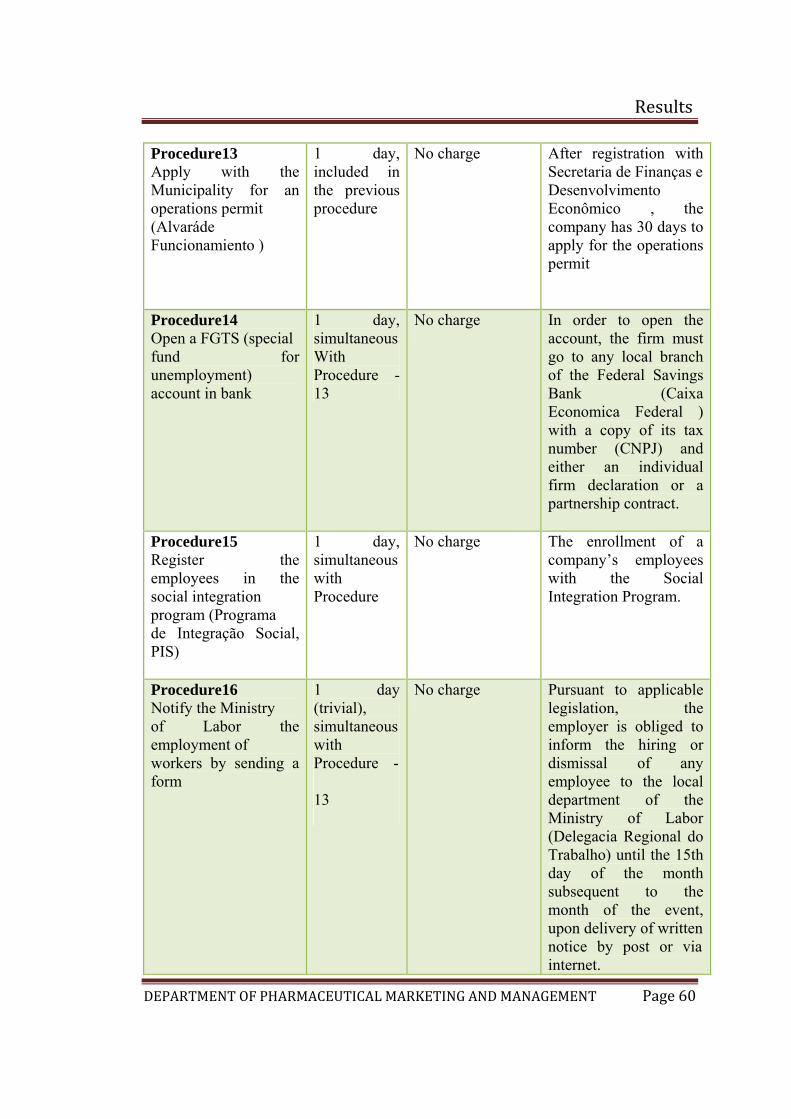
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 60
Procedure13 Apply with the Municipality for an operations permit (Alvaráde Funcionamiento )
1 day, included in the previous procedure
No charge After registration with Secretaria de Finanças e Desenvolvimento Econômico , the company has 30 days to apply for the operations permit
Procedure14 Open a FGTS (special fund for unemployment) account in bank
1 day, simultaneous With Procedure - 13
No charge In order to open the account, the firm must go to any local branch of the Federal Savings Bank (Caixa Economica Federal ) with a copy of its tax number (CNPJ) and either an individual firm declaration or a partnership contract.
Procedure15 Register the employees in the social integration program (Programa de Integração Social, PIS)
1 day, simultaneous with Procedure
No charge The enrollment of a company’s employees with the Social Integration Program.
Procedure16 Notify the Ministry of Labor the employment of workers by sending a form
1 day (trivial), simultaneous with Procedure -
13
No charge Pursuant to applicable legislation, the employer is obliged to inform the hiring or dismissal of any employee to the local department of the Ministry of Labor (Delegacia Regional do Trabalho) until the 15th day of the month subsequent to the month of the event, upon delivery of writtennotice by post or via internet.
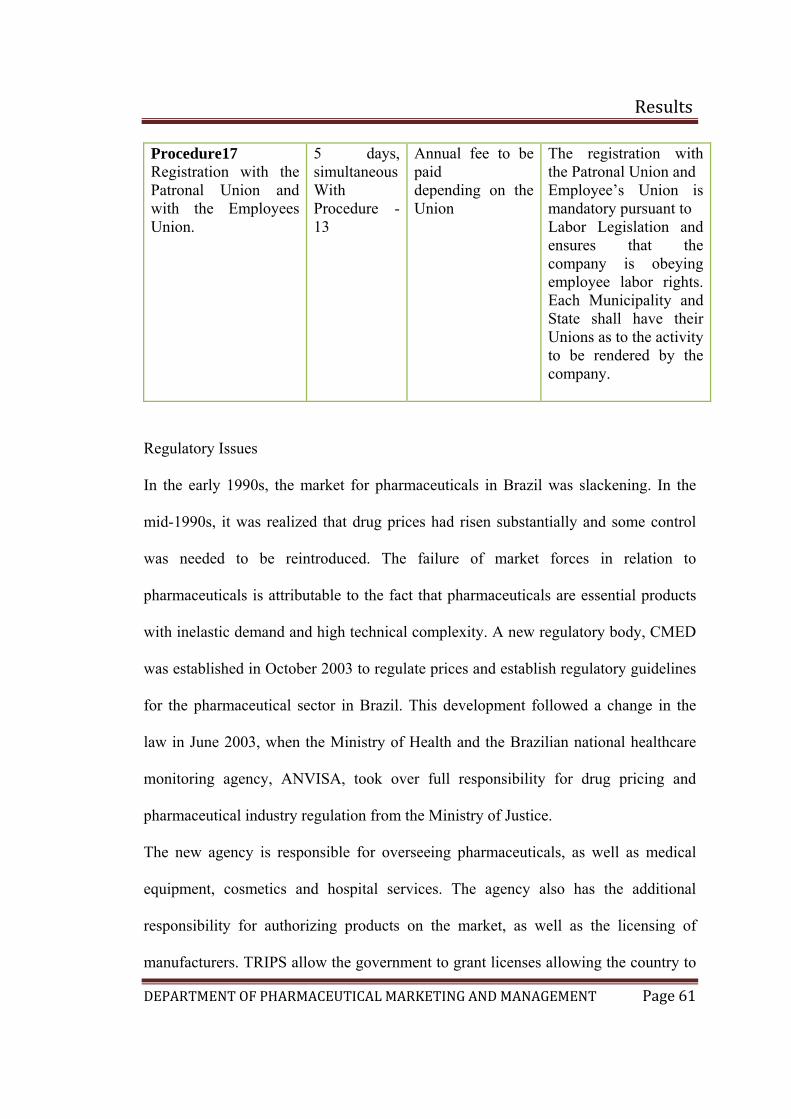
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 61
Procedure17 Registration with the Patronal Union and with the Employees Union.
5 days, simultaneous With Procedure - 13
Annual fee to be paid depending on the Union
The registration with the Patronal Union and Employee’s Union is mandatory pursuant to Labor Legislation and ensures that the company is obeying employee labor rights. Each Municipality and State shall have their Unions as to the activity to be rendered by the company.
Regulatory Issues
In the early 1990s, the market for pharmaceuticals in Brazil was slackening. In the
mid-1990s, it was realized that drug prices had risen substantially and some control
was needed to be reintroduced. The failure of market forces in relation to
pharmaceuticals is attributable to the fact that pharmaceuticals are essential products
with inelastic demand and high technical complexity. A new regulatory body, CMED
was established in October 2003 to regulate prices and establish regulatory guidelines
for the pharmaceutical sector in Brazil. This development followed a change in the
law in June 2003, when the Ministry of Health and the Brazilian national healthcare
monitoring agency, ANVISA, took over full responsibility for drug pricing and
pharmaceutical industry regulation from the Ministry of Justice.
The new agency is responsible for overseeing pharmaceuticals, as well as medical
equipment, cosmetics and hospital services. The agency also has the additional
responsibility for authorizing products on the market, as well as the licensing of
manufacturers. TRIPS allow the government to grant licenses allowing the country to
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 62
manufacture generic versions of patented drugs. Brazil's intellectual property law
allows the government to break patents in a health emergency or if it decides prices
are exorbitant.
In recent years, Brazil has repeatedly obtained price reductions from big
pharmaceutical companies by threatening to break patents on the drugs.
Regulatory and approval processes to enter the Brazilian Market
Imported products controlled by ANVISA – the National Sanitary Vigilance Agency,
including pharmaceuticals, vitamins and medical devices products, can be sold only
if:
A) The foreign company establishes a local Brazilian manufacturing unit or local
office, fully responsible for its products; or
B) The foreign company appoints a Brazilian distributor, who has the registration
with the ANVISA as an importer and distributor of the types of products being
offered.
The first step a foreign company must take is to decide whether it is going to
commercialize its products, through the Brazilian distributor or through its own
structure in Brazil. With either option, the distributor has to be duly registered at
ANVISA and authorized to operate by the sanitary agencies both municipal and
federal jurisdiction.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 63
India: (22)(23)(24)(25)
Industrial growth numbers for the months of May, June and July 2009 indicate that
the Indian industry is coming out of the distressed state. The upswing in the industrial
growth came as a result of upswing in the production of the manufacturing sector that
accounts for 80% of industrial output. Along with the manufacturing sector, mining
and electricity sectors were also seen to register high rates of growth. The average
growth numbers of the overall industry calculated for first four months of 09-10 was
4.6%. This was marginally lower the average growth posted in the corresponding
period of 2008-09. The improvement in industrial growth numbers came as a result of
measures taken by the government and Reserve Bank of India (RBI) to support
overall economic activity.
Latest figures show that FDI inflows in India for July 09 totaled US$ 3.4 billion.
Portfolio investments during the same month totaled US$ 2077 million. With the
Indian economy on the recovery path, it is expected that with time both portfolio
investments and foreign direct investments would go up further.
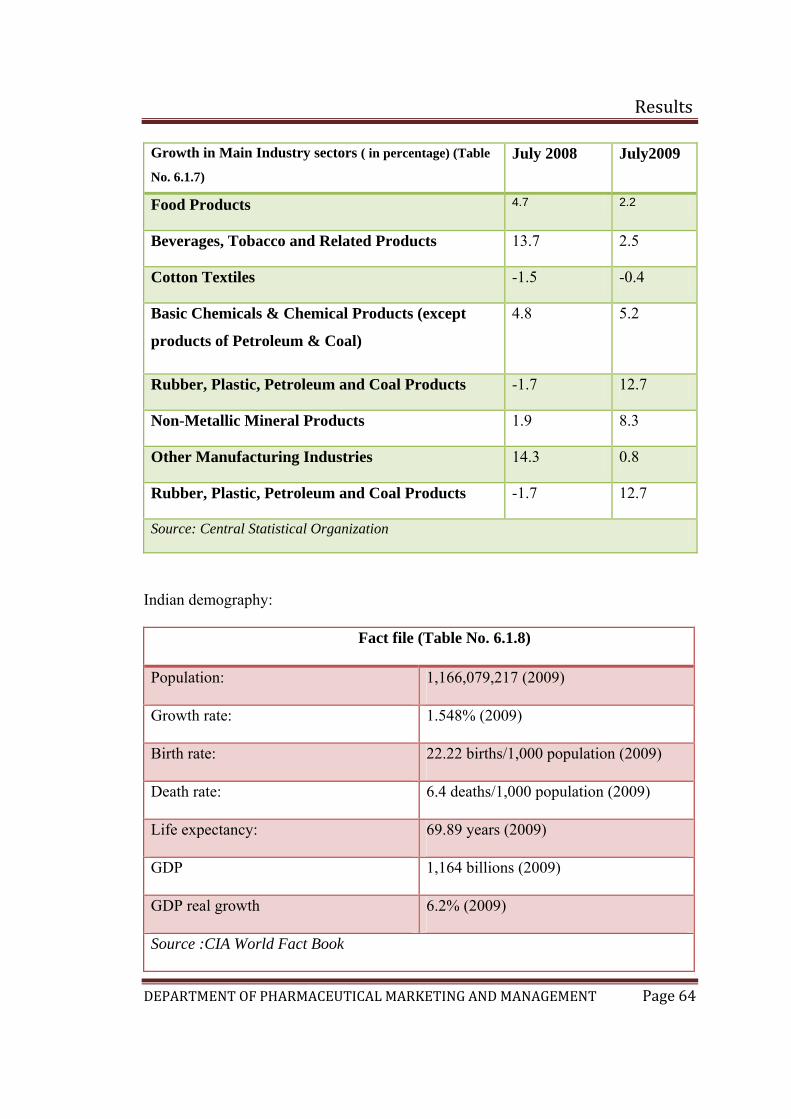
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 64
Growth in Main Industry sectors ( in percentage) (Table
No. 6.1.7) July 2008 July2009
Food Products 4.7 2.2
Beverages, Tobacco and Related Products 13.7 2.5
Cotton Textiles -1.5 -0.4
Basic Chemicals & Chemical Products (except
products of Petroleum & Coal)
4.8 5.2
Rubber, Plastic, Petroleum and Coal Products -1.7 12.7
Non-Metallic Mineral Products 1.9 8.3
Other Manufacturing Industries 14.3 0.8
Rubber, Plastic, Petroleum and Coal Products -1.7 12.7
Source: Central Statistical Organization
Indian demography:
Fact file (Table No. 6.1.8)
Population: 1,166,079,217 (2009)
Growth rate: 1.548% (2009)
Birth rate: 22.22 births/1,000 population (2009)
Death rate: 6.4 deaths/1,000 population (2009)
Life expectancy: 69.89 years (2009)
GDP 1,164 billions (2009)
GDP real growth 6.2% (2009)
Source :CIA World Fact Book
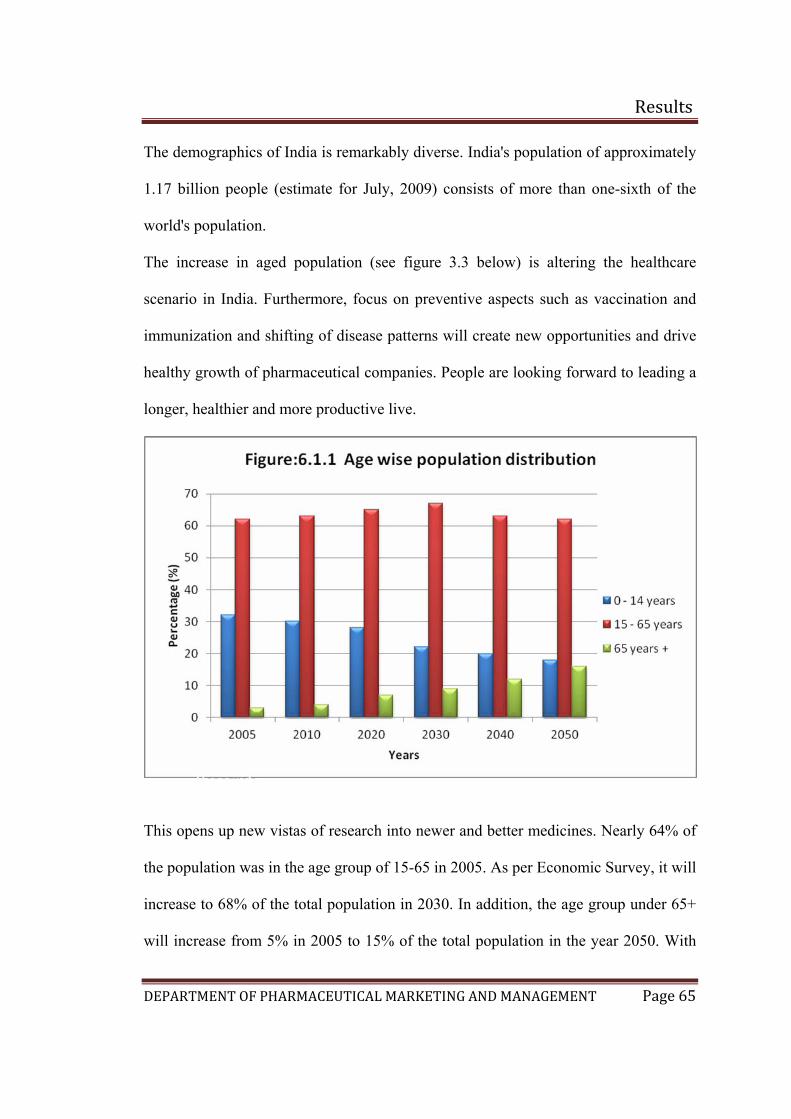
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 65
The demographics of India is remarkably diverse. India's population of approximately
1.17 billion people (estimate for July, 2009) consists of more than one-sixth of the
world's population.
The increase in aged population (see figure 3.3 below) is altering the healthcare
scenario in India. Furthermore, focus on preventive aspects such as vaccination and
immunization and shifting of disease patterns will create new opportunities and drive
healthy growth of pharmaceutical companies. People are looking forward to leading a
longer, healthier and more productive live.
This opens up new vistas of research into newer and better medicines. Nearly 64% of
the population was in the age group of 15-65 in 2005. As per Economic Survey, it will
increase to 68% of the total population in 2030. In addition, the age group under 65+
will increase from 5% in 2005 to 15% of the total population in the year 2050. With
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 66
improvement in healthcare in terms of increase in life expectancy and decrease in
infant mortality, India has certainly made progress. Life expectancy during 1996-2008
increased from 60.6 to 69.2 years and has been the major contributor to the
pharmaceutical industry growth.
Lifestyle Drugs
The changing disease profile calls for more advanced and innovative therapies.
Lifestyle drugs have become the leading segment for the Indian pharmaceutical
industry. Fast-growing lifestyle segments such as Anti-diabetic segment, Cardio
Vascular segment and Central Nervous System are driving the demand for multi-
specialty and super-specialty healthcare services. Heart disease and diabetes are
growing at 10.7% and CNS is growing at 4.9%. Antiinfective (17.7%) was a major
contributor to the domestic sales in 2007-08. It was followed by gastro-intestinal at
11%. Diabetes is recognised as a major lifestyle disease in the India, with the country
having possibly the largest number of diabetics in the world. Ageing population,
sedentary lifestyles, high stress levels, improper sleep and deteriorating eating habits
are the factors contributing to India’s dubious distinction as the world's diabetic
capital.
The Indian pharmaceutical industry is among the front ranks of the country’s science
based industries with wide ranging capabilities in the complex field of drug
manufacture and technology. In 2006-2007, the Indian pharma market has grown to
US$ 8.16 billion and reached US$ 9.77 billion in 2007-2008.(see figure 6.1.2)
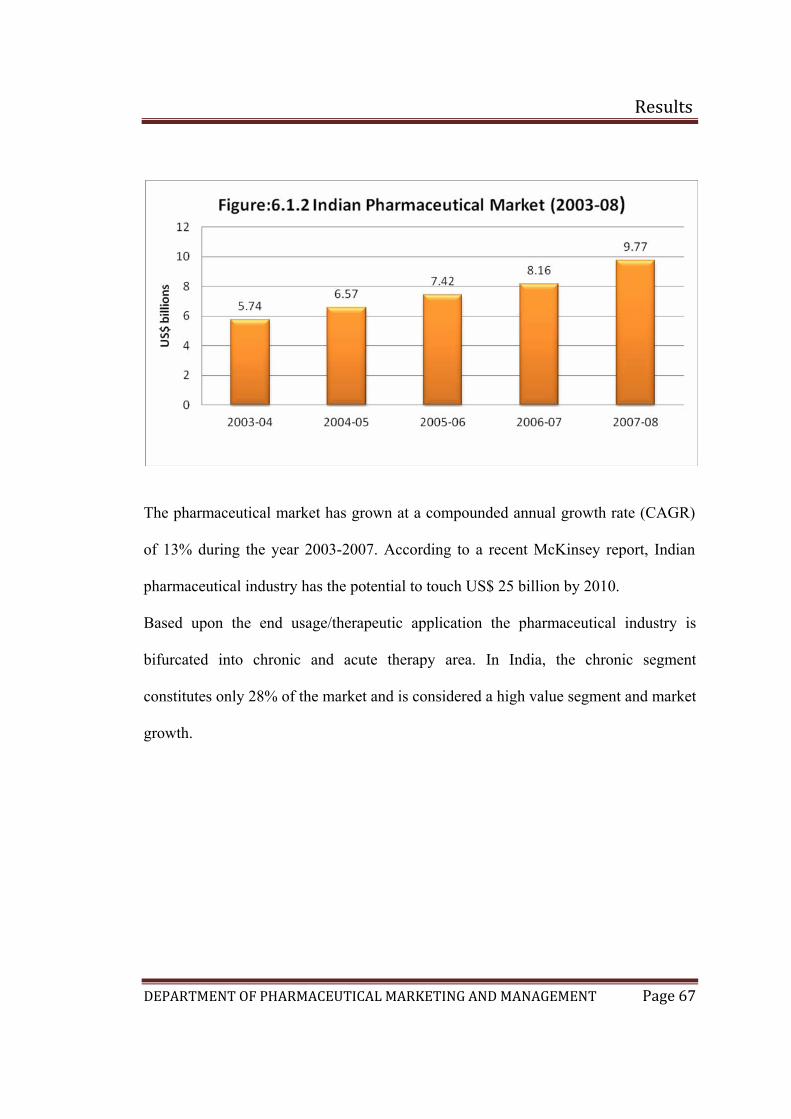
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 67
The pharmaceutical market has grown at a compounded annual growth rate (CAGR)
of 13% during the year 2003-2007. According to a recent McKinsey report, Indian
pharmaceutical industry has the potential to touch US$ 25 billion by 2010.
Based upon the end usage/therapeutic application the pharmaceutical industry is
bifurcated into chronic and acute therapy area. In India, the chronic segment
constitutes only 28% of the market and is considered a high value segment and market
growth.
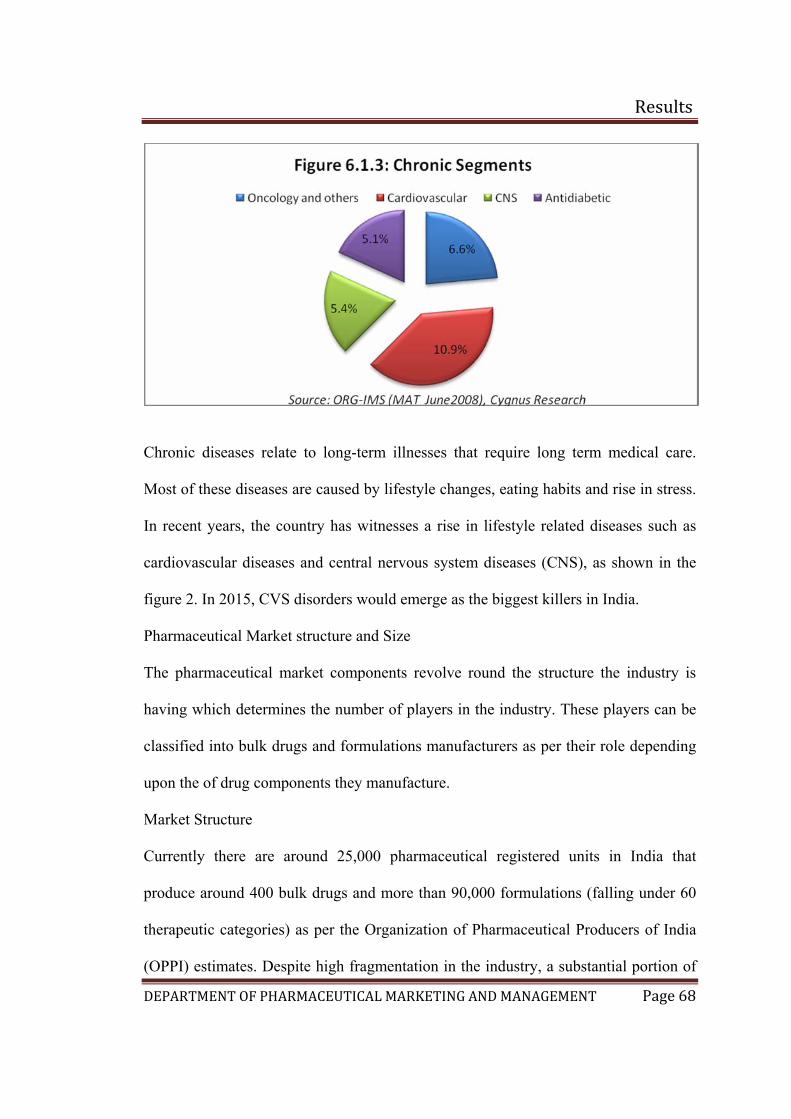
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 68
Chronic diseases relate to long-term illnesses that require long term medical care.
Most of these diseases are caused by lifestyle changes, eating habits and rise in stress.
In recent years, the country has witnesses a rise in lifestyle related diseases such as
cardiovascular diseases and central nervous system diseases (CNS), as shown in the
figure 2. In 2015, CVS disorders would emerge as the biggest killers in India.
Pharmaceutical Market structure and Size
The pharmaceutical market components revolve round the structure the industry is
having which determines the number of players in the industry. These players can be
classified into bulk drugs and formulations manufacturers as per their role depending
upon the of drug components they manufacture.
Market Structure
Currently there are around 25,000 pharmaceutical registered units in India that
produce around 400 bulk drugs and more than 90,000 formulations (falling under 60
therapeutic categories) as per the Organization of Pharmaceutical Producers of India
(OPPI) estimates. Despite high fragmentation in the industry, a substantial portion of
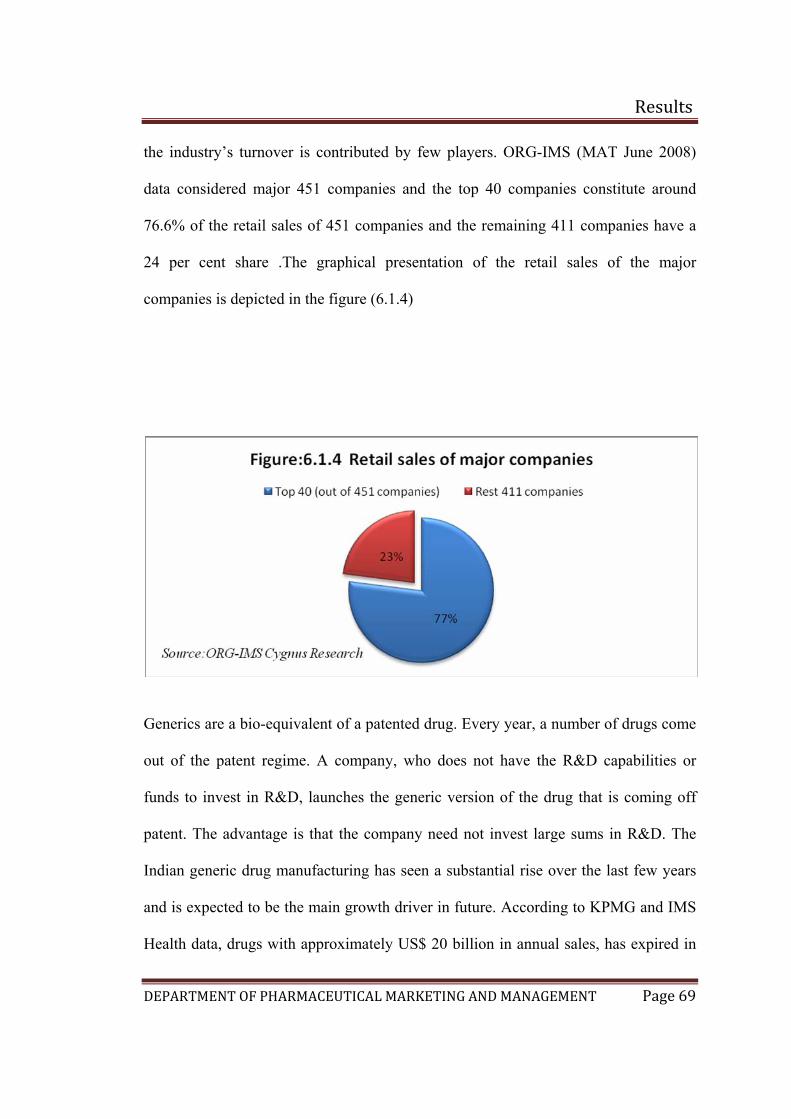
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 69
the industry’s turnover is contributed by few players. ORG-IMS (MAT June 2008)
data considered major 451 companies and the top 40 companies constitute around
76.6% of the retail sales of 451 companies and the remaining 411 companies have a
24 per cent share .The graphical presentation of the retail sales of the major
companies is depicted in the figure (6.1.4)
Generics are a bio-equivalent of a patented drug. Every year, a number of drugs come
out of the patent regime. A company, who does not have the R&D capabilities or
funds to invest in R&D, launches the generic version of the drug that is coming off
patent. The advantage is that the company need not invest large sums in R&D. The
Indian generic drug manufacturing has seen a substantial rise over the last few years
and is expected to be the main growth driver in future. According to KPMG and IMS
Health data, drugs with approximately US$ 20 billion in annual sales, has expired in
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 70
2008. This market will be converted into generics market, which will provide an
opportunity of US$ 2-3 billion. Buying generic drugs is the only option for most of
the companies in India as the drug pipeline is very lean at present. Moreover, the
USFDA is getting more stringent in granting product approvals. India is capturing a
large portion of generic drugs by influencing its inherent strengths in technology,
R&D facilities and trained human capital.
Major growth drivers:
CRAMS
Contract Research and Manufacturing services (CRAMS) is the most talked about in
the Pharmaceutical industry in India as it turns out to be the biggest opportunity for
Indian Industry. The pressure on big Pharmaceutical companies to evolve a cost-
cautious operations model has resulted in the need to outsource.
Pressure to cut prices Pharmaceutical expenditure is only 7- 9% of total healthcare
cost. Inspite of this, very often the blame for rising healthcare costs is fixed on
pharma industry all over the world. The Pharmaceutical Industry is perceived to be
making high profits, ruthless in their approach & manipulative, with no regard for
patients and their problems. There is on going pressure on the Industry to cut prices.
Outsourcing production to low costs regions offers a way to lower prices without
cutting the margins.
Contract Manufacturing
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 71
Majority of the global companies have started outsourcing the manufacture of
intermediates, APIs & generic drugs to countries like India and China. India has easy
availability of trained manpower. Manpower costs in India are 70% lower than USA.
Setting up FDA approved plant is 30% cheaper here. All these factors make the cost
of manufacture lower than the goods manufactured in the USA and Europe. Quality of
Indian Pharma. products is strictly regulated & accepted all over the globe.
Middle Class, Rural Market to Fuel Pharma Growth
According to the Confederation of Indian Industry (CII), the Indian pharma industry
is expected to touch the growth rate of 19% in 2015 from the growth rate of 13% in
2007. The incremental growth of 6.6% will be mainly supported by two factors:
middle class (2%) and untapped rural markets (2%). At present, the middle class
population, defined as households with an annual income in the range of Rs. 200,000-
Rs. 10,00,000, is estimated to be around 91 million in the country. The middle class
consists of around 8% of total population and is expected to grow four-fold by 2015
to reach 364 million. This will generate an additional demand for the existing and new
medical products.
Most of the rural markets in India, which were not feasible even a few years back,
have now become easily accessible for the companies. Hence, pharmaceutical
companies are thinking beyond larger cities and plugging into rural sectors, purely to
ramp up volumes. Although urban markets are still more lucrative and will continue
to be the focus for the industry, the untapped potential of Indian rural markets is now
seen as the next volume driver. With rising rural incomes and a strong distribution
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 72
network, India's rural pharma market is also experiencing strong growth. Small towns
contribute 20% to the country's pharma market, whereas rural areas account for 21%.
Exports:
Before the patent regime, most Indian companies focused on exports. Exports
improved the valuation of companies owing to higher margin in overseas markets.
Indian companies built fortunes by making cheaper versions of blockbuster drugs and
selling them in domestic and export markets. They built strong position in
manufacture of bulk drugs. Out of the total phrama exports, formulations constitute
55% and the bulk drugs constitute 45%. Success in export market allowed some
Indian companies to build a strong position in the domestic market organically and
through acquisitions of brands and companies.
In the post-patents regime, exports will continue to be a priority for Indian companies.
Major blockbuster drugs will come off patent in the near future, creating a big generic
opportunity for Indian companies. Generic market is growing at a faster rate (20%)
than the pharma market. A growing demand for anti-AIDS drugs in Africa will keep
Indian companies busy.
Exports will provide Indian companies with the strength to withstand the onslaught of
multinationals in the domestic markets and is critical for bulk drug manufacturers. But
the costs of regulatory compliance will increase in domestic and export markets.
In the Indian pharmaceutical industry, drugs worth approximately US$ 20 billion in
annual sales has expired in 2008. Hence, this market will convert into generic market,
providing an opportunity of US$ 2-3 billion. With drug pipeline drying up and
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 73
USFDA getting more stringent in granting product approvals, buying generic is only
option for most of the companies.
The US patent's expirations of branded products will substantially contribute to the
growth of Indian pharmaceutical industry, thereby pushing a great deal of its exports,
particularly in generic drugs markets. This is because low production costs give India
an edge over other countries. This will also provide adequate opportunities for the
Indian generic drug manufactures to capture the largest market share. The major part
of the Indian pharmaceutical industry is supported by exports. Hence, exports are a
must for the domestic market. Indian companies can initiate exports by forming
subsidiaries and joint ventures. It will generate more revenues for the industry.
Epidemiology study of hypertension: (17)
Cardiovascular diseases have emerged as an important health problem in India. High
blood pressure (BP) is a major risk factor and better control can lead to prevention of
300,000 of the 1.5 million annual deaths from cardiovascular diseases in India.
Epidemiological studies demonstrate that prevalence of hypertension is increasing
rapidly among Indian urban populations and using the current definitions more than
two-fifths of the Indian urban adult population has hypertension. The prevalence is
lower in rural populations, but is increasing. Jaipur Heart Watch (JHW) is an ongoing
cross-sectional epidemiological study in western India. Successive studies have been
performed in rural (JHW-R, 1992–93) and urban locations (JHW-1, 1993–94; JHW-2,
1999–2000; JHW-3, 2002–03, and JHW-4, 2004–05). The studies evaluated adults
≥20 years using standardized methodology and in the present analyses subjects aged
20–59 years from these JHW studies [4102 men (1700, 1294, 469, 179 and 413) and
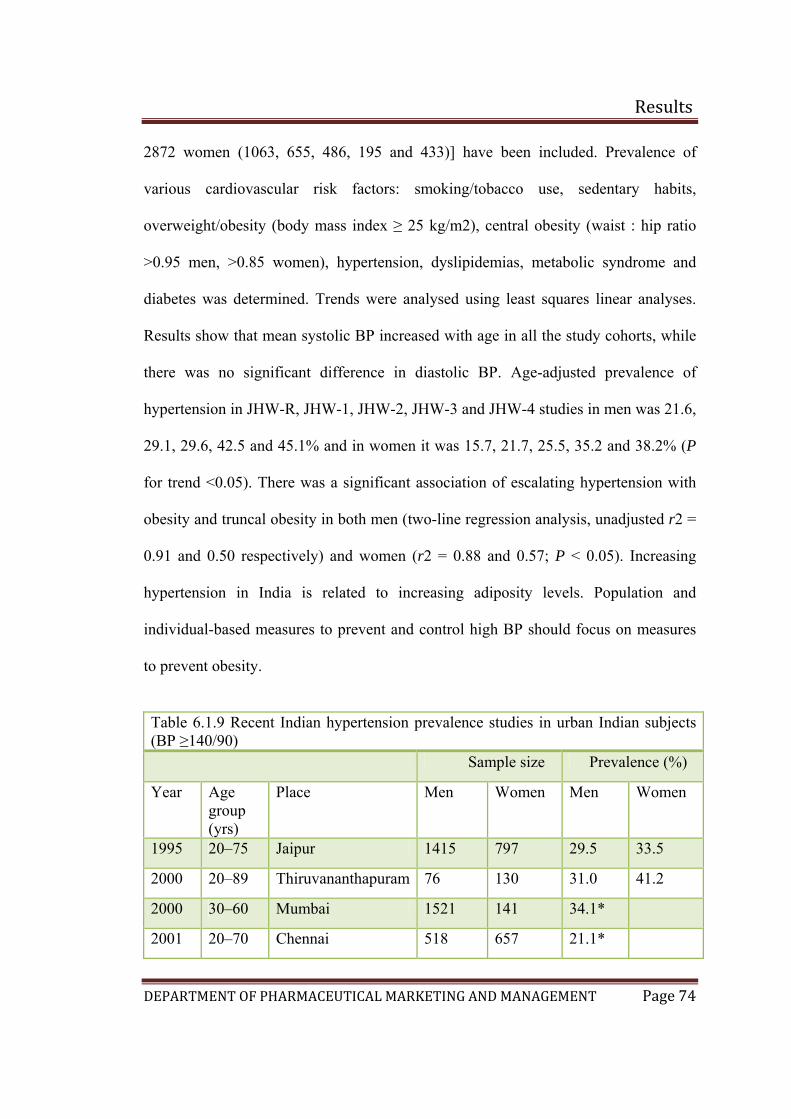
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 74
2872 women (1063, 655, 486, 195 and 433)] have been included. Prevalence of
various cardiovascular risk factors: smoking/tobacco use, sedentary habits,
overweight/obesity (body mass index ≥ 25 kg/m2), central obesity (waist : hip ratio
>0.95 men, >0.85 women), hypertension, dyslipidemias, metabolic syndrome and
diabetes was determined. Trends were analysed using least squares linear analyses.
Results show that mean systolic BP increased with age in all the study cohorts, while
there was no significant difference in diastolic BP. Age-adjusted prevalence of
hypertension in JHW-R, JHW-1, JHW-2, JHW-3 and JHW-4 studies in men was 21.6,
29.1, 29.6, 42.5 and 45.1% and in women it was 15.7, 21.7, 25.5, 35.2 and 38.2% (P
for trend <0.05). There was a significant association of escalating hypertension with
obesity and truncal obesity in both men (two-line regression analysis, unadjusted r2 =
0.91 and 0.50 respectively) and women (r2 = 0.88 and 0.57; P < 0.05). Increasing
hypertension in India is related to increasing adiposity levels. Population and
individual-based measures to prevent and control high BP should focus on measures
to prevent obesity.
Table 6.1.9 Recent Indian hypertension prevalence studies in urban Indian subjects (BP ≥140/90) Sample size Prevalence (%)
Year Age group (yrs)
Place Men Women Men Women
1995 20–75 Jaipur 1415 797 29.5 33.5
2000 20–89 Thiruvananthapuram 76 130 31.0 41.2
2000 30–60 Mumbai 1521 141 34.1*
2001 20–70 Chennai 518 657 21.1*
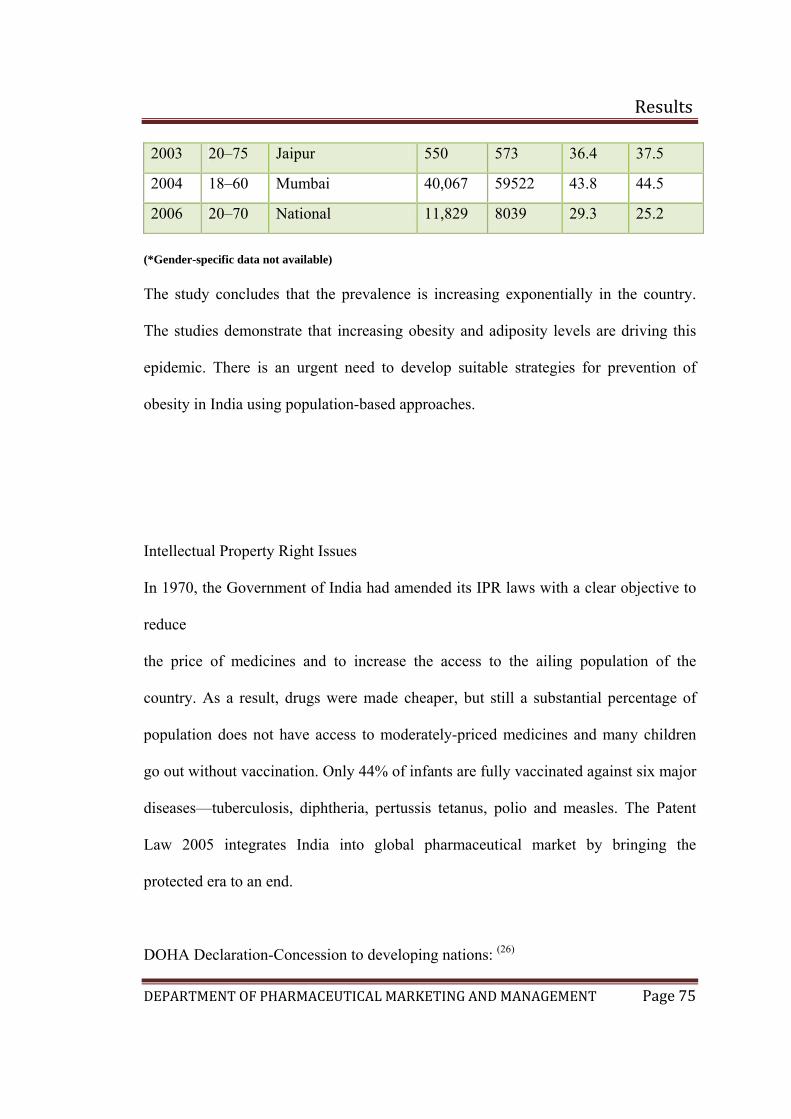
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 75
2003 20–75 Jaipur 550 573 36.4 37.5
2004 18–60 Mumbai 40,067 59522 43.8 44.5
2006 20–70 National 11,829 8039 29.3 25.2
(*Gender-specific data not available) The study concludes that the prevalence is increasing exponentially in the country.
The studies demonstrate that increasing obesity and adiposity levels are driving this
epidemic. There is an urgent need to develop suitable strategies for prevention of
obesity in India using population-based approaches.
Intellectual Property Right Issues
In 1970, the Government of India had amended its IPR laws with a clear objective to
reduce
the price of medicines and to increase the access to the ailing population of the
country. As a result, drugs were made cheaper, but still a substantial percentage of
population does not have access to moderately-priced medicines and many children
go out without vaccination. Only 44% of infants are fully vaccinated against six major
diseases—tuberculosis, diphtheria, pertussis tetanus, polio and measles. The Patent
Law 2005 integrates India into global pharmaceutical market by bringing the
protected era to an end.
DOHA Declaration-Concession to developing nations: (26)
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 76
The first significant achievement of the World Trade Organization's Doha ministerial
Conference came on the morning of 13 November 2000 when a compromise on the
'declaration on the TRIPS Agreement and Public Health' was reached. It was as a
result of staunch effort by India Brazil and about 55 other African nations. This is one
of the areas where there is an assurance that the restrictive clause under the TRIPS
agreement on drug patents will not over ride public health concerns. It is a positive
development that in TRIPS, a public health crisis has been included as an exception
for granting compulsory license (CL).
In the new Doha Declaration is that it recognizes the fact which was implicit under
Articles 7 and 8 of TRIPS, that considerations of Public Good which includes public
health could be the over riding factor while offering IPR protection for medicines for
specified diseases and 'epidemics' , particularly for DCs and LDCs . The one hundred
and forty two countries who came together at the 4th WTO Ministerial Conference at
Doha clearly affirmed that governments are free to take all necessary measures to
protect public health. The declaration gave primacy to public health over intellectual
property rights.
It is viewed that this declaration on public health is trophy for India since WTO had
accepted, unequivocally, that patents will not stand in way of Public health . This is a
very important aspect for India because, now national governments can decide if a
particular situation or crisis is an emergency and that whether it would warrant
sidelining of patents. How far this declaration would help India would be seen in
future.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 77
It is inevitable that the industry now has to face these challenges and the opportunities
that the new regime would throw open. To overcome the resource crunch the industry
may have to consider many options like mergers with other pharma firms,
collaborations with foreign companies, joining an R&D consortia etc. The industry
would learn to change its axis of expertise from re-engineering to innovation.
Aggressive marketing, good branding, better products, R&D and a patent protection
would be their tools of success. The past has shown that India appears to have the
technological and the commercial capability to adopt to more competitive
environment. It has often caught up with world technological frontiers in other
sectors. It can continue to do so again in future, if the industry wants to be an
important pharmaceutical development center on world map.
6.2 Risk analysis (1)(4)(28)(29)
If a company is to survive in the international marketplace, it is important that it searches for
methods to reduce, as far as possible, the risk of making wrong decision. Lack of knowledge
of foreign markets is one of the major barriers an international marketing manager has to
overcome.
Before making a decision to go abroad, the company must weigh several risks, such as
• the company might not understand foreign customer preferences,
• they might not understand the foreign country’s business culture or know how to deal
effectively with foreign nationals,
• the company might underestimate foreign regulations and incur unexpected costs,
• the company might realize that it lacks managers with international experience,
• the foreign country might change its commercial laws, devalue its currency or
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 78
undergo a political revolution and expropriate foreign property.
Because of the conflicting advantages and risks, companies often do not act until
some event thrusts them into the international arena. In the markets where
opportunities have been identified, researchers need to make an assessment first as to
the type of risk.
Over recent years marketers have developed various indices to help assess the risk
factors in the evaluation of potential market opportunities. The four major categories
of risks identified are namely:
a) Macro-environmental risks arises from cataclysmic events such as wars, as
well as unstable political or economic conditions over which the firm has no
control.
b) Political risks arise from decisions by governments, such as tariffs, product
regulation, and restrictions on foreign investment which the firm can control
or influence to some extent
c) Competitive risks arise from the actions of competitors in domestic and
international markets, such entering a market, launching new products,
attacking or defending a position.
d) Operational risks are those associated with actions taken by the firm in
international markets, such as such as introducing products or services into
countries where there is no established market or they appear to run counter to
existing behavioral life-style patterns.
For any business, risks stemming from poor governance, political violence and an
unstable regulatory environment can significantly affect performance and reputation.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 79
For responsible business, considerations including a country’s human rights record,
such as the performance of its security forces or child labour, are also key to avoiding
accusations of complicity and maintaining brand equity. Managing risks well not only
improves profitability, but also enhances a company’s social license to operate, as
well as attractiveness to customers, clients, investors and other stakeholders.
Maplecroft’s Political Risk Report 2009 offers a distinct approach by dividing
political risk into two groupings. The first, dynamic risks, assesses ‘traditional’
political risk, such as regime stability, the rule of law, terrorism, expropriation and the
business environment. The second, structural risks, measures long-term trends and
intrinsic features of a country, such as its human rights record, its energy, food and
water security, its development status or its vulnerability to climate change.
This approach of differentiating between dynamic and structural risks more accurately
reflects new challenges in an increasingly interdependent world and supports
responsible business by:
• Examining the relationship between immediate political events and a
country’s resilience to long-term challenges
• Generating a point-specific, sub-national risk profile for terrorism, conflict
and political violence
• Forecasting potential instability and unrest
• Highlighting areas with greater supply-chain risks such as child labour and
forced labour
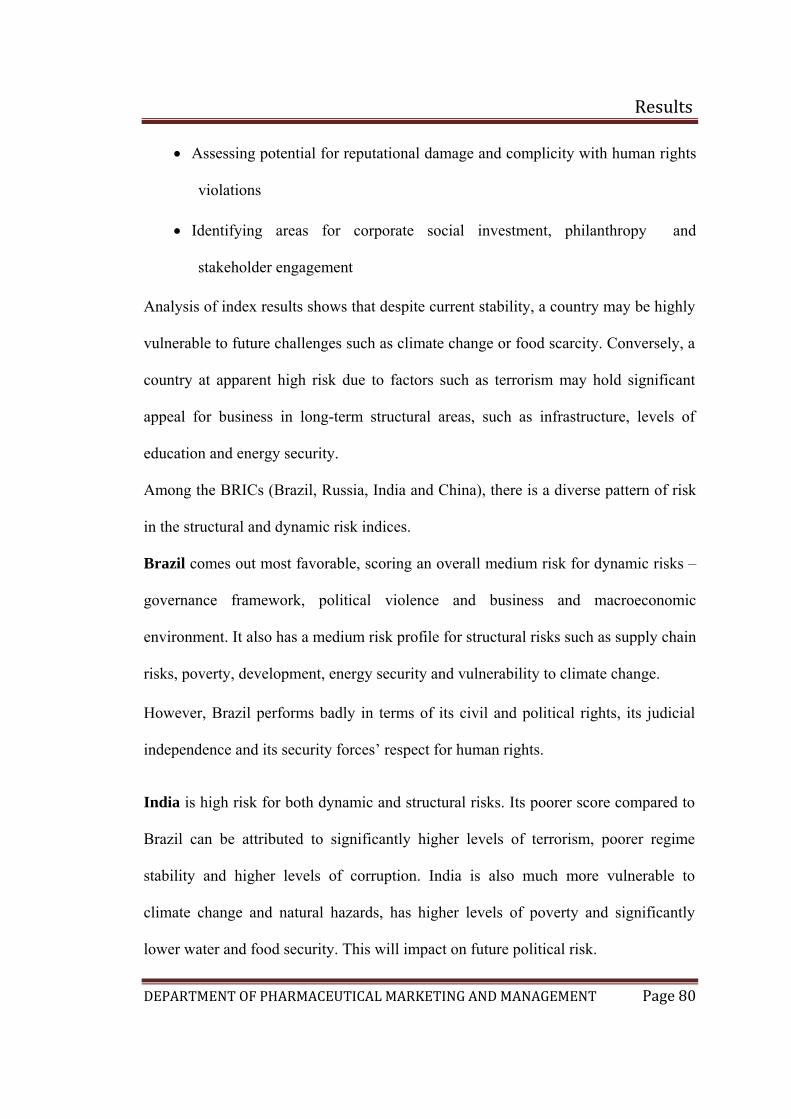
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 80
• Assessing potential for reputational damage and complicity with human rights
violations
• Identifying areas for corporate social investment, philanthropy and
stakeholder engagement
Analysis of index results shows that despite current stability, a country may be highly
vulnerable to future challenges such as climate change or food scarcity. Conversely, a
country at apparent high risk due to factors such as terrorism may hold significant
appeal for business in long-term structural areas, such as infrastructure, levels of
education and energy security.
Among the BRICs (Brazil, Russia, India and China), there is a diverse pattern of risk
in the structural and dynamic risk indices.
Brazil comes out most favorable, scoring an overall medium risk for dynamic risks –
governance framework, political violence and business and macroeconomic
environment. It also has a medium risk profile for structural risks such as supply chain
risks, poverty, development, energy security and vulnerability to climate change.
However, Brazil performs badly in terms of its civil and political rights, its judicial
independence and its security forces’ respect for human rights.
India is high risk for both dynamic and structural risks. Its poorer score compared to
Brazil can be attributed to significantly higher levels of terrorism, poorer regime
stability and higher levels of corruption. India is also much more vulnerable to
climate change and natural hazards, has higher levels of poverty and significantly
lower water and food security. This will impact on future political risk.
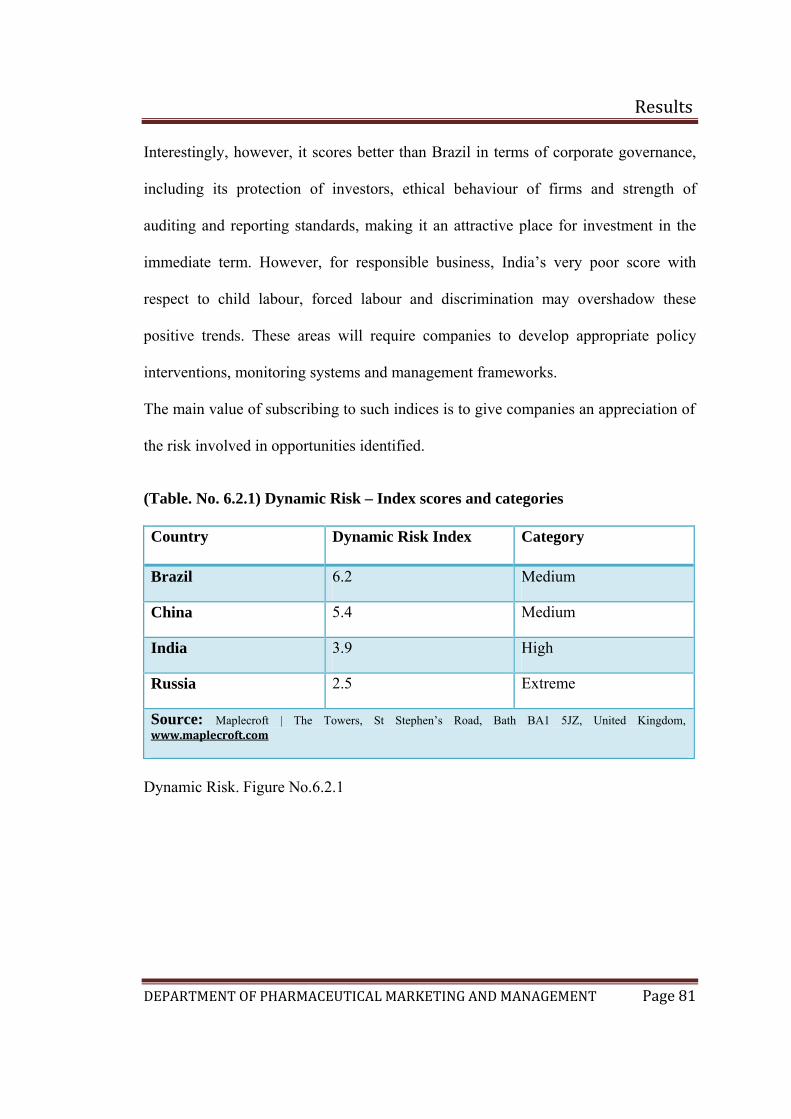
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 81
Interestingly, however, it scores better than Brazil in terms of corporate governance,
including its protection of investors, ethical behaviour of firms and strength of
auditing and reporting standards, making it an attractive place for investment in the
immediate term. However, for responsible business, India’s very poor score with
respect to child labour, forced labour and discrimination may overshadow these
positive trends. These areas will require companies to develop appropriate policy
interventions, monitoring systems and management frameworks.
The main value of subscribing to such indices is to give companies an appreciation of
the risk involved in opportunities identified.
(Table. No. 6.2.1) Dynamic Risk – Index scores and categories
Country Dynamic Risk Index Category
Brazil 6.2 Medium
China 5.4 Medium
India 3.9 High
Russia 2.5 Extreme
Source: Maplecroft | The Towers, St Stephen’s Road, Bath BA1 5JZ, United Kingdom, www.maplecroft.com
Dynamic Risk. Figure No.6.2.1
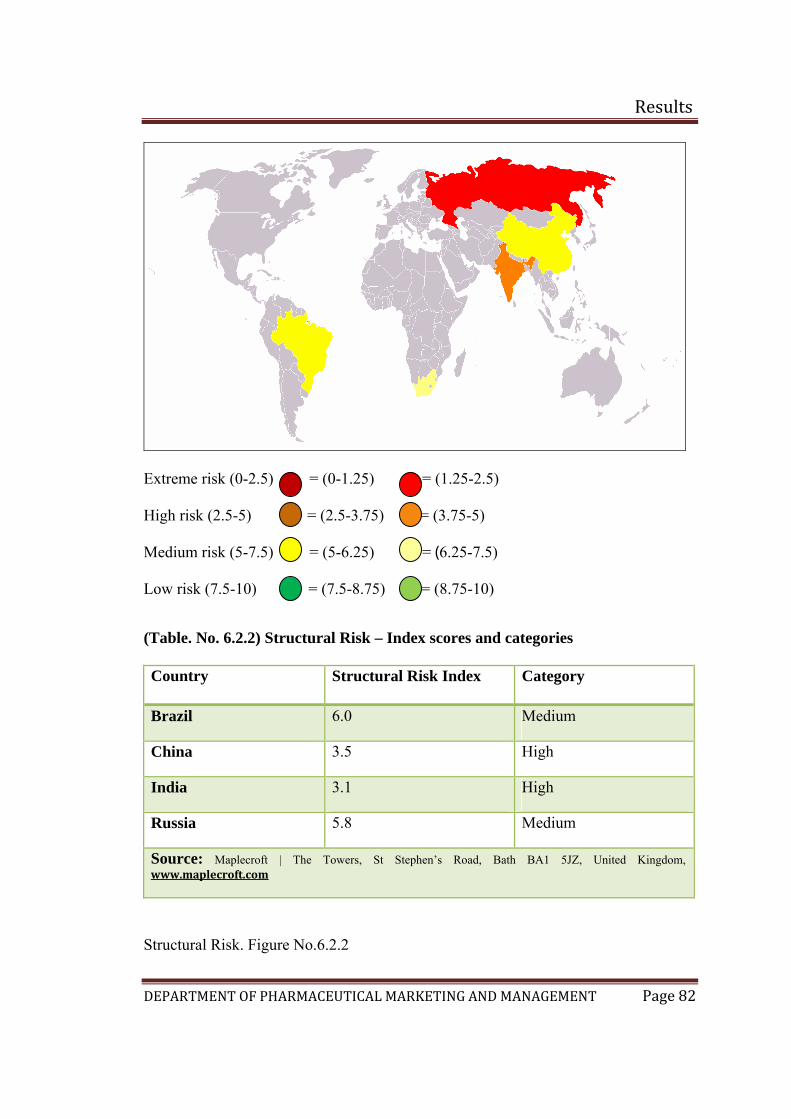
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 82
Extreme risk (0-2.5) = (0-1.25) = (1.25-2.5)
High risk (2.5-5) = (2.5-3.75) = (3.75-5)
Medium risk (5-7.5) = (5-6.25) = (6.25-7.5)
Low risk (7.5-10) = (7.5-8.75) = (8.75-10) (Table. No. 6.2.2) Structural Risk – Index scores and categories
Country Structural Risk Index Category
Brazil 6.0 Medium
China 3.5 High
India 3.1 High
Russia 5.8 Medium
Source: Maplecroft | The Towers, St Stephen’s Road, Bath BA1 5JZ, United Kingdom, www.maplecroft.com
Structural Risk. Figure No.6.2.2
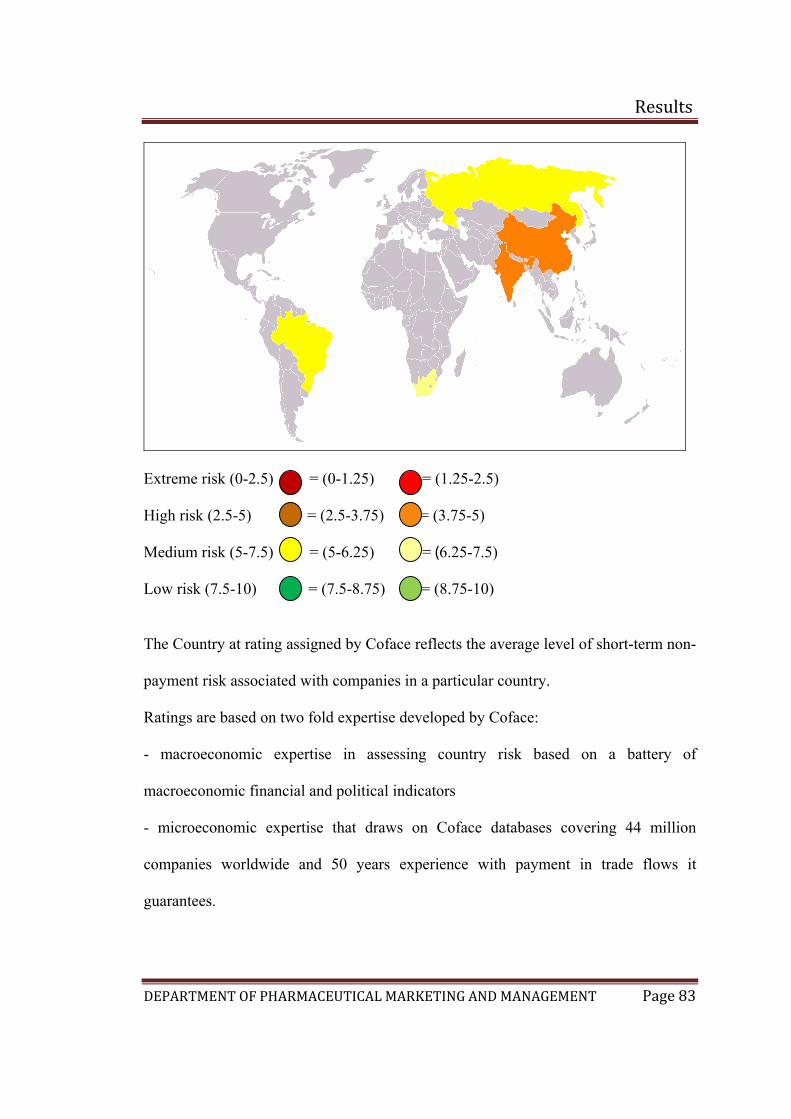
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 83
Extreme risk (0-2.5) = (0-1.25) = (1.25-2.5)
High risk (2.5-5) = (2.5-3.75) = (3.75-5)
Medium risk (5-7.5) = (5-6.25) = (6.25-7.5)
Low risk (7.5-10) = (7.5-8.75) = (8.75-10)
The Country at rating assigned by Coface reflects the average level of short-term non-
payment risk associated with companies in a particular country.
Ratings are based on two fold expertise developed by Coface:
- macroeconomic expertise in assessing country risk based on a battery of
macroeconomic financial and political indicators
- microeconomic expertise that draws on Coface databases covering 44 million
companies worldwide and 50 years experience with payment in trade flows it
guarantees.
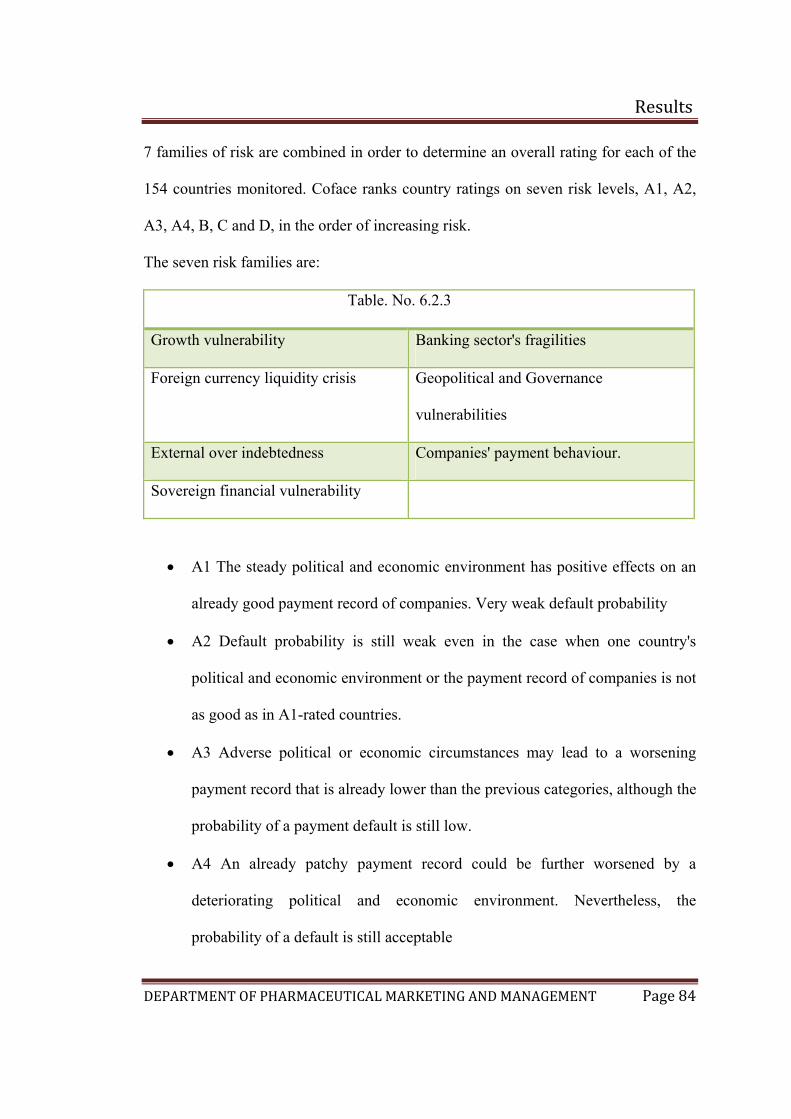
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 84
7 families of risk are combined in order to determine an overall rating for each of the
154 countries monitored. Coface ranks country ratings on seven risk levels, A1, A2,
A3, A4, B, C and D, in the order of increasing risk.
The seven risk families are:
Table. No. 6.2.3
Growth vulnerability Banking sector's fragilities
Foreign currency liquidity crisis Geopolitical and Governance
vulnerabilities
External over indebtedness Companies' payment behaviour. Sovereign financial vulnerability
• A1 The steady political and economic environment has positive effects on an
already good payment record of companies. Very weak default probability
• A2 Default probability is still weak even in the case when one country's
political and economic environment or the payment record of companies is not
as good as in A1-rated countries.
• A3 Adverse political or economic circumstances may lead to a worsening
payment record that is already lower than the previous categories, although the
probability of a payment default is still low.
• A4 An already patchy payment record could be further worsened by a
deteriorating political and economic environment. Nevertheless, the
probability of a default is still acceptable
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 85
• B An unsteady political and economic environment is likely to affect further
an already poor payment record.
• C An very unsteady political and economic environment could deteriorate an
already bad payment record.
• D The high risk profile of a country's economic and political environment will
further worsen a generally very bad payment record
The business climate rating is to assess overall business environment quality in a
country which comprises two modules ( )
1) The core of the new rating rests on the Coface experience with the quality of
information available on companies and the legal protection given to creditors.
The module was developed based on the responses by Coface entities
worldwide to a questionnaire covering:
the quality and availability of financial information (legal framework for
financial statement publication, availability, accessibility, and reliability of
corporate accounts, and so on)
creditor protection and debt collection efficiency (rating grids for summary
legal procedures, ordinary legal procedure, court costs, bankruptcy procedures,
for example)
The above ratings may be compared to other sources like the "institutional profiles"
database
maintained by the French Ministry of Finance and validated by an internal committee
to ensure homogeneous and consistent responses.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 86
2) The above ratings based on the Coface experience is supplemented by a
module on institutional framework quality. This module reflects the quality of
institutions whose strengths and weaknesses can affect companies.
The parameters considered include, for example, public service effectiveness
(government, education, health, infrastructures), regulatory quality, respect for
the law, and extent of corruption. The calculations are bases on data from
external sources notably including:
the government effectiveness indicator maintained by the World Bank
Institute based on the quality of public services provided and on civil service
efficiency
the HDI, or human development index, a composite statistical index created
by the United Nations to rank countries according to their qualitative
development based on the average of three quantitative indices reflecting
respectively health/life expectancy, knowledge or education level, and
standard of living
an infrastructure quality index (energy, transport, telecommunications)
published by the World Economic Forum in its "Global competitiveness
report"
a regulatory quality indicator (World Bank Institute) that reflects the possible
existence of policies contrary to the smooth running of a market economy (like
prices controls or poor bank oversight), and the apparent influence of local
regulations on foreign trade and the business climate.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 87
a rule of law indicator (World Bank Institute) reflecting the confidence of
economic a gents in their judicial system, legal system efficiency and
transparency.
an indicator of corruption (World Bank Institute) reflects the apparent extent
of corruption, defined as misappropriation of public property for private
purposes.
The above indicators and indices are generally based on information derived from
company surveys. • A1 The business environment is very good. Corporate financial information is
available and reliable. Debt collection is efficient. In stitutional quality is very
good. Intercompany transactions run smoothly in environments rated A1.
• A2 The business environment is good. When available, corporate financial
information is reliable. Debt collection is reasonably efficient. Institutions
generally perform efficiently. Intercompany transactions usually run smoothly
in the relatively stable environment rated A2.
• A3 The business environment is relatively good. Although not always
available, corporate financial information is usually reliable. Debt collection
and the institutional framework may have some shortcomings. Intercompany
transactions may run into occasional difficulties in the otherwise secure
environments rated A3.
• A4 The business environment is acceptable. Corporate financial information is
sometimes neither readily available nor sufficiently reliable. Debt collection is
not always efficient and the institutional framework has shortcomings.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 88
Intercompany transactions may thus run into appreciable difficulties in the
acceptable but occasionally unstable environments rated A4.
• B The business environment is mediocre. The availability and the reliability of
corporate financial information vary widely. Debt collection can sometimes be
difficult. The institutional framework has a few troublesome weaknesses.
Intercompany transactions run appreciable risks in the unstable, largely
inefficient environments rated B.
• C The business environment is difficult. Corporate financial information is
often unavailable and when available often unreliable. Debt collection is
unpredictable. The institutional framework has many troublesome weaknesses.
Intercompany transactions run major risks in the difficult environments rated
C.
• D The business environment is very difficult. Corporate financial information
is rarely available and when available usually unreliable. The legal system
makes debt collection very unpredictable. The institutional framework has
very serious weaknesses. Intercompany transactions can thus be very difficult
to manage in the highly risky environments rated D.
Brazil Country Rating: A4
A somewhat shaky political and economic outlook and a relatively volatile business
environment can affect corporate payment behaviour. Corporate default probability is
still acceptable on average.
India Country Rating : A3
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 89
Adverse political or economic circumstances may lead to a worsening payment record
that is already lower than the previous categories, although the probability of a
payment default is still low.
Brazil and India Business Climate Rating : A4 (both)
The business environment is acceptable. Corporate financial information is sometimes
neither readily available nor sufficiently reliable. Debt collection is not always
efficient and the institutional framework has shortcomings. Intercompany transactions
may thus run into appreciable difficulties in the acceptable but occasionally unstable
environments rated A4.
6.3 Cultural aspects (2)(4)(30)
Markets in countries around the world are subject to many influences. The
development of successful international marketing strategies is based on a sound
understanding of the similarities and differences that exist in the countries around the
world. The differences between social and cultural factors in different parts of the
world can be a central consideration in developing and implementing international
marketing strategies. Differences in language can alter the intended meaning of a
promotional campaign and differences in the way a culture organizes itself socially
may affect the way a product is positioned in the market.
There are few components which does matters mainly when a organization is going
global. In pharmaceutical sector the market is focused and maximum promotional
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 90
activities are targeted not for the end users, because drugs are prescribed by the
doctors and the end users has no other choice, but to buy the prescribed product. So
following are few things which are to be taken into consideration,
Education: the level of formal primary and secondary education in a foreign market
will have a direct impact upon the target customer or in business. The labeling of
products, especially which can cause fatal side effects, need to be taken seriously for a
market that has a very low literacy rate. Messages can be disseminated through
pictures or diagrams in low literacy sectors.
Law and politics: The legal and political environments in a foreign market are often
seen as consequences of the cultural traditions of that market
Aesthetics: This area covers the local culture perception of things. A firm needs to
ensure that their product and communications strategies is sympathetic and acceptable
to the local culture.
Values and attitudes: The values consumers from different countries place on things
such as time, achievement, work will effect seriously not only the products offered
but also the packaging, distribution and communication strategies.
Religion: It is a major cultural variable and has significant if not always apparent
effects on marketing strategy. No violation of religion by advertising and other
promotional practices no matter how significant, will go unnoticed or unpunished
either by the government or the consumer.
Language: It can be divided into two major elements. The spoken language is the
actual words spoken and the ways in which the words are pronounced and silent
language which is the communication through body language, silences and social
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 91
distance. Silent languages are particularly important in sales negotiations and other
forms of business meetings for example time, friendship, agreements.
A study was carried out in Brazil by Department of Anthropology, the University of
Alabama, USA and departamento de Clínica Médica, Faculdade de Medicina de
Ribeirão Preto, Universidade de São Paulo, Brazil, to get an insight of the Social and
cultural dimensions of hypertension in Brazil.
Elevated arterial blood pressure varies substantially in relation to social and cultural
variables. Early work on acculturation, socioeconomic status, and blood pressure
documented this variation, which could not be explained entirely by conventional
factors such as diet, physical activity, or access to medical care. These findings
stimulated the development of a model of stress and disease. The stress model
emphasizes social and psychological factors that are perceived by individuals to be
stressful, as well as factors that help individuals to respond to those stressors.
Conventional stress models are, however, problematic because the primary emphasis
is on individual perception, with little consideration of the social and cultural context
in which stress occurs. Findings from research in Brazil indicate that the higher an
individual’s cultural consonance, the lower his or her blood pressure. These results
indicate the importance of linking different levels of analysis – the cultural, the
individual, and the biological – to understand disease risk.
In this paper it was examined, in the context of Brazil, theory and research on social
and cultural factors and cardiovascular disease risk. The earliest observations
regarding social and cultural factors and disease risk documented the mean
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 92
differences in blood pressure (and rates of related cardiovascular diseases) between
societies with very different economic and social systems. Studies of isolated tribal
groups showed conclusively that certain kinds of associations – most prominently that
between age and blood pressure – that were thought to be “natural” based on research
in North American and Europe were actually not. Rather, the associations of age and
sex and blood pressure, and even adiposity and blood pressure, depended upon the
type of society studied. Explanations for this phenomenon included the low levels of
obesity, high activity levels, and low sodium intake observed in tribal societies, as
well as the possibility that individuals who might develop high blood pressure at a
later date had been selectively eliminated from the population by infectious or
parasitic disease. Detailed studies showed, however, that these explanations could not
account entirely for observed differences.
The association between societal type and blood pressure was further confirmed by
the study of two kinds of social change: the migration of groups from more traditional
to more modern communities, and social and cultural change occurring within a
single community. Results of these studies show that, as social and cultural change
occurs, mean blood pressure and rates of hypertension increase. Detailed studies show
that changes in physical activity and diet accompany culture change, but these
changes cannot account entirely for the magnitude of differences in mean blood
pressures and rates of hypertension between groups.
Cassel et al. (1960) were among the first investigators to suggest that social and
cultural processes might underlie these associations. Cassel acknowledged that
changes in diet, physical activity, adiposity, and health habits such as smoking
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 93
certainly were occurring in contexts of culture change. But, he argued, other
fundamental changes were occurring. Individuals who had been socialized in one
culture were confronting another. Literally, individuals who had been raised with one
body of shared knowledge that guided their behavior and enabled them to understand
and interpret others’ behaviors were now in a situation in which they were attempting
to negotiate a social world governed by a different set of meanings. This, Cassel
argued, would lead to many situations of confusion and frustration in mundane social
interaction, a situation likely to be stressful and, repeated over years, conducive to
sustained disease.
This emphasis on the stressful nature of culture change led researchers to adopt the
stress model developed in research in industrialized societies as their theoretical
orientation, but with modifications introduced on the basis of ethnographic research in
developing societies. So, for example, concepts like lifestyle incongruity were based
on observations regarding the changing status value of lifestyles in developing
societies. Similarly, in studying buffers against social stressors, researchers adapted
existing concepts of social supports to knowledge of the importance of various kinds
of social relationships in specific cultural contexts. These efforts can be seen as
modifying somewhat the content of the stress model, but still working within that
tradition.
The emphasis on the stress model for studying culture change and health was also
consistent with socio epidemiological work on stress, which grew primarily out of the
observations linking social class or socioeconomic status differences and health. With
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 94
conventional factors (such as obesity or diet) unable to explain social class differences
in health, researchers turned to the stress model.
More recent work on cultural consonance takes a different direction. Since the early
and pioneering work of Cassel, with its central importance of culture as a system of
knowledge and meaning, emphasis on culture per se has diminished in favor of the
specification of (culturally relevant) biobehavioral processes. The results of studying
cultural consonance, albeit tentative based on the results presented here from Brazil
and a replication study in the United States (Dressler et al., 1998), suggest that
Cassel’s original ideas may need to be reconsidered. The model of cultural
consonance provides theory and method for understanding how individuals are
distributed in cultural space, relative to prototypical shared cultural models of some
domain of life. Cassel suggested that individuals could find themselves in a state of
“cultural incongruity” because their own culture was not relevant in a particular
context. Similarly, we are suggesting that individuals can be low in cultural
consonance (or “culturally dissonant”) because they are, for whatever reason, unable
to act upon the widely shared ideas about how to live life appropriately. In either
respect, individuals (or groups of individuals) are prevented from effective
participation in their own society.
It would be straightforward to simply label this a stressful experience and leave it at
that. There is, however, a growing body of laboratory research to suggest that the
context of meaning surrounding social interaction can alter cardiovascular reactivity
to that interaction. For example, Lynch (1985) found that transitory blood pressure
elevations associated with social interaction can increase, and recovery to baseline
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 95
lengthen, if the participants in the interaction are of unequal social status. Similarly,
cardiovascular reactivity to laboratory social stimuli can be diminished by the
presence of a supportive friend in the testing situation.
These laboratory studies suggest that when social interaction is more orderly and
meaningful, an individual’s cardiovascular system maintains a more stable state.
Individuals who attain and maintain a higher cultural consonance along several
dimensions are living a life that is, by definition, more meaningful. Their lived
experience of the world, not just in thought but in actual behavior, conforms to the
widely shared ideas about (or cultural models of) the world. Individuals low in
cultural consonance are literally not experiencing this stable and meaningful world.
Instead, their lives are a constant reminder, in very concrete ways, of this instability
and lack of meaning. It may be, then, that in response to mundane stimuli in the
world, including social interaction, they are more highly reactive physiologically, a
reactivity that in turn can lead to sustained changes in the vascular bed and higher
blood pressure. This interpretation is not entirely speculative. A recent study from the
West Indies has shown that males who do not conform to the local cultural ideal of
male behavior have higher circulating levels of cortisol, and show greater reactivity in
cortisol to mundane stimuli.
The model of cultural consonance can also account for our earlier findings in Brazil.
For example, careful examination of the measurement of lifestyle incongruity shows
that people are not really trying to live a lifestyle of conspicuous consumption in the
context of low income. Rather, a careful examination of this measure shows that it
actually measures individuals’ difficulty in maintaining a very conventional lifestyle.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 96
Instead of living beyond their means, they do not have the means to maintain a very
basic lifestyle. By isolating the elements of that lifestyle that are most highly
culturally salient, the measure of cultural consonance in lifestyle simplifies the
detection of that association. (This is analogous to isolating different fractions of
serum lipids and observing the different effects of those fractions.) Similarly, the
more careful assessment of cultural consonance in social support, based on the
cultural model of social support, clarifies the basis for different kinds of supports
having different effects on health.
This is not to say, however, that the model of cultural consonance can completely
replace models of stress. As here, in Brazilian sample, cultural consonance conditions
or moderates the effects of perceived stress. This review demonstrates the importance
of incorporating a cultural perspective into an understanding of psychological and
behavioral influences on blood pressure. The concept of cultural consonance links the
cultural level of analysis to individual behavior, and this dimension of behavior and
its effects on health cannot be reduced to psychological or behavioral influences.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT
6.4 Competitor analysis (1)(18)(22)
Competition is becoming intense with every passing year. Companies
their customer and competitor orientation in order to be success
changing environment. Competitive analysis is a program for gathering
information about competitor’s activities and general business tren
company’s own goal
There are five forces that determine the intrinsic long run attractiveness
market segment. They are as follows:
• Industry competitors - A segment is unattractive if it al
numerous, strong or aggressive competitors. There condition
frequent price wars and new product introductions and will ma
to compete. It is more even unattractive if it is stable or dec
costs are high etc.
Results
Page 97
need to balance
ful in the fast
and analyzing
ds to further a
of a market or
ready contains
s will lead to
ke it expensive
lining, if fixed
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 98
• Potential entrants - A segment’s attractiveness varies with the height of its
entry and exit barriers. The most attractive segment is one in which entry
barriers are high and exit barriers are low. Few new firms can enter the
industry and poor performing firms can easily exit.
• Substitutes - A segment is unattractive when there are actual or potential
substitutes for the product. Substitutes place a limit on prices and on profit.
• Buyers - A segment is unattractive if buyers possess strong or growing
bargaining power. But in pharmaceutical market it is not applicable as the
drug to be bought, by the patient is decided by the doctor
• Suppliers - A segment is unattractive if company’s suppliers are able to raises
prices or reduce quantity supplied
Competition refers to rivalry among various firms operating in a particular market that
satisfy the same customer
Their action can spoil an attractive industry
Their weakness can be a target for exploitation
Their response to a firm’s marketing initiatives can have impact on a firm’s
success
Once a company identifies its primary competitors, it must ascertain their
strategies, objectives, strengths and weakness
Brazil plays a leading role in Latin America, being the main manufacturing center in
the region. The majority of the market volume is supplied by the domestic industry,
but in value terms, multinationals accounts for 70 per cent of market.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 99
The major part of pharmaceutical industry in Brazil includes Medley, EMS,
Biosintética and Eurofarma. Laboratórios Biosintética is one of the best
pharmaceutical companies in Brazil having major presence in cardiology,
dermatology, respiratory and oncology segments.
The other state-owned laboratory is Far-Manguinhos. International generic players
investing in the Brazilian pharmaceutical market are Hexal (Germany), Apotex
(Canada), Ranbaxy Farmaceutica Ltda (India), Teva (Israel), Ratiopharm (Germany),
Cinta (Spain) and Torrent Do Brasil (India).
The world’s largest generic drug maker, Teva entered into a joint venture with
Brazil’s leading generic company Biosintetica and formed BioTeva for distribution
and production of Teva generics. The latter also formed an agreement with Novartis
for marketing Valsartan (used as an anti-hypertensive). Teva invested between US$30
to 50 million towards production activities in Brazil. In another major event,
Denmark-based pharmaceutical major - Novo Nordisk acquired the Brazilian insulin
pharmaceutical company, Biobras. The wholly owned Brazilian subsidiary of India’s
Torrent Pharmaceuticals Ltd, Torrent Do Brasil, introduced ten products in Brazil.
Aurobindo Pharma Limited also targeted the Brazilian generic market for its
formulation business.
In Indian market the major players in cardiovascular segments are as follows:
I. Ranbaxy Laboratories Ltd is India’s largest pharmaceutical company,
manufacturing and marketing world class generics, branded generic
pharmaceuticals and active pharmaceutical ingredients. It is ranked amongst
the top ten generic companies worldwide. Ranbaxy has an expanding
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 100
international portfolio of affiliates, joint ventures and representative offices
across the globe with a presence in 23 of the top 25 pharma markets of the
world. With respect to Candesartan, the company has 2 brands that is
Candesar and Candesar-H available in the market
II. Since its inception in 1984, Dr Reddy’s Laboratories (DRL) has chosen to
walk the path of discovery and innovation in health sciences. The company
operates in over 100 countries worldwide. It has more than 75 patents to its
name with its pharmaceutical value chain ranging from API and Intermediates,
Finished Dosages (Branded and Generic) and New Chemical Entity (NCE)
Research. The company is engaged in manufacturing and marketing
pharmaceutical products. Cantar is the only brand of Candesartan available in
the market.
III. Lupin Ltd is the merged entity of Lupin Chemicals and Lupin Laboratories.
Lupin limited is among the top six Indian pharma companies with an
increasing global presence. It is USFDA & UKMCA approved and has a
strong R&D which focuses on process chemistry, fermentation, ANDA,
NDDS and NCE. It is one of India's largest manufacturers of bulk actives and
formulations. Its major therapeutic focus areas are anti TB, Cephalosporin,
Ace-inhibitors, Statins and Prils. Telma is one of the leading brand currently in
the ARB category in the Indian market. It has also other brands such as Valent
which was a leading brand too few years ago.
IV. Cadila Healthcare Ltd, the flagship company of the Ahmedabad based Zydus
Group, is one of India's leading integrated pharmaceutical companies. The
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 101
company is also a leading producer of niche and complex bulk drugs. Zydus
Research Centre (ZRC) is the research and development wing of Zydus
Cadila. The company plans to develop new markets in Latin America, Asia
and the Middle East.
V. Glenmark Pharmaceuticals is one of the leading Indian pharmaceutical
companies. It marketsits products to over 27 countries across the globe with
2000 employees, over 150 scientistsand 15 offices. It is a leading research &
development firm with a thrust on manufacturing &product marketing
globally. Glenmark follows a branded generic model in markets across Asia,
Africa, CIS countries, Russia and Latin America.
VI. Torrent Pharmaceuticals Ltd (TPL) is the flagship company of the Torrent
Group. Founded in 1972, it is based in Ahmedabad. It manufactures bulk
drugs and formulations. It also manufactures and markets medical diagnostic
instruments. In a major move to restructure, the company has carved out five
divisions: prima, psycan, vista, axon and neuron. Of its divisions, prima offer
mass products, psycan focus on cardiology, vista is a sub-speciality division
and axon and neuron focus on neuro psychiatry
VII. Aventis Pharma Limited is the second largest pharmaceutical multinational
company in India which has a commercial presence in 80 countries. Aventis
Pharma Limited previously known as Hoechst Marion Roussel deals in a
number of activities ranging form prescription drugs, vaccines, therapeutic
proteins and diagnostics. It has the distinction of being the only MNC to have
the most current product portfolio equivalent to its parent company. It
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 102
provides high performance industrial facilities and is equipped with an
exceptional sales force
Results
Primary survey
Bangalore chemist’s survey:
Q.1. How many prescriptions for medications used in the treatment of hypertension
do you receive per week?
A) Less than10 = 10% B) 10-20 = 42% C) 20-30 = 20% D) More than 30 = 28%
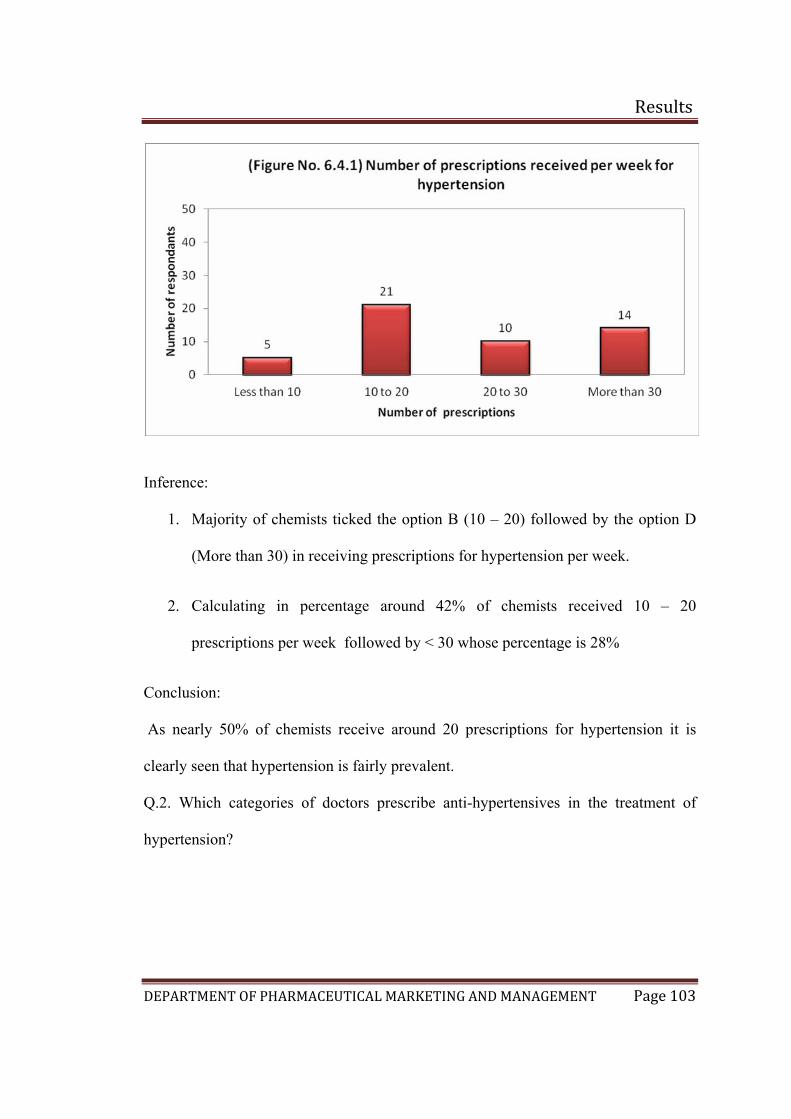
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 103
Inference:
1. Majority of chemists ticked the option B (10 – 20) followed by the option D
(More than 30) in receiving prescriptions for hypertension per week.
2. Calculating in percentage around 42% of chemists received 10 – 20
prescriptions per week followed by < 30 whose percentage is 28%
Conclusion:
As nearly 50% of chemists receive around 20 prescriptions for hypertension it is
clearly seen that hypertension is fairly prevalent.
Q.2. Which categories of doctors prescribe anti-hypertensives in the treatment of
hypertension?
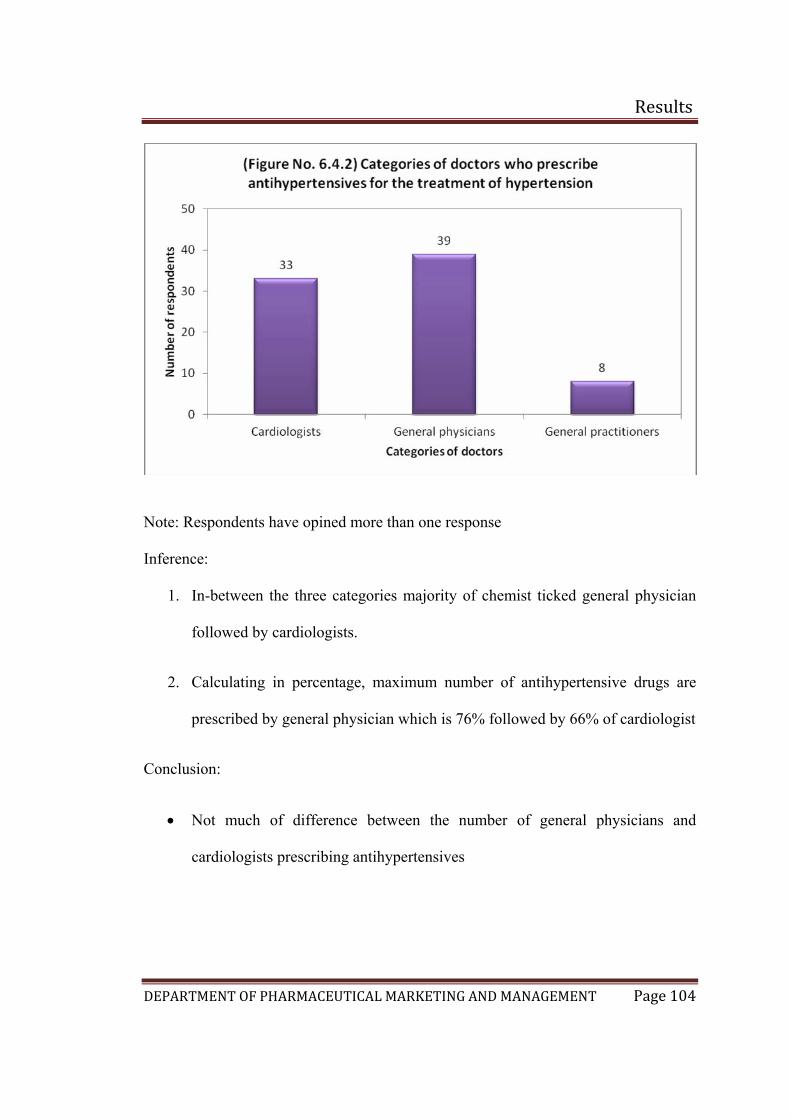
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 104
Note: Respondents have opined more than one response
Inference:
1. In-between the three categories majority of chemist ticked general physician
followed by cardiologists.
2. Calculating in percentage, maximum number of antihypertensive drugs are
prescribed by general physician which is 76% followed by 66% of cardiologist
Conclusion:
• Not much of difference between the number of general physicians and
cardiologists prescribing antihypertensives
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 105
• Not many general practitioners prescribe antihypertensives probably they refer
the patients to cardiologist or general physicians
General physicians are the maximum prescription givers for antihypertensive
drugs followed by Cardiologist. So the major target for the company should be the
general physicians and cardiologists

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 106
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 107
Inference:
1. The top 5 brands in the market which has the maximum presence in the market
are Cardace, Listril, Ramace, Envas and Ramistar, in which Cardace has the
highest number of preferences
2. Calculating the percentage 92% of chemist ticked Cardace, followed by Listril
86%, Ramace 84%, Envas 76%, and Ramistar 62%
3. The chemical entity in Cardace is Ramipril which is marketed by Sanofi
Aventis followed by Listril whose chemical entity is lisnopril marketed by
Torrent Pharma.
4. Captopril was the first agent to be developed for the treatment of hypertension.
Since then, enalapril, lisinopril, quinapril, ramipril, benazepril, moexipril are
also available in market, but from the above survey carried out in Bangalore,
Ramipril is the top molecule sold in market followed by Lisinopril as per 50
chemists.

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 108
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 109
Inference:
1. The top 5 brands in the market was found to be Telma followed by Losacar,
Telista, Tozaar and Convance.
2. Calculating in percentage, 84% of the chemist ticked Telma, followed by
Losacar 82%, Telista 66%, Tozaar 64% and Covance 56%
3. Telma whose chemical entity is Telmisartan is markeed by Glenmark followed
by Losacar whose chemical entity is Losartan potassium of Zydus Cadilla.
4. The importance of angiotensin II in regulating cardiovascular function has led
to the development of nonpeptide antagonists of the AT1 angiotensin II
receptor for clinical use. Losartan, candesartan, irbesartan, valsartan ,
telmisartan, and eprosartan have been approved for the treatment of
hypertension and are available in market.
The survey carried out in Bangalore for the 50 chemists showed that
Telmisartan is the top molecule sold in market followed by Losartan.
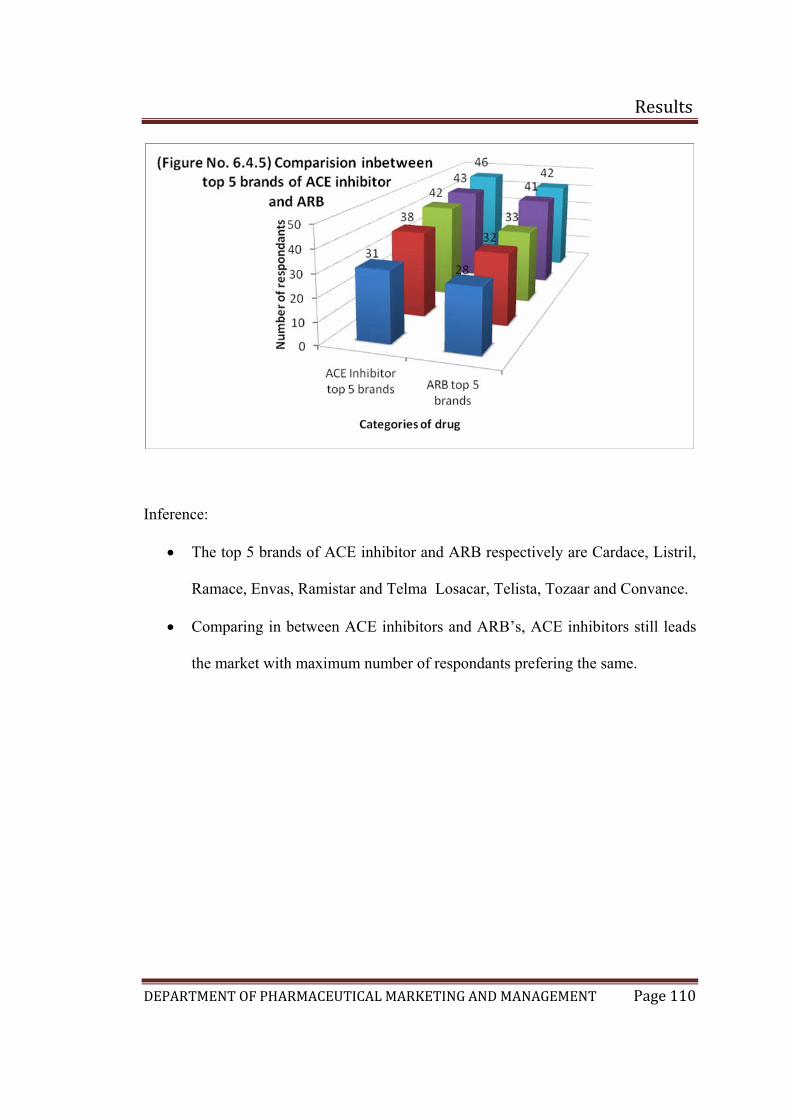
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 110
Inference:
• The top 5 brands of ACE inhibitor and ARB respectively are Cardace, Listril,
Ramace, Envas, Ramistar and Telma Losacar, Telista, Tozaar and Convance.
• Comparing in between ACE inhibitors and ARB’s, ACE inhibitors still leads
the market with maximum number of respondants prefering the same.
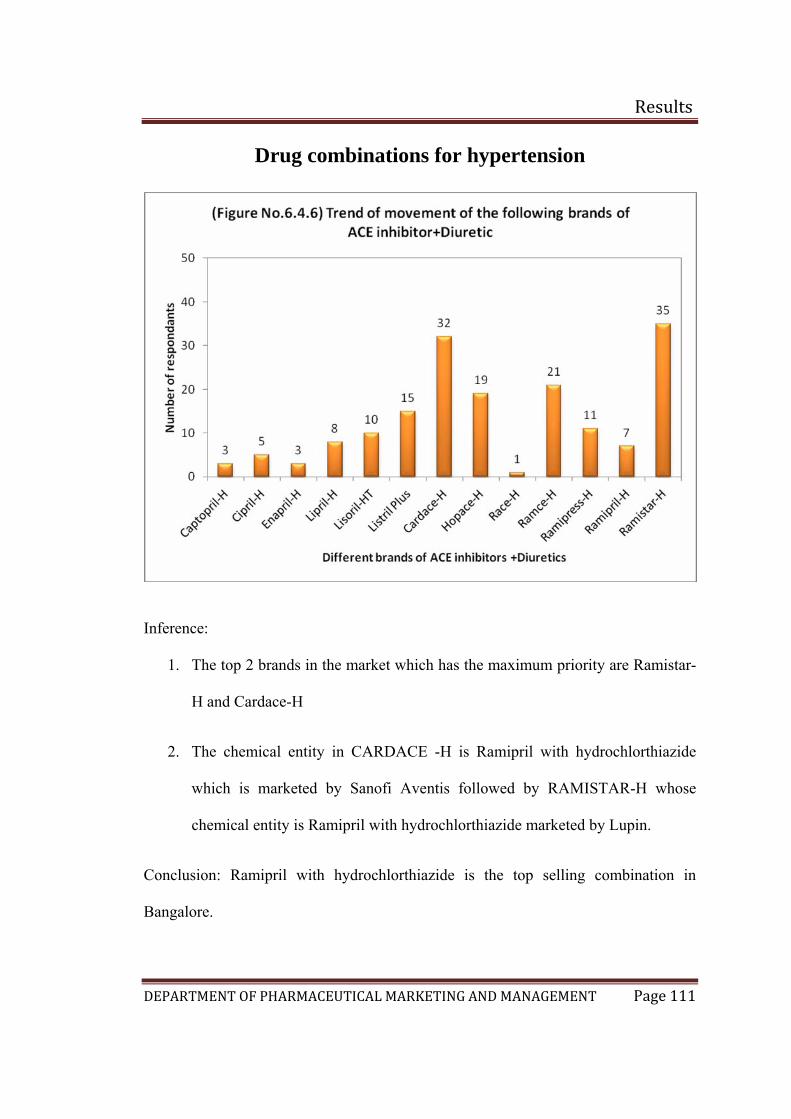
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 111
Drug combinations for hypertension
Inference:
1. The top 2 brands in the market which has the maximum priority are Ramistar-
H and Cardace-H
2. The chemical entity in CARDACE -H is Ramipril with hydrochlorthiazide
which is marketed by Sanofi Aventis followed by RAMISTAR-H whose
chemical entity is Ramipril with hydrochlorthiazide marketed by Lupin.
Conclusion: Ramipril with hydrochlorthiazide is the top selling combination in
Bangalore.
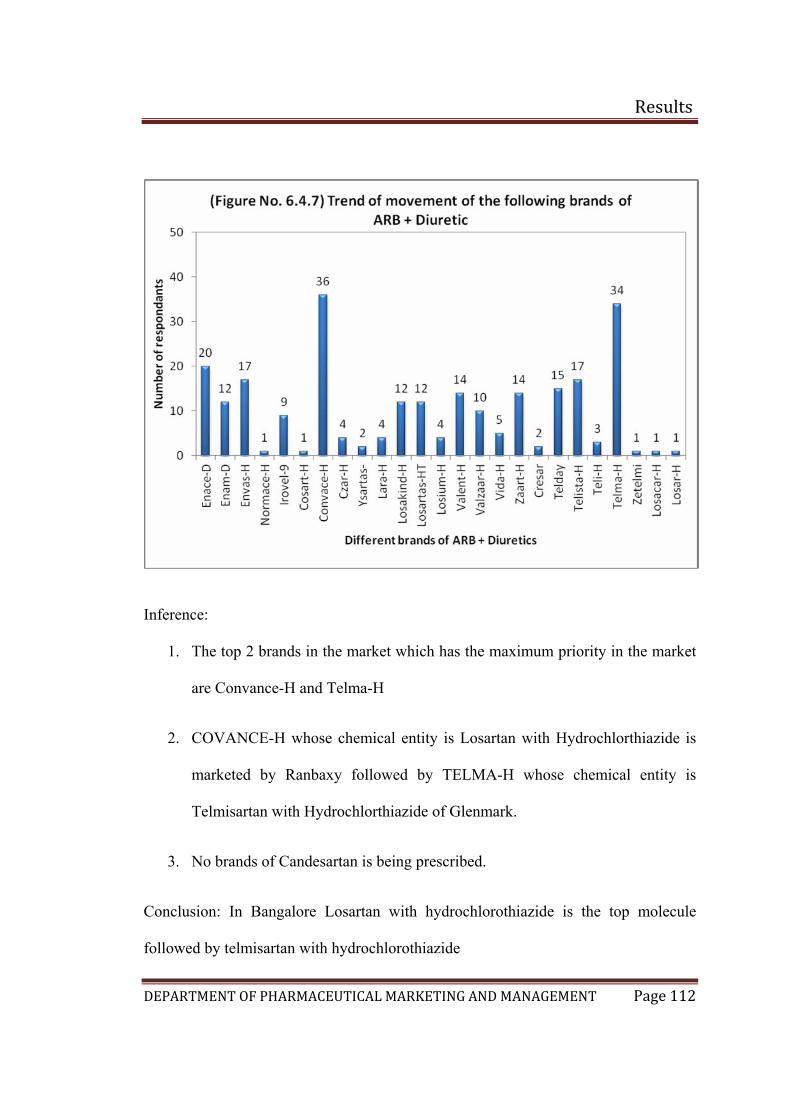
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 112
Inference:
1. The top 2 brands in the market which has the maximum priority in the market
are Convance-H and Telma-H
2. COVANCE-H whose chemical entity is Losartan with Hydrochlorthiazide is
marketed by Ranbaxy followed by TELMA-H whose chemical entity is
Telmisartan with Hydrochlorthiazide of Glenmark.
3. No brands of Candesartan is being prescribed.
Conclusion: In Bangalore Losartan with hydrochlorothiazide is the top molecule
followed by telmisartan with hydrochlorothiazide
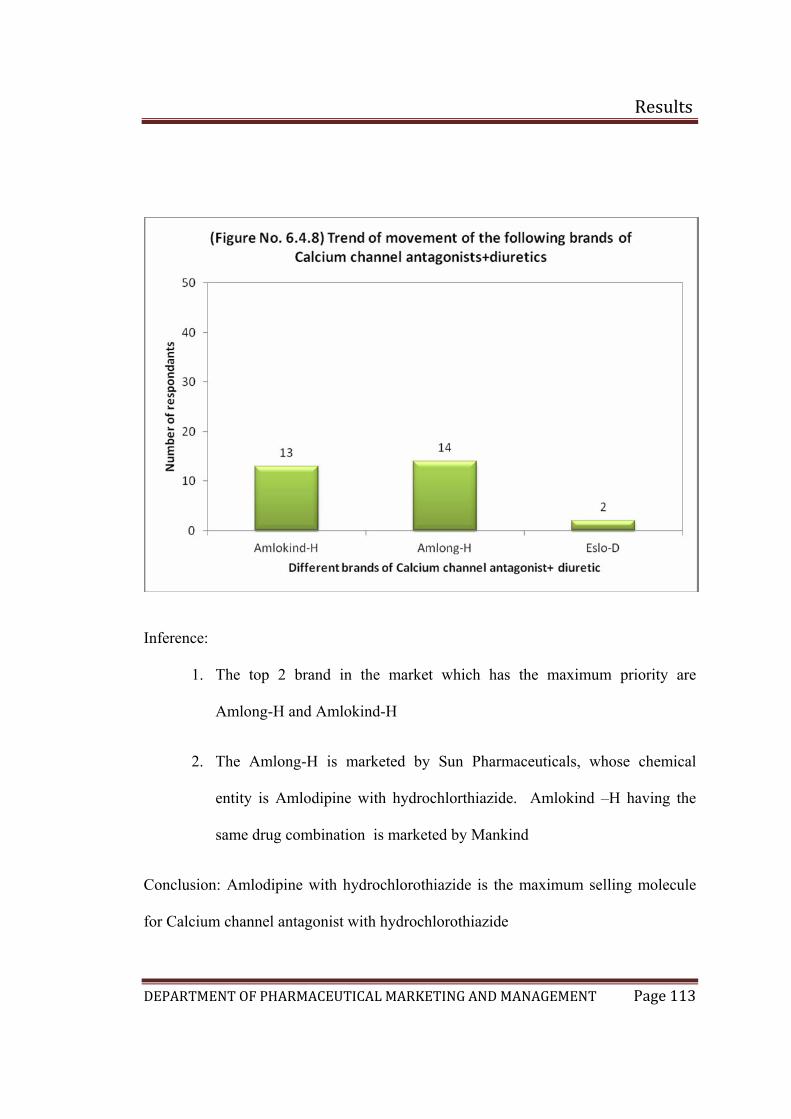
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 113
Inference:
1. The top 2 brand in the market which has the maximum priority are
Amlong-H and Amlokind-H
2. The Amlong-H is marketed by Sun Pharmaceuticals, whose chemical
entity is Amlodipine with hydrochlorthiazide. Amlokind –H having the
same drug combination is marketed by Mankind
Conclusion: Amlodipine with hydrochlorothiazide is the maximum selling molecule
for Calcium channel antagonist with hydrochlorothiazide
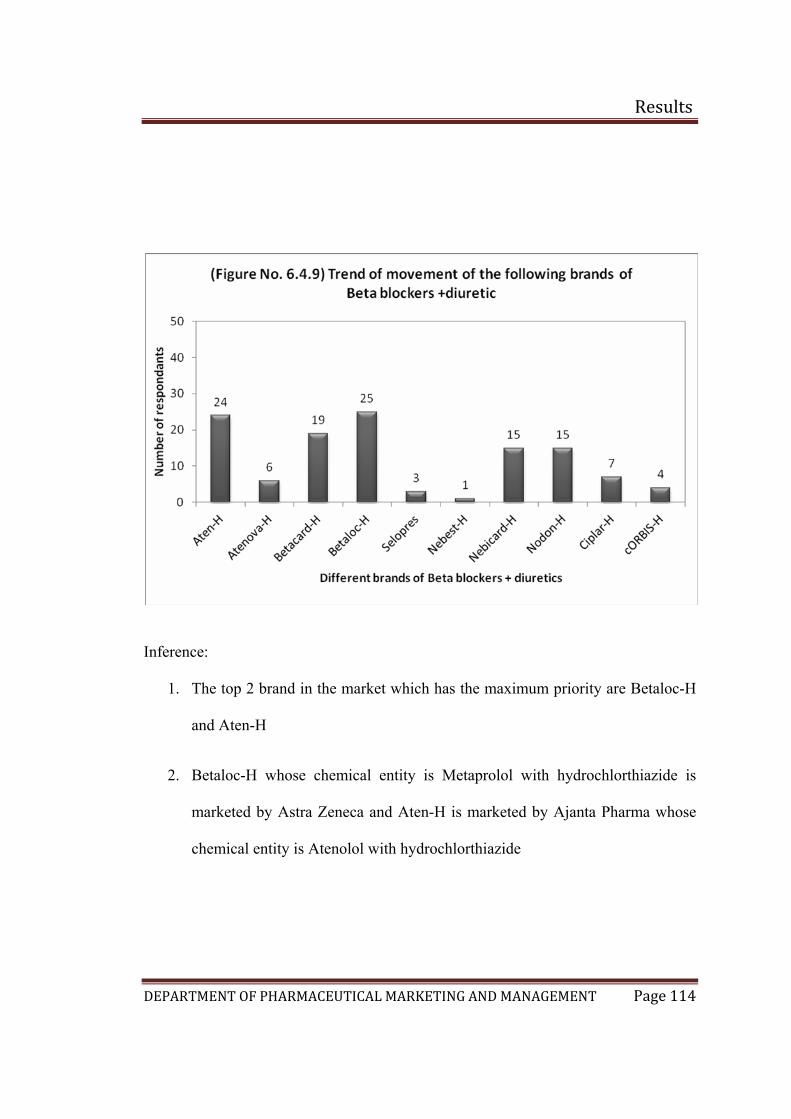
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 114
Inference:
1. The top 2 brand in the market which has the maximum priority are Betaloc-H
and Aten-H
2. Betaloc-H whose chemical entity is Metaprolol with hydrochlorthiazide is
marketed by Astra Zeneca and Aten-H is marketed by Ajanta Pharma whose
chemical entity is Atenolol with hydrochlorthiazide
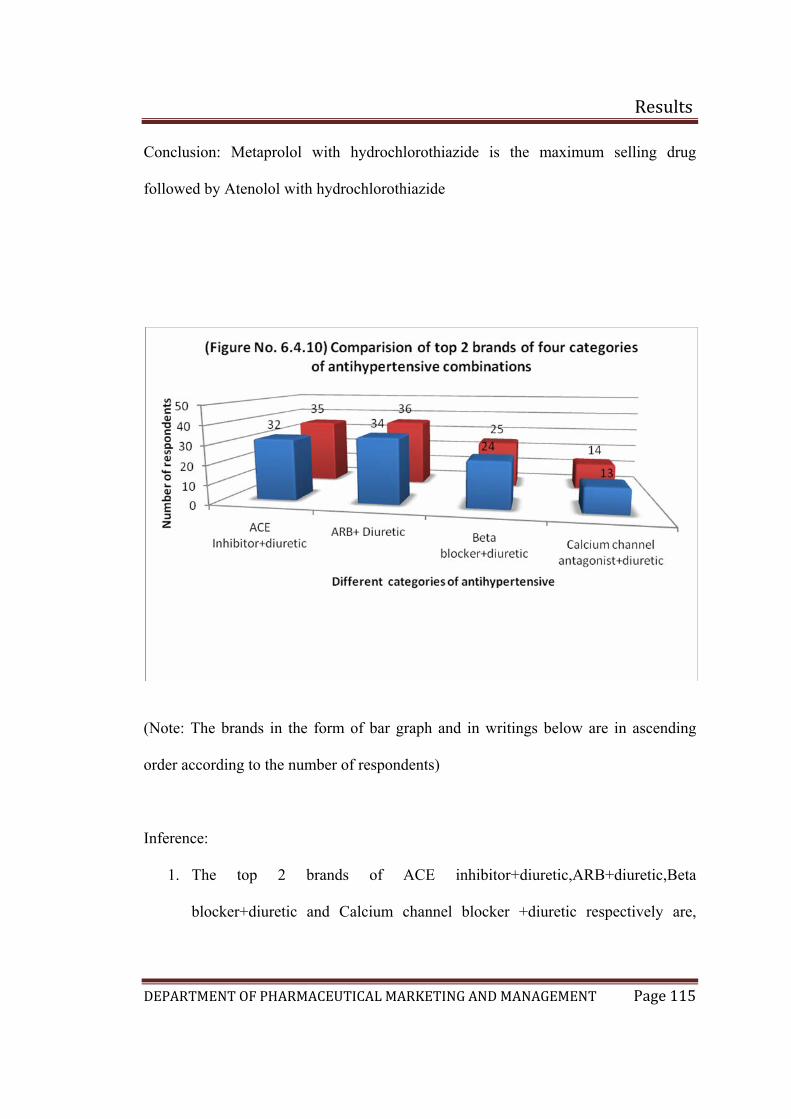
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 115
Conclusion: Metaprolol with hydrochlorothiazide is the maximum selling drug
followed by Atenolol with hydrochlorothiazide
(Note: The brands in the form of bar graph and in writings below are in ascending
order according to the number of respondents)
Inference:
1. The top 2 brands of ACE inhibitor+diuretic,ARB+diuretic,Beta
blocker+diuretic and Calcium channel blocker +diuretic respectively are,
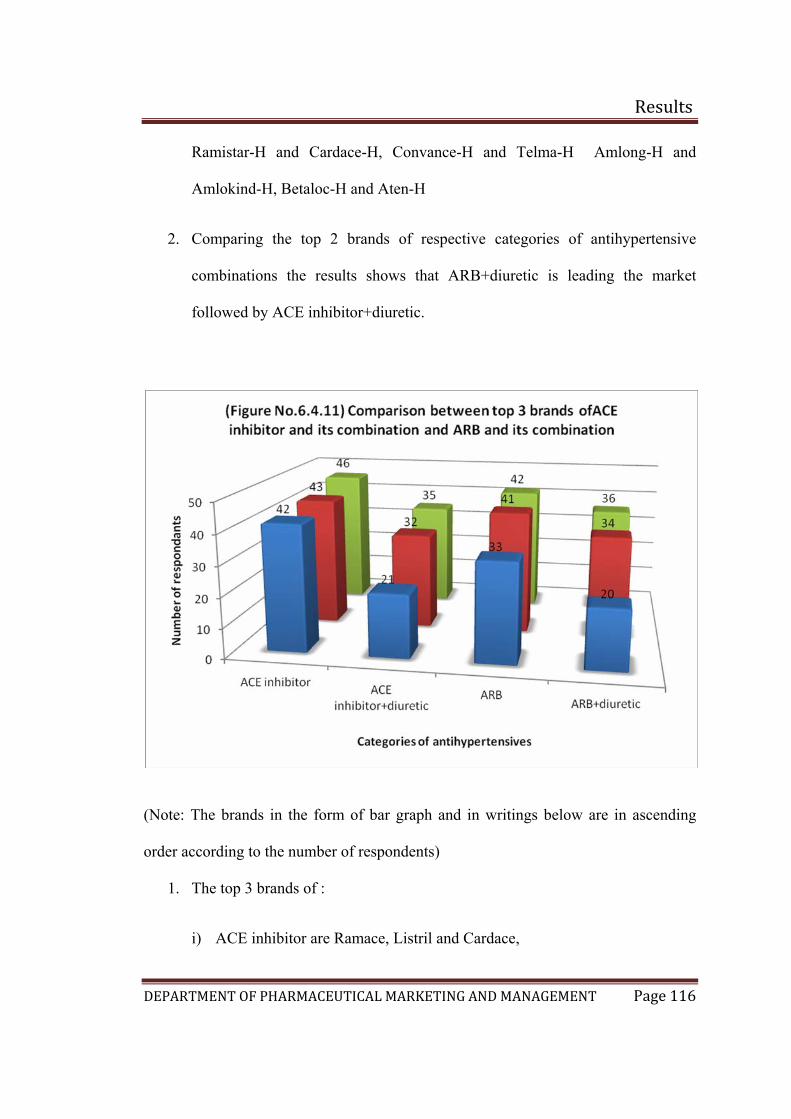
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 116
Ramistar-H and Cardace-H, Convance-H and Telma-H Amlong-H and
Amlokind-H, Betaloc-H and Aten-H
2. Comparing the top 2 brands of respective categories of antihypertensive
combinations the results shows that ARB+diuretic is leading the market
followed by ACE inhibitor+diuretic.
(Note: The brands in the form of bar graph and in writings below are in ascending
order according to the number of respondents)
1. The top 3 brands of :
i) ACE inhibitor are Ramace, Listril and Cardace,
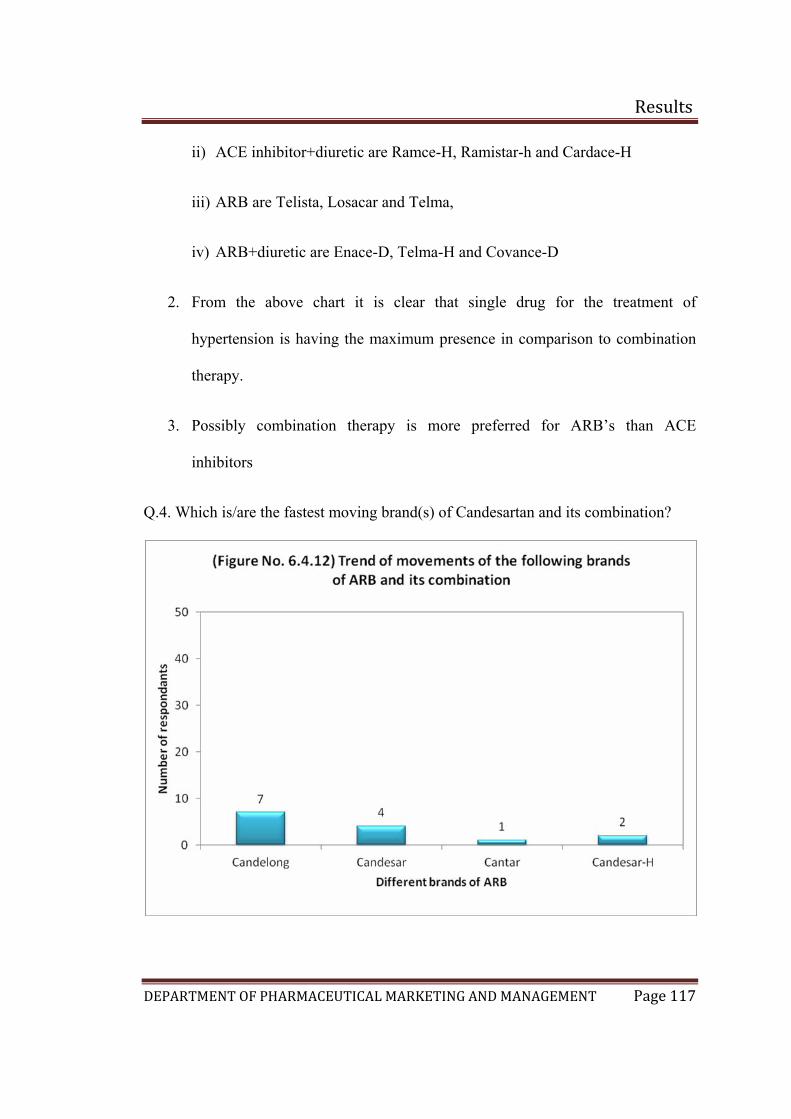
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 117
ii) ACE inhibitor+diuretic are Ramce-H, Ramistar-h and Cardace-H
iii) ARB are Telista, Losacar and Telma,
iv) ARB+diuretic are Enace-D, Telma-H and Covance-D
2. From the above chart it is clear that single drug for the treatment of
hypertension is having the maximum presence in comparison to combination
therapy.
3. Possibly combination therapy is more preferred for ARB’s than ACE
inhibitors
Q.4. Which is/are the fastest moving brand(s) of Candesartan and its combination?
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 118
1. The fastest moving brand is Candelong whose chemical entity is Candesartan
which is marketed by Micro Labs.
2. From the above data acquired, it is quite clear that the base molecule does not
yet have a good market share.
3. Some chemists are not even aware of the brands and in maximum number of
cases the chemists did not have a stock of the products containing
Candesartan.
Conclusion: Only 3 brands of Candesartan and 1 brand of Candesartan and its
combination are available among which Candelong is the moving brand.
Chemist survey Kolkata
Q.1. How many prescriptions for medications used in the treatment of hypertension
do you receive per week?
A) Less than10 =16% B) 10-20 =30% C) 20-30 =14% D) More than 30 =40%
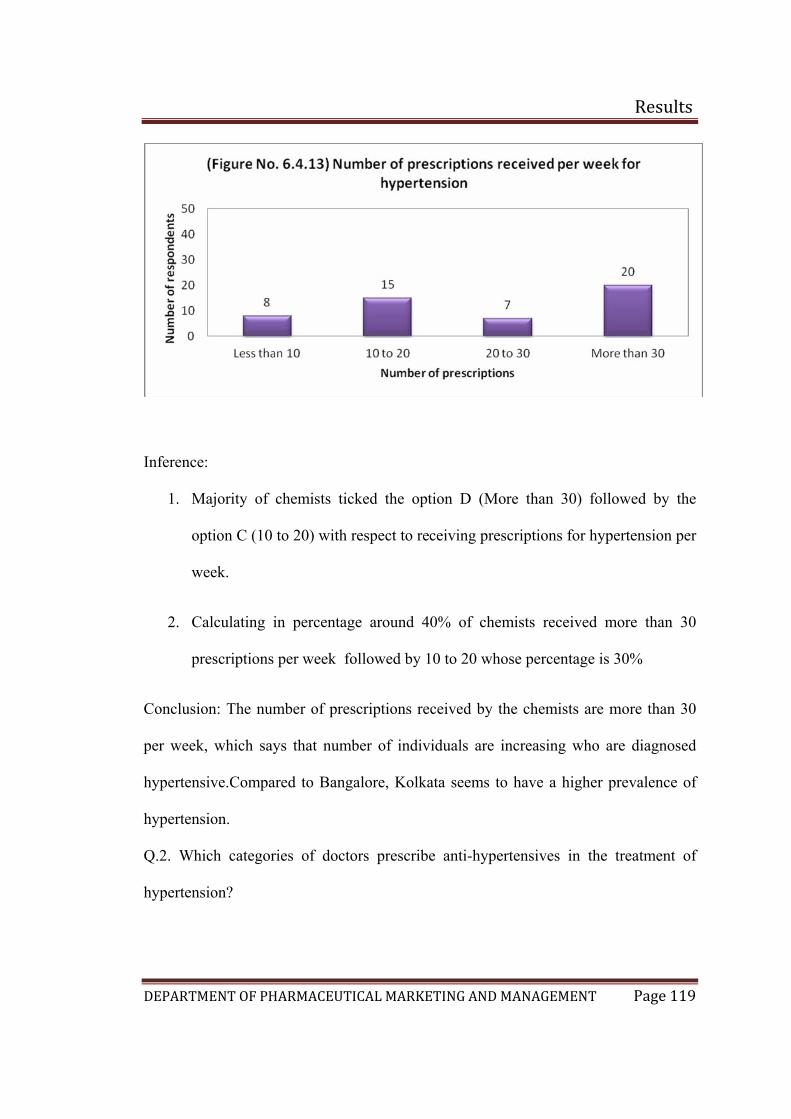
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 119
Inference:
1. Majority of chemists ticked the option D (More than 30) followed by the
option C (10 to 20) with respect to receiving prescriptions for hypertension per
week.
2. Calculating in percentage around 40% of chemists received more than 30
prescriptions per week followed by 10 to 20 whose percentage is 30%
Conclusion: The number of prescriptions received by the chemists are more than 30
per week, which says that number of individuals are increasing who are diagnosed
hypertensive.Compared to Bangalore, Kolkata seems to have a higher prevalence of
hypertension.
Q.2. Which categories of doctors prescribe anti-hypertensives in the treatment of
hypertension?
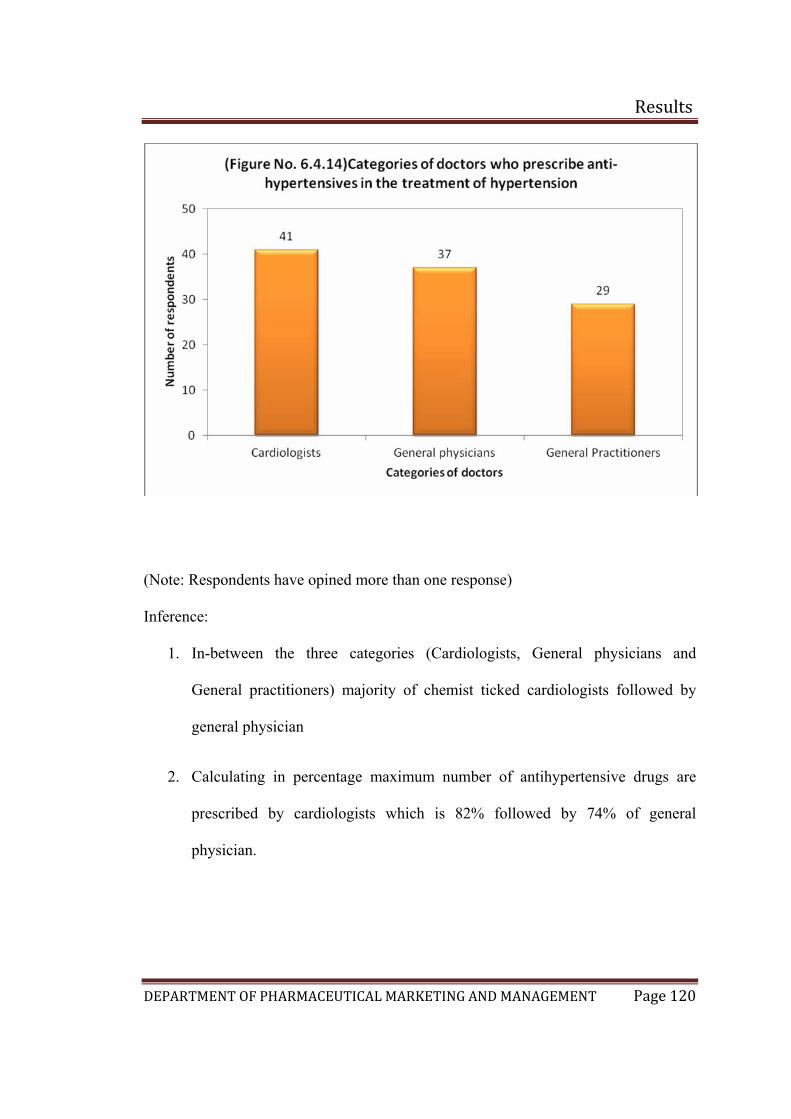
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 120
(Note: Respondents have opined more than one response)
Inference:
1. In-between the three categories (Cardiologists, General physicians and
General practitioners) majority of chemist ticked cardiologists followed by
general physician
2. Calculating in percentage maximum number of antihypertensive drugs are
prescribed by cardiologists which is 82% followed by 74% of general
physician.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 121
3. In Kolkata, General practitioners (58%) are also prescribing anti-
hypertensives, which is quite higher in percentage in comparison to Bangalore
(10%)
Conclusion:
Cardiologists are the maximum prescription givers for antihypertensive drugs
followed by General physicians. So the major target for the company should be the
Cardiologists. In Kolkata general practitioners are also prescribing antihypertensives
and this is higher than that in Bangalore

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 122
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 123
Inference:
1. The top 6 brands in the market which has the maximum priority in the market
are Cardace, Ramace, Envas, Ramistar,Lipril and Cardiopril in which
Cardace got the highest number of preferences
2. Calculating the percentage 94% of chemist ticked Cardace, followed by
Ramace 84%, Envas 72%, Ramistar 68%, Lipril 62% and Cardiopril 60%
3. The chemical entity in Cardace is Ramipril which is marketed by Sanofi
Aventis followed by Ramace whose chemical entity is Ramipril marketed by
Astra Zeneca
4. Captopril was the first agent to be developed for the treatment of hypertension.
Since then, enalapril, lisinopril, quinapril, ramipril, benazepril, moexipril are
also available in market, but from the above survey carried out in Kolkata,
Ramipril is the top molecule sold in market as per the study undertaken.

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 124
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 125
Inference:
1. The top 5 brands in the market was found to be Telma followed by Losacar,
Telday, Tozar, Losakind and Covance.
2. Calculating in percentage, 90% of the chemist ticked Telma, followed by
Losacar and Telday 84% which has the equal number of respondants, Tozaar
78%, Losakind 74% and Covance 62%.
3. Telma whose chemical entity is Telmisartan is marketed by Glenmark
followed by Losacar whose chemical entity is Losartan potassium of Zydus
Cadilla and Telday whose chemical entity is once again Telmisartan of
Torrent.
4. The survey carried out in Kolkata for the 50 chemists proved that Telmisartan
is the top molecule sold in market followed by Losartan.
5. In compare to Bangalore the preference to the molecule Telmisartan is higher
in Kolkata.
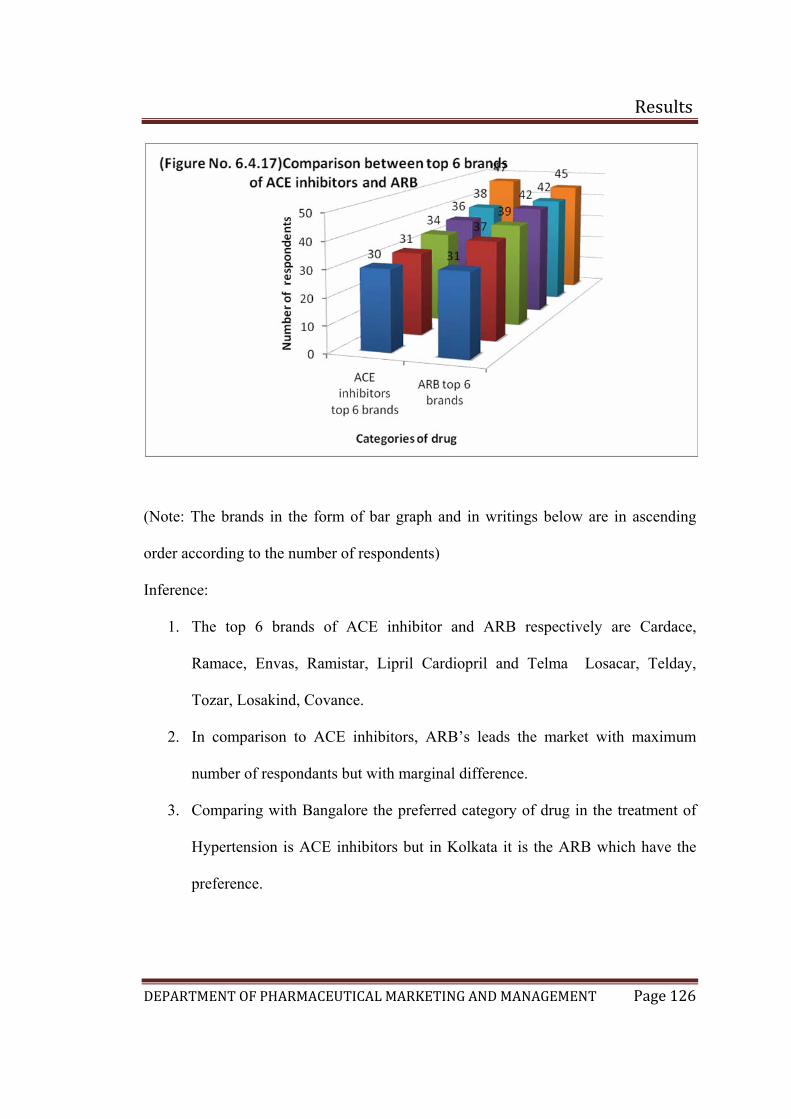
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 126
(Note: The brands in the form of bar graph and in writings below are in ascending
order according to the number of respondents)
Inference:
1. The top 6 brands of ACE inhibitor and ARB respectively are Cardace,
Ramace, Envas, Ramistar, Lipril Cardiopril and Telma Losacar, Telday,
Tozar, Losakind, Covance.
2. In comparison to ACE inhibitors, ARB’s leads the market with maximum
number of respondants but with marginal difference.
3. Comparing with Bangalore the preferred category of drug in the treatment of
Hypertension is ACE inhibitors but in Kolkata it is the ARB which have the
preference.
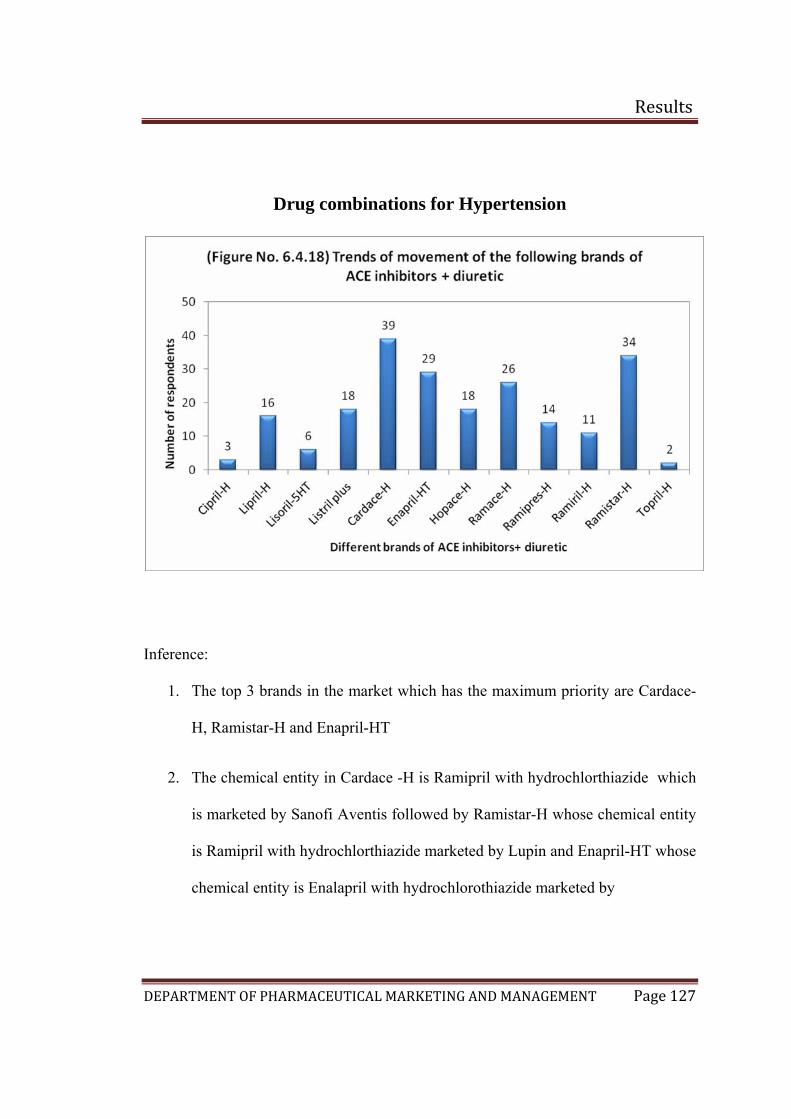
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 127
Drug combinations for Hypertension
Inference:
1. The top 3 brands in the market which has the maximum priority are Cardace-
H, Ramistar-H and Enapril-HT
2. The chemical entity in Cardace -H is Ramipril with hydrochlorthiazide which
is marketed by Sanofi Aventis followed by Ramistar-H whose chemical entity
is Ramipril with hydrochlorthiazide marketed by Lupin and Enapril-HT whose
chemical entity is Enalapril with hydrochlorothiazide marketed by
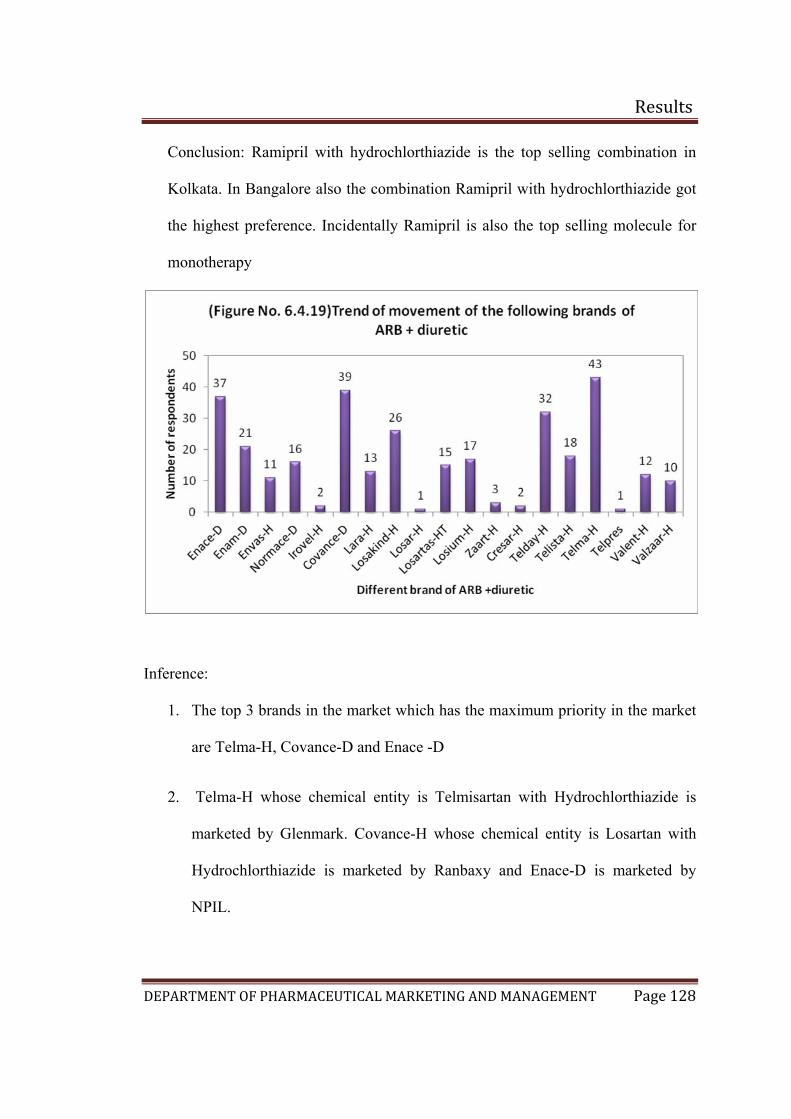
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 128
Conclusion: Ramipril with hydrochlorthiazide is the top selling combination in
Kolkata. In Bangalore also the combination Ramipril with hydrochlorthiazide got
the highest preference. Incidentally Ramipril is also the top selling molecule for
monotherapy
Inference:
1. The top 3 brands in the market which has the maximum priority in the market
are Telma-H, Covance-D and Enace -D
2. Telma-H whose chemical entity is Telmisartan with Hydrochlorthiazide is
marketed by Glenmark. Covance-H whose chemical entity is Losartan with
Hydrochlorthiazide is marketed by Ranbaxy and Enace-D is marketed by
NPIL.
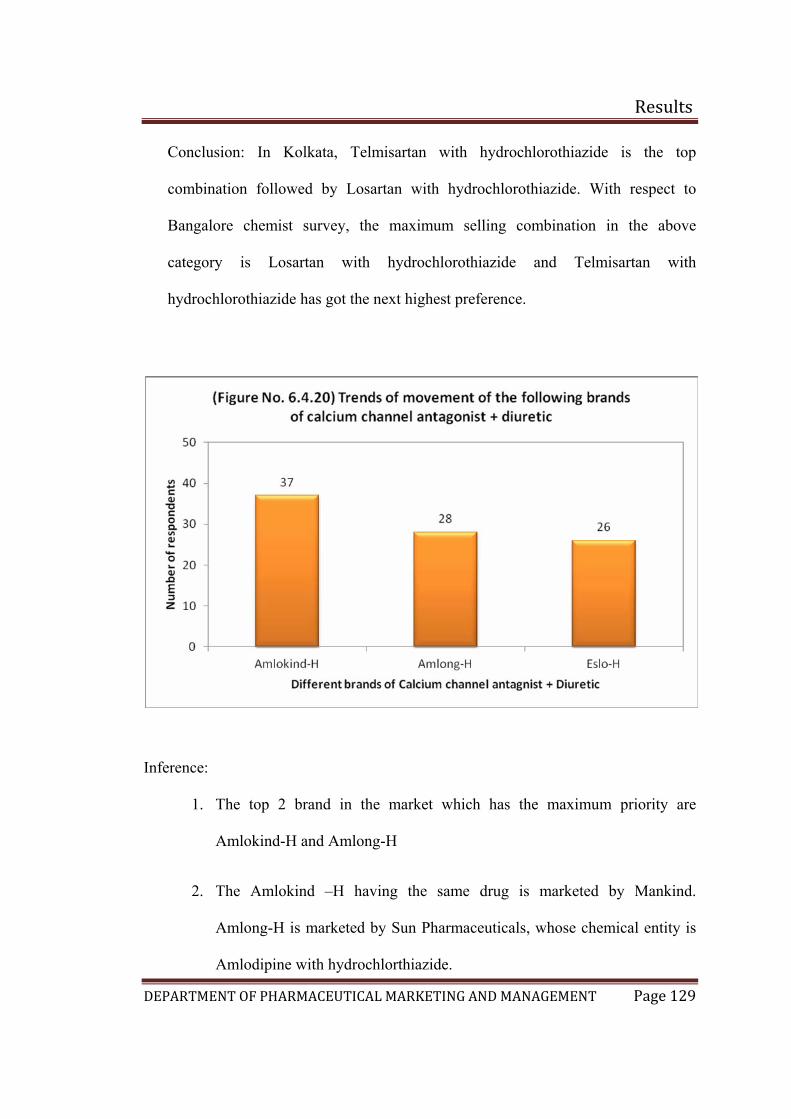
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 129
Conclusion: In Kolkata, Telmisartan with hydrochlorothiazide is the top
combination followed by Losartan with hydrochlorothiazide. With respect to
Bangalore chemist survey, the maximum selling combination in the above
category is Losartan with hydrochlorothiazide and Telmisartan with
hydrochlorothiazide has got the next highest preference.
Inference:
1. The top 2 brand in the market which has the maximum priority are
Amlokind-H and Amlong-H
2. The Amlokind –H having the same drug is marketed by Mankind.
Amlong-H is marketed by Sun Pharmaceuticals, whose chemical entity is
Amlodipine with hydrochlorthiazide.
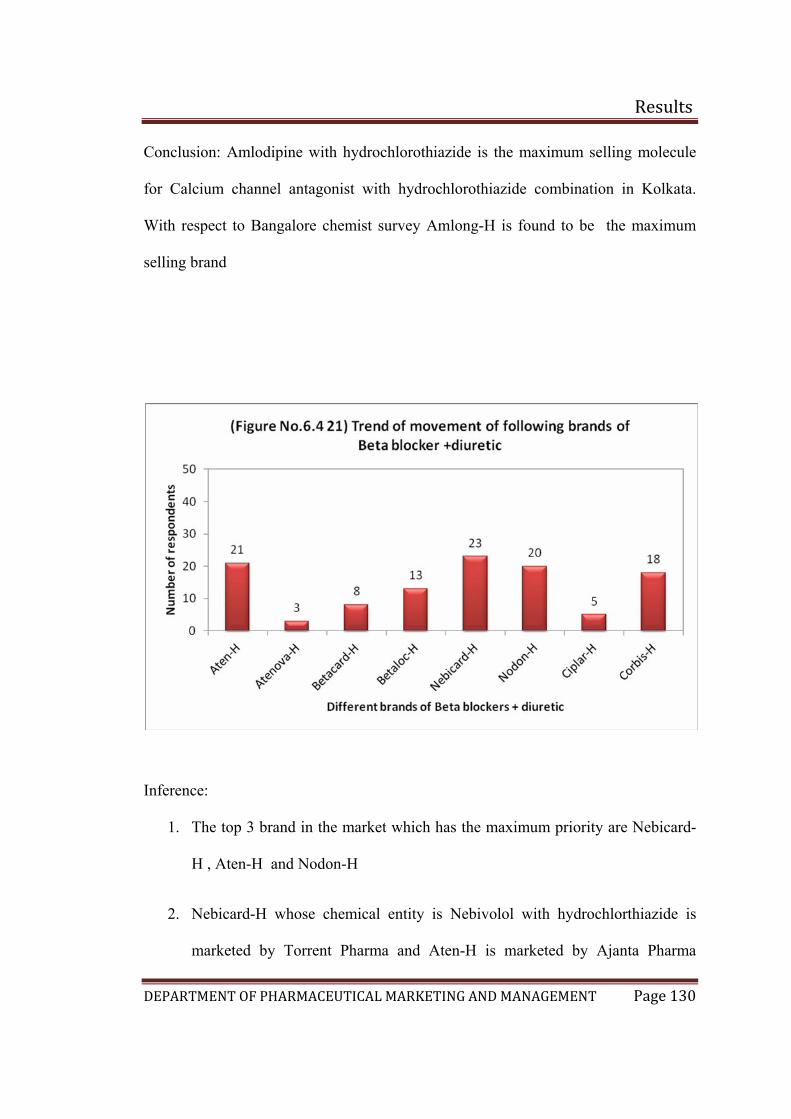
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 130
Conclusion: Amlodipine with hydrochlorothiazide is the maximum selling molecule
for Calcium channel antagonist with hydrochlorothiazide combination in Kolkata.
With respect to Bangalore chemist survey Amlong-H is found to be the maximum
selling brand
Inference:
1. The top 3 brand in the market which has the maximum priority are Nebicard-
H , Aten-H and Nodon-H
2. Nebicard-H whose chemical entity is Nebivolol with hydrochlorthiazide is
marketed by Torrent Pharma and Aten-H is marketed by Ajanta Pharma
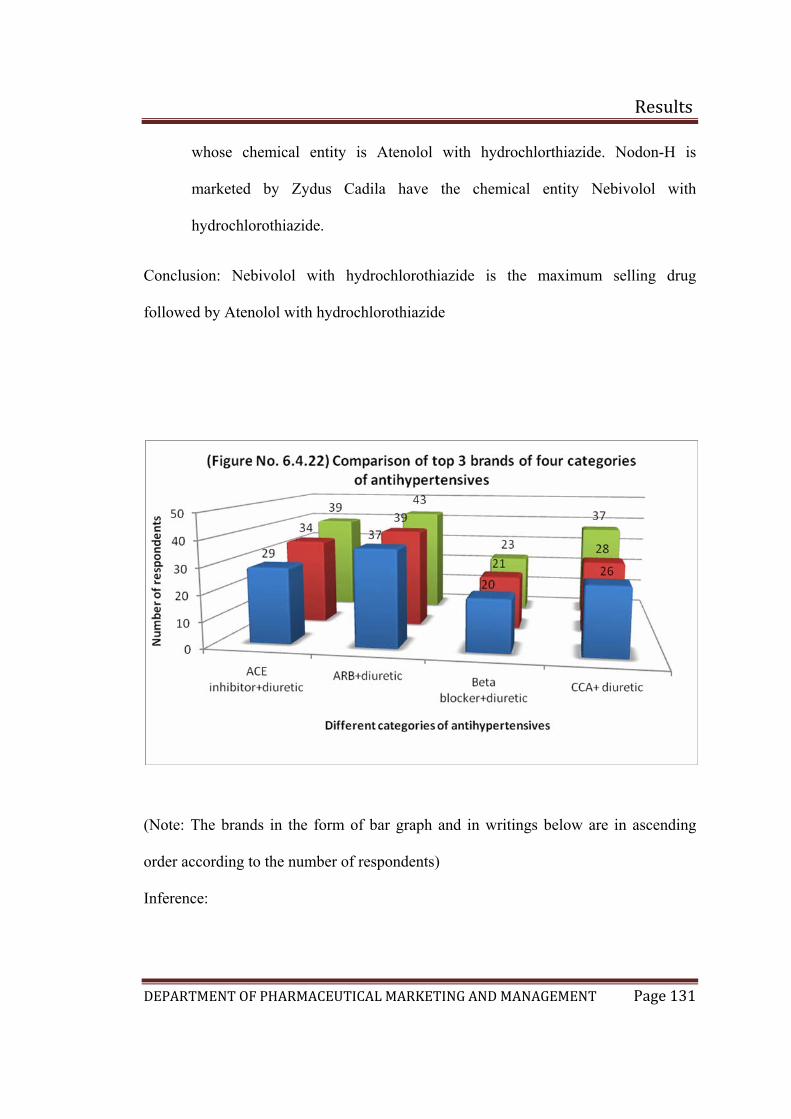
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 131
whose chemical entity is Atenolol with hydrochlorthiazide. Nodon-H is
marketed by Zydus Cadila have the chemical entity Nebivolol with
hydrochlorothiazide.
Conclusion: Nebivolol with hydrochlorothiazide is the maximum selling drug
followed by Atenolol with hydrochlorothiazide
(Note: The brands in the form of bar graph and in writings below are in ascending
order according to the number of respondents)
Inference:
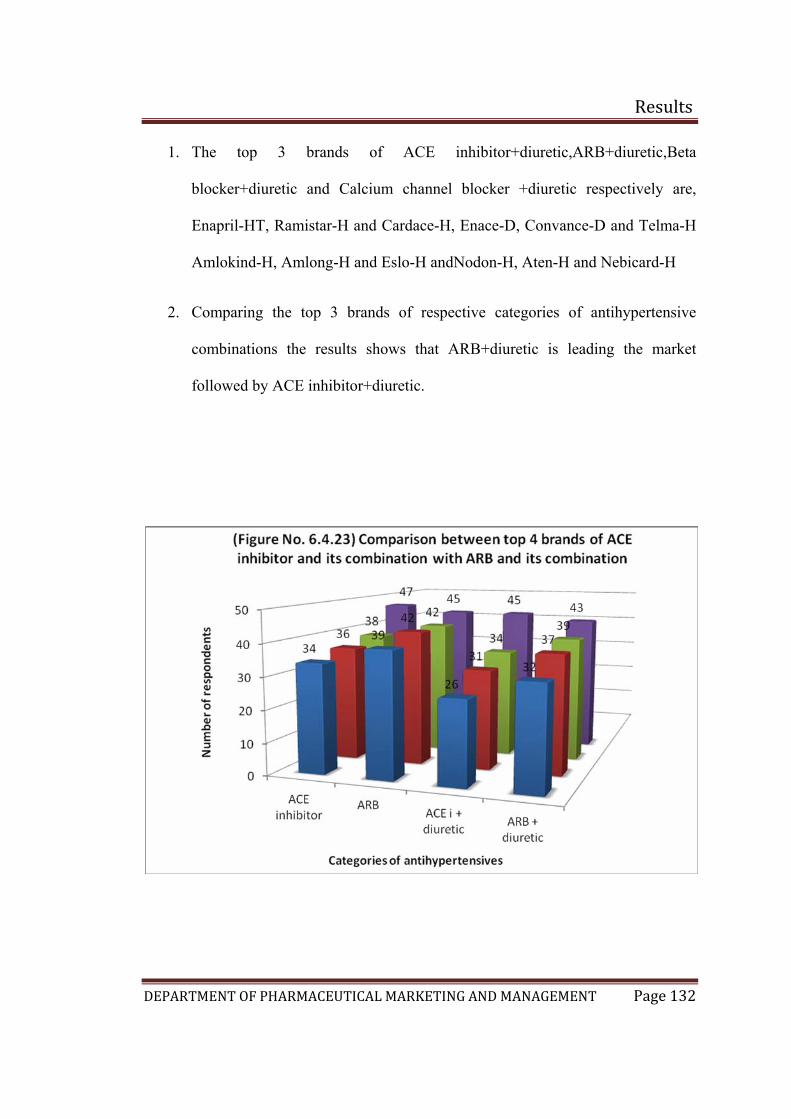
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 132
1. The top 3 brands of ACE inhibitor+diuretic,ARB+diuretic,Beta
blocker+diuretic and Calcium channel blocker +diuretic respectively are,
Enapril-HT, Ramistar-H and Cardace-H, Enace-D, Convance-D and Telma-H
Amlokind-H, Amlong-H and Eslo-H andNodon-H, Aten-H and Nebicard-H
2. Comparing the top 3 brands of respective categories of antihypertensive
combinations the results shows that ARB+diuretic is leading the market
followed by ACE inhibitor+diuretic.
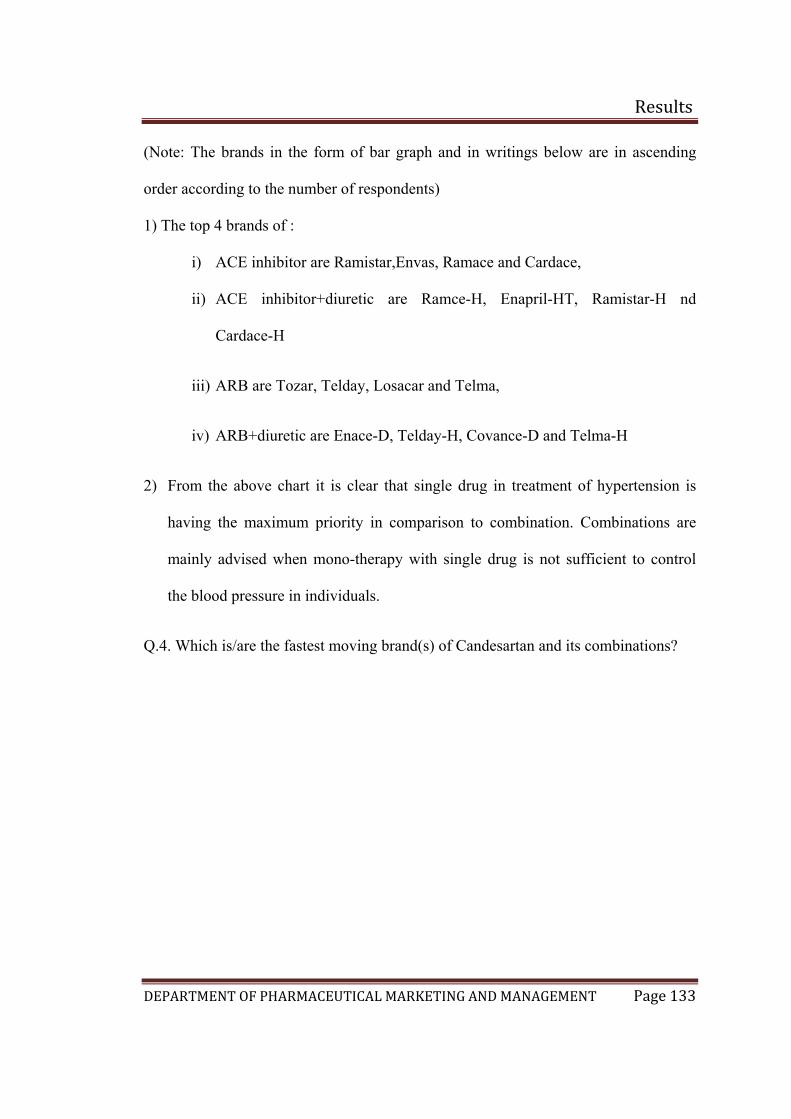
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 133
(Note: The brands in the form of bar graph and in writings below are in ascending
order according to the number of respondents)
1) The top 4 brands of :
i) ACE inhibitor are Ramistar,Envas, Ramace and Cardace,
ii) ACE inhibitor+diuretic are Ramce-H, Enapril-HT, Ramistar-H nd
Cardace-H
iii) ARB are Tozar, Telday, Losacar and Telma,
iv) ARB+diuretic are Enace-D, Telday-H, Covance-D and Telma-H
2) From the above chart it is clear that single drug in treatment of hypertension is
having the maximum priority in comparison to combination. Combinations are
mainly advised when mono-therapy with single drug is not sufficient to control
the blood pressure in individuals.
Q.4. Which is/are the fastest moving brand(s) of Candesartan and its combinations?
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 134
Inference:
1. The fastest moving brand is Candesar whose chemical entity is Candesartan
which is marketed by Ranbaxy.
2. From the above data acquired, it is quite clear that the base molecule does not
yet have a good market share but in comparison to Bangalore data it has a
higher market.
3. Some chemists are not aware of the brands and in maximum cases the
chemists did not have a stock of the products such as Candelong, Candesar,
Cantar and Candesar-H.
Conclusion: Candesartan has a very low visibility in the market. Only 4 brands are
available in which Candesar is the top moving brand. In comparison to Bangalore’s
survey, Candesartan has a slightly higher market, which means the doctors are
prescribing the drug.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 135
Final conclusion of Kolkata and Bangalore chemists:
With respect to the first question of the chemist questionnaire in Kolkata and
Bangalore the results shows that, prevalence of hypertension is more in Kolkata with
respect to Bangalore. In Bangalore the particular disease condition is fairly prevalent
in individuals.
The results for the second question in the chemist’s questionnaire showed that in
Kolkata Cardiologists are the maximum prescriber of anti-hypertensive medicines
followed by General physicians. With respect to Bangalore General physicians are the
maximum prescriber of antihypertensive medicines followed by the Cardiologists. So
in Kolkata and Bangalore the company should target more General physicians and
Cardiologists respectively to increase its customer base. Among General practitioners,
the trend of prescribing antihypertensive drugs are very less in Bangalore in
comparison to Kolkata. So targeting general practitioners is another primary focus of
the company to increase its customer base.
The chemist survey with respect to single drug therapy, the results showed that ACE
inhibitors got higher priority in comparison to ARBs in Bangalore market. In Kolkata
ARBs are having maximum sales in comparison to ACE inhibitors. After asking the
chemists verbally about the other categories of drug which are having the major sale
in market, it was found that Calcium channel blockers got a good response in the
market. The reason behind this may be the cheaper cost of the products in this
category or doctors are not willing to shift in newer categories of drug for the
treatment of hypertension.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 136
With respect to combination drugs ARB with Diuretic got the maximum preference
followed by ACE inhibitor with Diuretic in Bangalore and Kolkata both.
The results with respect to Candesartan is poor in both the cities. In Kolkata, the
molecule still has a better market in comparison to Bangalore. In Bangalore maximum
chemists did not have a stock only for this particular molecule
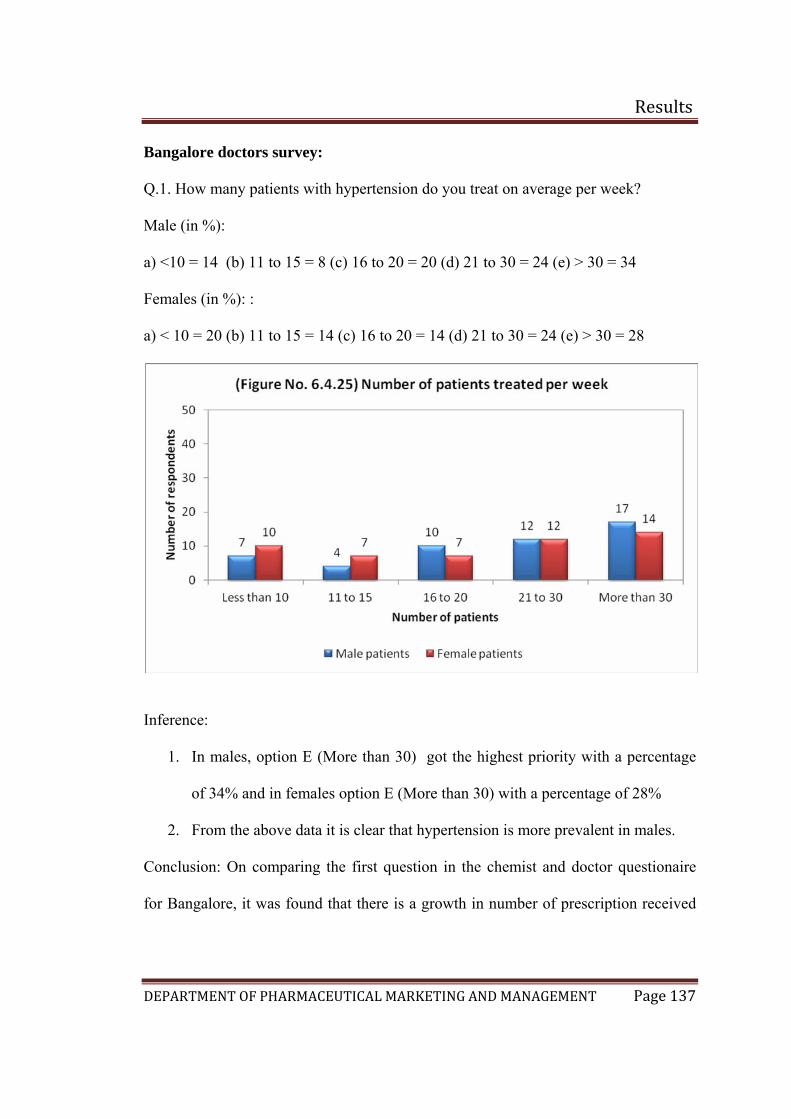
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 137
Bangalore doctors survey:
Q.1. How many patients with hypertension do you treat on average per week?
Male (in %):
a) <10 = 14 (b) 11 to 15 = 8 (c) 16 to 20 = 20 (d) 21 to 30 = 24 (e) > 30 = 34
Females (in %): :
a) < 10 = 20 (b) 11 to 15 = 14 (c) 16 to 20 = 14 (d) 21 to 30 = 24 (e) > 30 = 28
Inference:
1. In males, option E (More than 30) got the highest priority with a percentage
of 34% and in females option E (More than 30) with a percentage of 28%
2. From the above data it is clear that hypertension is more prevalent in males.
Conclusion: On comparing the first question in the chemist and doctor questionaire
for Bangalore, it was found that there is a growth in number of prescription received
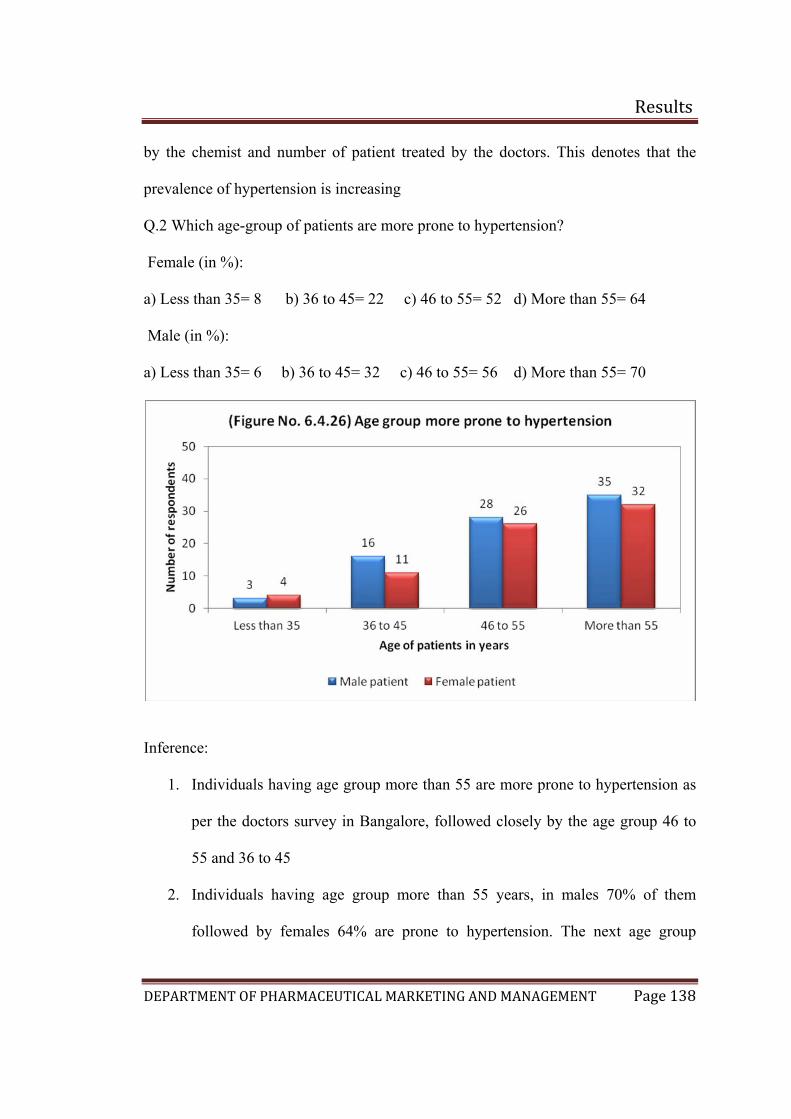
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 138
by the chemist and number of patient treated by the doctors. This denotes that the
prevalence of hypertension is increasing
Q.2 Which age-group of patients are more prone to hypertension?
Female (in %):
a) Less than 35= 8 b) 36 to 45= 22 c) 46 to 55= 52 d) More than 55= 64
Male (in %):
a) Less than 35= 6 b) 36 to 45= 32 c) 46 to 55= 56 d) More than 55= 70
Inference:
1. Individuals having age group more than 55 are more prone to hypertension as
per the doctors survey in Bangalore, followed closely by the age group 46 to
55 and 36 to 45
2. Individuals having age group more than 55 years, in males 70% of them
followed by females 64% are prone to hypertension. The next age group
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 139
which is prone to hypertension is 46 to 55 years where males got 56%
followed by females 52% .
3. From the data it was found that males again have the higher tendency to have
hypertension
Conclusion: The 2nd question reflects the age group which is more prone to
hypertension. The survey reports says that the age group more than 55 are most prone
to hypertension followed by the age group 46 to 55 years.
According to literature survey, the prevalence of hypertension increases with age
proportionally.(31 ) As per the survey in the age group between 36 to 45 years the
prevalence of hypertension is also growing in Bangalore. From this we can predict
that as there is a change in lifestyle now a days, the tendency of developing
hypertension is there in both genders .
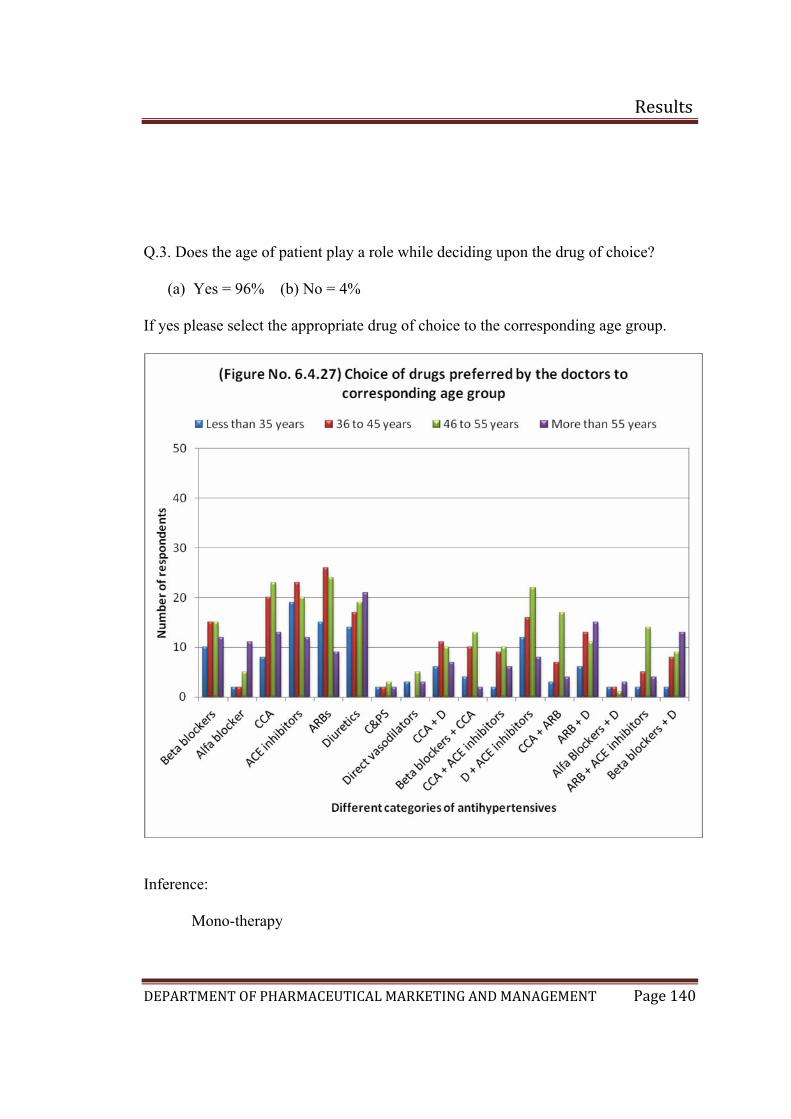
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 140
Q.3. Does the age of patient play a role while deciding upon the drug of choice?
(a) Yes = 96% (b) No = 4%
If yes please select the appropriate drug of choice to the corresponding age group.
Inference:
Mono-therapy
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 141
1. From the above data it was found that, for single drug therapy age group less
than 35 years ACE inhibitors followed by ARBs and diuretics are preferred.
2. For the age group 36 to 45 years, ARB’s got the highest preference followed
by ACE inhibitors and Calcium channel antagonist.
3. For the next age group that is 46 to 55 years, ARBs followed by Beta blockers
and Calcium channel antagonists got the higher preferences.
4. Coming to the last age group that is above 55 years Diuretics got the highest
preference followed by Calcium channel antagonist in Bangalore.
Combination therapy
5. With respect to the combination therapy, CCA with ACE inhibitors, CCA with
Diuretic, Beta blockers with CCA, ACE inhibitors with Diuretic, ARB with
CCA, ARB with Diuretic, ARBs with ACE inhibitors and Beta blockers with
Diuretics are being used in all corresponding age groups for treating
hypertension.
6. In age group less than 35 years, ACE inhibitors with Diuretics are preferred
followed by CCA and Diuretics are preferred.
7. For the age group 36 to 45 years, ACE inhibitors with Diuretic got the highest
preference followed by ARB with diuretic
8. For the age group 46 to 55 years, the same ACE inhibitors with Diuretic got
the highest preference followed by CCA with ARB and ACE inhibitor with
ARB.
9. The drug preferences for the last age group which is above 55 years is ARB
with Diuretic followed by Beta blocker with Diuretic
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 142
Conclusion:
• Single drug therapy has got the first preference in the treatment of
hypertension. Combination therapy is used when single drug treatment is not
sufficient in maintaining the blood pressure in individuals.
• Within the categories of drugs such as beta blockers, Calcium channel
blockers, Alfa blockers, Calcium channel blockers still have major preferences
in the treatment of hypertension.
ACE inhibitors are preferred by the doctors as well. According to literature
survey the most commonly prescribed drug categories are Calcium channel
blockers and ACE inhibitors.(32)
• With respect to combination therapy, ACE inhibitor with Diuretic and ARB
with Diuretic has got major preferences.
• The preference of using ARB’s in the treatment of hypertension is also good
and is increasing. As per literature survey hypertension is directly responsible
for 57% of all stroke deaths and 42% of coronary heart disease death in
India.(31) So there will be a demand of drugs which serve both the conditions
such as hypertension and heart attacks. Candesartan cilexetil with
hydrochlorothiazide is the only ARB approved by US FDA for the treatment
of hypertension and heart attack.
• Comparing with the chemist survey report, ACE inhibitors are having higher
preference than ARB’s matches the report of doctor’s preference.

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 143
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 144
Inference:
1. The top 5 brands in the market which has the maximum priority in the market
are Cardace, Envas, Ramace, Ramistar and Rampres in which Cardace got
the highest number of preferences
2. Calculating the percentage 92% of doctors ticked Cardace, followed by Envas
62%, Ramace 58%, Ramistar 54%, and Ramipres 46%
3. The chemical entity in Cardace is Ramipril which is marketed by Sanofi
Aventis followed by Envas whose chemical entity is enalapril maleate
marketed by Zydus cadilla.
4. Captopril was the first agent to be developed for the treatment of hypertension.
Since then, enalapril, lisinopril, quinapril, ramipril, benazepril, moexipril are
also available in market.
5. From the survey carried out in Bangalore, Ramipril is the top molecule sold in
market followed by Enalapril as per the doctors.
6. As per the survey among both doctors and chemists, Cardace got 92% of
preference which made it a top moving brand of ACE inhibitor

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 145
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 146
Inference:
1. The top 5 brands in the market was found to be Telma followed by Losacar,
Tozaar, Convance and Arbitel.
2. Calculating in percentage, 60% of the doctors ticked Telma, followed by
Losacar 58%, Tozaar 54%, Covance 38% and Arbitel 34%.
3. Telma whose chemical entity is Telmisartan is marketed by Glenmark
followed by Losacar whose chemical entity is Losartan potassium of Zydus
Cadilla.
4. The importance of angiotensin II in regulating cardiovascular function has led
to the development of nonpeptide antagonists of the AT1 angiotensin II
receptor for clinical use. Losartan, candesartan, irbesartan, valsartan ,
telmisartan, and eprosartan have been approved for the treatment of
hypertension and are available in market.
5. The survey carried out in Bangalore for the doctors showed that Telmisartan is
the top molecule sold in market followed by Losartan.
6. As per the survey of doctors and chemists conducted, Telmisartan got 60%
and 84% of preference respectively which made it a top moving brand of
ARB.
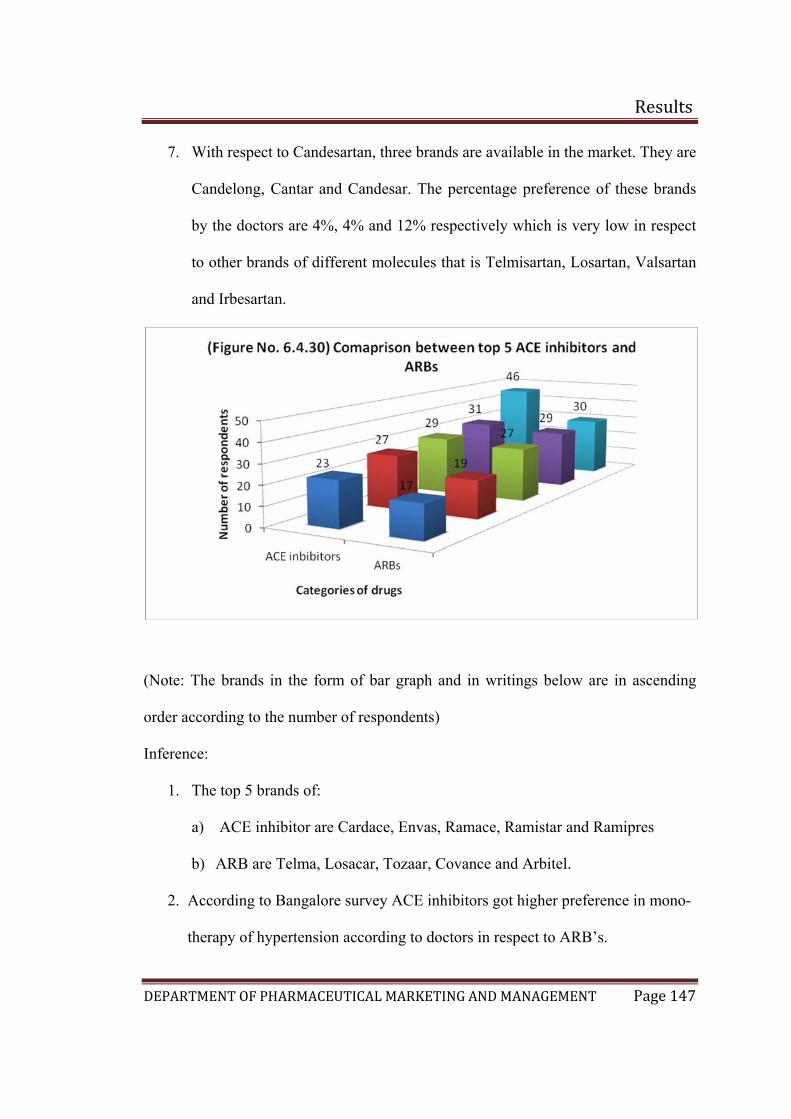
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 147
7. With respect to Candesartan, three brands are available in the market. They are
Candelong, Cantar and Candesar. The percentage preference of these brands
by the doctors are 4%, 4% and 12% respectively which is very low in respect
to other brands of different molecules that is Telmisartan, Losartan, Valsartan
and Irbesartan.
(Note: The brands in the form of bar graph and in writings below are in ascending
order according to the number of respondents)
Inference:
1. The top 5 brands of:
a) ACE inhibitor are Cardace, Envas, Ramace, Ramistar and Ramipres
b) ARB are Telma, Losacar, Tozaar, Covance and Arbitel.
2. According to Bangalore survey ACE inhibitors got higher preference in mono-
therapy of hypertension according to doctors in respect to ARB’s.
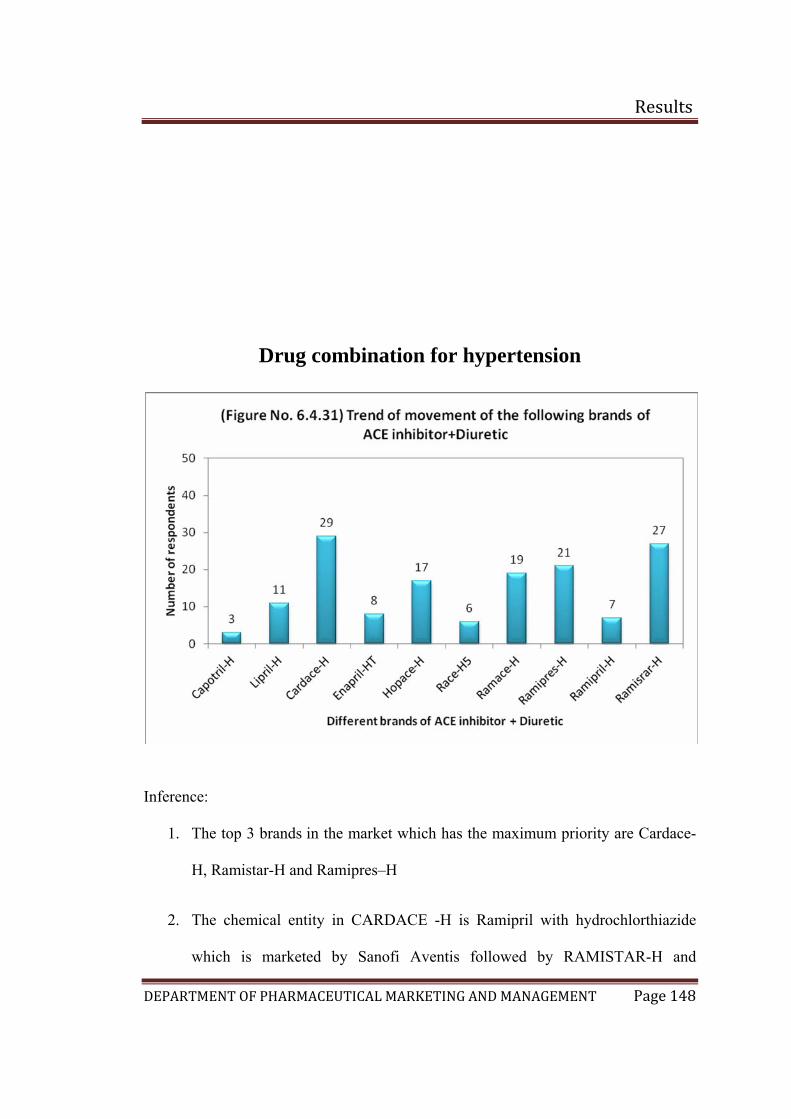
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 148
Drug combination for hypertension
Inference:
1. The top 3 brands in the market which has the maximum priority are Cardace-
H, Ramistar-H and Ramipres–H
2. The chemical entity in CARDACE -H is Ramipril with hydrochlorthiazide
which is marketed by Sanofi Aventis followed by RAMISTAR-H and
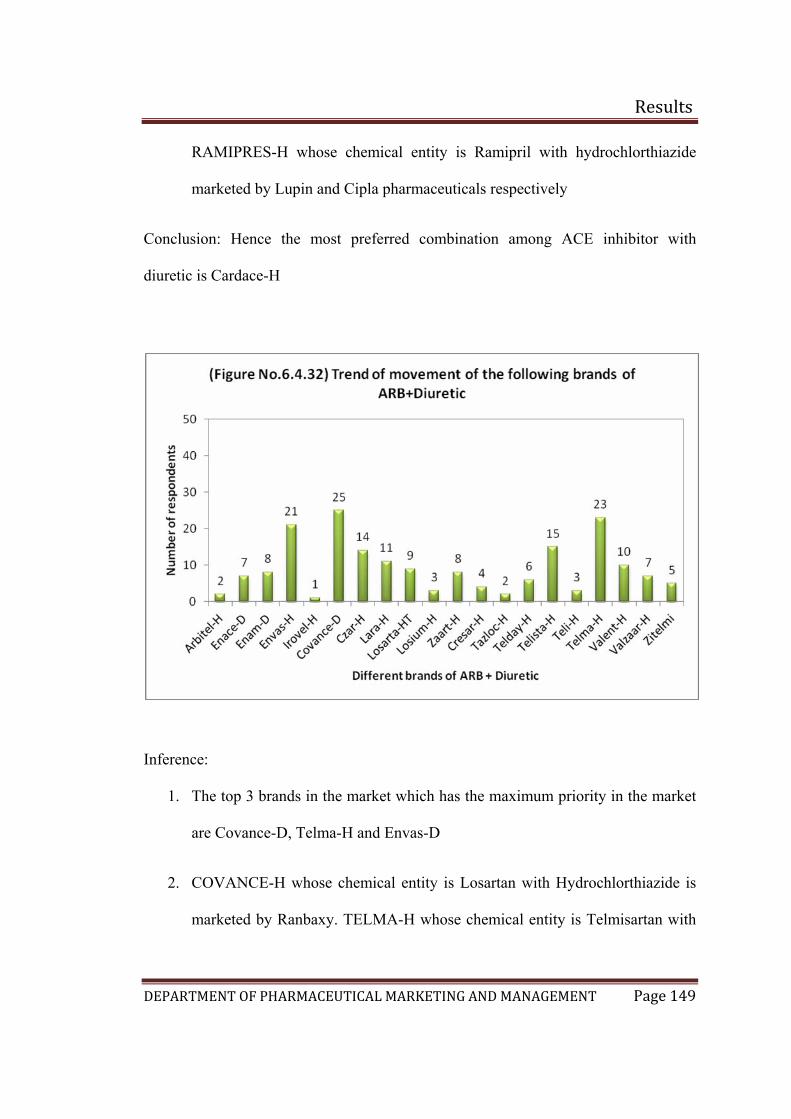
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 149
RAMIPRES-H whose chemical entity is Ramipril with hydrochlorthiazide
marketed by Lupin and Cipla pharmaceuticals respectively
Conclusion: Hence the most preferred combination among ACE inhibitor with
diuretic is Cardace-H
Inference:
1. The top 3 brands in the market which has the maximum priority in the market
are Covance-D, Telma-H and Envas-D
2. COVANCE-H whose chemical entity is Losartan with Hydrochlorthiazide is
marketed by Ranbaxy. TELMA-H whose chemical entity is Telmisartan with
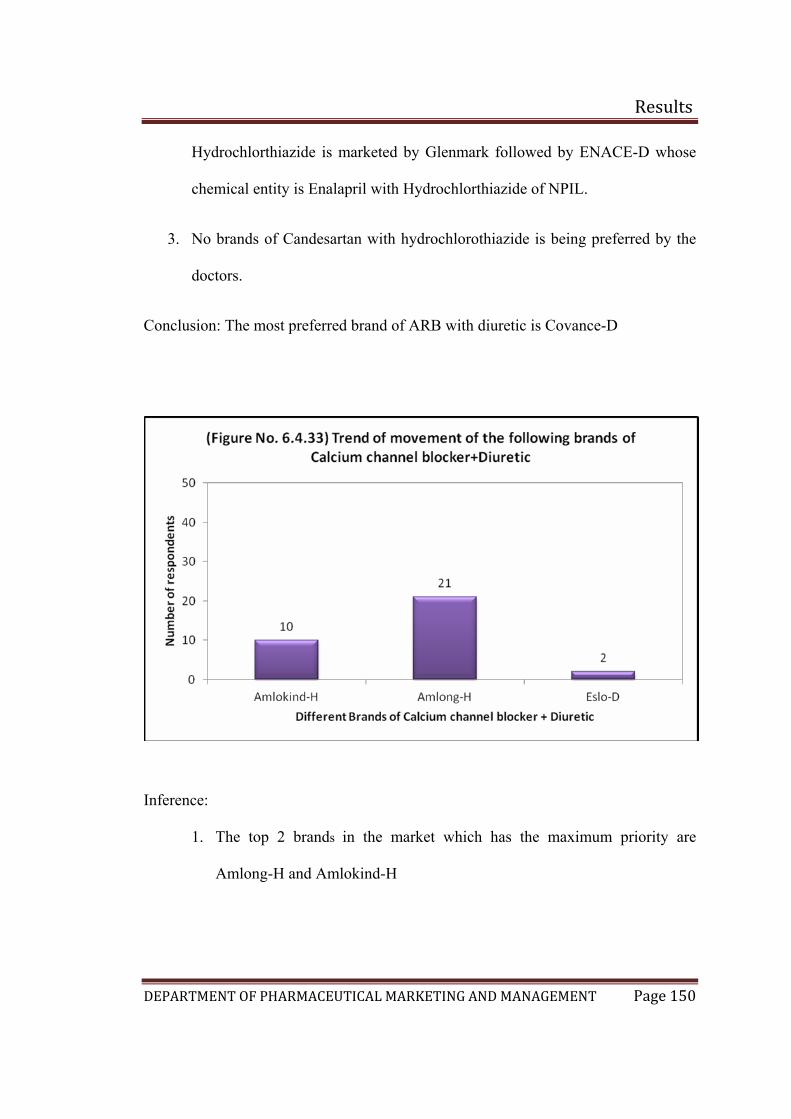
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 150
Hydrochlorthiazide is marketed by Glenmark followed by ENACE-D whose
chemical entity is Enalapril with Hydrochlorthiazide of NPIL.
3. No brands of Candesartan with hydrochlorothiazide is being preferred by the
doctors.
Conclusion: The most preferred brand of ARB with diuretic is Covance-D
Inference:
1. The top 2 brands in the market which has the maximum priority are
Amlong-H and Amlokind-H
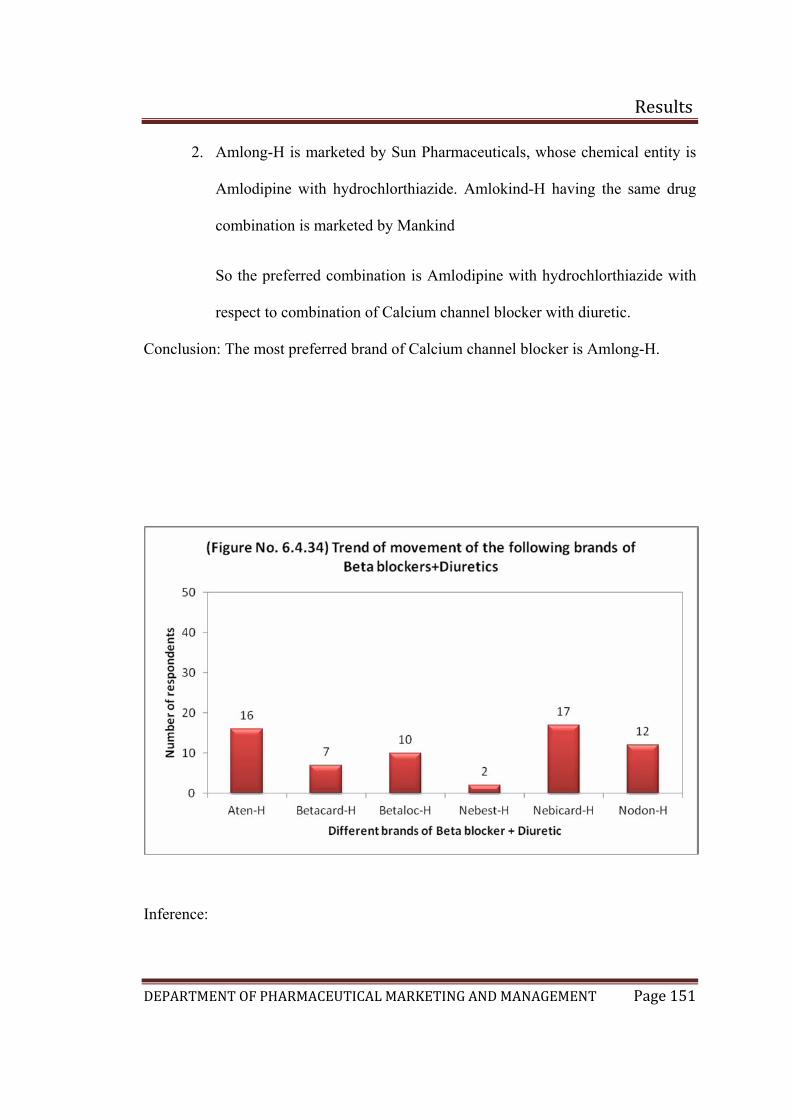
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 151
2. Amlong-H is marketed by Sun Pharmaceuticals, whose chemical entity is
Amlodipine with hydrochlorthiazide. Amlokind-H having the same drug
combination is marketed by Mankind
So the preferred combination is Amlodipine with hydrochlorthiazide with
respect to combination of Calcium channel blocker with diuretic.
Conclusion: The most preferred brand of Calcium channel blocker is Amlong-H.
Inference:
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 152
1. The top 3 brand in the market which has the maximum priority are Nebicard-
H, Aten-H, and Nodon-H
2. Nebivolol with hydrochlorthiazide is marketed by Torrent pharma and Aten-
H is marketed by Asjanta pharma whose chemical entity is Atenolol with
hydrochlorthiazide followed by Nodon-H which is marketed by Cadilla.
Conclusion: Nebicard-H has got the highest preference in doctors
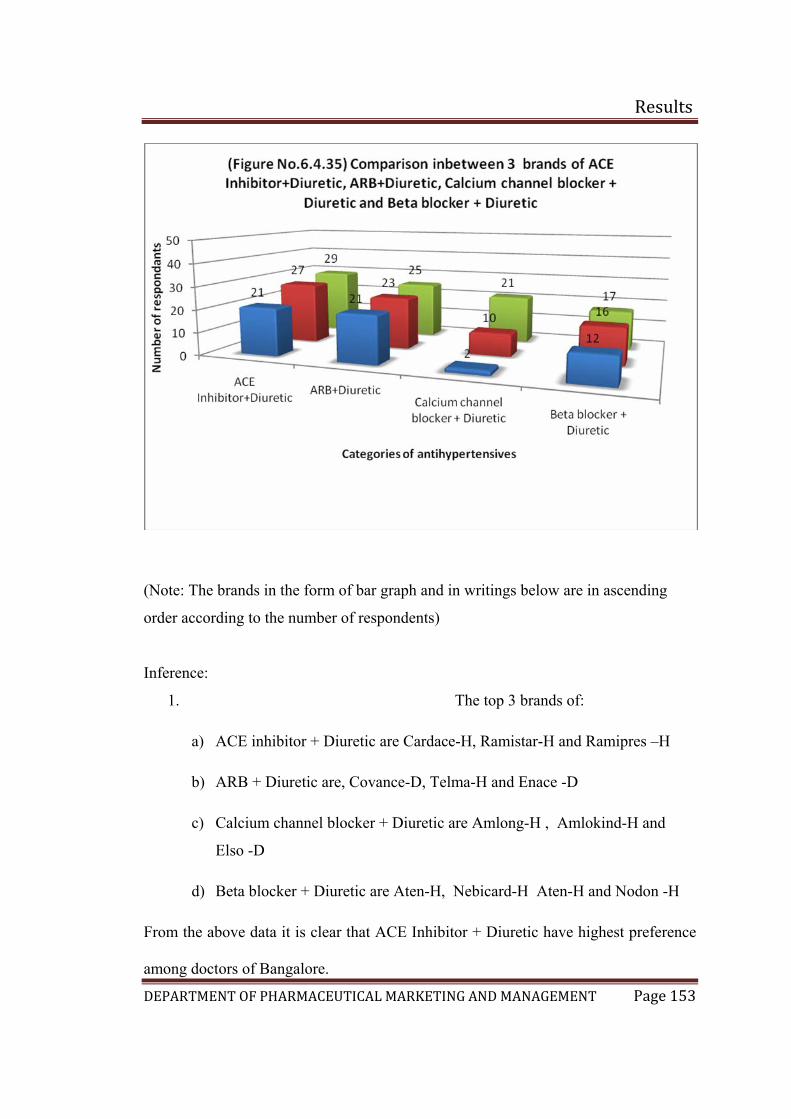
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 153
(Note: The brands in the form of bar graph and in writings below are in ascending
order according to the number of respondents)
Inference:
1. The top 3 brands of:
a) ACE inhibitor + Diuretic are Cardace-H, Ramistar-H and Ramipres –H
b) ARB + Diuretic are, Covance-D, Telma-H and Enace -D
c) Calcium channel blocker + Diuretic are Amlong-H , Amlokind-H and
Elso -D
d) Beta blocker + Diuretic are Aten-H, Nebicard-H Aten-H and Nodon -H
From the above data it is clear that ACE Inhibitor + Diuretic have highest preference
among doctors of Bangalore.
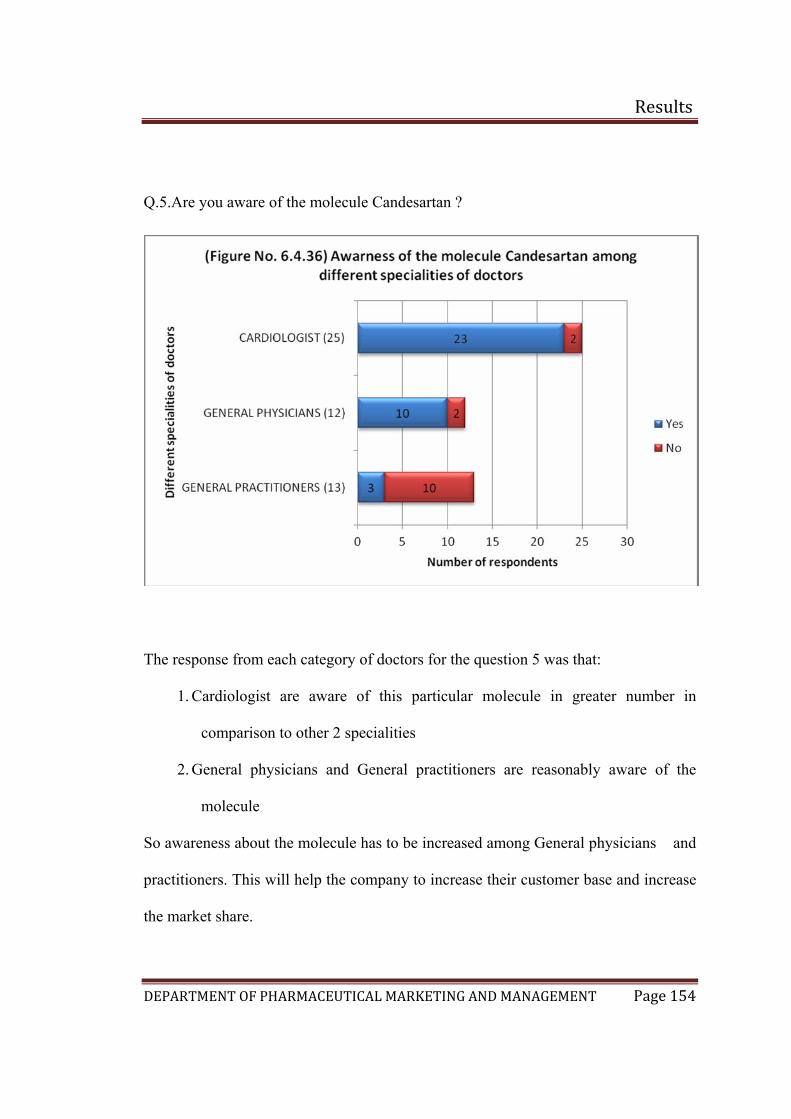
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 154
Q.5.Are you aware of the molecule Candesartan ?
The response from each category of doctors for the question 5 was that:
1. Cardiologist are aware of this particular molecule in greater number in
comparison to other 2 specialities
2. General physicians and General practitioners are reasonably aware of the
molecule
So awareness about the molecule has to be increased among General physicians and
practitioners. This will help the company to increase their customer base and increase
the market share.
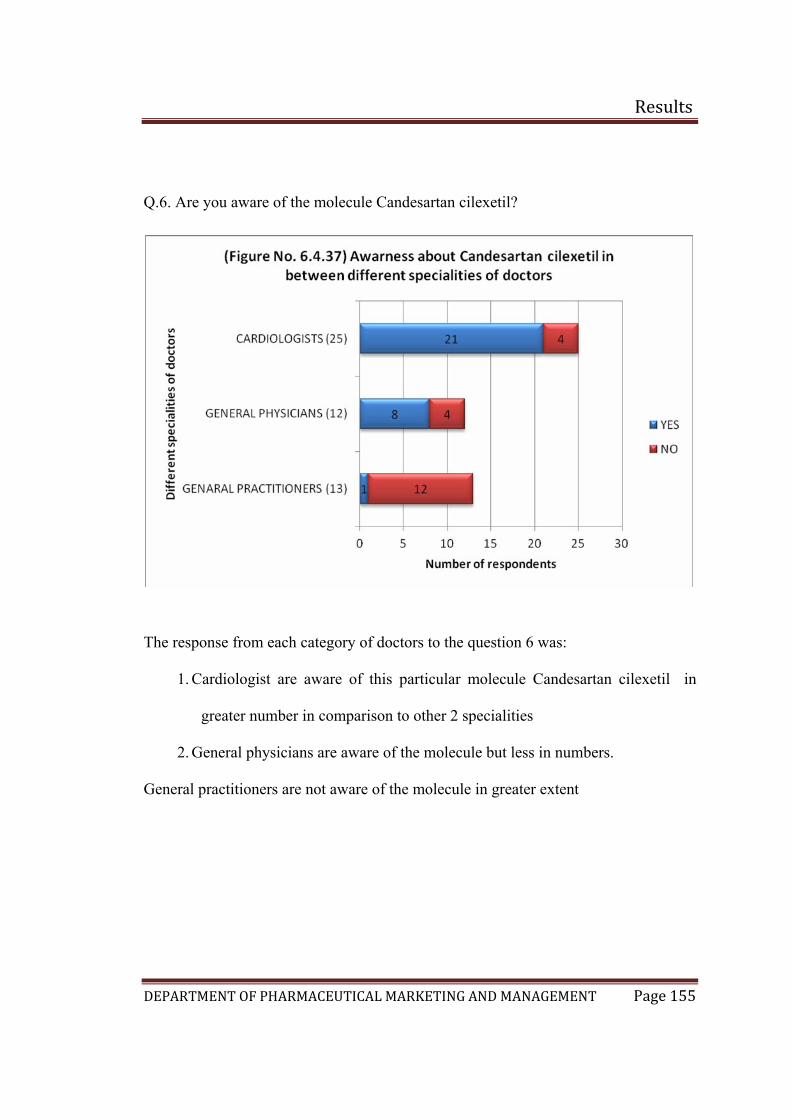
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 155
Q.6. Are you aware of the molecule Candesartan cilexetil?
The response from each category of doctors to the question 6 was:
1. Cardiologist are aware of this particular molecule Candesartan cilexetil in
greater number in comparison to other 2 specialities
2. General physicians are aware of the molecule but less in numbers.
General practitioners are not aware of the molecule in greater extent
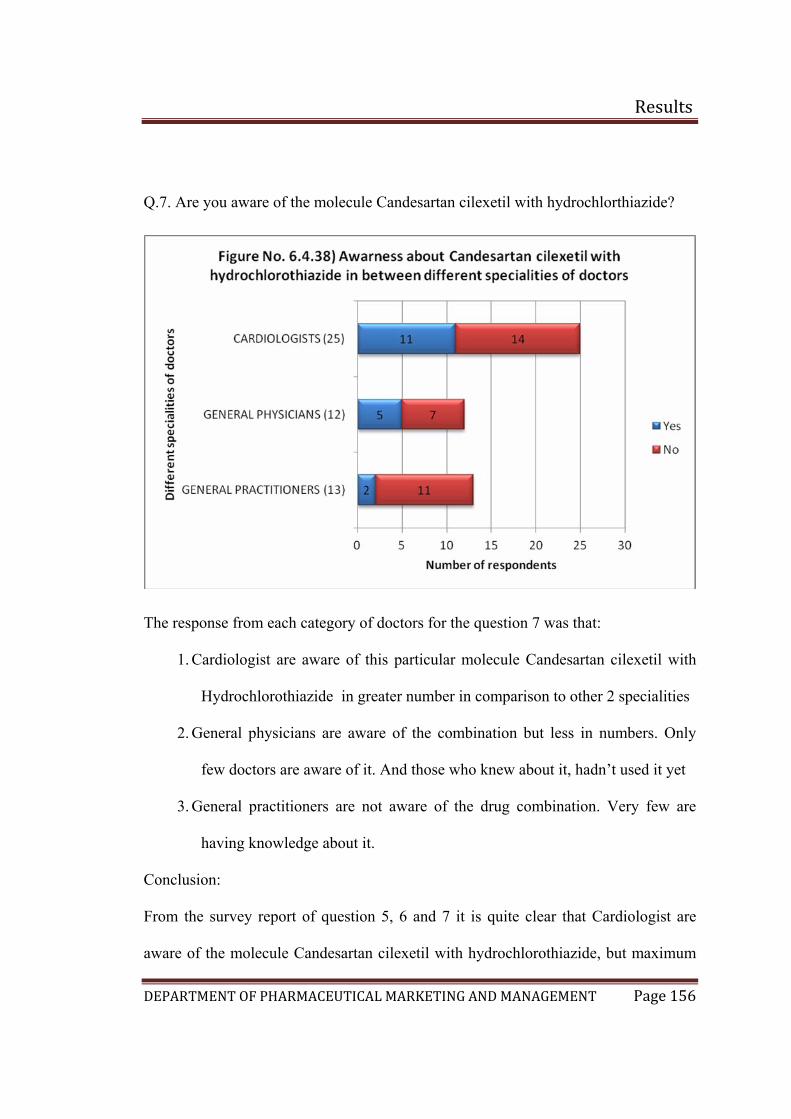
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 156
Q.7. Are you aware of the molecule Candesartan cilexetil with hydrochlorthiazide?
The response from each category of doctors for the question 7 was that:
1. Cardiologist are aware of this particular molecule Candesartan cilexetil with
Hydrochlorothiazide in greater number in comparison to other 2 specialities
2. General physicians are aware of the combination but less in numbers. Only
few doctors are aware of it. And those who knew about it, hadn’t used it yet
3. General practitioners are not aware of the drug combination. Very few are
having knowledge about it.
Conclusion:
From the survey report of question 5, 6 and 7 it is quite clear that Cardiologist are
aware of the molecule Candesartan cilexetil with hydrochlorothiazide, but maximum
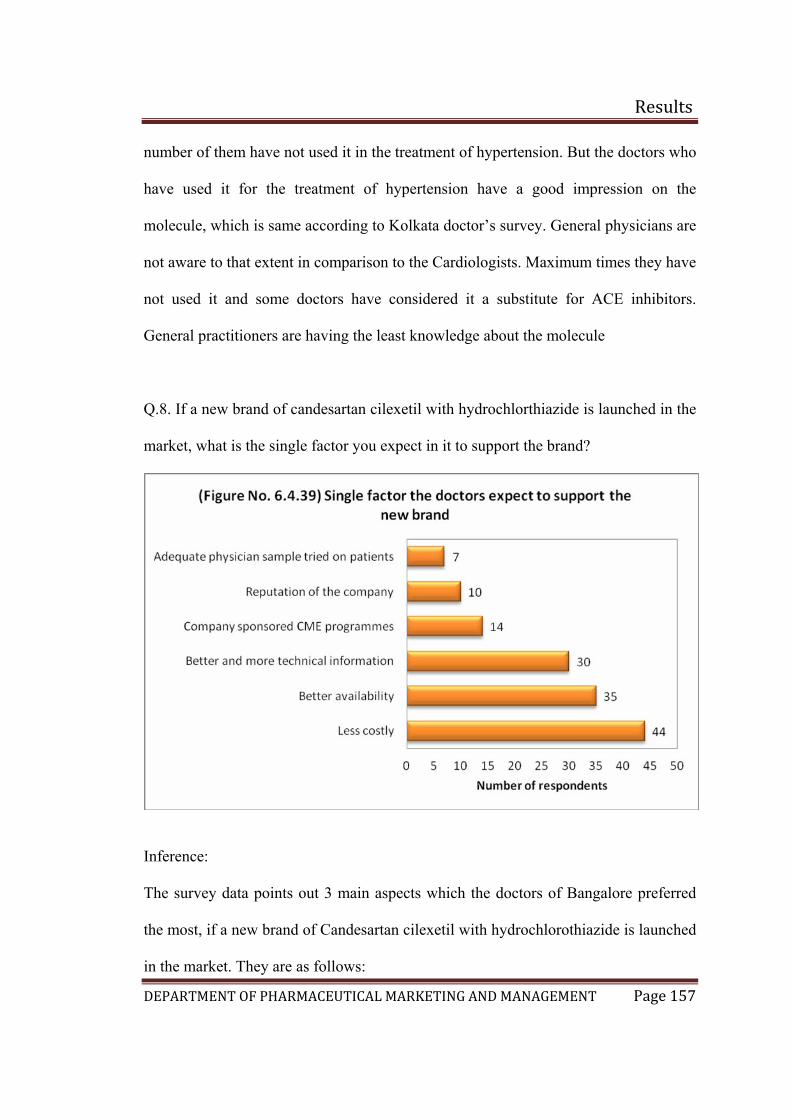
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 157
nched in the
arket, what is the single factor you expect in it to support the brand?
number of them have not used it in the treatment of hypertension. But the doctors who
have used it for the treatment of hypertension have a good impression on the
molecule, which is same according to Kolkata doctor’s survey. General physicians are
not aware to that extent in comparison to the Cardiologists. Maximum times they have
not used it and some doctors have considered it a substitute for ACE inhibitors.
General practitioners are having the least knowledge about the molecule
Q.8. If a new brand of candesartan cilexetil with hydrochlorthiazide is lau
m
Inference:
he survey data points out 3 main aspects which the doctors of Bangalore preferred
f a new brand of Candesartan cilexetil with hydrochlorothiazide is launched
in the market. They are as follows:
T
the most, i
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 158
.
Conclu
To the the questionaire for Bangalore doctors the results indicate the
me as for that in Kolkata. Doctors gave first preference to the cost of the drug which
w followed by better availability of the drug and better technical
1. The product should be less costly as maximum number of doctors ticked
option “a”. Calculating the percentage, 88% of doctors wants the brand to be
less costly.
2. The next highest preference goes to option “c”. Calculating the percentage
70% of doctors preferred it. So the doctors want that the drug to be available
in maximum
3. The third preference goes to option “e”. The doctors want more and better
technical information about the molecule. Around 60% of doctors gave their
opinion for it.
sion:
last question in
sa
should be lo
information should be provided by the company. Continuous Medical Education is
also a preferred option ticked by the doctors which the company has to consider and
develop the strategies.
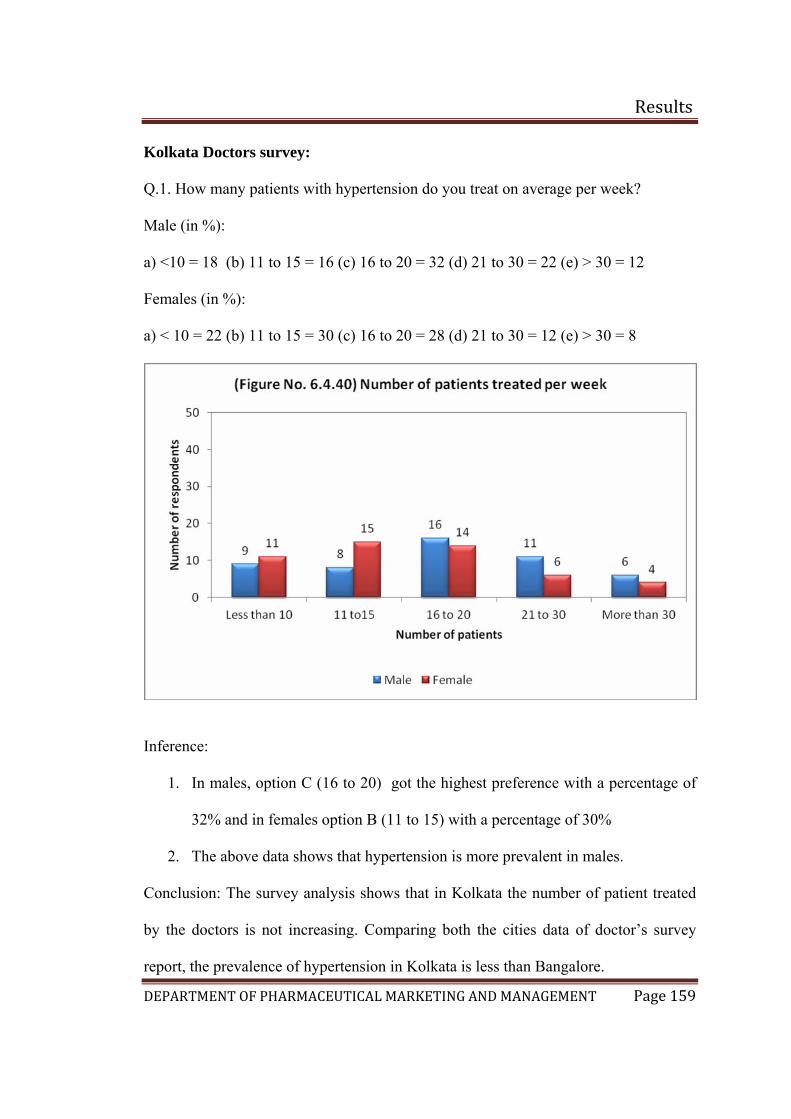
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 159
olkata Doctors survey:
on do you treat on average per week?
Male (in %):
16 (c) 16 to 20 = 32 (d) 21 to 30 = 22 (e) > 30 = 12
) 11 to 15 = 30 (c) 16 to 20 = 28 (d) 21 to 30 = 12 (e) > 30 = 8
K
Q.1. How many patients with hypertensi
a) <10 = 18 (b) 11 to 15 =
Females (in %):
a) < 10 = 22 (b
Inference:
1. In males, option C (16 to 20) got the highest preference with a percentage of
32% and in females option B (11 to 15) with a percentage of 30%
above data shows that hypertension is more prevalent in males.
Con
by the tor’s survey
rep
2. The
clusion: The survey analysis shows that in Kolkata the number of patient treated
doctors is not increasing. Comparing both the cities data of doc
ort, the prevalence of hypertension in Kolkata is less than Bangalore.
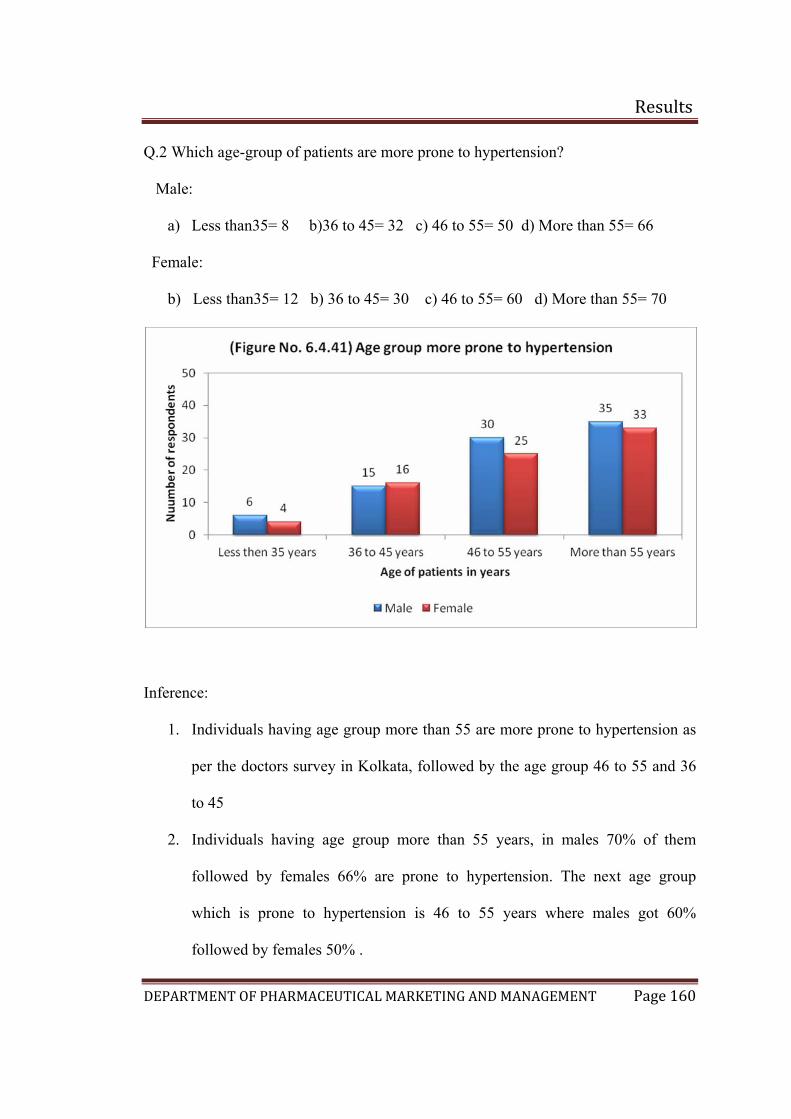
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 160
5= 66
ess than35= 12 b) 36 to 45= 30 c) 46 to 55= 60 d) More than 55= 70
Q.2 Which age-group of patients are more prone to hypertension?
Male:
a) Less than35= 8 b)36 to 45= 32 c) 46 to 55= 50 d) More than 5
Female:
b) L
Inference:
1. Individuals having age group more than 55 are more prone to hypertension as
per the doctors survey in Kolkata, followed by the age group 46 to 55 and 36
5
is prone to hypertension is 46 to 55 years where males got 60%
followed by females 50% .
to 4
2. Individuals having age group more than 55 years, in males 70% of them
followed by females 66% are prone to hypertension. The next age group
which
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 161
Conclu
hypertension. The survey reports say that the age group more than 55 are most prone
to
Bangalore doctors survey report with Kolkata the results are found to be same. In both
3. From the data it was found that males again have a higher tendency to have
hypertension
sion: The 2nd question reflects the age group which is more prone to
hypertension followed by the age group 46 to 55 years. Comparing with the
the places the prevalence of hypertension increases with age proportionally.
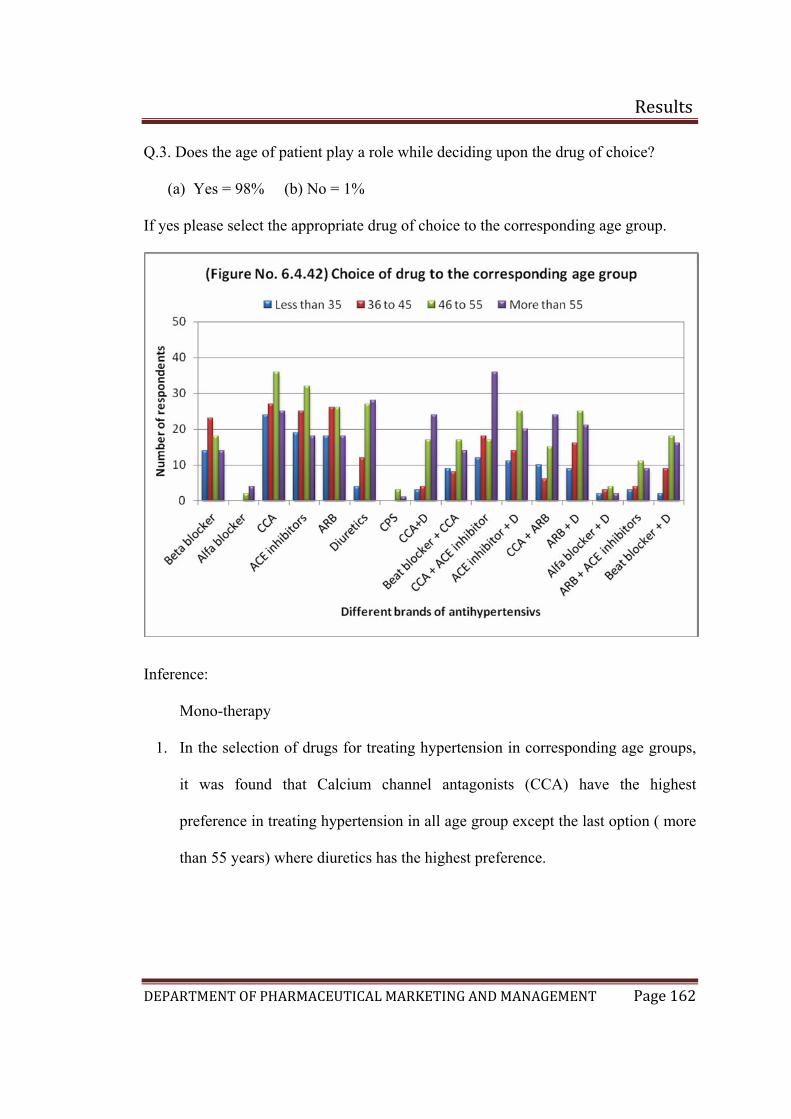
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 162
.3. Does the age of patient play a role while deciding upon the drug of choice?
(a) Yes = 98% (b) No = 1%
yes please select the appropriate drug of choice to the corresponding age group.
Q
If
Inference:
Mono-therapy
1. In the selection of drugs for treating hypertension in corresponding age groups,
it was found that Calcium channel antagonists (CCA) have the highest
nce in treating hypertension in all age group except the last option ( more
here diuretics has the highest preference.
prefere
than 55 years) w
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 163
2. itors, ACE inhibitors
ith Diuretic, ARB with CCA and ARB with Diuretic is being used in all
ifferent age groups for treating hypertension.
3. CA with ACE inhibitors are used in maximum in age group more than 55
with ARB.
uretic
Conc
Combination therapy:
Coming to the combination therapy, CCA with ACE inhib
w
d
C
years, followed by CCA
4. For the age group 46 to 55 years both ARB with Diuretic and ACE inhibitor
with Diuretic has the same preference followed by CCA with ACE inhibitors
and CCA with Diuretic.
5. In the age group of 35 to 45 years, CCA with ACE inhibitors has got the highest
preference followed by ARB with Di
6. Finally the age group less than 35 years, CCA with ACE inhibitors has got the
higher preference followed by ACE inhibitors with Diuretic.
lusion:
•
when single drug treatment is not
The doctors of Kolkata also preferred the single drug therapy for hypertension.
They use to shift to combination therapy
sufficient in maintaining the blood pressure. The same result is seen with
respect to Bangalore doctor’s survey.
• The major categories of drug in the treatment of hypertension in single drug
therapy are Calcium channel antagonist and Diuretic followed by ACE
inhibitors and ARBs. In combination therapy, Calcium channel antagonist
with ACE inhibitor, ACE inhibitor with Diuretic and ARB with Diuretic has
got the maximum preferences.

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 164
With respect to Bangalore doctor’s survey report, Calcium channel antagonist
got the major preference in both the cities in single drug therapy. Diuretics are
mainly used for higher age groups according to literatures and it was found to
be the same according to primary survey in Kolkata and Bangalore.

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 165
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 166
ference:
1. The top 6 brands in the market which has the maximum presence in the market
are Cardace, Ramace, Ramistar, Envas, Cardiopril and Ramipres in which
Cardace got the highest number of preferences
2. Calculating the percentage 96% of doctors ticked Cardace, followed by
Ramace 80%, Ramistar 70%, Envas 66%, Cardiopril 60% and Ramipres 50%
3. The chemical entity in Cardace is Ramipril which is marketed by Sanofi
Aventis followed by Ramace whose chemical entity is Ramipril marketed by
Astra Zeneca.
Captopril was the first agent to be developed for the treatment of hypertension.
Since then, enalapril, lisinopril, quinapril, ramipril, benazepril, moexipril are
also available in market. From the survey result obtained in Kolkata shows
that, Ramipril is the top molecule sold in market as per 50 doctors followed by
Enalapril
In

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 167
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 168
ference:
1. The top 5 brands in the market was found to be Telma followed by Losacar,
Telista, Covance, Tozaar and Telday
2. Calculating in percentage, 92% of the doctors ticked Telma, followed by
Losacar and Telista 80% which has the equal number of respondants, Covance
62%, Tozaar 66% and Telday 52%
3. Telma whose chemical entity is Telmisartan is marketed by Glenmark
followed by Losacar whose chemical entity is Losartan potassium of Zydus
Cadilla and Telista whose chemical entity is once again Telmisartan of Lupin
4. The importance of angiotensin II in regulating cardiovascular function has led
to the development of nonpeptide antagonists of the AT1 angiotensin II
receptor blocker for clinical use. Losartan, Candesartan, Irbesartan, Valsartan ,
Velmisartan, and Eprosartan have been approved for the treatment of
hypertension and are available in market.
The survey carried out in Kolkata for the 50 doctors indicated that Telmisartan
is the top molecule sold in market followed by Losartan.
In
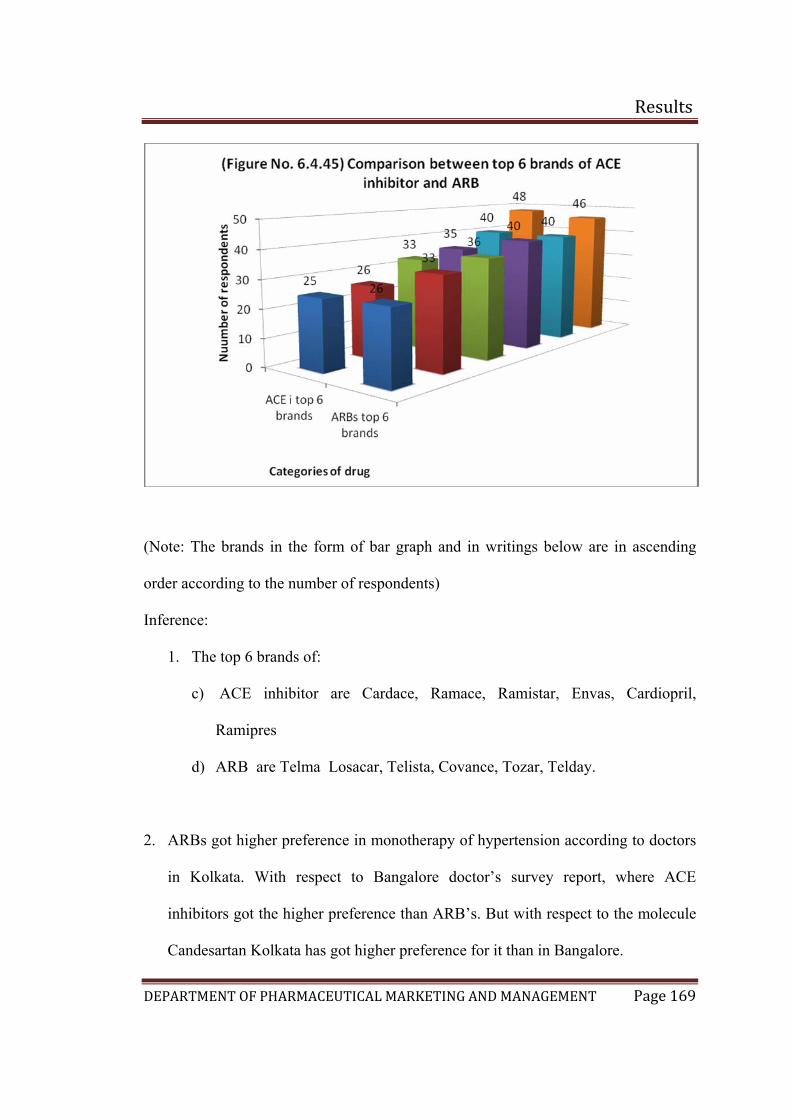
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 169
(Note: The brands in the form of bar graph and in writings below are in ascending
order according to the number of respondents)
Inference:
1. The top 6 brands of:
c) ACE inhibitor are Cardace, Ramace, Ramistar, Envas, Cardiopril,
Ramipres
d) ARB are Telma Losacar, Telista, Covance, Tozar, Telday.
2. ARBs got higher preference in monotherapy of hypertension according to doctors
in Kolkata. With respect to Bangalore doctor’s survey report, where ACE
inhibitors got the higher preference than ARB’s. But with respect to the molecule
Candesartan Kolkata has got higher preference for it than in Bangalore.
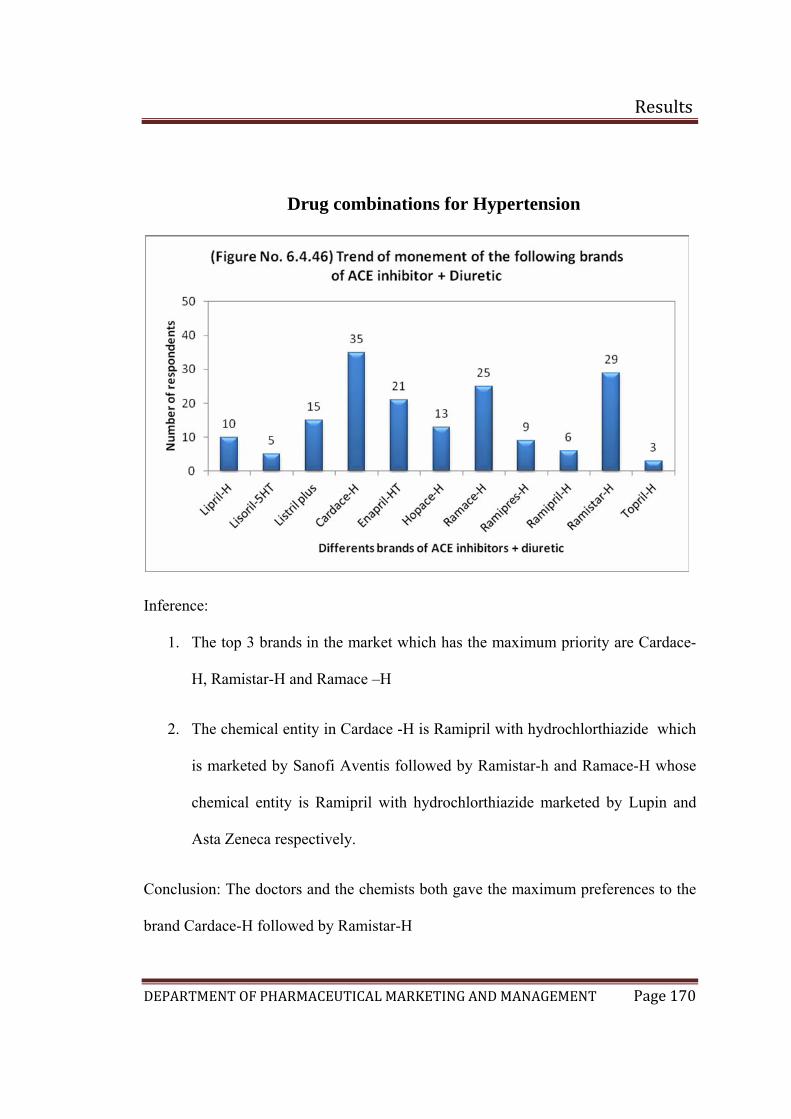
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 170
Drug combinations for Hypertension
Inference:
1. The top 3 brands in the market which has the maximum priority are Cardace-
H, Ramistar-H and Ramace –H
2. The chemical entity in Cardace -H is Ramipril with hydrochlorthiazide which
is marketed by Sanofi Aventis followed by Ramistar-h and Ramace-H whose
ical entity is Ramipril with hydrochlorthiazide marketed by Lupin and
Conclusion: The doctors and the chemists both gave the maximum preferences to the
brand Cardace-H followed by Ram
chem
Asta Zeneca respectively.
istar-H
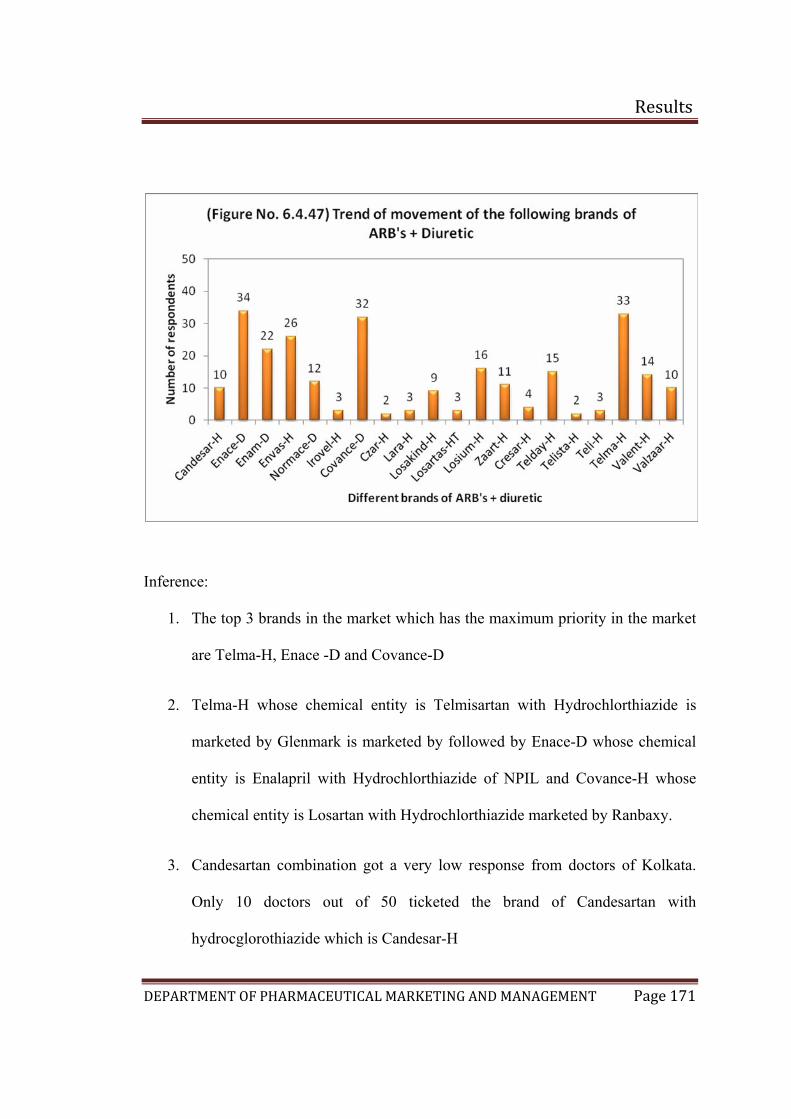
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 171
Inference:
1. The top 3 brands in the market which has the maximum priority in the market
are Telma-H, Enace -D and Covance-D
2. Telma-H whose chemical entity is Telmisartan with Hydrochlorthiazide is
marketed by Glenmark is marketed by followed by Enace-D whose chemical
iazide of NPIL and Covance-H whose
3. w response from doctors of Kolkata.
entity is Enalapril with Hydrochlorth
chemical entity is Losartan with Hydrochlorthiazide marketed by Ranbaxy.
Candesartan combination got a very lo
Only 10 doctors out of 50 ticketed the brand of Candesartan with
hydrocglorothiazide which is Candesar-H
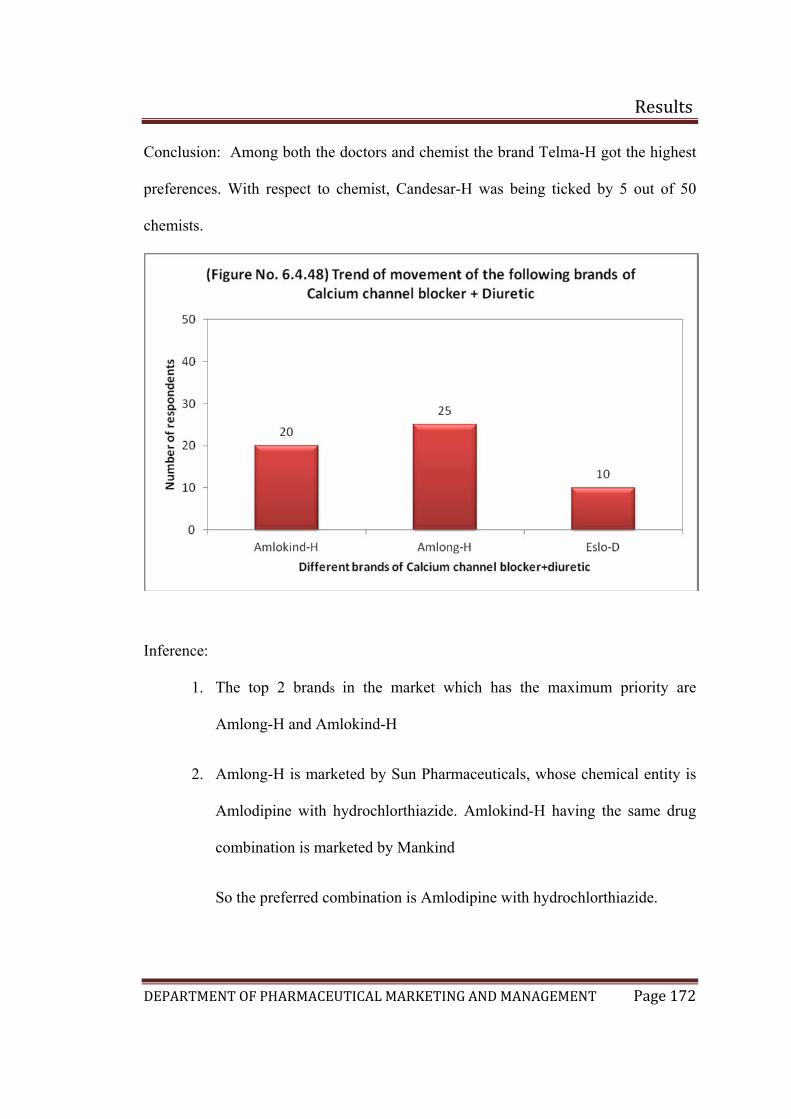
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 172
Conclu
prefere 50
chem
sion: Among both the doctors and chemist the brand Telma-H got the highest
nces. With respect to chemist, Candesar-H was being ticked by 5 out of
ists.
Inference:
1. The top 2 brands in the market which has the maximum priority are
Amlong-H and Amlokind-H
2. Amlong-H is marketed by Sun Pharmaceuticals, whose chemical entity is
Amlodipine with hydrochlorthiazide. Amlokind-H having the same drug
combination is marketed by Mankind
So the preferred combination is Amlodipine with hydrochlorthiazide.
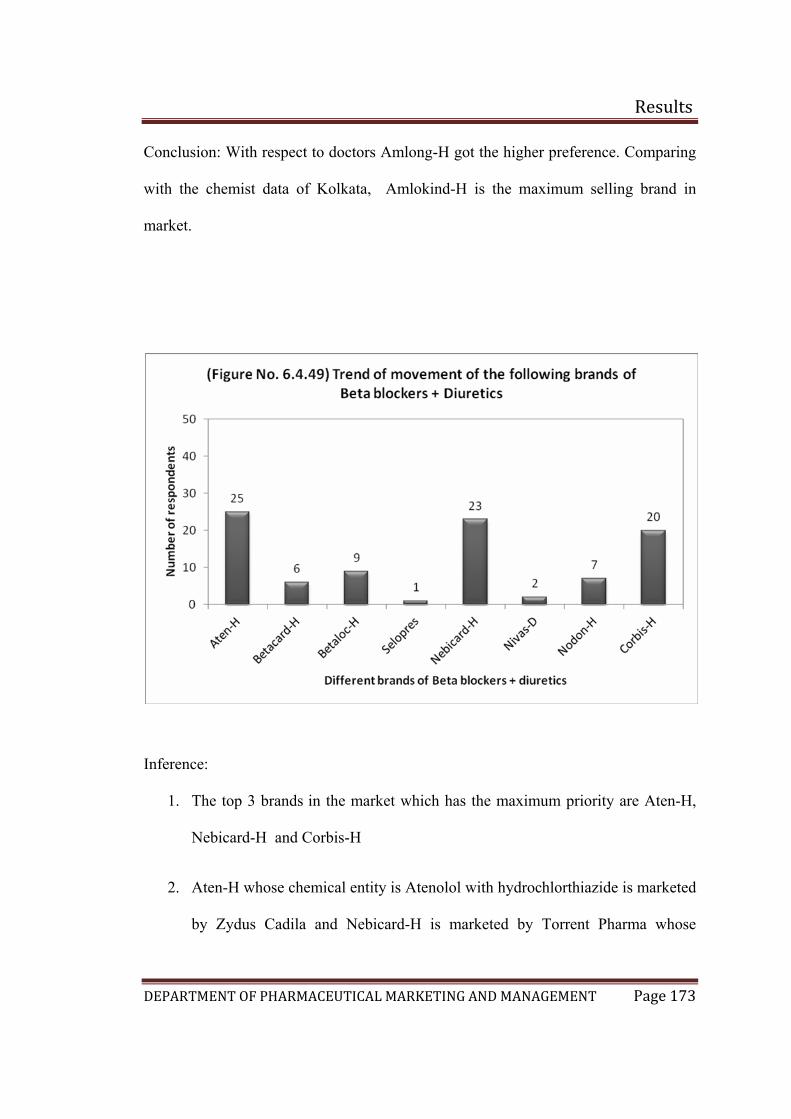
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 173
Conclu
with the c
market.
sion: With respect to doctors Amlong-H got the higher preference. Comparing
hemist data of Kolkata, Amlokind-H is the maximum selling brand in
Inference:
1. The top 3 brands in the market which has the maximum priority are Aten-H,
Nebicard-H and Corbis-H
2. Aten-H whose chemical entity is Atenolol with hydrochlorthiazide is marketed
by Zydus Cadila and Nebicard-H is marketed by Torrent Pharma whose
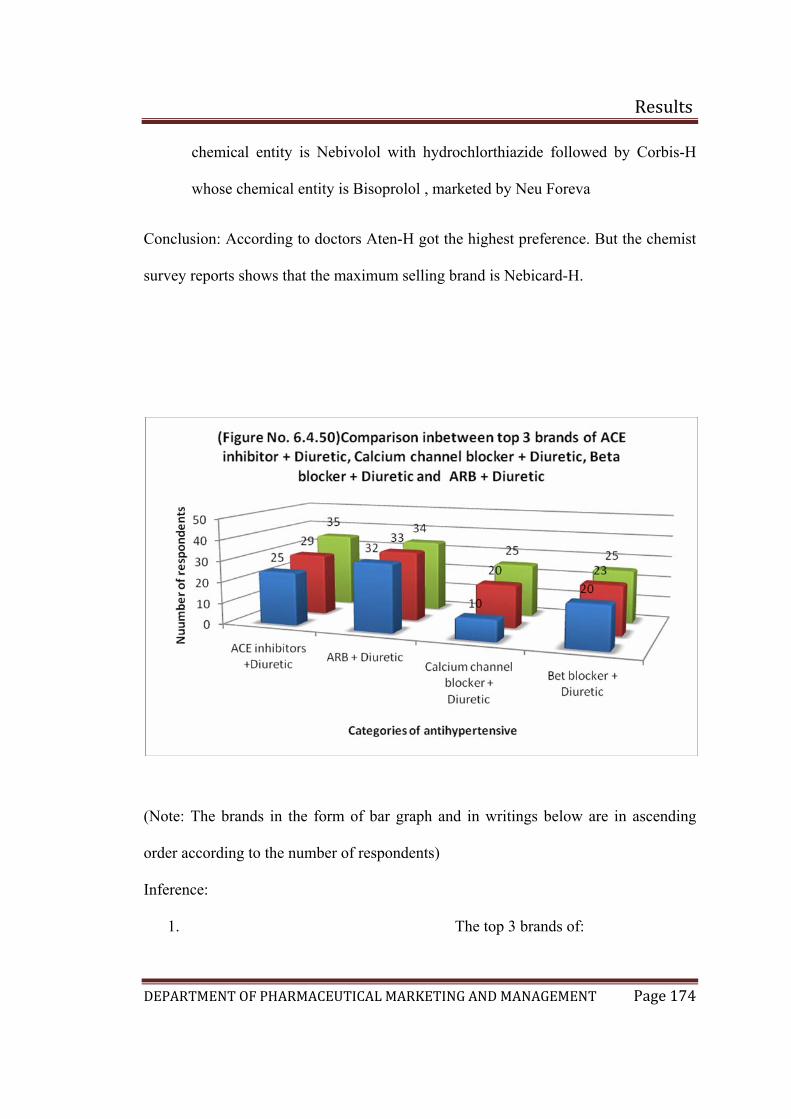
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 174
chemical entity is Nebivolol with hydrochlorthiazide followed by Corbis-H
whose chemical entity is Bisoprolol , marketed by Neu Foreva
Con
survey
clusion: According to doctors Aten-H got the highest preference. But the chemist
reports shows that the maximum selling brand is Nebicard-H.
(Note: The brands in the form of bar graph and in writings below are in ascending
order according to the number of respondents)
Inference:
1. The top 3 brands of:
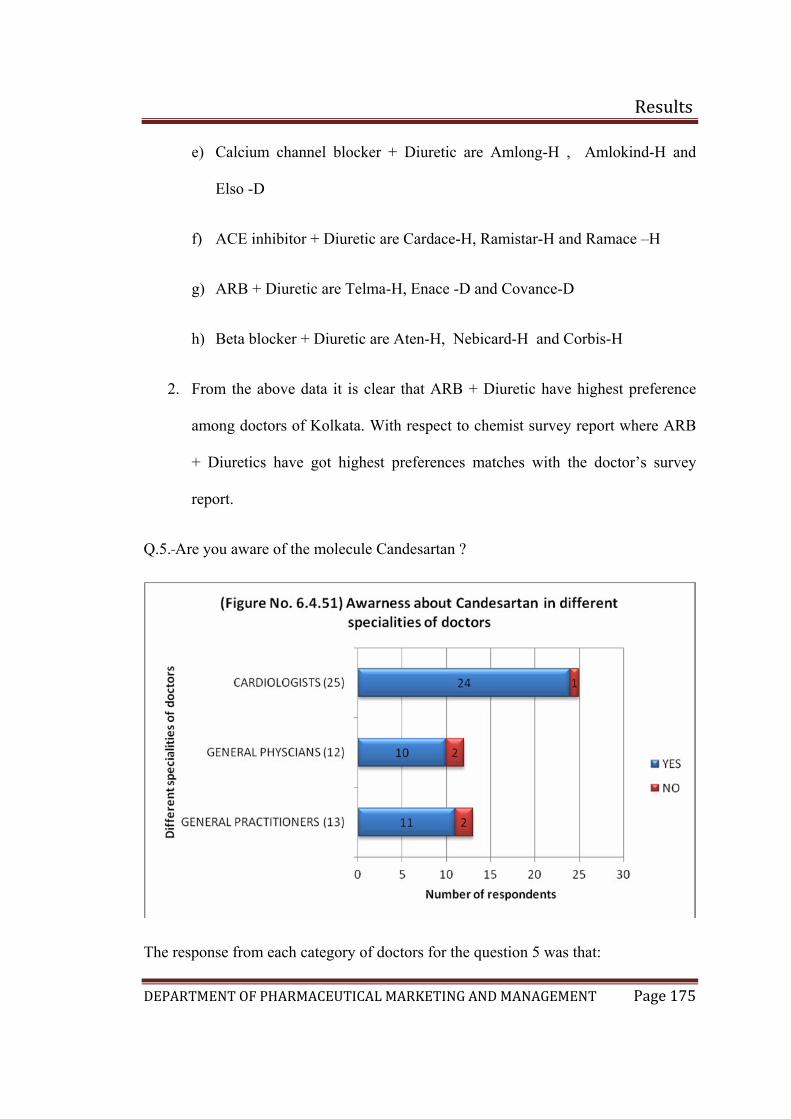
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 175
e) Calcium channel blocker + Diuretic are Amlong-H , Amlokind-H and
Elso -D
f) ACE inhibitor + Diuretic are Cardace-H, Ramistar-H and Ramace –H
g) ARB + Diuretic are Telma-H, Enace -D and Covance-D
h) ker + Diuretic are Aten-H, Nebicard-H and Corbis-H
2. ence
among doctors of Kolkata. With respect to chemist survey report where ARB
e doctor’s survey
Q.5
Beta bloc
From the above data it is clear that ARB + Diuretic have highest prefer
+ Diuretics have got highest preferences matches with th
report.
. Are you aware of the molecule Candesartan ?
The response from each category of doctors for the question 5 was that:
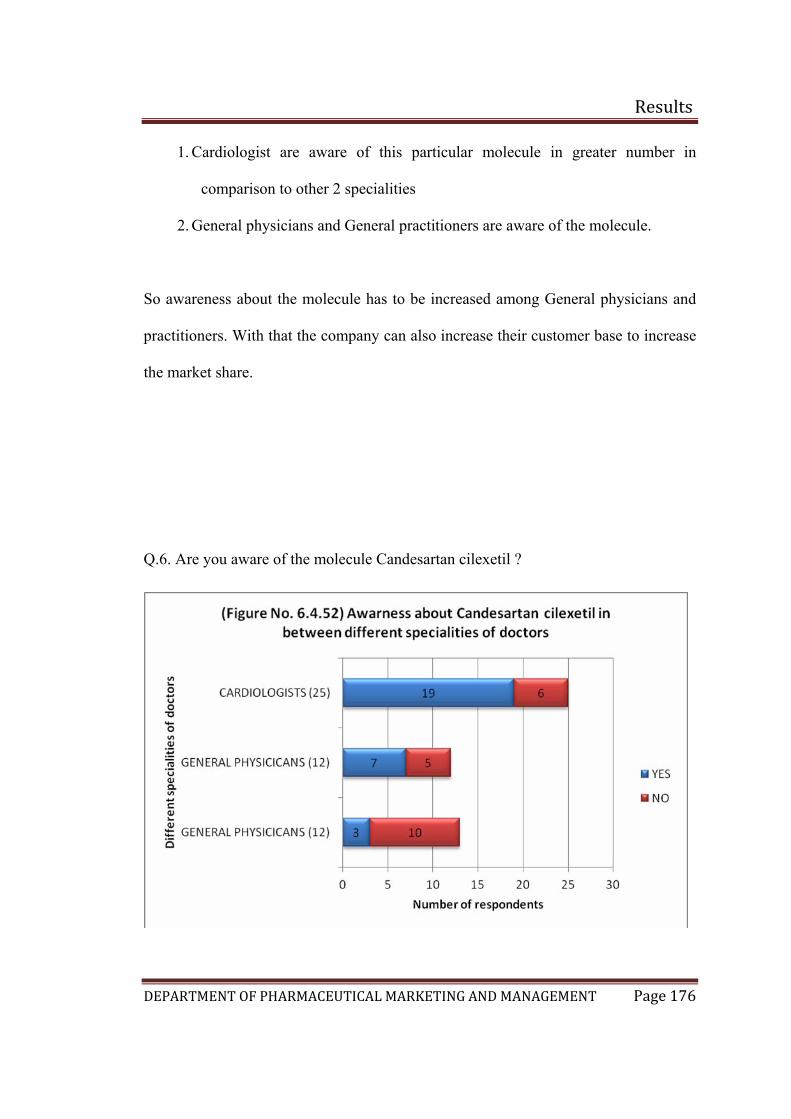
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 176
1. Cardiologist are aware of this particular molecule in greater number in
comparison to other 2 specialities
2. General physicians and General practitioners are aware of the molecule.
So awareness about the molecule has to be increased among General physicians and
practitioners. With that the company can also increase their customer base to increase
the market share.
Q.6.
Are you aware of the molecule Candesartan cilexetil ?
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 177
6 was that:
1. Cardiologist are aware of this particular molecule Candesartan cilexetil in
greater number in comparison to other 2 types
2. General physicians are aware of the molecule but less in numbers.
3. General practitioners are not aware of the molecule in greater extent.
rthiazide?
The response from each category of doctors for the question
Q.7. Are you aware of the molecule Candesartan cilexetil with hydrochlo
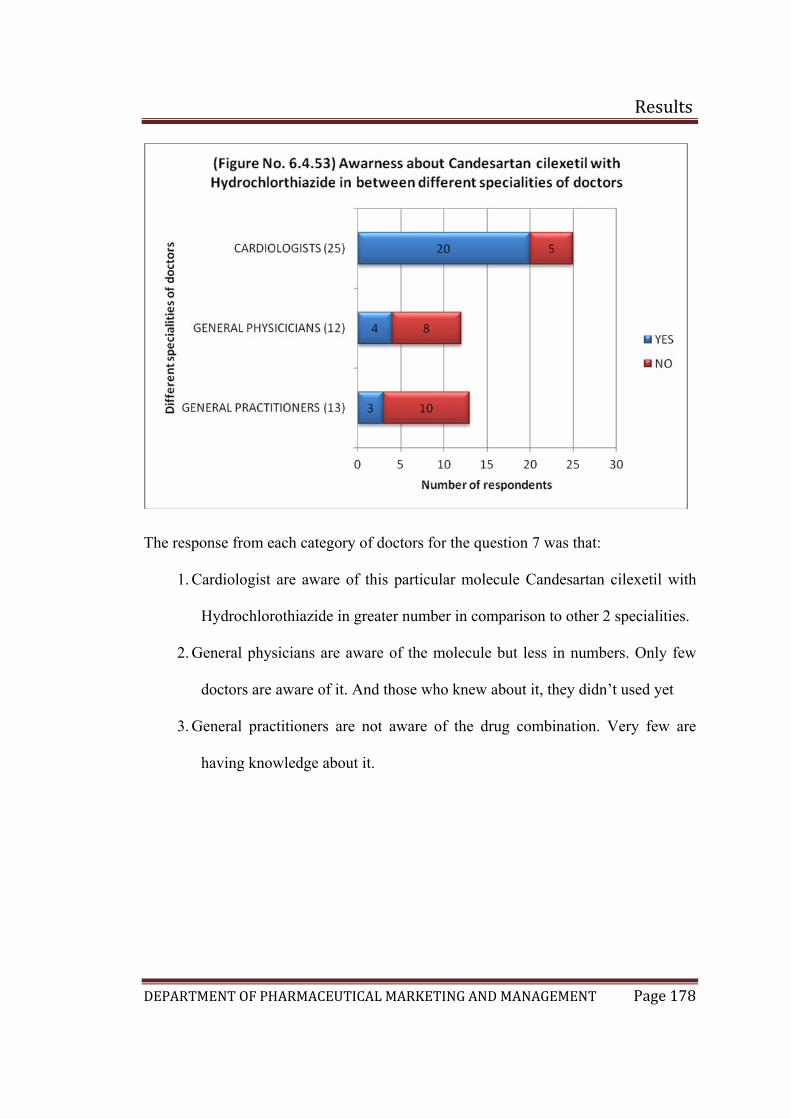
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 178
The response from each category of doctors for the question 7 was that:
til with
2. G
3. G re
1. Cardiologist are aware of this particular molecule Candesartan cilexe
Hydrochlorothiazide in greater number in comparison to other 2 specialities.
eneral physicians are aware of the molecule but less in numbers. Only few
doctors are aware of it. And those who knew about it, they didn’t used yet
eneral practitioners are not aware of the drug combination. Very few a
having knowledge about it.
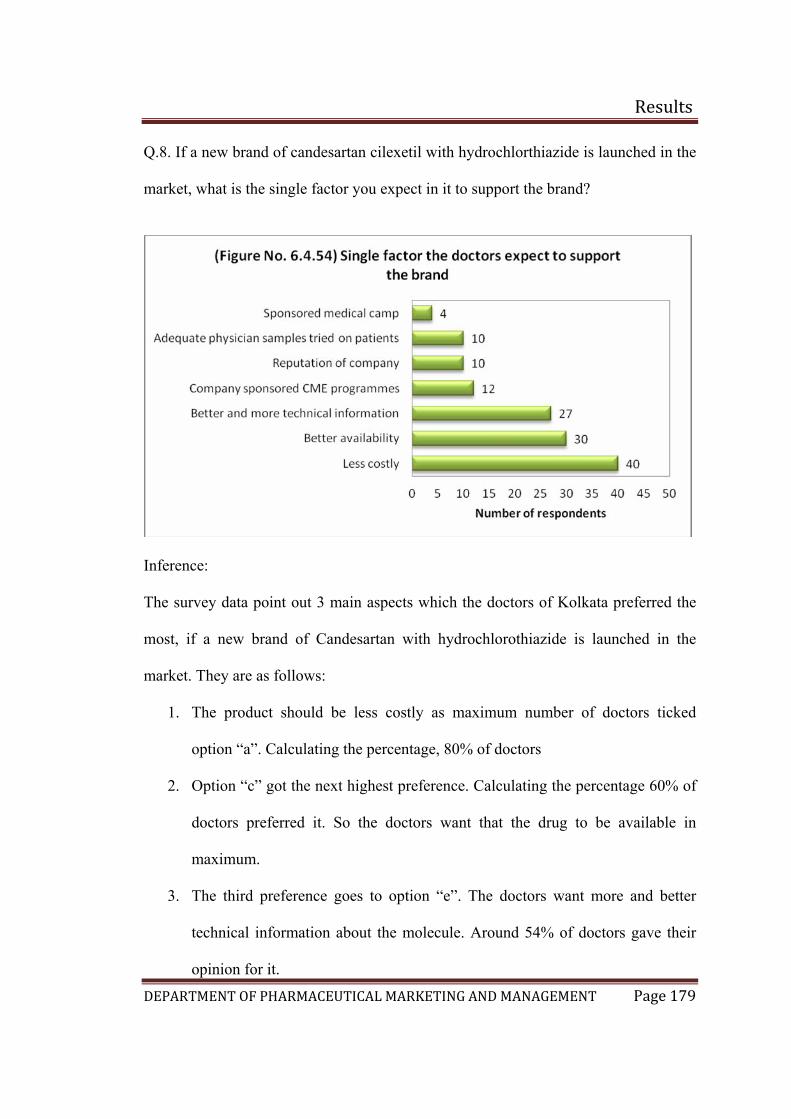
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 179
Q.8. If a new brand of candesartan cilexetil with hydrochlorthiazide is launched in the
market, what is the single factor you expect in it to support the brand?
Inference:
The survey data point out 3 main aspects which the doctors of Kolkata preferred the
most, if a new brand of Candesartan with hydrochlorothiazide is launched in the
market. They are as follows:
1. The product should be less costly as maximum number of doctors ticked
option “a”. Calculating the percentage, 80% of doctors
2. Option “c” got the next highest preference. Calculating the percentage 60% of
doctors preferred it. So the doctors want that the drug to be available in
maximum.
3. The third preference goes to option “e”. The doctors want more and better
technical information about the molecule. Around 54% of doctors gave their
opinion for it.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 180
Final conclusion of Doctors in Kolkata and Bangalore:
After carrying out surveys in Bangalore and Kolkata for doctors and chemists, the
major competitors are found to be ACE inhibitors, Calcium channel blockers, ARBs
and Diuretics. With respect to combination therapy the above mentioned categories of
drugs with Diuretics are the competitors. Combinations other than the mentioned ones
above, includes Calcium channel antagonist with ACE inhibitors and ACE inhibitor
with ARB which will also be a competitor in Kolkata and Bangalore respectively.
May the combination of ACE inhibitor with ARB, did not enjoy a higher preferences
among the doctors presently but according to literature survey it was found that ARB
combined with ACE inhibitor reduces morbidity and mortality in patients with heart
failure.(33)
With respect to ACE inhibitors and ARBs, both of them are used in all different age
groups for treatment of hypertension. From the above conclusion it was quite clear
that if a new brand of ARB with diuretic is launched in market the major competitor
will be CCA and ACE inhibitors in mono-therapy as well as in combination therapy.
In both the cities the preferred molecule among ACE inhibitors are Ramipril followed
by Enalapril and with respect to ARBs, Telmisartan has the higher preference
followed by Losartan as per doctors preference and chemists sales experience.
With respect to Candesartan, the molecule has a very low preference in the market but
doctors specially the cardiologist has a good impression on this particular molecule
which is supported by the response gathered from the question 5, 6 and 7 of the
questionnier for the doctors. The preference of Candesartan by the doctors in Kolkata
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 181
is higher than Bangalore which means the drug is being prescribed by the doctors in
Kolkata.
Although the molecule is a preferred one, it didn’t have a response to that extent in
comparison to Telmisartan and Losartan. The reason which can be the cause is less
number of quality brands in market or very less awareness about the molecule among
the doctors or less promotional awareness. The drug may not have higher plus points
in comparison to Telmisartan but it has some positive advantages in comparison to it
according to literature. Such as the maintenance dose of Candesartan is less than
Telmisartan(34) and it being the only drug licensed by US FDA for the treatment of
hypertension and heart failure. These can be used as a plus point to position the
product against Telmisartan. Candesartan is also the most cost effective ARB for the
treatment of hypertension and Heart failure. (33)
In comparison to Losartan, Candesartan has much higher superiority according to
literature survey. The plus points of candesartan over Losartan are greater
bioavailability, long duration of action, less side effects and better efficacy.(34) So if a
new brand of Candesartan is launched in the market, it can beat the second preferred
molecule in market if properly positioned.
In respect to the other category such as the ACE inhibitors and Calcium channel
antagonists, they are generally well tolerated.
The most preferred Calcium channel antagonist is Amlodipine as per the survey
carried out in both the above mentioned cities. Literature survey says that Candesartan
is better tolerated than Amlodipine.(9) So positioning the molecule Candesartan
against Amlodipine will have a plus point. However, ARBs unlike ACE inhibitors, do

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 182
not block the synthesis of Kinins and are therefore less likely to be associated with the
adverse effects of cough and angioedema. So, ARBs are an appropriate alternative
when treatment with an ACE inhibitor is strongly indicated but poorly tolerated.
So finally we can conclude that, strategies which are to be made for the launch
program should focus on the gaps which the above categories of the drug could not
fulfill in respect to therapeutic aspects or promotional aspects or positioning aspects.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 183
6.5 Deciding how to enter the market (1)(18)
Once the company decides to target a particular country, it has to determine the best
mode of entry. Its broad choices are indirect exporting, direct exporting, licensing,
joint ventures and direct investment.
The normal way to get involved in an international market is through export. The
company produces its goods in the country and might or might not adapt them to
international markets. Companies typically start with indirect exporting that is they
work through independent intermediaries.
Domestic based export merchants buy the manufacturer’s products and then sell them
abroad. Domestic based export agents seek and negotiate foreign purchases and are
paid a commission. Cooperative organizations carry on exporting activities on behalf
of several producers and are partly under their administrative control. Export
management companies agree to manage a company’s export activities for a fee.
Indirect export has two advantages, first it involves less investment second it involves
less risk.
Company eventually may decide to handle their own exports. the investment and
risk are somewhat greater, but so is the potential return. A company can carry on
direct exporting in several ways:
1. domestic based export department or division
2. overseas sales branch or subsidiary
3. traveling export sales representatives
4. foreign based distributors or agents
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 184
Licensing is a simple way to become involved in international marketing. The
licensor issues a license to a foreign company to use a manufacturing process,
trademark, patent, trade secret or other item of value for a fee or royalty. The licensor
gains entry at little risk. Licensing has potential disadvantages. The licensor has less
control over the licensee than it does over its own production and sales facilities.
Furthermore, if the licensee is very successful, the firm has given up profits and if and
when the contract ends, the company might find that it has created a competitor.
Foreign investors may join with local investors to create a joint venture company in
which they share ownership and control. A joint venture may be necessary or
desirable for economic or political reasons. It has certain drawbacks too. The partners
might disagree over investment, marketing or other policies. Joint ownership can also
prevent a multinational company from carrying out specific manufacturing and
marketing policies on a worldwide basis.
The ultimate form of foreign involvement is direct ownership of foreign based
assembly or manufacturing facilities. The foreign company can buy part or full
interest in a local company or build its own facilities. It has distinct advantages like
the firm secures cost economies in the form of cheaper labor or raw materials, foreign
government investment incentives and freight savings. The firm strengthens its image
in the host country because it creates jobs. The firm develops a deeper relationship
with government, customers, local suppliers and distributors enabling it to adapt its
products better to the local environment. The firm retains full control over its
investment and therefore develop manufacturing and marketing policies that serve its
long-term international objectives. The main disadvantage is that the firm exposes a
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 185
large investment to risks such as blocked or devalued currencies, worsening markets
or expropriation. The firm will find it expensive to reduce or close down its
operations, because the host country might require substantial severance pay to the
employees.
To enter the Brazilian market products such as pharmaceuticals, vitamins and medical
devices products, can be sold only if:
A) The foreign company establishes a local Brazilian manufacturing unit or local
office, fully responsible for its products; or
B) The foreign company appoints a Brazilian distributor, who has the registration
with the ANVISA as an importer and distributor of the types of products being
offered.
The first step a foreign company must take is to decide whether it is going to
commercialize its products, through the Brazilian distributor or through its own
structure in Brazil. With either option, the distributor has to be duly registered at
ANVISA and authorized to operate by the sanitary agencies both municipal and
federal jurisdiction.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 186
6.4 Deciding on the marketing program (1)(3)(35)
International companies must decide how much to adapt their marketing strategy to
local conditions. At one extreme are companies that use a globally standardized
marketing mix worldwide. Standardization of the product, communication and
distribution channels promises the lowest costs. At other extreme is an adapted
marketing mix, where the producer adjust the marketing program to each target
market.
Product:
Establishing Global Service Brands describes some of the special concerns for
marketing services globally. There are different strategies of product and
communication to a foreign market. Straight extension means introducing the product
in the foreign market without any change. Product adaptation involves altering the
product to meet local conditions or preferences
Communications:
Company can run the same marketing communications programs as used in the home
market or change them for local market, a process called communication adaptation.
Marketers must also adapt sales promotion techniques to different markets. As the
company is tapping in Brazilian market where the local languages are Spanish and
Portuguese, sales promotion should be done taking language into consideration, so
that accurate understanding takes place in-between the middle men and the company
as well as with customers
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 187
Price:
Multinationals face several pricing problems when selling abroad. They must deal
with price escalations, transfer process, dumping charges and gray market.
Differences comes due to addition of costs such as cost of transportation, tariffs,
importer margin, wholesaler margin and retailer margin to its factory price. As there
are regulations in Brazil for pharmaceutical products the company has to follow those
and place a competitive price in the market for its product.
Basically, the following items have been agreed upon:
Price increases prior to March 1, 2003 cannot be implemented. After March 1, 2003,
companies will be allowed to increase the prices by 8.63 percent. CAMED--the
government medicines price control agency published a list of products and
therapeutic classes that was excluded from the price increases rules in the near future.
Once again, Inter-pharma supports free market and freedom of pricing.
Pharmaceutical companies are responsible for determining wholesale drug prices but
the prices which the consumer pays at the pharmacy also reflects other costs and
taxes. Prices for retail drugs also include a pharmacy mark-up, a federal tax and a
state tax.
Distribution:
“If your product is not there, your customer cannot buy it.” Distribution will be driven
by company’s product positioning and target market. In developing the launch
strategy, key distribution channels should be identified. A launch plan should be
developed specifically for each account based on factors such as their trading policy,
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 188
promotional plans, customer profile and competitive set. This plan should then be
presented to each account within their necessary time frames. This presentation is the
first stage of securing distribution. Assuming a positive response, further negotiation
may take place alongside product sampling. Technical requirements for launch will
also need to be supplied e.g. New Product Listing forms which will provide key
technical information like barcode, case code, sizes, pallet configuration.
As the company is tapping in international market, it should take a whole channel
view of the problem of distributing products to final users. In the first link, seller’s
international marketing headquarters makes decisions on channels and other
marketing mix elements. The second link, channels between nations, gets the product
to the borders of the foreign nation. The decisions made in this link include the types
of intermediaries (agents, trading companies) that will be used, the type of
transportation (air, sea) and the financing and risk arrangements. The third link,
channels within foreign nations, gets the products from their point to final buyers.
When company first enter a foreign market, its better to work with local distributors
who have good local knowledge.
In Brazil a foreign company has to distribute its pharmaceutical products through
local distributors who are registered to ANVISA or set up its own subsidiary and built
its own marketing or sales team. The problem with local distributors are they do not
invest in business growth, do not follow company policy, do not share enough
information and may not promote the product due to less margin given in respect to
other companies. The positive side is the company Does not have to invest on
infrastructure and other things which need further investment. With that its own
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 189
marketing team may fail to understand the market properly or the way the business is
being carried over there and the problem of language to interact with other people. So
the company should choose the right local distributors, invest in them and set up
performance goals to which they can agree. If the company is able to find an
exclusive distributor for its products then it’s most helpful.
After few years, when the company is able to understand its business dealings
properly in the foreign country, it can built its own distribution channels and invest in
the same.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 190
6.5 Business analysis(1)(36)
After management develops the product concept the next step is to conduct the
business analysis.
Sales volume potential: before making any estimates of expected sales it is important
to size up the opportunity. What is the size of the total market? Adding up the retail
sales volumes of all competitive products, the size of the total market can be found.
What is the extent of competition both direct and indirect? The indirect competition
includes all the products that can be used as substitutes for the same condition or
indication. Now as per the market survey the direct competitor of Candesartan
cilexetil is Telmisartan followed by Losartan with hydrochlorothiazide. The major
indirect competitor is found to be drugs under ACE inhibitors, such as Ramipril
followed by Enalapril. There is another category of drugs which are also competing as
a indirect competitior which is Calcium channel blockers specially Amlodipine.
The company also has to find out the growth trends of the market. From the
epidemiology study of hypertension it was found that hypertension is one of the major
risk factor for mortality and which is continuously increasing in both India and Brazil
as per WHO. So the potentiality to run a business in this particular sector is worth
while for an emerging company.
The company also has to estimate the extent of share the product entry could expect to
capture during the first and second year.
Estimating costs: Costs are estimated by R&D, manufacturing, marketing and finance
department. The company has to measure 5 years projection of sales costs and profits.
Factors such as sales revenue, cost of goods sold, gross margin, development costs,
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 191
marketing costs and allocated overheads should be projected in cash flow statement of
the company.
Profit potential: The company should also assess or evaluate the profit potentials of
the new product. For that the following aspects have to be taken into considerations:
a) What will be the product’s gross margin? How are they comparable to the
existing products?
b) What levels of marketing expenditure are needed to achieve the projected
sales volumes in the first and the second year?
c) What is the break even point? By what time the company likely to achieve the
break-even point as per the projected sales volume?
d) Are the raw materials and packaging materials freely available and their costs
stable? Are there any shortage forecasts for these that might lead to cost
escalation?
e) Do the returns on investment projection for the product under consideration
offer the best alternative use of capital?
f) Considering that the product should be priced at par with competition and
since the trade margins are virtually the same for all competitors in India in a
given product category, (the retail margins are fixed by the DPCO and
wholesale margins by the industry and trade agreement) will the product
generate a gross margin equal to or in excess of current products?
Things will be different when the company wants to launch in international
market due to discrepant international laws.
g) What is the projected pay back period?
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 192
h) Introductory marketing investment in terms of months after the product
introduction date?
So for a company to launch a new product in an international and domestic market
the financial status of the company should be strong. This will finally help the
company to meet up all the business steps and expectations, planned for the successful
launch for its new product.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 193
6.6 Operational plans (1)(4)( 35)
Once the firm has determined which markets to enter, the mode of entry and its goals
and objectives relative to international expansion, it next has to draw up operational
plans for marketing the product or service in the international market. These plans
will be guided by the firm’s competitive posture in international market and the nature
of its strategic thrust. All marketing strategy is built on STP-Segmentation, Targeting
and Positioning. A company discovers different market place, targets those needs and
groups that it can satisfy in a superior way, and then positions its offering so that the
target market recognizes the company’s distinctive offering and image.
Understanding product market structure:
In domestic markets, the firm must determine the place its product could occupy
within a given market, what benefits it will stress and what customers or market
segment it will target. In international markets, these positioning decisions are broader
in scope, and in some respects more crucial. A clear understanding of product market
structure is crucial to effective positioning decisions and for that the firm must first
establish the relevant set of competing products and identify relevant product market
boundaries.
Next management has to assess the dimensions of the product market in the
international market. Here management should consider the size, intensity and growth
rate of demand in the targeted foreign market. These factors impact, not only the
profit potential of a given market, but also the costs associated with market
development.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 194
Segmenting international and domestic market:
Next management has to determine how to segment markets. Markets usually fall into
natural segments, which contain customers who exhibit the same broad characteristic.
The discerning marketer is conscious of this fact and fine tunes his product, offering
specially to reach these segments effectively. The essential criteria for effective
segmentation is (36)
Measurability: the segment must be measurable or definable in some specific
way.
Accessibility: the segment must be reachable with proper communication
package in cost effective manner.
Desirability: the segment must be large enough to service profitably.
Homogeneity: there should be a proper match or fit between the need profile
of the members of the segment and the satisfaction qualities or attributes of the
product
Vulnerability: the market must not be excessively vulnerable to competition
The customer segmentation has been done on the basis of the various doctor
specialties that treat hypertensive patients. The results of the primary market research
indicate the presence of three major segments, these are:
1. Cardiologists
2. General physicians
3. General practitioners
The results of the primary market research conducted among chemists indicate that
the Cardiologists and General physicians treat the maximum number of hypertensive
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 195
patients. This result is further augmented by the doctor’s survey that concluded that
the Cardiologists and General Physicians are the major prescribers for the categories
of drugs indicated for hypertension. Other than these two, General practitioners are
also prescribing ARB’s for hypertension but comparatively less than the above
mentioned two categories. From the market survey it was found that the general
practitioners are not so much aware about the efficacy of the ARB’s, or never used
them in the treatment of hypertension of their patients. So an effort from the
company’s scientific business development team is very much necessary to create an
awareness in doctors for their better effectiveness in hypertensive patients.
ARB’s also has additional effects. There are studies which proves that Candesartan,
in respect to other ARB’s such as Telmisartan and Losartan, improves arterial
stiffness independently of blood pressure lowering possibly by direct action resulting
from its potent affinity and binding capacity for the angiotensin II type 1 receptor, and
thus concludes that candesartan is a potentially useful therapy against arterial
stiffness in hypertensive patients with type 2 diabetes mellitus.(37)
In another study it was concluded that candesartan in type 2 diabetic patients with
mild to moderate retinopathy induced significant improvement in retinopathy over 4
years irrespective of hypertension status at baseline.(38)
So Diabetologist can also be targeted to treat patients with hypertension or other
complications mentioned above in type II diabetics, which will finally increase the
customer base.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 196
Branding of the product:
The American marketing association defines a brand as a name, term sign, symbol, or
design or a combination of them, intended to identify the product of one seller or
group of seller and to differentiate them from those of competitors. Brands identify
the source or marker of a product and allow consumers either individuals or
organizations to assign responsibility to a particular manufacturer or a distributor.
Branding is all about creating differences. To brand a product, it is necessary to teach
customers “who” the product is by giving it a name, as well as “what” the product
does and “why” customers should care.
For pharmaceutical products the brand name should be such that it should be easy to
remember, pronounce and write. The brand name should not resemble any other
pharmaceutical product, after the confirmation of the foresaid the product launch
should be undertaken. Since getting brand name registered takes a minimum of two to
three years, it is better to have ready in the category the company is entering.
The following is the proposed brand name for the product which will be available:
Proposed brand name is CANDEBEAT-HCT, the product contains (Candesartan
cilexetil 16mg + Hydrochlorothiazide 12.5mg) and (Candesartan cilexetil 32mg +
Hydrochlorothiazide 12.5mg) and (Candesartan cilexetil 32mg + Hydrochlorothiazide
25mg)
The brand name “CANDEBEAT-HCT” is coined from the parent molecule
Candesartan and Heartbeat. The part “CANDE” is taken from Candesartan and
“BEAT” from heart beat. Beat also means to defeat. So the brand name delivers a
message that the product can defeat hypertension if treated with it.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 197
Product positioning:
Once the competitive frame of reference for positioning has been fixed by defining
customer target market and nature of competition, the appropriate points of difference
(PODs) and points of parity (POPs) can be defined.
POD are attributes or benefits consumers strongly associate with a brand, positively
evaluate and believe that they could not find them to the same extent and nature in the
competitive brand. Creating strong, favorable and unique associations as POD is a
real challenge, but essential in terms of competitive brand positioning. In choosing
POD two important considerations are that customers find the POD desirable and that
the firm has the capabilities to deliver on the POD.
POP on the other hand are associations that are not necessarily unique to the brand but
may in fact be shared with other brands. These types of associations come in two
basic forms: category and competitive.
Category POP are associations customer view as essential to be a legitimate and
credible offering within a certain product.
Competitive POP are associations designed to negate competitors POD
There are three key consumer desirability criteria for PODs.
1. Relevance. Target customers must find the POD personally relevant and
important.
2. Distinctiveness. Target customers must find the POD distinctive and superior
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 198
3. Believability. Target customers must find the POD believable and credible. A
brand must offer a compelling reason for choosing it over the other options.
There are three key deliverability criteria.
1. Feasibility. The firm must be able to actually create the POD. The product
design and marketing offering must support the desired association.
2. Communicability. It is very difficult to create an association that is not
consistent with existing customer knowledge or that customers, for whatever
reason, have trouble believing. Customer must be given a compelling reason
and understandable rationale as to why the brand can deliver the desired
benefit.
3. Sustainability. It will depend on internal commitment and use of resources as
well as external market forces
Candesartan cilexetil with Hydrochlorothiazide will be positioned for the treatment of
hypertension and heart failure.
Positioning statement for the above mentioned molecule: “A NEW HORIZON FOR
HEART PATIENT” Angiotensin II is formed from angiotensin I in a reaction
catalyzed by angiotensin-converting enzyme (ACE, kininase II). Angiotensin II is the
principal pressor agent of the rennin- angiotensin system, with effects that include
vasoconstriction, stimulation of synthesis and release of aldosterone, cardiac
stimulation and renal reabsorption of sodium. Candesartan blocks the vasoconstrictor
and aldosterone secreating effects of angiotensin II by selectively blocking the
binding of angiotensin II to the AT1 receptor in many tissues, such as vascular
smooth muscle and the adrenal gland.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 199
Candesartan cilexetil is the only ARB currently licensed for the treatment of heart
failure.
Hydrochlorothiazide works mainly by stopping the re-absorption of sodium (salt) and
water from the kidneys back into the blood stream
Unlike ACE inhibitors Candesartan cilexetil does not inhibit the breakdown of
bradykinin and are therefore associated with a lower incidence of cough.
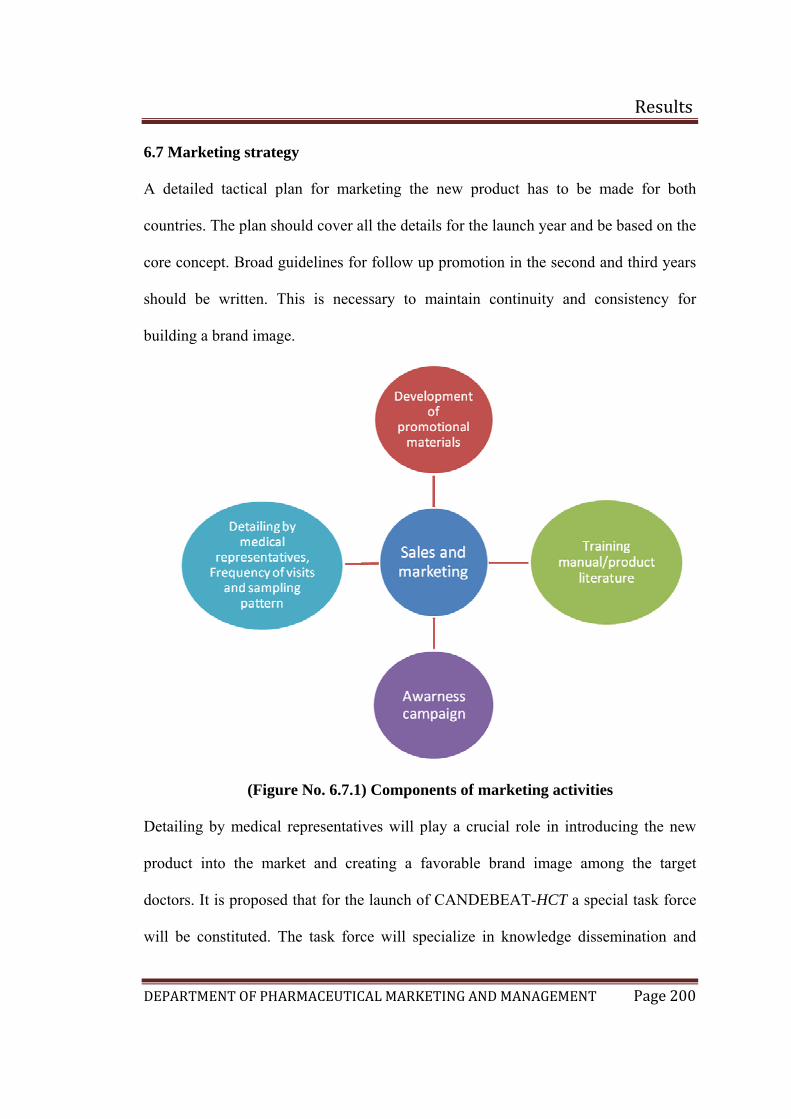
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 200
6.7 Marketing strategy
A detailed tactical plan for marketing the new product has to be made for both
countries. The plan should cover all the details for the launch year and be based on the
core concept. Broad guidelines for follow up promotion in the second and third years
should be written. This is necessary to maintain continuity and consistency for
building a brand image.
(Figure No. 6.7.1) Components of marketing activities
Detailing by medical representatives will play a crucial role in introducing the new
product into the market and creating a favorable brand image among the target
doctors. It is proposed that for the launch of CANDEBEAT-HCT a special task force
will be constituted. The task force will specialize in knowledge dissemination and
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 201
introducing the product in the market. The activities of the special task force will be to
identify the key opinion leaders, introduce the product among them and disseminate
the latest advances in the field of hypertension. The sales force will integrate the
marketing efforts for CANDEBEAT-HCT and promote the prescription strategy.
The detailing part for CANDEBEAT-HCT will focus upon the role of Candesartan
cilexetil in the treatment of hypertension as well as heart failure. Further, the detailing
story will involve the role of Hydrochlorothiazide in CANDEBEAT-HCT and how it
will enhance both doctors compliance. After that it will emphasize on the
improvement of blood pressure on long term treatment. The sales representative will
compare the efficacy of CABDEBEAT-HCT versus other brands of ARB’s in the
same and different categories and also the advantages of the molecule in respect to
other beneficial effects. The frequency of visits will depend upon the category of
doctors. In the initial phase focus will be upon the targeted doctor categories
(Cardiologists and General physicians) later general practitioners will also be
targeted. The frequency of visit will be calculated for 100 doctors. Each individual of
the special task force will cover 100 doctors in a month and on an average 10 calls
will be made per day.
Now in Brazil the promotional aspects will be different according to their country’s
promotional regulations. As the cost of investment in Brazil is very high for
promotion, the company has to invest very carefully. Company also has to decide
whether they will promote the product through local sales force in Brazil or should
teach their marketing people in its home ground and let it done by them. As the
promotional cost is high in Brazil, unless the company is not opening a subsidiary
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 202
over their or an office setup in Brazil, its better to promote the product through local
distributors and their sales force.
Product training manual:
What is Hypertension?
According to WHO, Hypertension is the state of body in which systolic BP is 150
mmHg or more & diastolic BP is 95 mmHg or more.
Hypertension can be classified either essential (primary) or secondary. Secondary
hypertension indicates that the high blood pressure is a result of (i.e., secondary to)
another condition, such as kidney disease or tumors (pheochromocytoma and
paraganglioma).
What is Pre-hypertension?
Recently, the JNC 7 (the Seventh Report of the Joint National Committee on
Prevention, Detection, Evaluation, and Treatment of High Blood Pressure) has
defined blood pressure 120/80 mmHg to 139/89 mmHg as "Pre-hypertension.“
Pre-hypertension is not a disease category rather, it is a designation chosen to identify
individuals at high risk of developing hypertension
Another way of classifying hypertension is as follows:
Normal – (Systolic 90-120, diastolic 60-80)
Pre-hypertension – (Systolic 120-139, diastolic 80-99)
Hypertension Mild, Stage 1 - (Systolic 140-159 or diastolic 90-99)
Hypertension Moderate, Stage 2 - (Systolic 160 - 179 diastolic 100 – 109)
Hypertension Severe, Stage 3 - (Systolic 180 - 209 or diastolic 110 – 119)
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 203
Hypertension Very Severe, Stage 4 - (Systolic > or = 210 or diastolic > or =
120)
What are the Risk Factors involved in Hypertension?
Persistent hypertension is one of the risk factors for strokes, heart attacks, heart failure
and arterial aneurysm, and is a leading cause of chronic renal failure.
Hypertension is a significant public health problem in urban and rural areas of India.
It is directly responsible for 57% of all stroke deaths and 42% of coronary heart
disease death in India. It is also a leading cause of blindness, renal failure and
congestive heart failure.
Mortality as a consequence of morbidity has increased, with stroke being a leading
cause of death. 11.3% of total deaths, 10.1% of all deaths in the 20−59 year-old age
group, and 33.9% of cardiovascular deaths in Brazilian Capitals also and the reason
for this is elevated blood pressure level.
What is CANDEBEAT-HCT?
CANDEBEAT-HCT is a combination of two medicines used in the treatment of high
blood pressure (hypertension): the angiotensin II receptor blocker candesartan
cilexetil and the diuretic (water tablet) hydrochlorothiazide. Both medicines are
provided in one tablet.
What is CANDEBEAT-HCT used for?
The product contains (Candesartan cilexetil 16mg + Hydrochlorothiazide 12.5mg) and
(Candesartan cilexetil 32mg + Hydrochlorothiazide 12.5mg) and (Candesartan
cilexetil 32mg + Hydrochlorothiazide 25mg)
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 204
CANDEBEAT-HCT is used to treat high blood pressure (hypertension) when one
medicine (monotherapy) is not sufficiently effective.
How does CANDEBEAT-HCT work?
CANDEBEAT-HCT combines two medicines that have different ways of working
(modes of action) and leads to a greater lowering of blood pressure in more people
than with either medicine used alone.
• Angiotensin II is formed from angiotensin I in a reaction catalyzed by
angiotensin- converting enzyme (ACE, kininase II). Angiotensin II is the
principal pressor agent of the renin-angiotensin system, with effects that
include vasoconstriction, stimulation of synthesis and release of aldosterone,
cardiac stimulation, and renal reabsorption of sodium. Candesartan blocks the
vasoconstrictor and aldosterone-secreting effects of angiotensin II by
selectively blocking the binding of angiotensin II to the AT1 receptor in many
tissues, such as vascular smooth muscle and the adrenal gland. Its action is,
therefore, independent of the pathways for angiotensin II synthesis.
There is also an AT2 receptor found in many tissues, but AT2 is not known to
be associated with cardiovascular homeostasis. Candesartan has much greater
affinity (>10,000-fold) for the AT1 receptor than for the AT2 receptor.
Blockade of the renin-angiotensin system with ACE inhibitors, which inhibit
the biosynthesis of angiotensin II from angiotensin I, is widely used in the
treatment of hypertension. ACE inhibitors also inhibit the degradation of
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 205
bradykinin, a reaction also catalyzed by ACE. Because candesartan does not
inhibit ACE (kininase II), it does not affect the response to bradykinin.
Whether this difference has clinical relevance is not yet known. Candesartan
does not bind to or block other hormone receptors or ion channels known to be
important in cardiovascular regulation.
Blockade of the angiotensin II receptor inhibits the negative regulatory feedback of
angiotensin II on renin secretion, but the resulting increased plasma renin activity and
angiotensin II circulating levels do not overcome the effect of candesartan on blood
pressure.
• Hydrochlorothiazide is a thiazide diuretic. Thiazides affect the renal tubular
mechanisms of electrolyte reabsorption, directly increasing excretion of
sodium and chloride in approximately equivalent amounts. Indirectly, the
diuretic action of hydrochlorothiazide reduces plasma volume, with
consequent increases in plasma renin activity, increases in aldosterone
secretion, increases in urinary potassium loss, and decreases in serum
potassium. The renin-aldosterone link is mediated by angiotensin II, so
coadministration of an angiotensin II receptor antagonist tends to reverse the
potassium loss associated with these diuretics.
The mechanism of the antihypertensive effect of thiazides is unknown
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 206
Pharmacokinetics of the combination:
Candesartan Cilexetil
Candesartan cilexetil is rapidly and completely bioactivated by ester hydrolysis during
absorption from the gastrointestinal tract to candesartan, a selective AT1 subtype
angiotensin II receptor antagonist. Candesartan is mainly excreted unchanged in urine
and feces (via bile). It undergoes minor hepatic metabolism by O-deethylation to an
inactive metabolite. The elimination half-life of candesartan is approximately 9 hours.
After single and repeated administration, the pharmacokinetics of candesartan are
linear for oral doses up to 32 mg of candesartan cilexetil. Candesartan and its inactive
metabolite do not accumulate in serum upon repeated once-daily dosing.
Following administration of Candesartan cilexetil, the absolute bioavailability of
candesartan was estimated to be 15%. After tablet ingestion, the peak serum
concentration (Cmax) is reached after 3 to 4 hours. Food with a high fat content does
not affect the bioavailability of Candesartan after candesartan cilexetil administration.
Hydrochlorothiazide
When plasma levels have been followed for at least 24 hours, the plasma half-life has
been observed to vary between 5.6 and 14.8 hours.
Distribution:
Candesartan Cilexetil
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 207
The volume of distribution of Candesartan is 0.13 L/kg. Candesartan is highly bound
to plasma proteins (>99%) and does not penetrate red blood cells. The protein binding
is constant at Candesartan plasma concentrations well above the range achieved with
recommended doses. In rats, it has been demonstrated that Candesartan crosses the
blood-brain barrier poorly, if at all. It has also been demonstrated in rats that
Candesartan passes across the placental barrier and is distributed in the fetus.
Hydrochlorothiazide
Hydrochlorothiazide crosses the placental but not the blood-brain barrier and is
excreted in breast milk.
Metabolism and Excretion:
Candesartan Cilexetil
Total plasma clearance of candesartan is 0.37 mL/min/kg, with a renal clearance of
0.19 mL/min/kg. When candesartan is administered orally, about 26% of the dose is
excreted unchanged in urine. Following an oral dose of 14C-labeled candesartan
cilexetil, approximately 33% of radioactivity is recovered in urine and approximately
67% in feces. Following an intravenous dose of 14C-labeled candesartan,
approximately 59% of radioactivity is recovered in urine and approximately 36% in
feces. Biliary excretion contributes to the elimination of candesartan.
Hydrochlorothiazide
Hydrochlorothiazide is not metabolized but is eliminated rapidly by the kidney. At
least 61% of the oral dose is eliminated unchanged within 24 hours.
How is CANDEBEAT-HCT given?
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 208
Candebeat-HCT supplied as tablets. It is very important to take medicines for high
blood pressure. This is because high blood pressure, if not treated, can get
progressively worse and can lead to number of other complications.
What are the contra-indications for usage of the brand?
CANDEBEAT-HCT is contraindicated in patients who are hypersensitive to any
component of this product. Because of the hydrochlorothiazide component, this
product is contraindicated in patients with anuria or hypersensitivity to other
sulfonamide-derived drugs.
What are the possible adverse reactions or side effects with CANDEBEAT-HCT?
Candesartan cilexetil:
These include hypotension, hyperkalemia, and reduced renal function, including that
associated with bilateral renal artery stenosis and stenosis in the artery of a solitary
kidney. Hypotension is most likely to occur in patients in whom the blood pressure is
highly dependent on angiotensin II, including those with volume depletion (e.g., with
diuretics), renovascular hypertension, cardiac failure, and cirrhosis; in such patients
initiation of treatment with low doses and attention to blood volume is essential.
Hyperkalemia may occur in conjunction with other factors that alter K+ homeostasis,
such as renal insufficiency, ingestion of excess K+, and the use of drugs that promote
K+ retention.
Hydrochlorothiazide:
Erectile dysfunction is a troublesome adverse effect of the thiazide-class diuretics,
and physicians should inquire specifically regarding its occurrence in conjunction
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 209
with treatment with these drugs. Gout may be a consequence of the hyperuricemia
induced by these diuretics. The occurrence of either of these adverse effects is a
reason for considering alternative approaches to therapy. However, precipitation of
acute gout is relatively uncommon with low doses of diuretics. Hydrochlorothiazide
may cause rapidly developing, severe hyponatremia in some patients. Thiazides
inhibit renal Ca2+ excretion, occasionally leading to hypercalcemia; although
generally mild, this can be more severe in patients subject to hypercalcemia, such as
those with primary hyperparathyroidism. The thiazide-induced decreased Ca2+
excretion may be used therapeutically in patients with osteoporosis or hypercalciuria.
What are the possible drugs Interactions with this combination?
Candesartan Cilexetil
No significant drug interactions have been reported in studies of Candesartan cilexetil
given with other drugs such as glyburide, nifedipine, digoxin, warfarin,
hydrochlorothiazide, and oral contraceptives in healthy volunteers. Because
Candesartan is not significantly metabolized by the cytochrome P450 system and at
therapeutic concentrations has no effects on P450 enzymes, interactions with drugs
that inhibit or are metabolized by those enzymes would not be expected.
• Lithium− Reversible increases in serum lithium concentrations and toxicity
have been reported during concomitant administration of lithium with ACE
inhibitors, and with some angiotensin II receptor antagonists. An increase in
serum lithium concentration has been reported during concomitant
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 210
administration of lithium with candesartan cilexetil, so careful monitoring of
serum lithium levels is recommended
during concomitant use.
Hydrochlorothiazide
When administered concurrently the following drugs may interact with thiazide
diuretics:
• Alcohol, barbiturates, or narcotics: Potentiation of orthostatic hypotension
may occur.
• Antidiabetic drugs (oral agents and insulin): Dosage adjustment of the
antidiabetic drug may be required.
• Other antihypertensive drugs− Additive effect or potentiation.
• Cholestyramine and colestipol resins− Absorption of hydrochlorothiazide is
impaired in the presence of anionic exchange resins. Single doses of either
cholestyramine or colestipol resins bind the hydrochlorothiazide and reduce its
absorption from the gastrointestinal tract by up to 85 and 43 percent,
respectively.
• Corticosteroids, ACTH− Intensified electrolyte depletion, particularly
hypokalemia.
• Pressor amines (eg, norepinephrine)− Possible decreased response to pressor
amines but not sufficient to preclude their use.
• Skeletal muscle relaxants, nondepolarizing (eg, tubocurarine)−Possible
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 211
increased responsiveness to the muscle relaxant.
• Lithium−Generally should not be given with diuretics. Diuretic agents reduce
the renal clearance of lithium and add a high risk of lithium toxicity.
• Non-steroidal Anti-inflammatory Drugs− In some patients, the administration
of a non-steroidal anti-inflammatory agent can reduce the diuretic, natriuretic,
and antihypertensive effects of loop, potassium-sparing and thiazide diuretics.
Therefore, when CANDEBEAT HCT and non-steroidal anti-inflammatory
agents are used concomitantly, the patient should be observed closely to
determine if the desired effect of the diuretic is obtained
Warnings:
Drug that act directly on the rennin-angiotensin system can cause fetal and neonatal
morbidity and death when administered to pregnant women. Post-marketing
experience has identified reports of fetal and neonatal toxicity in babies born to
women treated with Candesartan cilexetil during pregnancy. The use of drugs that act
directly on the rennin-angiotensisn system during the second and third trimesters of
pregnancy has been associated with fetal and neonatal injury, including hypotension,
neonatal skull hypoplasia, anuria, reversible or irreversible renal failure and death.
Oligohydramnios has been reported, presumably resulting from decreased fetal renal
functions.
Hypotension in volume and salt depleted patients:
Based on adverse events reported from all clinical trials, excessive reduction of blood
pressure was rarely seen in patients with uncomplicated hypertension treated with
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 212
candesartan cilexetil and hydrochlorothiazide. Initiation of antihypertensive therapy
may cause symptomatic hypotension in patients with intravascular volume or sodium
depletion. These conditions should be corrected prior to administration of the drug
What is the recommended dosage for CANDEBEAT-HCT?
The daily dose range for CANDEBEAT HCT tablets is Candesartan cilexetil 16 mg
combined with Hydrochlorothiazide 12.5 mg to Candesartan 32 mg combined with
Hydrochlorothiazide 25 mg to Candesartan cilexetil 32mg combined with
Hydrochlorothiazide 25mg.
To minimize dose-independent side effects, it is usually appropriate to begin
combination therapy only after a patient has failed to achieve the desired effect with
monotherapy.
Hypertension awareness campaign:
The hypertension awareness campaign will be designed nationally and delivered
locally to ensure dissemination not only to the mainstream population but also to the
diverse, underserved section of the population. The main campaign seeks to promote
awareness among all older men and women, their family and improve the
responsiveness of doctors.
In the international community, the campaign can only be launched after judging its
feasibility in respect to company’s strength and capability and constrains in the
foreign community.
Message to the communities:
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 213
How can we help COMMUNITIES that don’t GO TO THE DOCTOR as often as
they should?
We see real health problems in our communities such as Asthma, diabetes, Heart
diseases. “And too many folks don’t see a doctor in time. So we are working with
community groups to offer free health screenings and connect local doctors with the
people that really need help. That does make our heart good, too.”
To find out more visit www.healthycommunities.com
Title of the campaign: “An important public issue”
Launch of the campaign: “WORLD HEART DAY ”
Our objectives:
To make the masses aware of hypertension.
To tell them about its prevalence.
To teach prevention and treatment of this “complication”.
To tell the measures to control it.
To encourage and boost the morale of those suffering from the same.
Target audiences:
Obese people
Geriatrics
Patients
Working women and housewives
People working in BPO’s
Working men
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 214
Shopkeepers
Students
Planning of the campaign:
1. Identify the past and existing hypertension awareness campaign (sponsorships
by pharma companies) and ascertain their impact on national and local level
2. Ascertain the opportunities and barriers involved in implementing a national
hypertension awareness campaign
3. To identify and highlight the “best practices” which have laid an impact in
terms of efficacy, overall quality of life and cost effectiveness
4. To device strategies to fill the voids in awareness levels
5. Implement the approach that support the program and sustains the impact
6. Creating messages that are meaningful, culturally relevant and stimulating
7. To build the campaign on the existing health and community framework
8. To device and adapt strategies that cater to vast section of the population
Implementation of the campaign:
Built and mobilize a robust network for knowledge dissemination on
hypertension
Health care camps.
Reach the greatest number of men and women of age group starting from 45
years and above through a national campaign
Deliver the campaign locally, this will ensure greater likelihood of success
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 215
To partner with trusted organization and key doctors
Call on helpline number provided by the campaign organizers..
Providing with a postal address.
Pamplets inserted in newspapers and health magazines.
Hoardings on road side especially at bus stops and public places.
Tactics used to ensure success of the campaign:
1) Information must be compelled by driving action: The information should
clearly covey the consequences of Hypertension if untreated and communicate
the ways to prevent it. Scare strategy should not be used as such tactics have a
short run and are effective. Focus should also be given to those who are
working in companies where work stress is more to create awareness for
future prevalence of hypertension. According to the JNC 7 (the Seventh Report
of the Joint National Committee on Prevention, Detection, Evaluation, and
Treatment of High Blood Pressure) has defined blood pressure 120/80 mmHg
to 139/89 mmHg as "Prehypertension.“ Prehypertension is not a disease
category; rather, it is a designation chosen to identify individuals at high risk
of developing hypertension. People can be motivated by messages that point
out the importance of taking care of themselves for their family.
2) Deploying nontraditional channels for communication such as ethenic media,
particularly multilingual news papers and television can be used for catering to
the mass.
The communication plan:
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 216
Key promise statement: “By preventing and treating hypertension, I am avoiding the
silent killer to spoil my happiness and making me dependent on others. If I get
treated, I can enhance my quality of life and contribute more to my family and finally
to society”
sMessages and support statement:
Protect your vital part of your life “Heart” and it will support you for today
and tomorrow
Know your blood pressure. Take time to get tested
Weight Reduction, Increased Exercise, Salt Restriction, Relaxation & Stress
Management Supplementation of potassium, calcium, & magnesium, Use of
Fish oil and Cessation of smoking can control your blood pressure
Untreated Hypertension can lead to other Heart diseases and other complex
disorders.
Take the early first step to avoid happiness to run out from your life.
Evaluation of the campaign:
The purpose of evaluation will help in assessing the effectiveness of the awareness
campaign, reveal how well the campaign was implemented, the barriers encountered
and were the foresaid objectives attained. The following are the questions which need
to be answered for evaluation
Are the messages likely to be effective in increasing awareness and motivating
changes in the target audiences?
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 217
Are the messages culturally sensitive and cater to the diverse group?
Did awareness of the campaign/messages increase?
Did awareness of the consequences of hypertension increase?
Did awareness of the blood pressure screening increase?
What actions did the target audience take
Constraints: the following are the constraints that can impact the launch of the
proposed products in the market:
Investments: this can be one of the leading factors that can impact the over all
framework of the strategy, adequate investments will be required at every level of the
implementation of the proposed launch strategy.
Strength of the sales force: the medical representatives will be forming the interface
between the various doctors’ categories and the company. The quality (which is the
function of the training program) and quantity (number of Medical representative’s
deployed by the company per territory) will play an important role at the time of
introduction of the product in the market
Image of the company: more than the proposed product, the image of the company
matters in recruiting the key opinion leaders. For a new product to make at impact on
the market a strong presence among the key opinion leaders is necessary.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 218
6.8 Product development (1)(36)
Up to now, the product has existed only as a word description, a drawing, or a
prototype. The next step involves a jump in investment that dwarfs the costs incurred
in the earlier stages. At this stage the company will determine whether the product
idea can be translated into a technically and commercially feasible product.
The R&D department will develop the physical versions of the product concept of
Candesartan cilexetil with hydrochlorothiazie. Its goal is to make the prototype which
performs safely with having key attributes described and within budgeted
manufacturing costs. The company has to make checklist, such as
I. The raw material specifications
II. The production specifications
III. Determining the shipper sizes
IV. Developing the packing including specifications of packaging materials.
As the company is also targeting a foreign market (Brazil) the
specifications should be according to the Brazilian regulations. The
company has to check whether your labeling is accordance with drug laws.
The language in brazil is Spanish, it better to label the product in local
language.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 219
V. Decision on the price: According to literature survey Candesartan is the
least expensive at maintenance doses for hypertension.(33)
VI. Fulfillment of all the licensing and other legal requirements.
After management is satisfied with functional and psychological performance, the
product is ready to be dressed up with a brand name and packaging and put into a
market test. The new product shall be introduced into an authentic setting to learn
how large the market is and how doctors and dealers react to handling and using the
product
Monitor performance: Elementary and fundamental as it may see, monitoring
performance of new products on a regular basis is an important task. Once the product
is commercialized, probably the newness and the consequent excitement are gone.
The common temptation is to revise the forecasts of new product for six months or
even longer instead of analyzing and finding out reasons. Monitoring the performance
of new products regularly against the original plan forecasts can provide significant
insights and leverages in the development of successful new product.
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 220
6.9 Commercialization
To introduce a major new product into the national and international market, the
company may have to spend a huge amount of money in advertising, promotion and
other communications in the first year. A survey carried out by IBOPE Monitor
compared the first trimesters of the years 2000 through 2007, and found that
pharmaceutical industry investment in publicity had grown almost 70% over the past
three years, as opposed to 33,6% growth in publicity in general.( ) So for an emerging
company it’s a huge investment.
Most new-product campaigns rely on a sequenced mix of market communication
tools.
WHEN (timing): In commercializing a new product, market entry timing is critical.
WHERE (geographic strategy): The company must decide whether to launch the new
product in a single locality, a region, several regions in national and international
market. Company size is an important factor here. Small companies have to select an
attractive city and put a blitz campaign. They should enter other cities one at a time.
Now as per the survey carried out in domestic market such as Kolkata and
Bangalore the report says the awareness of the molecule Candesartan cilexetil with
hydrochlorothiazide in Kolkata is bit higher than Bangalore and ARB’s are also being
used in higher amount according to survey. So Kolkata is a target city for the
Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 221
company. As Bangalore is the home town of the company it can be the second choice.
The company may also target 3 other metros such as Mumbai, Delhi and Chennai.
This is because literature says that the prevalence of hypertension has increased by 30
times among the urban population over a period of 55 years and about 10 times
among the rural population over a period of 36 years. Dramatic changes in life style
from traditional to modern have lead to physical inactivity due to technological
advances. Rising affluence has modified the dietary pattern characterized by increased
consumption of diets rich in fat, sugar and calories.
Furthermore, increasing population growth at the current rate of about 2% in each
year and technological advances have shrunken the employment opportunities
particularly among young generation leading to stress and hypertension in young
persons, including students and laborers
As the company is also targeting a rollout market (Brazil), the major criteria are
market potential, the company’s local reputation, the cost of communication media
and competitive penetration.
HOW (introductory market strategy): The company must develop an action plan for
introducing the new product into the rollout markets. To coordinate the many
activities involved in launching a new product, management can use network planning
techniques. By estimating how much time each activity takes, the planners estimate
completion time for the entire project. Any delay in any activity on the critical path
will cause the project to be delayed. If the launch must be completed earlier, the
planner searches for ways to reduce time along the critical path.

Results
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 222
Discussion
DEPARTMENT OF PHARMCEUTICAL MARKETING AND MANAGEMENT Page 222
7. Discussion
The key difference between domestic marketing and marketing on an international
scale is the multi-dimensionality and complexity of the many foreign country markets
a company may operate in. Developing a new product and launching in the market is
time and resource consuming, as great care must be taken to ensure the best decisions
are made before the product reaches channel members and final consumers.
Once the company decides to target a particular country, it has to determine the best
mode of entry. Its broad choices are indirect exporting, direct exporting, licensing,
joint ventures and direct investment. The normal way to get involved in an
international market is through export. The company produces its goods in the
country and might or might not adapt them to international markets. Companies
typically start with indirect exporting that is they work through independent
intermediaries.
To enter the Brazilian market products such as pharmaceuticals, vitamins and medical
devices products, can be sold only if:
A) The foreign company establishes a local Brazilian manufacturing unit or local
office, fully responsible for its products; or
B) The foreign company appoints a Brazilian distributor, who has the registration
with the ANVISA as an importer and distributor of the types of products being
offered.
The first step a foreign company must take is to decide whether it is going to
commercialize its products, through the Brazilian distributor or through its own
structure in Brazil. With either option, the distributor has to be duly registered at
Discussion
DEPARTMENT OF PHARMCEUTICAL MARKETING AND MANAGEMENT Page 223
ANVISA and authorized to operate by the sanitary agencies both municipal and
federal jurisdiction.
After the company decides the way to enter the Brazilian market the company must
decide how much to adapt their marketing strategy to local conditions. Deciding on
the marketing program that is standardization of the product, communication and
distribution channels in the lowest costs is a challenging one. As the company is
tapping in Brazilian market where the local languages are Spanish and Portuguese,
sales promotion should be done taking language into consideration, so that accurate
understanding takes place in-between the middle men and the company as well as
with customers. For price structure there are regulations in Brazil for pharmaceutical
products which the company has to follow those and place a competitive price in the
market for its product. In Brazil a foreign company has to distribute its
pharmaceutical products through local distributors who are registered to ANVISA or
set up its own subsidiary and built its own marketing or sales team.
After management develops the product concept the next step is to conduct the
business analysis. Before making any estimates of expected sales it is important to
size up the opportunity. What is the size of the total market? Adding up the retail sales
volumes of all competitive products, the size of the total market can be found. What is
the extent of competition both direct and indirect? The indirect competition includes
all the products that can be used as substitutes for the same condition or indication.
From IMS health audit 2007 world wide. ARB ranked 8th amounting to a globle sales
of US$ 19.4 billion with a growth of 13.6% within the top therapeutic segment. Now
Discussion
DEPARTMENT OF PHARMCEUTICAL MARKETING AND MANAGEMENT Page 224
as per the domestic market survey, the direct competitor of Candesartan cilexetil is
Telmisartan followed by Losartan with hydrochlorothiazide. The major indirect
competitor is found to be drugs under ACE inhibitors, such as Ramipril followed by
Enalapril. There is another category of drugs which are also competing as an indirect
competitior which is Calcium channel blockers specially Amlodipine. So the
company has to develop their strategies on the basis of primary data.
The company also has to find out the growth trends of the market. From the
epidemiology study of hypertension it was found that hypertension is one of the major
risk factor for mortality and which is continuously increasing in both India and Brazil
as per WHO. So the potentiality to run a business in this particular sector is worth
while for an emerging company.
Once the firm has determined which markets to enter, the mode of entry and its goals
and objectives relative to international expansion, it next has to draw up operational
plans for marketing the product or service in the international market. All marketing
strategy is built on STP-Segmentation, Targeting and Positioning. The customer
segmentation has been done on the basis of the various doctor specialties that treat
hypertensive patients. The results of the primary market research indicate the presence
of three major segments, these are:
1. Cardiologists
2. General physicians
3. General practitioners
Discussion
DEPARTMENT OF PHARMCEUTICAL MARKETING AND MANAGEMENT Page 225
The results of the primary market research conducted among chemists indicate that
the Cardiologists and General physicians treat the maximum number of hypertensive
patients. This result is further augmented by the doctor’s survey that concluded that
the Cardiologists and General Physicians are the major prescribers for the categories
of drugs indicated for hypertension. Other than these two, General practitioners are
also prescribing ARB’s for hypertension but comparatively less than the above
mentioned two categories.
So an effort from the company’s scientific business development team is very much
necessary to create an awareness in doctors for their better effectiveness in
hypertensive patients.
Branding is an important aspect before positioning the product in customers mind.
The following is the proposed brand name for the product which will be available.
The brand name “CANDEBEAT-HCT” is coined from the parent molecule
Candesartan and Heartbeat. The part “CANDE” is taken from Candesartan and
“BEAT” from heart beat. Beat also means to defeat. So the brand name delivers a
message that the product can defeat hypertension if treated with it.
Once the competitive frame of reference for positioning has been fixed by defining
customer target market and nature of competition, the appropriate points of difference
(PODs) and points of parity (POPs) can be defined.
Candesartan cilexetil with Hydrochlorothiazide will be positioned for the treatment of
hypertension. Candesartan cilexetil is the only ARB currently licensed for the
treatment of heart failure which is an additional advantage of the molecule and will
help to develop more confidence in the doctors about the product. Unlike ACE
Discussion
DEPARTMENT OF PHARMCEUTICAL MARKETING AND MANAGEMENT Page 226
inhibitors Candesartan cilexetil does not inhibit the breakdown of bradykinin and are
therefore associated with a lower incidence of cough
Coming to the marketing strategies, a detailed tactical plan for marketing the new
product has to be made for both countries. The plan should cover all the details for the
launch year and be based on the core concept. For the proposed project development
of promotional materials, detailing by medical representatives and frequency of visits
and sampling pattern, training manual/product literature for the sales team, awarness
campaign for hypertension are the major components of marketing activities. The
detailing part for CANDEBEAT-HCT will focus upon the role of Candesartan
cilexetil in the treatment of hypertension as well as heart failure. Further, the detailing
story will involve the role of Hydrochlorothiazide in CANDEBEAT-HCT and how it
will enhance both doctors compliance.
In Brazil the promotional aspects will be different according to their country’s
promotional regulations. As the cost of investment in Brazil is very high for
promotion, the company has to invest very carefully. Company also has to decide
whether they will promote the product through local sales force in Brazil or should
teach their marketing people in its home ground and let it done by them.
The next step involves a jump in investment that dwarfs the costs incurred in the
earlier stages. At this stage the company will determine whether the product idea can
be translated into a technically and commercially feasible product.
The R&D department will develop the physical versions of the product concept of
Candesartan cilexetil with hydrochlorothiazie.
Discussion
DEPARTMENT OF PHARMCEUTICAL MARKETING AND MANAGEMENT Page 227
To introduce a major new product into the national and international market, the
company may have to spend a huge amount of money in advertising, promotion and
other communications in the first year. As per the survey carried out in domestic
market such as Kolkata and Bangalore the report says the awareness of the molecule
Candesartan cilexetil with hydrochlorothiazide in Kolkata is bit higher than Bangalore
and ARB’s are also being used in higher amount according to survey. So Kolkata is a
target city for the company. As Bangalore is the home town of the company it can be
the second choice. The company may also target 3 other metros such as Mumbai,
Delhi and Chennai. As the company is also targeting a rollout market (Brazil), the
major criteria are market potential, the company’s local reputation, the cost of
communication media and competitive penetration.
Conclusion
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 228
8. Conclusion
A strategy is like a route or road the company wants to take to reach its objectives. A
decision on strategy, therefore involves all aspects like the target audience, key
product attributes, allocation of resource-mix and the segment the company will
attack.
Market penetration and development strategies:
Market penetration and development suggests how the company will increase the
market share and profits of its new product in its own existing markets. Before
offering a new product in the market, the company must define its market. It is the
process by which products select the market in which they propose to operate.
Candesartan cilexetil with hydrochlorothiazide will be launched in the anti-
hypertensive drugs market. CANDEBEAT-HCT will be positioned for treatment of
hypertension and heart failure. The combination of hydrochlorothiazide with the
parent molecule will increase the synergy of the brand and will provide better market
penetration and enhance the market share in antihypertensive market.
CANDEBEAT-HCT will adopt market penetration strategy in the existing product
market, this will be achieved by deploying the following:
Hypertension is a highly prevalent risk factor for cardiovascular deaths and disability
worldwide. A study carried out in Brazil which reveled that cardiovascular diseases
are a leading cause of mortality, and systemic hypertension is a major risk factor. In
India it is directly responsible for 57% of all stroke deaths and 42% of coronary heart
Conclusion
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 229
disease deaths. It is also a leading cause of blindness, renal failure and congestive
heart failure. So, the cardiologists will be made aware to start therapy with
CANDEBEAT-HCT for better management of high blood pressure. The brand
CANDEBEAT-HCT have been specifically formulated for the patients who are not
tolerant to ACE inhibitors and are admitted for heart failure. But according to
literature the effects of ARBs in hypertension is probably a class effect. As the
molecule is the only licensed ARB for the treatment of heart failure and the condition
is one of the major causes of death in India as well as in Brazil, proper positioning
will help the company to attract customers from competitors and also will help the
product to penetrate in the market. As per the survey it is clear that doctors who
prescribed Candesartan for the treatment of hypertension showed a positive response.
But maximum of them have not used it, specially the general practitioners followed
by the general physicians. With respect to this aspect the company has to increase the
awareness of the molecule to the maximum extent which will help to develop its
market by changing the prescription habit.
So among the general physicians and general practitioners, the initial tactic will be to
promote the cumulative action of the brand CANDEBEAT-HCT. This will be done by
providing the latest scientific knowledge about the combination effect of the
molecule.
Operational strategies:
The operational strategy has been devised across product differentiation, product
positioning, targeting and segmentation strategy.
Conclusion
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 230
The product positioning will be done with respect to the product by explaining how
CANDEBEAT-HCT is different from other products in its and other categories.
After doing the primary survey in Kolkata and Bangalore, the results shows that the
molecule is a preferred one, but didn’t have a response to that extent in comparison to
Telmisartan and Losartan which are the top selling molecule in the ARB category.
The drug may not have higher plus points in comparison to Telmisartan but it has
some positive advantages in compared to it according to literature. Such as the
maintenance dose of Candesartan is less than Telmisartan and it is the only drug
licensed by US FDA for the treatment of hypertension and heart failure.
In comparison to Losartan, Candesartan has much higher superiority according to
literature survey. The plus points of Candesartan over Losartan are greater
bioavailability, long duration of action, less side effects and better efficacy.
The most preferred Calcium channel antagonist is Amlodipine as per the survey
carried out in both the above mentioned cities. Literature survey says that Candesartan
is better tolerated than Amlodipine
Focusing on the above aspects will help the brand for its better positioning in the
customers mind.
The customer segmentation has been done on the basis of the various doctor
specialties that treat hypertensive patients. The results of the primary market research
indicate the presence of three major segments, these are cardiologists, general
physicians and general practitioners
Conclusion
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 231
Promotional strategies:
Before the actual launch, a special task force will be created that will help to increase
the knowledge regarding the product among the various category of doctors
(especially targeting the cardiologists and the general practitioners). The initial
promotion of the products will be handled by the special task force which will help to
reinforce the credibility of the firm and the product among the doctors’ mind.
Continuing Medical Education (CME) programmes shall be conducted
simultaneously in the targeted states of India as a future strategy for product recalling.
The availability of the product will be ensured at chemist outlets and hospital
pharmacies before the actual prescription generation starts. The distribution channel
will be streamlined from the carrying and forwarding agent (C&F Agent) to the
distributors/ super-stockists and the retailer in India and in Brazil. Product handling
guidelines will be provided to all the elements across the distribution channel.
As part of new commercial model the company can focus on more targeted
communication to doctors through its representatives (if any in Brazil), e-detailing
and video detailing which can be useful for promoting the product in Brazilian
market. Extensive use of new media such as the internet can be implemented.
By identifying the sales promotion strategy, company will be able to align its plan
with the short-term incentives used to encourage prescription sales. If the company is
going to run a special campaign in the first three months of the launch, then the sales
team should be given some type of incentive to push that particular promotion (i.e.
discounts, rebates, samples), such as rewarding the reps with a specific dollar amount
Conclusion
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 232
for each prescription filled. If it is only being offered in a particular region, than that
also needs to be considered when devising national incentive compensation plan.
In order to measure the actual effectiveness of the strategy, the company must first
define success. Is it based on the number of samples distributed, coupons used or total
prescriptions sold? The strategy needs to incorporate different scenarios. By using
effective ways to model and forecast launch product performance they can optimize
the compensation plans and predict compensation expenses.
Awareness among the patients will be generated by providing scientific information
in layman language in the leading magazines which target the aged individuals and
young professionals. The campaign conducted by the company will also help to create
awareness in individuals which will help to recognize the initial symptoms of
hypertension and also make aware of pre-hypertension which is not a disease
category; rather it is a designation chosen to identify individuals at high risk of
developing hypertension and urge the patients to consult a doctor.
Investment strategies:
The investment option for the product will be; to enter and grow in the Brazilian and
Indian market for the treatment of Hypertension. There should be aggressive
promotion of the product and try and differentiate product from competitors, for
which substantial amount of cash inflow for the product will be needed. A product's
success during the first six months of a launch has a significant impact on sales over
the entire product life cycle. Therefore, it is critical to know the budget in order to
determine how much the sales team can be compensated for attaining certain goals.
Conclusion
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 233
Emphasis will also be laid on generating awareness programs among elderly
population and promoting diagnosis in the high risk population.
Launch program:
Before launching the products in the domestic market, test marketing can be an
option, but to make an impact in the market CABDEBEAT-HCT will be launched
countrywide at the same day (the preferred day will be World Heart Day). The launch
can also be integrated with the proposed Hypertension Awareness Conference; this
will further help to live up to the product hype created before the product launch.
The launch program shall include-details of the launch including the ambience setting,
the invitees, public relations arrangements, the guests of honor and any specific doctor
(specifically a key opinion leader). Before, the actual launch event it is always viable
to do dummy rounds of the whole launch program which will involve both the
scientific and the marketing activities.
The review of the launch strategy will be done on a constant basis and it will be a
function of the sales achieved for the products in a given time frame.
Finally taking every aspects concluded above, we can come to an idea that before
launching a product in the international and domestic market by the company, it has
to decide extensively in proper budgeting of the overall project for launching a new
product and come out with answers which are not covered in this proposed such as
how the company will do an cost effective branding and maintaining brand equity and
reasons behind competitors not promoting the molecule which are operating in
present market even though the molecule is having potential for the treatment of
hypertension.
Summary
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 234
9. Summary
Emerging from a highly protected economy and an insulated business environment,
many companies in India have come a long way in their quest to become global
players. To develop a new product and launching in the market is time and resource
consuming, as great care must be taken to ensure the best decisions are made before
the product reaches channel members and final consumers.
Therefore to launch a new product in the domestic and international market, some
important aspects such as analysis of targeted country, risks, cultural aspects,
competitors, deciding how to enter the market, deciding on the marketing programme,
development of the product and its commercialization, company financial status
should be extensively analyzed. The proposed study involves the consideration of all
the relevant aspects for the launch of a new brand of a combination product that is
Candesartan cilexetil with Hydrochlorothiazide in domestic and international markets.
It involves the development of tactics, plans and strategies which helps to introduce
the proposed new brand successfully. The apparent reasons for selecting Brazilian and
Indian market is due to their market growth of 13.4% and 13% respectively which is
higher in comparison to other major pharmaceutical markets, such as North America,
Europe and Japan according to IMS health report. The driving force behind the
growth is the rising consumption levels in both the countries.
The top 10 key pharmaceutical markets accounts for majority of sales amounting to
US$529.5 billion. The seven emerging markets such as China, Brazil, Mexico, South
Korea, India, Turkey and Russia has a growth by 12-13% (US$ 85-90 billion) in
2008.
Summary
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 235
Generic medicines continue to grow at a higher rate than overall pharmacy sales, and
are expected to represent 20% of the sector by volume in 2010.
Lifestyle drugs have become the leading segment for the Indian pharmaceutical
industry. Heart disease and diabetes are growing at 10.7% and CNS is growing at
4.9%. According to a recent McKinsey report, Indian pharmaceutical industry has the
potential to touch US$ 25 billion by 2010.
According to risk analysis Brazil comes out most favorable, scoring an overall
medium risk for dynamic risks – governance framework, political violence and
business and macroeconomic environment. It also has a medium risk profile for
structural risks such as supply chain risks, poverty, development, energy security and
vulnerability to climate change.
India is high risk for both dynamic and structural risks. Its poorer score compared to
Brazil can be attributed to significantly higher levels of terrorism, poorer regime
stability and higher levels of corruption. This will impact on future political risk.
The differences between social and cultural factors in different parts of the world can
be a central consideration in developing and implementing international marketing
strategies.
To enter the Brazilian market products such as pharmaceuticals, vitamins and medical
devices products, the company has to establishes a local Brazilian manufacturing unit
or local office, fully responsible for its products; or the foreign company appoints a
Brazilian distributor, who has the registration with the ANVISA as an importer and
distributor of the types of products being offered.
Summary
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 236
Candesartan cilexetil with hydrochlorothiazide belonging to the therapeutic category
antihypertensives will be introduced in the market by formulating an effective launch
strategy. .
The objectives of the study was to find out the prevalence of hypertension in Brazil
and India. To study the anti-hypertensive drugs market in the above mentioned
countries with special reference to Candesartan cilexetil with Hydrochlorothiazide
followed by the prescription trends for the treatment of Hypertension. And finally
preparing an effective launch strategy for a new brand of Candesartan cilexetil with
Hydrochlorothiazide in international and domestic market.
This open prospective and comparative study was conducted in Bangalore and
Kolkata. The survey was conducted amongst the doctors and chemists to explore the
anti-hypertensive drugs market with special reference to Candesartan cilexetil with
Hydrochlorothiazide and to find out the prescription trends for the treatment of
hypertension. The secondary data was obtained from Journals and internet. The
method of data collection was preliminary communication and personal interview
with doctors and chemists to get their consent to participate in the survey.
The sampling technique adopted was convenience sampling and the sample size was
100 doctors and 100 chemists in total from the cities. The data obtained was tabulated
and compared.
The results of the primary market research showed that the major competitors are
found to be ACE inhibitors where Ramipril followed by Enalapril is the top molecule
and with respect to ARBs, Telmisartan has the higher preference followed by
Summary
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 237
Losartan as per doctors preference and chemists sales experience. Amlodipine is the
preferred molecule among Calcium channel blockers. Diuretics are mainly have
preference for higher age groups. With respect to combination therapy the above
mentioned categories of drugs with Diuretics are the competitors. Combinations other
than the mentioned ones above, includes Calcium channel antagonist with ACE
inhibitors and ACE inhibitor with ARB which will also be a competitor in Kolkata
and Bangalore respectively.
With respect to Candesartan, the molecule has a very low preference in the market but
doctors specially the cardiologist has a good impression on this particular molecule.
But maximum doctors have not prescribed this molecule and also within them the
awareness of the molecule is not there. As per chemists over view about the molecule,
in Bangalore the molecule has very low market but Kolkata do have higher market
with respect to Bangalore.
The market analyses identified the following key competency areas required for
success of the product such as:
1. Recognizing the right segment, that is the anti-hypertensive market and
targeting the doctors specially the Cardiologists, General physicians and
General practitioners who will generate the maximum number of
prescriptions.
2. Customizing the product according to the requirement of segment and needs
of the customer.

Summary
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 238
3. Promotion strategy should emphasize on contrasting the efficacy and benefits
of the proposed product. In this proposed project the promotional strategy
followed here are, visual aid preparation, making an awareness campaign for
hypertension.
Bibliography
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 239
10. BIBLIOGRAPHY
1. Kotler Philip, Keller Kevin Lane , Koshy Abraham , Jha Mithileswar,
Marketing and management, a south asian perspective, 12th ed. India: India
Dorling Kindersley Pvt. Ltd, Copyright © 2007
2. Daole Isobel, Lowe Robin. International marketing strategy.2nd ed.
Singapore: Thomson Learning; Copyright ©1999
3. Hoffman K. Douglas, Czinkota Michael R, Dickson Peter R, Dunne Patrick,
Griffin Abbie, Hutt Michael D et al. Marketin best practices, 2nd ed. South-
Western division of Thomson Learning, Copyright © 2003
4. Douglas Susan P, Craig C. Samuel, Global marketing strategy, international
edition, McGraw-Hill, Inc. Copyright © 1995
5. Aaker D.A. Strategic marketing management, John Wiley and Sons Asia Pvt.
Ltd, ©2000
6. Öhman K.P, Milon H. and Valnes K. , Candesartan cilexetil-HCT in primary
hypertension insufficiently controlled on monotherapy a comparison with
losartan-HCT, American journal of hypertension [Online] Abstract number
(A069). 2010 Available from: URL:
http://www.nature.com/ajh/journal/v13/n2s/abs/ajh2000564a.html
7. Mcinnes G.T.; Istad H.; Keinänen-Kiukaanniemi S.; Van Mierlo
H.F.C.M.Blood Pressure, Volume 9, Supplement 1, 15 May 2000 , pp. 61-
61(1)
Bibliography
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 240
8. Greg L. Plosker, Susan J. Keam ; Candesartan Cilexetil: A
Pharmacoeconomic Review of its Use in Chronic Heart Failure and
Hypertension. Journal Pharmaco Economics [Online] 2006 Dec; Available
from: URL: http://ideas.repec.org/a/wkh/phecon/v24y2006i12p1249-
1272.html
9. Roberto Fogari, Amedeo Mugellini , Giuseppe Derosa ; Efficacy and
tolerability of candesartan cilexetil/hydrochlorothiazide and amlodipine in
patients with poorly controlled mild-to-moderate essential hypertension.
Journal of Renin-Angiotensin-Aldosterone System [Online] 2007; Vol. 8,
No. 3, 139-144, Available from: URL:
http://jra.sagepub.com/cgi/content/abstract/8/3/139
10. Bertram G. Katzung, Susan B. Masters, Anthony J. Trevor. Basic clinical
pharmacology,11th ed, The McGraw-Hill Companies, Copyright © 2007
11. Mohan Harsh . Essential Pathology for Dental Students, 2nd ed. Jaypee
Brothers Medical Publishers (P) Ltd; © 2002
12. Atacand HCT ® (candesartan-cilexetil-hydrochlorothiazide) Tablets,
AstraZeneca group of companies [Online] 2009 Available from: URL:
http://www1.astrazeneca-us.com/pi/atacandhct.pdf
13. Thomas Mengden, Sakir Uen, Peter Bramlage. Management of hypertension
with fixed dose combinations of candesartan cilexetil and hydrochlorothiazide:
patient perspectives and clinical utility, November 2009, Volume 2009:5,
Available from: URL: http://www.dovepress.com/management-of-
Bibliography
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 241
hypertension-with-fixed-dose-combinations-of-candesartan-peer-reviewed-
article-VHRM
14. Dr Peter A. Meredith. Candesartan cilexetil – a review of effects on
cardiovascular complications in hypertension and chronic heart failure, 2007,
Vol. 23, No. 7, Pages 1693-1705, Available from URL:
http://informahealthcare.com/doi/abs/10.1185/030079907X210723
15. CIMS, Malleswaram Bangalore, CMPMedica India Private Limited, 2008.
P.103
16. L Ala, G Gill, R Gurgel, L Cuevas. Evidence for affluence-related
hypertension in urban Brazil, Journal of Human Hypertension, 2004 June 24,
775–779. doi:10.1038/sj.jhh.1001750, Available from URL:
http://www.nature.com/jhh/journal/v18/n11/full/1001750a.html
17. Gupta Rajeev, Gupta V. P. Hypertension epidemiology in India: lessons from
Jaipur Heart Watch, Current Science, 2009 August 10, Vol. 97, No. 3,
Available from URL: http://www.ias.ac.in/currsci/aug102009/349.pdf
18. Country profile Brazil. [Online]; 2005 May, [17 screens], Available from
URL: www.cygnusindia.com
19. EDC Brazil [online]. 2009 July; [2screens]. Available from URL:
http://www.edc.ca/english/docs/gbrazil_e.pdf
20. Global Pharmaceuticals. [Online]; 2008 July, [36 screens], Available from
URL: www.cygnusindia.com
21. Maria Ines et al. Prevalence of diabetes and hypertension based on self-
reported morbidity survey, Brazil, 2006. Rev. Saúde Pública [Online]. 2009,
Bibliography
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 242
vol.43, suppl.2, pp. 74-82. Available from URL:
http://www.scielosp.org/pdf/rsp/v43s2/en_ao801.pdf
http://www.scielosp.org/scielo.php?pid=S003489102009000900010&script=s
ci_arttext&tlng=en 22. Pharmaceuticals Industry Insight. [Online]; 2009 Jan, [242 screens],
Available from URL: www.cygnusindia.com
23. Portilho Deborah, Gosain Rana. The Pharmaceutical IP Environment in Brazil
[Online] 2007 [6 screens]; Available from URL:
http://www.daniel.adv.br/eng/artigos/rana/THE_PHARMACEUTICAL_IP_E
NVIRONMENT_IN_BRAZIL.pdf
24. Federation of Indian Chambers of Commerce and Industry. Current state of
Indian Economy. [Online] 2009 Sep [12 screens]; Available from URL:
http://www.indiainbusiness.nic.in/indian-economy.pdf
25. EDC India [Online]. 2009 November; [2screens]. Available from URL:
http://www.edc.ca/english/docs/gindia_e.pdf
26. Priolkar Subodh. Can India be Pharmaceutical Superpower in 2020?. [Online]
2009 Jan; [6 screens]. Available from URL:
http://www.ipapharma.org/pt/January_2009/Can%20India%20be%20Pharmac
eutical%20Supperpower%20in%202020.pdf
27. Ram Kumar Ashok. Impact of TRIPS on Indian Pharma. [Online] 2009
December 11 [2004 December 02]; [1 screen]. Available from URL:
http://www.pharmabiz.com/article/detnews.asp?articleid=25005§ionid=5
0
Bibliography
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 243
28. Maplecroft. New analysis of dynamic and structural political risk identifies
opportunities in the BRICs. [Online]. 2009 [5 screens]. Available from URL:
http://www.maplecroft.com/Political_Risk_Media_Release.pdf
29. Coface North America. Brazil Country Risk Overview. [Online] 2008; [8
screens]. Available from URL:
http://www.cofaceusa.com/CofacePortal/US_en_EN/pages/home/risks_home/
country_risks/country_file//Brazil?nodeUid=572099
30. William W. Dressler, José Ernesto dos Santos. Social and cultural dimensions
of hypertension in Brazil: a review. [Online]. 2000; [13 screens]. Available
from URL: http://www.scielosp.org/pdf/csp/v16n2/2081.pdf
31. Todkar SS, Gujarathi VV, Tapare VS. Period prevalence and
sociodemographic factors of hypertension in rural Maharashtra: A cross-
sectional study. Indian J Community Med [serial online] 2009 [cited 2010 Mar
1st]; 34:183-7. Available from
URL: http://www.ijcm.org.in/text.asp?2009/34/3/183/55269
32. Ravi Sankar P, Partha Praveen, Shenoy Mister Nagesh. Prescribing patterns of
drugs among patients admitted with cardiovascular disorders in the internal
medicine ward: Prescribing patterns in inpatients. The Internet Journal of
Pharmacology [serial online] 2009 [cited 2010 Feb 09]; 14:01:44. Available
from URL:
http://www.ispub.com/journal/the_internet_journal_of_pharmacology/volume
_1_number_2_53/article/prescribing_patterns_of_drugs_among_patients_adm
Bibliography
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 244
itted_with_cardiovascular_disorders_in_the_internal_medicine_ward_prescrib
ing_patterns_in_inpatients_1.html
33. Drug update angiotensin II receptor antagonists. [Online] 2005 May.
Available from URL:
http://www.nyrdtc.nhs.uk/docs/dud/DU_42_Angiotensin_II_a.pdf
34. Barreras Amy, Turner Gurk Cheryle. Angiotensin II receptor blockers. 2003
Jan ;16:123–126. Available from URL:
http://www.baylorhealth.edu/proceedings/16_1/16_1_barreras.pdf
35. Leonidas C. Leonidou, Constantine S. Katsikeas, and Nigel F. Piercy,
“Identifying Managerial Influences on Exporting: Past Research and Future
Directions,” Journal of International Marketing 6, no. 2 (1998): 74 – 102
36. Changanti Subba Rao. Pharmaceutical Marketing in India, first edition. Gitam
institute of foreign trade, Copyright © 2005, P. 42 – 43
37. Uehara G, Takeda H. Relative effects of telmisartan, candesartan and losartan
on alleviating arterial stiffness in patients with hypertension complicated by
diabetes mellitus: an evaluation using the cardio-ankle vascular index. J Int
Med Res. 2008 Sep-Oct; 36(5):1094-102. Available from URL:
http://www.ncbi.nlm.nih.gov/pubmed/18831906?itool=EntrezSystem2.PEntre
z.Pubmed.Pubmed_ResultsPanel.Pubmed_RVDocSum&ordinalpos=18
38. Sjolie A. K., Klein R, Chaturvedi N, Porta M, Fuller J, Orchard T. The Effect
of the Angiotensin Receptor Blocker Candesartan on Regression of
Retinopathy in Type 2 Diabetes. [Online]. 2009; [1 screen]. Available from
URL:
Bibliography
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 245
http://abstracts.iovs.org/cgi/content/abstract/50/5/1679?maxtoshow=&HITS=1
0&hits=10&RESULTFORMAT=1&author1=sjolie&andorexacttitle=and&and
orexacttitleabs=and&andorexactfulltext=and&searchid=1&FIRSTINDEX=0&
sortspec=relevance&resourcetype=HWCIT,HWELTR

Annexure
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 246
11. ANNEXURES
Annexure
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 247
List of Doctors Surveyed in Bangalore
Sl. No. Name (CARDIOLOGISTS) Location 1. Dr. A Gopi Apollo Hospital
2. Dr. Balram Sri Jayadeva Institute of Cardiology
3. Dr. B G Baliga Cardiac Care Centre, Jayanagar
4. Dr. B Kumar K R Hospital
5. Dr. B Ramesh Sri Jayadeva Institute of Cardiology
6. Dr. B Srinivas Sri Jayadeva Institute of Cardiology
7. Dr. Jaya Prakash Jaya Prakash Clinic, Bansankari
8. Dr. Joshwa Sri Jayadeva Institute of Cardiology
9. Dr. Harsha Jeevan Sri Jayadeva Institute of Cardiology
10. Dr. H. R Jagdish Sri Jayadeva Institute of Cardiology
11. Dr. K B Prasad Apollo Hospital
12. Dr. K R Samsundar Sagar Hospital
13. Dr. M. R Prasad Sri Jayadeva Institute of Cardiology
14. Dr. Mahesh B. V Vinayaka Hospital
15. Dr. N. G Shivaswamy Sri Jayadeva Institute of Cardiology
16. Dr. Narendra Kori Sri Jayadeva Institute of Cardiology
17. Dr. Nagesh Sri Jayadeva Institute of Cardiology
18. Dr. Nagesh Vinayaka Hospital
19. Dr. N Sridhar Wockhard Hospital
20. Dr. N M Prasad Sri Jayadeva Institute of Cardiology
21. Dr. Prabhabati Sri Jayadeva Institute of Cardiology
22. Dr. Santosh Sri Jayadeva Institute of Cardiology
23. Dr. Satish Sri Jayadeva Institute of Cardiology
24. Dr. S Venkatesh Wockhard Hospital
25. Dr. T R Raghu Sri Jayadeva Institute of Cardiology
Annexure
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 248
Sl. No. Name (GENERAL PHYSICIANS)
Location
1 Dr. Addis Jayanagar General Hospital
2 Dr. B P Allan Hari Pandu Hospital
3 Dr. Chandrasheker Chiranjeevi Clinic
4 Dr. Mahesh P Shiva Specialist Clinic
5 Dr. Prasanna Kumar Apollo Clinic Bangalore, Koramangala
6 Dr. Ravindra Victoria Hospital
7 Dr. Saroja Jayanagar General Hospital
8 Dr. S N Mohan K R Hospital
9 Dr Susma Nagesh Poly Clinic
10 Dr.K.Sukumar Shetty Bangalore Hospital
11 Dr.Sandip Malli Bangalore Hospital
12 Dr. Vijaya Vardhan Apollo Clinic Bangalore, Koramangala
Sl. No. Name
(GENERAL PRACTITIONERS) Location
1 Dr. Amarnath Victoria Hospital
2 Dr. Anitha KIMS
3 Dr. Deepti KIMS
4 Dr. Kesava Sri Srinivas Nursing Home
5 Dr. Murthy Pandu Hospital
6 Dr. Satish Kumar Jain Padmashree Clinic
7 Dr. Santosh Jeevana Deepa Hospital
8 Dr. S Sridhar Sri Srinivas Nursing Home
9 Dr. Srinivas Sri Srinivas Nursing Home
10 Dr. Sowmya Shree KIMS
11 Dr Eshwari Prasad Ashwin Family Health Clinic
12 Dr. Manjunath Cubbonpet
13 Dr.Ganesh Prasad Kamath Rajarajeswari Hospital
Annexure
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 249
List of chemists surveyed in Bangalore
Sl. No. Name Location
1. Santhosh Medicals Hanumathanagar
2. Med Plus Ramamurthynagar
3. Sri Gurudev Medical Centre Ramamurthynagar
4. B K Medicals Ramamurthynagar
5. Murthy Medicals V V Puram
6. Ram Medicals Nagartpost
7. Apple Pharma Jayanagar
8. Shree Lakshmi Pharma Basavanagudi
9. Venus Medicals Doddamavalli
10. Divine Medicals BTM Layout
11. Manjunatha Medicals Lalbagh Fort Road
12. Jagannath Medicals SBM Colony
13. Prime Pharma V V Puram
14. Sree Balaji Medicals Corporation, Market
15. Gupta Medicals Bansankari
16. Sree Manjunatha Medicals V V Puram
17. Medplus SBM Colony
18. Sapthagiri Medicals Lalbagh Road
19. Nataraj Medicals Vijayanagar
20. Manoj Medicals Cox Town
21. Apollo Pharma Jayanagar
22. Eshwar Medicals R T Nagar
23. Apollo Pharma Bansankari
24. Maruthi Medicals J P Nagar
25. Chetak Pharma Residency Road
Annexure
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 250
Sl. No. Name Location
26 Om Medicals BTM II Stage
27 Trust Cmemist and Druggists BTM II Stage
28 Anand Medicals Jayanagar
29 Lifetime Health Care Hanumanthanagar
30 Trust Cmemist and Druggists Mabanahalli
31 Balaji Medicals J C Nagar
32 Sahay Chemists and Druggists Bellandur
33 The Consumer’s Pharma Basavanagudi
34 Medplus Basavanagudi
35 Essar Pharma R T Nagar
36 Yash Pharma Residency Road
37 Medplus Hanumanthanagar
38 Mamta Medicals Srinagar
39 Sagar Pharma Srinagar
40 Balaji Pharma Residency Road
41 Vasavi Medicals Kengeri
42 Maruthi Medicals Vijayanagar
43 Shreya Medicals K S Town
44 Shreaa Medicals BTM Layout
45 Sri Naresh Pharma Srinagar
46 Master Medicals Srinagar
47 Durga Medicals J P Nagar
48 Medplus J P Nagar
49 Apollo Pharma Shivajinagar
50 Apollo Pharma Yelanka
Annexure
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 251
List of Doctors Surveyed in Kolkata
Sl. No. Name (CARDIOLOGISTS) Location
1 Dr. Asit Kumar Satpati Cittaranjan National Medical Hospital
2 Dr. Asis Kumar Mondal Cittaranjan National Medical Hospital
3 Dr. A.K. AgarwaL Peerless Diagnostic
4 Dr. A.K Bardhan Woodlands Hospital
5 Dr. A.K. Mahapatra Aram Clinic (Boubazar)
6 Dr. Anjan Lal Dutta Nightingale Diagnostic Centre
7 Dr. B Halder N R S Medical Hospital
8 Dr. Bhabotosh Biswas Peerless Hospital
9 Dr. C.C. Kar A.G. Hospital & Research Centre
10 Dr. Debal Sen Woodlands Hospital
11 Dr Dhiman Kahali Kolkata Medical Hospital
12 Dr. J. Maitra Kolkata Medical Hospital
13 Dr. K Ganguly N R S Medical Hospital
14 Dr. K.K. Mitra Kolkata Medical Hospital
15 Dr. Sunil Sarkar R.N. Tagore Medical Research Institute
16 Dr. Mrinal Kanti Das Lala Lajpat Rai Sarani
17 Dr. P K Biswas Burdwaman Medical Hospital
18 Dr. R K Sharma Cittaranjan National Medical Hospital
19 Dr. Sadhan Roy B.M. Birla Heart Research Centre
20 Dr. S Mandal Cittaranjan National Medical Hospital
21 Dr. Suchet Mukherjee N R S Medical Hospital
22 Dr. Subhanan Roy Apollo Hospital
23 Dr. Sibananda Dutta N R S Medical Hospital
24 Dr. Suvro Banerjee Kolkata Medical Hospital
25 Dr. Tapas Roychowdhury B.M. Birla Heart Research Centre
Annexure
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 252
Sl.No.
Name (GENERAL PHYSICICANS)
Location
1 Dr. A. K Bera Cittaranjan National Medical Hospital
2 Dr. A. K Kundu Cittaranjan National Medical Hospital
3 Dr. Amitava Chatterjee Kolkata Medical Hospital
4 Dr. M.Banerjee N R S Medical Hospital
5 Dr. Mani Chetri A.M.R.I.(Near Dhakuria Bridge)
6 Dr. N.Karmakar N R S Medical Hospital
7 Dr. Sanjay Banerjee N R S Medical Hospital
8 Dr. S Banerjee N R S Medical Hospital
9 Dr.Samar Banerjee N R S Medical Hospital
10 Dr. Subhashish Ganguly Venus Diagnostic
11 Dr. Salil Pal N R S Medical Hospital
12 Dr. U S Ghosh N R S Medical Hospital
Sl.No.
Name (GENERAL PRACTITIONER)
Location
1 Dr. Amlan Banerjee K.D. Cure Nursing Home
2 Dr. Anraj Singh Asia Rescue & Medical Services
3 Dr. B Chatterjee Cittaranjan National Medical Hospital
4 Dr. B Sarkar Cittaranjan National Medical Hospital
5 Dr. Debasis Das Cittaranjan National Medical Hospital
6 Dr. Debobroto Nandi N R S Medical Hospital
7 Dr. Manjul Kr. Roy Kolkata Medical Hospital
8 Dr. Mousumi Dutta Matrimoyee Medicals
9 Dr. Ranjit Das Cittaranjan National Medical Hospital
10 Dr. Sayantan Banerjee Kolkata Medical Hospital
11 Dr. Santi Saha Kalindi, CESC staff Quarter
12 Dr. Shashwata Tuhi Annada Neogi Lane
13 Dr. Vijay Mehta Apsara Building,
Annexure
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 253
List of chemists surveyed in Kolkata Sl. No. Name Location
1. Roy Clinic Behala
2. Blue Print Esplanade
3. Apollo Pharmacy Bagha Jatin
4. Drug Point Pharmacy Shyambazar
5. Dey's Medical Hall Shobhabazar
6. Bengal Medical Hall Salkia
7. Frank Ross Pharmacy New Alipore
8. Central Medical Stores Beadon Street
9. Chowranghee Blue Print New Market,
10. Kothari Medical Centre Alipur
11. Dhanwantary Medical Shop Hazra Road
12. Astha Bangur Avenue
13. Rejuv Pharmacy Bidhan Nagar (Salt Lake)
14. The Relife Pharmacy New Alipore
15. Gemini Pharmacy Barobazar
16. Health Pharmacy Dhakuria
17. Medica Pharmacy Regent Park
18. Medina Pharmacy Jodhpur Park
19. Deys Clinic Pharmacy Jadavpur
20. Samcon Pharmacy Bow Bazar
21. Seetal Pharmacy Kankurgachi
22. Wardex Aarogya Pharmacy Dhakuria
23. Adeline Pharmacy Joka, Kolkata
24. Medi-aid Pharmacy Shreebhumi
25. Medicon Pharmacy Baguihati
26. Medicos Pharmacy Bhawanipur
Annexure
DEPARTMENT OF PHARMACEUTICAL MARKETING AND MANAGEMENT Page 254
Sl. No. Name Location
26 Medicus Pharmacy Dum Dum, Kolkata
27 Vintage Pharmacy Park Street
28 Blue Sky Pharmacy Dum Dum, Kolkata
29 Deepneel Pharmacy Belgachia
30 Gadadhar Pharmacy Hati Bagan
31 Apollo Pharmacy Barahanagar
32 Apollo Pharmacy Barasat
33 Apollo Pharmacy Barrackpore
34 Apollo Pharmacy E.M Bypass
35 Medicino Pharmacy New Alipore
36 G D Enterprise Park Circus
37 Sarada Medical Jessore Road
38 Sarkar Medicine Park Circus
39 Blue Print Sealdah
40 Ma Sarada Pharmacy Jessore Road
41 Chandra Prova Medicals Jessore Road
42 Roy Medicals Jessore Road
43 Deepali Drugs Park Circus
44 Ramkrishna Medicals Shyambazar
45 Dey’s Medical Shyambazar
46 Nirmal Medical Nagendra Nath Road
47 Apollo Pharmacy Nagerbazar
48 Jibandeep Pharmacy Nagerbazar
49 GM Stores Pharmacy Dalhousie
50 Jibandeep Pharmacy Kalighat
Page 217
* ABC Journal of Hypertension Page 218
Rx
Candesartan cilexetil 16mg + Hydrochlorothiazide 12.5mg TabletsCandesartan celexitil 32mg + Hydrochlorothiazide 12.5 mg TabletsCandesartan cilexetil 32mg + Hydrochlorothiazide 25 mg Tablets
Candesartan celexitil works by blocking the action of a hormone called angiotensin II
with Hydrochlorothiazide
New combination
IndicationsHypertensionHeart failure
1. (www.patienthealthinternational.com)
®
1
Page 219
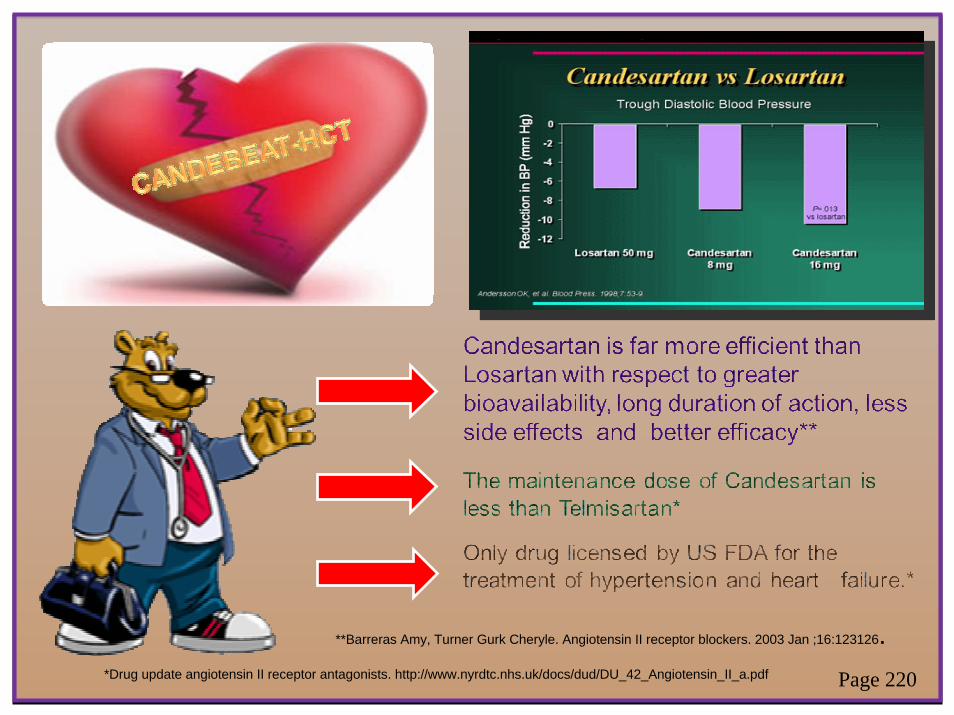
**Barreras Amy, Turner Gurk Cheryle. Angiotensin II receptor blockers. 2003 Jan ;16:123126.*Drug update angiotensin II receptor antagonists. http://www.nyrdtc.nhs.uk/docs/dud/DU_42_Angiotensin_II_a.pdf Page 220

Rx
Better tolarated than LISINOPRIL-HCT and AMLODIPINE
Effective and well tolerated in patients with essential hypertension, including elderly patients
2. Blood Pressure, Volume 9, Supplement 1, 15 May 2000 , pp. 61-61(1)3. Journal of the renin-angiotensin aldosterones syatemISSN 1470- 3203 Source / Source, 2007)4. Journal of human hypertension, Volume 13, Supplement 1, Pages S27S31
®
2 34
Page 221
Recommended










![partial] fulfillment Town](https://img.pdfslide.us/doc/110x75/61cbd0e20c1fcf7e016f4ea2/partial-fulfillment-town.jpg)






