Crowdsourcing Accountability: ICT for Service Delivery
⇤
Guy Grossman† Melina Platas‡ Jonathan Rodden§
August 27, 2017
Abstract
We examine the e↵ect on service delivery outcomes of a new information commu-nication technology (ICT) platform that allows citizens to send free and anonymousmessages to local government o�cials, thus reducing the cost and increasing the e�-ciency of communication about public services. In particular, we use a field experimentto assess the extent to which the introduction of this ICT platform improved monitor-ing by the district, e↵ort by service providers, and inputs at service points in health,education and water in Arua District, Uganda. Despite relatively high levels of systemuptake, enthusiasm of district o�cials, and anecdotal success stories, we find evidenceof only marginal and uneven short-term improvements in health and water services,and no discernible long-term e↵ects. Relatively few messages from citizens providedspecific, actionable information about service provision within the purview and resourceconstraints of district o�cials, and users were often discouraged by o�cials’ responses.Our findings suggest that for crowd-sourced ICT programs to move from isolated suc-cess stories to long-term accountability enhancement, the quality and specific contentof reports and responses provided by users and o�cials is centrally important.
⇤Data collection was conducted by Innovations for Poverty Action Uganda and Hatchile Consult, Ltd.The project was approved by the Uganda National Council for Science and Technology (#SS 3266), O�ceof the President in Uganda, Mildmay Uganda Research Ethics Committee (#REC REF 0204-2015) andInstitutional Review Boards at Stanford University and the University of Pennsylvania. A pre-analysis planis registered at EGAP (ID 20160819AA). We would like to thank Jon Helfers, Maximillian Seunik, ZacharyTausanovich, Areum Han, Hardika Dayalani, Siyao Li, and Mitchell Goist for research assistance at variousstages in the project. We also thank our research partners at Social Impact, and our implementing partners:GAPP, UNICEF Uganda, and the Uganda USAID mission. Most importantly, we thank the Arua districtlocal government for their interest and collaboration in implementing the project, and the thousands ofresidents of Arua district who participated in the U-Bridge program and our research activities.
†Department of Political Science, University of Pennsylvania and EGAP, [email protected]‡Department of Political Science, New York University Abu Dhabi, [email protected]§Department of Political Science, Stanford University, [email protected]

1 Introduction
In many low-income countries, the long route of accountability—citizens holding service
providers to account via their representatives in government—has been frequently sidelined
in favor of community monitoring programs (Andrabi, Das, and Khwaja, 2017; Banerjee
et al., 2007; Bjorkman and Svensson, 2009; Duflo, Hanna, and Rya, 2012). Circumvent-
ing governments and politicians that have been seen as di�cult to reach, non-responsive
and ine↵ective, programs encouraging citizens to directly hold service providers to account
have yielded mixed results while also raising sustainability concerns (de Laat, Kremer, and
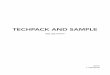
Vermeersch, 2008; Banerjee et al., 2010). Concurrently, in the past decade, access to mobile-
phones has increased exponentially (Figure 1), prompting an interest in harnessing innova-
tions in information communication technology (ICTs) to solve some of the most intractable
development challenges (Grossman, Humphreys, and Sacramone-Lutz, 2014). In this paper,
we return to the older “long route” model of accountability, armed with new technology that
dramatically reduces the cost citizens incur in accessing policymakers.
Specifically, we explore the e↵ects of a new ICT platform, U-Bridge, on the delivery
of local public services in the health, education and water sectors. The platform has been
designed to bridge the gap between citizens, who possess information on local service delivery
problems, and subnational government o�cials, who have the authority and ability to hold
service providers to account. Implemented in Arua district in northwestern Uganda, U-
Bridge allows citizens to report service delivery issues directly to district local government
o�cials through a free and anonymous text-messaging system.
The U-Bridge program is based on the simple idea that participatory grassroots programs
need not necessarily be designed to circumvent government actors. Instead, grassroots e↵orts
can be harnessed to better inform government o�cials of service delivery deficiencies. This
division of labor between those who are best positioned to collect information (community
members) and those who are best positioned to act upon the information (actors outside
the community, such as public o�cials), lies at the heart of U-Bridge and other recent
“crowdsourcing” initiatives (Meier and Munro, 2010).
We assume that public o�cials have the means to improve at least some areas of ser-
vice provision, but are constrained in part by a dearth of targeted information on local
service delivery problems. We further assume that citizens possess such information but
are constrained in the ability to share it with government o�cials due to high monetary
and social costs. To the extent that citizens believe that local government o�cials will be
responsive, we expect citizens to use the ICT platform to make requests, complain and raise
concerns (Grossman, Michelitch, and Santamaria, 2016). Knowing that local public o�cials
1

0
20
40
60
80
(per
100
peo
ple)
1985 1990 1995 2000 2005 2010 2015
sub-Saharan Africa Uganda
Mobile cellular subscriptions
Figure 1: Source: The World Bank; International Telecommunication Union, World Telecommu-nication/ICT Development Report and database.
have more and better information can increase citizens’ expectations from government, which
in turn, may incentivize public o�cial to exert greater e↵ort (Gottlieb, 2016). Moreover, rel-
atively high usage of the platform can improve the e↵orts of service providers, independently
of public o�cials’ actions, to the extent that service providers internalize the possibility of
top-down sanctioning. The overall e↵ect should be an improvement in local governments’
monitoring capacity and input targeting, as well as service providers’ e↵orts.
To test the above theoretical expectations, we collaborated with GAPP, a non-government
organization that has been working in Arua to improve the capacity of the district local gov-
ernment. GAPP developed the U-Bridge platform and implemented it in the district local
government, training the district’s political and technocratic arms on utilizing the system’s
functions. While all district residents could potentially contact Arua local district govern-
ment via U-Bridge, only villages randomly selected by the research team were encouraged
to use the ICT platform during the study period. Specifically, we constructed clusters of
villages around Arua’s 48 mid-level government health centers, and randomly assigned half
of those clusters to the treatment group and half to the control. Each cluster consists of
about 4-5 villages that are served by the same public health center and by at least one
local public primary school. Villagers in treatment areas were informed of the new political
communication channel via community meetings and an extensive door-to-door registration
exercise that yielded more than 3,000 registered (potential) users.
We collected outcome data on the performance of schools and health centers culled from
Arua’s line ministries (e.g., district health o�ce) as well as from unannounced audits orga-
2

nized independently by the research team. We also collected administrative data on village-
level requests for water parts, and the equipment received by villages to build and fix water
service points. In addition, we conducted an endline survey in sixteen treatment villages
to assess knowledge about, use of, and satisfaction with the U-Bridge service. For health
and education, we examine three core outcomes: monitoring (e.g., inspections and calls to
the facilities from district o�cials), e↵ort (e.g., rates of sta↵ absenteeism), and input out-
comes (e.g., supplies of essential medicines, books and desks). We further collected data on
health services utilization and on school test scores. We created indices combining these data
sources for each type of outcome in each sector, by period (baseline, midline and endline).
Between August 2014 and November 2015, more than 11,000 messages were sent via
U-Bridge to government o�cials in Arua district, though we estimate that only a quarter of
these were directly relevant to service delivery. We find that U-Bridge had a sizable e↵ect
on water parts and services (about two-fifths standard deviation) and on education services
(between one quarter and one third of a standard deviation in terms of the control group
outcome distribution), but only in the short-term (first year). By contrast, we do not find
that U-Bridge had a discernible e↵ect on education services beyond the first year, nor on
health services at any point in time.
In the final part of this article we discuss some of the reasons that may account for
our mixed findings regarding the e↵ectiveness of U-Bridge on service delivery outcomes, as
well as the reasons behind the fact that the modest e↵ects of the program on education
services were not sustained into the second year. Since there was relatively high uptake of
U-Bridge compared to similar ICT platforms for political communication, at least in the
first year, we can rule out the possibility that there was simply no demand for the service
by citizens.1 Instead, we find that uptake of U-Bridge was highly uneven, concentrated in a
handful of treatment villages, and that even in high-uptake villages, a majority of citizens
were not satisfied with the response of Arua district o�cials, which may have led to the
dramatic drop in usage we observe over time. Low satisfaction may have resulted in part
from a mismatch in expectations about what constituted a useful and appropriate response
to problems reported. For example, many responses by district o�cials referred users to
lower level local government or local institutions rather than directly following up on the
problem reported. We also find that a considerable number of messages did not contain
su�cient information that could be acted upon by local bureaucrats, or concerned issues
that could not have been addressed in the immediate term.
Our paper contributes to a growing literature on ICT for better governance by high-
1See Grossman, Humphreys, and Sacramone-Lutz (2014, 2016) that reach a similar conclusion withrespect to ICT platforms for communicating political priorities and preferences (rather than service issues).
3

lighting several important insights. First, we show that ICT innovations linking citizens to
government o�cials has a genuine potential to improve local government services, at least in
the water and education sectors. Second, we point to the key role that common knowledge
likely plays in creating incentives for both government o�cials and service providers to exert
greater e↵ort. Third, we learn valuable lessons about the importance of citizens’ perceptions
and beliefs about what local government can and should do.
From a policy perspective, the paper points out that in order to a↵ect the behavior of
o�cials and service providers, it is important that messages from citizens are actionable
and that o�cials’ responses match user expectations. The first step in ensuring that ICT
platforms are useful is to ensure that the crowd-sourced information is itself meaningful
to message recipients. We demonstrate that in contexts such as rural Uganda, it is non-
trivial for citizens to craft a message containing information with a level of specificity that
is usable for government o�cials. One policy implication, therefore, is that for crowd-
sourced platforms to be e↵ective, potential users must receive substantial training on what
kind of information they should share. Second, we discuss how o�cials’ responses, even if
accurate, may not have met users’ expectations about how the program would work, leading
to dissatisfaction and ultimately disengagement. Third, the paper points toward the need to
better understand di↵erential uptake of new political communication technologies; i.e., why
seemingly similar communities have di↵erent capacity and/or willingness to take advantage
of community reporting platforms. Understanding the drivers of individual- and village-level
uptake is essential for the design and future implementation of similar ICT programs.
Our paper also contributes, more broadly, to the literature on information and account-
ability. This body of work is mostly concerned with the dearth of information in the hands
of citizens. Much of the existing literature assumes, often correctly, that voters lack infor-
mation about the quality of service provision that would otherwise allow them to better hold
front-line service providers to account. While there are certainly features of service quality
that are di�cult for users to observe, there are others that are visible—and perhaps uniquely
visible—to users.2 Even if citizens posses reliable targeted information, they may be reluc-
tant to confront service providers due to collective action problems inherent in community
monitoring. Instead, in our study, citizens themselves are the providers of information to
actors that are in a better position to act upon that information: public o�cials.
One possible benefit of an ICT platform like U-Bridge is to provide a way to transmit
information from far-flung villages about a one-o↵ problem that can be resolved quickly or
that requires emergency resources. Examples of such issues include wind blowing the roof
2Teacher absenteeism is an example of poor service quality that is visible to villagers, but not necessarilyto local government o�cials in far-flung district capitals.
4

o↵ of a classroom block, or an outbreak of a disease a↵ecting farmers’ produce or husbandry.
In this way, such a program might solve problems in a piecemeal manner. However, a second
set of issues revolves not around isolated or idiosyncratic problems, but rather the more
intractable challenge of monitoring and accountability – in particular, making sure teachers
and health workers show up and perform their duties. Thus the second possible benefit
of a program like U-Bridge is to generate a sea change in accountability – an equilibrium
shift – via the production of common knowledge between citizens, bureaucrats, and service
providers, such that local service providers improve their performance because they believe
they are being monitored and might be punished for poor performance. Our study suggests
that the second goal is substantially more di�cult than the first.
2 Theoretical Framework: Bringing the State Back In
– with Technology
Notwithstanding the almost ubiquitous adoption of political liberalization and decentral-
ization reforms, many low-income countries still exhibit a disappointing persistence of an
abysmal state of public services. Teachers and nurses are often absent without authoriza-
tion (Chaudhury et al., 2006), and many of those who do show up to work are unmotivated
and exhibit low e↵ort levels (Kremer, Duflo, and Dupas, 2011). Patients regularly receive in-
correct diagnoses and treatments (Amin, Das, and Goldstein, 2008), and schools and clinics
are often short of vital inputs (Glewwe, Kremer, and Moulin, 2009). Weak service provider
e↵orts may be due in part to poor remuneration and resources, but they are also partly
the result of poorly functioning local governments that lack the capacity and/or the will to
adequately monitor front-line service providers and hold them accountable.
Following the publication of the 2004 World Development Report, Making Services Work
for Poor People, numerous programs have sought to improve front-line services by focusing on
the “short route” of accountability – empowering citizens to hold service providers account-
able directly rather than indirectly via public o�cials (Kosack and Fung, 2014). This has
coincided with a growing perception that local government o�cials are hard to reach and may
have interests and policy preferences that do not align with those of their constituents (Bard-
han, 2002). Short-route accountability models are based on two key assumptions: first, that
communities can identify service delivery problems; i.e., that they posses information on
both the quality of existing services and the level and quality of services to which they are
entitled; second, that communities can coordinate on their expectations from providers and
on their own monitoring, and can do so in a sustainable manner.
5

Studies of programs designed explicitly to achieve short-route accountability, however,
find mixed results. Alongside several notable successes (for example, Bjorkman and Svensson
(2009) and Andrabi, Das, and Khwaja (2017)), other studies find no e↵ect of community
monitoring initiatives on service delivery and associated outcomes (Banerjee et al., 2010). In-
deed, there is growing evidence that direct community monitoring is subjected to non-trivial
collective action problems (World Bank, 2016). Specifically, there is growing recognition
of the power and status asymmetry that make rural villagers reluctant to confront service
providers, partly due to fear of retribution (Kaawa-Mafigiri and Walakira, 2017).
Our research project revisits an old idea—bringing the state back in—while patching up
holes in the logic of long-route accountability models with a new technology that reduces the
costs of political communication. Long-route accountability models based on crowd-sourcing
start with the idea that the direct principals to which service provider agents answer are dis-
trict o�cials, not citizens. If a health worker is routinely absent, community members have
no means of firing, transferring, or otherwise penalizing the health worker, except through
informal social sanctions, to which the health worker may or may not respond. However,
contacting public o�cials to demand that they hold service providers accountable has tra-
ditionally been (a) expensive and thus infrequent, and (b) perceived as potentially risky for
citizens due to fear of retribution, especially for those residing in small communities. The
modal way of contacting public o�cials still entails traveling in-person to the district head-
quarters. Due to poor roads and dearth of personal and public transit options, transportation
costs in sub-Saharan Africa are notoriously high—at least twice those of the typical Asian
country (Kessides, 2005). The crowd-sourced model of accountability explicitly addresses
these twin problems. ICT platforms can link citizens directly to local government o�cials
and allow free, unmediated communication as frequently as citizens wish. If user anonymity
can be secured, personal risk can be dramatically minimized or eliminated.
Reducing the monetary and social costs of political communication, does not, however,
guarantee that citizens will share information that is di�cult for the local government to
collect (Grossman, Michelitch, and Santamaria, 2016). Citizens will only use ICT platforms
for service-related communication to the extent that they believe that message recipients
are both resourceful and responsive (Grossman, Humphreys, and Sacramone-Lutz, 2016).
Unlike similar ICT platforms linking citizens to public o�cials, the primary recipients of
messages in our study were not local politicians—who commonly lack the knowledge and
capacity to a↵ect social services (Ra✏er, 2016)—but rather district bureaucrats who are
directly responsible for implementing public services, control resources, and who have the
mandate to promote, sanction, hire, and fire service providers.
The crowd-sourced model assumes that public o�cials are interested in improving service
6

provision, but are constrained by a dearth of reliable information on targeted problems. This
may be a reasonable assumption in meritocratic bureaucracies that cultivate an esprit de
corps among civil servants. It may, however, be overly optimistic in patronage-ridden sys-
tems where citizens have low expectations from public o�cials. We argue that crowd-sourced
platforms might be positioned to increase public o�cials’ motivation by creating common
knowledge around the reporting of service delivery problems. In the status quo, citizens know
that distant public o�cials lack reliable information on specific problems, which reduces cit-
izens’ expectations that o�cials will address service delivery deficiencies. Low expectations
from citizens further reduces the pressure on public o�cials to perform (Gottlieb, 2016). By
allowing citizens to easily report problems, ICT crowd-sourcing platforms may also increase
citizens’ expectations, since they now know that public o�cials know about problems, and
public o�cials know that citizens know that public o�cials posses better and more accurate
information. Such common knowledge—if created—can serve to increase citizens expecta-
tion, and in turn, public o�cials’ incentive to address problems.
Importantly, if citizens choose to use the platform to report service delivery problems,
and if public o�cials follow up on citizens’ reports, then service providers might increase
their e↵orts, endogenously, in order to avoid sanctioning. In this case, the possibility of
reporting ‘bad behavior’ (rather than actual reporting) may sustain relatively high level of
provision over time. Our study is thus designed to compare both short-term (year-1) and
longer-term (year-2) e↵ects.
We expect that there are a set of preconditions that must be met in order for either of
these two pathways to operate. These preconditions include the following:
1. Underlying demand for a means of communicating with local government.
2. Potential users do not fear retribution for reporting (e.g. they believe that messagesare anonymous).
3. Potential users believe the local government has the mandate, capability, and interestin solving service delivery problems.
4. Messages contain actionable information – that is, information that is a) new to thelocal government, b) detailed enough to allow for a response, and c) about a problemthe local government has the resources and capacity to address.
5. Local government has the capability and interest to solve problems reported by users
The data we present below allows us to evaluate the extent to which these preconditions
were met, and evaluate the evidence to determine if U-Bridge was able to a↵ect service
delivery outcomes.
7

Domains of Service Delivery and Hypotheses
Building on the above discussion, we developed the expectation that an ICT platform fa-
cilitating communication between citizens and district o�cials would a↵ect three distinct
domains of service delivery: (1) monitoring, (2) e↵ort, and (3) inputs, described below.
Monitoring : If the new communication platform is being used as expected, the first-order
change we anticipate is that local government o�cials increase their monitoring of facilities.
The district headquarters and thus district o�cials are often located quite far from facilities
(in our study, the mean distance between Arua town and study villages is 25 kilometers as
the crow flies, and longer by road), and have limited time and resources to spend physically
visiting facilities. Though district o�cials generally know that there are problems with
service delivery, as mentioned above, they commonly lack specific and timely information on
delivery deficiencies. Thus, we expect that if local government o�cials hear complaints from
a particular area via the ICT platform, they will be more likely to exert e↵ort on monitoring
and supervising these facilities, for example by making phone calls to or visiting the facility.
E↵ort : We expect that a secondary outcome may be an increase in e↵ort at the level of the
facility to improve services. Here we focus on activities that are under the direct control of
individuals employed in the facilities: for instance making requests to the district for addi-
tional goods and sta↵ and conducting outreach activities. We also consider direct measures
of e↵ort in schools and health clinics, including absenteeism among teachers and health care
workers. Increased e↵ort at the facility level might emerge either as a response to increased
monitoring from district-level o�cials, the expectation thereof, or the anticipation of greater
direct local involvement in the monitoring of service provision.
Inputs : If district-level o�cials grow accustomed to receiving feedback from citizens in the
areas where U-Bridge was implemented and thereby become more sensitive to the needs of
the corresponding facilities, we should expect to see improvements in inputs. These include
the number of sta↵ and supplies like drugs in health clinics; for schools, these inputs include
the number of teachers and school supplies; for water, these inputs include parts and repair
services.
We thus hypothesize that access to an ICT platforms for political communication will:
H1 increase monitoring in health and education.
H2 increase e↵ort in health and education.
H3 increase the availability of inputs in health, education, and water.
8

3 Research Design
To test whether a crowd-sourced monitoring and reporting platform facilitates the long route
of accountability and improves service delivery, we employ a field experimental research
design. Specifically, we test the e↵ect of encouraging (randomly selected) villages in Arua
district in northern Uganda to report service delivery problems via U-Bridge. U-Bridge, an
open-source software package, is designed to open a new channel of communication from
citizens to local government o�cials.3 Citizens are able to contact district o�cials via U-
Bridge by sending a text message to a short-code number at no cost. District o�cials, in both
technical and political positions, are equipped with 3G tablets that enable them to access
the messages anywhere, provided they have Internet access. Once logged into the platform’s
dashboard, government o�cials can read tagged text messages from Arua residents, and reply
to messages from within the system.4 Importantly, incoming text messages from citizens are
anonymized such that government o�cials can only use a unique case ID (and not a phone
number) to track the status of complaints over time.
The U-Bridge Program
Receiving information and implementing a response in the line ministries is a district-wide
activity. The U-Bridge program also included three additional activities that were only
implemented in treatment villages:
1. Community meetings: GAPP organized both an inception meeting and periodic com-
munity dialogue meetings in treatment areas. The inception meeting was used to
introduce the ICT platform, and to provide attendees with information, based on cod-
ified service delivery standards, on the level and quality of services to which citizens
are entitled. Community dialogue meetings took place on a quarterly basis, allowing
citizens to interact directly with district o�cials that have attended the meetings and
providing an overview of actions that the district has taken around service delivery.
Community dialogue meetings were also intended to help create common knowledge
between district o�cials and villagers, the importance of which is detailed in the theory
of change above. Finally these meetings shared feedback with facilities about the mes-
sages that users had sent about service delivery problems. The first round of meetings
3The platform was been developed as part of a collaboration between UNICEF Uganda and RTI Interna-tional. RTI is the prime contractor for the United States Agency for International Development (USAID)-funded program, Governance, Accountability, Participation, and Performance (GAPP), of which U-Bridgeis a part.
4GAPP employed a full-time intern responsible for training public o�cials in Arua on how to log ontothe platform.
9

was held by GAPP in the last quarter of 2014 as part of the launch of the U-Bridge
service. The last round of community dialogue meetings took place in early 2016.
2. User registration: GAPP created a database of potential users, which entailed register-
ing a phone number and basic demographic information.5 Registration took place at
community meetings, but also through a door-to-door registration drive implemented
by the research team. While registration is not necessary for sending or receiving mes-
sages via the U-Bridge platform, it allowed GAPP to contact registered users with
reminders, or to share information about the services to which they were entitled as
Ugandan citizens.
3. Periodic polls: U-Bridge registered members were also invited to respond to short
periodic polls, usually a single question, administered by the research team. The polls
were conducted on weekends via a robocall system operated by VotoMobile, a Ghanian-
based social enterprise. At the height of the program, in mid-2015, there were 3, 062
registered and verified U-Bridge users, who consented to respond to such polls.6
The U-Bridge program was rolled out beginning in August 2014, and several adjustments
were made to the program along the way. Perhaps most importantly, a few months into
the program, it became clear that in the absence of a fully dedicated community liaison
o�cer, district o�cials were unable or had insu�cient time to manage the organization
of the platform. Specifically, the filtering of relevant messages to the appropriate district
o�cial was time consuming. Filtering, which reduces the ratio of noise to signal, included
deciding which messages are relevant and thus “worth” being forwarded to district o�cials
as well as which o�ce is most appropriate to deal with the request. In December 2014 the
implementing partner GAPP hired a full-time sta↵ member to work with district o�cials to
filter messages and help follow up on user messages. This change is important to note as it
suggests that the platform would not have functioned as well in the absence of a third party
to facilitate district o�cials’ responses.
5The process entailed texting “Join” to 8500, after which the sender would receive a series of messagesto collect basic demographic information, such as age, gender, and village name.
6The majority of users (2, 591) have entered the program through a door-to-door registration campaignthat took place between October and November 2014 in treatment villages. An additional 251 users regis-tered following GAPP’s community meetings, where sign-up sheets were passed between attendees. Finallythere are 220 users from Arua that have registered with U-Bridge independently; for example, by followingregistration instruction on fliers that were distributed during the community meetings.
10

Randomization to Treatment
Our study focuses primarily on two salient public services—health and education—and as
such, the research team randomized treatment around places where these public services
are delivered. While there are hundreds of government primary schools in Arua, there
are only 48 mid-level government health centers.7 Thus we use health centers as the unit
of randomization. Specifically, we constructed 48 village-clusters, defined as the group of
nearby villages that are serviced by the same public health center. Half of Arua’s 48 clusters
were randomly assigned to treatment (U-Bridge access) and half to control. All the villages
within a cluster are assigned to the same treatment status.
In each cluster, about 5 villages were selected to be included in the study. These villages
included (a) the village in which the health center was located (primary village), and (b)
three or four additional nearby villages. The selection of additional villages was determined
by the presence of a government primary school, and the location of the village relative
to other clusters. Whenever possible, we selected villages that had a government primary
school within their administrative boundaries, and/or that were located nearby the health
center. We excluded villages that were located close to other clusters in order to limit the
likelihood of spillovers. In total, there are 131 villages in 24 clusters across Arua that were
assigned to the U-Bridge treatment group, and 112 villages in the control group. The mean
number of villages per cluster is 5; the minimum number of villages per cluster is 2 (Yinga)
and the maximum is 9 (Bondo). Figure 2 illustrates our randomization scheme.
A balance test at the cluster level, derived from the 2014 Ugandan census, reveals that
the treatment and control clusters are balanced on a number of dimensions commonly shown
to a↵ect service delivery outcomes and collective action, including ethnolinguistic fraction-
alization (ELF), share employed in the formal sector, poverty, and distance to the local
government headquarters (Table 2).8 The clusters are slightly unbalanced with respect to
the share of literate residents, but the di↵erence in means is substantively small and probably
not meaningful.
4 Data and estimation strategy
We measure outcomes in service delivery in the three domains outlined above using two pri-
mary data sources: (1) unannounced audits of schools and clinics conducted by the research
7Mid-level health centers include the second and third tiers (Health Center II and III) in of a four tiersystem. We excluded Health Center IV, district, and regional hospitals as these have quite di↵erent mandates,focusing on more specialized care, and often di↵erent management structures as well.
8We report covariates balance at the village level in the online appendix.
11

Figure 2: Treatment assignment in Arua district; treatment clusters are in yellow while controlclusters are in blue.
team and (2) administrative data culled from the district education o�ce (DEO), the district
health o�ce (DHO), the district finance o�ce (DFO), and the district water o�ce, compiled
and entered by research assistants hired and supervised by the research team.
Both of these data sources have strengths and weaknesses. On the one hand, a major
benefit of audits is that they are conducted by a source independent of the government or
facility, and are therefore less subject (though not immune) to manipulation. On the other
hand, some measures collected during the audit capture data from a specific day, producing
somewhat noisy measures. Administrative data, by contrast, may be subject to manipulation
and misreporting (a head teacher or health center in charge, for example, may have incentives
to report that the facility is performing well on a number of dimensions even if it is not in
fact), but is collected more regularly. Notwithstanding this limitation, there is no reason to
12

believe that biases in reporting from the facility level to the district level are correlated with
treatment. In the analysis, we combine data from both the audits and administrative data
into indices organized by domain.
Unannounced audits
Unannounced audits were conducted in treatment and control schools and clinics at three
points in time: baseline (June and July 2014), before U-Bridge was implemented; midline
(June 2015), a year after the program launched; and endline (March 2016), almost two
years since inception and after all GAPP meetings and all poll messaging had concluded.9
Audits took place in each of the 48 health centers, and in 134 primary schools, the latter of
which were divided among 46 in treatment clusters, 44 in control clusters, and the rest in
quasi-control facilities in neighboring districts. The audits aimed to collect comprehensive
information on all three domains: monitoring, e↵ort, and inputs. For example, we collected
data on communication with district o�cials (monitoring), on absenteeism on the day we
visited the facility (e↵ort), and the stock of supplies (inputs).
Administrative data
Arua local district government collects regular reports from public facilities. Enumerators
from the research team compiled data collected by the district in order to supplement data
collection via the unannounced audits. Specifically, we assembled data at the district line
ministries that can help determine whether more resources (and attention) have been allo-
cated toward service provision in treatment communities; i.e., that have access to U-Bridge.
For example, the DHO received monthly reports from each facility in which the facility
reports the number of patients treated and procedures undertaken. The research team ex-
tracted performance trends directly from these reports. Both the DHO and DEO keep
records of inspectors’ visits in school and clinics; these data allow testing whether greater
administrative attention is being directed at service units in treatment areas. We also assem-
ble data on stockouts and sta�ng information from the DHO, and sta�ng information from
the DEO. These data thus provide a secondary source, in addition to the audits discussed
above, of absenteeism rates and stockouts. Descriptive statistics for all outcomes measured
can be found in the SI, Tables 1-3.
9The system was still operational at this time, but there were no supplementary activities.
13

Analysis
The key outcome variables are organized by sector (health, education, water) and domain
(monitoring, e↵ort, inputs and utilization). We combine outcomes from each sector-domain
into summary indices using two methods. First, following Kling, Liebman, and Katz (2007)
and Casey, Glennerster, and Miguel (2012), we estimate mean treatment e↵ect, which entails
(1) recoding outcome variables so that higher values always indicate “better” outcomes; (2)
standardizing those variables to allow comparability of e↵ect magnitudes;10 (3) imputing
missing values at the treatment assignment group mean; and (4) compiling a summary index
that gives equal weight to each outcome component. The second method follows Anderson
(2008), who recommends constructing the summary index at stage (4) as a weighted mean
of the standardized outcome component, where the weights—the inverse of the covariance
matrix—are used to maximize the amount of information captured by the index.11
We measure all outcomes in two periods, short-term and long-term. Short-term out-
comes are measured approximately one year into the program, while long-term outcomes are
measured after the program activities, including village meetings, have concluded, close to
two years since the program launched. Following Banerjee et al. (2007) we report results for
each time period separately. We further follow Bruhn and McKenzie (2009), in using the
following ordinary least squares (OLS) regression model:
Yijt = ↵ + ⌧T + Yij0 + �X + ✏ijt
where Yijt is a service point i (say health or school), in cluster j at time t (short or
long-term), modeled as a function of the treatment indicator T , the value of the dependent
variable at baseline (t = 0). We report all outcomes with and without our pre-specified set
of covariates X, cluster standard errors at the cluster level (the level of randomization), and
compute one-sided p-values using randomization inference.
5 Uptake
Prior to reporting the study’s core findings, we begin with reporting overall uptake, which
is not an experimental quantity. Data culled from the U-Bridge system suggests high levels
of adoption in comparison to similar ICT programs studied elsewhere (Blair, Littman, and
Paluck, 2017; Grossman, Humphreys, and Sacramone-Lutz, 2016). Between August 2014
10Standardization is obtained by subtracting the mean and dividing by the standard deviation in thecontrol group.
11Inverse covariance weighting applies an assumption that there is one latent trait of interest, and con-structs an optimal weighted average on the basis of that assumption.
14

and November 2015 over 10,000 messages were sent via the platform. However, the content
of the messages was highly variable in quality, and in the majority of cases did not report
a specific problem that could have plausibly been addressed by the local government. The
vast majority of irrelevant messages were screened by the implementing partner and were
never seen by district o�cials.
We hand-coded the messages sent by users in this time period into three types: actionable,
relevant, and irrelevant. Actionable messages were those we determined to contain informa-
tion about a specific problem in a specific location that could plausibly have been addressed
by the district without further information. Relevant messages were messages about ser-
vice delivery, but included messages that were vague or included insu�cient information to
which local governments could have directly responded. Finally, irrelevant messages did not
contain content related to service delivery.12 Figure 3 provides information on monthly (left-
panel) and cumulative (right-panel) number of relevant and actionable messages overtime.
The figure underscores the fact that rural Ugandans were willing to use the ICT system, but
their e�cacy in reporting problems—knowing how to send an actionable message–has been
low. The figure also suggests that the monthly number of messages peaked after about six
months (May, 2015), and then dropped, though still registering over 100 monthly messages
even 15 months after the program launch.
6 Results
We turn to report our main findings with respect to service delivery outcomes in health,
education and water. The results, capturing both short and long-term e↵ect of U-Bridge
encouragement, are reported in Figures 4–9. Specifically we report models with covariates
adjustment for the weighted mean indices. Results in tabular form with and without co-
variates adjustment can be found in Tables 3-6; in these tables we report, in addition, the
e↵ect of the program on the variables that make up each family of outcomes. Finally, for ro-
bustness, we report similar results using mean e↵ect (unweighted) indices (with and without
covariates adjustment) in the online appendix.
First, we find that the U-Bridge program had no e↵ect on any domain of health services
in either the short (Figure 4) or long term (Figure 5). The coe�cients on the treatment
indicator (⌧) are negative across all health outcomes indices, suggesting that this null is not
simply due to relatively low statistical power.
12Table 7 provides a sample of messages that were coded as actionable, relevant (a subset of not actionablebut relevant messages shown here), and irrelevant messages. Any identifying information has been removed.Some content has been slightly edited to correct spelling mistakes or explain acronyms.
15

0
50
100
150
200
N. M
essa
ges
2014m7 2014m10 2015m1 2015m4 2015m7 2015m10
Monthly
0
500
1000
1500
2000
2500
3000
N. M
essa
ges
2014m7 2014m10 2015m1 2015m4 2015m7 2015m10
Relevant Actionable
Cumulative
Message Intesnity Overtime
Figure 3: The monthly (left-panel) and cumulative (right-panel) number of relevant and actionablemessages over time. Lines are derived from locally weighted regression (lowess).
Second, we find suggestive evidence of positive e↵ects for education, at least in the short
term (Figure 6). There is a positive treatment e↵ect for school inputs where the e↵ect size
is both large (⌧ = .35) and significant (pvalue = .042), and to a lesser extent for both school
monitoring and e↵ort where the e↵ect size is about a quarter of a standard deviation, with p
values falling slightly below the 90% significance level (.134 and .115, respectively). Notably,
teachers in primary schools in treatment clusters exhibit greater e↵orts—they were more
likely to be present during our unannounced audits and engaged in meaningful teaching—
and thus treated schools seem to have received greater supervision and somewhat greater
input. These e↵orts did not translate to higher standardized test scores for students taking
the Primary Leaving Exam (Tables 3-4); however it is important to recognize that these
scores come at the culmination of seven years of schooling, of which the treatment occurred
in only the last.
Even if they are genuine, these suggestive positive e↵ects in the education sector, mea-
sured after the first year, were not sustained into the second year (Figure 7). While the
coe�cients on all three indices are positive, they are smaller than the coe�cients in year-1,
and all are insignificant.
16

pval=.86τ=-.331
0
.5
1
1.5
2
Den
sity
-.8 -.7 -.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6 .7 .8_b[ treat ]
Health monitoring
pval=.91τ=-.486
0
.5
1
1.5
2
Den
sity
-.8-.7-.6-.5-.4-.3-.2-.1 0 .1 .2 .3 .4 .5 .6 .7 .8_b[ treat ]
Health effort
pval=.774τ=-.199
0
.5
1
1.5
2
Den
sity
-.8 -.7 -.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6 .7 .8_b[ treat ]
Health input
pval=.634τ=-.087
0
.5
1
1.5
2
Den
sity
-.8 -.7 -.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6 .7 .8_b[ treat ]
Health utilization
Health: Short-Term (RI)
Figure 4: The e↵ect of U-Bridge on health services– year 1 (short-term). Indices constructed asthe weighted mean of the standardized outcomes. Models control for baseline level of the dependentvariable and adjust for pre-specified set of cluster-level covariates.
pval=.8290000000000001τ=-.312
0
.5
1
1.5
Den
sity
-.8-.7-.6-.5-.4-.3-.2-.1 0 .1 .2 .3 .4 .5 .6 .7 .8_b[ treat ]
Health monitoring
pval=.67τ=-.159
0
.5
1
1.5
Den
sity
-.8-.7-.6-.5-.4-.3-.2-.1 0 .1 .2 .3 .4 .5 .6 .7 .8_b[ treat ]
Health effort
pval=.398τ=.074
0
.5
1
1.5
Den
sity
-.8 -.7 -.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6 .7 .8_b[ treat ]
Health input
pval=.675τ=-.122
0
.5
1
1.5
Den
sity
-.8 -.7 -.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6 .7 .8_b[ treat ]
Health utilization
Health: Long-Term (RI)
Figure 5: The e↵ect of U-Bridge on health services– year 2 (long-term). Indices constructed as theweighted mean of the standardized outcomes. Models control for baseline level of the dependentvariable and adjust for pre-specified set of cluster-level covariates.
17

pval=.134
τ=.276
0
.5
1
1.5
2
2.5
Den
sity
-.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6_b[ treat ]
Education monitoring
pval=.115
τ=.268
0
.5
1
1.5
2
2.5
Den
sity
-.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6_b[ treat ]
Education effort
pval=.042
τ=.352
0
.5
1
1.5
2
2.5
Den
sity
-.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6_b[ treat ]
Education input
pval=.789
τ=-.174
0
.5
1
1.5
2
2.5
Den
sity
-.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6_b[ treat ]
Education outcome
Education: Short-Term (RI)
Figure 6: The e↵ect of U-Bridge on schooling- year 1 (short-term). Indices constructed as theweighted mean of the standardized outcomes. Models control for baseline level of the dependentvariable, adjust for pre-specified set of village-level covariates, and cluster standard errors at thecluster-level.
pval=.333
τ=.124
0
.5
1
1.5
2
Den
sity
-.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6_b[ treat ]
Education monitoring
pval=.621
τ=-.08
0
.5
1
1.5
2
Den
sity
-.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6_b[ treat ]
Education effort
pval=.285
τ=.116
0
.5
1
1.5
2
Den
sity
-.6 -.5 -.4 -.3 -.2 -.1 0 .1 .2 .3 .4 .5 .6_b[ treat ]
Education input
Education: Long-Term (RI)
Figure 7: The e↵ect of U-Bridge on schooling- year 2 (long-term). Indices constructed as theweighted mean of the standardized outcomes. Models control for baseline level of the dependentvariable, adjust for pre-specified set of village-level covariates, and cluster standard errors at thecluster-level.
18

Turning to the water sector (Figure 9 and Table 1), where the post-treatment village-
level data is aggregated across two years (2015-2016), we find positive coe�cients for the
treatment indicator on parts and services provided (⌧ = .427 standard deviations), and for
the number of village requests for any water service (⌧ = .122). As with the education
sector, these treatment e↵ects fall slightly below the 90% significance level (.107 and .185,
respectively). In order to gauge the substantive implications of the above coe�cients, for the
two outcome measures, Figure 8 provides information on the number villages by treatment
group and period. Ultimately five more villages in treatment clusters had made requests for
water parts and services in the post-treatment period (13 against 8 control villages), and
five more villages ultimately received any water service in that period (9 treatment villages
as compared to 4 control villages).
0
2
4
6
8
10
Num
ber o
f villa
ges
Baseline EndlineControl Treatment Control Treatment
Parts and services
0
5
10
15
20N
umbe
r of v
illage
s
Baseline EndlineControl Treatment Control Treatment
Village requests
Water services
Figure 8: Number of villages receiving parts and services (left panel) and making requests (right),by treatment status and period. Data obtained from Arua district local government, works o�ce.
19

pval=.107
τ=.427
0
.5
1
1.5
Den
sity
-1 -.5 0 .5 1_b[ treat ]
water: parts and services
pval=.185
τ=.122
0
1
2
3
4
Den
sity
-.4 -.2 0 .2 .4_b[ treat ]
water: village requests
Water analysis (RI)
Figure 9: The e↵ect of U-Bridge on water: parts and services and village requests. Indicescreated using weighted mean of standardized outcomes. All models control for baseline level ofthe dependent variable, adjust for pre-specified set of village-level covariates, and cluster standarderrors at the cluster-level.
Table 1: Water services and requests
Parts and services Village requests
(1) (2) (3) (4)
Treatment 0.386 0.427 0.079 0.122(0.318) (0.330) (0.107) (0.120)
Constant 0.000 -0.043 -0.000 -0.047(0.083) (0.118) (0.080) (0.078)
Controls no yes no yesPeriod post post post postR2 0.17 0.19 0.03 0.07N 243 243 243 243
Notes: DV: Water services.p<0.10, ** p<0.05, *** p<0.01
20

7 Discussion: exploring mixed results
In this section we explore our mixed findings. In particular, why is there suggestive evidence—
albeit slightly below conventional levels of statistical significance—of positive e↵ects of U-
Bridge on education and water but not on health? Why do these e↵ects, if in fact they exist,
disappear by year two? In exploring these questions, we further evaluate the extent to which
the preconditions for change, discussed above, were met.
Specifically, in addition to the audits and administrative data, we analyze the response
messages sent by district o�cials, an endline survey of a subset of treatment villages and
qualitative interviews and focus group discussions with local government o�cials and U-
Bridge users. The evidence at hands suggests that some but not all preconditions were met,
and that any e↵ects of U-Bridge on service outcomes are mostly due to piecemeal change.
That is, it appears U-Bridge was able to resolve isolated incidents, but the evidence is not
consistent with the creation of common knowledge that would allow for an equilibrium shift
away from underperformance of service providers.
Why no e↵ects in health?
Why did we find evidence of (short-term) e↵ects in education and water, but none whatsoever
in health? There are several possible explanations. First, it could be that there was less
demand for improvements in health than in the other sectors, perhaps related to the fact that
most citizens use schools and water points far more frequently than health clinics. Relatedly,
perhaps citizens are less able to construct useful messages in health than education, as
health may require a higher degree of comprehension or expertise. Second, perhaps the local
government has greater control over the education and water sectors than the health sector,
and thus is better able to a↵ect outcomes in the former than the latter. This could occur if
inputs and human resources are managed to a greater extent by the central government in
the case of health, or if health workers are more specialized and thus there is a lower supply
than in education, which would give health workers relatively more bargaining power and
job security.
To address the first possibility, we examine whether there are di↵erences in the number
of messages sent by sector over time. Messaging intensity can serve as a good proxy of
citizens’ demand for change. While many citizens interact with schools on a nearly daily
basis, perhaps reminded often about problems at their children’s schools, and are confronted
every day with the struggle associated with dysfunctional water sources, most people do not
interact with medical care on a regular basis. Thus, it may be that our mixed findings are
simply a result of a di↵erence in underlying demand for or salience of health care. Figure 10
21

suggests that this is unlikely a plausible explanation. Consistent with public opinion data
on Ugandans’ priorities over public services (Gottlieb, Grossman, and Robinson, 2016), the
number of incoming messages (both relevant and actionable) exhibit similar patterns across
public service type. It is not the case that there are more messages about problems in
education and water than about problems in health. Nor are health-related messages less
likely to be relevant or actionable.
0
10
20
30
40
N. M
essa
ges
2014m7 2014m10 2015m1 2015m4 2015m7 2015m10
Education Health Water
Relevant messages
0
10
20
30
40
N. M
essa
ges
2014m7 2014m10 2015m1 2015m4 2015m7 2015m10
Education Health Water
Actionable messages
Messages overtime, by type
Figure 10: The number of relevant (left-panel) and actionable (right) messages by service sector,overtime. Lines are derived from locally weighted regression (lowess).
Next we explore whether it is easier for the district to address complaints in the education
sector than complaints in the health sector. This may be because health inputs are expensive
and many aspects of health services, such as hiring doctors or stocking medicines, involve
the central government, while education and water services are more decentralized. We thus
plot the change in sectoral outcome indices between the baseline and the midline (year-1),
against the number of relevant messages coming from each village. The data at hand does not
o↵er support to this alternative. At least in the case of Arua district local government, the
district education o�ce is not more e↵ective in translating messages into better outcomes
(Figure 11), as compared to the district health o�ce (Figure ??). Note, however, that
this analysis is not definitive because (a) not all incoming messages could be assigned to a
specific village or cluster, and (b) not all actionable complaints were captured by U-Bridge’s
platform.13
13GAPP, for example, organized quarterly community meetings in two villages in treatment clusters.
22

-4
-2
0
2
4
Cha
nge
mon
itorin
g
0 100 200 300 400All relevant messages
School monitoring
-4
-2
0
2
4
Cha
nge
effo
rt
0 100 200 300 400All relevant messages
School effort
-4
-2
0
2
4
Cha
nge
inpu
t
0 100 200 300 400All relevant messages
School input
-4
-2
0
2
4
Cha
nge
mon
itorin
g
0 2 4 6Education messages
School monitoring
-4
-2
0
2
4
Cha
nge
effo
rt
0 2 4 6Education messages
School effort
-4
-2
0
2
4
Cha
nge
inpu
t
0 2 4 6Education messages
School input
Figure 11: Education: change from baseline to midline (short-term) against messages sent
-2
-1
0
1
2
Cha
nge
mon
itorin
g
0 100 200 300 400All relevant messages
Health monitoring
-2
-1
0
1
2
Cha
nge
effo
rt
0 100 200 300 400All relevant messages
Health effort
-2
-1
0
1
2
Cha
nge
inpu
t
0 100 200 300 400All relevant messages
Health input
-2
-1
0
1
2
Cha
nge
mon
itorin
g
0 5 10Health messages
Health monitoring
-2
-1
0
1
2
Cha
nge
effo
rt
0 5 10Health messages
Health effort
-2
-1
0
1
2
Cha
nge
inpu
t
0 5 10Health messages
Health input
Figure 12: Health: change from baseline to midline (short-term) against messages sent
Meeting attendees have certainly raised service delivery issues with district representatives and these mayor may not have been captured as a complaint in the system’s platform.
23

More generally, Figure 11 suggests that positive e↵ects in the first year for education
were not driven disproportionately by villages with a higher volume of messages. Both
the above explanations implicitly assume that change occurs due to the responsiveness of
district o�cials to specific citizen complaints. However, another possibility identified in the
theory of change outlined above is that following the introduction of the ICT platform,
service providers internalize the possibility of sanctioning, and increase e↵ort independently
of actual messages. This mechanism is consistent with Figure 11, and could explain the
divergence across sectors if health workers somehow were more secure in their position than
teachers, perhaps due to shortages of qualified workers or less responsive management in the
district health o�ce. Unfortunately, we have no data that would allow us to test this claim.
Why don’t the e↵ects in education persist?
Perhaps the most exciting possibility of a program like U-Bridge is that it can generate
common knowledge between service providers, citizens, and district o�cials about monitor-
ing, thus generating incentives for better performance of teachers and headmasters in the
long run. If common knowledge of this kind were being created in treatment clusters in
Arua, however, we would expect that positive e↵ects would strengthen over time, even as
the volume of messages decline. For example, the e↵ect of U-Bridge could be sustained as
teachers gained personal experience of being monitored, or perhaps heard that colleagues had
been sanctioned for poor performance identified via the program, or that district education
o�cials were visiting more often or asking harder questions.
Since the positive e↵ects disappeared by the second year, it seems unlikely that this inter-
nalization took place. In our interviews with district o�cials, we learned of some examples
in which information gleaned from messages was indeed used for disciplinary action, but this
seems not to have been enough to generate sustainable changes in outcomes we could track.
Moreover, in some cases, the disciplinary action taken was not very costly to the service
provider. For example, district o�cials cited the transfer of a poor performing teacher from
one school to another as evidence of the program’s success. Such a transfer would obviously
have been a relief for the school where the complaint had been made, but a burden for the
recipient school, and not terribly costly for the teacher in question. Thus, it could be that
the sanctions the district is able or willing to impose on poorly performing service providers
simply are not costly enough to deter poor performance.
The results are consistent with a scenario in which initial excitement about and engage-
ment with the program led to a temporary increase in monitoring activity from district
o�cials, as well as short-term improvements in performance and physical inputs. However,
24

it appears that this is di�cult to sustain. As demonstrated above, the volume of education
(and other) messages declined substantially over time, and it is possible that service providers
learned over time that the threat of vigorous monitoring and sanctioning was minimal. These
possibilities are addressed in further detail below.
Why did the number of messages decline over time?
Although, as discussed above, there does not appear to be a relationship between the number
of messages sent and a change in outcomes, it is still worth exploring the question of why the
number of messages sent declined over time. First, it could be the case that after an initial
registration drive and encouragement to use the system, which drove initial usage, users
found the district government’s responses unsatisfactory or ine↵ective in fixing the problems
they had reported about. Discouraged, they stopped using the platform.
A second possibility is that after a flurry of initial activity, people forgot about U-Bridge
and simply returned to their busy lives. U-Bridge was nowhere near as interactive or en-
tertaining as the most globally successful applications. Users would have to remember to
use it, and remember the shortcode required to submit a message. Registered users received
frequent informational messages from U-Bridge, but, like email spam, users could easily have
dismissed these messages. A third possibility is that the initial messages, combined with the
quarterly community meetings, satisfied users needs, such that there were fewer problems
they wanted to report.
In order to learn about citizens’ attitudes and knowledge of the U-Bridge system, we
conducted a number of interviews and focus groups with users and government o�cials. In
addition, we conducted an endline survey in spring 2016, interviewing all available adults
(3,192 respondents) in sixteen treatment villages; eight with high uptake of U-Bridge, and
eight with low uptake. This exercise included a set of basic demographic questions, a set of
questions that allow us to construct individuals’ social network, and questions on knowledge
and use of U-Bridge. This survey allows us to probe questions about variable uptake of
U-Bridge—which we address in a companion paper (Ferrali et al., 2017)—as well as to assess
the extent to which assumptions required for U-Bridge to a↵ect service delivery outcomes
were met. Specifically, the endline survey sheds further light on the extent to which citizens
expect that the district government has the capacity to a↵ect service delivery, and their
experiences in using U-Bridge.
The endline survey reveals important findings. First, despite having had an intensive
door-to-door registration campaign and a series of community meetings about the program,
less than third (31%) of respondents reported having heard of U-Bridge. Of those, 15 percent
25

reported that they had sent at least one message. Thus, only a minority of potential users
had in fact used the program, making it impossible to create the kind of knowledge that
might sustain an initial response.
35 percent of users reported that they were somewhat or very unsatisfied with the dis-
trict’s response to their message (compared to 39% that were satisfied, with the remaining
are neither satisfied nor unsatisfied). The majority of unsatisfied users were also those who
had reported they never heard back from district o�cials. While attitudes toward the pro-
gram were not entirely negative, nor do they indicate an overwhelming endorsement of the
program. It is possible that the district did not respond to messages whose content was not
relevant, and that these users were unsatisfied through no fault of the district. Neverthe-
less, the relatively low levels of satisfaction may provide support to the idea that messaging
dropped o↵ after citizens realized it did not live up to their expectations.
On the other hand, 62 percent of users said they heard back from the district most or
all of the time after sending a message, and the vast majority of respondents, 84 percent,
stated that they believed the local government was “somewhat capable” or “very capable”
of improving public service delivery. Thus, it is unlikely that users stopped sending messages
because they came to believe district o�cials were unable to address service delivery prob-
lems. But perhaps despite hearing back from district o�cials, users did not see much change
on the ground, and thus came to believe the system would not solve the problems they had
hoped it would. The drop in messaging after six months, combined with low satisfaction
rates at endline, is consistent with users becoming disillusioned over time.
How did o�cials respond to the program?
We turn to explore how government o�cials respond to the program. Did they find it help-
ful? Did it provide them with new information? Did they provide regular and informative
responses to users? Did they use the information from messages they received to solve prob-
lems? To answer some of these questions, we conducted a focus group with district o�cials
in late 2015 and conducted a second round of interviews in mid 2017.
First, these discussions suggest that district o�cials were generally positive about the
program, and pointed to specific instances in which they received new information that they
were then able to act upon. Some illustrative comments from these focus groups are provided
below:
- “U-Bridge allows for responses in near real-time. Example: [date] Community Dia-logue Meeting showed that the In-Charge of [XXX] Health Centre had been absent forseveral months. Following the meeting, the DS reported to both the CAO and DHO.
26

This resulted in district action and the In-Charge returned to his post, apologized andexplained his absence to constituents.”
- “While we remain constrained by resources, the platform improves the ability of coun-cilors to reach out to constituents.”
- “Additionally, the platform has catalyzed how quickly the district responds to issues.For instance, community members reported that the Youth Chairperson was embezzlingmillions of shillings. They communicated to the district and police action was takenimmediately.”
- “Some messages require drastic changes in budgetary allocations. These are the hardestto respond to (e.g. “there are not enough health workers”) or, those messages thatrequire action at the central level.”
- “U-Bridge also allows the District to broaden our mandate more fully. For instance,issues of domestic violence, child abuse, family matters, etc. can also be addressed. TheU-Bridge allows district o�cials to refer issues more e↵ectively (e.g. to the police).”
These comments and other input provided from district o�cials shed additional light
on the kinds of outcomes services such as U-Bridge could plausibly have a↵ected and how
o�cials perceived the program. First, district o�cials reported many requests that could not
have been implemented in a short-time period, and others that were unrealistic given their
budget. Thus, some of the information shared by users was not actionable due to binding
resource constraints. Second, it appears that a non-trivial number of individuals used U-
Bridge to report problems not necessarily related to service delivery, such as corruption by
politicians and crime. The message log also contains a number of complaints about issues
like noise and excessive drinking. As these outcomes were not among the targeted goals of
the project by either the implementer or the research team, we do not have systematic data
collected on such outcomes.
Third, district o�cials do report receiving information that they did not previously have,
and that they subsequently acted upon, as the anecdote about the absent health center in-
charge suggests. Several of these instances can be identified in the message logs in which U-
Bridge users thanked government o�cials for satisfactory responses to complaints, especially
about water infrastructure. Thus, there is evidence U-Bridge did help o�cials to resolve
at least some service delivery problems. Perhaps these were simply few and far between in
comparison to the problems that the district could not address, or that were beyond the
purview of this study.
While we do not have a full log of all the responses sent by district o�cials to users
through the system, we have responses for the period from the start of the program through
August 2015. An analysis of these messages reveals that many responses given by district
27

o�cials referred users to lower-level local government or other local institutions or bodies.
For example, in response to concerns reported about the number of latrines, discipline of
teachers, quality of teacher housing, and misuse of school funds, the district education o�ce
frequently referred users to consult the Parent Teacher Associations (PTAs), School Man-
agement Committees (SMCs), or head teachers. Indeed, these institutions may be the first
point of call for parents, but it is possible that the reason users were reporting directly to the
district was because e↵orts at lower levels to resolve problems had failed. Similar responses
were often given to users reporting issues in the water and health sector.
It is therefore possible that part of the disappointment expressed by users was a result
of a mismatch in their expectations about the type of response that would be provided by
district o�cials and the response actually provided. Relatedly, the relatively weak e↵ects
of the program on service delivery outcomes could in part be the result of district o�cials’
responses, which in many cases did not directly solve problems but rather provided users
with additional information about the service delivery process and actors.
These insights yield potential lessons for future ICT programs like U-Bridge in settings
with multiple overlapping layers of local government. O�cials at the level of government
receiving the messages might respond—perhaps truthfully—that the solution to the problem
lies most clearly within the purview of another layer of government. Such responses are
unlikely to solve the problem or satisfy the sender. Arua district-level o�cials told us that
in the future, tablets should also be made available to lower-level (sub-county) o�cials as
well. This would have the beneficial impact of improving not only the flow of information
from citizens to o�cials, but also between layers of government for whom communication
and coordination are often di�cult.
Together, we can rule out some possible explanations for a lack of lasting impact, while
providing suggestive evidence of others. Many but not all of the preconditions for the e�cacy
of U-Bridge were met. First, we can rule out the possibility that there is no or low demand
for a program like U-Bridge. Uptake was high in comparison to similar programs, and this
was despite the fact that many of those living in treatment areas had never heard about the
program. We expect uptake would be even higher with a more extensive outreach campaign.
Second, we have evidence that many of the assumptions about the conditions under which
citizens would use U-Bridge were met: people believed the district had capacity to respond,
highlighted the importance of the anonymity of the program, and do not seem to have
been free-riding, at least with respect to messages sent by friends and peers (Ferrali et al.,
2017). Third, the evidence suggests that the content of messages was often insu�cient to
allow district o�cials to respond, and perhaps that even when messages were actionable, the
district did not have the resources to respond to many of them, at least in the short term.
28

This precondition—that messages are actionable—was therefore only partially met, at best.
Self-reports from district o�cials as well as logs of outgoing messages from district o�cials
suggest that the cases in which o�cials were directly involved in resolving service delivery
problems were relatively few. More often, o�cials referred users to other institutions or indi-
viduals. Users may or may not have taken this advice, and those institutions and individuals
to whom they were referred may or may not have helped solve the problem. We further find
no sustained evidence of an increase in the monitoring activities by district o�cials that we
measured, such as calls or visits to facilities, though it is conceivable that district o�cials
employed forms of communication or monitoring that were not recorded, such as calling the
subcounty local government or a member of a local committee for a particular facility.
We thus cannot rule out the possibility that district o�cials had insu�cient incentives
to act upon all of the information they received. The primary recipients of messages were
bureaucrats holding unelected positions. We had positive and encouraging interactions with
them in our numerous visits to the district headquarters, and as noted, they seemed interested
and enthusiastic about the program. Many bureaucrats are surely motivated by a desire to
improve the work of government, but they are not directly accountable to the beneficiaries of
government programs. It is possible that for a program such as U-Bridge to be e↵ective, closer
“monitoring of the monitors” is necessary, but we cannot say definitively whether district
o�cial incentives, or lack thereof, were consequential in this particular case. The program
may also have been more e↵ective if lower levels of local government, such as subcounties,
were also involved in receiving and responding to messages.
8 Conclusion
Circumventing government actors has become a popular strategy to improve service deliv-
ery in recent years, as researchers have tested whether the short route of accountability—
empowering communities to directly monitor providers—can be e↵ective in improving ser-
vices, particularly in the context of rural and low-income settings. A key barrier in the long
route of accountability has always been the cost of sharing information between service users
and government o�cials responsible for overseeing providers of those services. We evaluated
a program designed to overcome this barrier by providing a free and anonymous text messag-
ing service through which citizens could quickly and cheaply share information about service
delivery problems they witnessed on the ground.
We examined the extent to which the U-Bridge program, operating in Arua district in
northern Uganda, could improve monitoring, e↵ort, and inputs in health, education and
water. Over the course of the period for which we have data, close to 10,000 messages were
29

sent, and district o�cials reacted positively to the program. While anecdotes of service
improvements were plentiful, when we compared a variety of service outcomes in treatment
villages—where the program was actively introduced and facilitated and where service re-
quests were made—with a group of control villages, we do not find evidence of significant,
sustained improvements in a variety of (pre-specified) outcomes. We find short-term im-
provements in the education sector, but these were not sustained in the second year of the
program. We also find evidence of greater activity in the water sector.
We evaluate a variety of reasons why we may not have have found a robust e↵ect of the
program on service delivery. Importantly, we find that most of the preconditions for program
success were met, with the (important) exception that a relatively low share of messages had
su�ciently specific information to act upon. We are able to rule out the possibility that
there was no demand for such a program, that citizens did not believe the district would
respond, or that potential users feared retribution.
We also provide suggestive evidence for some possible explanations for our mixed results.
First, despite relatively high levels of uptake, knowledge about the program was relatively low
in treatment areas, such that usage was likely lower than it might have been if all potential
users had been fully aware of the program. Second, those that did send messages often sent
messages that did not contain information the local government could act upon; in other
words, messages that were not actionable. Then, even when information was actionable,
the district did not always have the resources or ability to respond, at least in the short-
term, and this may have been frustrating for some users. Third, some messages that were
actionable were not related to service delivery, such as crime, and thus their impact was
not measured. Fourth, users who had sent actionable messages were frequently referred to
lower-level local government or institutions, which they may or may not have contacted and
which may or may not have been responsive. Indeed, it is entirely likely that the reason users
sent a message through U-Bridge was because local institutions had failed or users feared
retribution from service providers. A related concern is that in a multi-layered decentralized
system, a direct line of communication from citizens to one layer of government might simply
allow o�cials at that layer to shift responsibility or blame for poor service provision to other
layers.
Perhaps because so many messages did not result in problem-solving on the ground, user
satisfaction with the program was relatively low, and declined over time. It is possible that
as a result of the decline in messages or decline in the salience of the program in communities
and government facilities, the already weak short-term treatment e↵ects were not sustained
over time.
A program like U-Bridge can provide information that is extremely useful in specific
30

instances. For example, if an important bridge is washed out in a storm, a roof is blown o↵ a
classroom, a teacher is abusive, or if there is a disease outbreak, word will probably eventually
travel to the district headquarters. But a program like U-Bridge allows the information to
travel to district o�cials much more quickly, potentially facilitating a quicker response. In
this respect, it can function much like a hotline. This kind of piecemeal impact, however,
di↵ers considerably from a situation in which the program ushers in a new equilibrium in
monitoring and accountability, such that local service providers– when tempted to request
extra fees from users or take the day o↵—are deterred because of an enhanced concern that
monitoring will facilitate sanctioning. We are confident that U-Bridge achieved the first goal
in some instances, but were unable to find evidence for the second.
Several policy implications emerge from this work. First, there appears to be significant
demand for programs like U-Bridge, and thus it is worth investigating the ways in which such
programs can be improved to better a↵ect the intended outcomes. Second, such programs
are unlikely to bring about a substantial change in the incentives of service providers, and
hence discernible long-term improvements in service provision, unless large numbers of people
learn about the program and learn how to send actionable messages that focus on service
provision outcomes that governments have the resources and ability to improve. Third, even
if citizens report actionable problems, local government o�cials must have the interest and
mandate to resolve them, and coordination problems between layers of local government
must be resolved.
31

References
Amin, Samia, Jishnu Das, and Markus P Goldstein. 2008. Are you being served?: new tools
for measuring service delivery. Washington D.C.: World Bank Publications.
Anderson, Michael L. 2008. “Multiple Inference and Gender Di↵erences in the E↵ects of Early
Intervention: A Reevaluation of the Abecedarian, Perry Preschool, and Early Training
Projects.” Journal of the American Statistical Association 103 (484): 1481–1495.
Andrabi, Tahir, Jishnu Das, and Asim Ijaz Khwaja. 2017. “Report Cards: The Impact of
Providing School and Child Test-scores on Educational Markets.” American Economic
Review 107 (6): 1535—1563.
Banerjee, Abhijit V, Rukmini Banerji, Esther Duflo, Rachel Glennerster, and Stuti Khemani.
2010. “Pitfalls of Participatory Programs: Evidence from a randomized evaluation in
education in India.” American Economic Journal: Economic Policy pp. 1–30.
Banerjee, Abhijit V., Shawn Cole, Esther Duflo, and Leigh Linden. 2007. “Remedying Ed-
ucation: Evidence from Two Randomized Experiments in India.” The Quarterly Journal
of Economics 122 (3): 1235–1264.
Bardhan, Pranab. 2002. “Decentralization of Governance and Development.” The Journal
of Economic Perspectives 16 (4): 185–205.
Bjorkman, Martina, and Jakob Svensson. 2009. “Power to the People: Evidence from a
Randomized Field Experiment on Community-Based Monitoring in Uganda.” Quarterly
Journal of Economics 124 (2): 735–769.
Blair, Graeme, Rebecca Littman, and Elizabeth Levy Paluck. 2017. “Motivating the adop-
tion of new community-minded behaviors: An empirical test in Nigeria.” Unpublished
manuscript .
Bruhn, Miriam, and David McKenzie. 2009. “In Pursuit of Balance: Randomization in Prac-
tice in Development Field Experiments.” American economic journal: applied economics
1 (4): 200–232.
Casey, Katherine, Rachel Glennerster, and Edward Miguel. 2012. “Reshaping Institutions:
Evidence on External Aid and Local Collective Action.” Quarterly Journal of Economics
127 (4): 1755–1812.
32

Chaudhury, Nazmul, Je↵rey Hammer, Michael Kremer, Karthik Muralidharan, and F Halsey
Rogers. 2006. “Missing in action: teacher and health worker absence in developing coun-
tries.” The Journal of Economic Perspectives 20 (1): 91–116.
de Laat, Joost, Michael Kremer, and Christel Vermeersch. 2008. “Local Participation and
Teacher Incentives: Evidence from a randomized experiment.”.
Duflo, Esther, Rema Hanna, and Stephen P Rya. 2012. “Incentives work: Getting teachers
to come to school.” The American Economic Review 102 (4): 1241–1278.
Ferrali, Romain, Guy Grossman, Melina Platas, and Jonathan Rodden. 2017. “Social Net-
works and Community Reporting.” Working Paper .
Glewwe, Paul, Michael Kremer, and Sylvie Moulin. 2009. “Many children left behind?
Textbooks and test scores in Kenya.” American Economic Journal: Applied Economics 1
(1): 112–135.
Gottlieb, Jessica. 2016. “Greater Expectations: A Field Experiment to Improve Account-
ability in Mali.” American Journal of Political Science 60 (1): 143–157.
Gottlieb, Jessica, Guy Grossman, and Amanda Lea Robinson. 2016. “Do Men and Women
Have Di↵erent Policy Preferences in Africa? Determinants and Implications of Gender
Gaps in Policy Prioritization.” British Journal of Political Science pp. 1–26.
Grossman, Guy, Kristin Michelitch, and Marta Santamaria. 2016. “Texting Complaints to
Politicians Name Personalization and Politicians’ Encouragement in Citizen Mobilization.”
Comparative Political Studies .
Grossman, Guy, Macartan Humphreys, and Gabriella Sacramone-Lutz. 2014. ““I wld like
u WMP to extend electricity 2 our village”: On Information Technology and Interest
Articulation.” American Political Science Review 108 (03): 688–705.
Grossman, Guy, Macartan Humphreys, and Gabriella Sacramone-Lutz. 2016. “Informa-
tion technology and political engagement: Mixed evidence from Uganda.” Unpublished
manuscript .
Kaawa-Mafigiri, David, and Eddy Walakira, eds. 2017. Child Abuse and Neglect in Uganda.
Springer.
Kessides, Christine. 2005. “The Urban Transition in Sub-Saharan Africa: Implications for
Economic Growth and Poverty Reduction.” The World Bank, Africa Region Working
Paper Series No. 97 .
33

Kling, Je↵rey R, Je↵rey B Liebman, and Lawrence F Katz. 2007. “Experimental Analysis
of Neighborhood E↵ects.” Econometrica 75 (1): 83–119.
Kosack, Stephen, and Archon Fung. 2014. “Does Transparency Improve Governance?” An-
nual Review of Political Science 17: 65–87.
Kremer, Michael, Esther Duflo, and Pascaline Dupas. 2011. “Peer E↵ects, Teacher Incentives,
and the Impact of Tracking.” American Economic Review 101 (5).
Meier, Patrick, and Rob Munro. 2010. “The unprecedented role of SMS in disaster response:
Learning from Haiti.” SAIS Review 30: 91–103.
Ra✏er, Pia. 2016. Does political oversight of the bureaucracy increase accountability? Field
experimental evidence from an electoral autocracy. Technical report Working paper, Yale
University.
World Bank, The. 2016. Making Politics Work for Development: Harnessing Transparency
and Citizen Engagement. Conference edition ed. World Bank, Washington, DC.: Policy
Research Report.
34

Appendix
Table 2: Balance test (cluster)
ControlMean
TreatmentMean
Di↵erence ofMeans
p-value forDi↵erence of Means
Adult population (>= 16) 1460.292 1602.917 -142.625 0.464(116.970) (153.786) (193.215)
Mean age 20.575 21.059 -0.484 0.066(0.197) (0.166) (0.257)
Share Lugbara tribe 0.895 0.971 -0.076 0.162(0.052) (0.010) (0.053)
Ethnic polarization 0.501 0.514 -0.013 0.836(0.049) (0.041) (0.064)
Ethnic fractionalization (ELF) 0.060 0.049 0.011 0.669(0.019) (0.017) (0.025)
Religion fractionalization 0.289 0.282 0.007 0.860(0.031) (0.025) (0.039)
Share literate 0.595 0.636 -0.041 0.098(0.016) (0.018) (0.024)
Mean education (0-4 scale) 1.166 1.182 -0.016 0.744(0.025) (0.042) (0.049)
Share with secondary education 0.235 0.241 -0.007 0.784(0.011) (0.021) (0.024)
Share employed 0.845 0.855 -0.009 0.722(0.019) (0.018) (0.026)
Share employed non-agri sectors 0.226 0.255 -0.028 0.518(0.021) (0.038) (0.043)
Poverty Index -0.086 -0.119 0.033 0.468(0.023) (0.039) (0.045)
Distance to Arua (kms) 36.708 28.083 8.625 0.162(5.090) (3.309) (6.071)
N 24 24 48
35

Table 3: Education Outcomes Analysis (no covariates)
Short-term Long-term
Variable Coef SE P-val CI Coef SE P-val CI
Monitoring weighted index 0.170 (0.222) 0.442 [-0.264 ,0.605]
-0.002 (0.230) 0.994 [-0.453 ,0.449]
DEO calls 0.307 (0.202) 0.128 [-0.089 ,0.702]
0.025 (0.222) 0.911 [-0.411 ,0.460]
Inspector calls 0.432 (0.227) 0.057 [-0.013 ,0.876]
-0.177 (0.211) 0.401 [-0.590 ,0.236]
DEO visits 0.048 (0.217) 0.826 [-0.378 ,0.473]
0.257 (0.239) 0.281 [-0.210 ,0.725]
Inspector visits -0.218 (0.216) 0.313 [-0.641 ,0.205]
0.034 (0.215) 0.874 [-0.386 ,0.455]
E↵ort weighted index 0.240 (0.181) 0.186 [-0.116 ,0.596]
0.106 (0.237) 0.656 [-0.360 ,0.571]
% Teachers present (records) -0.186 (0.192) 0.333 [-0.563 ,0.191]
0.048 (0.225) 0.830 [-0.392 ,0.489]
% Teachers present (observed) 0.317 (0.202) 0.116 [-0.079 ,0.713]
0.317 (0.222) 0.153 [-0.118 ,0.752]
Meaningful board 0.201 (0.178) 0.258 [-0.147 ,0.550]
-0.034 (0.245) 0.889 [-0.515 ,0.446]
Teacher engaged 0.423 (0.215) 0.049 [0.001 ,0.845]
0.310 (0.227) 0.172 [-0.135 ,0.756]
Sta↵ meetings 0.024 (0.209) 0.910 [-0.386 ,0.434]
Input weighted index 0.372 (0.223) 0.096 [-0.066 ,0.810]
0.244 (0.194) 0.209 [-0.137 ,0.624]
N. teachers employed 0.250 (0.129) 0.052 [-0.002 ,0.502]
0.142 (0.171) 0.408 [-0.194 ,0.478]
Teachers transferred to school 0.394 (0.288) 0.171 [-0.170 ,0.958]
0.223 (0.214) 0.297 [-0.196 ,0.641]
Students per uniform 0.031 (0.243) 0.898 [-0.445 ,0.508]
-0.214 (0.211) 0.310 [-0.626 ,0.199]
Students per book 0.276 (0.185) 0.135 [-0.086 ,0.638]
0.124 (0.231) 0.593 [-0.330 ,0.577]
Students per pencil 0.099 (0.254) 0.696 [-0.398 ,0.596]
0.226 (0.203) 0.266 [-0.172 ,0.623]
Performance weighted index -0.180 (0.184) 0.329 [-0.541 ,0.181]
Enrollment 0.018 (0.116) 0.878 [-0.209 ,0.244]
% PLE Grade 1 0.052 (0.370) 0.889 [-0.673 ,0.776]
% PLE Grade 2 -0.304 (0.134) 0.023 [-0.567 ,-0.042]
PLE pass rate -0.106 (0.165) 0.520 [-0.429 ,0.217]
In columns 2-5 we report short-term e↵ects (1 year), and in columns 6-9, long-term e↵ects (year 2). Indices are constructed using
the approach developed by Anderson (2008). Standard errors are corrected by combining estimation results using Seemingly
Unrelated Regression estimation; p-values are two-sided.
36

Table 4: Education Outcomes Analysis (with covariates adjustment)
Short-term Long-term
Variable Coef SE P-val CI Coef SE P-val CI
Monitoring weighted index 0.276 (0.208) 0.185 [-0.132 ,0.684]
0.124 (0.289) 0.666 [-0.441 ,0.690]
DEO calls 0.240 (0.222) 0.279 [-0.194 ,0.675]
-0.010 (0.221) 0.963 [-0.444 ,0.424]
Inspector calls 0.402 (0.245) 0.101 [-0.078 ,0.882]
-0.189 (0.213) 0.375 [-0.607 ,0.229]
DEO visits 0.097 (0.188) 0.606 [-0.272 ,0.465]
0.241 (0.290) 0.405 [-0.327 ,0.809]
Inspector visits -0.152 (0.190) 0.425 [-0.525 ,0.221]
-0.064 (0.244) 0.792 [-0.543 ,0.415]
E↵ort weighted index 0.268 (0.195) 0.170 [-0.115 ,0.651]
-0.080 (0.224) 0.720 [-0.520 ,0.359]
% Teachers present (records) -0.330 (0.180) 0.066 [-0.683 ,0.022]
0.021 (0.193) 0.915 [-0.357 ,0.398]
% Teachers present (observed) 0.202 (0.212) 0.340 [-0.213 ,0.617]
0.241 (0.218) 0.267 [-0.185 ,0.668]
Meaningful board 0.324 (0.195) 0.097 [-0.059 ,0.708]
-0.199 (0.256) 0.437 [-0.700 ,0.303]
Teacher engaged 0.340 (0.214) 0.111 [-0.078 ,0.759]
0.202 (0.215) 0.348 [-0.219 ,0.622]
Sta↵ meetings -0.145 (0.178) 0.415 [-0.495 ,0.204]
Input weighted index 0.352 (0.172) 0.040 [0.015 ,0.689]
0.116 (0.205) 0.570 [-0.285 ,0.518]
N. teachers employed 0.269 (0.116) 0.021 [0.041 ,0.497]
0.120 (0.173) 0.487 [-0.219 ,0.459]
Teachers transferred to school 0.422 (0.266) 0.112 [-0.099 ,0.942]
0.102 (0.205) 0.617 [-0.299 ,0.504]
Students per uniform 0.116 (0.241) 0.629 [-0.355 ,0.588]
-0.163 (0.182) 0.372 [-0.520 ,0.194]
Students per book 0.215 (0.205) 0.295 [-0.187 ,0.617]
0.029 (0.230) 0.900 [-0.422 ,0.480]
Students per pencil 0.002 (0.234) 0.994 [-0.456 ,0.460]
0.010 (0.191) 0.959 [-0.364 ,0.384]
Performance weighted index -0.174 (0.160) 0.277 [-0.487 ,0.139]
Enrollment 0.034 (0.109) 0.755 [-0.180 ,0.248]
% PLE Grade 1 -0.111 (0.238) 0.641 [-0.577 ,0.355]
% PLE Grade 2 -0.210 (0.157) 0.182 [-0.517 ,0.098]
PLE pass rate -0.086 (0.170) 0.614 [-0.420 ,0.248]
In columns 2-5 we report short-term e↵ects (1 year), and in columns 6-9, long-term e↵ects (year 2). Indices are constructed using
the approach developed by Anderson (2008). Standard errors are corrected by combining estimation results using Seemingly
Unrelated Regression estimation; p-values are two-sided.
37

Table 5: Health Outcomes Analysis (no covariates)
Short-term Long-term
Variable Coef SE P-val CI Coef SE P-val CI
Monitoring weighted index -0.311 (0.246) 0.207 [-0.794 ,0.172]
-0.296 (0.253) 0.242 [-0.791 ,0.199]
DHO visits -0.122 (0.262) 0.641 [-0.635 ,0.391]
-0.128 (0.256) 0.617 [-0.629 ,0.373]
DHO calls -0.361 (0.257) 0.161 [-0.865 ,0.144]
-0.227 (0.125) 0.071 [-0.472 ,0.019]
Inspector calls -0.257 (0.254) 0.312 [-0.756 ,0.242]
-0.124 (0.276) 0.652 [-0.665 ,0.416]
Inspector visits -0.057 (0.279) 0.839 [-0.603 ,0.490]
-0.146 (0.277) 0.599 [-0.688 ,0.397]
Inspection reports -0.019 (0.055) 0.731 [-0.127 ,0.089]
-0.033 (0.095) 0.731 [-0.218 ,0.153]
E↵ort weighted index -0.331 (0.271) 0.222 [-0.862 ,0.201]
-0.154 (0.291) 0.597 [-0.723 ,0.416]
% Sta↵ Present 0.063 (0.280) 0.822 [-0.486 ,0.613]
0.298 (0.282) 0.290 [-0.255 ,0.852]
% unauthorized absent -0.014 (0.276) 0.960 [-0.555 ,0.527]
0.185 (0.243) 0.447 [-0.292 ,0.662]
Register book -0.301 (0.283) 0.287 [-0.856 ,0.254]
-0.301 (0.283) 0.287 [-0.856 ,0.254]
N. Outreach events -0.527 (0.282) 0.062 [-1.079 ,0.026]
-0.379 (0.304) 0.212 [-0.974 ,0.216]
Input weighted index 0.085 (0.244) 0.727 [-0.393 ,0.564]
0.148 (0.221) 0.503 [-0.285 ,0.582]
Days w/o antimalarials 0.335 (0.247) 0.174 [-0.148 ,0.819]
0.962 (0.227) 0.000 [0.518 ,1.407]
Days w/o ORS 0.151 (0.275) 0.583 [-0.388 ,0.691]
0.219 (0.246) 0.374 [-0.264 ,0.701]
Funds received (millions) 0.005 (0.370) 0.989 [-0.720 ,0.731]
0.093 (0.375) 0.804 [-0.641 ,0.828]
Antimalaria SO 0.056 (0.280) 0.841 [-0.493 ,0.605]
ORS SO -0.174 (0.268) 0.516 [-0.699 ,0.351]
Total SO -0.203 (0.241) 0.398 [-0.675 ,0.268]
Utilization weighted index -0.227 (0.260) 0.384 [-0.737 ,0.283]
-0.209 (0.263) 0.427 [-0.724 ,0.307]
Out patients 0.256 (0.205) 0.212 [-0.146 ,0.658]
-0.253 (0.306) 0.410 [-0.853 ,0.348]
N. patients visiting clinic -0.125 (0.094) 0.183 [-0.309 ,0.059]
0.070 (0.142) 0.619 [-0.207 ,0.348]
OP referrals -0.106 (0.176) 0.545 [-0.450 ,0.238]
-0.005 (0.302) 0.988 [-0.596 ,0.586]
OP diagnoses 0.040 (0.104) 0.702 [-0.164 ,0.244]
0.189 (0.164) 0.247 [-0.131 ,0.510]
Tetanus doses 0.159 (0.184) 0.388 [-0.202 ,0.520]
-0.073 (0.195) 0.706 [-0.455 ,0.308]
Children immunized 0.411 (0.329) 0.212 [-0.235 ,1.056]
-0.119 (0.212) 0.573 [-0.534 ,0.295]
IPT doses 0.122 (0.225) 0.588 [-0.319 ,0.563]
-0.047 (0.163) 0.771 [-0.367 ,0.272]
Iron acid -0.013 (0.280) 0.962 [-0.562 ,0.535]
-0.130 (0.217) 0.548 [-0.556 ,0.295]
Free ITN -0.001 (0.247) 0.998 [-0.485 ,0.484]
-0.370 (0.237) 0.119 [-0.834 ,0.095]
Syphilis test -0.268 (0.214) 0.210 [-0.687 ,0.151]
-0.162 (0.295) 0.583 [-0.741 ,0.417]
Maternity admission -0.180 (0.194) 0.353 [-0.560 ,0.200]
-0.144 (0.139) 0.299 [-0.417 ,0.128]
Maternity delivery -0.248 (0.174) 0.155 [-0.590 ,0.093]
0.175 (0.332) 0.597 [-0.475 ,0.825]
Vitamin A (mothers) -0.398 (0.165) 0.016 [-0.722 ,-0.074]
-0.216 (0.189) 0.253 [-0.585 ,0.154]
Post natal -0.127 (0.132) 0.337 [-0.385 ,0.132]
0.087 (0.246) 0.724 [-0.395 ,0.569]
Vitamin A (children) 0.036 (0.306) 0.907 [-0.564 ,0.636]
0.235 (0.303) 0.438 [-0.358 ,0.829]
Deworming doses 0.090 (0.378) 0.812 [-0.651 ,0.830]
-0.215 (0.175) 0.218 [-0.557 ,0.127]
In columns 2-5 we report short-term e↵ects (1 year), and in columns 6-9, long-term e↵ects (year 2). Indices are constructed using
the approach developed by Anderson (2008). Standard errors are corrected by combining estimation results using Seemingly
Unrelated Regression (SUR) estimation.
38

Table 6: Health Outcomes Analysis (with covariates adjustment)
Short-term Long-term
Variable Coef SE P-val CI Coef SE P-val CI
Monitoring weighted index -0.331 (0.265) 0.211 [-0.850 ,0.187]
-0.312 (0.363) 0.390 [-1.024 ,0.399]
DHO visits -0.104 (0.350) 0.767 [-0.791 ,0.583]
-0.142 (0.313) 0.649 [-0.755 ,0.471]
DHO calls -0.495 (0.353) 0.161 [-1.187 ,0.196]
-0.407 (0.184) 0.027 [-0.768 ,-0.046]
Inspector calls -0.566 (0.314) 0.071 [-1.182 ,0.049]
-0.327 (0.423) 0.438 [-1.156 ,0.501]
Inspector visits -0.454 (0.362) 0.209 [-1.164 ,0.255]
-0.337 (0.366) 0.357 [-1.054 ,0.381]
Inspection reports 0.010 (0.053) 0.846 [-0.094 ,0.114]
0.018 (0.092) 0.846 [-0.162 ,0.197]
E↵ort weighted index -0.486 (0.419) 0.246 [-1.308 ,0.335]
-0.159 (0.276) 0.564 [-0.699 ,0.381]
% Sta↵ Present 0.063 (0.391) 0.872 [-0.703 ,0.830]
0.294 (0.272) 0.280 [-0.239 ,0.827]
% unauthorized absent 0.047 (0.504) 0.926 [-0.942 ,1.035]
0.202 (0.248) 0.415 [-0.283 ,0.688]
Register book -0.363 (0.351) 0.302 [-1.052 ,0.326]
-0.192 (0.254) 0.450 [-0.689 ,0.306]
N. Outreach events -0.892 (0.353) 0.012 [-1.585 ,-0.200]
-0.552 (0.346) 0.111 [-1.231 ,0.126]
Input weighted index -0.199 (0.222) 0.369 [-0.635 ,0.236]
0.074 (0.270) 0.784 [-0.455 ,0.603]
Days w/o antimalarials -0.011 (0.235) 0.963 [-0.472 ,0.450]
0.770 (0.258) 0.003 [0.265 ,1.275]
Days w/o ORS -0.082 (0.363) 0.821 [-0.794 ,0.630]
0.247 (0.246) 0.317 [-0.236 ,0.730]
Funds received (millions) -0.223 (0.389) 0.566 [-0.987 ,0.540]
-0.131 (0.514) 0.799 [-1.138 ,0.876]
Antimalaria SO -0.244 (0.377) 0.518 [-0.983 ,0.495]
ORS SO -0.241 (0.246) 0.327 [-0.723 ,0.241]
Total SO -0.507 (0.264) 0.055 [-1.025 ,0.011]
Utilization weighted index -0.087 (0.228) 0.703 [-0.534 ,0.360]
-0.122 (0.272) 0.653 [-0.655 ,0.411]
Out patients 0.490 (0.212) 0.021 [0.075 ,0.906]
-0.024 (0.298) 0.936 [-0.608 ,0.560]
N. patients visiting clinic -0.235 (0.108) 0.029 [-0.446 ,-0.024]
0.061 (0.155) 0.693 [-0.242 ,0.364]
OP referrals -0.091 (0.148) 0.541 [-0.382 ,0.200]
0.018 (0.307) 0.953 [-0.583 ,0.619]
OP diagnoses -0.013 (0.115) 0.908 [-0.238 ,0.212]
0.161 (0.182) 0.376 [-0.195 ,0.517]
Tetanus doses 0.173 (0.220) 0.431 [-0.258 ,0.605]
-0.208 (0.201) 0.299 [-0.601 ,0.185]
Children immunized 0.337 (0.418) 0.420 [-0.483 ,1.156]
0.019 (0.211) 0.927 [-0.394 ,0.433]
IPT doses 0.410 (0.244) 0.092 [-0.067 ,0.888]
-0.084 (0.139) 0.544 [-0.356 ,0.188]
Iron acid 0.380 (0.304) 0.212 [-0.216 ,0.976]
0.038 (0.205) 0.853 [-0.365 ,0.441]
Free ITN 0.243 (0.301) 0.419 [-0.346 ,0.832]
-0.116 (0.265) 0.663 [-0.635 ,0.404]
Syphilis test 0.029 (0.187) 0.878 [-0.338 ,0.395]
-0.143 (0.350) 0.682 [-0.830 ,0.543]
Maternity admission 0.079 (0.202) 0.695 [-0.317 ,0.476]
-0.334 (0.131) 0.011 [-0.591 ,-0.078]
Maternity delivery 0.001 (0.176) 0.996 [-0.344 ,0.346]
0.035 (0.345) 0.919 [-0.642 ,0.712]
Vitamin A (mothers) -0.183 (0.139) 0.187 [-0.456 ,0.089]
-0.506 (0.158) 0.001 [-0.815 ,-0.196]
Post natal 0.176 (0.130) 0.178 [-0.080 ,0.431]
0.180 (0.232) 0.437 [-0.274 ,0.634]
Vitamin A (children) -0.212 (0.337) 0.529 [-0.872 ,0.448]
0.104 (0.386) 0.788 [-0.652 ,0.860]
Deworming doses -0.110 (0.277) 0.692 [-0.653 ,0.433]
-0.430 (0.260) 0.098 [-0.940 ,0.080]
In columns 2-5 we report short-term e↵ects (1 year), and in columns 6-9, long-term e↵ects (year 2). Indices are constructed using
the approach developed by Anderson (2008). Standard errors are corrected by combining estimation results using Seemingly
Unrelated Regression (SUR) estimation.
39

Table 7: Example messages
Type Message contextActionable In [XXX] health Centre, they have given us sta↵ but they are not at the
work placewe have problem of water source in [XXX] villageIn [XXX] village, [XXX] parish, [XXX] subcounty there is no road, noteachers in schools, and no sta↵ in the health centres please help us fromthese situations.Too much consumption of alcohol by the head teacher and some teachershas spoilt [XXX] primary school please help us.We in [XXX] Health Center are su↵ering from lack of nurses we lost oneof our nurses so can they help us with some nurses we are just left withone nurse hereIn our village [XXX], we have nothing like borehole. women go & fetchwater for 1km away from the village. How can government help ourvillage?There are no drugs in [XXX] HEALTH CENTER. In which ways canU-Report help us?[XXX] Health Centre charges women for delivery at Health Unit anddemand cash for visits
Relevant Help us to eradicate poverty, please!(not actionable) those who monitor Government programs, are those children important
or not?what do you think about EducationI want to discus about education.
Irrelevant HAPPY XMAS FOR YOU.Its pleasure greeting you, thank youI have good papers and commitment,punctuality,trustworth.Where is the game won?
40

SUPPLEMNTARY INFORMATION
August 27, 2017
Contents
1 Variable description 3
2 Descriptive statistics 7
3 Outcomes at baseline 10
4 Results in tabular form 12
5 Change in outcome variables overtime 16
6 Treatment e↵ects and messaging intensity 19
7 Heterogenous e↵ects by distance to district HQs 21
8 Heterogenous e↵ects by community’s wealth 24
List of Tables
1 Education outcomes (descriptive statistics) . . . . . . . . . . . . . . . . . . . . . . . 7
2 Water outcomes (descriptive statistics) . . . . . . . . . . . . . . . . . . . . . . . . . 7
3 Health outcomes (descriptive statistics) . . . . . . . . . . . . . . . . . . . . . . . . . 8
4 Balance test (village) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
5 Health Outcomes at Baseline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
6 Education at Baseline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
1

7 Education Outcomes Analysis (no covariates) . . . . . . . . . . . . . . . . . . . . . . 12
8 Education Outcomes Analysis (with covariates adjustment) . . . . . . . . . . . . . . 13
9 Health Outcomes Analysis (no covariates) . . . . . . . . . . . . . . . . . . . . . . . . 14
10 Health Outcomes Analysis (with covariates adjustment) . . . . . . . . . . . . . . . . 15
List of Figures
1 School monitoring: bar plots of outcome variables overtime . . . . . . . . . . . . . . 16
2 Health monitoring: bar plots of outcome variables overtime . . . . . . . . . . . . . . 16
3 School e↵ort: bar plots of outcome variables overtime . . . . . . . . . . . . . . . . . 17
4 Health e↵ort: bar plots of outcome variables overtime . . . . . . . . . . . . . . . . . 17
5 School inputs: bar plots of outcome variables overtime . . . . . . . . . . . . . . . . . 18
6 Health inputs: bar plots of outcome variables overtime . . . . . . . . . . . . . . . . . 18
7 Education: change from baseline to midline (short-term) against messages sent . . . 19
8 Health: change from baseline to midline (short-term) against messages sent . . . . . 19
9 Education: outcome indices at baseline against messages sent . . . . . . . . . . . . . 20
10 Health: outcome indices at baseline against messages sent . . . . . . . . . . . . . . . 20
11 Cluster-level: SMS messaging by distance to Arua . . . . . . . . . . . . . . . . . . . 21
12 Village-level: SMS messaging by distance to Arua . . . . . . . . . . . . . . . . . . . . 21
13 Education services: Heterogenous treatment e↵ect by distance to Arua . . . . . . . . 22
14 Health services: Heterogenous treatment e↵ect by distance to Arua . . . . . . . . . . 22
15 Water: Heterogenous treatment e↵ect by distance to Arua . . . . . . . . . . . . . . . 23
16 Cluster-level: SMS messaging by poverty . . . . . . . . . . . . . . . . . . . . . . . . . 24
17 Village-level: SMS messaging by wealth . . . . . . . . . . . . . . . . . . . . . . . . . 24
18 Education services: Heterogenous treatment e↵ect by poverty . . . . . . . . . . . . . 25
19 Health services: Heterogenous treatment e↵ect by poverty . . . . . . . . . . . . . . . 25
20 Water: Heterogenous treatment e↵ect by poverty . . . . . . . . . . . . . . . . . . . . 26
2

1 Variable description
Below we describe the variables included in the indices for which we have both baseline and endline
data. For these outcomes, we will conduct a di↵erence-in-di↵erence analysis; for outcome measures
where we have endline data only, we will conduct a cross-sectional analysis. For education and
water, where the data is at the village level, we run two regressions without controls, one with and
one without cluster fixed e↵ects. For health we did not include cluster fixed e↵ects as there is only
one health center per cluster by design.
1. Health
(a) Monitoring:
• DHO visits: number of visits to the facility by DHO in the past three months, asrecorded in facility registration book. Count variable, (Audit variable, V dho visit)
• DHO calls: frequency of calls made by DHO to facility in the past three months,categorical variable. 1 = Never, 2 = about once a month, 3 = about once a week,4 = several times a week, 5 = every day (Audit variable, V dho call)
• Health inspector visits: number of visits to the facility by health inspector in thepast three months, as recorded in facility registration book, count variable (Auditvariable, V BE q67 q62 )
• Health inspector calls: frequency of calls made by health inspector to facility inthe past three months, categorical variables. 1 = Never, 2 = about once a month,3 = about once a week, 4 = several times a week, 5 = every day (Audit variable,V freq calls)
• Inspection reports (Counted at the District of Health): number of inspectionreports completed by the district/health inspector (Administrative data variable,A insp qtr)
• Inspection (yr.): number of times health center inspected according to inspectorsummary reports for financial year (Administrative variable, A insp yr)
(b) E↵ort:
• Outreach: frequency of outreach campaigns/events the clinic undertook in previousthree months, like a visit to a rural village or an immunization drive (Audit variable,V outreach)
• Sta↵ present: average of total sta↵ present across four days, based on registerbook (Audit variable, V sta↵present
• Sta↵ attendance rate: four day average of total employees present over totalemployees expected to be present (Audit variable, V perc employ pres)
• Register book: whether or not health center has attendance register book (Auditvariable, RegisterBook)
(c) Inputs:
• Days w/o antimalarials: number of days in the past 30 days that anti-malarialmedication has been out of stock (Audit variable, V inv so antimalarials)
• Oral rehydration stockout month: number of days in the past 30 days that oralrehydration salts (ORS) have been out of stock (Audit variable, V inv so ors analysis)
3

• Anti-malarial stockout half-year (HMIS:Form 105 Section 5.1): numberof days in the 7 month period before/after program initiation that anti-malarialmedication has been out of stock (Admin variable, A so antimalarial)
• Oral rehydration stockout half-year (HMIS:Form 105 Section 5.1): numberof days in the 7 month period before/after program initiation that oral rehydrationsalts (ORS) have been out of stock (Admin variable HMIS:Form 105 Section 5.1,A so ors)
• Total stockout: the average number of days in a month that a preventative med-ication was out of stock (Admin variable, A total so rate)
• Funds received: the total amount of funds that a health center received overone financial year, millions of shillings (Admin variable HMIS:Form 105 Section 7,A Funds Received)
(d) Utilization:
• Out patient: total out patient attendance at the health clinic including new at-tendance and re-attendance (Admin variable, A OutPat Att Total)
• OP referral: total out patient referrals at health clinic (Admin variable, A OutPat Ref Total)
• OP diagnoses: total diagnoses for out patients at the health clinic (Admin variable,A OutPat Diag total)
• Attendance: total number of new attendances at health clinics (Admin variable,A total attendence)
• Tetanus doses: total doses of tetanus administered to women, pregnant womenincluded. Patients are administered 1 to 5 doses (Admin variable, A TI Total)
• Children immunized: total number of children from 0 to 4 years old that areimmunized (Admin variable, A CI Tot)
• IPT doses: total number of first dose and second dose of IPT/IPT1/IPT2 admin-istered at the antenatal clinic (Admin variable, A ANC IPT )
• Iron/acid: number of pregnant women receiving iron/folic acid on 1st antenatalclinic visit (Admin variable, A ANC Iron)
• Free ITN: number of pregnant women receiving free ITNs at the antenatal clinic(Admin variable, A ANC ITN )
• Syphilis test: number of pregnant women tested for syphilis at the antenatal clinic(Admin variable, A ANC Test Syph)
• Maternity admission: number of admissions to maternity unit (Admin variable,A Mat Admit)
• Maternity delivery: number of deliveries performed in the maternity unit (Adminvariable, A Mat Deliver InUnit)
• Vitamin A (mothers): number of mothers given Vitamin A supplement (Adminvariable, A Mat Moth VitA)
• Post natal: total number of post natal attendances (Admin variable, A PN Att)
• Vitamin A (children): total doses of 1st and 2nd doses of Vitamin A given tochildren, including infants aged 6-11 months and children aged 12-59 months (Adminvariable, A CH VitA totl)
• Deworming doses: total doses of 1st and 2nd doses of deworming administeredto children aged 1 to 14 years old (Admin variable, A CH Deworm Tot)
4

2. Schools
(a) Monitoring:
• DEO visits: Number of visits to the school by DEO in the past three months, asrecorded in facility registration book (Audit variable, V deo visit rec)
• DEO calls: frequency of calls made by DEO to school in the past three months,dichotomous variable 0 = Never, 1 = Ever called in previous three months (Auditvariable, V deo ever call)
• School inspector visits: number of visits to the school by school inspector inthe past three months, as recorded in facility registration book (Audit variable,V isp visit rec)
• School inspector calls: frequency of calls made by school inspector to the schoolin the past three months, categorical variables. 1 = Never, 2 = about once a month,3 = about once a week, 4 = several times a week, 5 = every day (Audit variable,V insp calls)
• School inspector reports: Number of reports written by school inspector, countvariable. (Administrative variable, A Q3 insprep
(b) E↵ort:
• Teacher absenteeism: Number of teachers present over total number of teachersexpected present, average over four days: day of the audit, and previous Monday,Wednesday, and Friday. Measured by enumerator using school attendance recordbook. (Audit variable, Teacher Absent)
• Teachers present (day): Fraction of teachers present during audit, as measuredby enumerator across 3-4 classes observed (Audit variable, V present teach e)
• Meaningful board: Extent to which something meaningful is written on the boardin observed classrooms (average over classrooms), as measured by enumerator, 0 =nothing meaningful written, 1 = something meaningful written (Audit variable,V perc alotwritten)
• Teacher engaged: Average across observed classrooms of teacher engagement, asmeasured by enumerator. 0 = absent, 1 = present and disengaged, 2 = present andengaged (Audit variable, V perc Engaged) Only for endline results
• Sta↵ meetings: Number of sta↵ meetings in past three months, categorical. 1 =None, 2 = between 1 and 3, 3 = more than 3. (Audit variable, V school sta↵ meet)
(c) Inputs:
• Number of teachers: Number of teachers in the school, according to school records(Audit variable, V n teachers)
• Teacher transfers: Number of teachers transferred to the school, according toschool records (Audit variable, V teach transf to)
• Students per uniform: Ratio of students to uniforms, observed by enumerator(Audit variable, V students per supply1 )
• Students per book: Ratio of students to books, observed by enumerator (Auditvariable, V students per supply2 )
• Students per pencil: Ratio of students to pencils, observed by enumerator (Auditvariable, V students per supply3 )
(d) Outcome:
5

• Enrollment: Total student enrollment in the school (Admin variable, A enrollment)
• PLE Grade 1: Fraction of students who scored a 1 (best score) on the primaryleaving examination (Admin variable, A PLE Grade1rate)
• PLE Grade 2: Fraction of students who scored a 2 (second best score) on theprimary leaving examination (Admin variable, A PLE Grade2rate)
• PLE pass rate: Fraction of students who passed the primary leaving examination,of those who sat for the exam (Admin variable, A PLE passrate)
3. Water
(a) • Parts and Services: sum of water related parts distributed and services completed(Admin variable, parts services 14 16, parts services 13 14 )
• Village Requests: sum of water related requests in villages (Admin variable,village requests1 14 16, village requests 13 14, A2 LC1Request0, A2 LC1Request1,A2 LC1Request2 )
6

2 Descriptive statistics
Table 1: Education outcomes (descriptive statistics)
Variable Mean (Std. Dev.) Min. Max. NMonitoringDEO calls 0.47 (0.5) 0 1 269Inspector calls 1.96 (0.88) 1 4 249DEO visits 0.16 (0.49) 0 5 267Inspector visits 0.70 (1.02) 0 7 267Inspector reports 1.93 (1.72) 0 6 258E↵ort% Teachers present (records) 0.71 (0.18) 0 1 270% Teachers present (observed) 0.4 (0.29) 0 1 267Meaningful board 0.26 (0.33) 0 1 267Teacher engaged 0.49 (0.35) 0 1 255Sta↵ meetings 1.82 (0.5) 1 3 179InputsN. teachers employed 13.72 (5.77) 2 34 269Teachers transferred to school 0.62 (1.11) 0 10 269Students per uniform 0.57 (0.27) 0 3.05 266Students per book 0.9 (0.16) 0.01 1.45 266Students per pencil 0.81 (0.19) 0.06 1.13 266PerformanceEnrollment 1020.27 (383.42) 352 4086 245% PLE Grade 1 0.01 (0.03) 0 0.25 144% PLE Grade 2 0.29 (0.2) 0 0.85 144PLE pass rate 0.85 (0.15) 0.36 1 144
Table 2: Water outcomes (descriptive statistics)
Variable Mean (Std. Dev.) Min. Max. NParts and services post-treatment 0.08 (0.51) 0 10 2022Parts and services baseline 0.05 (0.39) 0 9 2022Village requests post-treatment 0.06 (0.28) 0 3 2022Village requests baseline 0.13 (0.42) 0 2 2021Village requests (2nd round data) baseline 0.12 (0.4) 0 3 331Village requests (2nd round data) midline 0.2 (0.49) 0 3 331Village requests (2nd round data) endline 0.2 (0.49) 0 3 331
7

Table 3: Health outcomes (descriptive statistics)
Variable Mean (Std. Dev.) Min. Max. NMonitoringDHO visits 0.1 (0.3) 0 1 141DHO calls 1.44 (0.85) 1 5 120Inspector calls 1.62 (1.08) 0 5 120Inspector visits 0.61 (1.23) 0 8 140Inspection reports 3.05 (0.96) 1 5 144Inspection (yr.) 0.81 (0.63) 0 4 144E↵ortHealth sta↵ present 0.56 (0.23) 0.1 1 94Unauthorized health sta↵ absence (inverse) 0.92 (0.15) 0.3 1 94Register book 0.69 (0.46) 0 1 144Outreach 2.91 (1.76) 0 5 141InputsDays w/o antimalarials -6.58 (10.04) -30 0 137Days w/o ORS -7.92 (11.11) -30 0 136Antimalaria SO -9.35 (20.01) -90 0 144ORS SO -10.14 (23.41) -152 0 144Total SO -0.23 (0.46) -2.98 0 144Funds received (millions) 3.1 (3.69) 0 30.24 144UtlizationOut patient 6706.57 (5672.24) 0 37256 144OP referral 56.23 (83.37) 0 547 144New patients attendance 90.63 (54.55) 8.31 337.99 141OP diagnoses 6032.1 (4532.93) 421 31236 144Tetanus doses 603.84 (494.93) 0 2821 144Children immunized 4673.39 (3654.15) 0 22706 144IPT doses 487.1 (388.79) 0 1879 144Iron acid 311.72 (239.68) 0 1526 144Free ITN 111.37 (140.85) 0 759 144Syphilis test 156.63 (228.82) 0 1265 144Maternity admission 281.11 (267.56) 0 1346 144Maternity delivery 243.51 (271.9) 0 2231 144Vitamin A (mothers) 171.23 (177.29) 0 976 144Post natal 259.54 (402.88) 0 2451 144Vitamin A (children) 917.54 (994.34) 0 4502 144Deworming doses 2138.58 (2873.7) 0 17859 144
8

Table 4: Balance test (village)
ControlMean
TreatmentMean
Di↵erence ofMeans
p-value forDi↵erence of Means
Adult population (>= 16) 312.920 295.923 16.997 0.472(15.764) (17.208) (23.618)
Mean age 20.641 21.137 -0.495 0.003(0.124) (0.107) (0.163)
Share Lugbara tribe 0.910 0.970 -0.060 0.009(0.024) (0.007) (0.023)
Ethnic polarization 0.480 0.522 -0.042 0.267(0.028) (0.026) (0.038)
Ethnic fractionalization (ELF) 0.055 0.048 0.007 0.624(0.010) (0.009) (0.013)
Religion fractionalization 0.278 0.284 -0.006 0.777(0.018) (0.015) (0.023)
Share literate 0.598 0.642 -0.044 0.017(0.013) (0.013) (0.018)
Mean education (0-4 scale) 1.165 1.192 -0.026 0.392(0.016) (0.025) (0.031)
Share with secondary education 0.234 0.250 -0.016 0.307(0.008) (0.012) (0.015)
Share employed 0.840 0.856 -0.016 0.436(0.016) (0.012) (0.020)
Share employed non-agri sectors 0.241 0.263 -0.023 0.416(0.019) (0.020) (0.028)
Poverty Index -0.084 -0.103 0.019 0.526(0.018) (0.023) (0.030)
Distance to Arua (kms) 31.840 25.211 6.629 0.002(1.592) (1.417) (2.124)
Health center in village 0.205 0.183 0.022 0.665(0.038) (0.034) (0.051)
Primary school in village 0.384 0.305 0.079 0.199(0.046) (0.040) (0.061)
N 112 131 243
9

3 Outcomes at baseline
Table 5: Health Outcomes at Baseline
C mean T-C P-val N
DHO visits (baseline) 0.08 0.00 0.97 47DHO calls (baseline) 1.43 -0.32 0.12 40Inspector calls (baseline) 1.48 0.05 0.88 42Inspector visits (baseline) 0.21 0.06 0.65 46Inspection reports (baseline) 2.79 -0.33 0.13 48Inspection (yr.) (baseline) 1.04 0.00 1.00 48
Register book (baseline) 0.62 0.00 1.00 48Outreach (baseline) 3.73 -0.62 0.19 47
Days w/o antimalarials (baseline) -6.82 2.58 0.42 43Days w/o ORS (baseline) -10.67 4.76 0.19 42Antimalaria SO (baseline) -14.29 5.12 0.31 48ORS SO (baseline) -16.04 9.71 0.05 48Total SO (baseline) -0.35 0.17 0.05 48Funds received (millions) (baseline) 1.50 0.50 0.43 48
In this Table we explore the extent to which outcome variables used to constrcut summary indices (monitoring, e↵ort and
inputs) were balanced at baseline. Estimation results are derived from OLS regressions; p-values are two-sided.
10

Table 6: Education at Baseline
C mean T-C P-val N
DEO calls (baseline) 0.22 0.07 0.44 89Inspector calls (baseline) 2.07 -0.17 0.43 84DEO visits (baseline) 0.02 0.11 0.08 87Inspector visits (baseline) 0.45 0.20 0.32 87Inspector reports (baseline) 1.57 -0.35 0.29 86
% Teachers present (records) (baseline) 0.67 0.03 0.49 90% Teachers present (observed) (baseline) 0.35 -0.05 0.47 89Meaningful board (baseline) 0.36 0.13 0.19 89Teacher engaged (baseline) 0.60 0.01 0.94 77Sta↵ meetings (baseline) 1.84 0.02 0.89 89
N. teachers employed (baseline) 13.80 0.65 0.67 89Teachers transferred to school (baseline) 0.53 -0.19 0.48 89Students per uniform (baseline) 0.70 0.08 0.33 88Students per book (baseline) 0.92 0.06 0.10 88Students per pencil (baseline) 0.85 -0.01 0.91 88
Enrollment (baseline) 985.70 19.20 0.82 86% PLE Grade 1 (baseline) 0.00 0.01 0.13 72% PLE Grade 2 (baseline) 0.32 0.07 0.26 72PLE pass rate (baseline) 0.87 0.01 0.72 72
In this table we explore the extent to which outcome variables used to construct summary indices (monitoring, e↵ort and
inputs) were balanced at baseline. Estimation results are derived from OLS regressions with standard errors clustered at the
cluster-level; p-values are two-sided.
11

4 Results in tabular form
In the manuscript we report estimation result using indices constructed as weighted mean of the
standardized outcome component (Anderson, 2008). Here we report, for robustness, equivalent
results where the summary indices, following Kling, Liebman, and Katz (2007) were constructed
as non-weighted mean of the same set of standardized outcome variables.
Table 7: Education Outcomes Analysis (no covariates)
Short-term Long-term
Variable Coef SE P-val CI Coef SE P-val CI
Monitoring index 0.154 (0.123) 0.211 [-0.087 ,0.394]
0.025 (0.157) 0.871 [-0.282 ,0.333]
DEO calls 0.307 (0.202) 0.128 [-0.089 ,0.702]
0.025 (0.222) 0.911 [-0.411 ,0.460]
Inspector calls 0.432 (0.227) 0.057 [-0.013 ,0.876]
-0.177 (0.211) 0.401 [-0.590 ,0.236]
DEO visits 0.048 (0.217) 0.826 [-0.378 ,0.473]
0.257 (0.239) 0.281 [-0.210 ,0.725]
Inspector visits -0.218 (0.216) 0.313 [-0.641 ,0.205]
0.034 (0.215) 0.874 [-0.386 ,0.455]
E↵ort index 0.171 (0.124) 0.167 [-0.072 ,0.414]
0.120 (0.147) 0.417 [-0.169 ,0.408]
% Teachers present (records) -0.186 (0.192) 0.333 [-0.563 ,0.191]
0.048 (0.225) 0.830 [-0.392 ,0.489]
% Teachers present (observed) 0.317 (0.202) 0.116 [-0.079 ,0.713]
0.317 (0.222) 0.153 [-0.118 ,0.752]
Meaningful board 0.201 (0.178) 0.258 [-0.147 ,0.550]
-0.034 (0.245) 0.889 [-0.515 ,0.446]
Teacher engaged 0.423 (0.215) 0.049 [0.001 ,0.845]
0.310 (0.227) 0.172 [-0.135 ,0.756]
Sta↵ meetings 0.024 (0.209) 0.910 [-0.386 ,0.434]
Input index 0.193 (0.136) 0.155 [-0.073 ,0.458]
0.086 (0.141) 0.540 [-0.190 ,0.362]
N. teachers employed 0.250 (0.129) 0.052 [-0.002 ,0.502]
0.142 (0.171) 0.408 [-0.194 ,0.478]
Teachers transferred to school 0.394 (0.288) 0.171 [-0.170 ,0.958]
0.223 (0.214) 0.297 [-0.196 ,0.641]
Students per uniform 0.031 (0.243) 0.898 [-0.445 ,0.508]
-0.214 (0.211) 0.310 [-0.626 ,0.199]
Students per book 0.276 (0.185) 0.135 [-0.086 ,0.638]
0.124 (0.231) 0.593 [-0.330 ,0.577]
Students per pencil 0.099 (0.254) 0.696 [-0.398 ,0.596]
0.226 (0.203) 0.266 [-0.172 ,0.623]
Performance index -0.143 (0.109) 0.189 [-0.356 ,0.070]
Enrollment 0.018 (0.116) 0.878 [-0.209 ,0.244]
% PLE Grade 1 0.052 (0.370) 0.889 [-0.673 ,0.776]
% PLE Grade 2 -0.304 (0.134) 0.023 [-0.567 ,-0.042]
PLE pass rate -0.106 (0.165) 0.520 [-0.429 ,0.217]
In columns 2-5 we report short-term e↵ects (1 year), and in columns 6-9, long-term e↵ects (year 2). Indices are constructedusing the approach developed by Kling et al., (2007). Standard errors are corrected by combining estimation results usingSeemingly Unrelated Regression estimation (SUR); p-values are two-sided.
12

Table 8: Education Outcomes Analysis (with covariates adjustment)
Short-term Long-term
Variable Coef SE P-val CI Coef SE P-val CI
Monitoring index 0.156 (0.129) 0.224 [-0.096 ,0.408]
0.004 (0.173) 0.982 [-0.335 ,0.343]
DEO calls 0.240 (0.222) 0.279 [-0.194 ,0.675]
-0.010 (0.221) 0.963 [-0.444 ,0.424]
Inspector calls 0.402 (0.245) 0.101 [-0.078 ,0.882]
-0.189 (0.213) 0.375 [-0.607 ,0.229]
DEO visits 0.097 (0.188) 0.606 [-0.272 ,0.465]
0.241 (0.290) 0.405 [-0.327 ,0.809]
Inspector visits -0.152 (0.190) 0.425 [-0.525 ,0.221]
-0.064 (0.244) 0.792 [-0.543 ,0.415]
E↵ort index 0.133 (0.132) 0.313 [-0.125 ,0.391]
0.020 (0.145) 0.889 [-0.265 ,0.305]
% Teachers present (records) -0.330 (0.180) 0.066 [-0.683 ,0.022]
0.021 (0.193) 0.915 [-0.357 ,0.398]
% Teachers present (observed) 0.202 (0.212) 0.340 [-0.213 ,0.617]
0.241 (0.218) 0.267 [-0.185 ,0.668]
Meaningful board 0.324 (0.195) 0.097 [-0.059 ,0.708]
-0.199 (0.256) 0.437 [-0.700 ,0.303]
Teacher engaged 0.340 (0.214) 0.111 [-0.078 ,0.759]
0.202 (0.215) 0.348 [-0.219 ,0.622]
Sta↵ meetings -0.145 (0.178) 0.415 [-0.495 ,0.204]
Input index 0.184 (0.094) 0.051 [-0.000 ,0.369]
0.002 (0.115) 0.987 [-0.223 ,0.227]
N. teachers employed 0.269 (0.116) 0.021 [0.041 ,0.497]
0.120 (0.173) 0.487 [-0.219 ,0.459]
Teachers transferred to school 0.422 (0.266) 0.112 [-0.099 ,0.942]
0.102 (0.205) 0.617 [-0.299 ,0.504]
Students per uniform 0.116 (0.241) 0.629 [-0.355 ,0.588]
-0.163 (0.182) 0.372 [-0.520 ,0.194]
Students per book 0.215 (0.205) 0.295 [-0.187 ,0.617]
0.029 (0.230) 0.900 [-0.422 ,0.480]
Students per pencil 0.002 (0.234) 0.994 [-0.456 ,0.460]
0.010 (0.191) 0.959 [-0.364 ,0.384]
Performance index -0.133 (0.096) 0.163 [-0.321 ,0.054]
Enrollment 0.034 (0.109) 0.755 [-0.180 ,0.248]
% PLE Grade 1 -0.111 (0.238) 0.641 [-0.577 ,0.355]
% PLE Grade 2 -0.210 (0.157) 0.182 [-0.517 ,0.098]
PLE pass rate -0.086 (0.170) 0.614 [-0.420 ,0.248]
In columns 2-5 we report short-term e↵ects (1 year), and in columns 6-9, long-term e↵ects (year 2). Indices are constructedusing the approach developed by Kling et al., (2007). Standard errors are corrected by combining estimation results usingSeemingly Unrelated Regression estimation (SUR); p-values are two-sided.
13

Table 9: Health Outcomes Analysis (no covariates)
Short-term Long-term
Variable Coef SE P-val CI Coef SE P-val CI
Monitoring index -0.140 (0.127) 0.272 [-0.389 ,0.110]
-0.175 (0.122) 0.149 [-0.414 ,0.063]
DHO visits -0.122 (0.262) 0.641 [-0.635 ,0.391]
-0.128 (0.256) 0.617 [-0.629 ,0.373]
DHO calls -0.361 (0.257) 0.161 [-0.865 ,0.144]
-0.227 (0.125) 0.071 [-0.472 ,0.019]
Inspector calls -0.257 (0.254) 0.312 [-0.756 ,0.242]
-0.124 (0.276) 0.652 [-0.665 ,0.416]
Inspector visits -0.057 (0.279) 0.839 [-0.603 ,0.490]
-0.146 (0.277) 0.599 [-0.688 ,0.397]
Inspection reports -0.019 (0.055) 0.731 [-0.127 ,0.089]
-0.033 (0.095) 0.731 [-0.218 ,0.153]
E↵ort index -0.184 (0.167) 0.270 [-0.510 ,0.143]
-0.060 (0.138) 0.667 [-0.331 ,0.212]
% Sta↵ Present 0.063 (0.280) 0.822 [-0.486 ,0.613]
0.298 (0.282) 0.290 [-0.255 ,0.852]
% unauthorized absent -0.014 (0.276) 0.960 [-0.555 ,0.527]
0.185 (0.243) 0.447 [-0.292 ,0.662]
Register book -0.301 (0.283) 0.287 [-0.856 ,0.254]
-0.301 (0.283) 0.287 [-0.856 ,0.254]
N. Outreach events -0.527 (0.282) 0.062 [-1.079 ,0.026]
-0.379 (0.304) 0.212 [-0.974 ,0.216]
Input index 0.064 (0.148) 0.668 [-0.227 ,0.354]
0.055 (0.135) 0.686 [-0.210 ,0.319]
Days w/o antimalarials 0.335 (0.247) 0.174 [-0.148 ,0.819]
0.962 (0.227) 0.000 [0.518 ,1.407]
Days w/o ORS 0.151 (0.275) 0.583 [-0.388 ,0.691]
0.219 (0.246) 0.374 [-0.264 ,0.701]
Funds received (millions) 0.005 (0.370) 0.989 [-0.720 ,0.731]
0.093 (0.375) 0.804 [-0.641 ,0.828]
Antimalaria SO 0.056 (0.280) 0.841 [-0.493 ,0.605]
ORS SO -0.174 (0.268) 0.516 [-0.699 ,0.351]
Total SO -0.203 (0.241) 0.398 [-0.675 ,0.268]
Utilization index 0.005 (0.127) 0.967 [-0.243 ,0.253]
0.015 (0.093) 0.875 [-0.168 ,0.198]
Out patients 0.256 (0.205) 0.212 [-0.146 ,0.658]
-0.253 (0.306) 0.410 [-0.853 ,0.348]
N. patients visiting clinic -0.125 (0.094) 0.183 [-0.309 ,0.059]
0.070 (0.142) 0.619 [-0.207 ,0.348]
OP referrals -0.106 (0.176) 0.545 [-0.450 ,0.238]
-0.005 (0.302) 0.988 [-0.596 ,0.586]
OP diagnoses 0.040 (0.104) 0.702 [-0.164 ,0.244]
0.189 (0.164) 0.247 [-0.131 ,0.510]
Tetanus doses 0.159 (0.184) 0.388 [-0.202 ,0.520]
-0.073 (0.195) 0.706 [-0.455 ,0.308]
Children immunized 0.411 (0.329) 0.212 [-0.235 ,1.056]
-0.119 (0.212) 0.573 [-0.534 ,0.295]
IPT doses 0.122 (0.225) 0.588 [-0.319 ,0.563]
-0.047 (0.163) 0.771 [-0.367 ,0.272]
Iron acid -0.013 (0.280) 0.962 [-0.562 ,0.535]
-0.130 (0.217) 0.548 [-0.556 ,0.295]
Free ITN -0.001 (0.247) 0.998 [-0.485 ,0.484]
-0.370 (0.237) 0.119 [-0.834 ,0.095]
Syphilis test -0.268 (0.214) 0.210 [-0.687 ,0.151]
-0.162 (0.295) 0.583 [-0.741 ,0.417]
Maternity admission -0.180 (0.194) 0.353 [-0.560 ,0.200]
-0.144 (0.139) 0.299 [-0.417 ,0.128]
Maternity delivery -0.248 (0.174) 0.155 [-0.590 ,0.093]
0.175 (0.332) 0.597 [-0.475 ,0.825]
Vitamin A (mothers) -0.398 (0.165) 0.016 [-0.722 ,-0.074]
-0.216 (0.189) 0.253 [-0.585 ,0.154]
Post natal -0.127 (0.132) 0.337 [-0.385 ,0.132]
0.087 (0.246) 0.724 [-0.395 ,0.569]
Vitamin A (children) 0.036 (0.306) 0.907 [-0.564 ,0.636]
0.235 (0.303) 0.438 [-0.358 ,0.829]
Deworming doses 0.090 (0.378) 0.812 [-0.651 ,0.830]
-0.215 (0.175) 0.218 [-0.557 ,0.127]
In columns 2-5 we report short-term e↵ects (1 year), and in columns 6-9, long-term e↵ects (year 2). Indices are constructedusing the approach developed by Kling et al., (2007). Standard errors are corrected by combining estimation results usingSeemingly Unrelated Regression (SUR) estimation.
14

Table 10: Health Outcomes Analysis (with covariates adjustment)
Short-term Long-term
Variable Coef SE P-val CI Coef SE P-val CI
Monitoring index -0.220 (0.158) 0.163 [-0.529 ,0.089]
-0.231 (0.192) 0.228 [-0.606 ,0.145]
DHO visits -0.104 (0.350) 0.767 [-0.791 ,0.583]
-0.142 (0.313) 0.649 [-0.755 ,0.471]
DHO calls -0.495 (0.353) 0.161 [-1.187 ,0.196]
-0.407 (0.184) 0.027 [-0.768 ,-0.046]
Inspector calls -0.566 (0.314) 0.071 [-1.182 ,0.049]
-0.327 (0.423) 0.438 [-1.156 ,0.501]
Inspector visits -0.454 (0.362) 0.209 [-1.164 ,0.255]
-0.337 (0.366) 0.357 [-1.054 ,0.381]
Inspection reports 0.010 (0.053) 0.846 [-0.094 ,0.114]
0.018 (0.092) 0.846 [-0.162 ,0.197]
E↵ort index -0.274 (0.262) 0.296 [-0.788 ,0.240]
-0.059 (0.131) 0.654 [-0.315 ,0.197]
% Sta↵ Present 0.063 (0.391) 0.872 [-0.703 ,0.830]
0.294 (0.272) 0.280 [-0.239 ,0.827]
% unauthorized absent 0.047 (0.504) 0.926 [-0.942 ,1.035]
0.202 (0.248) 0.415 [-0.283 ,0.688]
Register book -0.363 (0.351) 0.302 [-1.052 ,0.326]
-0.192 (0.254) 0.450 [-0.689 ,0.306]
N. Outreach events -0.892 (0.353) 0.012 [-1.585 ,-0.200]
-0.552 (0.346) 0.111 [-1.231 ,0.126]
Input index -0.059 (0.143) 0.681 [-0.339 ,0.221]
-0.029 (0.157) 0.855 [-0.336 ,0.279]
Days w/o antimalarials -0.011 (0.235) 0.963 [-0.472 ,0.450]
0.770 (0.258) 0.003 [0.265 ,1.275]
Days w/o ORS -0.082 (0.363) 0.821 [-0.794 ,0.630]
0.247 (0.246) 0.317 [-0.236 ,0.730]
Funds received (millions) -0.223 (0.389) 0.566 [-0.987 ,0.540]
-0.131 (0.514) 0.799 [-1.138 ,0.876]
Antimalaria SO -0.244 (0.377) 0.518 [-0.983 ,0.495]
ORS SO -0.241 (0.246) 0.327 [-0.723 ,0.241]
Total SO -0.507 (0.264) 0.055 [-1.025 ,0.011]
Utilization index 0.123 (0.129) 0.343 [-0.131 ,0.376]
-0.022 (0.096) 0.815 [-0.210 ,0.165]
Out patients 0.490 (0.212) 0.021 [0.075 ,0.906]
-0.024 (0.298) 0.936 [-0.608 ,0.560]
N. patients visiting clinic -0.235 (0.108) 0.029 [-0.446 ,-0.024]
0.061 (0.155) 0.693 [-0.242 ,0.364]
OP referrals -0.091 (0.148) 0.541 [-0.382 ,0.200]
0.018 (0.307) 0.953 [-0.583 ,0.619]
OP diagnoses -0.013 (0.115) 0.908 [-0.238 ,0.212]
0.161 (0.182) 0.376 [-0.195 ,0.517]
Tetanus doses 0.173 (0.220) 0.431 [-0.258 ,0.605]
-0.208 (0.201) 0.299 [-0.601 ,0.185]
Children immunized 0.337 (0.418) 0.420 [-0.483 ,1.156]
0.019 (0.211) 0.927 [-0.394 ,0.433]
IPT doses 0.410 (0.244) 0.092 [-0.067 ,0.888]
-0.084 (0.139) 0.544 [-0.356 ,0.188]
Iron acid 0.380 (0.304) 0.212 [-0.216 ,0.976]
0.038 (0.205) 0.853 [-0.365 ,0.441]
Free ITN 0.243 (0.301) 0.419 [-0.346 ,0.832]
-0.116 (0.265) 0.663 [-0.635 ,0.404]
Syphilis test 0.029 (0.187) 0.878 [-0.338 ,0.395]
-0.143 (0.350) 0.682 [-0.830 ,0.543]
Maternity admission 0.079 (0.202) 0.695 [-0.317 ,0.476]
-0.334 (0.131) 0.011 [-0.591 ,-0.078]
Maternity delivery 0.001 (0.176) 0.996 [-0.344 ,0.346]
0.035 (0.345) 0.919 [-0.642 ,0.712]
Vitamin A (mothers) -0.183 (0.139) 0.187 [-0.456 ,0.089]
-0.506 (0.158) 0.001 [-0.815 ,-0.196]
Post natal 0.176 (0.130) 0.178 [-0.080 ,0.431]
0.180 (0.232) 0.437 [-0.274 ,0.634]
Vitamin A (children) -0.212 (0.337) 0.529 [-0.872 ,0.448]
0.104 (0.386) 0.788 [-0.652 ,0.860]
Deworming doses -0.110 (0.277) 0.692 [-0.653 ,0.433]
-0.430 (0.260) 0.098 [-0.940 ,0.080]
In columns 2-5 we report short-term e↵ects (1 year), and in columns 6-9, long-term e↵ects (year 2). Indices are constructedusing the approach developed by Kling et al., (2007). Standard errors are corrected by combining estimation results usingSeemingly Unrelated Regression (SUR) estimation.
15

5 Change in outcome variables overtime
0
.2
.4
.6
.8M
ean
DEO
cal
ls
Control TreatmentBase mid end Base mid end
DEO calls
0
.5
1
1.5
2
2.5
Mea
n In
spec
tor c
alls
Control TreatmentBase mid end Base mid end
Inspector calls
0
.1
.2
.3
Mea
n DE
O v
isits
Control TreatmentBase mid end Base mid end
DEO visits
0
.5
1
1.5
Mea
n In
spec
tor v
isits
Control TreatmentBase mid end Base mid end
Inspector visits
0
.5
1
1.5
2
2.5M
ean
Insp
ecto
r rep
orts
Control TreatmentBase mid end Base mid end
Inspector reports
Figure 1: School monitoring: bar plots of outcome variables overtime
0
.05
.1
.15
Mea
n DH
O v
isits
Control TreatmentBase mid end Base mid end
DHO visits
0
.5
1
1.5
2
Mea
n DH
O c
alls
Control TreatmentBase mid end Base mid end
DHO calls
0
.5
1
1.5
2
Mea
n In
spec
tor c
alls
Control TreatmentBase mid end Base mid end
Inspector calls
0
.2
.4
.6
.8
1
Mea
n In
spec
tor v
isits
Control TreatmentBase mid end Base mid end
Inspector visits
0
1
2
3
4
Mea
n In
spec
tion
repo
rts
Control TreatmentBase mid end Base mid end
Inspection reports
0
.2
.4
.6
.8
1
Mea
n In
spec
tion
(yr.)
Control TreatmentBase mid end Base mid end
Inspection (yr.)
Figure 2: Health monitoring: bar plots of outcome variables overtime
16

0
.2
.4
.6
.8
Mea
n %
Tea
cher
s pr
esen
t (re
cord
s)
Control TreatmentBase mid end Base mid end
% Teachers present (records)
0
.1
.2
.3
.4
.5
Mea
n %
Tea
cher
s pr
esen
t (ob
serv
ed)
Control TreatmentBase mid end Base mid end
% Teachers present (observed)
0
.1
.2
.3
.4
.5
Mea
n M
eani
ngfu
l boa
rd
Control TreatmentBase mid end Base mid end
Meaningful board
0
.2
.4
.6
Mea
n Te
ache
r eng
aged
Control TreatmentBase mid end Base mid end
Teacher engaged
0
.5
1
1.5
2
Mea
n St
aff m
eetin
gs
Control TreatmentBase mid end Base mid end
Staff meetings
Figure 3: School e↵ort: bar plots of outcome variables overtime
0
.2
.4
.6
Mea
n He
alth
sta
ff pr
esen
t
Control TreatmentBase mid end Base mid end
Health staff present
0
.2
.4
.6
.8
1
Mea
n Un
auth
orize
d he
alth
sta
ff ab
senc
e (in
vers
e)
Control TreatmentBase mid end Base mid end
Unauthorized health staff absence (inverse)
0
.2
.4
.6
.8
Mea
n Re
gist
er b
ook
Control TreatmentBase mid end Base mid end
Register book
0
1
2
3
4
Mea
n O
utre
ach
Control TreatmentBase mid end Base mid end
Outreach
Figure 4: Health e↵ort: bar plots of outcome variables overtime
17

0
5
10
15
Mea
n N
. tea
cher
s em
ploy
ed
Control TreatmentBase mid end Base mid end
N. teachers employed
0
.2
.4
.6
.8
1
Mea
n Te
ache
rs tr
ansf
erre
d to
sch
ool
Control TreatmentBase mid end Base mid end
Teachers transferred to school
0
.2
.4
.6
.8
Mea
n St
uden
ts p
er u
nifo
rm
Control TreatmentBase mid end Base mid end
Students per uniform
0
.2
.4
.6
.8
1
Mea
n St
uden
ts p
er b
ook
Control TreatmentBase mid end Base mid end
Students per book
0
.2
.4
.6
.8
Mea
n St
uden
ts p
er p
enci
l
Control TreatmentBase mid end Base mid end
Students per pencil
Figure 5: School inputs: bar plots of outcome variables overtime
-20
-15
-10
-5
0
Mea
n Da
ys w
/o a
ntim
alar
ials
Control TreatmentBase mid end Base mid end
Days w/o antimalarials
-15
-10
-5
0
Mea
n Da
ys w
/o O
RS
Control TreatmentBase mid end Base mid end
Days w/o ORS
-20
-15
-10
-5
0
Mea
n An
timal
aria
SO
Control TreatmentBase mid end Base mid end
Antimalaria SO
-20
-15
-10
-5
0
Mea
n O
RS S
O
Control TreatmentBase mid end Base mid end
ORS SO
-.5
-.4
-.3
-.2
-.1
0
Mea
n To
tal S
O
Control TreatmentBase mid end Base mid end
Total SO
0
1
2
3
4
5
Mea
n Fu
nds
rece
ived
(milli
ons)
Control TreatmentBase mid end Base mid end
Funds received (millions)
Figure 6: Health inputs: bar plots of outcome variables overtime
18

6 Treatment e↵ects and messaging intensity
-4
-2
0
2
4C
hang
e m
onito
ring
0 100 200 300 400All relevant messages
School monitoring
-4
-2
0
2
4
Cha
nge
effo
rt
0 100 200 300 400All relevant messages
School effort
-4
-2
0
2
4
Cha
nge
inpu
t
0 100 200 300 400All relevant messages
School input
-4
-2
0
2
4
Cha
nge
mon
itorin
g
0 2 4 6Education messages
School monitoring
-4
-2
0
2
4C
hang
e ef
fort
0 2 4 6Education messages
School effort
-4
-2
0
2
4
Cha
nge
inpu
t
0 2 4 6Education messages
School input
Figure 7: Education: change from baseline to midline (short-term) against messages sent
-2
-1
0
1
2
Cha
nge
mon
itorin
g
0 100 200 300 400All relevant messages
Health monitoring
-2
-1
0
1
2
Cha
nge
effo
rt
0 100 200 300 400All relevant messages
Health effort
-2
-1
0
1
2
Cha
nge
inpu
t
0 100 200 300 400All relevant messages
Health input
-2
-1
0
1
2
Cha
nge
mon
itorin
g
0 5 10Health messages
Health monitoring
-2
-1
0
1
2
Cha
nge
effo
rt
0 5 10Health messages
Health effort
-2
-1
0
1
2
Cha
nge
inpu
t
0 5 10Health messages
Health input
Figure 8: Health: change from baseline to midline (short-term) against messages sent
19

-1
0
1
2
3
4
base
line
edu
mon
itorin
g
0 2 4 6Education messages
School monitoring
-2
-1
0
1
2
3
base
line
edu
effo
rt
0 2 4 6Education messages
School effort
-1
0
1
2
3
4
base
line
edu
inpu
t
0 2 4 6Education messages
School input
-2
0
2
4
base
line
edu
outc
ome
0 2 4 6Education messages
School outcome
Messaging and baseline conditions
Figure 9: Education: outcome indices at baseline against messages sent. Figure shows that placesthat were worse o↵ to begin with did not necessarily send a larger number of messages via U-Bridge.
-2
-1
0
1
2
base
line
mon
itorin
g
0 5 10N. health messages
Health monitoring
-2
-1
0
1
base
line
effo
rt
0 5 10N. health messages
Health effort
-2
-1
0
1
2
base
line
inpu
t
0 5 10N. health messages
Health input
-1.5
-1
-.5
0
.5
1
base
line
utiliz
atio
n
0 5 10N. health messages
Health utilization
Figure 10: Health: outcome indices at baseline against messages sent. Figure shows that placesthat were worse o↵ to begin with did not necessarily send a larger number of messages via U-Bridge
20

7 Heterogenous e↵ects by distance to district HQs
0
100
200
300
Tota
l mes
sage
s (c
lust
er)
2 2.5 3 3.5 4Distance to Arua (log)
Total messaging
0
5
10
15
20
Educ
atio
n m
essa
ges
(clu
ster
)
2 2.5 3 3.5 4Distance to Arua (log)
Education messaging
0
5
10
15
20
Hea
lth m
essa
ges
(clu
ster
)
2 2.5 3 3.5 4Distance to Arua (log)
Health messaging
0
5
10
15
20
Wat
er m
essa
ges
(clu
ster
)
2 2.5 3 3.5 4Distance to Arua (log)
Water messaging
Messaging and distance to district HQs
Figure 11: Cluster-level: SMS messaging by distance to Arua
0
50
100
150
Tota
l mes
sage
s (c
lust
er)
0 20 40 60Distance to Arua (log)
Total messaging
0
5
10
15
Educ
atio
n m
essa
ges
(clu
ster
)
0 20 40 60Distance to Arua (log)
Education messaging
0
5
10
Hea
lth m
essa
ges
(clu
ster
)
0 20 40 60Distance to Arua (log)
Health messaging
0
5
10
15
Wat
er m
essa
ges
(clu
ster
)
0 20 40 60Distance to Arua (log)
Water messaging
Messaging and distance to district HQs
Figure 12: Village-level: SMS messaging by distance to Arua
21

L M H
-1.5-1-.5
0.51
1.5
Mar
gina
l Effe
ct o
f U-B
ridge
on
mon
itorin
g
0 20 40 60Moderator: Distance
School monitoring
L M H
-1.5-1-.5
0.51
1.5
Mar
gina
l Effe
ct o
f U-B
ridge
on
effo
rt
0 20 40 60Moderator: Distance
School effort
L M H
-2
-1
0
1
2
Mar
gina
l Effe
ct o
f U-B
ridge
on
inpu
t
0 20 40 60Moderator: Distance
School input
L M H
-1.5
-1
-.5
0
.5
1
Mar
gina
l Effe
ct o
f U-B
ridge
on
outc
ome
0 20 40 60Moderator: Distance
School outcome
Figure 13: Education services: Heterogenous treatment e↵ect by distance to Arua
L M H
-3
-2
-1
0
1
2
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
1 2 3 4 5Moderator: Distance
Health monitoring
L M H
-4
-2
0
2
4
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
1 2 3 4 5Moderator: Distance
Health effort
L M H
-2
-1
0
1
2
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
1 2 3 4 5Moderator: Distance
Health input
L M H
-3
-2
-1
0
1
2
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
1 2 3 4 5Moderator: Distance
Health utilization
Figure 14: Health services: Heterogenous treatment e↵ect by distance to Arua
22

L M H
-3
-2
-1
0
1
2
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
0 20 40 60Moderator: Distance
Water Services
L M H
-1
-.5
0
.5
1
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
0 20 40 60Moderator: Distance
Water Requests
Figure 15: Water parts & services: Heterogenous treatment e↵ect by distance to Arua
23

8 Heterogenous e↵ects by community’s wealth
0
100
200
300
Tota
l mes
sage
s (c
lust
er)
-2 -1 0 1 2Wealth
Total messaging
0
5
10
15
20
Educ
atio
n m
essa
ges
(clu
ster
)
-2 -1 0 1 2Wealth
Education messaging
0
5
10
15
20
Hea
lth m
essa
ges
(clu
ster
)
-2 -1 0 1 2Wealth
Health messaging
0
5
10
15
20
Wat
er m
essa
ges
(clu
ster
)
-2 -1 0 1 2Wealth
Water messaging
Messaging and cluster wealth
Figure 16: Cluster-level: SMS messaging by community’s wealth
0
50
100
150
Tota
l mes
sage
s (c
lust
er)
-4 -2 0 2 4Wealth
Total messaging
0
5
10
15
Educ
atio
n m
essa
ges
(clu
ster
)
-4 -2 0 2 4Wealth
Education messaging
0
5
10
Hea
lth m
essa
ges
(clu
ster
)
-4 -2 0 2 4Wealth
Health messaging
0
5
10
15
Wat
er m
essa
ges
(clu
ster
)
-4 -2 0 2 4Wealth
Water messaging
Messaging and village wealth
Figure 17: Cluster-level: SMS messaging by community’s wealth
24

L M H
-3
-2
-1
0
1
2
Mar
gina
l Effe
ct o
f U-B
ridge
on
mon
itorin
g
-2 0 2 4Moderator: Wealth
School monitoring
L M H
-3
-2
-1
0
1
2
Mar
gina
l Effe
ct o
f U-B
ridge
on
effo
rt
-2 0 2 4Moderator: Wealth
School effort
L M H
-3-2-10123
Mar
gina
l Effe
ct o
f U-B
ridge
on
inpu
t
-2 0 2 4Moderator: Wealth
School input
L M H
-3
-2
-1
0
1
Mar
gina
l Effe
ct o
f U-B
ridge
on
outc
ome
-2 0 2 4Moderator: Wealth
School outcome
Figure 18: Education services: Heterogenous treatment e↵ect by village wealth; lower values arepoorer villages
L M H
-3-2-1012
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
-2 -1 0 1 2Moderator: Wealth
Health monitoring
L M H
-3-2-1012
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
-2 -1 0 1 2Moderator: Wealth
Health effort
L M H
-3
-2
-1
0
1
2
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
-2 -1 0 1 2Moderator: Wealth
Health input
L M H
-3
-2
-1
0
1
2
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
-2 -1 0 1 2Moderator: Wealth
Health utilization
Figure 19: Health services: Heterogenous treatment e↵ect by cluster wealth; lower values arepoorer clusters
25

L M H
-3
-2
-1
0
1
2
3
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
-4 -2 0 2 4Moderator: Poverty
Water Services
L M H
-1
-.5
0
.5
1
Mar
gina
l Effe
ct o
f UBr
idge
on
Y
-4 -2 0 2 4Moderator: Poverty
Water Requests
Figure 20: Water village requests: Heterogenous treatment e↵ect by poverty
26

References
Anderson, Michael L. 2008. “Multiple Inference and Gender Di↵erences in the E↵ects of Early
Intervention: A Reevaluation of the Abecedarian, Perry Preschool, and Early Training Projects.”
Journal of the American Statistical Association 103 (484): 1481–1495.
Kling, Je↵rey R, Je↵rey B Liebman, and Lawrence F Katz. 2007. “Experimental Analysis of
Neighborhood E↵ects.” Econometrica 75 (1): 83–119.
27
Recommended