Muscles and Muscle TissueChapter 9
http://graphics8.nytimes.com/images/2012/05/09/health/09Physed/09Physed-tmagArticle.jpg
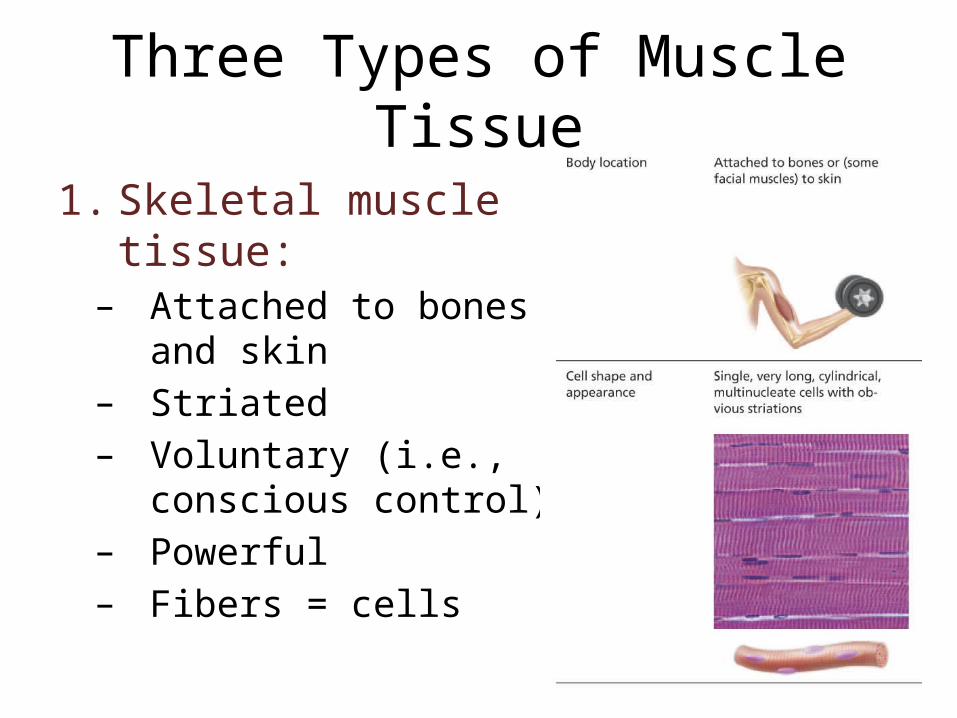
Three Types of Muscle Tissue
1. Skeletal muscle tissue:– Attached to bones and
skin– Striated – Voluntary (i.e., conscious
control)– Powerful– Fibers = cells

Three Types of Muscle Tissue
2. Cardiac muscle tissue:– Only in the heart – Striated – Involuntary– Branched cells– Intercalated disks

Three Types of Muscle Tissue
3. Smooth muscle tissue:– In the walls of hollow
organs (e.g., stomach, urinary bladder, and airways)
– Not striated– Involuntary– Fibers = cells
Special Characteristics of Muscle Tissue
1. Excitability (responsiveness or irritability): ability to receive and respond to stimuli
2. Contractility: ability to shorten when stimulated3. Extensibility: ability to be stretched 4. Elasticity: ability to recoil to resting length
Muscle Functions
1. Movement of bones or fluids (e.g., blood)2. Maintaining posture and body position 3. Stabilizing joints4. Heat generation (especially skeletal muscle)

Skeletal Muscle• Each muscle is served by one artery, one
nerve, and one or more veins– Enter near center, branch extensively through
connective tissue sheaths– Each muscle fiber has a nerve ending
• Connective Tissue sheaths– Epimysium– Perimysium – Endomysium
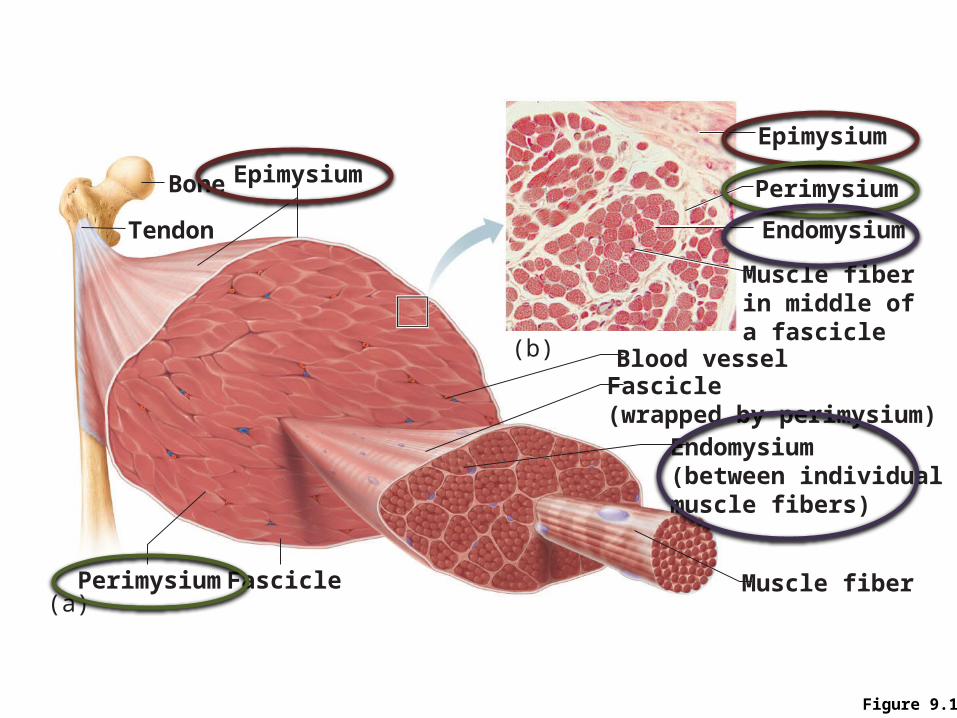
Figure 9.1
Bone
Perimysium
Endomysium(between individualmuscle fibers)
Muscle fiber
Fascicle(wrapped by perimysium)
Epimysium
Tendon
Epimysium
Muscle fiberin middle ofa fascicle
Blood vessel
Perimysium
Endomysium
Fascicle(a)
(b)
Skeletal Muscle: Attachments
• Muscles attach:– Directly—epimysium of muscle is fused to the
periosteum of bone or perichondrium of cartilage– Indirectly—connective tissue wrappings extend
beyond the muscle as a ropelike tendon or sheetlike aponeurosis

Table 9.1
Microscopic Anatomy of a Skeletal Muscle Fiber
• Cylindrical cell 10 to 100 m in diameter, up to 30 cm long
• Multiple peripheral nuclei• Many mitochondria• Glycosomes for glycogen storage, myoglobin
for O2 storage• Also contain myofibrils, sarcoplasmic
reticulum, and T tubules
Myofibrils
• Densely packed, rodlike elements • ~80% of cell volume • Exhibit striations: perfectly aligned repeating
series of dark A bands and light I bands

NucleusLight I bandDark A band
Sarcolemma
Mitochondrion
(b) Diagram of part of a muscle fiber showing the myofibrils. Onemyofibril is extended afrom the cut end of the fiber.
Myofibril
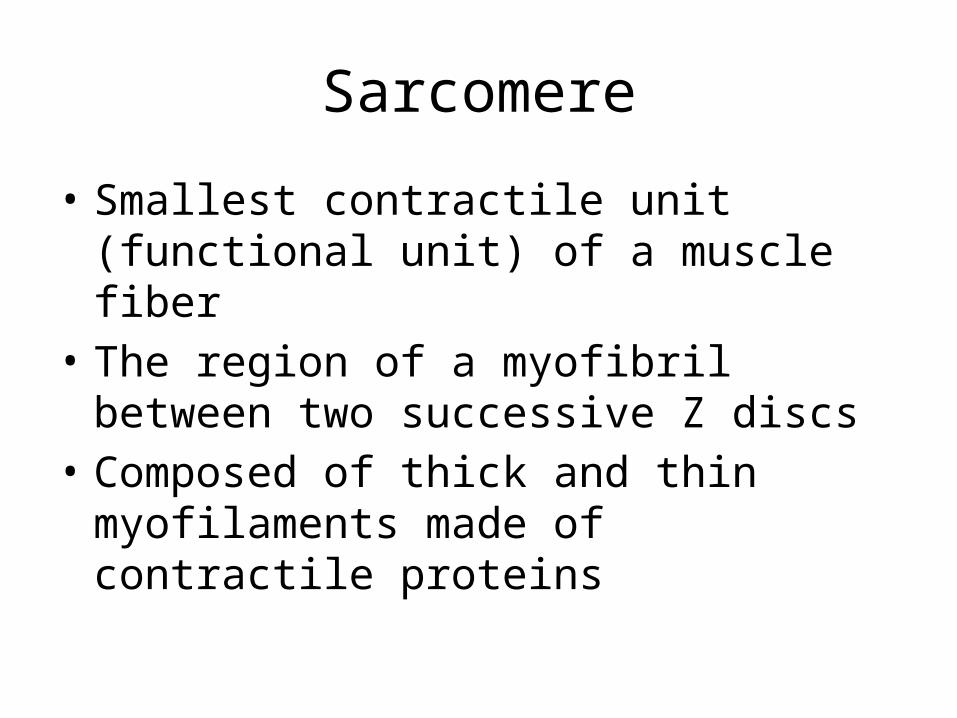
Sarcomere
• Smallest contractile unit (functional unit) of a muscle fiber
• The region of a myofibril between two successive Z discs
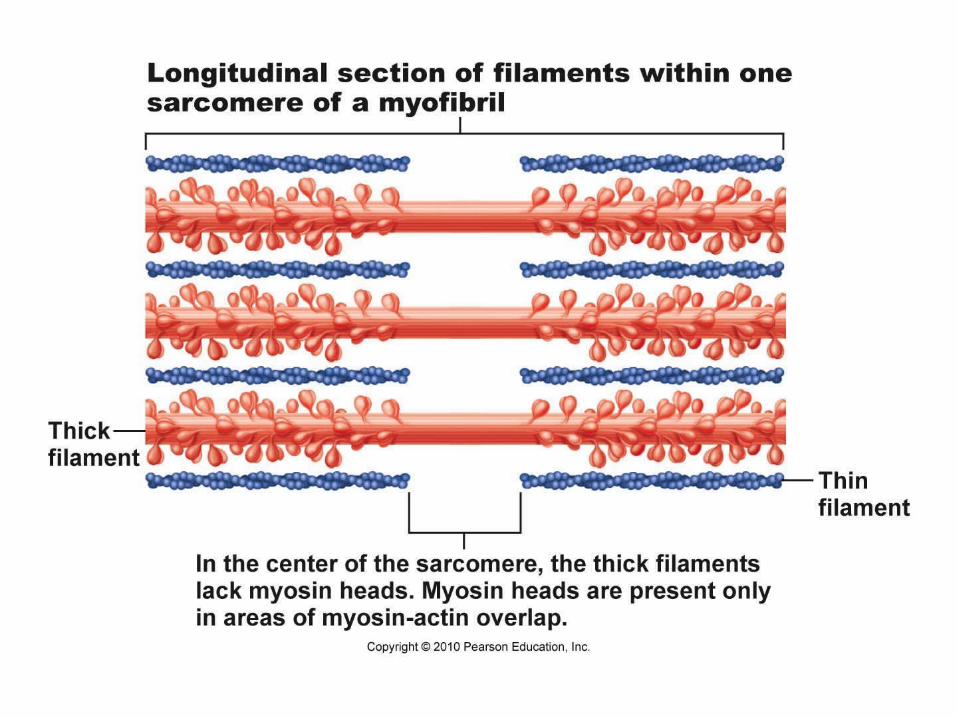
• Composed of thick and thin myofilaments made of contractile proteins

Features of a Sarcomere
• Thick filaments• Thin filaments• Z disc• H zone• M line

Ultrastructure of Thick Filament• Composed of the protein myosin
– Myosin tails contain: • 2 interwoven, heavy polypeptide chains
– Myosin heads contain: • 2 smaller, light polypeptide chains that
act as cross bridges during contraction • Binding sites for actin of thin filaments• Binding sites for ATP• ATPase enzymes

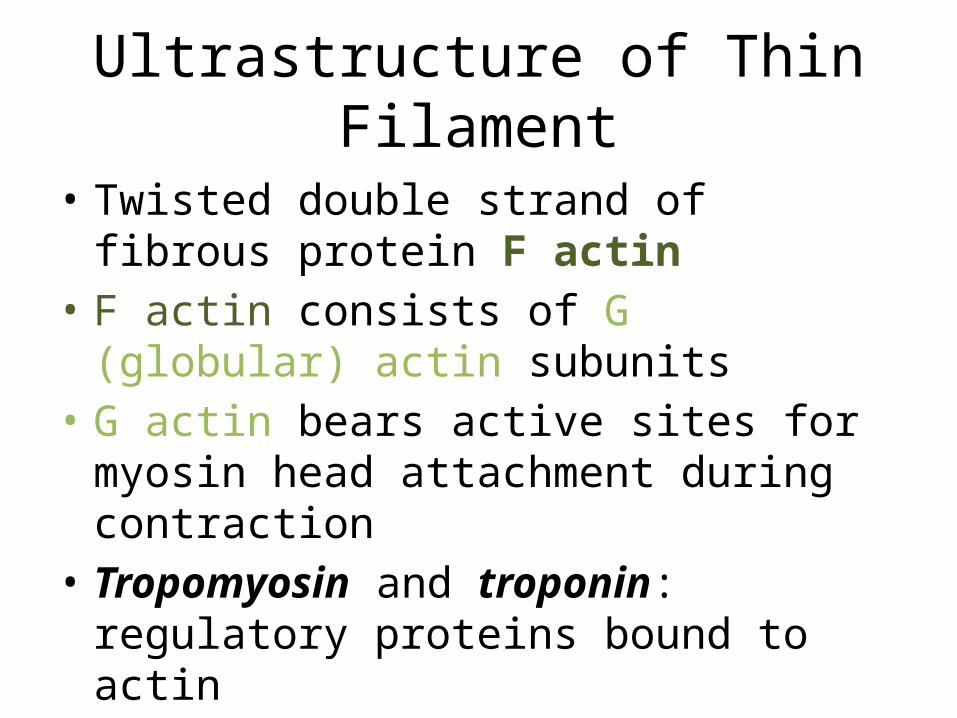
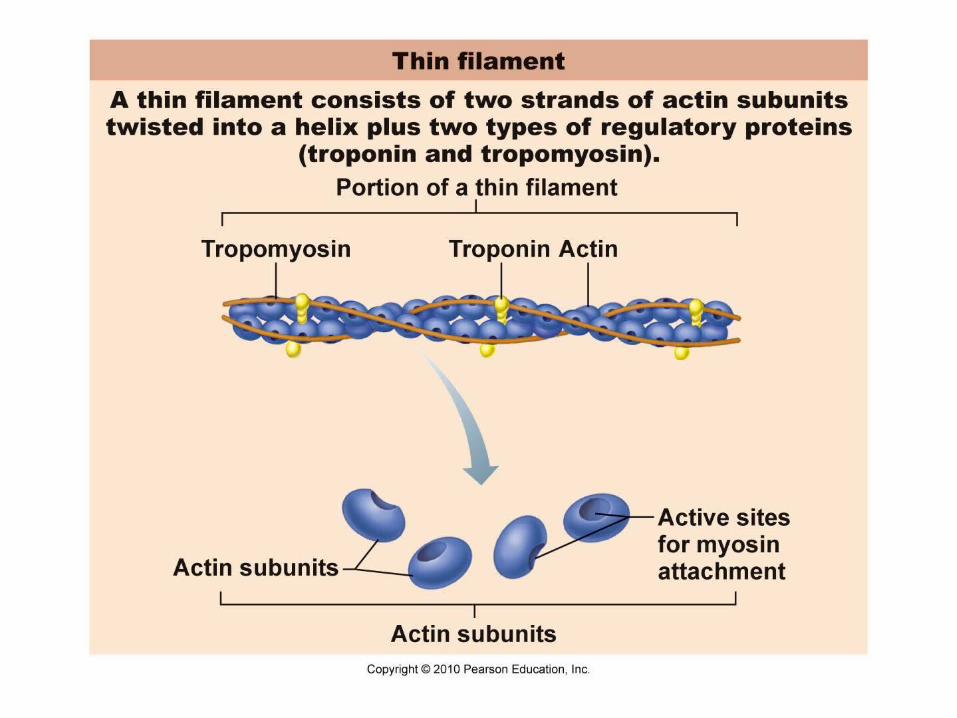
Ultrastructure of Thin Filament
• Twisted double strand of fibrous protein F actin
• F actin consists of G (globular) actin subunits • G actin bears active sites for myosin head
attachment during contraction• Tropomyosin and troponin: regulatory
proteins bound to actin

Sarcoplasmic Reticulum (SR)
• Network of smooth endoplasmic reticulum surrounding each myofibril
• Pairs of terminal cisternae form perpendicular cross channels
• Functions in the regulation of intracellular Ca2+ levels
T Tubules
• Continuous with the sarcolemma• Penetrate the cell’s interior at each A band–I
band junction• Associate with the paired terminal cisternae to
form triads that encircle each sarcomere

Figure 9.5
Myofibril
Myofibrils
Triad:
Tubules ofthe SR
Sarcolemma
Sarcolemma
Mitochondria
I band I bandA band
H zone Z discZ disc
Part of a skeletalmuscle fiber (cell)
• T tubule• Terminal
cisternaeof the SR (2)
M line
Triad Relationships
• T tubules conduct impulses deep into muscle fiber
• Integral proteins protrude into the intermembrane space from T tubule and SR cisternae membranes
• T tubule proteins: voltage sensors• SR foot proteins: gated channels that regulate
Ca2+ release from the SR cisternae

Contraction
• The generation of force • Does not necessarily cause shortening of the
fiber• Shortening occurs when tension generated by
cross bridges on the thin filaments exceeds forces opposing shortening

Sliding Filament Model of Contraction
• In the relaxed state, thin and thick filaments overlap only slightly
• During contraction, myosin heads bind to actin, detach, and bind again, to propel the thin filaments toward the M line
• As H zones shorten and disappear, sarcomeres shorten, muscle cells shorten, and the whole muscle shortens

Figure 9.6
Fully relaxed sarcomere of a muscle fiber
Z Z
II
HA
Z Z
II AFully contracted sarcomere of a muscle fiber

Requirements for Skeletal Muscle Contraction
1. Activation: neural stimulation at aneuromuscular junction
2. Excitation-contraction coupling: – Generation and propagation of an action
potential along the sarcolemma– Final trigger: a brief rise in intracellular Ca2+ levels

Events at the Neuromuscular Junction

Events at the Neuromuscular Junction

Figure 9.8
Nucleus
Actionpotential (AP)
Myelinated axonof motor neuron
Axon terminal ofneuromuscular junction
Sarcolemma ofthe muscle fiber
Ca2+Ca2+
Axon terminalof motor neuron
Synaptic vesiclecontaining AChMitochondrionSynapticcleft
Junctionalfolds ofsarcolemma
Fusing synaptic vesicles
ACh
Sarcoplasm ofmuscle fiber
Postsynaptic membraneion channel opens;ions pass.
Na+ K+
Ach–
Na+
K+
Degraded ACh
Acetyl-cholinesterase
Postsynaptic membraneion channel closed;ions cannot pass.
1 Action potential arrives ataxon terminal of motor neuron.
2 Voltage-gated Ca2+ channels open and Ca2+ enters the axon terminal.
3 Ca2+ entry causes some synaptic vesicles to release their contents (acetylcholine)by exocytosis.
4 Acetylcholine, aneurotransmitter, diffuses across the synaptic cleft and binds to receptors in the sarcolemma.
5 ACh binding opens ionchannels that allow simultaneous passage of Na+ into the musclefiber and K+ out of the muscle fiber.
6 ACh effects are terminated by its enzymatic breakdown in the synaptic cleft by acetylcholinesterase.
Events in Generation of an Action Potential
1. Local depolarization (end plate potential):– ACh binding opens chemically (ligand) gated ion
channels– Simultaneous diffusion of Na+ (inward) and K+
(outward)– More Na+ diffuses, so the interior of the
sarcolemma becomes less negative

Figure 9.9, step 1
Na+
Na+
Open Na+
ChannelClosed K+
Channel
K+
Na+ K+Action potential
++++++
+++++
+
Axon terminal
Synapticcleft
ACh
ACh
Sarcoplasm of muscle fiber
K+
1 Local depolarization: generation of the end plate potential on the sarcolemma
1
Wave
ofde
po
lari
zatio
n
Events in Generation of an Action Potential
2. Generation and propagation of an action potential:
– End plate potential spreads to adjacent membrane areas
– Voltage-gated Na+ channels open– Na+ influx decreases the membrane voltage
toward a critical threshold– If threshold is reached, an action potential is
generated
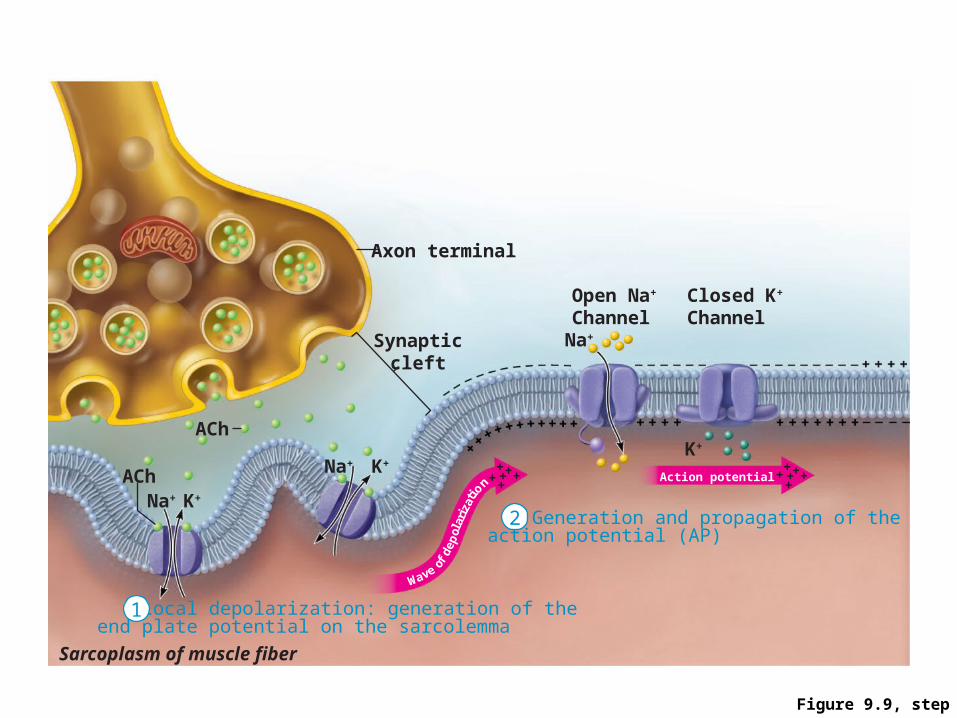
Figure 9.9, step 2
Na+
Na+
Open Na+
ChannelClosed K+
Channel
K+
Na+ K+Action potential
++++++
+++++
+
Axon terminal
Synapticcleft
ACh
ACh
Sarcoplasm of muscle fiber
K+
Generation and propagation of the action potential (AP)
1 Local depolarization: generation of the end plate potential on the sarcolemma
2
1
Wave
ofde
po
lari
zatio
n

Events in Generation of an Action Potential
• Local depolarization wave continues to spread, changing the permeability of the sarcolemma
• Voltage-regulated Na+ channels open in the adjacent patch, causing it to depolarize to threshold
Events in Generation of an Action Potential
3. Repolarization:• Na+ channels close and voltage-gated K+
channels open• K+ efflux rapidly restores the resting polarity• Fiber cannot be stimulated and is in a
refractory period until repolarization is complete
• Ionic conditions of the resting state are restored by the Na+-K+ pump

Figure 9.9
Na+
Na+
Open Na+
ChannelClosed K+
Channel
Action potential++++++
+++++
+
Axon terminal
Synapticcleft
ACh
ACh
Sarcoplasm of muscle fiber
K+
2 Generation and propagation ofthe action potential (AP)
3 Repolarization
1 Local depolarization: generation of the end plate potential on the sarcolemma
K+
K+Na+
K+Na+
Wave ofde
po
lari
zatio
n
Closed Na+
ChannelOpen K+
Channel
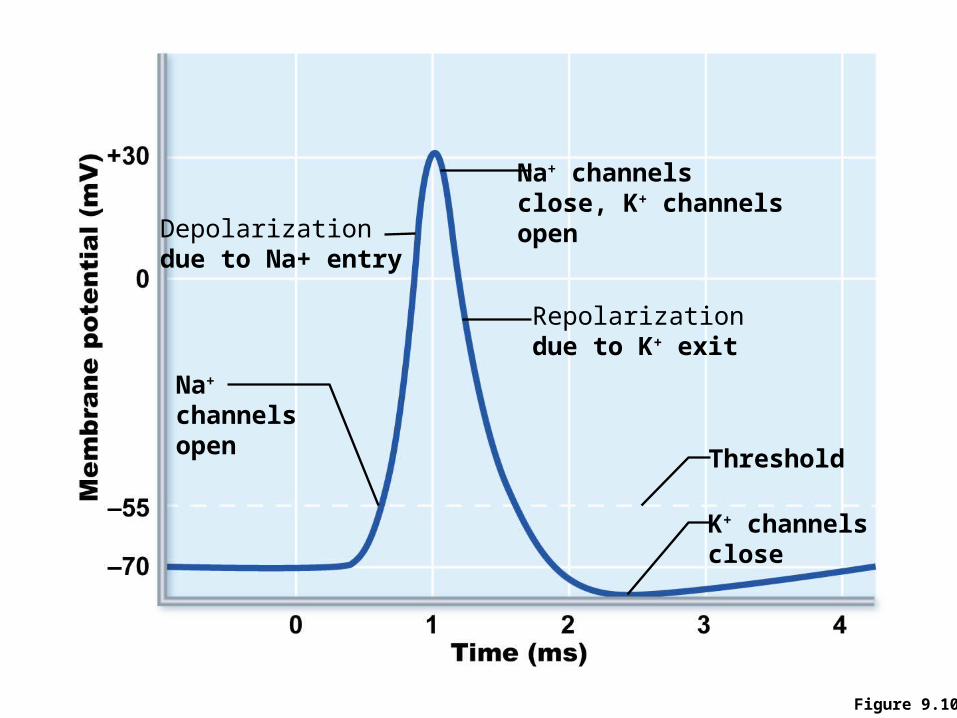
Figure 9.10
Na+ channelsclose, K+ channelsopen
K+ channelsclose
Repolarizationdue to K+ exit
Threshold
Na+
channelsopen
Depolarizationdue to Na+ entry

Excitation-Contraction (E-C) Coupling
• Sequence of events by which transmission of an AP along the sarcolemma leads to sliding of the myofilaments
• Latent period:– Time when E-C coupling events occur– Time between AP initiation and the beginning of
contraction

Events of Excitation-Contraction (E-C) Coupling
• AP is propagated along sarcomere to T tubules• Voltage-sensitive proteins stimulate Ca2+
release from SR – Ca2+ is necessary for contraction
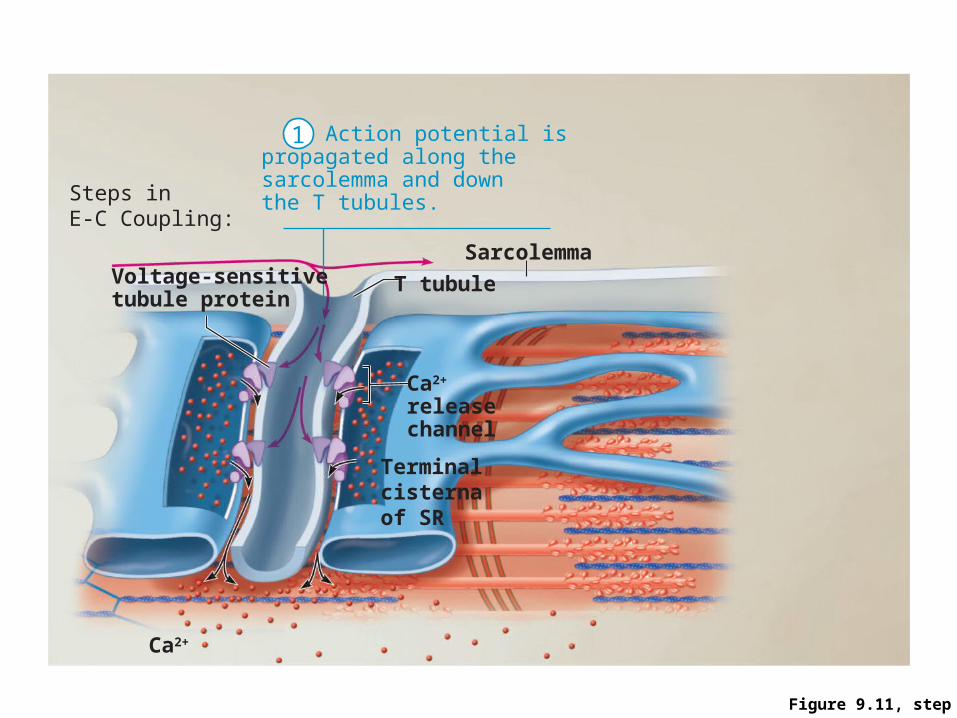
Figure 9.11, step 3
Steps inE-C Coupling:
Terminal cisterna of SR
Voltage-sensitivetubule protein
T tubule
Ca2+
releasechannel
Ca2+
Sarcolemma
Action potential ispropagated along thesarcolemma and downthe T tubules.
1

Figure 9.11, step 4
Steps inE-C Coupling:
Terminal cisterna of SR
Voltage-sensitivetubule protein
T tubule
Ca2+
releasechannel
Ca2+
Sarcolemma
Action potential ispropagated along thesarcolemma and downthe T tubules.
Calciumions arereleased.
1
2

Figure 9.11, step 5
Troponin Tropomyosinblocking active sitesMyosin
Actin
Ca2+
The aftermath

Figure 9.11, step 6
Troponin Tropomyosinblocking active sitesMyosin
Actin
Active sites exposed and ready for myosin binding
Ca2+
Calcium binds totroponin and removesthe blocking action oftropomyosin.
The aftermath
3

Figure 9.11, step 7
Troponin Tropomyosinblocking active sitesMyosin
Actin
Active sites exposed and ready for myosin binding
Ca2+
Myosincross bridge
Calcium binds totroponin and removesthe blocking action oftropomyosin.
Contraction begins
The aftermath
3
4
Role of Calcium (Ca2+) in Contraction
• At low intracellular Ca2+ concentration:– Tropomyosin blocks the active sites on actin– Myosin heads cannot attach to actin– Muscle fiber relaxes
Role of Calcium (Ca2+) in Contraction
• At higher intracellular Ca2+ concentrations:– Ca2+ binds to troponin – Troponin changes shape and moves tropomyosin
away from active sites– Events of the cross bridge cycle occur – When nervous stimulation ceases, Ca2+ is pumped
back into the SR and contraction ends
Cross Bridge Cycle
• Continues as long as the Ca2+ signal and adequate ATP are present
• Cross bridge formation—high-energy myosin head attaches to thin filament
• Working (power) stroke—myosin head pivots and pulls thin filament toward M line

Cross Bridge Cycle
• Cross bridge detachment—ATP attaches to myosin head and the cross bridge detaches
• “Cocking” of the myosin head—energy from hydrolysis of ATP cocks the myosin head into the high-energy state
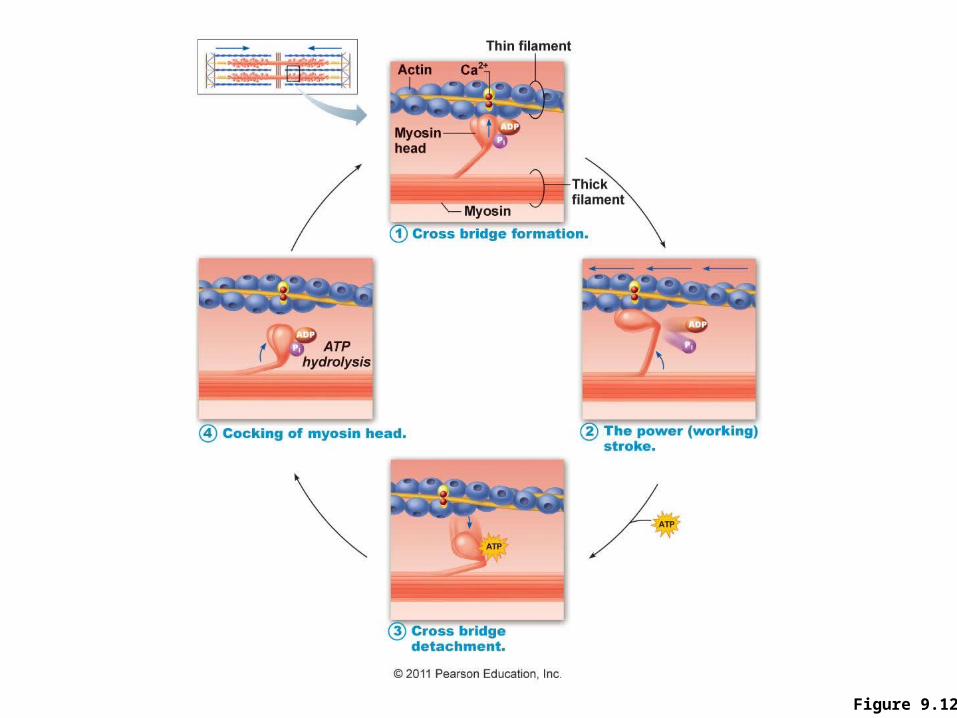
Figure 9.12

Principles of Muscle Mechanics
1. Same principles apply to contraction of a single fiber and a whole muscle
2. Contraction produces tension, the force exerted on the load or object to be moved
3. Contraction does not always shorten a muscle:
– Isometric contraction: no shortening; muscle tension increases but does not exceed the load
– Isotonic contraction: muscle shortens because muscle tension exceeds the load
Principles of Muscle Mechanics
4. Force and duration of contraction vary in response to stimuli of different frequencies and intensities

Motor Unit
• Motor unit = a motor neuron and all muscle fibers it supplies– Small motor units in muscles that control fine
movements (fingers, eyes) – Large motor units in large weight-bearing muscles
(thighs, hips) • Muscle fibers from a motor unit are spread
throughout the muscle• Motor units in a muscle usually contract
asynchronously
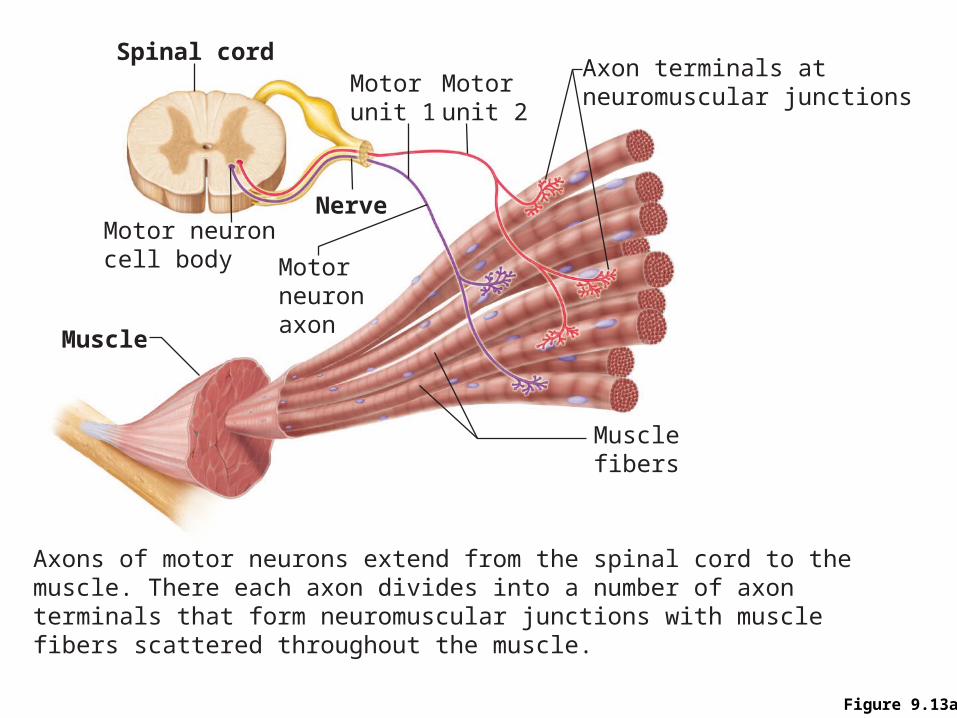
Figure 9.13a
Spinal cord
Motor neuroncell body
Muscle
Nerve
Motorunit 1
Motorunit 2
Musclefibers
Motorneuronaxon
Axon terminals atneuromuscular junctions
Axons of motor neurons extend from the spinal cord to the muscle. There each axon divides into a number of axon terminals that form neuromuscular junctions with muscle fibers scattered throughout the muscle.
Muscle Twitch
• Response of a muscle to a single, brief threshold stimulus
• Three phases of a twitch:– Latent period: events of excitation-contraction
coupling– Period of contraction: cross bridge formation;
tension increases– Period of relaxation: Ca2+ re-entry into the SR;
tension declines to zero
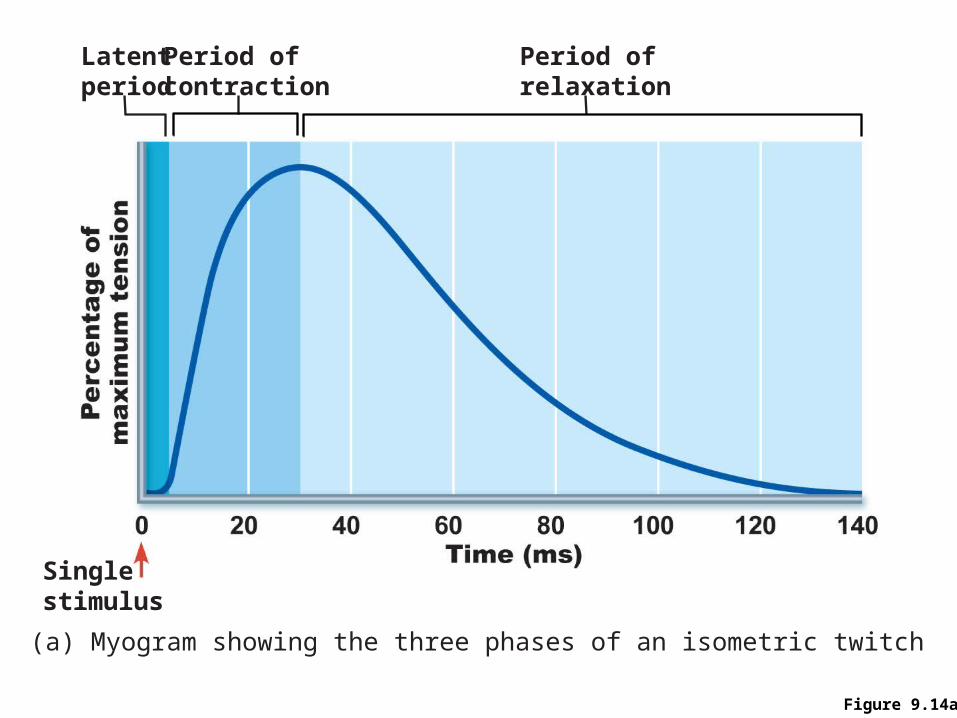
Figure 9.14a
Latentperiod
Singlestimulus
Period ofcontraction
Period ofrelaxation
(a) Myogram showing the three phases of an isometric twitch

Muscle Twitch Comparisons
Different strength and duration of twitches are due to variations in metabolic properties and enzymes between muscles

Graded Muscle Responses
• Variations in the degree of muscle contraction• Required for proper control of skeletal
movementResponses are graded by:
1. Changing the frequency of stimulation2. Changing the strength of the stimulus
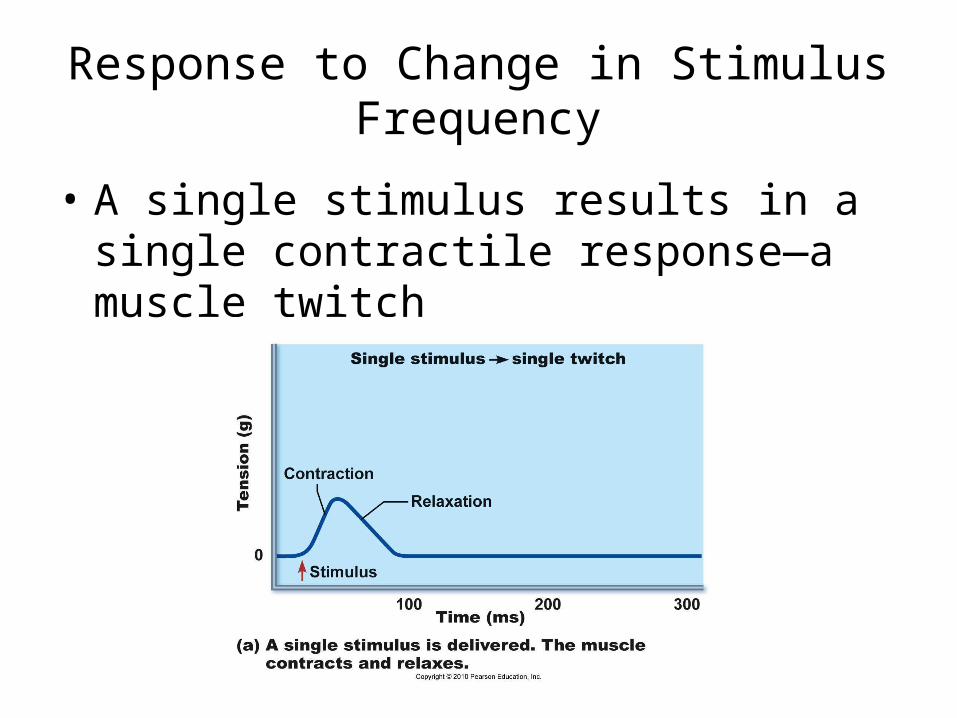
Response to Change in Stimulus Frequency
• A single stimulus results in a single contractile response—a muscle twitch

Response to Change in Stimulus Frequency
• Increase frequency of stimulus (muscle does not have time to completely relax between stimuli)
• Ca2+ release stimulates further contraction temporal (wave) summation
• Further increase in stimulus frequency unfused (incomplete) tetanus
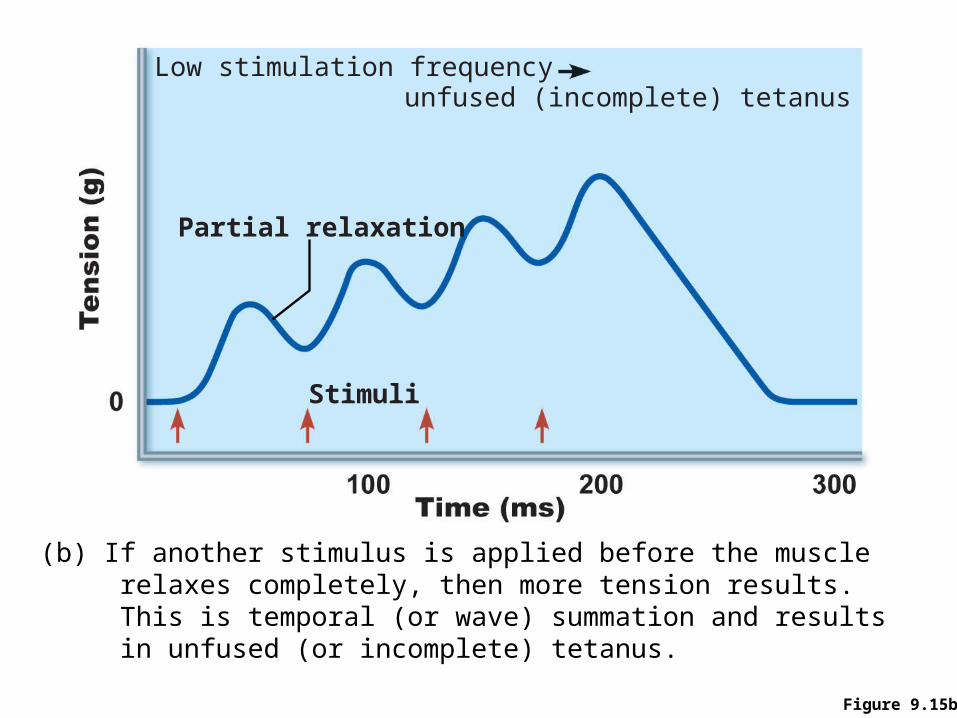
Figure 9.15b
Stimuli
Partial relaxation
Low stimulation frequencyunfused (incomplete) tetanus
(b) If another stimulus is applied before the muscle relaxes completely, then more tension results. This is temporal (or wave) summation and results in unfused (or incomplete) tetanus.
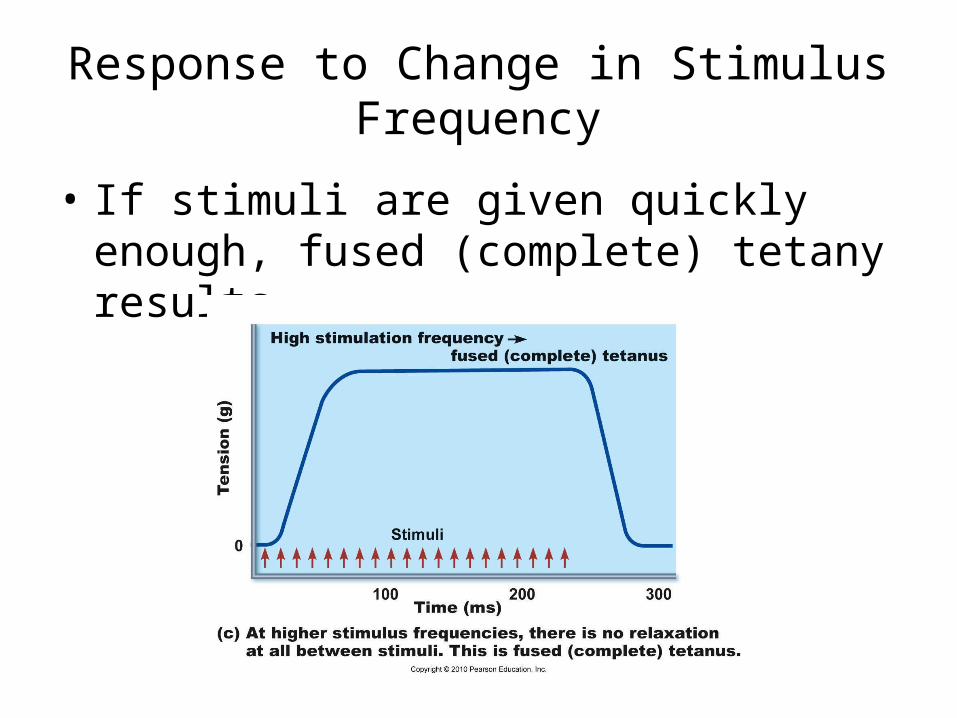
Response to Change in Stimulus Frequency
• If stimuli are given quickly enough, fused (complete) tetany results

Response to Change in Stimulus Strength
• Threshold stimulus: stimulus strength at which the first observable muscle contraction occurs
• Muscle contracts more vigorously as stimulus strength is increased above threshold
• Contraction force is precisely controlled by recruitment (multiple motor unit summation)– Increase in the number of active motor units

Figure 9.16
Stimulus strength
Proportion of motor units excited
Strength of muscle contraction
Maximal contraction
Maximalstimulus
Thresholdstimulus

Response to Change in Stimulus Strength
• Size principle: motor units with larger and larger fibers are recruited as stimulus intensity increases

Muscle Tone
• Constant, slightly contracted state of all muscles
• Due to spinal reflexes that activate groups of motor units alternately in response to input from stretch receptors in muscles
• Keeps muscles firm, healthy, and ready to respond

Isotonic Contractions
• Muscle changes in length and moves the load• Isotonic contractions are either concentric or
eccentric:– Concentric contractions—the muscle shortens and
does work– Eccentric contractions—the muscle contracts as it
lengthens

Figure 9.18a
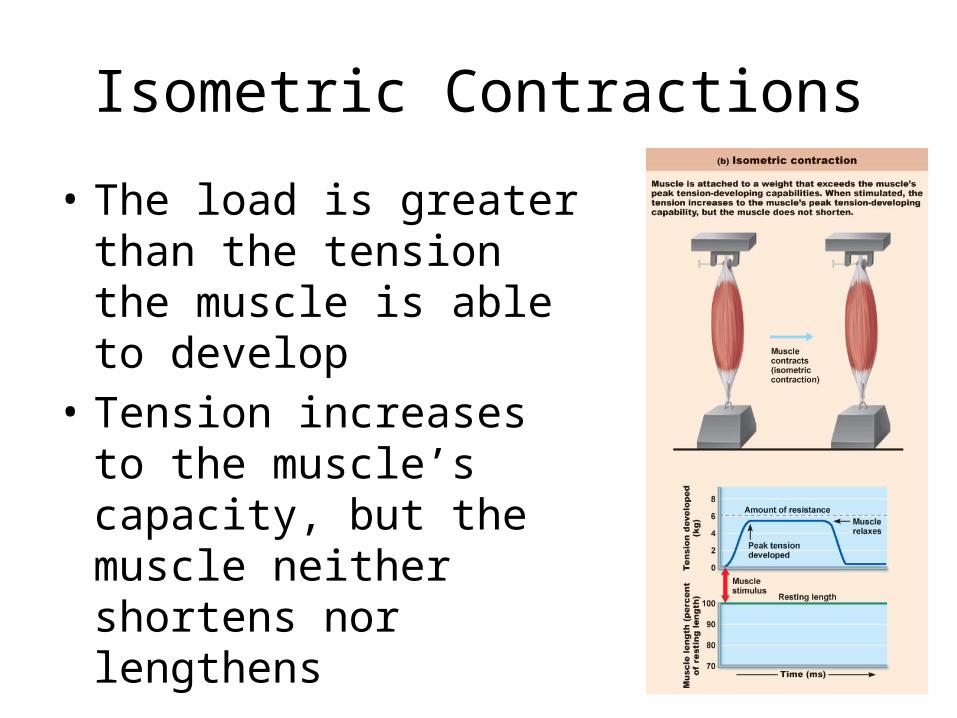
Isometric Contractions
• The load is greater than the tension the muscle is able to develop
• Tension increases to the muscle’s capacity, but the muscle neither shortens nor lengthens
Muscle Metabolism: Energy for Contraction
• ATP is the only source used directly for contractile activities
• Available stores of ATP are depleted in 4–6 seconds

Muscle Metabolism: Energy for Contraction
• ATP is regenerated by:– Direct phosphorylation of ADP by creatine
phosphate (CP) – Anaerobic pathway (glycolysis) – Aerobic respiration
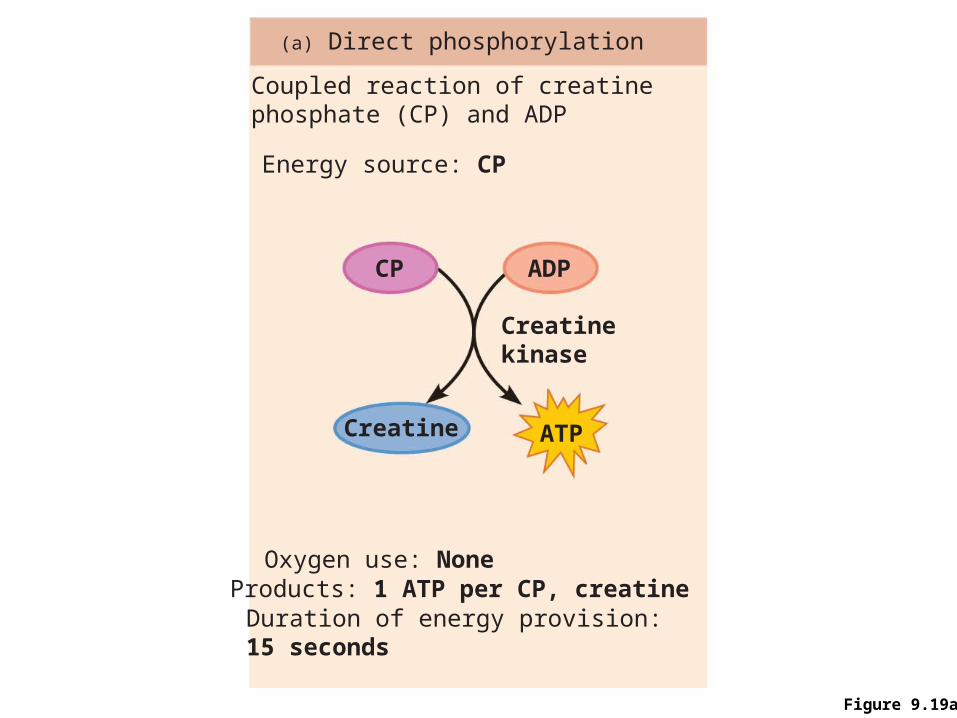
Figure 9.19a
Coupled reaction of creatinephosphate (CP) and ADP
Energy source: CP
(a) Direct phosphorylation
Oxygen use: NoneProducts: 1 ATP per CP, creatineDuration of energy provision:15 seconds
Creatinekinase
ADPCP
Creatine ATP

Anaerobic Pathway
• At 70% of maximum contractile activity:– Bulging muscles compress blood vessels– Oxygen delivery is impaired– Pyruvic acid is converted into lactic acid

Anaerobic Pathway
• Lactic acid:– Diffuses into the
bloodstream– Used as fuel by the liver,
kidneys, and heart– Converted back into
pyruvic acid by the liver

Aerobic Pathway
• Produces 95% of ATP during rest and light to moderate exercise
• Fuels: stored glycogen, then bloodborne glucose, pyruvic acid from glycolysis, and free fatty acids

Muscle Fatigue
• Physiological inability to contract• Occurs when:
– Ionic imbalances (K+, Ca2+, Pi) interfere with E-C coupling
– Prolonged exercise damages the SR and interferes with Ca2+ regulation and release
• Total lack of ATP occurs rarely, during states of continuous contraction, and causes contractures (continuous contractions)

Oxygen Deficit
Extra O2 needed after exercise for:• Replenishment of
– Oxygen reserves – Glycogen stores – ATP and CP reserves
• Conversion of lactic acid to pyruvic acid, glucose, and glycogen
Heat Production During Muscle Activity
• ~ 40% of the energy released in muscle activity is useful as work
• Remaining energy (60%) given off as heat • Dangerous heat levels are prevented by
radiation of heat from the skin and sweating

Force of Muscle Contraction
• The force of contraction is affected by:– Number of muscle fibers stimulated (recruitment)– Relative size of the fibers—hypertrophy of cells
increases strength– Frequency of stimulation— frequency allows
time for more effective transfer of tension to noncontractile components
– Length-tension relationship—muscles contract most strongly when muscle fibers are 80–120% of their normal resting length

Figure 9.22
Sarcomeresgreatly
shortened
Sarcomeres atresting length
Sarcomeres excessivelystretched
170%
Optimal sarcomereoperating length(80%–120% ofresting length)
100%75%

Velocity and Duration of Contraction
Influenced by:1. Muscle fiber type2. Load3. Recruitment

Muscle Fiber Type
Classified according to two characteristics:1. Speed of contraction: slow or fast, according
to:– Speed at which myosin ATPases split ATP– Pattern of electrical activity of the motor neurons
2. Metabolic pathways for ATP synthesis:– Oxidative fibers—use aerobic pathways– Glycolytic fibers—use anaerobic glycolysis

Muscle Fiber Type
Three types: – Slow oxidative fibers– Fast oxidative fibers– Fast glycolytic fibers

Table 9.2

Figure 9.24
FO
FG
SO
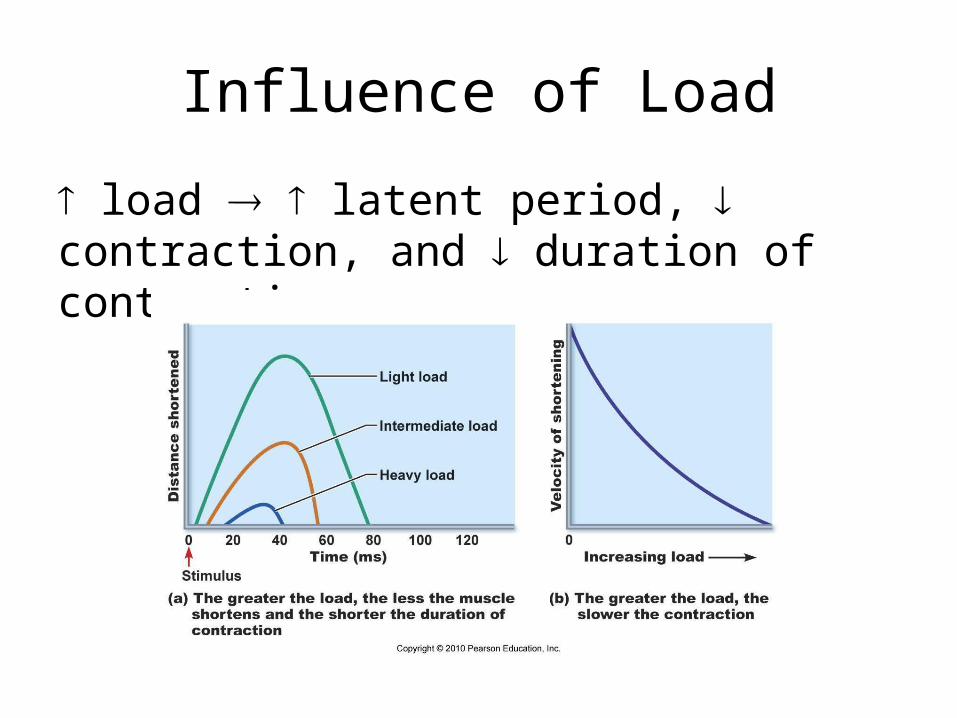
Influence of Load
load latent period, contraction, and duration of contraction

Influence of Recruitment
Recruitment faster contraction and duration of contraction
Effects of Exercise
Aerobic (endurance) exercise:• Leads to increased:
– Muscle capillaries– Number of mitochondria– Myoglobin synthesis
• Results in greater endurance, strength, and resistance to fatigue
• May convert fast glycolytic fibers into fast oxidative fibers
Effects of Resistance Exercise
• Resistance exercise (typically anaerobic) results in:– Muscle hypertrophy (due to increase in fiber size)– Increased mitochondria, myofilaments, glycogen
stores, and connective tissue

Smooth Muscle
• Found in walls of most hollow organs(except heart)
• Usually in two layers (longitudinal and circular)

Peristalsis
• Alternating contractions and relaxations of smooth muscle layers that mix and squeeze substances through the lumen of hollow organs– Longitudinal layer contracts; organ dilates and
shortens – Circular layer contracts; organ constricts and
elongates

Microscopic Structure
• Spindle-shaped fibers: thin and short compared with skeletal muscle fibers
• Connective tissue: endomysium only• SR: less developed than in skeletal muscle • Pouchlike infoldings (caveolae) of sarcolemma
sequester Ca2+
• No sarcomeres, myofibrils, or T tubules

Innervation of Smooth Muscle
• Autonomic nerve fibers innervate smooth muscle at diffuse junctions
• Varicosities (bulbous swellings) of nerve fibers store and release neurotransmitters
Myofilaments in Smooth Muscle
• Ratio of thick to thin filaments (1:13) is much lower than in skeletal muscle (1:2)
• Thick filaments have heads along their entire length• No troponin complex; protein calmodulin binds Ca2+
• Myofilaments are spirally arranged, causing smooth muscle to contract in a corkscrew manner
• Dense bodies: proteins that anchor noncontractile intermediate filaments to sarcolemma at regular intervals
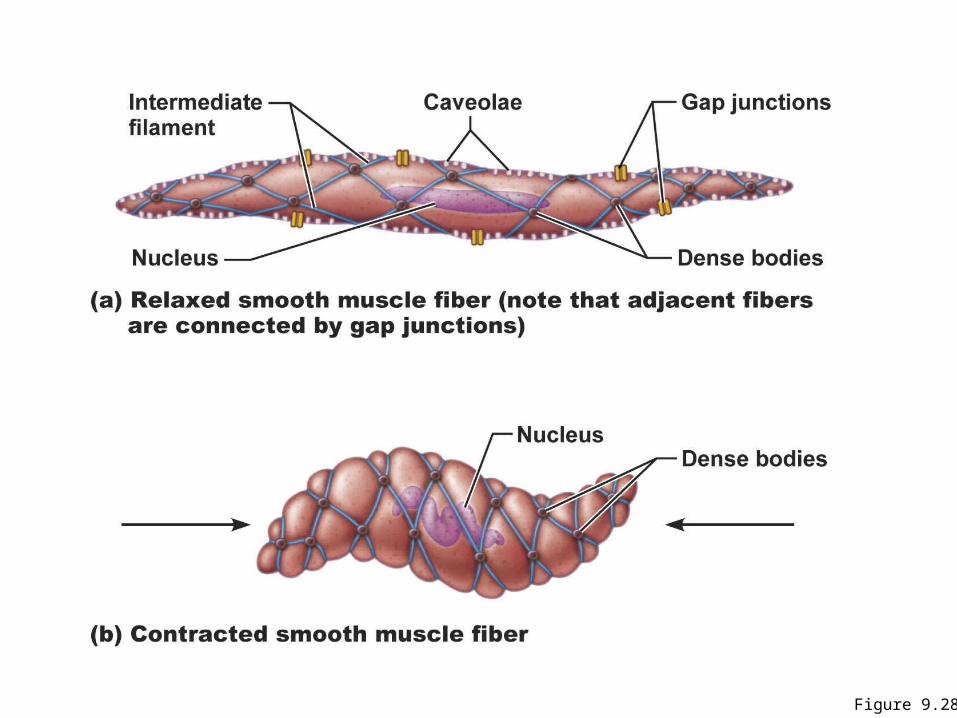
Figure 9.28

Contraction of Smooth Muscle
• Slow, synchronized contractions • Cells are electrically coupled by gap junctions• Some cells are self-excitatory (depolarize
without external stimuli); act as pacemakers for sheets of muscle – Rate and intensity of contraction may be modified
by neural and chemical stimuli
Contraction of Smooth Muscle
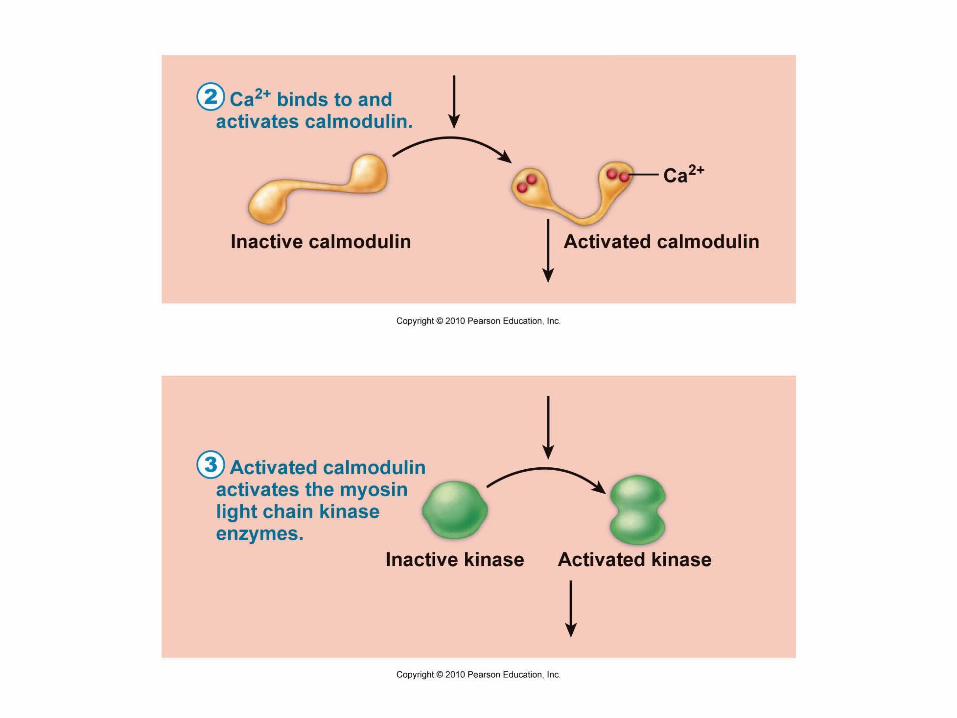
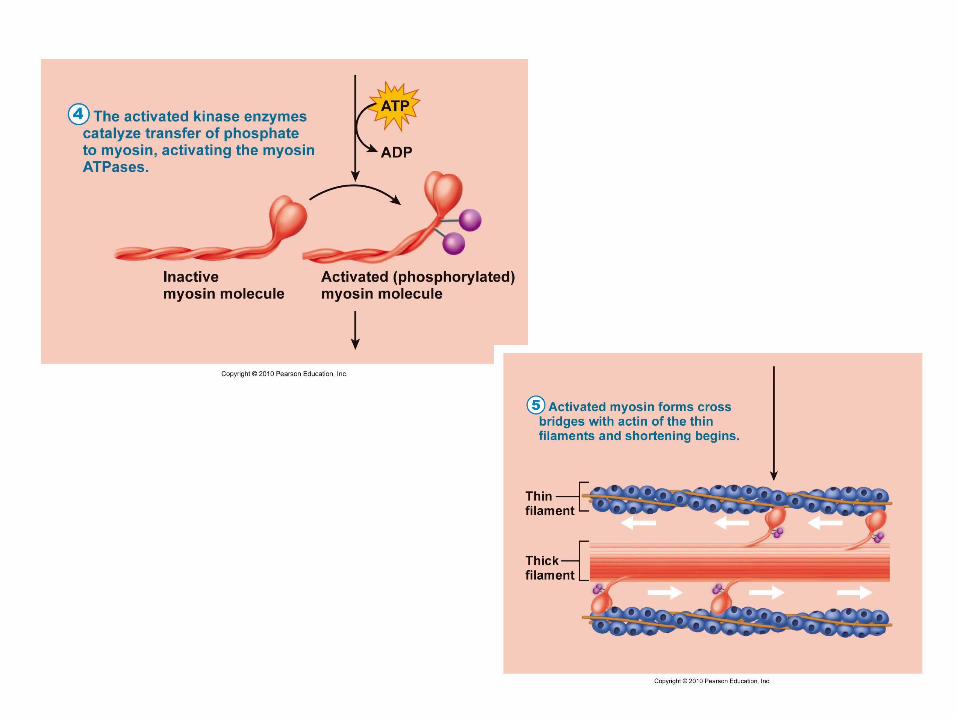
• Sliding filament mechanism• Final trigger is intracellular Ca2+
• Ca2+ is obtained from the SR and extracellular space• Ca2+ binds to and activates calmodulin • Activated calmodulin activates myosin (light chain)
kinase• Activated kinase phosphorylates and activates
myosin • Cross bridges interact with actin

Figure 9.29, step 1
Calcium ions (Ca2+)enter the cytosol fromthe ECF via voltage-dependent or voltage-independent Ca2+
channels, or fromthe scant SR.
Extracellular fluid (ECF)
Ca2+
Ca2+
Plasma membrane
Sarcoplasmicreticulum
Cytoplasm
1

Contraction of Smooth Muscle
• Very energy efficient (slow ATPases)• Myofilaments may maintain a latch state for
prolonged contractionsRelaxation requires:• Ca2+ detachment from calmodulin• Active transport of Ca2+ into SR and ECF• Dephosphorylation of myosin to reduce
myosin ATPase activity
Regulation of Contraction
Neural regulation:• Neurotransmitter binding [Ca2+] in
sarcoplasm; either graded (local) potential or action potential
• Response depends on neurotransmitter released and type of receptor molecules
Hormones and local chemicals:– May bind to G protein–linked receptors– May either enhance or inhibit Ca2+ entry

Special Features of Smooth Muscle Contraction
Stress-relaxation response: – Responds to stretch only briefly, then adapts to
new length– Retains ability to contract on demand– Enables organs such as the stomach and bladder
to temporarily store contentsLength and tension changes:
– Can contract when between half and twice its resting length
Special Features of Smooth Muscle Contraction
Hyperplasia:– Smooth muscle cells can divide and increase their
numbers– Example:
• estrogen effects on uterus at puberty and during pregnancy
Types of Smooth Muscle
Single-unit (visceral) smooth muscle: – Sheets contract rhythmically as a unit (gap junctions)– Often exhibit spontaneous action potentials– Arranged in opposing sheets and exhibit stress-relaxation
response
Multiunit smooth muscle:– Located in large airways, large arteries, arrector pili
muscles, and iris of eye– Gap junctions are rare– Arranged in motor units– Graded contractions occur in response to neural stimuli

Other interesting points..
• Athletics and training can improve neuromuscular control
• Female skeletal muscle makes up 36% of body mass, male 42% (testosterone!)– Body strength per unit muscle mass is the same in both
sexes• With age, connective tissue increases and muscle
fibers decrease• By age 30, loss of muscle mass (sarcopenia) begins
– Regular exercise reverses sarcopenia

Muscular Dystrophy
Duchenne muscular dystrophy (DMD):– Most common and severe type– Inherited, sex-linked, carried by females and expressed in
males (1/3500) as lack of dystrophin– Victims become clumsy and fall frequently; usually die of
respiratory failure in their 20s– No cure, but viral gene therapy or infusion of stem cells
with correct dystrophin genes show promise
Recommended

















