Hypersensitivity
Josyann Abisaab, MD
Department of Emergency Medicine
New York Presbyterian Hospital-
Weill Cornell Medical Center

Outline
• Types of Hypersensitivity
• Anaphylaxis
• Disposition
• Prevention

Definition of Hypersensitivity
• Undesirable reactions produced by the normal immune system.

Classification of Hypersensitivity
• Type I: Immediate/Anaphylactic
• Type II: Cytotoxic Antibody Reaction
• Type III: Immune Complex Reaction
• Type IV: Delayed-Type Hypersensitivity
• Type V: Stimulatory Hypersensitivity

Type I- Immediate hypersensitivity
• Provoked by reexposure to a specific antigen.
• IgE mediated• Mast cells and Basophils
stimulation• Release of Histamine and
other chemicals• Vasodilation, mucous
secretion, bronchospasm

Type I- Immediate
• Acute response within 1 hour
• Late-phase response 4-6 hours after original reaction, can last 1-2 days
• Local vs. systemic

Type I- Immediate
• Urticaria (hives)
• Angioedema
• Allergic conjunctivitis
• Allergic Rhinitis
• Allergic Asthma
• Anaphylaxis

Type II- Cytotoxic Antibody Reaction
• Antigen is on the patient’s own cell surfaces
• Mediated by IgG and IgM
• Complement activation
• Cell lysis and death• Reaction takes hours
to a day

Type II- Cytotoxic
• Transfusion reactions• Rh incompatibility• Autoimmune hemolytic anemia• Goodpasture’s syndrome• Pemphigus• ITP
• Rx: anti-inflammatory + immunosuppressive agents

Type III- Immune Complex Hypersensitivity
• Antigen-antibody complexes deposit in tissue
• Antigen is soluble- not attached to organ involved
• Classical pathway of complement activation
• Takes hours to days to develop

Type III- Immune Complex
• Serum sickness• SLE• Rheumatoid arthritis• Erythema nodosum• Arthus reaction (Farmer’s Lung)• Immune complex glomerulonephritis
• Rx: anti-inflammatory agents

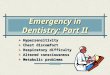
Type IV- Delayed-Type Hypersensitivity
• Mediated by T-Lymphocytes• Takes 2-3 days• Contact dermatitis (poison
ivy, nickel)• PPD• Transplant rejection (GVHD)• Rx: corticosteroids + other
immunosuppressive agents

Contact Dermatitis

Delayed Hypersensitivity Reactions
Type Reaction
time
Clinical
Appearance
Site Antigen
Contact 48-72 hr Eczema Epidermal Poison ivy, heavy metals
PPD 48-72 hr Local induration Intradermal Tuberculin
Granuloma 21-28 days Hardening Foreign body presence
TB, leprosy

Type V- Stimulatory Hypersensitivity
• IgG stimulate their target– Graves Disease– Myasthenia Gravis
• Ligand induced apoptosis– Stevens Johnson Syndrome/Toxic Epidermal
Necrolysis (TENS)

Type V- Stimulatory
Stevens Johnson Syndrome
TENS

Anaphylaxis
Case Presentation:
39 y.o male BIBA in respiratory distress with agonal pulse. Paramedics report patient was helping a friend paint when he was stung by a bee. He walked into the house, saying:”I don’t feel good” and collapsed.Intubated at scene, en route given endotracheal and IV Epi, IV Benadryl

Anaphylaxis
Case Presentation:
On arrival in ED, patient intubated, cyanotic from neck up, CPR in progress2nd Large bore IV, wide open fluidsDopamine dripEpnephrine dripCentral lineIsuprel drip, Levophed dripMonitor: agonal wide-complex

Anaphylaxis
Case presentation:
• TVP failed to capture
• After 20 min prehospital and 30 min hospital resuscitation, no response.
• Patient died.
• Cause: “Fatal Anaphylactic Reaction”

What is Anaphylaxis?
“A systemic reaction of multiple organ systems to an antigen-induced IgE-mediated immunologic mediator release in a previously sensitized individual”

What does the word mean?
• “ana” means against or backwards
• “phylaxis” means guard or protect
• Anaphylaxis= “without protection”
• Prophylaxis= “for protection”

What is Anaphylactoid?
• A nonimmunologic reaction
• Not mediated by IgE
• Direct histamine release
• Same manifestations & treatment as anaphylaxis
• Causes: RCM, opiates, ACEI, exercise, blood products, gammaglobulin, NSAIDs, ASA

Anaphylaxis: How does it manifest?
• Clinical severity varies from mild to fatal
• Majority of reactions are respiratory and dermatologic
• Innocent early findings may progress to lethal over a short time

What causes the deaths?
• Laryngeal edema and acute bronchospasm >70%
• Circulatory collapse >25%
• other <5% - ?brain ?MI

In USA
• 30,000 emergency room visits each year
• 400 to 800 deaths/year
• IV penicillin accounts for 100 to 500 deaths per year
• Hymenoptera stings account for 40 to 100 deaths per year
• Risk factors: protracted course, betablockers, adrenal insufficiency

Histamine
• Prime mediator of both local and systemic effects
• H1: smooth muscle contraction, vascular permeablility
• H2: gastric acid secretion, release of more histamine, vascular permeability
• H3: inhibition of central and peripheral neurotransmitter release, inhibition of further histamine

Clinical expression depends on:
• Degree of hypersensitivity
• Quantity, route, rate of antigen exposure
• Pattern of mediator release
• Target organ sensitivity and responsiveness

Timing
• Uniphasic• Biphasic• Protracted• Laryngeal edema
more common in biphasic (40%) or protracted (57%) cases

Usual culprits

Clinical manifestations
• Skin: urticaria and angioedema
• Respiratory: cough, dyspnea, wheezing, hoarseness

Clinical manifestations
• Lightheadedness or syncope
• Nasal congestion and sneezing
• Ocular itching and tearing
• Cramping abdominal pain with N/V/D
• Headache
• Sense of impending doom
• ↓ level of consciousness

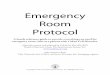
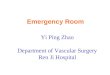
Examination
Urticaria

Examination
Angioedema

Examination
Angioedema of
oropharynx

Examination
• Conjunctivitis, rhinitis
• Tachypnea, tachycardia, hypotension
• Laryngeal stridor, hoarseness
• Wheezing, ronchi, diminished air flow

Optimal Management
• High index of suspicion
• Early diagnosis
• Pharmaceutical intervention
• Observation
• Disposition

Index of suspicion
• The motto of Emergency Medicine:
– TREAT FIRST
– ASK QUESTIONS LATER

Treating mild anaphylaxis
• Urticaria, rhinitis, conjunctivitis, mild bronchospasm
• Epinephrine 1:1000 – 0.3cc IM may repeat every 5-20min prn– 0.01mg per kg in children
• Benadryl 50 mg po or IM
• Consider: H2-blocker, prednisone, inhaled beta-agonists

Steroids
• Benefit 6-12 hrs after administration
• May prevent biphasic or protracted reaction

Myth: Epi is dangerous
Reality:• Risks of anaphylaxis far outweigh risks of
Epi administration
• Minimal cardiovascular effects in children (Simons et al, 1998)
• Caution in: elderly, known cardiac disease and tachyarrythmias

Treating moderate anaphylaxis
• Angioedema or hypotension with BP>80mmHg
• Epinephrine 1:1000- 0.3 cc IM
• Benadryl 50mg IM or IV
• Pepcid IV
• Solumedrol 40-125mg IV
• Oxygen, IVF, cardiac monitor

Treating severe anaphylaxis
• Laryngeal edema, respiratory failure, shock
• Epinephrine 1:10,000- 1cc IV over 5 min, repeat every 3-5 min prn
• Benadryl 50-100mg IV over 3 min
• H2 blockers
• Solumedrol
• Nebulizers: racemic epi, albuterol

Laryngeal edema
• Chin lift, jaw thrust
• Naso-or oropharyngeal airway
• Racemic epi 0.5 cc neb
• Heliox (Boorstein et al, AEM, 1989)
• Tracheal intubation prn
• Surgical airway prn

Persistent bronchospasm
• Albuterol by continuous nebulization
• Aminophylline 5.6 mg/kg IV over 20-30 min
• Atrovent by nebulization
• Heliox
• Steroids
• Intubation

Persistent hypotension
• Trendelenberg
• 2 largebore IV’s infusing crystalloid
• Monitor urine output and CVP
• PASG
• Consider: Naloxone 0.4-0.8mg IV
• Vasopressors: dopamine, isoproterenol, levophed

What about Glucagon?
• When epi contraindicated, may be an option
• Positive inotropic and chronotropic cardiac effects
• Consider in patients:– On beta blockers– With known CAD– Pregnant women– No response to other drugs

Disposition
• Systemic features: observe for 6-8 hours• Cannot predict biphasic reaction• Admission mandatory for:
– Moderate to severe reaction, even if they respond rapidly to Rx
• Consider admission for:– Elderly– CAD– Asthma– On beta blocker

May be discharged home if
• Mild anaphylaxis
• No hypotension
• No signs of airway obstruction
• Rapid response to ED therapy
• Observed for 6 hours without recurrence
• Safe discharge to care of responsible adult

Outpatient management
• 4 day course of Benadryl Q6h
• 4 day course of Pepcid BID
• 4 day course of Prednisone 50mg/day
(Ellis et al, CMAJ, 2003)
• Referral to an Allergist

Prevention
• Avoid the food• Aerosol spray containing Epi-Primatene or
Medihaler-Epi• Epi-Pen• Medic Alert bracelet

Board Type Questions
• A 27 year old man presents after a syncopal event following a long run. He c/o lightheadedness and itching, along with swelling of his hands and feet. His BP is 68/36 mmHg and pulse is 160. Lung examination shows he has diffuse wheezing. His blood glucose is 95 mg/dl. The most important initial IV therapy would be:
a. Epinephrineb. Diphenhydraminec. Methylprednisoloned. Normal Salinee. Pepcid

Board Type Questions
Type I Hypersensitivity:a. occurs 24 hours after the initial stimulus
b. is produced by IgE antibodies
c. is cell mediated
d. is best treated with steroids
e. is diagnosed by measuring serum histamine levels

Board Type Questions
• A 45 year old man with no PMH was playing golf when he complained of a sting on his hand, followed by shortness of breath and loss of consciousness. EMS at scene report a BP 70/40, HR 140 and bilateral wheezing. The most likely diagnosis is:
a. Vasovagal syncopeb. Asthmac. Psychogenic syncope related to bad golfing dayd. Anaphylactic shocke. Myocardial Infarction

Board Type Questions• A 19-year-old woman with a past history of seasonal allergic rhinitis
is referred to the ED from her family doctor’s office. She had received her routine injection of allergen immunotherapy (ragweed). Twenty minutes later, she began to notice itching in the palms of her hands, followed by shortness of breath and a sensation of throat swelling. In the ED, patient is noted to be flushed, sweating and in moderate distress. Her BP is 110/60 and her HR is 120. She is speaking in full sentences. The most appropriate initial emergency treatment would be:
a. Epinephrine 1:10,000- 1cc IVb. Racemic Epi 0.5 cc nebc. Epinephrine 1:1000- 0.3 cc IMd. Albuterol nebe. Benadryl 50mg po

Board Type Questions• A 40 year old woman presents to the ED 30 minutes after eating
chicken with cashews at a chinese restaurant. Patient complains of hives, itchy eyes, throat tightness as well as mild shortness of breath. The astute ED intern makes the diagnosis of urticaria and mild anaphylaxis. She administers IM Epi and Benadryl with immediate resolution of symptoms. Patient now feels well and wants to go home.
a. You agree with patient and write discharge orderb. You give her steroids first then discharge herc. You recommend observation in the ED for at least 6 hoursd. You recommend discharge home under the care of an adult after 2
hourse. You recommend admission to the hospital

Any questions?
Recommended