High Reliability / Human
Factors
Chris Hancock & Mike Fealey: Programme Managers, 1000 Lives
Plus
Acknowledgement
• Kind thanks to Atrainability for some of
the info and slides contained in this
presentation
Working Together
Rollercoaster
Mortality
• 1 in 1.5 billion chance of being fatally
injured at an amusement park
• Injury rates for golf and deckchairs are
higher
– US Consumer Product Safety Commission
(2007)
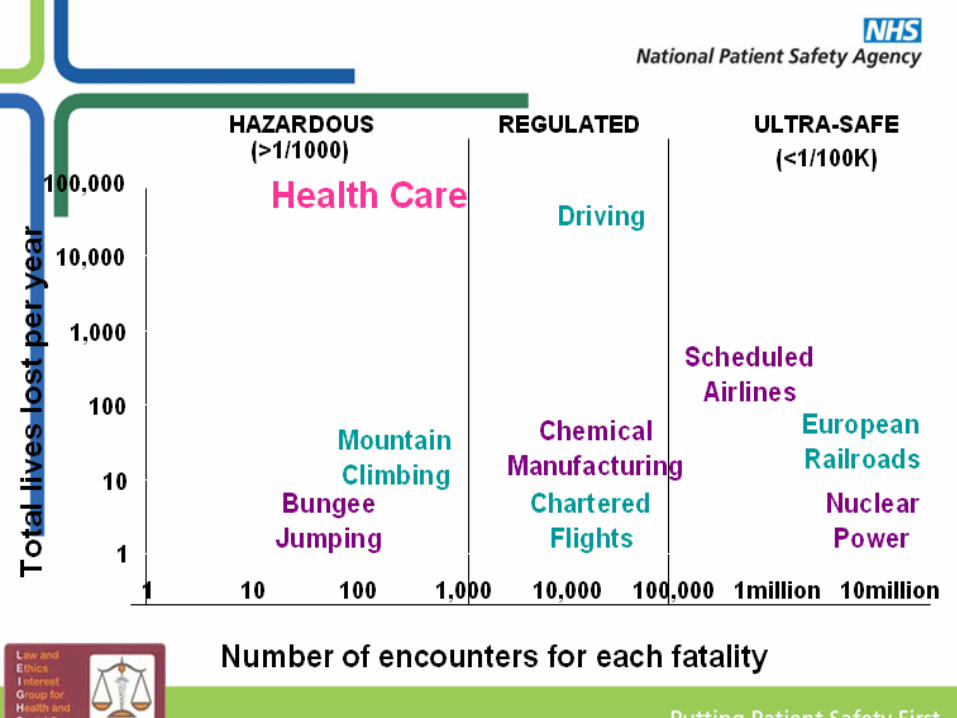
Hospital Mortality and
Harm• There is a one in 300
chance of accidental death
through errors in care. (Institute of Medicine, 2000)
• More than one in ten
people admitted to hospital
are harmed unintentionally
by its care. (Vincent et al. 2001)
• 11859 adult
preventable deaths
in hospitals in
England• Horgan et al 2012
Patient Safety
3,283 patients dead through preventable error, another 7,000 suffer severe harm
Equivalent to 9 medium size aircraft (Boeing 737/Airbus A320) being written off with total loss of life every year……
…..in the UK!
Shall We Save 100 Lives
www.1000livesplus.wales.nhs.uk
Mid Staffs Questions ...
• What are the warning signs that a hospital (or
any other part of the NHS) is in trouble?
• Why did so many senior staff in giving evidence
express their horror that they had not known
about the poor care on many of the wards?
• Is Stafford a classic case of organisational
blindness?
• The question I want you to keep asking
yourselves as we relay the story is, ‘Could it
happen on my patch? Could it happen in my
hospital and how would I know?’
– Prof Edwards 2012
Hands up
Who comes to
work to harm
people?
So who’s fault is it?
Insert name of presentation on Master Slide
Insert name of presentation on Master Slide
Insert name of presentation on Master Slide
Insert name of presentation on Master Slide
• Now take a minute per question to
come to agreement on each table
Insert name of presentation on Master Slide
Insert name of presentation on Master Slide
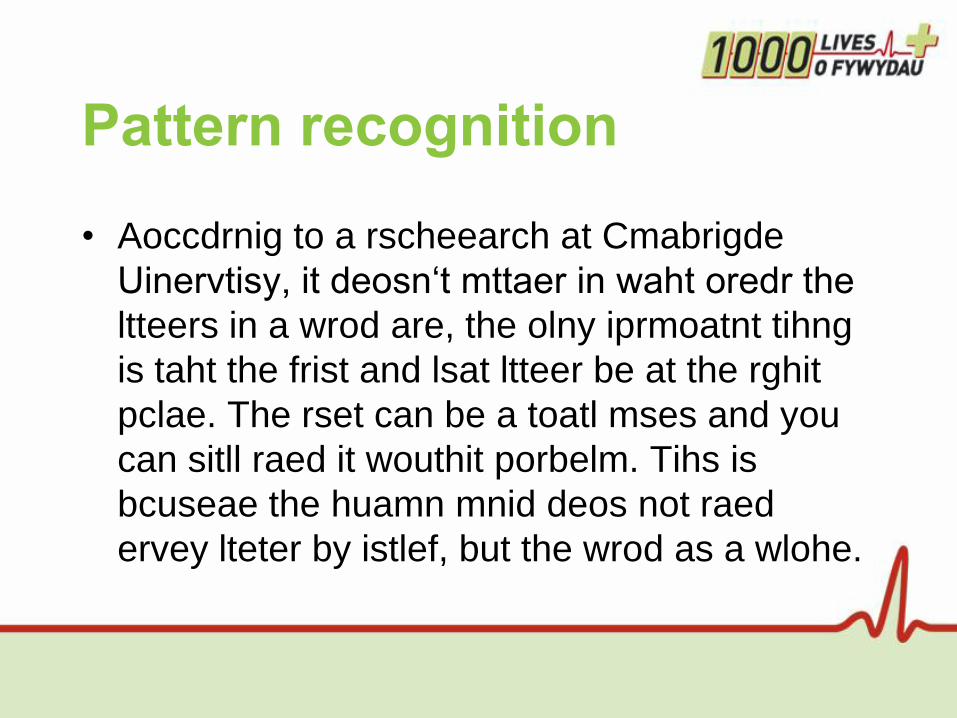
Pattern recognition
• Aoccdrnig to a rscheearch at Cmabrigde
Uinervtisy, it deosn‘t mttaer in waht oredr the
ltteers in a wrod are, the olny iprmoatnt tihng
is taht the frist and lsat ltteer be at the rghit
pclae. The rset can be a toatl mses and you
can sitll raed it wouthit porbelm. Tihs is
bcuseae the huamn mnid deos not raed
ervey lteter by istlef, but the wrod as a wlohe.
The Gap Between
Perception and
Practice
What We Think We Do
Vs.
What We Actually Do
Mitchell Levy,
Director, Surviving Sepsis
Campaign
• Human error is a natural consequence
of being human
Power of memory
Working Together
Working Together
Who are the best multi-taskers?
Working Together
Working Together
Working Together
Human cognition
Working Together
..and the result is..
Working Together
Stress – how full is your bucket?
Working Together
TOP TIPS
Beware
• Hungry
• Anxious / angry
• Late
• Tired
Working Together
It is important not to blame individuals for what went wrong but to understand why, what they did at the time, made sense to
them.
‘Just Culture’ - Dekker - 2007
High risk situations for
error
• Interruptions and distractions
• Tasks required out of normal sequence
• Unanticipated new tasks
• Multitasking.
Why Errors HappenFactors making error/violation more likely
• Fatigue
• Stress
• Illness
• Overload
• Inexperience
• Complacency.
Problem types
• Care Delivery Problem
– Direct provision of care, problem arises in
the process of care usually actions or
omissions by staff- Active Failures
• Service delivery problem
– Absence of guidance to enable actions to
take place- Latent Failures
The First Law of
Healthcare Improvement
“It is not bad people but bad systems that harm and kill our patients”
Source: Don Berwick, IHI (Boston)
Reliability
• Achieving reliability means doing the
right thing for every patient every time
Human Factors
• Making it easier to do the right thing
Human Factors
Approaches
• Make communications visible
• Decrease reliance on vigilance – error
proof
• Avoid reliance on memory - use prompts
• Simplify processes – SOP
• Use checklists
• Standardise
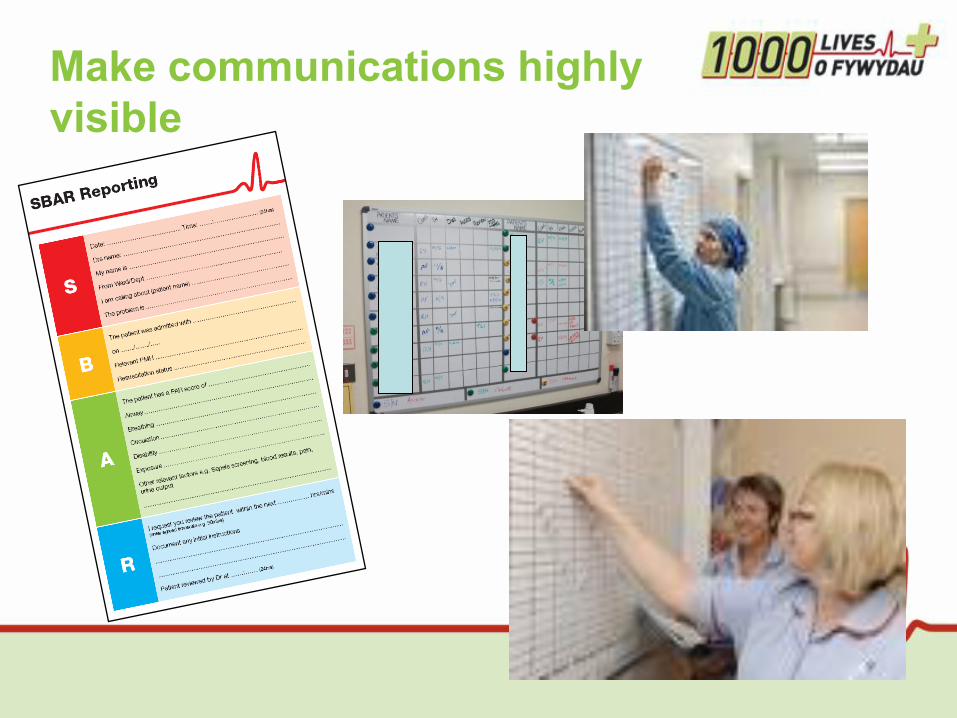
Make communications highly
visible
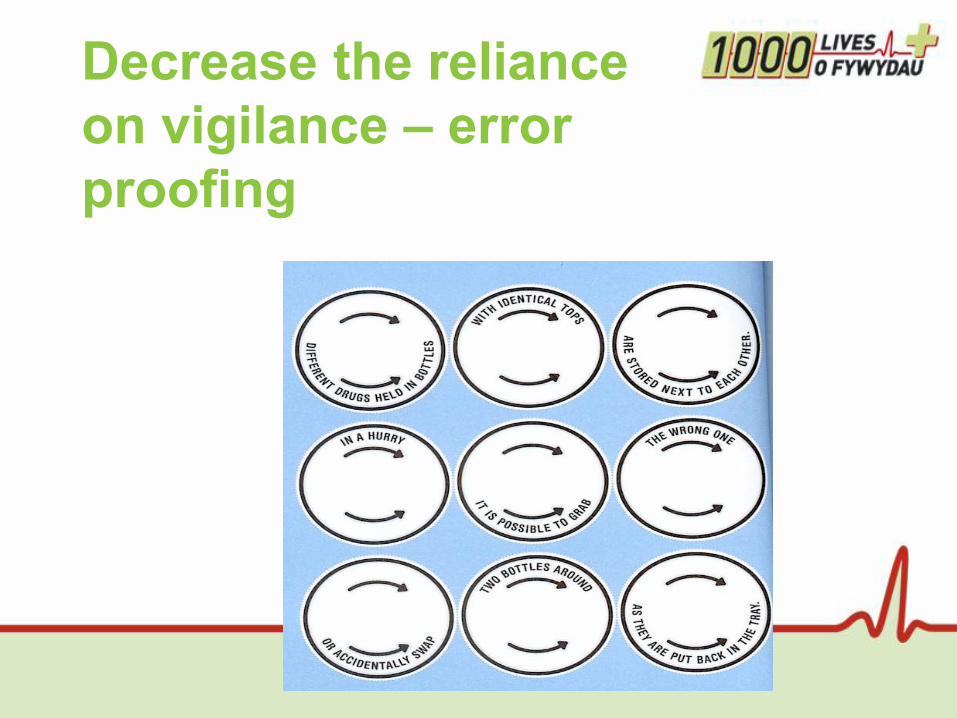
Decrease the reliance
on vigilance – error
proofing
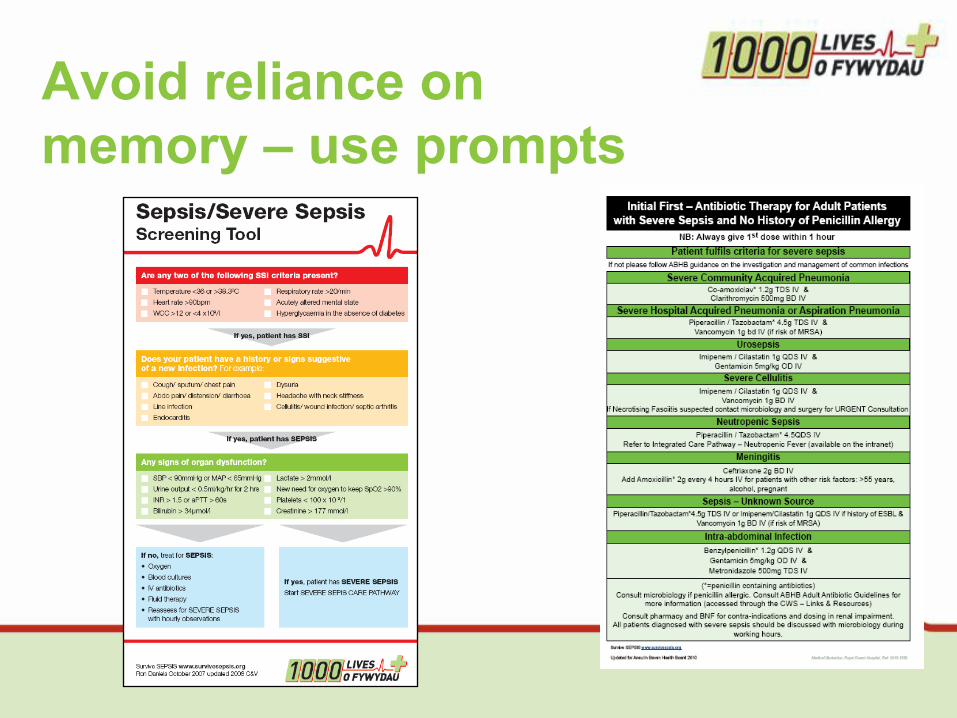
Avoid reliance on
memory – use prompts
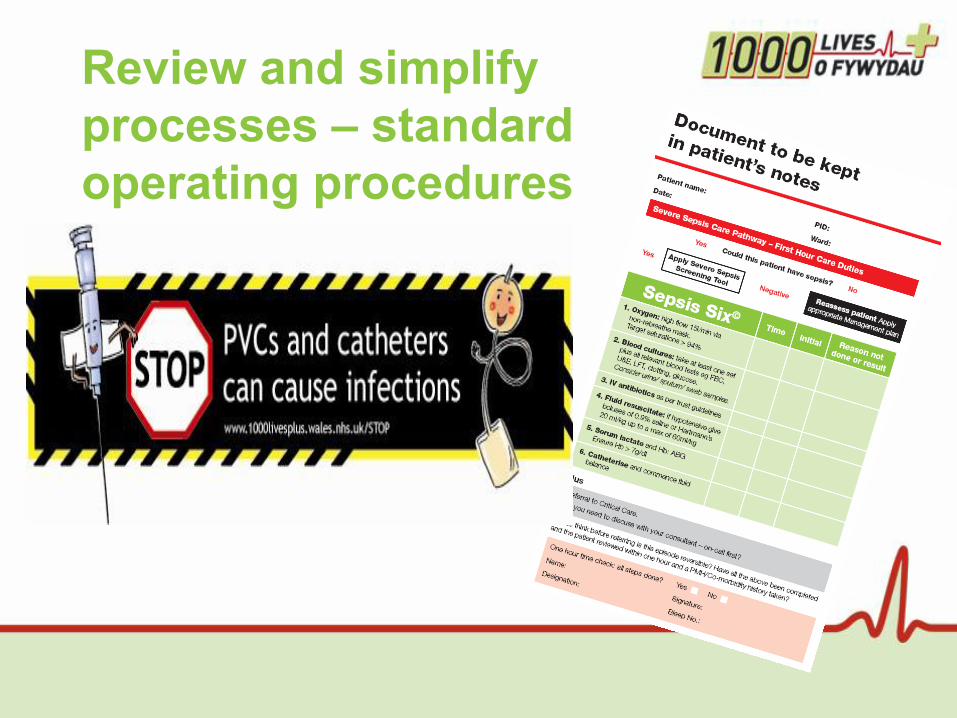
Review and simplify
processes – standard
operating procedures
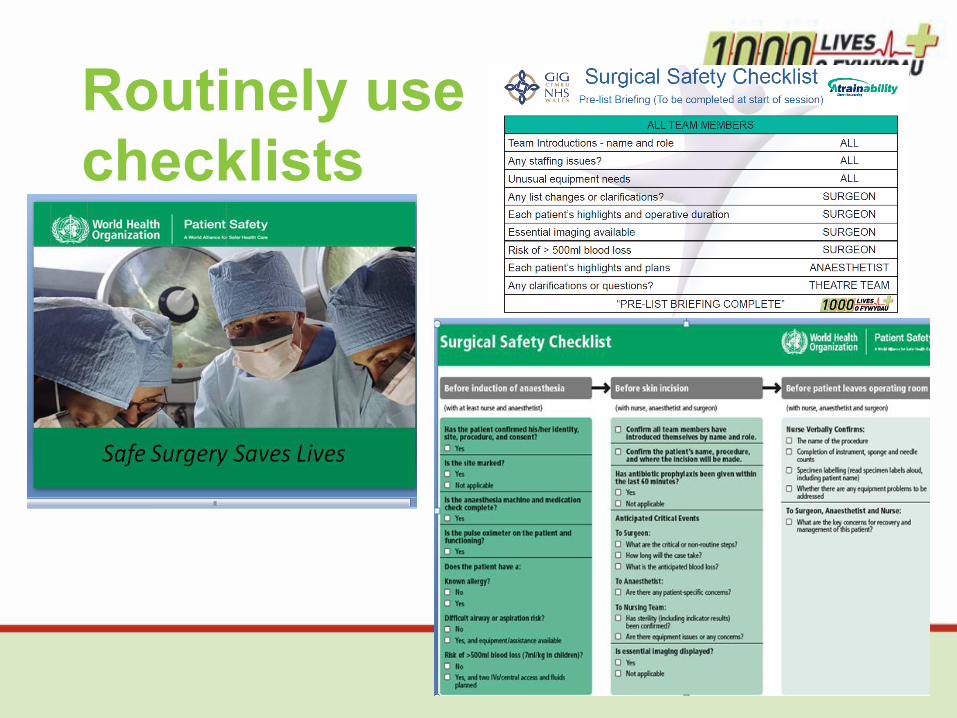
Routinely use
checklists

Standardise common
processes and procedures
NEWS card & iPhone App available
Summary
• It is not bad people but bad systems that cause harm and death
in healthcare – human error is inevitable
• Most error in healthcare is due to system rather than individual
failure
• Every system is perfectly designed to achieve the results that it
gets – use human factors thinking
• You cannot achieve reliable outcomes without first achieving
reliable processes
• You have 1 job with 2 roles
– Doing your job
– Improving your job
Recommended