I have financial relationships to disclose Consultant for: st Jude, Boston, Sorin, Biotronik, Medtronic, Sanofi, Merck,
Menarin Research support from: st Jude, Boston, Sorin, Biotronik, Medtronic, Sanofi,
Merck, Menarin
Atrial Fibrillation and Sports.
Hospital Clinic. Universitat de Barcelona
• 1777 competitive athletes without heart disease
• Mean age 24± 6 years
• Mean age at most recent assessment 33±6
• mean time of sports involvement 6 years
• 61 % continued with the training during FU
Pellicia et al. JACC 2005
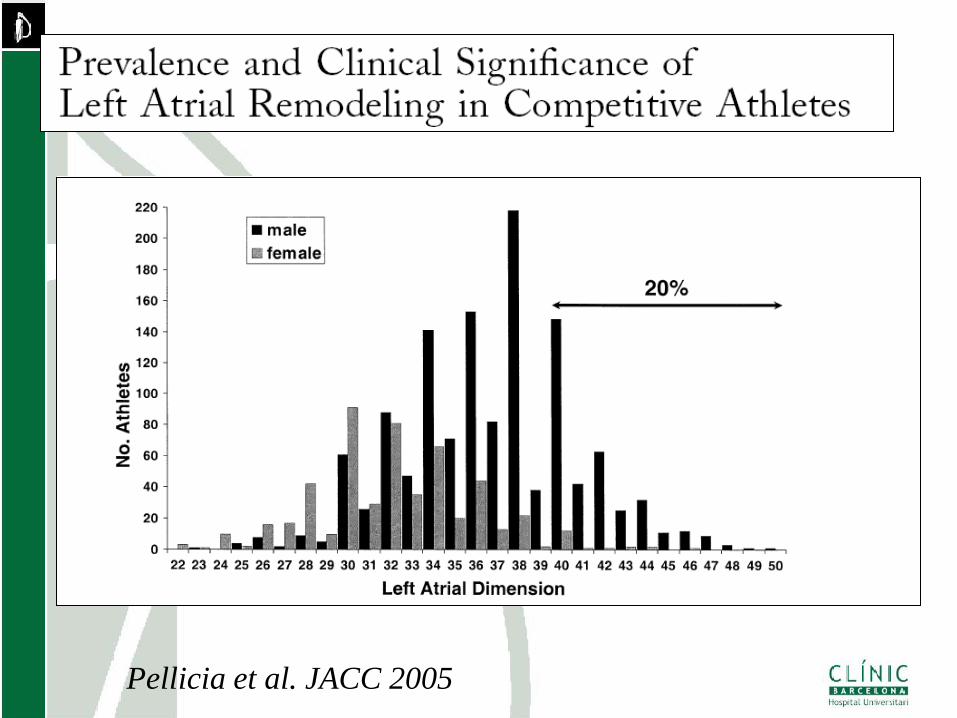
Pellicia et al. JACC 2005
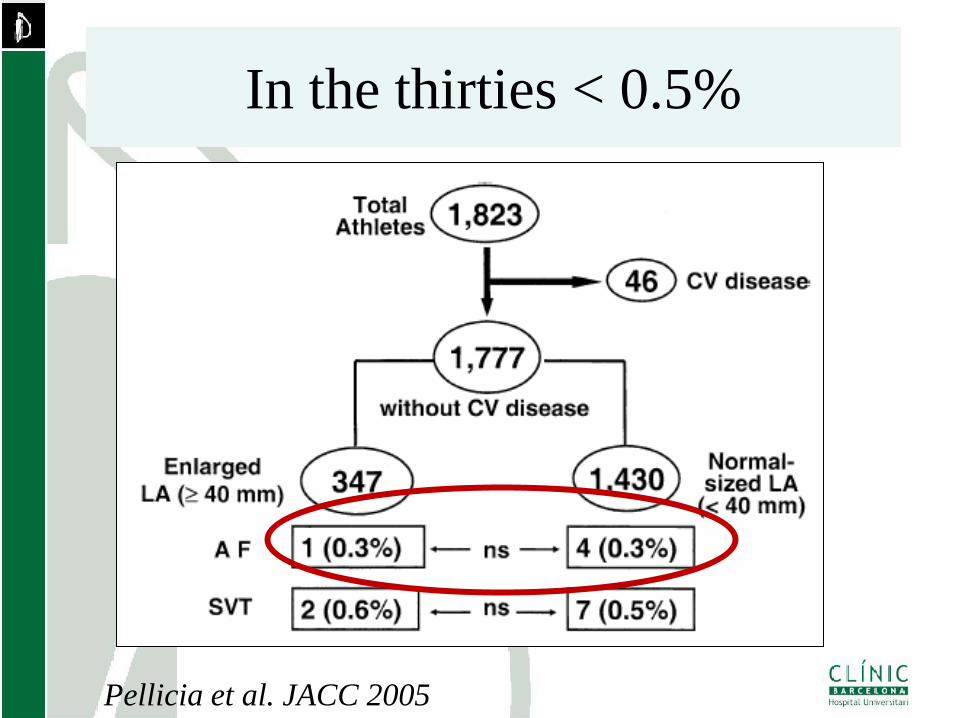
In the thirties < 0.5%
Pellicia et al. JACC 2005
Lone atrial fibrillation in Marathon runners
Hospital Clinic. Thorax Institute. University of Barcelona,
Hospital del Mar. Autonomous University of Barcelona
Institut Municipal Investigacions Mèdiques IMIM. Barcelona.
Molina et al. Europace 2008
• 270 healthy men that ran the marathon in
Barcelona in 1993.
• Control group: 305 healthy sedentary men <
300 Kcal/day of physical activity, recruited at
the REGICOR study
Methods
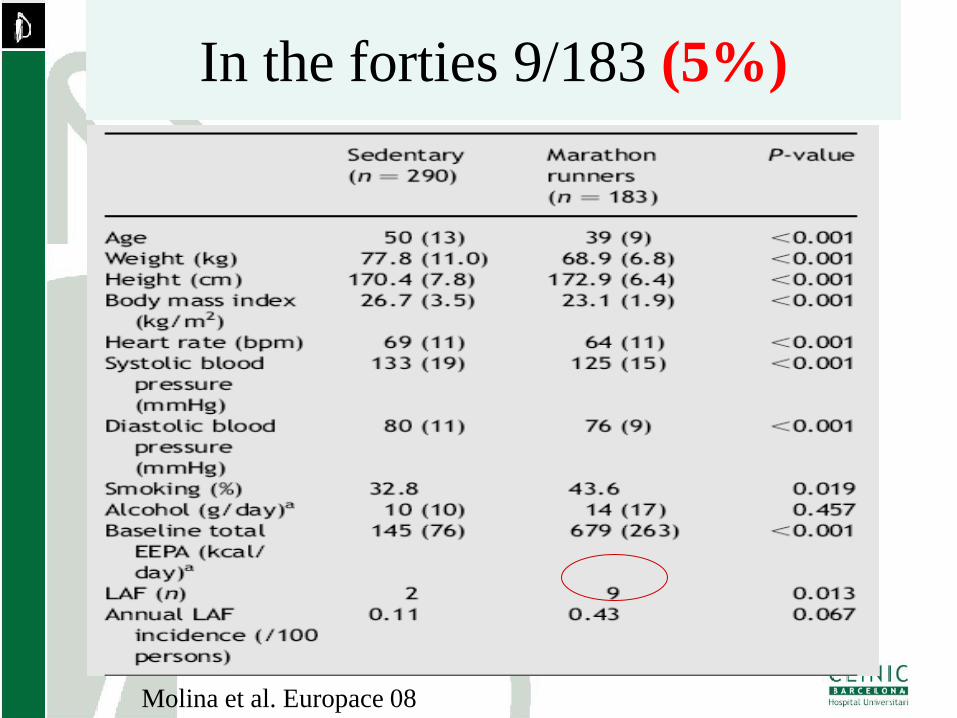
Molina et al. Europace 08
In the forties 9/183 (5%)
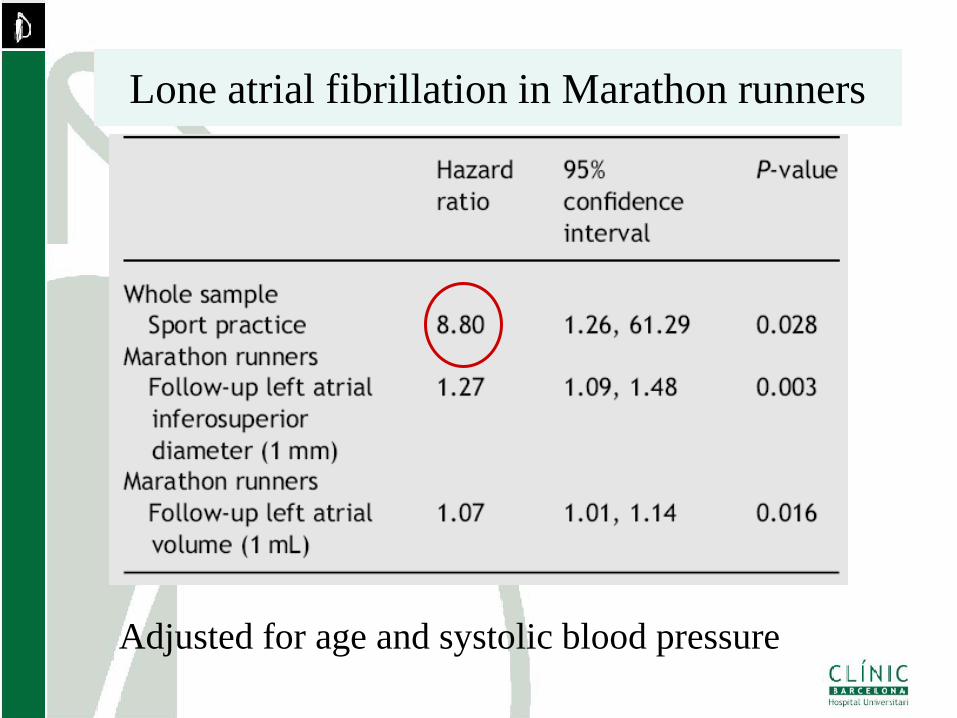
Lone atrial fibrillation in Marathon runners
Adjusted for age and systolic blood pressure
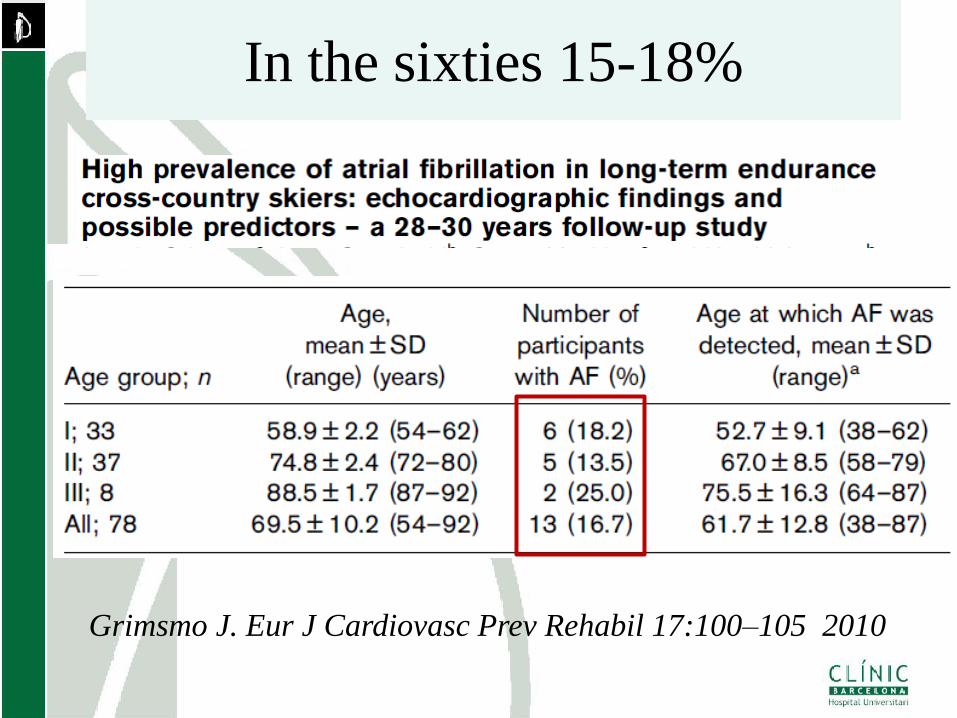
Grimsmo J. Eur J Cardiovasc Prev Rehabil 17:100–105 2010
In the sixties 15-18%
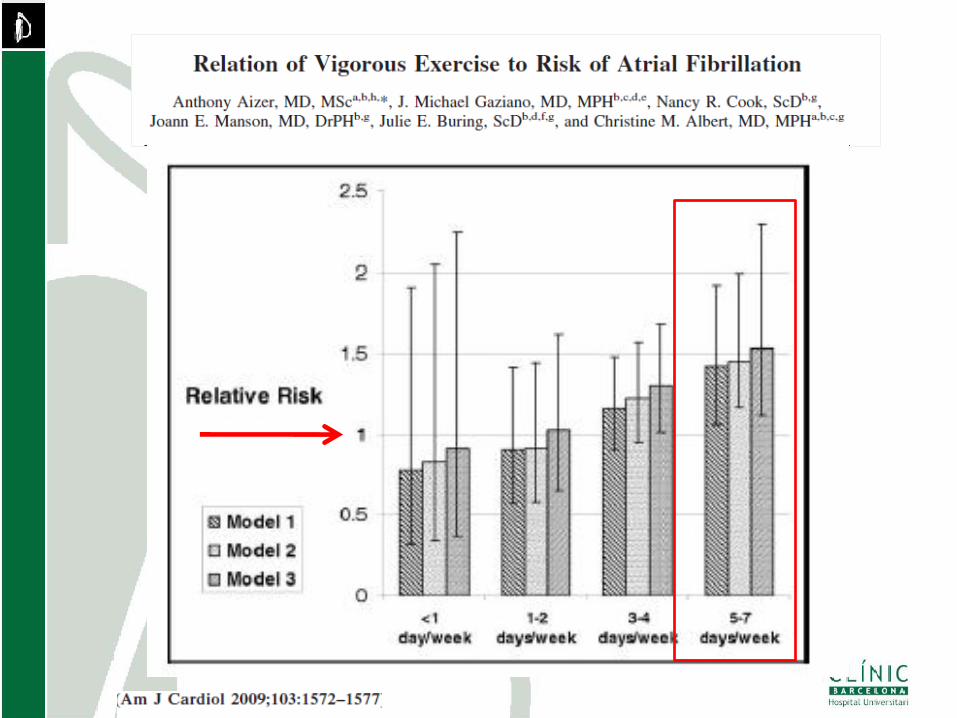
Athletes or vigorous exercise?
Is there a threshold?
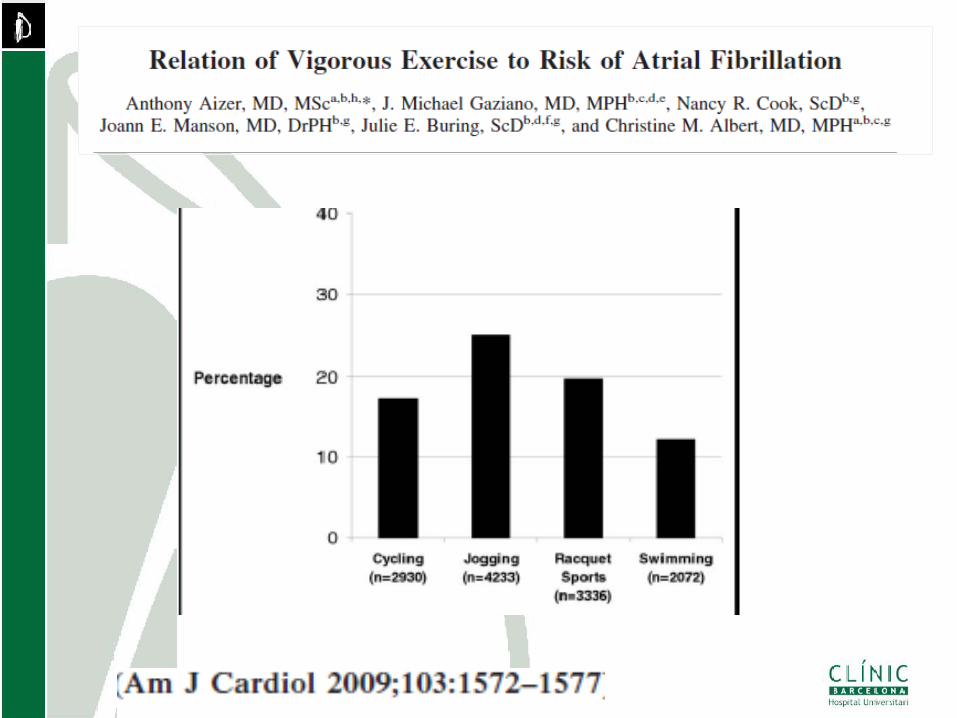
• 16921 participants at the Physicians
Health Study
• Healthy individuals
• 12 years follow up
• 70 patients with lone AF younger than 65y.
• Regular sport practice 65% among patients with
AF and 15% in the general male population of
individuals younger than 65 in Catalonia
(REGICOR study)
Hospital Clínic. University of Barcelona. Institut Municipal d’Investigacions Mèdiques de Barcelona.
Int J Cardiol 2005
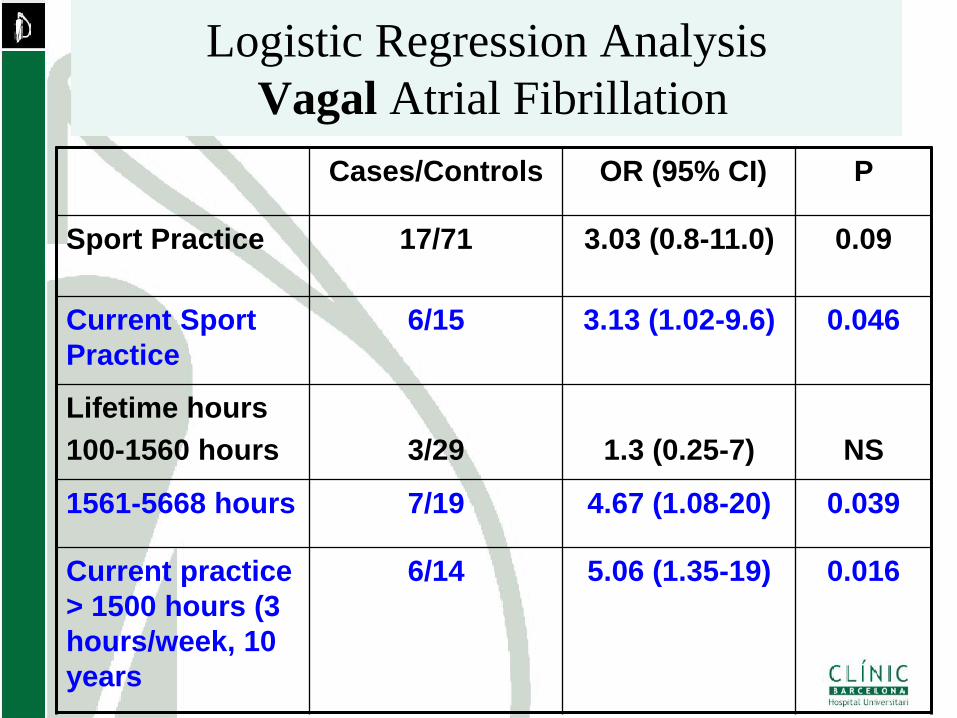
Logistic Regression Analysis
Vagal Atrial Fibrillation
Cases/Controls OR (95% CI) P
Sport Practice 17/71 3.03 (0.8-11.0) 0.09
Current Sport
Practice
6/15 3.13 (1.02-9.6) 0.046
Lifetime hours
100-1560 hours
3/29
1.3 (0.25-7)
NS
1561-5668 hours 7/19 4.67 (1.08-20) 0.039
Current practice
> 1500 hours (3
hours/week, 10
years
6/14 5.06 (1.35-19) 0.016

Is sports related lone AF a
familial disease?
Familial Atrial Fibrillation and
sports: hypothesis • “Dose related risk” of AF in sports goes
against a familial disease
• Genetic forms have a high penetrance and
does not need the “trigger effect of sport”
• Familial forms of AF are very uncommon
and a family history is rarely seen.
• Athletes show deep structural changes, that
may explain AF withouth the need of other
etiologic factors.
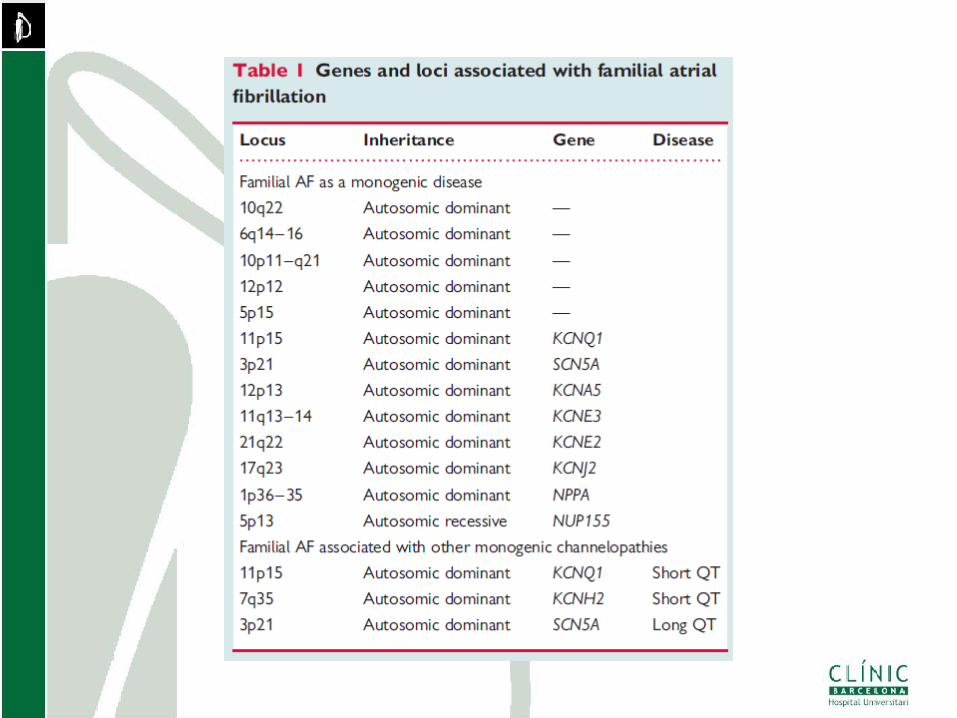
Genetic Predisposition or Genetic
Disease
• Atrial fibrillation as a monogenic disease
• Atrial firillation associated with other
monogenic diseases
• Genetic predispostion to acquired atrial
fibrillation
• Wolff L. N Engl J Med. 1943
• Gould WL Arch Int Med 1957
• Phair WB Canad Med Ass 1963
• Derrida JP et al Nouv Pres Med 1976
• Wen-tai Y Chin Med J 1983
• Ardiaca A et al Rev Esp Card 1987
ATRIAL FIBRILLATION AS A MONOGENIC
DISEASE
Historical Perspective
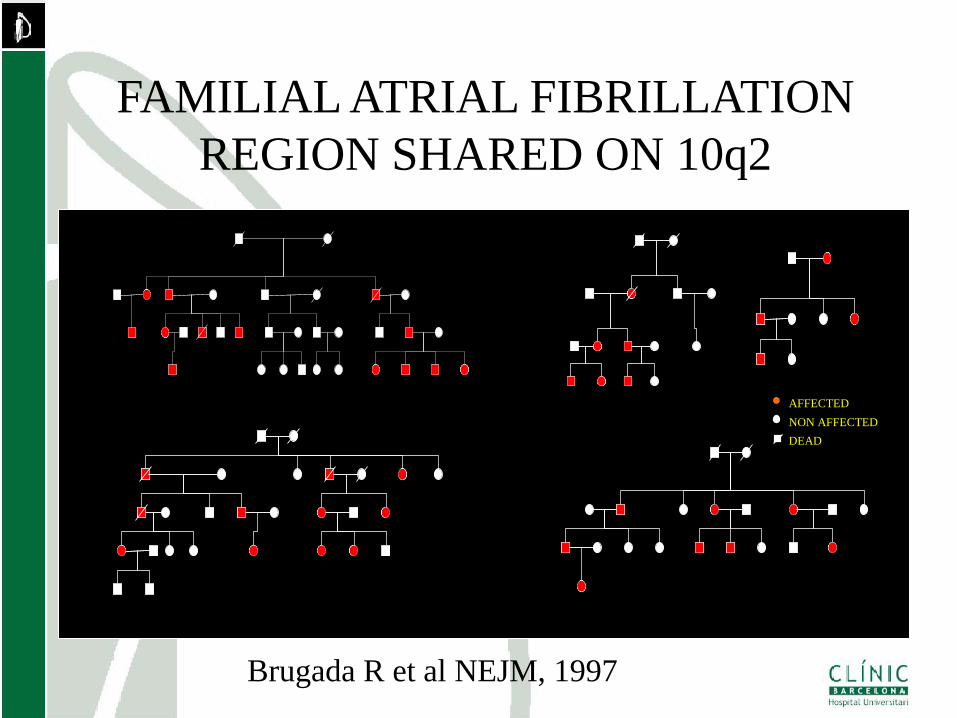
I:1 I:2
FAMILIAL ATRIAL FIBRILLATION
REGION SHARED ON 10q2
AFFECTED
NON AFFECTED
DEAD
Brugada R et al NEJM, 1997
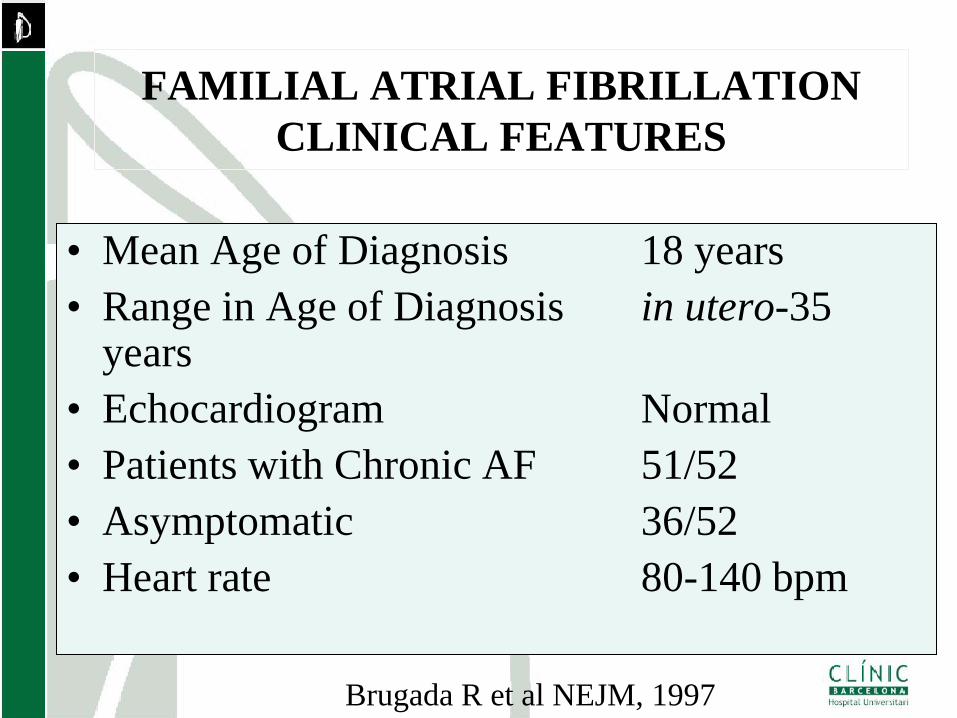
• Mean Age of Diagnosis 18 years
• Range in Age of Diagnosis in utero-35 years
• Echocardiogram Normal
• Patients with Chronic AF 51/52
• Asymptomatic 36/52
• Heart rate 80-140 bpm
FAMILIAL ATRIAL FIBRILLATION
CLINICAL FEATURES
Brugada R et al NEJM, 1997
Chen YH, et al. Science 2003
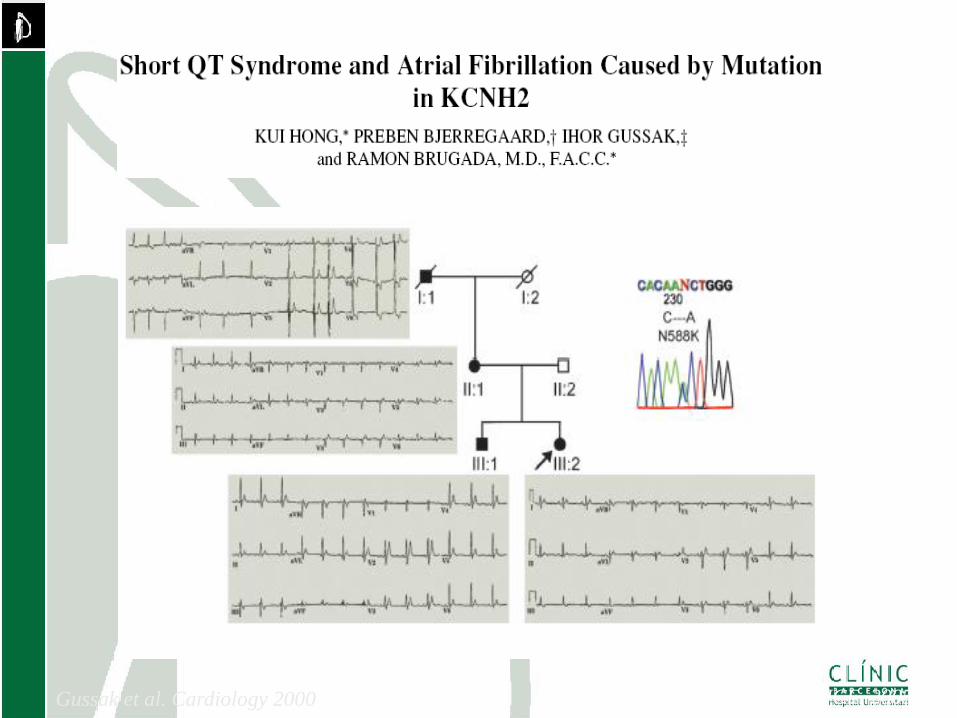
Hong et al. JCE, 2005 Gussak et al. Cardiology 2000
Clinical Implications
• Each family appears to have its own gene
• No change in clinical approach
• Penetrance appears high
Date of download: 8/18/2012 Copyright © 2012 American Medical
Association. All rights reserved.
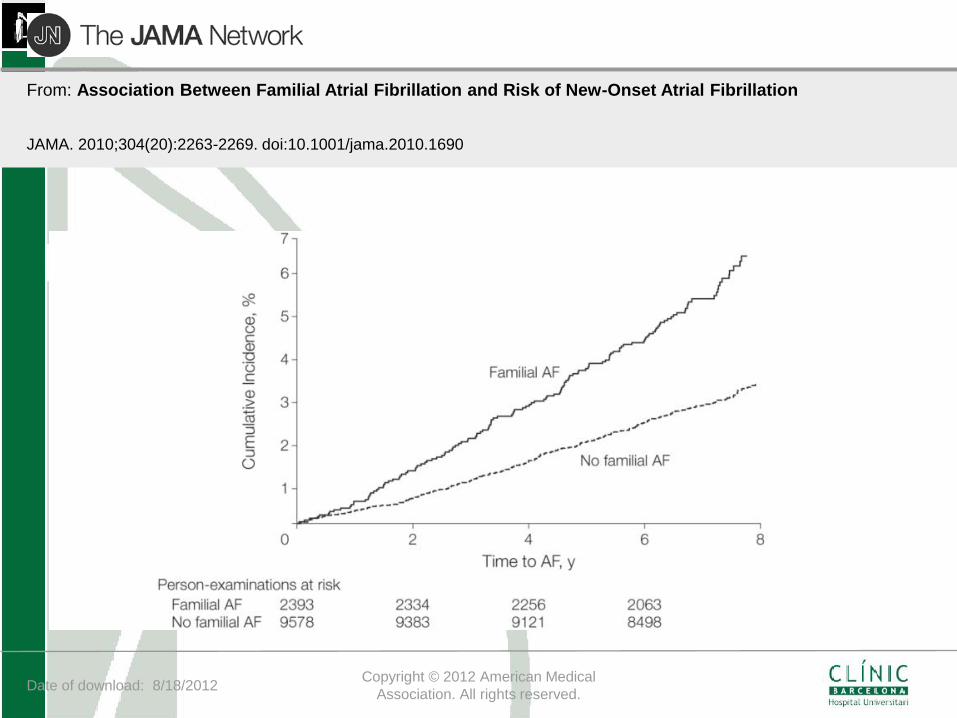
From: Association Between Familial Atrial Fibrillation and Risk of New-Onset Atrial Fibrillation
JAMA. 2010;304(20):2263-2269. doi:10.1001/jama.2010.1690
Date of download: 8/18/2012 Copyright © 2012 American Medical
Association. All rights reserved.
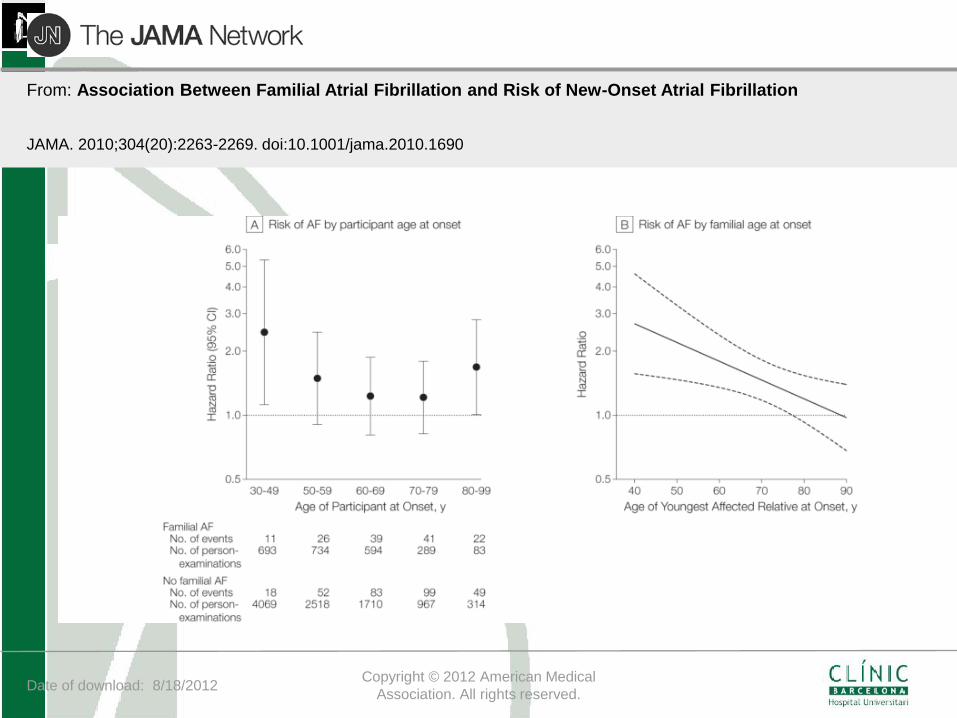
From: Association Between Familial Atrial Fibrillation and Risk of New-Onset Atrial Fibrillation
JAMA. 2010;304(20):2263-2269. doi:10.1001/jama.2010.1690
Physical activity, height and left atrial size are
independent risk factors for lone atrial fibrillation in
middle aged healthy individuals
- Thorax Institute. Hospital Clinic, University of Barcelona
- IMIM. Institut Municipal de Investigació Mèdica. Barcelona
Mont L, Tamborero D, Elosua R, Molina I, Collvinent B,
Sitges M, Vidal B, Scalise A, Tejeira A, Berruezo and
Brugada J on behalf of the GIRAFA (Grup Integrat de
Recerca en FA) investigators
Mont et al. Europace 2008
Methods
• Design: Prospective, case-control study
• Population:
– 107 consecutive patients younger 18 to 65
– Recent onset Lone AF, seen at the emergency
room (> 48 hours).
• Controls: 1:1 age and sex matched controls
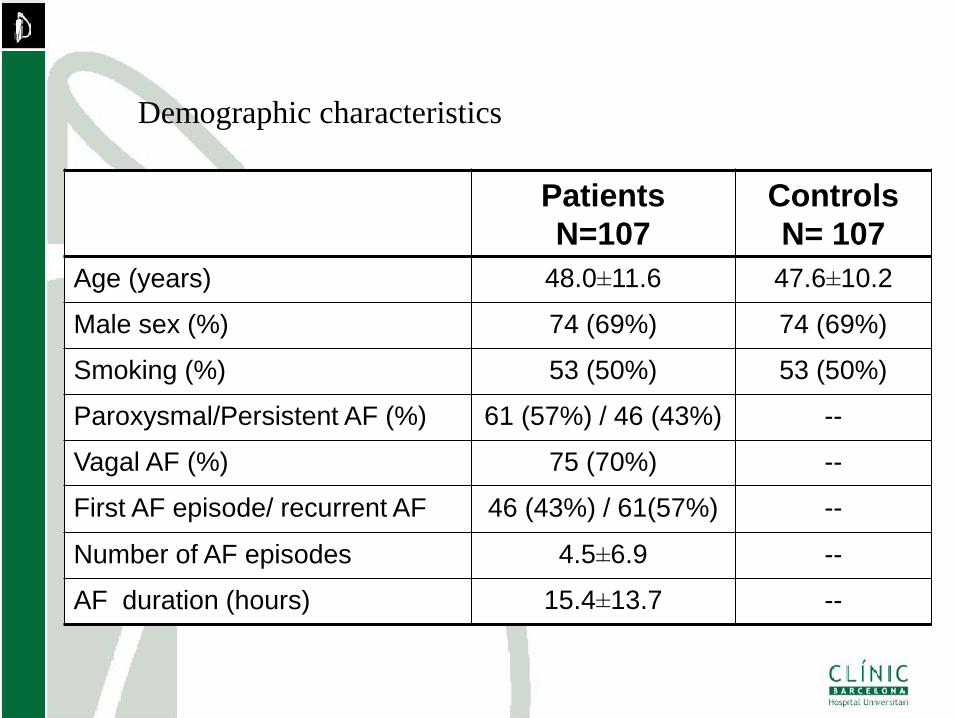
Patients
N=107
Controls
N= 107
Age (years) 48.0±11.6 47.6±10.2
Male sex (%) 74 (69%) 74 (69%)
Smoking (%) 53 (50%) 53 (50%)
Paroxysmal/Persistent AF (%) 61 (57%) / 46 (43%) --
Vagal AF (%) 75 (70%) --
First AF episode/ recurrent AF 46 (43%) / 61(57%) --
Number of AF episodes 4.5±6.9 --
AF duration (hours) 15.4±13.7 --
Demographic characteristics
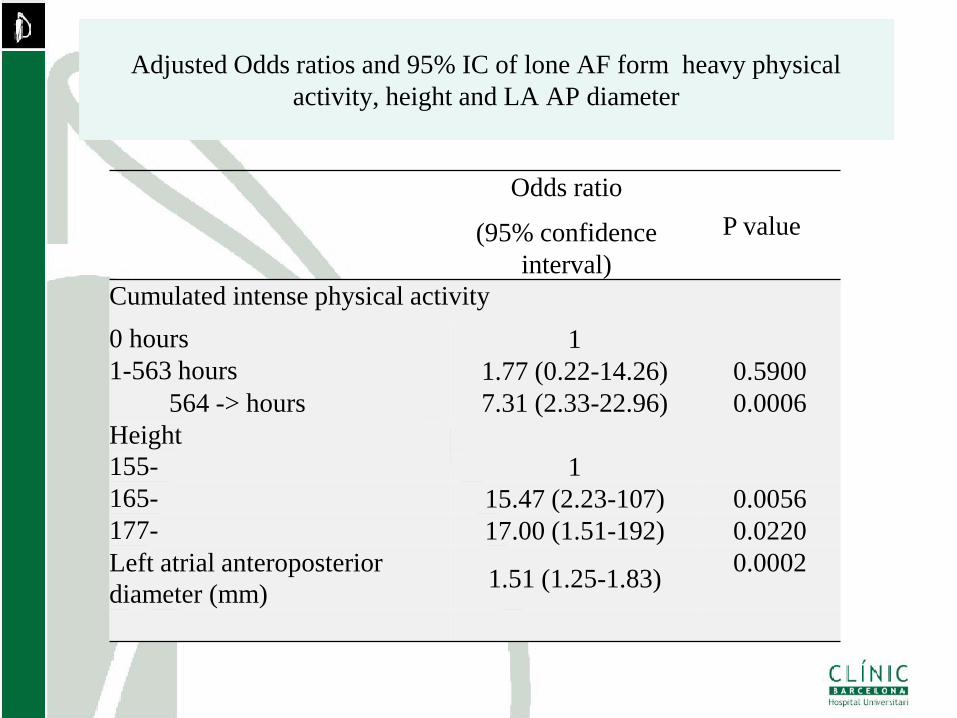
Adjusted Odds ratios and 95% IC of lone AF form heavy physical
activity, height and LA AP diameter
Odds ratio
(95% confidence
interval)
P value
Cumulated intense physical activity
0 hours 1
1-563 hours 1.77 (0.22-14.26) 0.5900
564 -> hours 7.31 (2.33-22.96) 0.0006
Height
155- 1
165- 15.47 (2.23-107) 0.0056
177- 17.00 (1.51-192) 0.0220
Left atrial anteroposterior
diameter (mm) 1.51 (1.25-1.83)
0.0002
Sustained Endurance Training Creates a
Substrate for Atrial Fibrillation in Rats
Hospital Clínic. University of Barcelona
Montreal Heart Institute
Sophie Cardin
Yanfen Shi
Patrick Lawler
Ange Maguy
Jean-Claude Tardif
Nathalie L’Heureux
Chantal St-Cyr
Audrey Bonard
Stanley Nattel
Begoña Benito
Gemma Gay
Eduard Guasch
Valeria Sirenko
David Tamborero
Anna Serrano
Lluis Mont
Benito et al. Circulation 2011
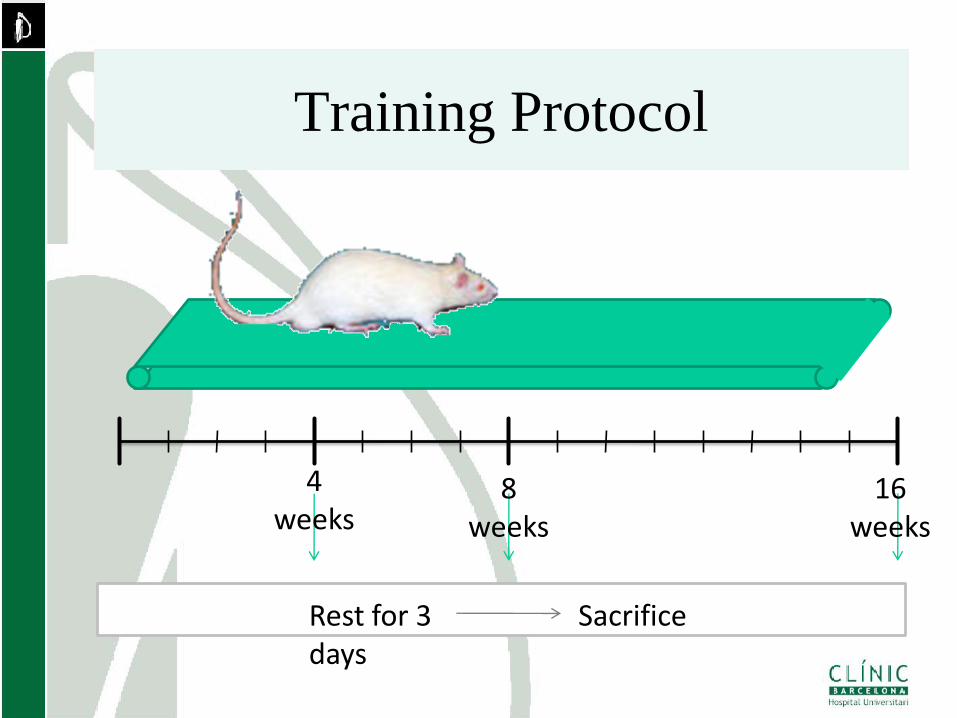
Training Protocol
4 weeks
8 weeks
16 weeks
Rest for 3 days
Sacrifice
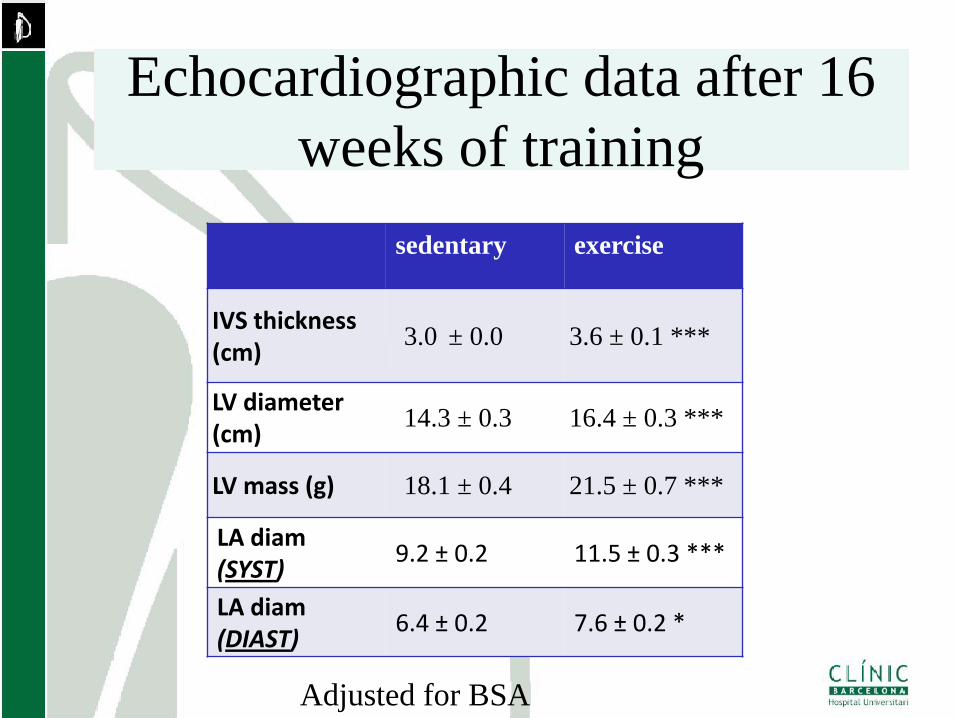
Echocardiographic data after 16
weeks of training
sedentary exercise
IVS thickness (cm)
3.0 ± 0.0 3.6 ± 0.1 ***
LV diameter (cm)
14.3 ± 0.3 16.4 ± 0.3 ***
LV mass (g) 18.1 ± 0.4 21.5 ± 0.7 ***
LA diam (SYST)
9.2 ± 0.2 11.5 ± 0.3 ***
LA diam (DIAST)
6.4 ± 0.2 7.6 ± 0.2 *
Adjusted for BSA
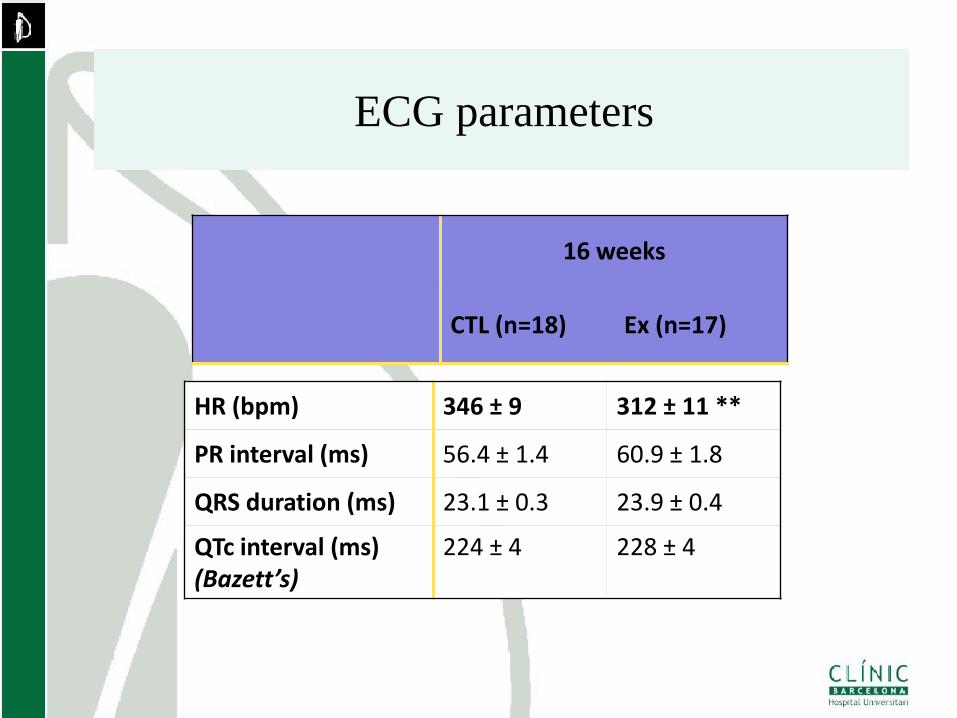
ECG parameters
16 weeks
CTL (n=18) Ex (n=17)
HR (bpm) 346 ± 9 312 ± 11 **
PR interval (ms) 56.4 ± 1.4 60.9 ± 1.8
QRS duration (ms) 23.1 ± 0.3 23.9 ± 0.4
QTc interval (ms) (Bazett’s)
224 ± 4 228 ± 4
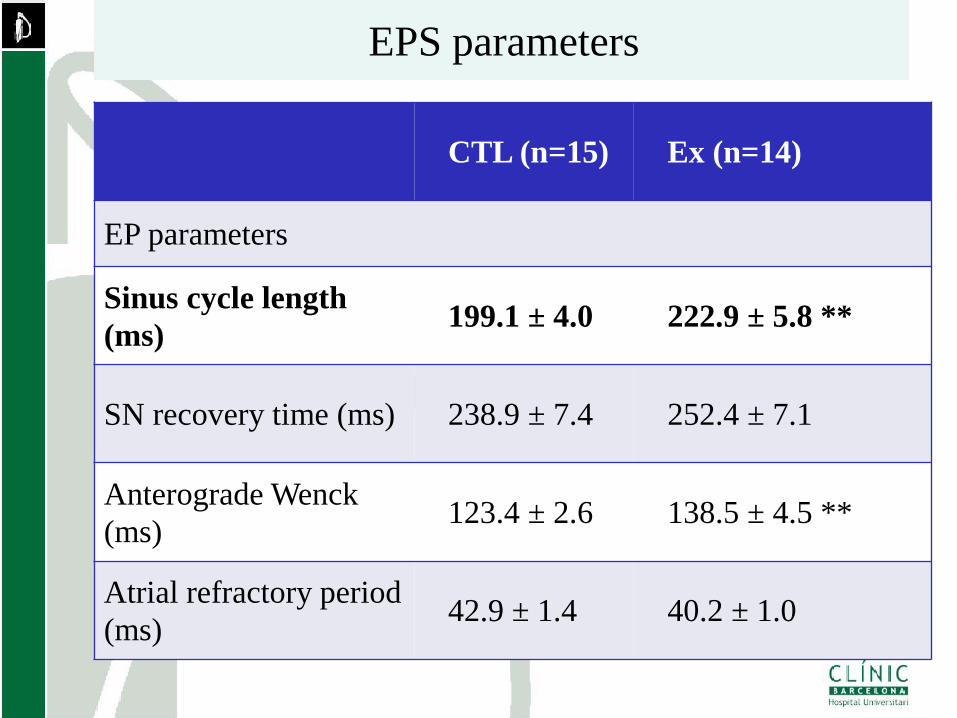
EPS parameters
CTL (n=15) Ex (n=14)
EP parameters
Sinus cycle length
(ms) 199.1 ± 4.0 222.9 ± 5.8 **
SN recovery time (ms) 238.9 ± 7.4 252.4 ± 7.1
Anterograde Wenck
(ms) 123.4 ± 2.6 138.5 ± 4.5 **
Atrial refractory period
(ms) 42.9 ± 1.4 40.2 ± 1.0
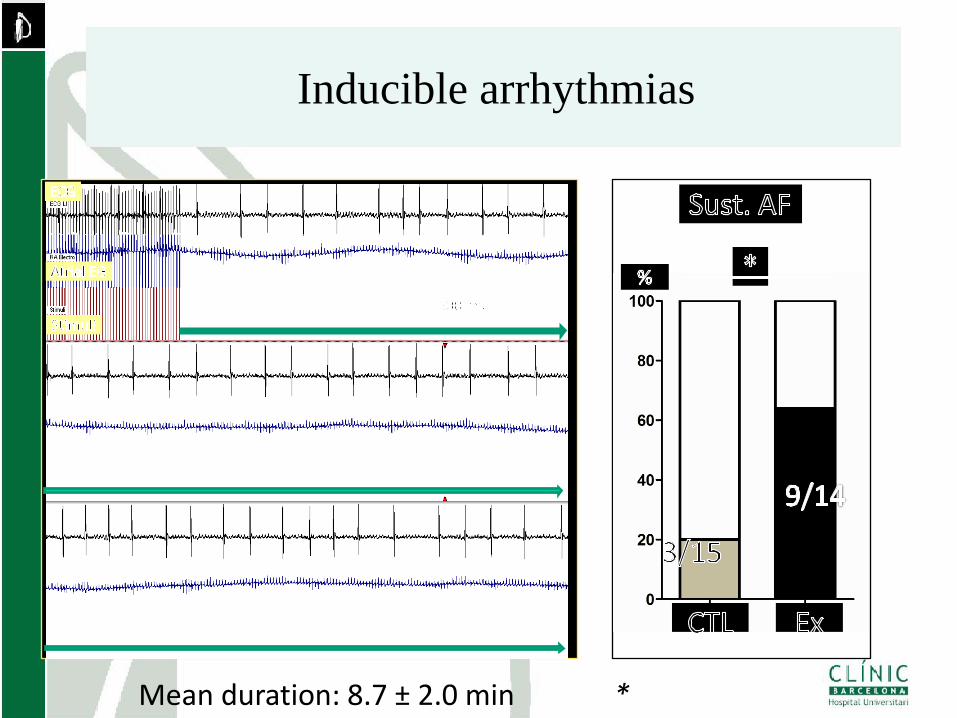
Inducible arrhythmias
* Mean duration: 8.7 ± 2.0 min
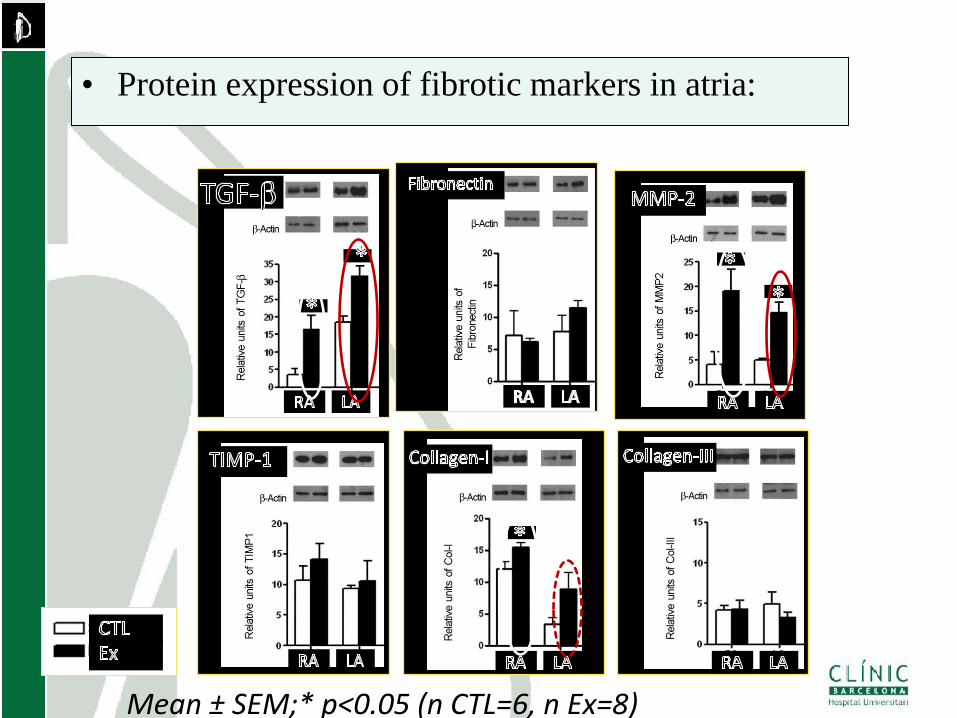
• Protein expression of fibrotic markers in atria:
Mean ± SEM;* p<0.05 (n CTL=6, n Ex=8)
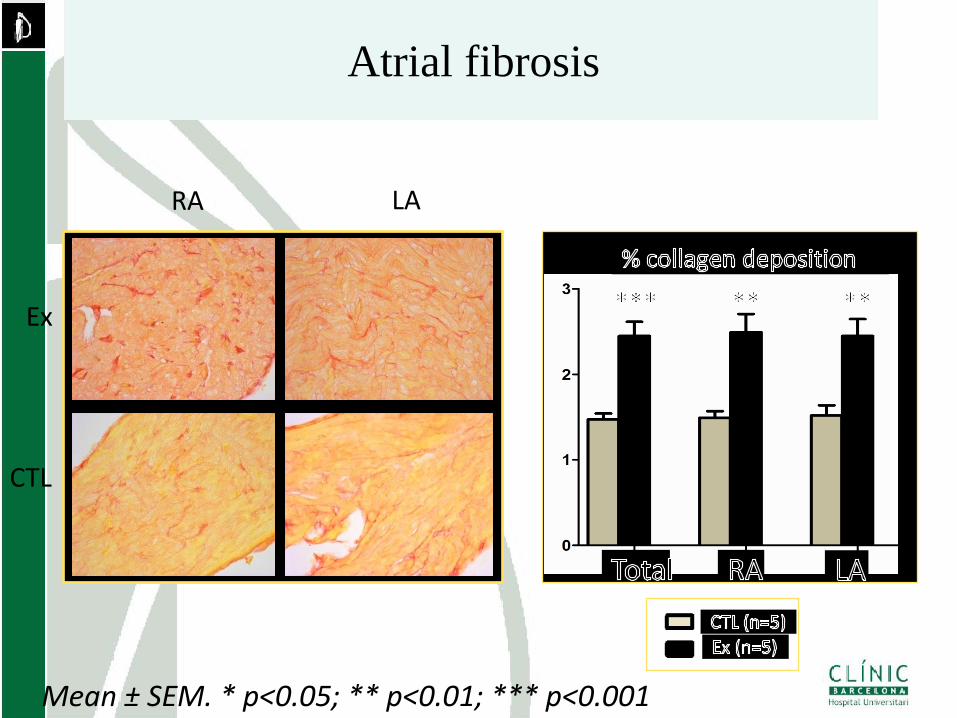
Atrial fibrosis
Ex
CTL
RA LA
Mean ± SEM. * p<0.05; ** p<0.01; *** p<0.001
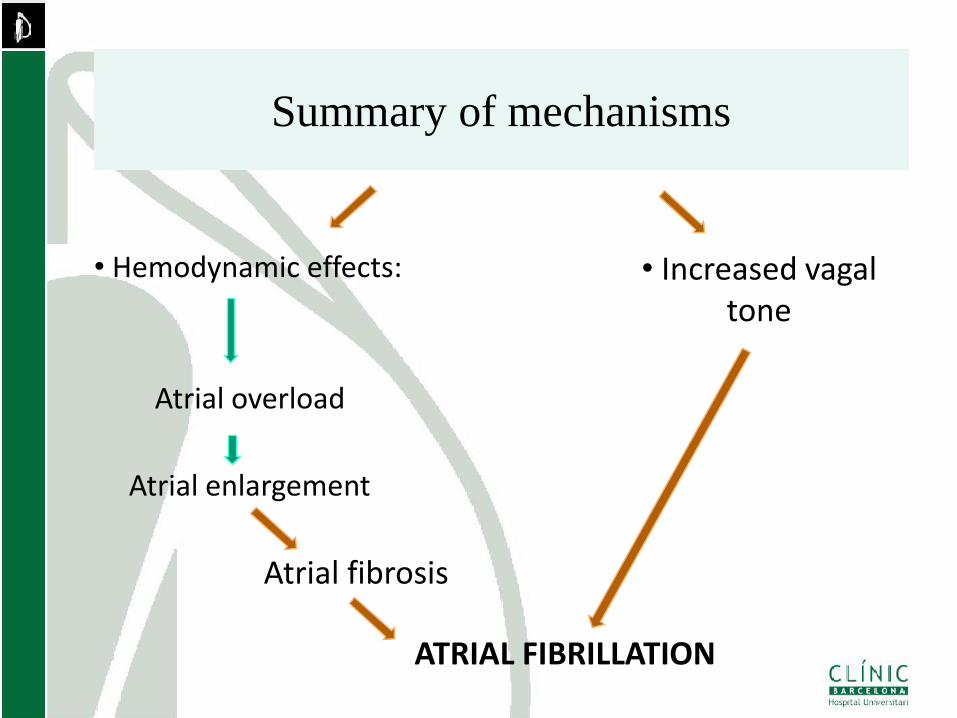
Chronic high-level exercise
• Hemodynamic effects:
Atrial overload
Atrial enlargement
Atrial fibrosis
ATRIAL FIBRILLATION
• Increased vagal tone
Summary of mechanisms
Summary
• AF related to sports seems to be the
consequence of atrial remodelling and
increased vagal tone.
• Monogenic AF seems to be a high
penetrance and not particularly linked to
sport practice
• A genetic predisposition may be present in
certain individuals.
Recommended