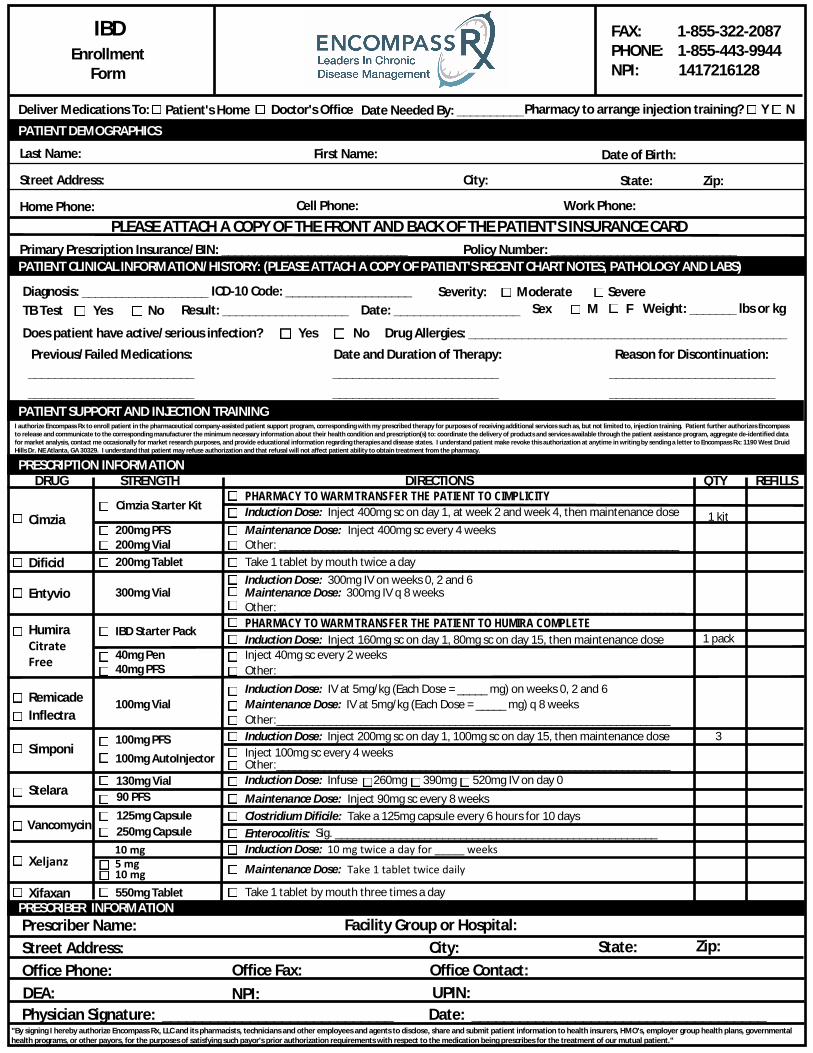
EnrollmentForm
FAX: 1-855-322-2087PHONE: 1-855-443-9944NPI: 1417216128
Deliver Medications To: Patient's Home Doctor's Office Date Needed By: __________Pharmacy to arrange injection training? Y N
PATIENT DEMOGRAPHICS
Last Name: First Name: Date of Birth:
Street Address: City:
Home Phone: Cell Phone: Work Phone:
State: Zip:
PLEASE ATTACH A COPY OF THE FRONT AND BACK OF THE PATIENT'S INSURANCE CARD
PATIENT CLINICAL INFORMATION/HISTORY: (PLEASE ATTACH A COPY OF PATIENT'S RECENT CHART NOTES, PATHOLOGY AND LABS)
Diagnosis: ___________________
PRESCRIPTION INFORMATION
Cimzia
Dificid
DRUG STRENGTH DIRECTIONS QTY REFILLS
PRESCRIBER INFORMATIONPrescriber Name:Street Address:Office Phone:DEA:Physician Signature: _____________________________
Facility Group or Hospital:
Office Fax:NPI: UPIN:
Date: _____________________________________
State: Zip:
ICD-10 Code: ___________________ Severity: Moderate SevereTB Test Yes No Result: ___________________ Date: ___________________ Sex M F
Does patient have active/serious infection? Yes No Drug Allergies: ________________________________________________
Weight: _______ lbs or kg
Previous/Failed Medications: Date and Duration of Therapy: Reason for Discontinuation:_________________________ _________________________ _________________________
PATIENT SUPPORT AND INJECTION TRAININGI authorize Encompass Rx to enroll patient in the pharmaceutical company-assisted patient support program, corresponding with my prescribed therapy for purposes of receiving additional services such as, but not limited to, injection training. Patient further authorizes Encompassto release and communicate to the corresponding manufacturer the minimum necessary information about their health condition and prescription(s) to: coordinate the delivery of products and services available through the patient assistance program, aggregate de-identified datafor market analysis, contact me occasionally for market research purposes, and provide educational information regarding therapies and disease states. I understand patient make revoke this authorization at anytime in writing by sending a letter to Encompass Rx: 1190 West DruidHills Dr. NE Atlanta, GA 30329. I understand that patient may refuse authorization and that refusal will not affect patient ability to obtain treatment from the pharmacy.
Cimzia Starter Kit
200mg PFS200mg Vial200mg Tablet
HumiraCitrateFree
IBD Starter Pack
40mg Pen40mg PFS
Simponi
Xifaxan
Inject 400mg sc on day 1, at week 2 and week 4, then maintenance doseInduction Dose:
Induction Dose:
Inject 400mg sc every 4 weeksOther: ___________________________________________________________________
Inject 160mg sc on day 1, 80mg sc on day 15, then maintenance dose
Take 1 tablet by mouth twice a day
Inject 40mg sc every 2 weeksOther:__________________________________________________________________
Inject 200mg sc on day 1, 100mg sc on day 15, then maintenance doseInject 100mg sc every 4 weeks
Take 1 tablet by mouth three times a day
_________________________ _________________________ _________________________
IBD
Induction Dose:
Other:__________________________________________________________________
Remicade
Maintenance Dose:
EntyvioInduction Dose:Maintenance Dose:Other: ____________________________________________________________________
300mg Vial300mg IV on weeks 0, 2 and 6
300mg IV q 8 weeks
100mg VialInduction Dose:Maintenance Dose:Other:__________________________________________________________________
IV at 5mg/kg (Each Dose = _____ mg) on weeks 0, 2 and 6IV at 5mg/kg (Each Dose = _____ mg) q 8 weeks
PHARMACY TO WARM TRANSFER THE PATIENT TO HUMIRA COMPLETE
VancomycinClostridium Dificile: Take a 125mg capsule every 6 hours for 10 daysEnterocolitis: Sig. ______________________________________________________
Induction Dose:Maintenance Dose:
Infuse 260mg 390mg 520mg IV on day 0Inject 90mg sc every 8 weeks
Stelara
1 kit
1 pack
3
"By signing I hereby authorize Encompass Rx, LLC and its pharmacists, technicians and other employees and agents to disclose, share and submit patient information to health insurers, HMO's, employer group health plans, governmentalhealth programs, or other payors, for the purposes of satisfying such payor's prior authorization requirements with respect to the medication being prescribes for the treatment of our mutual patient."
Primary Prescription Insurance/BIN: ____________________________ Policy Number: ____________________________
PHARMACY TO WARM TRANSFER THE PATIENT TO CIMPLICITY
Inflectra
City:Office Contact:
550mg Tablet
100mg PFS 100mg AutoInjector
130mg Vial90 PFS125mg Capsule250mg Capsule
Xeljanz 5 mg10 mg
10 mg Induction Dose: 10 mg twice a day for _____ weeks
Maintenance Dose: Take 1 tablet twice daily
Recommended

















