Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Immune Hemolytic Anemia
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Introduction
• Immune hemolytic anemia (IHA)
–RBCs destroyed prematurely by immune process mediated by antibody and/or complement
–Presence and severity of anemia depends on:
Severity of hemolysis
Ability of BM to compensate for RBC loss
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Introduction
• Immune hemolytic anemia (IHA)
– Initial confirmation of immune mechanism
Demonstration of attachment of Ab or complement to RBCs of patient
–Diagnosis of anemia:
↓ Hb and Hct, ↑ reticulocytes and/or unconjugated bilirubin,
↓ haptoglobin
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Classification of IHAs
• Based on stimulus for antibody production
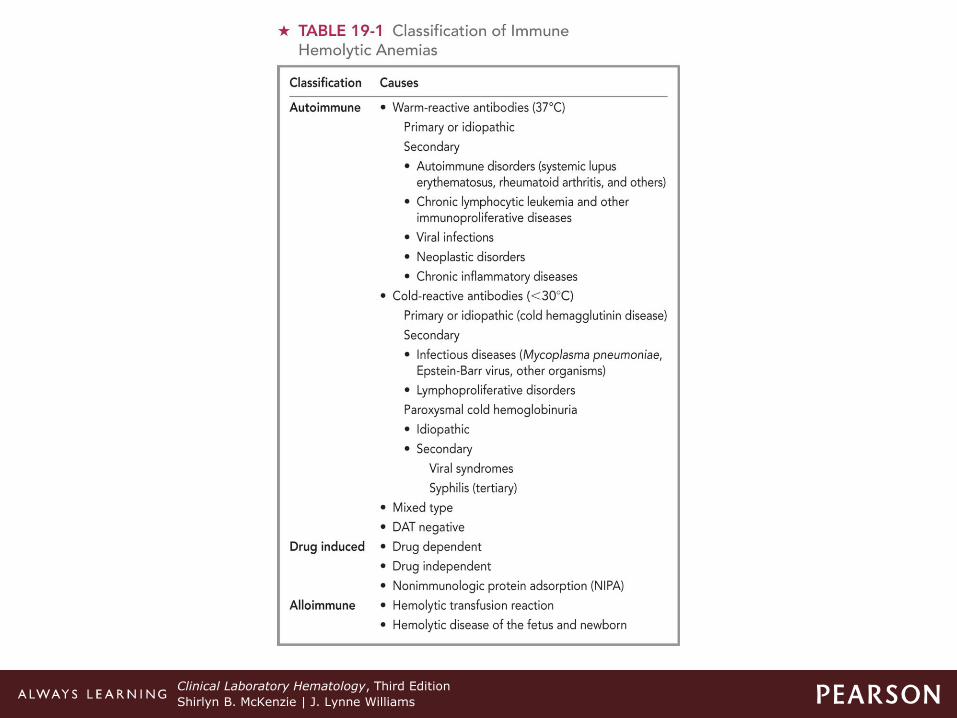
–Autoimmune hemolytic anemia
–Drug-induced hemolytic anemia
–Alloimmune hemolytic anemia
• Important to determine process because each type requires specific treatment
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Classification
• Autoimmune hemolytic anemia (AIHA)
–Shortened RBC survival
–Caused by production of autoantibodies against RBC antigens
–Ab-induced reactions include
Sensitization, agglutination, hemolysis
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Classification
• Autoimmune hemolytic anemia (AIHA)
–Further classified
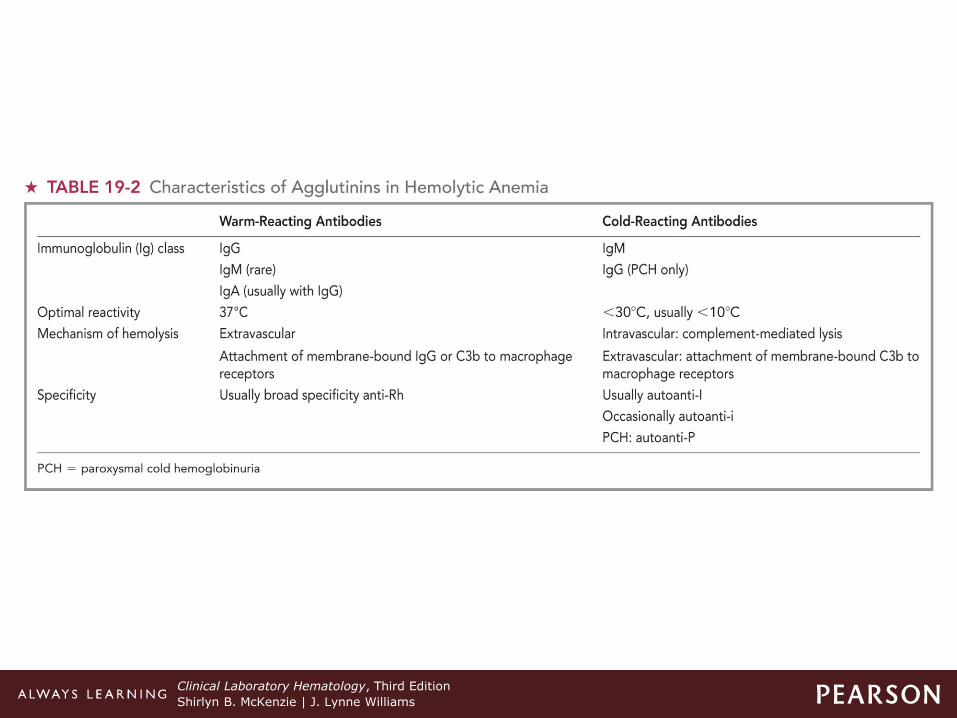
Warm-antibody autoimmune HA (WAIHA)
Cold-antibody AIHA (cold agglutinin disease/CAD)
Mixed-type AIHA (both warm-reacting and cold-reacting autoantibodies)
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Table 19-1 Classification of Immune Hemolytic
Anemias
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Table 19-2 Characteristics of Agglutinins in Hemolytic Anemia
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Classification
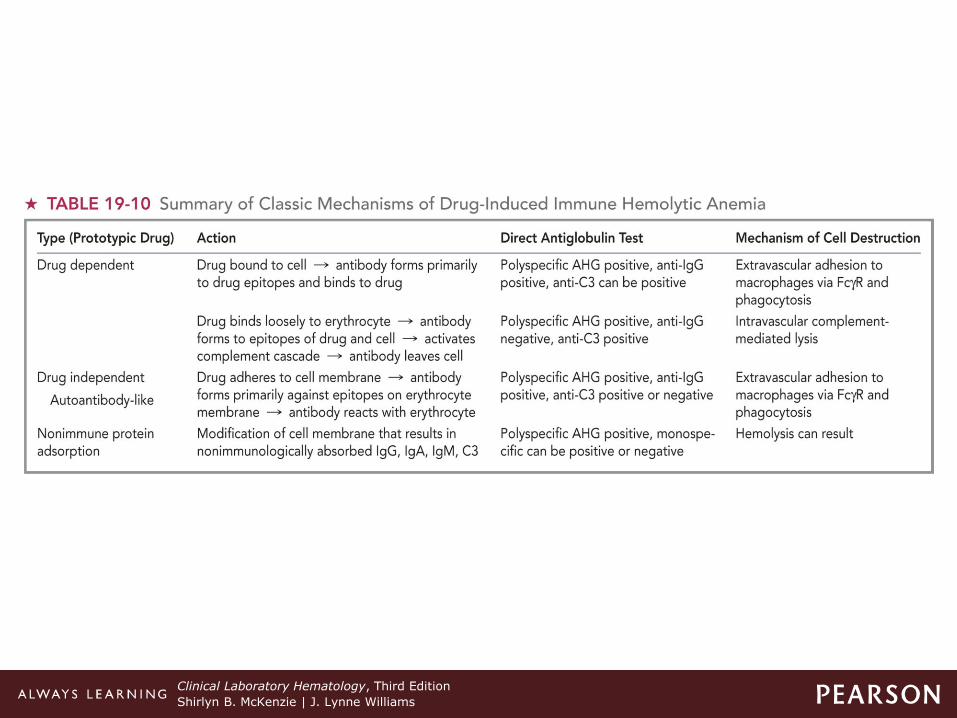
• Drug-induced hemolytic anemia
–Drugs attach to RBC membrane or alter it.
–Classified based on reactions of patient's RBCs and drug in vitro test system
Drug-dependent
Drug-independent
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Classification
• Alloimmune hemolytic anemia
–Antibody (Ab) development to RBC antigen (Ag) that individual lacks
Do not react with individual's own RBCs
HDFN-mother makes Abs against Ags on fetal RBCs
Transfusion reactions where recipient makes Abs to Ags on transfused (donor cells)
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Sites and Factors that Affect Hemolysis
• Intravascular or extravascular hemolysis
–Depends on:
Class of Ab
Ability to fully activate complement cascade
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Sites and Factors that Affect Hemolysis
• Intravascular or extravascular hemolysis
–Extravascular hemolysis
Most common
RBC sensitized with Ab or complement
Sensitized cells phagocytized by macrophages in spleen or liver
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Sites and Factors that Affect Hemolysis
• Intravascular or extravascular hemolysis
– Intravascular hemolysis
Complement cascade activated → C9 (MAC) → RBC lysis
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
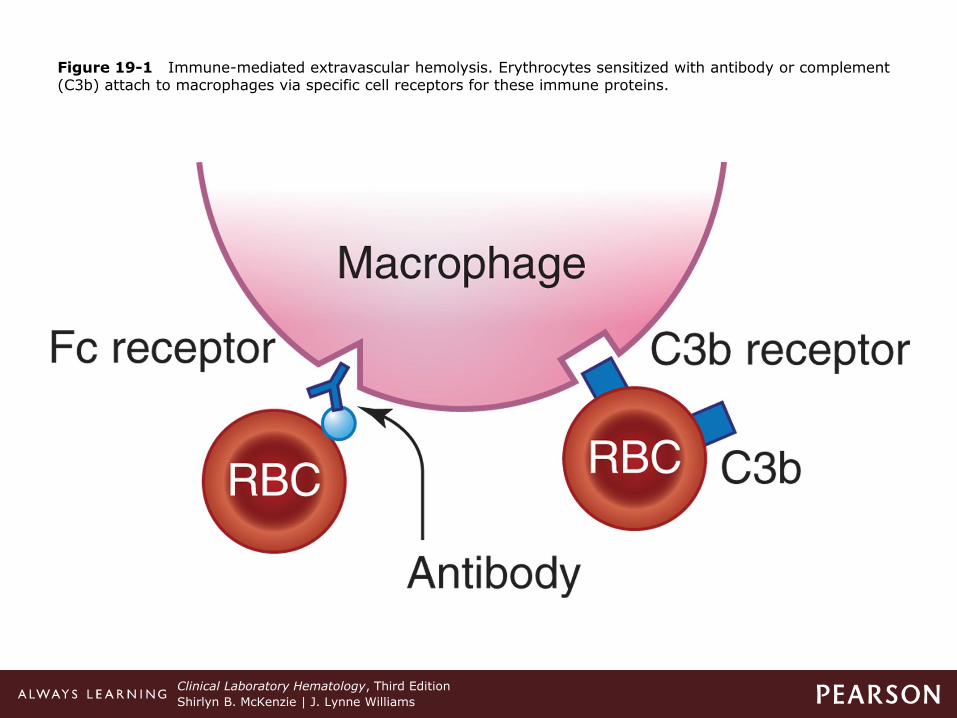
Figure 19-1 Immune-mediated extravascular hemolysis. Erythrocytes sensitized with antibody or complement (C3b) attach to macrophages via specific cell receptors for these immune proteins.
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
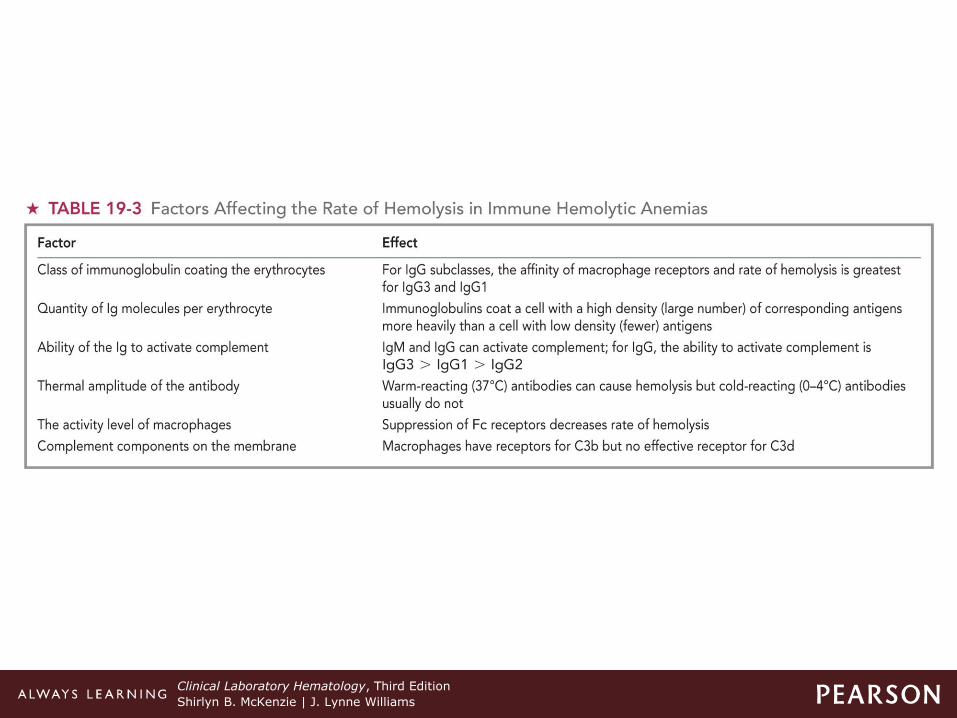
Table 19-3 Factors Affecting the Rate of Hemolysis in Immune Hemolytic Anemias
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Mechanisms of Hemolysis
• Based on whether IgM, IgG, and/or complement are present on RBC
• Three types:
– IgG-mediated
–Complement-mediated
– IgM-mediated
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
IgG-Mediated Hemolysis
• IgG attaches to RBC membrane Ags via Fab region.
• Fc receptors
–FcγR-I, -II, -III on macrophages of spleen
–Bind to Fc portion of Ab attached to RBC
–Macrophage pits the Ag/Ab complex
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
IgG-Mediated Hemolysis
• Fc receptors
–Damages RBC membrane
–RBC membrane reseals itself
–Repeated splenic passage—continues to lose membrane, forms spherocyte
Phagocytized by splenic macrophages
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
IgG-Mediated Hemolysis
• Ab-sensitized RBCs can be entirely engulfed by:
–Macrophages
–PMN (FcγR-I, -III)
• NK cells (FcγR-III)—results in ADCC (Ab dependent cell-mediated cytotoxicity)
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
IgG-Mediated Hemolysis
• Spleen
– Lightly opsonized cells more efficiently removed
• Liver
–Removes heavily sensitized cells
• Splenomegaly is common
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Complement-Mediated Hemolysis
• Role of complement
–Sensitization
Only portion of complement cascade activated and deposited on RBC membrane
– Lysis of RBCs
Entire complement system activated and deposited on RBC membrane
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Complement-Mediated Hemolysis
• Initiation of complement activation
–Classic, alternate, lectin mechanisms
• Classic pathway
– Initiated by Ag/Ab reaction
IgM
–Activates complement more efficiently
–Only requires one IgM molecule
IgG (IgG1 and IgG3; occasional IgG2)
–Activation requires two IgG molecules
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Complement-Mediated Hemolysis
• Cascade initiated
–C1 binds to the Fc region of IgG or IgM.
–Activates C4, C2, C3
–Activates the terminal components C5 to C9
Membrane attack complex (MAC)
–Lytic attack to RBC membrane
–Intravascular hemolysis when complement activation C1→C9 is complete
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Complement-Mediated Hemolysis
• Cascade initiated
–Activations through C3
RBC sensitized with C3b
–Totally or partially engulfed by macrophages with receptors for C3b
C3b on RBC cleaved by plasma C3b inactivator
C3c dissociates from membrane.
C3d no receptors on macrophages
–Normal RBC survival
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
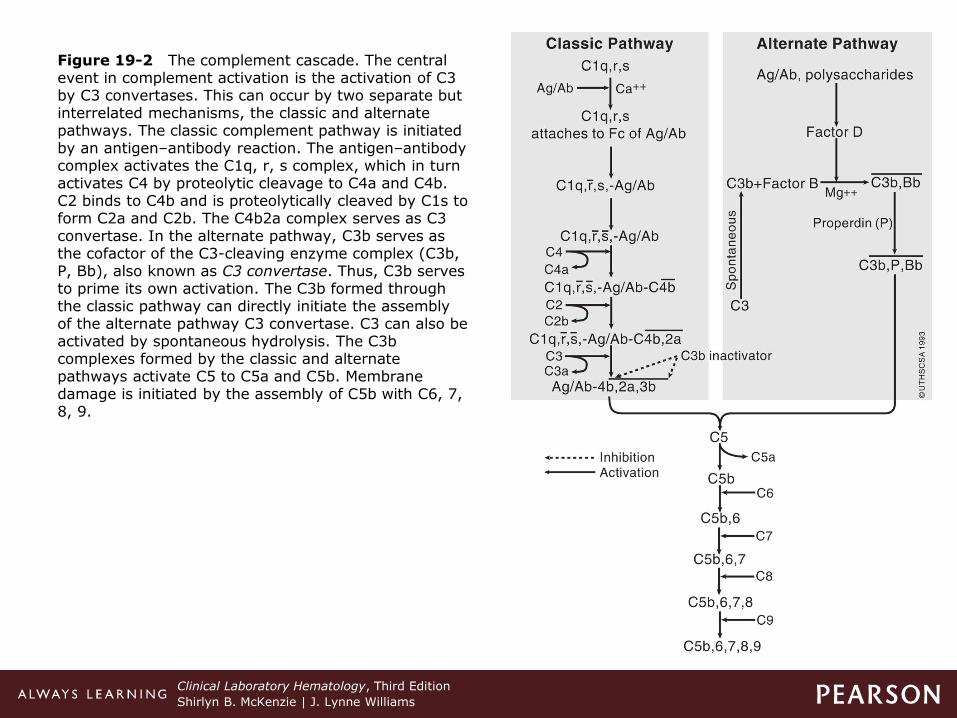
Figure 19-2 The complement cascade. The central event in complement activation is the activation of C3 by C3 convertases. This can occur by two separate but interrelated mechanisms, the classic and alternate pathways. The classic complement pathway is initiated by an antigen–antibody reaction. The antigen–antibody complex activates the C1q, r, s complex, which in turn activates C4 by proteolytic cleavage to C4a and C4b. C2 binds to C4b and is proteolytically cleaved by C1s to form C2a and C2b. The C4b2a complex serves as C3 convertase. In the alternate pathway, C3b serves as the cofactor of the C3-cleaving enzyme complex (C3b, P, Bb), also known as C3 convertase. Thus, C3b serves to prime its own activation. The C3b formed through the classic pathway can directly initiate the assembly of the alternate pathway C3 convertase. C3 can also be activated by spontaneous hydrolysis. The C3b complexes formed by the classic and alternate pathways activate C5 to C5a and C5b. Membrane damage is initiated by the assembly of C5b with C6, 7, 8, 9.
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
IgM-Mediated Hemolysis
• Macrophages do not have receptors for Fc portion of IgM.
– IgM is efficient activator of complement
Intravascular
–Complement activation through C9 and RBC hemolyzes
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
IgM-Mediated Hemolysis
• Macrophages do not have receptors for Fc portion of IgM.
– IgM is efficient activator of complement.
Extravascular
–Activation incomplete
–C3b coats RBCs and sensitized cells destroyed extravascularly via CR1 and CR3 receptors on macrophages.
– IgM can agglutinate cells in addition to activating complement.
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Laboratory ID of Sensitized RBCs
• Two agglutination techniques
–Saline—detects IgM antibodies
–AHG test—detects IgG and/or complement
Direct AHG (DAT)
–Detects RBCs coated in vivo
–Required to differentiate AIHA from other types of HA
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Laboratory ID of Sensitized RBCs
• Two agglutination techniques
–AHG test—detects IgG and/or complement
Indirect AHG (IAT)
–Detects antigens in plasma or serum (in vitro)
–Indicates alloimmunization or free autoAbs in patient's serum
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
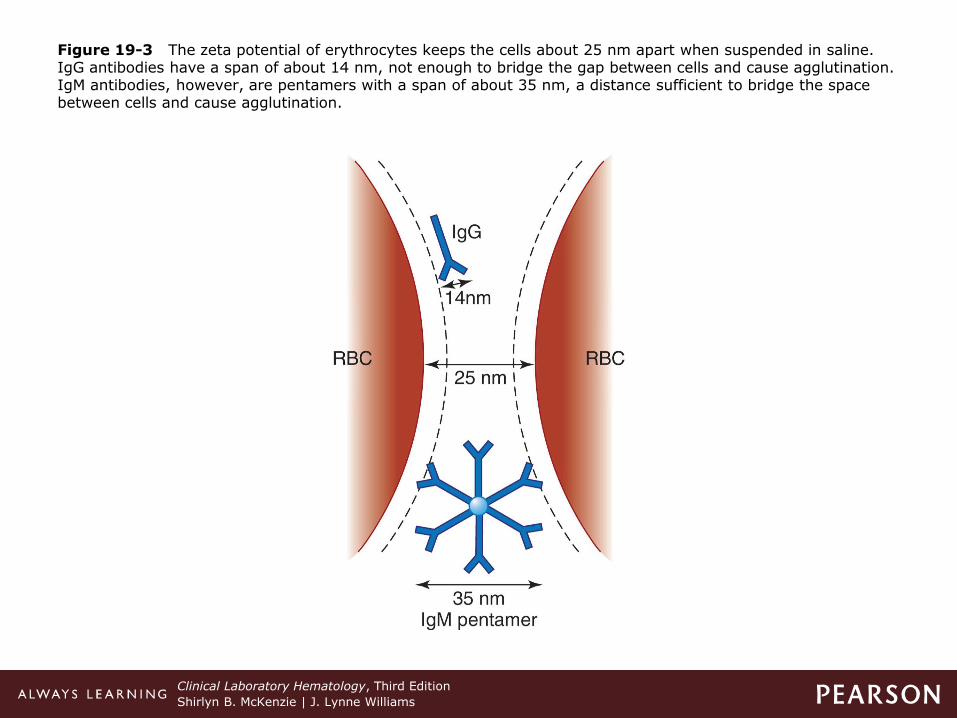
Figure 19-3 The zeta potential of erythrocytes keeps the cells about 25 nm apart when suspended in saline. IgG antibodies have a span of about 14 nm, not enough to bridge the gap between cells and cause agglutination. IgM antibodies, however, are pentamers with a span of about 35 nm, a distance sufficient to bridge the space between cells and cause agglutination.
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Laboratory ID of Sensitized RBCs
• Negative DAT in AIHA
–Can result from
Insufficient number IgG molecules on RBCs
Autoantibodies of IgA or IgM class
Autoantibodies with low affinity for RBCs
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Laboratory ID of Sensitized RBCs
• Negative DAT in AIHA
–Newer techniques more sensitive
Enzyme linked DAT
Gel tests
Flow cytometry
Polybrene tests
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Laboratory ID of Sensitized RBCs
• Positive DAT in normal individual
–Healthy blood donors and hospitalized patients
Positive DAT—No shortened RBC survival
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Laboratory ID of Sensitized RBCs
• Positive DAT in normal individual
–Possible causes:
Inefficient macrophage removal of sensitized RBCs
Insufficient quantity of Ab on cell surface
Subclass of Ab not recognized by macrophage
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Laboratory ID of Sensitized RBCs
• Positive DAT in normal individual
–Possible causes:
Thermal amplitude of antibody (< 37°C)
+ DAT due to presence of complement on RBCs
Patients with hypergammaglobulinemia or receiving high-dose IV gamma globulin exhibit nonspecific binding.
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Autoimmune Hemolytic Anemias (AIHA)
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
AIHA
• Immune tolerance normally prevents formation of autoantibodies
–Autoimmune diseases occur because:
Genetic predisposition
Exposure to infectious agents (molecular mimicry)
Defects in regulation of immune tolerance
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
AIHA
• Immune tolerance normally prevents formation of autoantibodies
–Subcategories
Warm vs cold autoantibodies
–Further categorized as
• Primary vs secondary AIHA
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Accounts for ~ 70% of cases AIHA
–Optimal reactivity at 37°C
–Usually IgG (rarely IgM, IgA)
–Most Abs react with "Rh protein" complex
Do not react with Rh null or Rh deleted cells
Occasionally have single specificity within Rh system (e.g., anti-e)
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Accounts for ~ 70% of cases AIHA
–Most hemolysis is extravascular via splenic macrophages.
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Idiopathic WAIHA
–Accounts for about 60% of cases of warm AIHA
–Acute idiopathic WAIHA
Severe anemia
Developing over two to three days
Hemolysis is self limited
Several weeks → several years duration
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Idiopathic WAIHA
–Chronic idiopathic WAIHS
Hemolysis is unabating.
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Secondary WAIHA associated with:
– Lymphoproliferative disease
CLL, HD
–Neoplastic diseases
–Autoimmune disorders
SLE, RA, Crohn's disease, and so on
–Certain viral and bacterial infections
–Vaccines
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Clinical findings
–Can occur at any age
Incidence ↑ after age 40
–Common presentation
Symptoms of anemia
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Clinical findings
–Secondary AIHA
Signs and symptoms of underlying disorder
–Mild to moderate splenomegaly > 50% patients, hepatomegaly in ⅓ patients
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
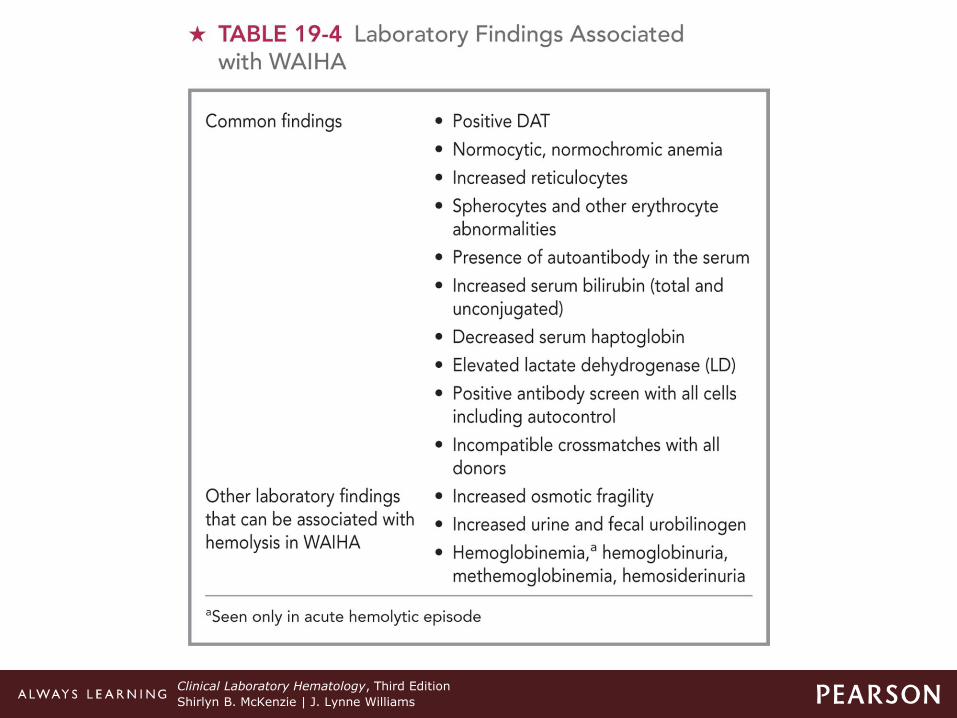
• Laboratory findings
– Immune-mediated hemolysis
+ DAT
Autoantibody in the serum
Presence of spherocytes
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Laboratory findings
–Peripheral blood
Moderate to severe normocytic/normochromic anemia
Reticulocytosis
Polychromasia, NRBCs, spherocytes, schistocytes
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
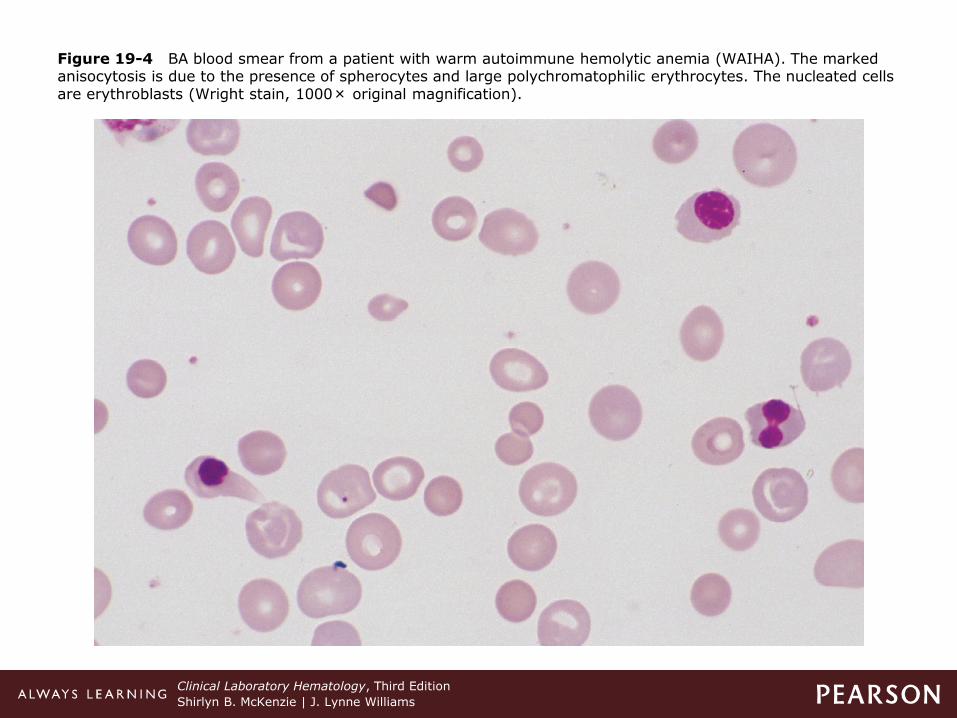
Figure 19-4 BA blood smear from a patient with warm autoimmune hemolytic anemia (WAIHA). The marked anisocytosis is due to the presence of spherocytes and large polychromatophilic erythrocytes. The nucleated cells are erythroblasts (Wright stain, 1000× original magnification).
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Laboratory findings
–Bone marrow
Erythroid hyperplasia, erythrophagocytosis
–Other lab tests
+ DAT
–+ polyspecific AHG and anti-IgG monospecific AHG
–30% + anti-C3
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Laboratory findings
–Differential diagnosis from HS
+ DAT
Autohemolysis test not corrected by glucose
Non-homogeneous population of spherocytes
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Table 19-4 Laboratory Findings Associated with WAIHA
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Therapy
–Self-limited hemolytic disorders
Do not require transfusions.
–Patients needing transfusions
Difficulty finding compatible donor cells
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Warm AIHA
• Therapy
–Other therapies
Immunosuppressive drugs, cytotoxic drugs
Splenectomy
Rituximab
IVIG—high dose intravenous immunoglobulin
Plasma exchange and plasmapheresis
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Cold AIHA
• Accounts for ~ 16–30% of cases of AIHA
–Optimal reactivity < 37°C
–Usually IgM, with complement activation
Rarely IgA or IgG
Most Abs react with I/i Ags or Pr Ags
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Cold AIHA
• Accounts for ~ 16–30% of cases of AIHA
–Severity of disease
Related to thermal range of the Ab
Most hemolysis due to complement-mediated lysis
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
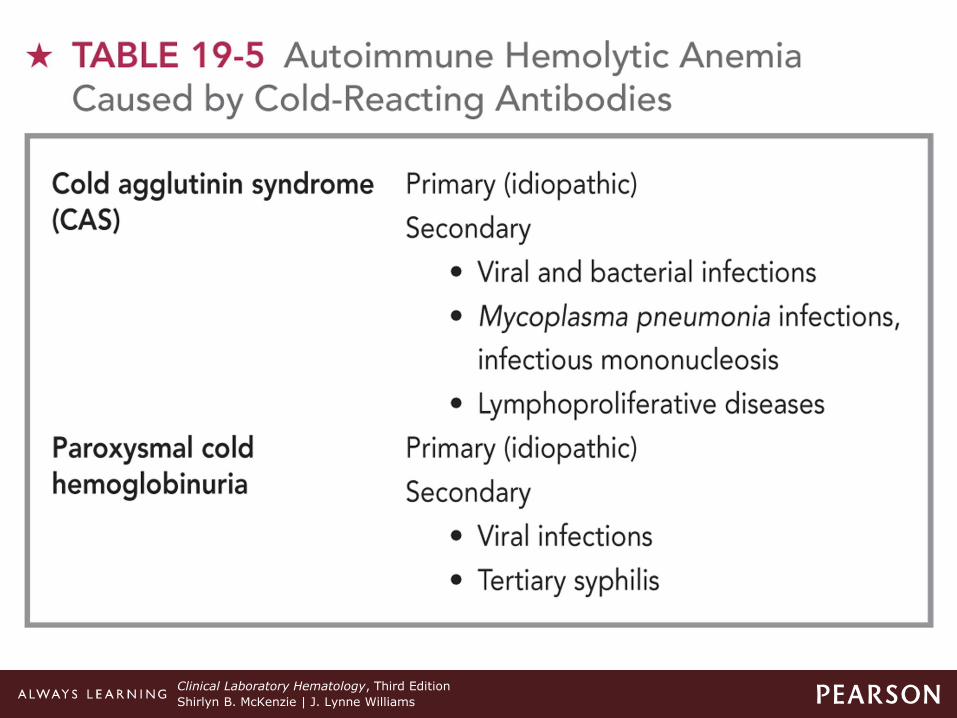
Cold AIHA
• Idiopathic or secondary
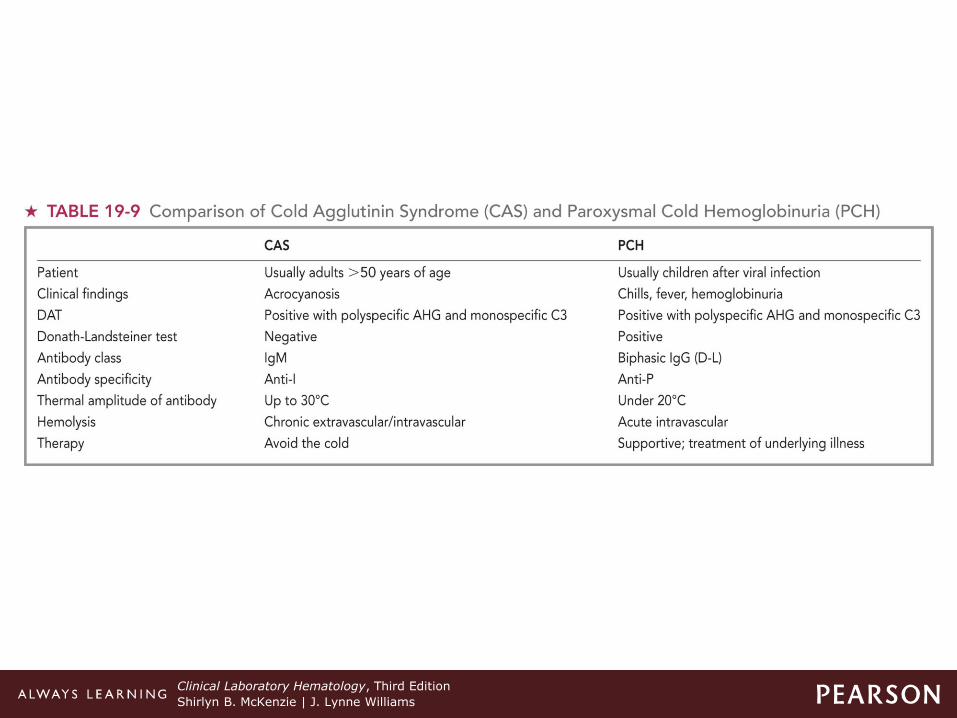
– Idiopathic CAS (cold agglutinin syndrome)
Usually chronic, occurring after age 50
Ab involved is usually
–Monoclonal IgM/kappa with autoanti-I specificity
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Cold AIHA
• Idiopathic or secondary
–Secondary CAS
Associated with infectious disease
–Usually acute, self-limiting
–Polyclonal autoAbs with specificity for Ii antigens
• anti-I—M. pneumoniae
• anti-I—Infectious mononucleosis
• anti-Pr—varicella, rubella
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Cold AIHA
• Idiopathic or secondary
–Secondary CAS
Associated with lymphoproliferative disorders
–Usually chronic, found in older individuals
–Monoclonal IgMκ Ab
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Table 19-5 Autoimmune Hemolytic Anemia Caused by Cold-Reacting Antibodies
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Cold AIHA
• Clinical findings
–Chronic or episodic hemolytic anemia
–RBC agglutination
Areas of the body that cool to the Ab thermal range
Sludging of blood flow within capillaries
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Cold AIHA
• Clinical findings
–Vascular changes
Acrocyanosis
Raynaud's phenomenon
–Pain with color change patterns in skin
–Hemoglobinuria and splenomegaly
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Cold AIHA
• Laboratory findings
–Automated blood counts
Falsely ↓ RBC
Falsely ↑ MCV
Must warm blood and diluting reagents
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Cold AIHA
• Laboratory findings
–Mild to moderate anemia
Normocytic/normochromic
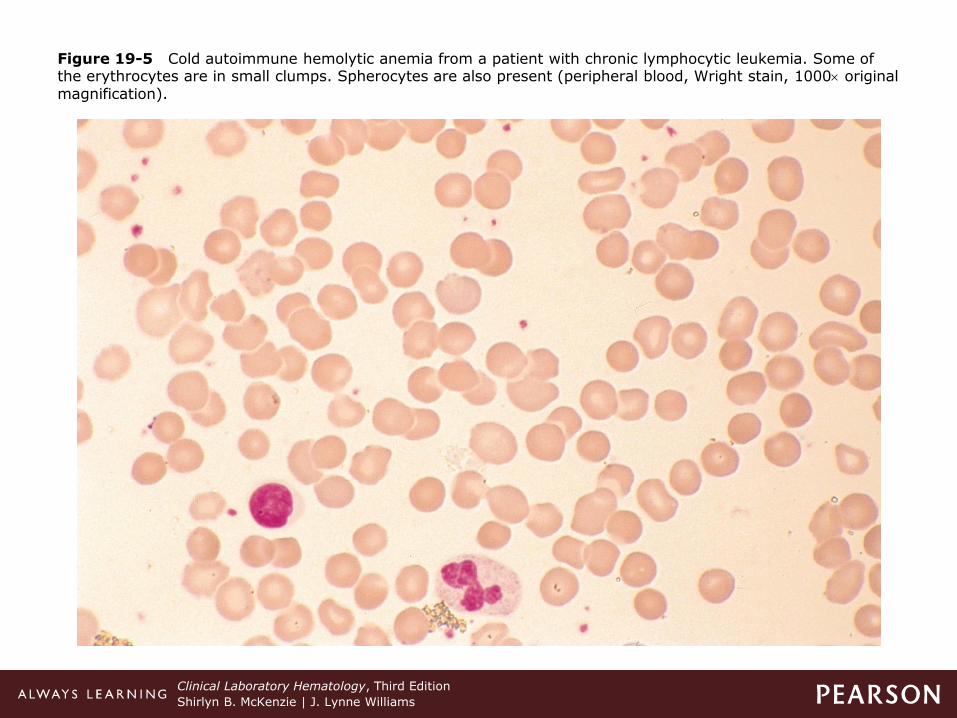
Polychromasia, spherocytes, clumps of RBCs, NRBCs, erythrophagocytosis
–Bone marrow
Normoblastic hyperplasia
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
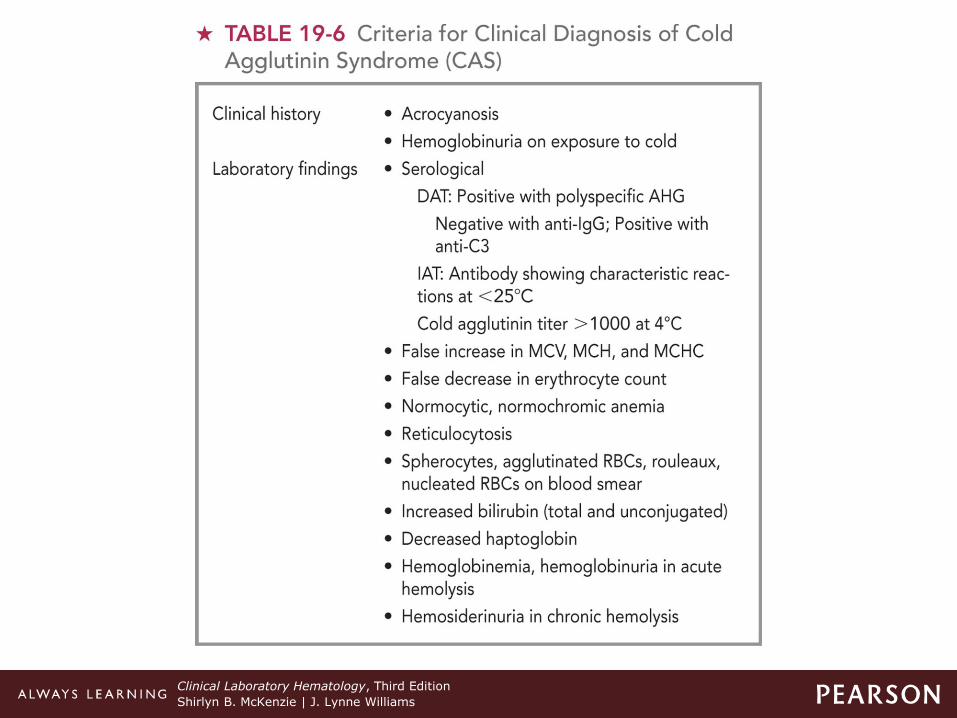
Table 19-6 Criteria for Clinical Diagnosis of Cold Agglutinin Syndrome (CAS)
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Figure 19-5 Cold autoimmune hemolytic anemia from a patient with chronic lymphocytic leukemia. Some of the erythrocytes are in small clumps. Spherocytes are also present (peripheral blood, Wright stain, 1000 original magnification).
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Cold AIHA
• Laboratory findings
–Differential diagnosis
Benign cold autoagglutinins vs pathologic cold agglutinins
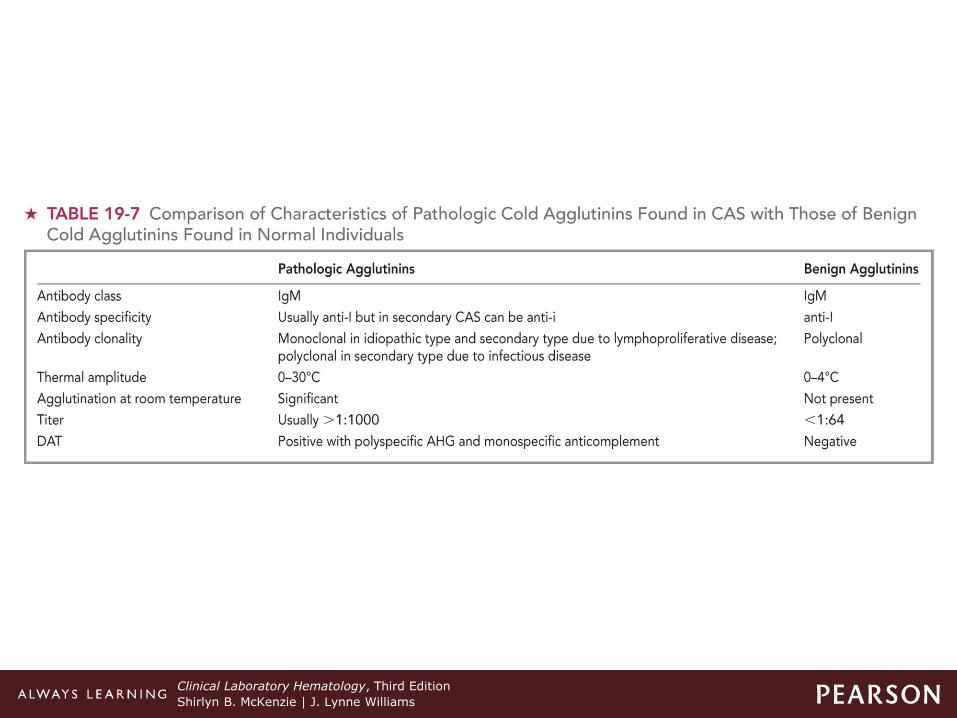
–Pathologic cold agglutinins
• + DAT for polyspecific AHG and monospecific anticomplement antiserum
• Cold agglutinin test—agglutinates RBCs at 0–20°C in saline, reversible at 37°C
• Titer usually > 1:1000 (normal 1:64)
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Table 19-7 Comparison of Characteristics of Pathologic Cold Agglutinins Found in CAS with Those of Benign Cold Agglutinins Found in Normal Individuals
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Cold AIHA
• Therapy
–Keeping extremities warm is most effective
–Secondary to lymphoproliferative disorder
Chemotherapy
–Plasma exchange for acute hemolytic episodes
Effective for short time
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Paroxysmal Cold Hemoglobinuria (PCH)
• Rare autoimmune hemolytic disorder
–Can occur at any age
–Massive intermittent acute hemolysis and hemoglobinuria
–Accounts for 30–40% of all AIHA in children
Most frequent < age 5
Associated with viral and bacterial infections
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Paroxysmal Cold Hemoglobinuria (PCH)
• Rare autoimmune hemolytic disorder
–Usually transient disorder
Resolves spontaneously
–Transfusions may be needed in severe cases.
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Paroxysmal Cold Hemoglobinuria (PCH)
• Pathophysiology
–Bi-phasic complement fixing IgG antibody
Donath Landsteiner antibody
Binds RBCs at low temps (< 20°C), activates complement
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Paroxysmal Cold Hemoglobinuria (PCH)
• Pathophysiology
–Bi-phasic complement fixing IgG antibody
Upon warming to 37°
–Ab detaches
–RBC lysed by complement activation through C9 (MAC)
Usual reactivity—autoanti-P antibody
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Paroxysmal Cold Hemoglobinuria (PCH)
• Clinical findings
–Hemoglobinuria most common clinical symptom
– Jaundice, pallor, hepatosplenomegaly
–Raynaud's phenomenon can occur
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Paroxysmal Cold Hemoglobinuria (PCH)
• Laboratory findings
–Anemia depends on frequency and severity of attack.
–Hb drops sharply—Can ↓ as low as 5
g/dL.
–Hemoglobinemia, methemalbuminemia, hemoglobinuria
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Paroxysmal Cold Hemoglobinuria (PCH)
• Laboratory findings
–Neutropenia, neutrophil shift to left
–Reticulocytopenia, spherocytes
– ↑ serum bilirubin, BUN, LD
– ↓ serum complement, haptoglobin
–Erythrophagocytosis
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Paroxysmal Cold Hemoglobinuria (PCH)
• Laboratory findings
–DAT usually negative for antibodies
–DAT weakly + for complement
– IAT + if performed in cold
–Donath-Landsteiner antibodies
Present in low titers < 1:32
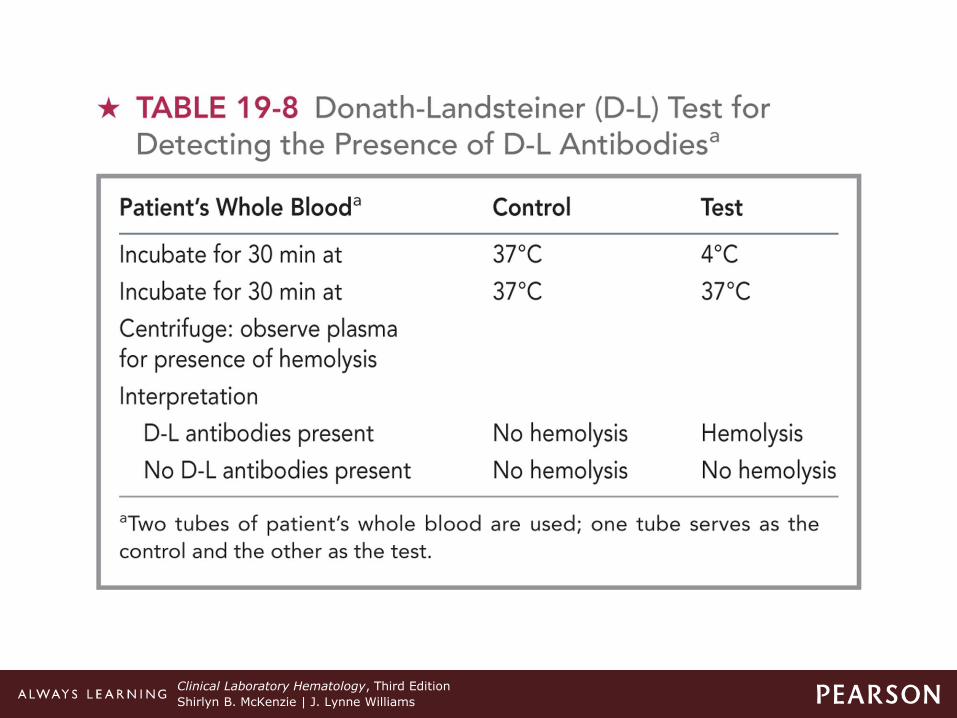
Verified by D-L test
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Table 19-8 Donath-Landsteiner (D-L) Test for Detecting the Presence of D-L Antibodiesa
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Paroxysmal Cold Hemoglobinuria (PCH)
• Therapy
–PCH terminates with recovery from infection.
–Transfusion if hemolysis is severe
–Plasmapheresis if hemolysis persists
–Rituximab
–Avoid exposure to cold
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Table 19-9 Comparison of Cold Agglutinin Syndrome (CAS) and Paroxysmal Cold Hemoglobinuria (PCH)
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Mixed-Type AIHA
• Due to presence of warm-reacting IgG autoAb and cold-reacting IgM autoAb
–Both have high titer and ↑ thermal
amplitude
–50% of cases are idiopathic.
–Remainder associated with lymphoproliferative diseases, autoimmune diseases (e.g., SLE), or HIV
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Mixed-Type AIHA
• Due to presence of warm-reacting IgG autoAb and cold-reacting IgM autoAb
–Mixture of both intravascular (IgM) and extravascular (IgG) hemolysis
–Most patients respond to corticosteroids without transfusions.
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Drug-Induced Hemolytic Anemias
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Drug-Induced HA
• Acquired cause of hemolytic anemia
–Not all individuals taking the same drug develop HA.
–> 125 drugs identified
– Immune response to drug-induced alteration of RBC
–Must differentiate from:
Drug-induced, nonimmune hemolysis
Spontaneous autoimmune disorders
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Drug-Induced HA
• Uncommon acquired cause of HA
–Resolution is withdrawal of drug.
–Classic mechanisms
Drug absorption, immune complex formation, autoantibody induction, membrane modification
–New "unifying" hypothesis
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Drug-Induced HA
• Uncommon acquired cause of HA
–New "unified" hypothesis
Drug binds to RBC membrane.
–Abs produced to react with epitopes specific to drug
–Combination of drug and RBC proteins
–Epitopes primarily on RBC membrane
Explains how patients develop more than one type of drug-induced Ab
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Drug-Induced HA
• Uncommon acquired cause of HA
–New "unified" hypothesis
–Two types:
Drug dependent—requires presence of drug during testing
Drug independent—reacts without presence of drug
Sensitized RBCs have shortened life span
+ DAT
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Table 19-10 Summary of Classic Mechanisms of Drug-Induced Immune Hemolytic Anemia
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Alloimmune Hemolytic Anemia
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Alloimmune HA
• Ab develops to a RBC Ag that the individual lacks.
– Individual exposed to transfused RBCs from another person
–Ags on transfused cells are lacking on RBCs of recipient.
–Stimulate production of Ab (alloAb)
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Alloimmune HA
• Ab develops to a RBC Ag that the individual lacks.
–Abs react only with cells that possess the Ag.
Not the individual's own RBC
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Alloimmune HA
• Ab develops to a RBC Ag that the individual lacks.
–Detected by Ab screen (indirect AHg test)
–Seen in transfusion reactions and Hemolytic disease of the fetus or newborn (HDFN)
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Transfusion Reactions
• Result of:
– Interaction of foreign (nonself) Ags on transfused RBCs and patient's plasma Abs
– Immunologic destruction of donor cells
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Transfusion Reactions
• Result of:
–Two types of transfusion reactions
Immediate (IgM)
–Occurring within 24 hr, intravascular hemolysis
Delayed (IgG)
–Occurring 2–14 days after transfusion, extravascular hemolysis
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
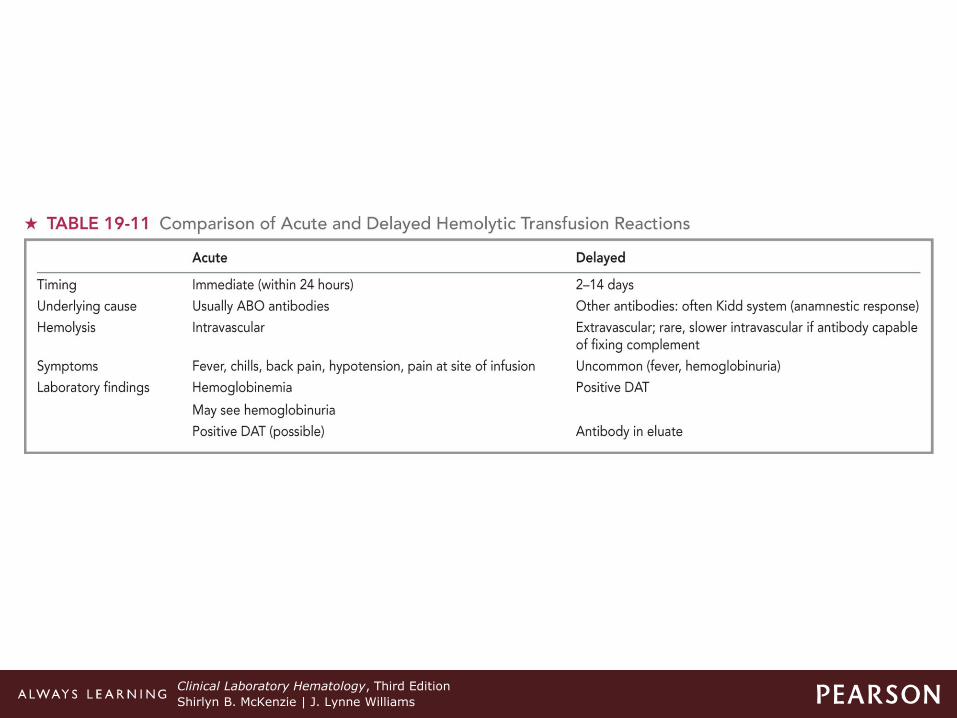
Table 19-11 Comparison of Acute and Delayed Hemolytic Transfusion Reactions
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Transfusion Reactions
• Therapy
–Acute
Terminate transfusion
Supportive care
–Delayed
No treatment
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Disease of the Fetus and Newborn (HDFN)
• Feto-maternal blood group incompatibility
–Mother forms alloantibodies against fetal RBC antigens.
– IgG antibodies cross placenta and destroy fetal RBCs in utero.
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Disease of the Fetus and Newborn (HDFN)
• Feto-maternal blood group incompatibility
–Three categories:
1. Rh(D) caused by anti-D (more severe disease)
2. ABO caused by anti-A and/or anti-B (more common)
3. “Other” caused by Abs to other blood group system Ags
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
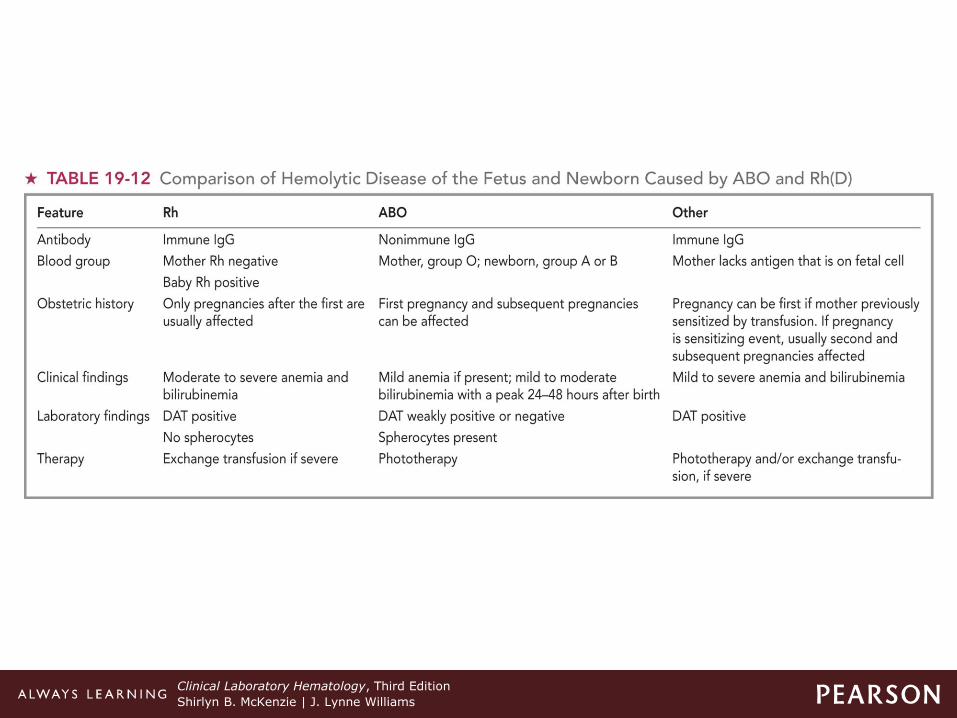
Table 19-12 Comparison of Hemolytic Disease of the Fetus and Newborn Caused by ABO and Rh(D)
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Disease of the Fetus and Newborn (HDFN)
• Pathophysiology
–Four conditions must be met for HDFN to occur:
Mother must be sensitized to RBC Ag that she lacks.
Fetus must possess Ag to which mother has been sensitized.
Mother must produce Abs to foreign Ags.
Mother's Ab must cross placenta, enter fetal circulation.
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Disease of the Fetus and Newborn (HDFN)
• Laboratory testing
–Mother
ABO and Rh typing, antibody screen (IAT)
–Baby
ABO and Rh typing, DAT (elution if necessary to identify Ab)
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Disease of the Fetus and Newborn (HDFN)
• Laboratory findings
–Baby's peripheral blood:
Macrocytic/normochromic, ↑ reticulocytes, leukocytosis with left shift, ↑ NRBCs
Rh HDFN
–Marked polychromasia, mild or absent poikilocytosis, few (if any) spherocytes, ↑
bilirubin, + DAT
continued on next slide
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Disease of the Fetus and Newborn (HDFN)
• Laboratory findings
–Baby's peripheral blood:
ABO HDFN
–NRBCs, schistocytes, spherocytes, polychromasia, sl ↑ bilirubin, weakly +
DAT
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Disease of the Fetus and Newborn (HDFN)
• Therapy
–Prevent hyperbilirubinemia and anemia
– Intrauterine transfusion
Viability of fetus affected
–Phototherapy (after birth) to reduce bilirubin
–Exchange transfusion if bilirubin is rising
> 1 mg/dL/hour or significant anemia
Clinical Laboratory Hematology, Third Edition
Shirlyn B. McKenzie | J. Lynne Williams
Hemolytic Disease of the Fetus and Newborn (HDFN)
• Rh immune globulin (RhIG)
–Passive injection that contains anti-D that prevents maternal immunization
Given at 28 weeks gestation and following birth of Rh+ infant
Dose determined on number of fetal cells in maternal circulation
–Kleihauer-Betke Test
–Rossette Test
–Flow cytometry
Recommended