7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 1/76
Hypertension
management:
key recommendations
This presentation is adapted with permission from the National Heart Foundation of Australia
(National Blood Pressure and Vascular Disease Advisory Committee). Guide to management of hypertension 2008.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 2/76
Summary of presentation
1 Background
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 3/76
Summary of presentation
1 Background
2 Key recommendation
areas…
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 4/76
Summary of presentation
1 Background
2 Key recommendation
areas…
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Measurement
of blood
pressure
BP)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 5/76
Summary of presentation
1 Background
2 Key recommendation
areas…
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Measurement
of blood
pressure
BP)
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 6/76
Summary of presentation
1 Background
2 Key recommendation
areas…
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Measurement
of blood
pressure
BP)
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 7/76
Summary of presentation
1 Background
2 Key recommendation
areas…
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Absolute
risk
Measurement
of blood
pressure
BP)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 8/76
Summary of presentation
1 Background
2 Key recommendation
areas…
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Absolute
risk
When to
intervene
Measurement
of blood
pressure
BP)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 9/76
Summary of presentation
1 Background
2 Key recommendation
areas…
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Absolute
risk
When to
intervene
Lifestyle
advice
Measurement
of blood
pressure
BP)
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 10/76
Summary of presentation
1 Background
2 Key recommendation
areas…
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Absolute
risk
When to
intervene
Drug
treatment
Lifestyle
advice
Measurement
of blood
pressure
BP)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 11/76
Summary of presentation
1 Background
2 Key recommendation
areas…
3 Development
process
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Absolute
risk
When to
intervene
Drug
treatment
Lifestyle
advice
Measurement
of blood
pressure
BP)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 12/76
Summary of presentation
1 Background
2 Key recommendation
areas…
3 Development
process
4 Endorsing organisations
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Absolute
risk
When to
intervene
Drug
treatment
Lifestyle
advice
Measurement
of blood
pressure
BP)
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 13/76
Background
Hypertension is common: The most frequently managed chronic problem in general
practice1
1 in 3 Australians are diagnosed with hypertension2
Hypertension is serious: Major risk factor for stroke and coronary heart disease3
Major contributor to chronic heart failure (CHF), chronic kidneydisease and its progression3
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
1. Australian Institute of Health and Welfare, Australia’s Health 2008
2. AusDiab 2005, The Australian Diabetes, Obesity and Lifestyle Study, Tracking the Accelerating Epidemic:
Its Causes and Outcomes, Australian Diabetes Institute 2006
3. Levy D, Larson MG, Vasan RS, et al. The progression from hypertension to congestive heart failure.
JAMA 1996; 275: 1557-1562

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 14/76
Background
‘Hypertension’ is an arbitrary term Generally, the lower the BP, the lower the risk Decision to treat is based on ‘absolute risk’ or evidence of
end-organ damage – not levels of blood pressure alone.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 15/76
ckground
What’s new in the 2008 guide? Revised recommendations based on new evidence Revised treatment targets Revised recommendations for drug treatment of uncomplicated
hypertension
Revised format for quick reference guide.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 16/76
Key recommendation areas
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 17/76
Key recommendation areas
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Measurement
of blood
pressure
BP)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 18/76
Key recommendation areas
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Measurement
of blood
pressure
BP)
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 19/76
Key recommendation areas
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Measurement
of blood
pressure
BP)
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 20/76
Key recommendation areas
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Absolute
risk
Measurement
of blood
pressure
BP)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 21/76
Key recommendation areas
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Absolute
risk
When to
intervene
Measurement
of blood
pressure
BP)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 22/76
Key recommendation areas
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Absolute
risk
When to
intervene
Lifestyle
advice
Measurement
of blood
pressure
BP)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 23/76
Key recommendation areas
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Diagnosis
and
classification
Assessment
Absolute
risk
When to
intervene
Drug
treatment
Lifestyle
advice
Measurement
of blood
pressure
BP)
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 24/76
1. Measurement of BP
Use recommended technique every time Use regularly validated and serviced sphygmomanometer Measure BP on both arms on first measurement Ensure patient is seated and relaxed Measure sitting and standing if orthostatic hypotension
is suspected Use right cuff size Repeat and average two readings
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 25/76
2. Diagnosis and classification
Obtain BP measurement outside clinic if possible Ambulatory monitoring
and/or Self-measurement at home
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 26/76
2. Diagnosis and classification
Diagnosis should be based on multiple BPmeasurements taken on separate occasions
Review at intervals determined by both BP category
and absolute risk
Click to see table
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 27/76

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 28/76
3 Assessment
Why assess all patients with ‘hypertension’? Identify all CVD risk factors Calculate absolute risk (see later) Detect end-organ damage Detect co-morbid conditions
Identify causes of secondary hypertension
If secondary hypertension is suspected, consider specialist
referral.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 29/76
3. Assessment
A thorough evaluation of all patients includes: Taking a full medical history Performing a physical examination, with
particular attention to CVD system Undertaking initial investigations
Urine dip stick –for proteinuria and microalbuminuria Blood analysis ECG
Undertaking further investigations as indicated Calculating absolute cardiovascular risk
See full guide for further details
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 30/76
4. Absolute cardiovascular risk AR)
Why assess AR in all patients? To determine optimal management plan To identify other modifiable risk factors that require management To communicate degree of urgency for reducing BP to patients
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 31/76
4. Absolute cardiovascular risk AR)
What is AR? Probability (as a %) of someone
experiencing a CVD event
(heart attack or stroke) Current risk calculators underestimate
cardiovascular risk in Aboriginal,Torres Strait Islander, Maori, and
Pacific Islander peoples
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 32/76
4. Absolute cardiovascular risk AR)
Who is at ‘high’ (>15%) AR?
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 33/76
4. Absolute cardiovascular risk AR)
Who is at ‘high’ (>15%) AR?
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Group
Patients aged
75 years and older
For almost allindividuals aged
≥75 years,the absolute risk of
a cardiovascular event>15 %
in the next 5 years

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 34/76
4. Absolute cardiovascular risk AR)
Who is at ‘high’ (>15%) AR?
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Group
Patients aged
75 years and older
For almost allindividuals aged
≥75 years,the absolute risk of
a cardiovascular event>15 %
in the next 5 years
Group B
Patients with existing
cardiovascular diseaseAssume risk of
cardiovascular event>15%
in the next 5 yearsif either of the following
is present: symptomaticcardiovascular disease
or left ventricularhypertrophy

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 35/76
4. Absolute cardiovascular risk AR)
Who is at ‘high’ (>15%) AR?
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Group
Patients aged
75 years and older
For almost allindividuals aged
≥75 years,the absolute risk of
a cardiovascular event>15 %
in the next 5 years
Group B
Patients with existing
cardiovascular diseaseAssume risk of
cardiovascular event>15%
in the next 5 yearsif either of the following
is present: symptomaticcardiovascular disease
or left ventricularhypertrophy
Group C
Patients with
associated clinicalconditionsand/or
end-organ disease
(including diabetes,coronary heart disease,
chronic kidney disease – see guide)
Assume >15 %in the next 5 years

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 36/76
4. Absolute cardiovascular risk AR)
Australian cardiovascular risk chart (See full guide for information on how to use the chart)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 37/76
5. When to intervene
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 38/76
5. When to intervene
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Management
of hypertension
aims to:
Reduce BP
Reduce absolutecardiovascular risk
Minimise end-organdamage

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 39/76
5. When to intervene
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Management
of hypertension
aims to:
Reduce BP
Reduce absolutecardiovascular risk
Minimise end-organdamage
Decision to
intervene should
be based on:
A thoroughassessment(Section 3)
Absolutecardiovascular risk
Evidence ofend-organ damage

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 40/76
5. When to intervene
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Management
of hypertension
aims to:
Reduce BP
Reduce absolutecardiovascular risk
Minimise end-organdamage
Decision to
intervene should
be based on:
A thoroughassessment(Section 3)
Absolutecardiovascular risk
Evidence ofend-organ damage
Lifestyle risk
reduction is
indicated for all
patients
Especially thosewith high – normal
BP or
hypertension

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 41/76
6. Lifestyle advice
Indicated for all patients with hypertension,regardless of drug therapy: 30 minutes moderate activity on most days
of the week Smoking cessation
Healthy weight: waist <94 cm for men and<80 cm for women, BMI <25 kg/m2
Dietary salt restriction: ≤4 g/day Limited alcohol: ≤two standard drinks per day for
men or ≤one standard drink per day for women.
(See the full guide for more information
on lifestyle modification)
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 42/76
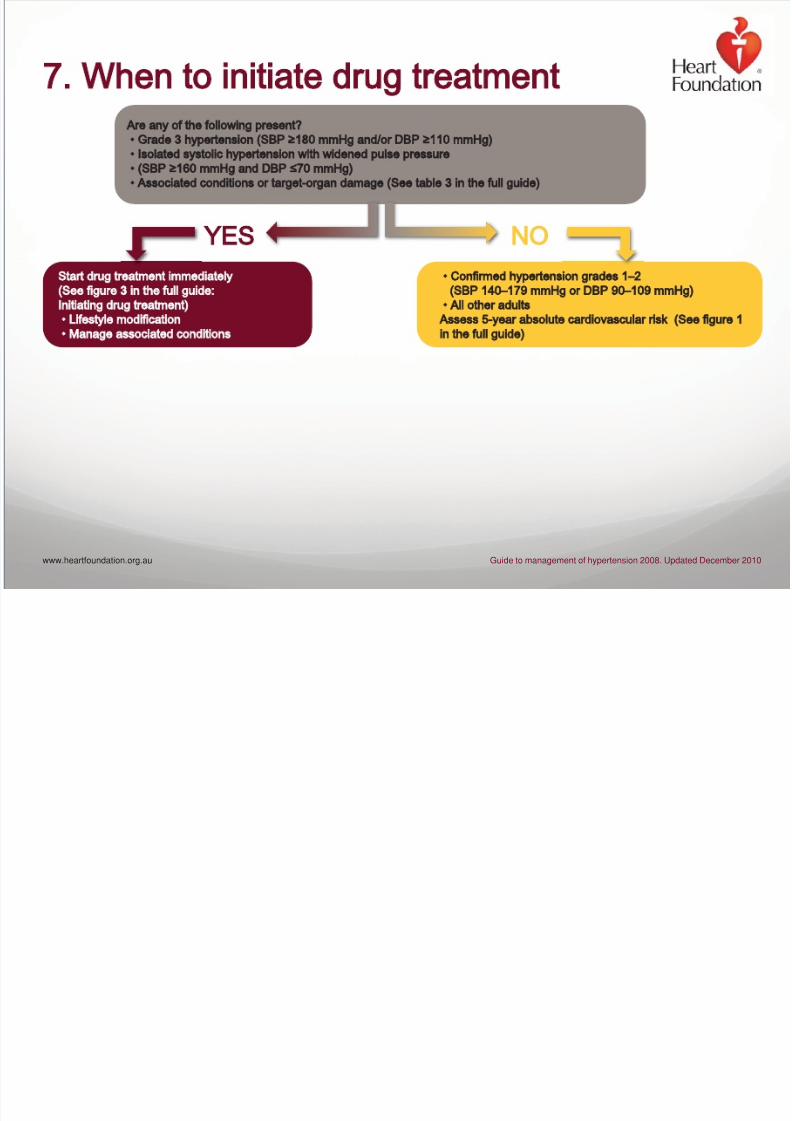
7. When to initiate drug treatment
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Are any of the following present?
• Grade 3 hypertension (SBP ≥180 mmHg and/or DBP ≥110 mmHg)
• Isolated systolic hypertension with widened pulse pressure
• (SBP ≥160 mmHg and DBP 70 mmHg)
• Associated conditions or target-organ damage (See table 3 in the full guide)
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 43/76
7. When to initiate drug treatment
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Start drug treatment immediately
(See figure 3 in the full guide:
Initiating drug treatment)
• Lifestyle modification
• Manage associated conditions
• Confirmed hypertension grades 1–2
(SBP 140–179 mmHg or DBP 90–109 mmHg)
• All other adults
Assess 5-year absolute cardiovascular risk (See figure 1
in the full guide)
Are any of the following present?
• Grade 3 hypertension (SBP ≥180 mmHg and/or DBP ≥110 mmHg)
• Isolated systolic hypertension with widened pulse pressure
• (SBP ≥160 mmHg and DBP 70 mmHg)
• Associated conditions or target-organ damage (See table 3 in the full guide)
YES NO

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 44/76
7. When to initiate drug treatment
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Start drug treatment immediately
(See figure 3 in the full guide:
Initiating drug treatment)
• Lifestyle modification
• Manage associated conditions
• Confirmed hypertension grades 1–2
(SBP 140–179 mmHg or DBP 90–109 mmHg)
• All other adults
Assess 5-year absolute cardiovascular risk (See figure 1
in the full guide)
• Lifestyle modification
• Monitor BP
Reassess 5-year absolute
cardiovascular risk in 3–6 mths
• Lifestyle modification
• Monitor BP
Reassess 5-year absolute
cardiovascular risk in 6–12 mths
Are any of the following present?
• Grade 3 hypertension (SBP ≥180 mmHg and/or DBP ≥110 mmHg)
• Isolated systolic hypertension with widened pulse pressure
• (SBP ≥160 mmHg and DBP 70 mmHg)
• Associated conditions or target-organ damage (See table 3 in the full guide)
YES
Moderate
(10–15%)
SEE NEXT SLIDE SEE NEXT SLIDE
High
(>15%)
Low
(<10%)
NO
Start drug treatment immediately
(See figure 3 in the full guide:
Initiating drug treatment)
• Lifestyle modification
• Manage associated conditions

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 45/76
7. When to initiate drug treatment
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
• Lifestyle modification
• Monitor BP
Reassess 5-year absolute
cardiovascular risk in 3–6 mths
• Lifestyle modification
• Monitor BP
Reassess 5-year absolute
cardiovascular risk in 6–12 mths
Moderate
(10–15%)
Low
(<10%)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 46/76
7. When to initiate drug treatment
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
• Lifestyle modification
• Monitor BP
Reassess 5-year absolute
cardiovascular risk in 3–6 mths
LOW <10%
SBP 140–150 mmHg
DBP <90 mmHg
Continue monitoring
• Lifestyle modification
• Monitor BP
Reassess 5-year absolute
cardiovascular risk in 6–12 mths
Moderate
(10–15%)
Low
(<10%)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 47/76
7. When to initiate drug treatment
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
• Lifestyle modification
• Monitor BP
Reassess 5-year absolute
cardiovascular risk in 3–6 mths
LOW <10%
MODERATE 10–15%
SBP <140 mmHg
DBP <90 mmHg
Continue monitoring
SBP 140–150 mmHg
DBP <90 mmHg
Continue monitoring
• Lifestyle modification
• Monitor BP
Reassess 5-year absolute
cardiovascular risk in 6–12 mths
Moderate
(10–15%)
Low
(<10%)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 48/76
7. When to initiate drug treatment
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
• Lifestyle modification
• Monitor BP
Reassess 5-year absolute
cardiovascular risk in 3–6 mths
Start drug treatment immediately
(See figure 3 in full guide:
Initiating drug treatment)
• Lifestyle modification
• Manage associated conditions
LOW <10%
MODERATE 10–15%
SBP <140 mmHg
DBP <90 mmHg
Continue monitoring
SBP ≥140 mmHg
DBP ≥90 mmHg
SBP 140–150 mmHg
DBP <90 mmHg
Continue monitoring
SBP ≥150 mmHg
DBP ≥90 mmHg
• Lifestyle modification
• Monitor BP
Reassess 5-year absolute
cardiovascular risk in 6–12 mths
Moderate
(10–15%)
Low
(<10%)

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 49/76
7. Drug treatments
The benefit from drug treatments is mainly due to BPlowering (not mechanism of action)
In uncomplicated hypertension, these are equally effective
as first-line treatment (see figure 3 in full guide): ACE inhibitor (or angiotensin II receptor antagonist) Calcium channel blocker Low-dose thiazide diuretics
(for people aged 65 years and older)
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 50/76
7. Drug treatments
* ACE inhibitors and angiotensin II
receptor antagonists have been
shown to be equally efficacious in
prevention of cardiovascular end
points, and in lowering BP.
† Thiazide diuretics are not
recommended for younger patients
due to risk of diabetes associated
with long-term use.
See table 7 in full guide for
information regarding choice of
antihypertensive agent in patients
with comorbid and associated
conditions.
See page 25 in full guide for
information on combination therapy.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
FIRST CHOICE
ACE inhibitor (or angiotensin ll receptor antagonist)*
or

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 51/76
7. Drug treatments
* ACE inhibitors and angiotensin II
receptor antagonists have been
shown to be equally efficacious in
prevention of cardiovascular end
points, and in lowering BP.
† Thiazide diuretics are not
recommended for younger patients
due to risk of diabetes associated
with long-term use.
See table 7 in full guide for
information regarding choice of
antihypertensive agent in patients
with comorbid and associated
conditions.
See page 25 in full guide for
information on combination therapy.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
FIRST CHOICE
ACE inhibitor (or angiotensin ll receptor antagonist)*
or
Calcium channel blocker
or

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 52/76
7. Drug treatments
* ACE inhibitors and angiotensin II
receptor antagonists have been
shown to be equally efficacious in
prevention of cardiovascular end
points, and in lowering BP.
† Thiazide diuretics are not
recommended for younger patients
due to risk of diabetes associated
with long-term use.
See table 7 in full guide for
information regarding choice of
antihypertensive agent in patients
with comorbid and associated
conditions.
See page 25 in full guide for
information on combination therapy.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
FIRST CHOICE
ACE inhibitor (or angiotensin ll receptor antagonist)*
or
Calcium channel blocker
or
Low-dose thiazide diuretic (consider for people aged ≥65 years only)†
or

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 53/76
7. Drug treatments
* ACE inhibitors and angiotensin II
receptor antagonists have been
shown to be equally efficacious in
prevention of cardiovascular end
points, and in lowering BP.
† Thiazide diuretics are not
recommended for younger patients
due to risk of diabetes associated
with long-term use.
See table 7 in full guide for
information regarding choice of
antihypertensive agent in patients
with comorbid and associated
conditions.
See page 25 in full guide for
information on combination therapy.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
FIRST CHOICE
If target BP not reached
ACE inhibitor (or angiotensin ll receptor antagonist)*
or
Calcium channel blocker
or
Low-dose thiazide diuretic (consider for people aged ≥65 years only)†
or
ACE inhibitor (or angiotensin ll receptor antagonist)* + calcium channel blocker
or

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 54/76
7. Drug treatments
* ACE inhibitors and angiotensin II
receptor antagonists have been
shown to be equally efficacious in
prevention of cardiovascular end
points, and in lowering BP.
† Thiazide diuretics are not
recommended for younger patients
due to risk of diabetes associated
with long-term use.
See table 7 in full guide for
information regarding choice of
antihypertensive agent in patients
with comorbid and associated
conditions.
See page 25 in full guide for
information on combination therapy.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
FIRST CHOICE
If target BP not reached
ACE inhibitor (or angiotensin ll receptor antagonist)*
or
Calcium channel blocker
or
Low-dose thiazide diuretic (consider for people aged ≥65 years only)†
or
ACE inhibitor (or angiotensin ll receptor antagonist)* + calcium channel blocker
or
ACE inhibitor (or angiotensin ll receptor antagonist)* + low-dose thiazide diuretic
or

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 55/76
7. Drug treatments
* ACE inhibitors and angiotensin II
receptor antagonists have been
shown to be equally efficacious in
prevention of cardiovascular end
points, and in lowering BP.
† Thiazide diuretics are not
recommended for younger patients
due to risk of diabetes associated
with long-term use.
See table 7 in full guide for
information regarding choice of
antihypertensive agent in patients
with comorbid and associated
conditions.
See page 25 in full guide for
information on combination therapy.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
FIRST CHOICE
If target BP not reached
If target BP not reached
ACE inhibitor (or angiotensin ll receptor antagonist)*
or
Calcium channel blocker
or
Low-dose thiazide diuretic (consider for people aged ≥65 years only)†
or
ACE inhibitor (or angiotensin ll receptor antagonist)* + calcium channel blocker
or
ACE inhibitor (or angiotensin ll receptor antagonist)* + low-dose thiazide diuretic
or
ACE inhibitor (or angiotensin ll receptor antagonist)*+ calcium channel blocker + low-dose thiazide diuretic

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 56/76
7. Drug treatments
* ACE inhibitors and angiotensin II
receptor antagonists have been
shown to be equally efficacious in
prevention of cardiovascular end
points, and in lowering BP.
† Thiazide diuretics are not
recommended for younger patients
due to risk of diabetes associated
with long-term use.
See table 7 in full guide for
information regarding choice of
antihypertensive agent in patients
with comorbid and associated
conditions.
See page 25 in full guide for
information on combination therapy.
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
FIRST CHOICE
If target BP not reached
If target BP not reached
If target BP not reached
Consider seeking specialist advice
ACE inhibitor (or angiotensin ll receptor antagonist)*
or
Calcium channel blocker
or
Low-dose thiazide diuretic (consider for people aged ≥65 years only)†
or
ACE inhibitor (or angiotensin ll receptor antagonist)* + calcium channel blocker
or
ACE inhibitor (or angiotensin ll receptor antagonist)* + low-dose thiazide diuretic
or
ACE inhibitor (or angiotensin ll receptor antagonist)*+ calcium channel blocker + low-dose thiazide diuretic

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 57/76
7. Drug treatments
Treat to recommended target level
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
Patient group Target mmHg)
People with proteinuria >1 g/day
(with or without diabetes)<125 / 75

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 58/76
7. Drug treatments
Treat to recommended target level
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
* Specific lower BP targets have not
been established for other high-risk
groups (e.g. those with peripheral
arterial disease, those with familial
hypercholesterolaemia or those at
high risk of cardiovascular disease)
due to the current lack of evidence
from clinical trials. Targets will be set
when evidence becomes available.
Patient group Target mmHg)
People with associated condition/s or
end-organ damage:*
• Coronary heart disease
• Diabetes
• Chronic kidney disease
• Proteinuria (>300 mg/day)
• Stroke / TIA
People with proteinuria >1 g/day
(with or without diabetes)<125 / 75
<130 / 80

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 59/76
7. Drug treatments
Treat to recommended target level
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
* Specific lower BP targets have not
been established for other high-risk
groups (e.g. those with peripheral
arterial disease, those with familial
hypercholesterolaemia or those at
high risk of cardiovascular disease)
due to the current lack of evidence
from clinical trials. Targets will be set
when evidence becomes available.
Patient group Target mmHg)
People with associated condition/s or
end-organ damage:*
• Coronary heart disease
• Diabetes
• Chronic kidney disease
• Proteinuria (>300 mg/day)
• Stroke / TIA
People with none of the following:
• Coronary heart disease
• Diabetes
• Chronic kidney disease
• Proteinuria (>300 mg/day)
• Stroke / TIA
People with proteinuria >1 g/day
(with or without diabetes)<125 / 75
<140 / 90
or lower
if tolerated
<130 / 80
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 60/76
7 Drug treatments
How to achieve target BP: Start with lowest dose of first drug If drug not tolerated, change to a different class If target BP not reached, add second low-dose drug
(different class) If target BP still not achieved and both drugs well tolerated,
increase doses Trial each dose regimen for at least 6 weeks
If necessary, use drugs from different classes in
combination to achieve target BP. See full guide for details of combination therapy About 50–75% of patients will not achieve BP targets with
monotherapy
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 61/76
7. Drug treatments
If BP remains elevated despite maximal doses of at leasttwo appropriate agents, reassess for: Non-adherence Undiagnosed secondary hypertension Hypertensive effects of other drugs
Treatment resistance due to sleep apnoea Undisclosed use of alcohol or recreational drugs Unrecognised high salt intake ‘White coat’ hypertension Technical factors affecting measurement Volume overload, especially with chronic kidney disease (CKD)
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 62/76
7. Drug treatments
Most effective combination:
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
PLUS
ACE inhibitor
or Angiotensin ll
receptor antagonist
Calcium channel
blocker
Particular role in the
presence of d iabetes or lipid
abnormalities

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 63/76
7. Drug treatments
Other effective combinations include:
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
PLUS
ACE inhibitor
or Angiotensin ll
receptor antagonist
Thiazide diuretic
Particular role in the presence
of heart failure or post stroke
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 64/76
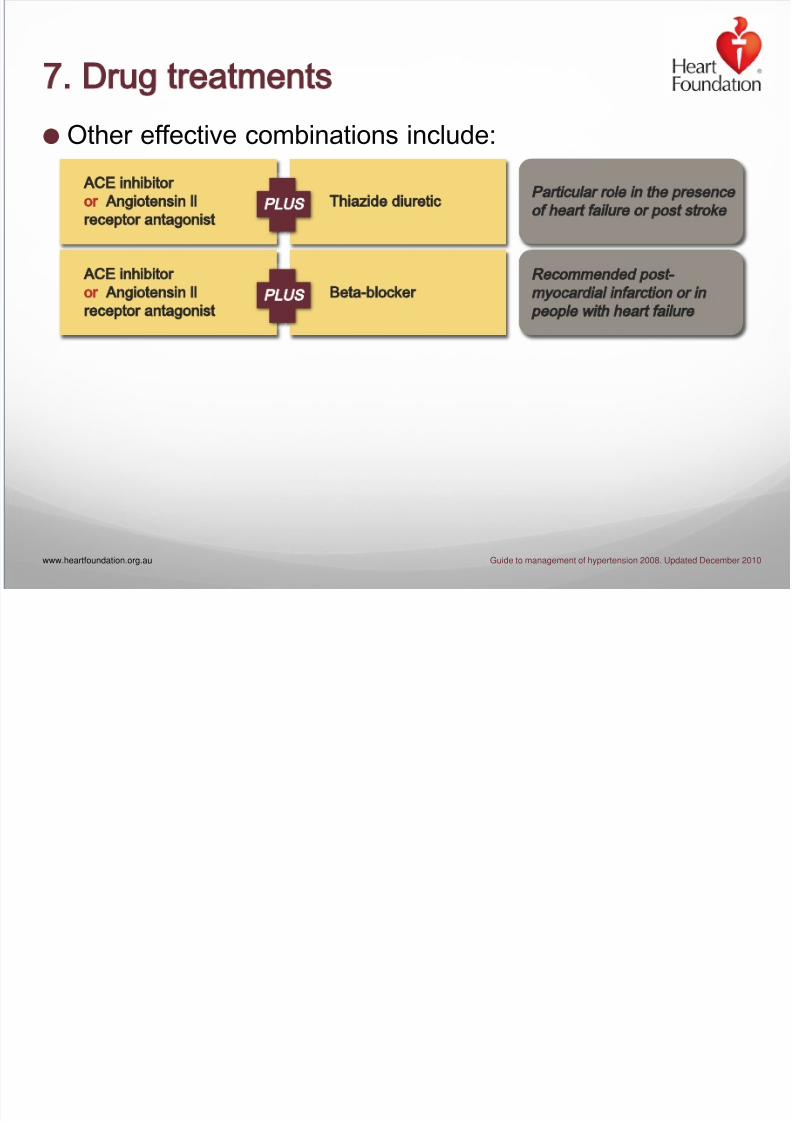
7. Drug treatments
Other effective combinations include:
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
PLUS
PLUS
ACE inhibitor
or Angiotensin ll
receptor antagonist
ACE inhibitor
or Angiotensin ll
receptor antagonist
Thiazide diuretic
Particular role in the presence
of heart failure or post stroke
Recommended post-
myocardial infarction or in
people with heart failure
Beta-blocker

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 65/76
7. Drug treatments
Other effective combinations include:
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
PLUS
PLUS
PLUS
ACE inhibitor
or Angiotensin ll
receptor antagonist
ACE inhibitor
or Angiotensin ll
receptor antagonist
Beta-blocker
Thiazide diuretic
Particular role in the presence
of heart failure or post stroke
Recommended post-
myocardial infarction or in
people with heart failure
Particular role in the presence
of coronary heart disease
Beta-blocker
Dihydropyridine calcium
channel blocker

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 66/76
7. Drug treatments
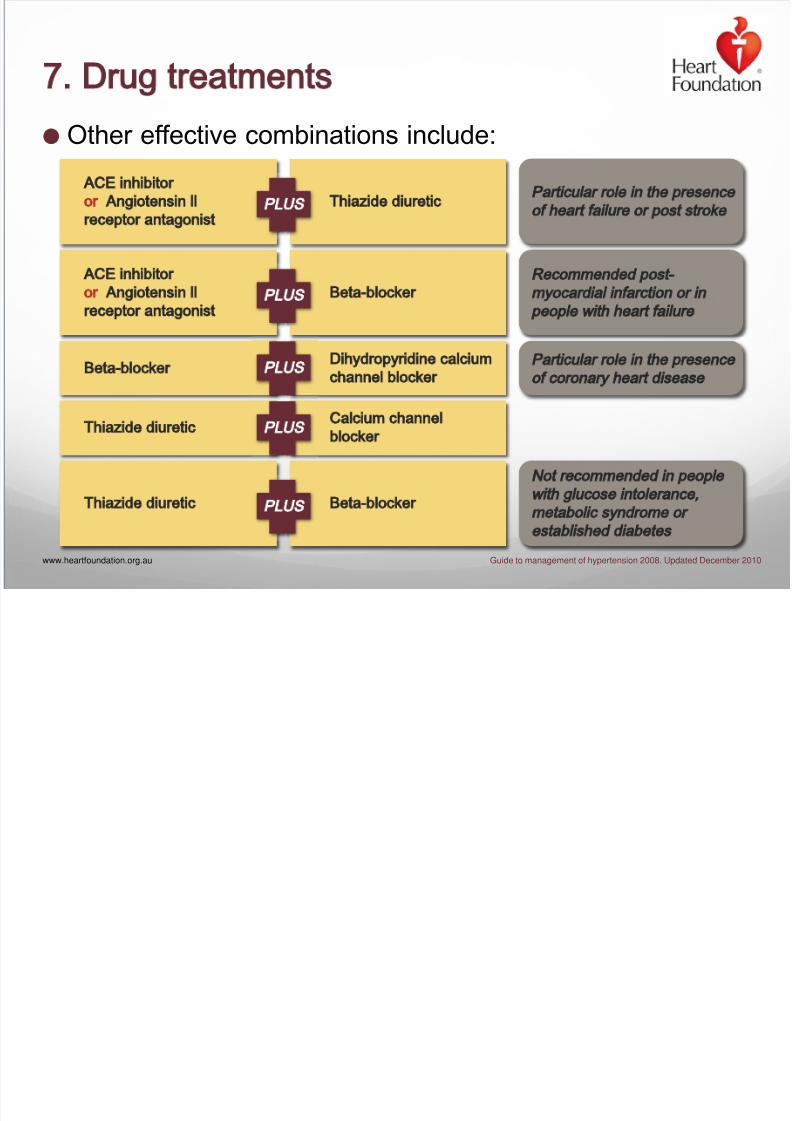
Other effective combinations include:
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
PLUS
PLUS
PLUS
PLUS
ACE inhibitor
or Angiotensin ll
receptor antagonist
ACE inhibitor
or Angiotensin ll
receptor antagonist
Beta-blocker
Thiazide diuretic
Thiazide diuretic
Particular role in the presence
of heart failure or post stroke
Recommended post-
myocardial infarction or in
people with heart failure
Particular role in the presence
of coronary heart disease
Beta-blocker
Dihydropyridine calcium
channel blocker
Calcium channel
blocker
7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 67/76
7. Drug treatments
Other effective combinations include:
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
PLUS
PLUS
PLUS
PLUS
PLUS
ACE inhibitor
or Angiotensin ll
receptor antagonist
ACE inhibitor
or Angiotensin ll
receptor antagonist
Beta-blocker
Thiazide diuretic
Thiazide diuretic
Thiazide diuretic
Particular role in the presence
of heart failure or post stroke
Recommended post-
myocardial infarction or in
people with heart failure
Not recommended in people
with glucose intolerance
metabolic syndrome or
established diabetes
Particular role in the presence
of coronary heart disease
Beta-blocker
Dihydropyridine calcium
channel blocker
Calcium channel
blocker
Beta-blocker

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 68/76
7. Drug treatments
Avoid the following combinations:
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
PLUS
Due to risk of hyperkalaemia
ACE inhibitor
or Angiotensin ll
receptor antagonist
Potassium-sparing
diuretic

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 69/76
7. Drug treatments
Avoid the following combinations:
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
PLUS
PLUS
Due to risk of hyperkalaemia
Due to risk of heart block
ACE inhibitor
or Angiotensin ll
receptor antagonist
Verapamil Beta-blocker
Potassium-sparing
diuretic

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 70/76
7. Drug treatments
Avoid the following combinations:
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010
PLUS
PLUS
Due to risk of hyperkalaemia
Due to risk of heart block
ACE inhibitor
or Angiotensin ll
receptor antagonist
Verapamil Beta blocker
PLUS
In a large trial comb ination therapy
did not reduce cardiovascular death
or morbidity in patients with vascular
disease or diabetes but increased
the risk of hypotensive symptoms
syncope and renal dysfunction
ACE inhibitor
Angiotensin ll
receptor antagonist
Potassium sparing
diuretic

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 71/76
7 Drug treatments
Once a combination regimen is established as long-term
therapy, a fixed combination preparation may be more
convenient
Co-morbidities may either favour or limit the use of
particular drug classes See table 7 in full guide for further details
Strategies to maximise adherence to treatment
recommendations should be used See table 8 in full guide for further details
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 72/76
Hypertension quick reference
guide 2008
Designed as a practical tool for
use in general practice
The quick reference guide is
a summarised version of the
full guide including key
recommendations and
treatment tables and
algorithms
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 73/76
Guide development process
Developed by the National Blood Pressure and Vascular
Disease Advisory Committee of the Heart Foundation Literature review conducted by experts on the Committee to
identify new evidence since 2004 Recommendations were derived from the evidence and/or
consensus of the Committee Draft guide sent to endorsing organisations and key
stakeholders for comment (including a small
group of Victorian GPs in a focus group)
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 74/76
Take home messages
1 Management is determined by assessment of
‘absolute risk’ and evidence of end-organ damage
2 Treat to ‘target’ blood pressure
3 Lifestyle modification is indicated for all
4 New recommendations for uncomplicated hypertension: Begin drug monotherapy with any of:
ACE inhibitor (or angiotensin II receptor antagonist) Calcium channel blockers Thiazide diuretics (consider for people aged 65 years or older only)
www.heartfoundation.org.au Guide to management of hypertension 2008. Updated December 2010

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 75/76

7/18/2019 Hypertension
http://slidepdf.com/reader/full/hypertension-56d5009c1e365 76/76
ow to get copies of the guide
The full guide, the quick reference guide and related
resources can be accessed online at
www.heartfoundation.org.au/information-for-
professionals/Clinical-Information/Pages/hypertension.aspx
Alternatively contact the Heart Foundation’s HealthInformation Service on 1300 36 27 87 or
Recommended