Linköping University Medical Dissertations
No. 1241
Hepatic and Portal Vein Thrombosis - studies on epidemiology and risk factors
Rupesh Rajani
Division of Gastroenterology and Hepatology
Department of Clinical and Experimental Medicine
Linköping University, Sweden
2011
1

Hepatic and portal vein thrombosis - studies on epidemiology and risk factors.
Rupesh Rajani, 2011
Cover picture: Courtesy of Dr Anders Persson, CMIV, Linköping University.
The published articles have been reprinted with the permission of the copyright holders.
Printed in Sweden by LiU-Tryck, Linköping, Sweden, 2011
ISBN 978-91-7393-187-8
ISSN 0345-0082
2

Dedicated to my parents,
Live as if you were to die tomorrow.
Learn as if you were to live forever.
Mahatma Gandhi
3

4

Contents
CONTENTS
ABSTRACT .................................................................................................................... 1
POPULÄRVETENSKAPLIG SAMMANFATTNING .................................................. 1
LIST OF PAPERS ........................................................................................................... 3
ABBREVIATIONS ......................................................................................................... 5
INTRODUCTION ........................................................................................................... 7
Vascular disorders of the liver .................................................................................. 7 Budd-Chiari syndrome ............................................................................................. 9 Portal vein thrombosis ............................................................................................ 11 Thrombophilia ........................................................................................................ 13 Myeloproliferative disorders .................................................................................. 15
JAK2 mutations and haplotype ......................................................................... 16 Thrombosis in myeloproliferative disorders .................................................... 17
AIMS ............................................................................................................................. 19
METHODS .................................................................................................................... 21
Patients .................................................................................................................... 21
Paper I and II ................................................................................................... 21
Paper III and IV ............................................................................................... 22
Methods .................................................................................................................. 24
Data collection ................................................................................................. 24
Database ........................................................................................................... 24
Laboratory tests (Paper III and IV) ................................................................. 25
Statistics .................................................................................................................. 26
5

Contents
RESULTS AND DISCUSSION .................................................................................... 27
Budd-Chiari syndrome (BCS) ................................................................................ 27
Epidemiology .................................................................................................... 27
Clinical features ............................................................................................... 28
Risk factors ....................................................................................................... 29
Survival ............................................................................................................. 31
Portal vein thrombosis (PVT) ................................................................................. 36
Epidemiology .................................................................................................... 36
Clinical features ............................................................................................... 38
Risk factors ....................................................................................................... 40
Medical treatment and interventions ................................................................ 42
Survival ............................................................................................................. 44
Thrombophilic factor VIII in BCS and PVT .......................................................... 48 JAK 2 46/1 haplotype and V617F mutation in BCS and PVT ............................... 51 General discussion .................................................................................................. 54
CONCLUSIONS ........................................................................................................... 55
ACKNOWLEDGEMENTS .......................................................................................... 57
REFERENCES .............................................................................................................. 59
6

Abstract
1
ABSTRACT
Budd-Chiari syndrome (BCS) i.e. thrombosis in the hepatic veins and/or inferior vena cava, and
portal vein thrombosis (PVT) are rare disorders. Epidemiological data are scarce and previous
reports have been from highly specialised referral centres.
The aims of the thesis were: (i) to investigate the epidemiology, clinical features and sur-
vival of Swedish patients with BCS or PVT, and to (ii) determine common underlying risk fac-
tors i.e. thrombophilic factors and genetic markers of myeloproliferative disorders (MPD).
In the first two papers we retrospectively reviewed the medical records of all BCS (1986-
2003) and PVT (1995-2004) patients identified by searching the computerized patient registers
of 11 hospitals including all university hospitals and liver transplantation units. In the following
two papers we excluded patients with malignancy and included new cases diagnosed during the
years 2004-2009; blood samples were collected and compared with controls and other patient
groups.
A total of 43 patients with BCS were identified (median age 40 years, 24 women). The
mean age-standardised incidence and prevalence rates were 0.8 per million per year and 1.4 per
million inhabitants respectively. Two or more risk factors were present in 44%. The overall
transplantation-free survival at 1, 5 and 10 years was 47%, 28% and 17% respectively.
173 patients (median age 57 years, 93 men) with portal vein thrombosis were identified.
The incidence and prevalence rates were 0.7 per 100 000 per year and 3.7 per 100 000 inhabi-
tants, respectively. In the absence of cirrhosis and malignancy, being the most common risk
factors, the survival at 1 year and 5 years was 92% and 76%, respectively.
We observed an increased plasma level of the procoagulant factor VIII in BCS (mean 1.63
kIE/L), PVT without cirrhosis (1.87 kIE/L), PVT with cirrhosis (1.97 kIE/L), deep vein throm-
bosis (1.41 kIE/L) and cirrhosis patients alone (2.22 kIE/L), all p <0.001 compared to healthy
controls (1.04 kIE/L). Elevated factor VIII levels were found in 50% of BCS and in 85% of
PVT patients without previously identified prothrombotic risk factors.
The somatic JAK2 V617F-mutation, a marker of MPD, was present in 63% of BCS and
14% of PVT patients. The frequency of the germline JAK2 46/1 haplotype was significantly
higher in BCS (53%) and PVT (36%) patients compared to controls (27%) (p=0.02). However,
the enrichment was only observed in JAK2 V617F positive patients.
Conclusions: The incidence and prevalence rates of BCS in Sweden were calculated to be
0.8/million inhabitants per year and 1.4/million inhabitants, respectively. The rates of PVT were
higher; 0.7/100 000 inhabitants per year and 3.7/100 000 inhabitants, respectively. In BCS the
transplantation-free survival was poor, whereas in PVT the survival was variable and highly
dependent on the presence of underlying disease. Concurrent prothrombotic risk factors are
common in both disorders. High plasma levels of procoagulant factor VIII was observed in a
majority of idiopathic BCS and PVT. The prevalence of the somatic JAK2 V617F mutation was
high in our cohort and associated with the presence of a germline JAK2 46/1 haplotype.
7

Abstract
2
8

Sammanfattning
1
POPULÄRVETENSKAPLIG SAMMANFATTNING
Blodproppssjukdom (trombos) är vanligt förekommande i samhället och orsakar betydande sjuklighet och dödlighet. Levervenstrombos, även kallat Budd-Chiaris syndrom (BCS) och portavenstrombos (PVT) har på senare år kommit att upp-märksammats i ökande utsträckning tack vare förbättrad bilddiagnostik och till-tagande kunskap om förekomsten av olika biokemiska, delvis ärftliga rubbningar, vilka medför en ökad risk för blodproppsbildning. En grupp blodsjukdomar, som kännetecknas av ett ökat antal blodkroppar, s.k. myeloproliferativ sjukdom (MPD) har förknippats med blodproppar i levern men inte i andra organ. Såväl nationellt som internationellt har det funnits begränsad information om dessa ovanliga, men potentiellt livshotande tillstånd.
Våra studier syftade till att kartlägga förekomst, klinisk bild, bakomliggande riskfaktorer och långtidsprognos vid BCS och PVT i Sverige.
Patienterna identifierades genom sökning i datoriserade sluten- och öppen-vårdsregister på elva sjukhus, däribland alla universitetssjukhus inom ramen för Svensk Internmedicinsk Leverklubb (SILK), det nationella nätverket för studier av leversjukdomar.
I delstudie I beskriver vi detaljerat 43 BCS patienter (medianålder 40 år) identifierade under åren 1986-2003. Nyinsjuknandet (incidensen) beräknades till cirka 1 patient per miljon invånare och år. Förekomsten (prevalensen) var 1,5 per million och år. Under studietiden avled 19 patienter och ytterligare 18 patienter behövde genomgå en livräddande levertransplantation. Överlevnaden var sämre än den som rapporterats i en jämförbar undersökning genomförd på högspeciali-serade utländska sjukhus.
I delstudie II fann vi 173 PVT patienter (medianålder 57 år) under åren 1995-2004. Incidensen och prevalensen var högre; cirka 1 per 100 000 invånare och år respektive 4 per 100 000 invånare och år. Två eller fler bakomliggande faktorer identifierads i nästan hälften av fallen. Den vanligaste bakomliggande riskfaktorn var skrumplever (cirros), följt av cancer. Utan dessa var långtidspro-gnosen god. Endast en patient dog på grund av tarminfarkt till följd av PVT.
I de efterföljande studierna belyste vi faktorer av betydelse för uppkomsten av blodproppar. Sammanlagt togs blodprover på 110 patienter med BCS eller PVT utan samtidig cancer och resultaten jämfördes med kontrollgrupper.
I delstudie III kunde vi rapportera förhöjda nivåer av en blodproppsstimule-rande faktor VIII i blodet hos 21% av BCS och 54% av PVT patienterna. Faktor VIII-nivåerna var tydligt förhöjda jämfört med hos friska individer samt med en
9

Sammanfattning
2
grupp patienter med djup ventrombos. De högsta värdena uppmättes hos patien-ter med skrumplever. Mätning av faktor VIII kan komma att utgöra en viktig analys vid utredning av BCS och PVT.
I delstudie IV undersökte vi nya markörer för MPD och kunde visa att en förvärvad genförändring (JAK2V617F mutation) förekom i hög omfattning hos våra svenska BCS- (63%) och PVT-patienter (14%) samt att genförändringen var associerad till bärarskap av en nedärvd genvariant (JAK2 46/1 haplotyp).
Sammanfattningsvis har vi för första gången kunnat ta fram tillförlitliga epi-demiologiska data för dessa ovanliga tillstånd i en västerländsk population. Nyin-sjuknandet för BCS var cirka 1 per miljon invånare och år och för PVT 1 per 100 000 invånare och år. Långtidsprognosen för BCS var dålig, framförallt utan levertransplantation. Möjligen kan avsaknaden av ett nationellt center för utred-ning och behandling av BCS ha påverkat utfallet. För PVT var prognosen god om man inte samtidigt hade skrumplever eller cancer.
Två eller flera samtidiga riskfaktorer är inte ovanligt. Faktor VIII-nivåerna var bestående förhöjda vid BCS och PVT. Fortsatta studier behövs för att under-söka om denna analys kan vara av värde för att förutspå trombosuppkomst hos leversjuka patienter som inte haft trombos och för att följa behandlingseffekter. Förekomsten av JAK2V617F-mutation i en svensk kohort var så hög som 63% vid BCS och 14% vid PVT utan bakomliggande cancer. Analysen kan vara till hjälp att hitta atypiska och tidiga fall av MPD samt vara ett stöd för beslut om utökad utredning och tidig behandling. Den bör rutinmässigt ingå i utredningen av dessa ovanliga patienter.
10

List of Papers
3
LIST OF PAPERS
I. Budd-Chiari syndrome in Sweden: epidemiology, clinical characteristics and survival - an 18-year experience.
Rajani R, Melin T, Björnsson E, Broomé U, Sangfelt P, Danielsson A, Gustavsson A, Grip O, Svensson H, Lööf L, Wallerstedt S, Almer SH.
Liver Int. 2009 Feb;29(2):253-9.
II. The epidemiology and clinical features of portal vein thrombosis: a multicentre study
Rajani R, Björnsson E, Bergquist A, Danielsson A, Gustavsson A, Grip O, Melin T, Sangfelt P, Wallerstedt S, Almer S.
Aliment Pharmacol Ther. 2010 Nov;32(9):1154-62.
III. Increased Factor VIII Activity in Portal Vein Thrombosis and Budd-Chiari Syndrome
Rajani R, Jennersjö C, Bergquist A, Melin T, Friis-Liby I, Kapraali M, Lindahl TL, Kechagias S, Almer S.
Submitted
IV. High prevalence of the germline JAK2 46/1 haplotype and V617F-
mutation in Swedish patients with Budd-Chiari syndrome and
Portal Vein Thrombosis
Rajani R, Haglund S, Bergquist A, Melin T, Friis-Liby I, Verbaan H, Kapraali M, Lindahl TL, Almer S.
In manuscript
11

List of Papers
4
12

Abbreviations
5
ABBREVIATIONS
ALT Alanine aminotransferase
APC Activated protein C
BCS Budd-Chiari syndrome
CI Confidence interval
C-PVT Non-malignant cirrhotic portal vein thrombosis
CRP C-reactive protein
CRF Case record form
CT Computerised tomography
df Degrees of freedom
DVT Deep vein thrombosis
EDTA Ethylenediaminetetraacetic acid
EN-Vie The European Network for Vascular Disorders of the Liver study group
hs-CRP High-sensitivity C-reactive protein
ICD International classification of diseases
INR International normalised ratio
IVC Inferior vena cava
JAK2 Janus kinase 2
LMWH Low-molecular-weight heparin
MELD Model for End-stage liver disease
MPD Myeloproliferative disorders
M-PVT Malignant portal vein thrombosis
NA Not applicable
N-PVT Non-cirrhotic non-malignant portal vein thrombosis
NS Not significant
OR Odds ratio
PVT Portal vein thrombosis
SD Standard deviation
SILK Swedish Internal Medicine Liver Club
SNP Single-nucleotide polymorphism
SPSS Statistical Package for Social Sciences
vs Versus
13

Abbreviations
6
VTE Venous thromboembolism
TIPS Transjugular intrahepatic portosystemic shunt
ULN Upper limit of normal value
WBC White blood cells
14

Introduction
7
INTRODUCTION
The liver, weighs on an average 1.5 kg and is the second largest organ in the body. It is a vital organ with various crucial functions such as protein synthesis, detoxification, bile secretion, and is involved in important metabolic pathways. Traditionally, the liver is divided into four anatomical lobes: right, left, caudate and quadrate. In clinical practice the subdivision into eight segments, each hav-ing its own vascular flow and biliary drainage (developed by the French surgeon Claude Couinaud), is frequently used (Wanless 2002).
Vascular disorders of the liver In recent years, there has been an increased awareness of vascular liver disorders due to the improvement and increased availability of imaging modalities, as well as better knowledge of prothrombotic factors.
Figure 1. The vascular anatomy of the liver.
Source: Illustration Typoform, from Gastroenteroloi och hepatologi, Hultcrantz R et al, 2011, Liber, Stockholm.
The liver has a unique dual blood supply and therefore infarctions are rare. The portal vein (Figure 1), which is formed by the merger of the superior mesenteric and splenic veins delivers 75% of the blood. It contains nutrient rich albeit less oxygenated blood drained from the gastrointestinal tract. The remaining 25% is provided by the hepatic artery which arises from the celiac artery and supplies 30-60% of the oxygen consumed. The blood volume corresponds to 20% of the
15

Introduction
8
cardiac output. If required, the liver can extract up to 95% of the oxygen deliv-ered (Moller et al. 2009).
The liver is drained via three main hepatic veins (Figure 1). The caudate lobe veins are drained directly into the inferior vena cava and less vulnerable to occlu-sion. Hence, caudate lobe enlargement due to hyperplasia is commonly seen when thrombosis of the main hepatic veins (e.g Budd-Chiari syndrome) occurs (Wanless 2002).
Blood flow from the portal vein is primarily intended for the hepatic paren-chyma, whereas hepatic artery supply is crucial for the biliary tree, and to a lesser extent hepatic mesenchyma and blood vessels (Wanless 2002).
The microanatomy of the blood supply is also unique with sinusoids, that unlike systemic capillaries are fenestrated and are low pressure channels. Sinu-soids bridge the gap between terminal portal veins and hepatic venules. The he-patic arterial buffer response ensures that a relatively constant sinusoidal pres-sure is maintained; i.e. when portal flow decreases, hepatic artery flow increases and vice versa (Wanless 2002).
Most vascular liver disorders are rare, and usually due to occlusion or oblit-eration of the vessels involved (Table 1). The lesion can be pre-hepatic (e.g. por-tal vein thrombosis) or post-hepatic (e.g. cardiac hepatopathy). The hepatic le-sions can be pre-sinusoidal (e.g. obliterative portal venopathy), sinusoidal (e.g. sinusoidal obstruction syndrome) or post-sinusoidal (e.g. Budd-Chiari syn-drome).
The term splanchnic vein thrombosis has been used to denote a combined patient group with Budd-Chiari Syndrome, portal-, mesenteric- and/or splenic vein thrombosis (Francoz et al. 2005; Amitrano et al. 2007).
Table 1. Vascular diorders of the liver
Portal vein thrombosis
Hepatic artery thrombosis or aneurysm
Ischemic cholangiopathy
Obliterative portal venopathy
Sinusoidal obstruction syndrome (Veno-occlusive disease)
Budd-Chiari syndrome
Congenital vascular malformations
Radiation-induced liver disease
Peliosis hepatis
Cardiac hepatopathy
Hypoxic hepatitis (Ischemic hepatitis)
16

Introduction
9
Budd-Chiari syndrome Budd-Chiari syndrome (BCS), is named after the British physician George Budd (1808 − 1882) and the Austrian pathologist Hans Chiari (1851 − 1916), who first described clinicopathological features of this disorder (Budd 1845; Chiari 1899).
According to current international consensus, BCS is a hepatic venous out-flow obstruction of any cause, and at any level from the small hepatic veins to the entire length of the hepatic and supra-hepatic inferior vena cava. Although symptoms and signs can be similar, an outflow obstruction due to cardiac disease or sinusoidal obstruction syndrome are excluded from the definition (Janssen et al. 2003; DeLeve et al. 2009; de Franchis 2010).
BCS is classified as primary if the obstruction is due to an intra-luminal le-sion e.g thrombosis, web or endophlebitis; secondary, if the lesion is due to ex-tra-luminal compression or invasion, e.g. cysts, abscess or tumor (Janssen et al. 2003). The main aetiological factor in primary BCS is a myeloproliferative dis-order present in 40-50% (DeLeve et al. 2009). Other common causes are inher-ited or acquired thrombophilia.
Due to the rarity of the disorder incidence and prevalence data have been sparse (Almdal and Sorensen 1991; Okuda et al. 1995; Valla 2004). There are reports indicating geographic variations between Eastern and Western countries with regards to occurrence i.e. being exceptionally high in Nepal (Shrestha et al. 1996); gender e.g. predominance of men in the East (Valla 2009); localisation of occlusion i.e. isolated hepatic vein occlusions dominating in the West; and causes e.g. more thombotic occlusions in the West compared to membranous-webs in the East (Valla 2004). Such membranous-webs are considered to be fibrotic rem-nants of a previous thrombotic occlusion (Okuda 2002).
The pathophysiological mechanisms involved are sinusoidal congestion, fol-lowed by ischemia, centrilobular necrosis and fibrosis causing portal hyperten-sion. In severe cases intra- and extra-hepatic portal vein thrombosis can occur (Tanaka and Wanless 1998; Murad et al. 2006). Gradually, large regenerative nodules and cirrhosis may develop (Tanaka and Wanless 1998). The cumulative incidence of hepatocellular cancer was recently reported to be 4% and associated with occlusion of the inferior vena cava (Moucari et al. 2008).
The clinical presentation is variable, ranging from asymptomatic patients to those with fulminant hepatic failure (DeLeve et al. 2009). Asymptomatic cases have been reported in up to 20% and were associated with the presence of large intra-hepatic collaterals and at least one patent main hepatic vein (Hadengue et al. 1994). The classical triad abdominal pain, ascites and hepatomegaly is present in a majority of patients (Panis et al. 1994; Murad et al. 2004). Even if the clini-cal presentation has been divided into acute, sub-acute, chronic or severe forms, established criteria for such characterisation are lacking (Janssen et al. 2003).
17

Introduction
10
The diagnosis of BCS is based on imaging findings demonstrating signs of out-flow obstruction (Janssen et al. 2003; DeLeve et al. 2009). Supporting features are large hepatic collaterals, spider web appearance, caudate lobe enlargement compressing the vena cava inferior, heterogeneous contrast enhancement, ascites and splenomegaly (Brancatelli et al. 2007). With the constantly improving non-invasive imaging techniques, liver biopsy or venograhpy, are nowadays rarely needed. Current guidelines recommends doppler ultrasound in experienced hands as a first hand approach, alternatively computerised tomography or magnetic resonance imaging (DeLeve et al. 2009).
Figure 2. Budd-Chiari syndrome. CT scan demonstrating hepatomegaly, heterogeneous contrast distribution (bold arrow) with enhancement of the left lobe due to outflow ob-struction (thin arrow).
Courtesy of the Department of Radiology, University hospital, Linköping.
Randomised controlled trials of comparing treatment options in BCS have not been performed. Based on local expertise and experience, favourable outcome has been suggested for anticoagulation theapy (Zeitoun et al. 1999), thrombolysis (Sharma et al. 2004), angioplasty (Zhang et al. 2003; Eapen et al. 2006), transjugular intrahepatic portosystemic shunt (TIPS) (Perello et al. 2002; Hernandez-Guerra et al. 2004; Rossle et al. 2004; Garcia-Pagan et al. 2008), sur-gical shunts (Orloff et al. 2000) and liver transplantation (Mentha et al. 2006; Segev et al. 2007). In recent years, guidelines based on expert opinion and previ-ous studies (Murad et al. 2004; Plessier et al. 2006) have emerged facilitating the management of this disorder (de Franchis 2005; DeLeve et al. 2009; de Franchis 2010).
Advances in management have indicated improvement of outcome in BCS with 5-year survival rates approaching 90% in highly specialised referral centres
18

Introduction
11
(Plessier et al. 2006). Based on clinical and laboratory findings at diagnosis, the Clichy (Zeitoun et al. 1999; Langlet et al. 2003) and the Rotterdam prognostic scores (Murad et al. 2004) have been developed to identify patients with poor prognosis, as has the more recently BCS-TIPS score (Garcia-Pagan et al. 2008). The Rotterdam score has been reported to have a better accuracy than scores used in patients with cirrhosis i.e. Child-Pugh and model for end-stage liver disease (MELD) score (Murad et al. 2007). However, these scores are not accurate enough to be used in clinical practice and should be limited to study purposes only (Rautou et al. 2009).
Portal vein thrombosis Portal vein thrombosis (PVT) was first described in the literature by Balfour and Stewart (Balfour and Stewart 1869). PVT is becoming more recognised as a clinical entity with the increasing use of non-invasive imaging in general, and with the recommendations for hepatocellular cancer surveillance in cirrhotic pa-tients in particular.
PVT, also referred to as extra-hepatic portal vein obstruction, is defined as a occlusion of the extra-hepatic portal vein with or without involvement of the in-tra-hepatic branches, superior mesenteric vein or splenic vein (Sarin et al. 2006; de Franchis 2010).
Recent data on the incidence and prevalence of PVT in the general popula-tion are lacking. Some attempts have been made using autopsy or inpatient hospi-tal registers from the 1970s and early 1980s with varied results (Okuda et al. 1985; Almdal and Sorensen 1991; Ogren et al. 2006). PVT has been suggested to be more common in developing countries where it accounts for 70% and 30% of paediatric and adult non-cirrhotic portal hypertension patients, respectively (Sarin et al. 2006; Poddar et al. 2008; DeLeve et al. 2009).
The aetiology of PVT is diverse (Janssen et al. 2001; DeLeve et al. 2009). Often a combination of local and systemic factors are present (Denninger et al. 2000; Fisher et al. 2000; Janssen et al. 2000; Amitrano et al. 2004; Mangia et al. 2005; Primignani et al. 2005) (Janssen et al. 2001; Primignani et al. 2006; Kiladjian et al. 2008). Local risk factors, e.g. liver cirrhosis, hepatobiliary malig-nancy, abdominal inflammation, infection or surgical intervention are the most common predisposing factors (Janssen et al. 2001; DeLeve et al. 2009). Com-mon systemic factors are myeloproliferative disorders and acquired or inherited thrombophilia (discussed in the next chapters). Taken together, the presence of risk factors and their relative pathophysiological contributions support the classi-cal model for clot formation i.e. Virchow´s triad including impaired blood flow, changes in blood composition resulting in hypercoaguability and endothelial in-jury (Virchow 1856; Dahlback 2008).
19

Introduction
12
↓↓
In patients with liver cirrhosis, the prevalence of PVT has been reported to lie between 0.6% and 44% with an increasing frequency in decompensated disease and/or concomitant hepatocellular cancer (Okuda et al. 1985; Pirisi et al. 1998; Amitrano et al. 2004). One study has indicated that PVT is more common in al-cohol or virus-induced cirrhosis than in cirrhosis of other causes (Nonami et al. 1992). In more recent ultrasound-based publications, the prevalence was 10% to 25% in cirrhotic patients without hepatocellular cancer (Tsochatzis et al. 2006). Compared to the number of studies on the prevalence of PVT in cirrhotics, only two studies have reported incidence rates; being 7% in patients listed for trans-plantation (Francoz et al. 2005), and 16% during a 12-month prospective follow-up (Zocco et al. 2009).
Although, the reduction in hepatic blood supply will instantly be compen-sated by hepatic artery dilatation, i.e. arterial buffer response, portal hypertension will remain (Henderson et al. 1992). Gradually, porto-portal and porto-systemic collaterals trying to bypass the thrombosis will develop i.e. cavernous transfor-mation or a cavernoma (Ohnishi et al. 1984; Valla 2009). If the thrombosis pro-gresses upstream into the mesenteric vein and its arches, there is a risk of intesti-nal infarction associated with a high mortality rate (Valla 2009).
PVT is classified as acute in the presence of a recent thrombus on imaging and absence of collateral formations. Signs such as abdominal pain and fever are present, albeit asymptomatic patients are not uncommon (DeLeve et al. 2009; de Franchis 2010). The manifestations of chronic PVT are variceal bleeding and an enlarged spleen. Cholangiopathy secondary to compression of the bile ducts by a cavernoma is common but rarely gives rise to symptoms (Condat et al. 2003; Dhiman et al. 2007). Cirrhotic patients with PVT may be asymptomatic in up to 43% (Amitrano et al. 2004) or present with life threatening complications related to aggravated portal hypertension (Tsochatzis et al. 2010). PVT may be the first manifestation of hepatocellular cancer which should be ruled out.
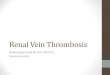
Figure 3. Portal vein thrombosis. CT scan of the abdomen with contrast enhancement showing filling defects consistent with acute portal vein thrombosis and mesenteric vein thrombosis.
Courtesy of the Department of Radiology, University hospital, Linköping.
20

Introduction
13
In the absence of randomised controlled trials the optimal management of PVT is not known. Consensus on treatment with anticoagulants, based on expert opinion and retrospective studies, exists for acute but not for chronic or cirrhotic PVT. (Chawla et al. 2009; DeLeve et al. 2009; de Franchis 2010).
Survival is determined by the underlying disease and age (Janssen et al. 2001). There is an increased risk for re-thrombosis in splanchnic or other sites in patients with prothrombotic factors (Condat et al. 2001; Amitrano et al. 2007).
Thrombophilia The key components of haemostasis are mediated by platelet protein interactions e.g. von Willebrand factor (primary haemostasis) and by blood coagulation e.g. a precise and balanced generation of the key enzyme thrombin (secondary haemo-stasis). During normal conditions the natural anticoagulant proteins (e.g. anti-thrombin, protein C and S) prevail over procoagulants (e.g. factors V and VIII) (Dahlback 2005) (Figure 4).
Figure 4. Factors in blood coagulation
Source: Wikimedia Commons. http://commons.wikimedia.org
21

Introduction
14
The designation thrombophilia refers to genetic or acquired disturbances of the normal balance between the pro- and anticoagulants as well as in fibrinolysis, resulting in venous thromboembolism (VTE).
Over the last decades there has been an increased expansion in the knowl-edge of thombophilic factors in common VTE such as deep vein thrombosis (DVT) (Dahlback 2008).
More recently, new insights have also emerged in the occurrence of inherited and acquired thrombophilia in BCS and predominantly PVT without cirrhosis and malignancy as reviewed by DeLeve et al. (DeLeve et al. 2009). The relative frequencies of specific factors in these often retrospective series differ due to dif-ferent diagnostic criteria, referral patterns, ethnic groups and geographical re-gions.
The prevalence of the factor V Leiden mutation, which causes activated pro-tein C (APC) resistance, has been found in the ranges of 6% to 32% in BCS and PVT patients (DeLeve et al. 2009). In one series, this mutation was more com-mon in BCS patients with occlusion of the IVC (73%) compared to hepatic vein thrombosis (23%), and associated with other concomitant risk factors in 70% of cases (Deltenre et al. 2001). In the general population the range varies from 0% to 15% (Dahlback 2008). Heterozygotes and homozygotes have an approxi-mately 5- and 50-fold increased risk of VTE, respectively.
The prothrombin (factor II) G20210A mutation, associated with excessive generation of prothrombin and thus causing a hypocoaguable state, is present in 5-7% of BCS cases as compared to 14-40% in PVT (DeLeve et al. 2009). In the general population the mutation is carried by 1-2% in northern countries com-pared to 2-4% in southern Europe, and causes a 3 to 4-fold increased risk of VTE (Dahlback 2008).
A recent meta-analysis showed a stronger association of PVT with the prothrombin gene mutation (OR 4.5 95% CI 3.1-6.5) as compared to the factor V Leiden mutation (OR 1.9 (95% CI 1.3-2.9) (Dentali et al. 2008).
Inherited deficiencies of protein C, S and antithrombin are more difficult to diagnose in these disorders as a specific mutation analyses are not available. Since most coagulation factors are produced by the liver, low values measured, can be secondary to the impaired liver function in BCS and PVT. Family history and calculation of ratios in relation to other vitamin K dependant factors have been adopted in case-control studies, however, with disparate results (Janssen et al. 2000; Primignani et al. 2005).
Factor VIII is a procoagulant protein synthesized in the liver and in the vas-cular endothelium and involved in thrombin generation. In plasma, factor VIII circulates bound to the high molecular weight von Willebrand factor and throm-bin activation results in the liberation of an activated form (Dahlback 2005). In-creased levels have been reported in 25% of patients with DVT (Koster et al.
22

Introduction
15
1995) and is considered to be an independent risk factor both for single and re-current thrombotic events (Kraaijenhagen et al. 2000). In recent studies increased plasma concentrations of factor VIII have been found in patients with cirrhosis (Hollestelle et al. 2004; Tripodi et al. 2009), attributable to a decreased clearance from the circulation (Hollestelle et al. 2004). These findings are accompanied by decreased levels of the naturally occurring anticoagulants - protein C and anti-thrombin, due to impaired liver synthesis (Tripodi et al. 2009). Thus, an in-creased risk of VTE in patients with chronic liver disease (Sogaard et al. 2009) has been proposed to be caused by an imbalance in procoagulant and anticoagu-lant activity (Tripodi et al. 2009).
Alterations in the fibrinolytic system have been reported in acute and chronic liver disease (Lisman and Leebeek 2007). Recently, impaired fibrinolysis by means of genetic variations in the thrombin-activatable fibrinolysis inhibitor (TAFI) was found to be associated with higher risk for PVT or BCS combined (de Bruijne et al. 2007) but not in isolated BCS (Hoekstra et al. 2010). In the lat-ter study, plasminogen activator inhibitor 1 (PAI-1) was significantly higher and TAFI and plasmin inhibitor levels were lower than in controls (Hoekstra et al. 2010).
Myeloproliferative disorders Myeloproliferative disorders (MPD), in recent nomenclature referred to as mye-loproliferative neoplasms (Vardiman et al. 2009), are a group of clonal stem cell disorders. Clinically they are characterised by an over-production of one or more mature blood cells, overlapping features and a variable tendency to develop acute myeloid leukaemia. The annual incidence is 1-3 per 100 000 inhabitants with a peak at 70 years of age (Johansson et al. 2004).
Polycythemia vera, essential thrombocythemia, primary myelofibrosis and chronic myeloid leukemia are the main entities. Less common are systemic mas-tocytosis, chronic eosinophilic leukaemia, chronic neutrophilic leukaemia and unclassifiable types (Vardiman et al. 2009).
The key features are an increased red-cell mass in polycythemia vera, high platelet count in essential thrombocythemia, bone marrow fibrosis in primary myelofibrosis and increased number of granulocytes in chronic myeloid leukae-mia. Splenomegaly is common in these disorders due to extramedullary hemato-poiesis (Campbell and Green 2006).
Arterial and venous thrombotic complications are the main causes of mor-bidity and mortality, although, in some patients haemorrhage may also occur (Elliott and Tefferi 2005). Over time a minority of polycythemia vera and essen-tial thrombocythemia patients develop progressive disease such as transformation to myelofibrosis or acute myeloid leukaemia (Campbell and Green 2006). Aspi-
23

Introduction
16
rin and cytoreductive therapies are recommended since untreated patients have a poor prognosis (Nordic MPD study group 2009).
At a molecular level, MPD are characterised by altered tyrosine kinase sig-nalling due to chromosomal rearrangements or localised mutations. For instance, in chronic myeloid leukaemia a reciprocal translocation between chromosome 9 and 22, denoted the Philadelphia chromosome, causes a BCR-ABL1 fusion gene (Campbell and Green 2006). This oncogene increases the tyrosine kinase activity and is associated with an autonomic clonal cell expansion. (Baccarani et al. 2009).
In Philadelphia chromosome negative MPD, i.e. polycythemia vera, essential thrombocythemia and primary myelofibrosis, mutations in Janus kinase 2 (JAK2), a cytoplasmic tyrosine kinase, are predominantly involved in the patho-genesis.
JAK2 mutations and haplotype
JAK2 is important in relaying signalling between activated cytokine receptors, such as the erythropoietin receptor, and intracellular proliferation mechanisms. In 2005, five groups reported the landmark finding of an acquired point mutation, 1849G>T in exon 14 of the JAK2 gene on chromosome 9, in the majority of pa-tients with Philadelphia negative MPD (Baxter et al. 2005; James et al. 2005; Kralovics et al. 2005; Levine et al. 2005; Zhao et al. 2005). The G1849T substi-tution results in a valine to phenylalanine change at position 617 (V617F) of the molecule, resulting in a cytokine-independent activation, uncontrolled down-stream signalling, and eventually to unregulated cell proliferation. In the pioneer-ing studies above, JAK2 V617F was found in 90-95% of polycythemia vera cases, and in 50%-60% of patients with essential thrombocythemia or primary myelofibrosis. As a consequence, JAK2 mutation status is now included in the World Health Organization diagnostic algorithm of MPD (Vardiman et al. 2009)
Since the discovery, an increasing number of other genetic events responsi-ble for MPD pathogenesis have been uncovered (Vardiman et al. 2009) (Abdel-Wahab 2011). These include a range of somatic mutations in JAK2 exon 12 (Scott et al. 2007) and in the thrombopoietin receptor, MPL, identified in 5% or less of MPD patients (Pardanani et al. 2006).
A Swedish population-based study has found a 5 to 7-fold increased risk of MPD among first-degree relatives supporting the hypothesis of germline suscep-tibility genes which predispose to MPD development (Landgren et al. 2008). Re-cently, three independent groups reported that individuals carrying a germline haplotype block, denoted 46/1 and including JAK2 itself, had an increased risk of acquiring the somatic JAK2 V617F mutation (Jones et al. 2009; Kilpivaara et al. 2009; Olcaydu et al. 2009). The likelihood of developing MPD was also in-creased 3 to 4-fold compared to matched controls.
24

Introduction
17
Further studies have reported an association between JAK2 46/1 and V617F negative MPD (Jones et al. 2009; Andrikovics et al. 2010; Pardanani et al. 2010; Tefferi et al. 2010).
Subsequently, another group reported in a letter that the JAK2 46/1 haplo-type tagged by the single-nucleotide polymorphism (SNP) rs12343867 CC geno-type frequently occurs in Italian patients with splanchnic venous thrombosis (e.g. BCS or PVT) without the JAK2 V617F mutation (Colaizzo et al. 2010).
The mechanism by which a germline genetic variant in the 46/1 haplotype block could result in increased risk of developing the JAK2 V617F mutation and clinical MPD is not known.
Thrombosis in myeloproliferative disorders
The incidence of thrombosis in MPD has been difficult to establish. Neverthe-less, a thrombotic event is the initial presentation in up to 39% of Philadelphia negative MPD patients and the main cause of mortality (Austin and Lambert 2008). The risk of rethrombosis is estimated to be 7.6% per patient-year (De Stefano et al. 2008). Established risk factors for thrombosis in MPD are age over 60 years, hematocrit over 0.50 and a previous thrombotic event: Concomitant thrombophilia and conventional cardiovascular risk factors are controversial as risk factors, and there are some indications that activated leukocytes and JAK2 V617F status could be potential novel risk factors to consider in MPD (Austin and Lambert 2008).
BCS or PVT are unexpectedly frequent presenting features of MPD, particu-larly in young patients for which the reason is unknown (Elliott and Tefferi 2005). However, a recent brief report demonstrated JAK2 V617F mutation in endothelial cells lining the hepatic venules; shedding new light in the pathogene-sis as being a local predisposing factor (Sozer et al. 2009).
Using previous diagnostic criteria, the classical features of MPD could be masked in BCS or PVT by consequences of portal hypertension, e.g. splenomegaly, haemodilution and variceal bleeding (Chait et al. 2005). In an early series by Valla et al., latent MPD was demonstrated by means endogenous erythroid colony formation (EEC) in 16/20 patients of which only two had overt signs of MPD (Valla et al. 1985). However, very few centres have the capability to perform an EEC assessment.
In this sense, the JAK2 mutation analysis has dramatically facilitated the early detection of latent and overt MPD in BCS and PVT patients. In a recent meta-analysis the mean prevalence of JAK2 mutation was calculated to be 32.7% (95% CI 25.5%-35.9%) in BCS and PVT patients combined (Dentali et al. 2009). The mean prevalence of JAK2 mutation in other VTE patients was low, ranging from 0.88% to 2.57% (Dentali et al. 2009).
25

Aims
18
26

Aims
19
AIMS
The aims of the thesis were:
To calculate the incidence, prevalence and survival rates of Swedish patients with BCS and PVT, and to describe the clinical features (Paper I and II).
To investigate procoagulant factor VIII and the presence of other acquired or he-reditary prothrombotic risk factors in primary BCS and non-malignant PVT and to compare to patients with deep venous thrombosis, cirrhotic patients and healthy controls (Paper III).
To determine the distribution of a germline (inherited) JAK 2 46/1 haplotype in primary BCS and non-malignant PVT compared to population controls, and to relate this haplotype to the presence of the somatic (acquired) JAK2 V617F mu-tation, a sensitive marker for myeloproliferative disorders (Paper IV).
27

Aims
20
28

Methods
21
METHODS
Patients These studies were retrospective and performed in collaboration with the Swed-ish Internal Medicine Liver Club (SILK), consisting of hepatologists from all university hospitals in Sweden.
Paper I and II
We searched the computerised patient registers of eleven hospitals, comprising all nine university hospitals, including the liver transplantation units in Sweden. The background population of these centres was 4.4 million, which constitutes approximately half of the Swedish population.
In Paper I, consecutive patients during the full calendar years 1986 – 2003 registered with the ICD-9 (453A, 453C and 453W) or ICD-10 (I82.0, I82.2 and I82.8) diagnosis codes suggestive of BCS were identified. Patients with an he-patic outflow obstruction at any level from the small hepatic veins to the entire length of supra hepatic inferior vena cava (Janssen et al. 2003) visualised at im-aging, were included (n=43).
In Paper II, consecutive patients between January 1995 and October 2004 registered with the ICD-9 (452 and 572B) or ICD-10 (I81, and K75.1) diagnosis codes suggestive of PVT were identified. All patients with a partial or complete thrombotic obstruction of the portal vein visualised at imaging, were included (n=173).
Epidemiology
Patient care during the study period was almost exclusively public and popula-tion based. The referral patterns were based on geographic grounds rather than on socio-economic factors. The inpatient register contains individual-based informa-tion on a regional level since 1964 and on a nationwide level since 1987 (Patientregistret 1998). For each patient, one or more diagnosis at the discharge from hospital is available in 99% of cases. The diagnosis of BCS or PVT has not been validated but results on other disorders have shown an 85–90% registry ac-curacy (Patientregistret 1998). The scientific use of the Swedish patient register is well established including previous studies on venous thromboembolism (Baron et al. 1998; Ludvigsson et al. 2007).
29

Methods
22
Paper I & II (n=216)Paper IV (n=110) Paper III (n=102)
43 BCS173 PVT
19 BCS91 PVT
19 BCS83 PVT
+ 65 patientsNew patients (2004-2009) including Danderyd hospital
- 171 patients Deceased 81%No consent 13% Intra-abdominal malignancy 3% Örebro University hospital 3%
- 8 patients MalmöUniversity hospital
To assure full catchment of BCS and PVT cases, analysis of epidemiology was restricted to primary catchment area-patients in six centres (Linköping, Sahlgren-ska Göteborg, Umeå, Örebro, Malmö and Jönköping) which had used both in- and outpatient registers to identify their patients. The mean population figure for each year and each primary catchment area were available from Statistics Swe-den, Stockholm. The combined population of these six centres was 1.3 million, comprising approximately 15% of the Swedish population in 2001.
The crude incidence and prevalence rates were age-standardised according to the population census in 1970. Patients were not included in the analysis of prevalence rates following orthotopic liver transplantation, as they were consid-ered to be ‘disease-free’ after transplantation.
Paper III and IV
Cases
To evalutate the presence of prothrombotic factors in primary BCS and non-malignant PVT, we designed two case-control studies. Eligible for inclusion were all patients in Papers I and II without intra-abdominal malignancy, as were new cases diagnosed during the years 2004-2009 at the participating centres by means of patient register search. In total, 102 cases (19 BCS and 83 PVT) were included in Paper III and 110 cases (19 BCS and 91 PVT) in Paper IV. These were recruited as follows (Figure 4):
Of the total 216 patients (43 BCS and 173 PVT) in Paper I and II, 171 were excluded (deceased, 81%; consent was not obtained, 13%; one hospital could not participate, 3%; intra-abdominal malignancy, 3%). Thus, 45 cases (10 BCS and 35 PVT) remained from previous studies and 65 (9 BCS and 56 PVT) were newly diagnosed (2004-2009). These new patients were recruited from the same hospitals as in Paper I and II except for the fact that Örebro univerisity hospital was replaced by Danderyd hospital. In paper III, citrate plasma from 8 patients in Malmö could not be analyzed due to technical failure.
Figure 4. Recruitment of patients in Paper III and IV.
30

Methods
23
Controls and other patient groups for comparison
For comparison, three other groups were investigated in Paper III: (i) consecutive non-malignant patients without any known liver disorder and diagnosed with a lower-limb DVT (with or without pulmonary embolism) (n=95) between Febru-ary 1998 and January 2000 at Linköping university hospital. These patients were sampled after anticoagulant therapy was stopped. No liver-related morbidity or mortality has occurred during a 7-year follow-up period of these patients; (ii) randomly chosen patients with cirrhosis without history or imaging of portal vein thrombosis (n=26) followed at Linköping university hospital or Karolinska uni-versity hospital. The aetiology was alcohol (n=11), non-alcoholic steatohepatitis (n=5), viral (n=4), autoimmune (n=4), haemochromatosis (n=1) or cryptogenic (n=1). Neither PVT nor BCS was present at the diagnosis of cirrhosis (between June 2002 and September 2010) or during the regular (6-12 monthly) imaging studies performed thereafter; and, (iii) healthy controls (n=17).
In paper IV, DNA samples (n = 283); 136 males, 62 (25-80) years of age and 147 females, 64 (25-80) years of age were obtained from a regional DNA-bank (Professor Peter Söderkvist, Department of Cell biology, Linköping University) which consists of genomic DNA from 800 individuals. These individuals have been randomly selected from the Swedish population register and anonymously included in the DNA-bank after informed consent.
31

Methods
24
Methods
Data collection
Available information on clinical characteristics, catchment area, investigations undertaken, laboratory findings, treatment given, as well as the outcome were retrospectively retrieved from the medical records by using structured case record forms (CRF).
The date of diagnosis was defined as the year and month on which a throm-botic obstruction was evident on at least one of the following imaging modalities: ultrasonography, computerised tomography scan (CT), magnetic resonance imag-ing, echocardiography (Paper I only) or angiography. The presence of cirrhosis or not was based on clinical data, i.e. past history of liver disease, results of im-aging and laboratory studies and/or by liver biopsy, if performed.
Rotterdam prognostic scores (Murad et al. 2004) for BCS were calculated if complete data were available. This numerical score is composed of weighted val-ues at diagnosis for bilirubin, prothrombin-INR, ascites and encephalopathy, by which patients can be categorised into three classes: I (good prognosis), II (in-termediate prognosis) and III (poor prognosis) (Murad et al. 2004). Child-Pugh scores, were assessed in BCS (irrespective of the presence of cirrhosis or not) and in cirrhotic PVT patients with complete data to allow a comparison with other published cohorts (Zeitoun et al. 1999; Murad et al. 2004; Murad et al. 2006; Plessier et al. 2006).
The presence of any liver disease, intra-abdominal malignancy, gastrointes-tinal inflammation or abdominal surgery performed less than three months prior to diagnosis, were categorised as local risk factors. Blood disorders (including MPD), hormone therapy, septicaemia, rheumatoid disorders, paroxysmal noctur-nal haemoglobinuria and pregnancy were considered systemic risk factors. Pri-mary and secondary BCS were defined as previously described (Janssen et al. 2003).
The follow-up period was from the date of diagnosis until death, study clo-sure in November 2004, or, in the case of loss to follow-up, the last visit.
The causes of death were acquired from the medical records, or if absent, from the Cause-of-death register, the National board of health and welfare, Stockholm (Paper I and II). Register search was made possible through the na-tional registration number, unique for each citizen (Lunde et al. 1980).
Database All data (Paper I and II) were entered into a Microsoft Access 2002 database (Microsoft Corp. Redmond, WA, USA) and subsequently transferred to the Sta-tistical Package for Social Sciences version 13.0 (SPSS Inc, Chicago, IL, USA).
32

Methods
25
To minimize errors, logical tests were carried out and the database was internally validated by re-checking the entered data with the collected data in 20% of ran-domly selected CRFs.
Laboratory tests (Paper III and IV)
Blood samples were collected after an overnight fast from antecubital veins in sodium 1/10 volume of 0.13 mol/l citrate, EDTA and serum tubes (Becton Dick-inson, Meylan, France). These were centrifuged within two hours at 2500g for 10 minutes at 10°C. Plasma, buffy coat and serum, were immediately stored at -70°C pending analyses.
The median duration from diagnosis to sampling was 78 (1-246) months for BCS, 46 (1-164) months for PVT, 6 (3-13) months for DVT patients (Paper III), and 13 (0-96) months for cirrhotic patients (Paper III).
Factor VIII and high-sensitivity C-reactive protein (Paper III)
Factor VIII activity (HemosIL™ Electrachrome™ Factor VIII) was measured in citrate plasma by using a chromogenic method utilising ACL TOP (Instrumenta-tion Laboratory, Milan, Italy). The reference interval was 0.50-1.80 kIE/L and concentrations above 1.80 kIE/L were considered to be increased. In order to minimise the effect of an acute phase reaction influencing the plasma levels of factor VIII, blood samples were collected during a follow-up visit after the acute event.
High-sensitivity C-reactive protein (hs-CRP) was measured by means of the automated analyser Advia 1800 (Siemens Healthcare Diagnostics, Stockholm).
Thrombophilia screening (Paper III and IV)
The prothrombotic mutations factor V Leiden, and prothrombin gene mutation G2010A were analysed in all patients utilising pyrosequencing technology and the instrument Pyromark Q24 with a similar procedure as for to the published method for VKORC1 gene (Enstrom et al. 2007). A factor Xa-based assay, He-mosIL™ Liquid Antithrombin, (Instrumentation Laboratory, Milan, Italy), for antithrombin, and functional antigenic assays for plasma protein C (Vinazzer and Pangraz 1987) and protein S (Serra et al. 2002) were performed in all patients.
If two or more of these naturally occurring anticoagulant proteins, i.e. anti-thrombin, protein C and protein S were low with or without a family history, this was considered as being secondary to liver dysfunction and not due to a heredi-tary deficiency. The presence of a confirmed antiphospholipid syndrome was judged by the notes in the medical records and not further verified by additional laboratory testing.
33

Methods
26
Genotyping JAK2 (Paper IV)
Genotyping of the JAK2 V617F variant was performed as previously described by Olsen et al. (Olsen et al. 2006) using LightCycler 2.0 (Roche Diagnostics, Basel, Switzerland) with the following modifications. The LightCycler FAST start DNA master PLUS hybridization probes mix (Roche Diagnostics) was used. Each reaction was based on 25 ng genomic DNA isolated from whole blood (EDTA samples) and was run in a final volume of 20 µL. Genotyping of the two intronic Tag-SNPs of the 46/1 JAK2 haplotype (Jones et al. 2009), rs12343867 (T>C) and rs12340895 (C>G), was performed using the FAST 7500 real-time PCR system from Applied Biosystems (Foster City, CA, USA). Each reaction was based on ~20 ng (patients) or 3 ng (DNA-bank) ge-nomic DNA in a final reaction volume of 10 µL. A 97% probability cut off for correctly assigned genotypes was applied when evaluating data.
Statistics Quantitative variables were expressed as medians with range and qualitative variables as absolute or relative frequencies. Comparisons between independent groups were made by Mann–Whitney U-test or Kruskal–Wallis one-way analysis of variance as appropriate for continuous variables. For categorical variables, chi-squared tests were performed and Fisher’s exact test was used when more than 20% of the expected values were less than five.
In addition, the Kaplan–Meier estimate was applied for calculating overall and transplantation-free survival rates in Paper I and II. Univariate analysis of factors at diagnosis influencing survival was assessed using the log-rank test. Multivariate analysis was carried out using Cox’s proportional hazard model if number of events were adequate (i.e. only in Paper II).
In Paper III factor VIII levels were expressed as mean (standard deviation) and one-way ANOVA with Bonferroni post hoc test used, when comparing pa-tient results to those of the healthy controls. Correlations were analysed using the Kendall´s tau coefficient test .
In Paper IV allele frequencies were evaluated using the SNPStats software http://bioinfo.iconcologia.net/SNPStats_web (Sole et al. 2006) (Catalan Institute of Oncology, Barcelona, Spain) and odds ratios (OR) calculated.
All other analyses were carried out in the SPSS versions 13.0 or 16.0 (SPSS Inc, Chicago, IL, USA). Two-tailed p values < 0.05 were considered statistically significant.
34

Results and Discussion
27
RESULTS AND DISCUSSION
Budd-Chiari syndrome (BCS) During the 18-year study period (1986–2003), 43 patients with a median of three cases per hospital (range 0–8) were identified (Paper I). The majority (93%) were regarded as primary BCS cases and the remaining (7%) were secondary to ma-lignant obstruction. Fourteen patients (33%) were diagnosed at the two transplan-tation centres. No patient was lost to follow-up when the study ended in Novem-ber 2004.
Epidemiology
Twelve new cases of BCS were diagnosed (1990–2001) at the six centres eligible for analysis of epidemiological data. The mean age-standardised incidence rate was calculated to be 0.8 (95% CI 0–2.2) per million inhabitants per year. The mean age-standardised prevalence was 1.4 (95% CI 0–3.3) per million for the same years. The percentages of patients reported to be living in the primary catchment area of liver transplantation and non-liver transplantation centres were comparable: 70 and 69% respectively, thus probably excluding an undue selec-tion of severe cases.
Our retrospective study is the first to address the incidence and prevalence rates of BCS in a Western population. Some attempts have previously been made (Table 2). In Japan, the incidence and prevalence rates in 1989 were estimated to be 0.2 and 2.4 per million inhabitants, respectively (Okuda et al. 1995). In Europe, analysis of nationwide registry data from Denmark for the years 1981–1985 gave an estimated incidence rate of 0.5 per million inhabitants and year (Almdal and Sorensen 1991), similar to a questionnaire survey from France that indicated an incidence of 0.4 per million (unpublished data cited in (Valla 2004)).
35

Results and Discussion
28
Table 2. Reported annual incidence and prevalence rates per million inhabitants for Budd-Chiari syndrome.
Author Design Setting Incidence (per million)
Prevalence (per million)
Okuda et al, 1995
Hospital questionnaire
Japan 1989 (n=6 &160)*
0.2 2.4
Almdal et al, 1990
Inpatient register
Denmark 1981-1985 (n=13)
0.5 -
Valla 2004
Hospital qusetionnaire
France 1989 (n=20)
0.4 -
Rajani et al, 2009
In- & outpatient register
Sweden 1990-2001 (n=12)
0.8 1.4
* Incidence rate based on 6 new patients, and prevalence rate on 160 patients included in the survey.
There are two probable explanations for the higher incidence rate that we found. In contrast to the study from Denmark, we also included data from outpatient registers and covered a later time period, 1990–2001, during which the diagnostic awareness of this rare disorder increased and better imaging modalities had be-come available.
The lower prevalence rate in our study, compared with the one from Japan, is probably explained by a high frequency of liver transplantation (42%), after which patients were censored as being ‘disease-free’ and therefore not included in the prevalence analysis.
Our figures should be considered more reliable than previous results from Japan as these non-standardised rates were calculated on the basis of a hospital questionnaire survey with a response rate of 65% or less. Furthermore, autopsy register data were used, with large variations in autopsy rates between hospitals varying from 10 to 75%.
Clinical features
The median age at diagnosis of the 43 studied patients (24 women) was 40 years (range 4–80). Nine of these (21%) had concomitant PVT.
At diagnosis the classical triad of ascites (88%), abdominal pain (81%) and hepatomegaly (72%) was present in the majority of patients at diagnosis; no pa-tient was asymptomatic. The occurrence of unexpectedly diagnosed, asympto-
36

Results and Discussion
29
matic subjects in recent cohorts has been no more than 6% (Murad et al. 2004; Amarapurkar et al. 2008; Darwish Murad et al. 2009).
To establish the diagnosis, a combination of various imaging modalities had to be performed: abdominal ultrasonography (n = 41), CT-abdomen (n = 39), an-giography (n = 18), echocardiography (n = 17), CT-thorax (n = 10) and MRI (n = 7). Further investigations performed were as follows: bone marrow aspiration (n = 24), laparocentesis (n = 22), gastroscopy (n = 18) and laparotomy (n = 5).
In Table 3 patients are classified according to the site of hepatic outflow ob-struction at presentation.
Table 3. Anatomical localisation of thrombosis at presentation in 43 patients with Budd-Chiari Syndrome.
n %
IVC* (isolated) 2 5
Hepatic vein (isolated) 24 56
One hepatic vein 1
Two hepatic veins 1
Three hepatic veins 22
Both IVC* and hepatic vein 10 23
One hepatic vein 1
Two hepatic veins 1
Three hepatic veins 8
Not specified 7 16
Concomitant thrombosis in:
Portal vein (n=36) 9 25
Acute 6
Chronic 2
Unknown 1
Mesenteric vein (n=28) 2 7
Splenic vein (n=29) 2 7
All three veins (n=28) 1 4
* Inferior vena cava (supra-hepatic)
Risk factors
The spectrum of blood and coagulation disorders are listed in Table 4. The most prevalent risk factor was a myeloproliferative disorder in 14 patients (38%; 10 women and 4 men). The diagnosis was verified in eleven (79%) of these patients with a bone marrow biopsy. Cultures of progenitors (14) were not performed and
37

Results and Discussion
30
the JAK2 V617F mutation analysis (15) was not available at the time of the first study. JAK2 mutations were therefore assessed in a follow-up study (Paper IV) discussed in a later section.
Table 4. Blood and coagulation disorders in 43 patients with Budd-Chiari syndrome (patients can have more than one of the disorders stated below).
n %
Myeloproliferative disorder (n=37) 14 38
Polycythaemia vera rubra 8
Essential thrombocythaemia 6
Thrombophilic factor* (n=35) 11 31
Cardiolipin antibodies 2
Lupus anticoagulant 2
Factor V Leiden mutation 3
Heterozygous 2
Homozygous 1
Antithrombin deficiency** 2
Protein C deficiency** 1
Protein S deficiency** 0
Hyperhomocysteinaemia 1
Hyperfibrinogenaemia 1
Other blood disorders (n=37) 3 8
Myelodysplastic syndrome 2
Acute myeloid leukaemia 1
*One patient has more than one factor (cardiolipin antibodies and hyperhomocystein-aemia).
**Defined as an isolated decrease in value to exclude secondary deficiencies due to liver failure.
The prevalence of other inherited or acquired thrombophilic conditions (31%) in our cohort were of the same order as in previous studies from western countries (Mahmoud et al. 1997; Denninger et al. 2000; Smalberg et al. 2006).
Oral contraceptive use was reported in six (30%) women, and in each of them a second aetiological factor was present. Three of these six women under-went liver transplantation of whom one ultimately died. Of the other oral contra-ceptive users, two died of liver and multiorgan failure, respectively. The preva-lence of oral contraceptive use ranges from 0-52% in other series (Mahmoud et
38

Results and Discussion
31
al. 1997; Denninger et al. 2000; Janssen et al. 2000; Mentha et al. 2006; Smalberg et al. 2006) and an increased relative risk of hepatic vein thrombosis has been reported to be 2.4 compared to non-users (Valla et al. 1986).
None of our cases were associated with paroxysmal nocturnal haemoglo-binuria or pregnancy.
We could not identify a risk factor in 10 patients (23%). However, not all pa-tients had undergone a full diagnostic work-up for coagulation disorders and MPD. Fourteen patients (32%) had one risk factor identified; two or more risk factors were present in 19 (44%) patients confirming a multicausal aetiology as has been shown for VTE in general (Rosendaal 1999). In the small subset of nine BCS cases with concomitant PVT, six (67%) had multiple risk factors. A similar high frequency (58%) has been reported in a previous series with extensive thrombosis of the splanchnic veins (Murad et al. 2006).
When categorising risk factors as being systemic or local, 25 patients (78%) had a systemic factor, three (9%) had a local precipitating factor, and four (13%) a combination of both.
Survival
Cause of death
19 patients (44%) died during a median follow-up of 2.7 years (range 0.04–16). The cause of death was predominately liver failure (47%) (Table 5). Two patients died from GI bleeding; one of them had not received anticoagulant therapy. One MPD patient progressed to leukaemia. As long-term survival rates are improving, this complication is a future concern in BCS patients in whom MPD is com-monly diagnosed at a young age (DeLeve et al. 2009).
Table 5. Cause of death in patients with Budd-Chiari syndrome (n=19).
BCS (n=19)
n %
Liver failure 9 47
Malignancy* 3 16
Cardiac failure 2 11
GI bleeding 2 11
Multiorgan failure 1 5
Infection 1 5
Pulmonary embolism 1 5
* Hepatocellular cancer (n=2), Leukemia (n=1)
39

Results and Discussion
32
Survival rates
The overall survival at 1, 5 and 10 years, including the 18 patients who had undergone a liver transplantation, was 67% (95% CI, 54-81), 60% (95% CI 45-75) and 52% (95% CI 35-69) (Figure 5).The transplantation-free survival was poor; at 1, 5 and 10 years it was 47% (95% CI 32-61), 28% (95% CI 14-41) and 17% (95% CI 4-30), respectively (Figure 5).
Figure 5. Overall and transplantation-free survival rates for patients with Budd-Chiari syndrome (n=43). Patients at risk after 1, 5 and 10 years of follow-up were n=29, n=21 and n=11 (overall survival), and n=20, n=9 and n=2 (transplantation-free survival), re-spectively.
When considering the benefits of liver transplantation, the overall survival rates are in line with a recently published Canadian cohort (Montano-Loza et al. 2009) (Table 6).
When comparing our results with the findings in the largest study so far in BCS (Murad et al. 2004), we found a less favourable transplantation-free sur-vival rate (47 % vs. 82% at 1 year and 28% vs. 69% at 5 years) as outlined in Table 6. Both studies included patients seen during the same time period (1986-2003 vs. 1984-2001), and the median follow-up time (32 vs. 44 months) and the
40

Results and Discussion
33
median age at diagnosis (40 vs. 35 years) were roughly similar (Table 6). The differences in outcome (without transplantation) was most probably not due to different inclusion criteria; only non-malignant (primary) BCS cases were in-cluded in the cohort of Murad et al. (Murad et al. 2004). Excluding the three pa-tients with intra-abdominal malignancy (secondary BCS) from our analysis did not have any sizeable impact on transplantation-free survival.
The proportion of patients living in the primary catchment area of transplan-tation centres was similar to that of patients from non-transplantation centres, ruling out referral bias. However, it is possible that subjects with clinically mild hepatic dysfunction seen in non-academic hospitals could have been overlooked (and therefore not referred). Moreover, asymptomatic cases of BCS, usually in-volving one or two veins, were not recognised in our study. Such limited in-volvement was noted in only four of the 43 (10%) which may have influenced the poor outcome. Furthermore, the lack of a national reference centre for BCS in Sweden might have contributed.
The patients diagnosed early (1986-1994, n=13) did not have a worse out-come compared to patients diagnosed later (1995-2003, n=30) when assessed using Kaplan-Meier statistics. The use of anticoagulants, a crucial factor for the better survival in Zeitoun´s paper (Zeitoun et al. 1999), did not differ between these two time periods, 77% (10/13) vs. 72% (21/30). Neither the use of antico-agulants during the first year after diagnosis (p=0.13), nor the presence of MPD (p=0.95) had any significant effect on survival, which has also been reported in other studies (Murad et al. 2004; Smalberg et al. 2006; Kiladjian et al. 2008).
Our survival estimates could partly be explained by a higher proportion (83 vs. 73%) of patients in Rotterdam class II and III, i.e. the patients in our cohort had a more severe disorder at diagnosis, which is also illustrated by the absence of any single patient in Child-Pugh class A. Furthermore, the percentage of pa-tients with a concomitant PVT was higher in our study (21% vs. 14%) which has been associated with poorer survival (Mahmoud et al. 1997; Murad et al. 2006), although this was not evident in our univariate assessment.
Regarding therapeutic interventions, the proportion of patients undergoing portosystemic shunt surgery were considerably lower in our study compared to the one by Murad et al. (Murad et al. 2004) (14% vs. 42%), and in favour of liver transplantation (42% vs. 12%) (Table 6). The majority of patients received anti-coagulant therapy (72% vs. 72%) and TIPS was equally often performed (9% vs. 7%). In a recent series, in which a more aggressive therapeutic approach was ap-plied, TIPS was inserted in as much as 49% of the patients (Plessier et al. 2006). When considering the benefits of liver transplantation, the overall survival rates in our study was 67% and 60% at 1- and 5-year, respectively. These results are in line with a recently published Canadian cohort (Montano-Loza et al. 2009) (Ta-ble 6).
41

35 Tab
le 6
. Cha
ract
eris
tics
of
BC
S in
rec
ent p
ubli
cati
ons
42

Results and Discussion
34
43

Results and Discussion
36
Actuarial survival rates after liver transplantation in large register studies have been reported to be good and comparable to other chronic liver diseases, with 1- and 5-year survival of 76-88% and 71%, respectively (Mentha et al. 2006; Segev et al. 2007).
As prospective randomised trials are lacking in BCS, the best therapeutic ap-proach is not clear-cut (Horton et al. 2008). In a single-centre study in which a stepwise, minimal invasive therapeutic strategy was used, the 1- and 5-year mor-tality rates were found to be 4% and 11%, respectively during the years 1997-2004, much better than results from case series dating back to 1965-1972 (32% and 90%, 1- and 5-year mortality), 1970-1985 (38% and 50%), and 1984-2001 (18% and 31%) (Plessier et al. 2006).
Recent consensus reports therefore recommend a step-up management (DeLeve et al. 2009; de Franchis 2010), i.e. early anticoagulation in all patients without contraindications. If a venous stenosis is causing the outflow obstruction, percutaneous angioplasty/stenting should be considered or if not possible, TIPS inserted in patients who do not respond to medical therapy. Finally, if these pro-cedures fail or if the patient presents with fulminant liver failure, liver transplan-tation is indicated.
Portal vein thrombosis (PVT) In Paper II a total of 173 patients (median age 57 years, 93 men) with portal vein thrombosis were identified. Fifty-five patients (32%) were diagnosed at the two transplantation centres. The median age at diagnosis was 57 years (range 15-94). Only one patient (0.6%) was lost to follow-up due to emigration when the study ended in October 2004. An acute thrombosis was present in 128 patients (74 %), chronic thrombosis in 32 (18%) and was unspecified in 13 (8%). The thrombosis was limited to the portal vein in 102 patients (59%) and in the remaining 71 pa-tients (41%) one or more accessory veins, i.e. the mesenteric and/or splenic veins were also involved.
Epidemiology
At the six centres eligible for the epidemiological analysis, 124 patients with PVT were diagnosed (1995-2003), of whom 97 were from the primary catchment areas. The mean age-standardised incidence and prevalence rates of PVT were calculated to be 0.7 (95% CI 0.3–1.2) per 100 000 inhabitants per year and 3.7 (95% CI 2.6–4.8) per 100 000 inhabitants, respectively. The percentages of pa-tients living in the primary catchment area of liver transplantation and non-liver transplantation units were comparable, being 81% and 78%, respectively (NS).
We report for the first time both incidence and prevalence rates of unselected PVT in a population-based cohort. Previous studies have mainly reported preva-lence figures of PVT in cirrhotic patients.
44

Results and Discussion
37
In Denmark, nationwide register data limited to inpatients for the years 1981–1985 gave an estimated incidence rate of 0.27 per 100 000 inhabitants and year (Almdal and Sorensen 1991), i.e. half the rate reported herein (Table 7). In con-trast to that study, we also included data from outpatient registers and covered a later time period, 1995–2004, during which the diagnostic awareness of this con-dition increased.
Tabell 7. Reported annual incidence and prevalence rates for portal vein thrombosis.
Author Design Setting Incidence (per 100 000)
Prevalence (per 100 000)
Okuda et al, 1985
Autopsy register
Japan 1975-1982 (n=136)
- 54.9
Ögren et al, 2006
Autopsy register
Sweden 1970-1982 (n=254)
- 1067*
Almdal et al, 1990
Inpatient register
Denmark 1981-1985 (n=69)
0.3 -
Rajani et al, 2010
In- & outpatient register
Sweden 1990-2001 (n=97)
0.8 3.7
* Life time cumulative incidence
Population-based prevalence rates for PVT have been addressed in two older au-topsy studies (Table 7). In the Japan Autopsy Register of 1975–1982 (n = 247 728), PVT was found in 0.05% (≈ 50 per 100 000 inhabitants) (adapted from Okuda et al.(Okuda et al. 1995), whereas in Malmö city, Sweden, the prevalence was as high as 1.0% (≈1000 per 100 000) in 1970–1982 (n = 23 796 representing 84% of all in-hospital deaths) (Ogren et al. 2007). The difference between these results is striking and could be due to a lower occurrence of PVT in Japan com-pared with Europe. However, considering that both studies originate from ne-cropsy data in which there is a selection for the more severe cases per se, variable autopsy rates in different centres as well as ascertainment bias (Ogren et al. 2007), our lower prevalence rate should be considered more reliable.
This assumption is underlined by the high proportion of patients with intra-abdominal neoplasia (67%) in one of the autopsy studies (Ogren et al. 2007) as compared to our data (21%) and with a previous large case series (24%) (Janssen et al. 2001).
45

Results and Discussion
38
Clinical features
The clinical characteristics of PVT are diverse and represent a patient population with different underlying aetiologies. The characteristics in our large Swedish cohort are comparable to findings in a previous Dutch study (Janssen et al. 2001) (Table 8).
Table 8. Clinical characteristics at diagnosis in two large unselected cohorts with portal vein thrombosis.
Rajani et al, 2010,
n=173 Janssen et al, 2001, n=172
Demographics % %
Male/Female 54/46 50/50
Age, years* 57 (15-94) 51 (14-91)
Country SE NL
Centres / of which tertiary 11/9 8/8
Year of diagnosis 1995-2004 1984-1997
Follow-up, years* 2.5 (0-10) 3.9 (0-13)
Lost to follow-up 1 3
Symptoms & signs
Ascites 38 48
Abdominal pain 69 -
Fever 35 -
Splenomegaly 43 -
Oesophageal varices 61 70
Variceal bleeding 20 30
Asymptomatic 5 -
Labratory findings*
CRP, mg/L 39 (4-480)
Haemoglobin, g/L 121 (39-188) 121 (-)
WBC x109/L 8 (1-57)
Platelet count x109/L 223 (16-1074) 179 (-)
Bilirubin, μmol/L 20 (4-690) 20 (-)
ALT xULN* 1.0 (0.1-98.3) 0.8 (-)
Albumin, g/L 30 (13-53) 35 (-)
Prothrombin, INR 1.2 (0.9-2.9) -
46

Results and Discussion
39
Child-Pugh classification**
A 10 -
B 69 -
C 22 -
Type of obstruction
Acute 74 -
Chronic 18 -
Not specified 8 -
Concomitant thrombosis in
Mesenteric veins 33 24
Splenic vein 25 -
Two or more veins 45
All three 15 -
Treatment
Anticoagulants 67 27
Thrombolysis 3
Acetylsalicylic acid 8
TIPS/surgical shunting 3 8
Liver transplantation*** 5 2
Splenectomy 3
Bowel resection 3
* Median (range)
** Calculated in cirrhotic patients only
*** Due to underlying liver disease.
The total study population (n=173) was grouped into three strata; N-PVT, non-malignant, non-cirrhotic PVT (n=89), C-PVT, non-malignant, cirrhotic PVT (n=38), and, M-PVT, malignant PVT (n=46).
N-PVT patients were younger at the time of diagnosis (median age 54 years) compared to patients with C-PVT (60 years) or M-PVT (67 years), p<0.001 (for both comparisons) and presented more often with fever, 48% (p=0.004). On the other hand ascites (p<0.001), splenomegaly (p<0.001), oesophageal varices (p=0.001), jaundice (p=0.005) and signs of hypertensive gastropathy (p=0.017) were more prevalent in C-PVT and M-PVT. Abdominal pain was a common complaint in N-PVT (78%) and M-PVT patients (70%), but less frequent in C-
47

Results and Discussion
40
PVT (46%) (p=0.002). Ileus was diagnosed in 6 cases (4%). Eight patients (5%) were asymptomatic of whom six were N-PVT patients.
Classification according to Child-Pugh was, for the cirrhotic patients (n=38) grade A 14%, grade B 61% and grade C 25%, and, for patients with malignancy (n=46), 0%, 87% and 13%, respectively.
The median C-reactive protein (CRP) in N-PVT (67mg/L) and M-PVT (44mg/L) was higher than in C-PVT patients (13mg/L) (p=0.003). Few patients had an increase in prothrombin-INR and the transaminase levels were generally normal or slightly elevated.
Risk factors
The spectrum of risk factors is listed in Table 9 and 10. Overall, 76 patients (44%) had one or more local precipitating factors, and 42 patients (24%) had a systemic risk factor. No obvious risk factor was evident in 17 patients (10%).
The most prevalent risk factor was a liver disorder, present in 70 patients (40%) of whom 54 (76%) had liver cirrhosis. Alcoholic liver disease was present in 21 patients (12%), viral hepatitis in 15 (9%), cryptogenic cirrhosis in 14 (8%), autoimmune hepatitis in 6 (3%), non-alcoholic fatty liver disease in 4 (2%) and other liver disorders in 10 (6%).
Table 9. Local risk factors in Portal vein thrombosis (n=173). Patients can have more than one factor. N %
Liver disease 70 40
With cirrhosis 54
Without cirrhosis 16
Intra-abdominal malignancy 37 21
Hepatocellular cancer 21
Colorectal cancer 4
Other 12
GI-inflammation (n=166)* 24 14
Abdominal surgery** 8 5
Severe local infection (n=169)* 5 3
No local factor identified 59 34
*Denotes number of evaluable cases.
**Within three months prior to diagnosis.
48

Results and Discussion
41
N %
Thrombophilic factor† (n=126)* 28 22
Factor V Leiden mutation 13
Hyperfibrinogenemia 4
Lupus anticoagulant 4
Cardiolipin antibodies 3
Antithrombin deficiency‡ 3
Prothombin gene mutation 2
Protein S deficiency‡ 1
Previous thrombosis (n=156)* 29 19
Venous 19
Arterial 10
Myeloproliferative disorder (n=158)* 18 11
Polycytemia vera rubra 12
Essential Thrombocythemia 5
Chronic Myeloid Leukaemia 1
Severe systemic infection (n=169)* 14 8
Hormone replacement therapy (n=75/80)* 9 12
Rheumatoid disorder (n=165)* 8 5
Blood malignancy 6 13
Lymphoma 4
Leukaemia 2
Extra-abdominal malignancy 3 7
Oral contraceptives (n=74/80)* 3 4
Pregnancy (n=79/80)* 3 4
No systemic factor identified 93 54
†Two patients had more than one factor (antithrombin deficiency and hyperfibrino-genemia, protein S deficiency and lupus anticoagulant, respectively).
*Denotes number of evaluable cases.
‡Deficiency due to liver failure not included i.e. patients with combined low levels of protein S and protein C and/or antithrombin were excluded.
Of systemic factors, thrombophilic conditions were present in 22% of patients. 19% had a previous history of any extra-splanchnic thrombotic event with a trend to concurrent presence of these two (chi-square 3.3; df 1, p=0.07). Eighteen pa-tients (11%) had an underlying MPD. The occurrence of MPD was 26% in N-PVT, 6% in C-PVT and, 2% in M-PVT patients, respectively. MPD and severe infections were more common in N-PVT compared to the two other groups (p=0.015 and p=0.046, respectively). Although the highest frequency of inherited or acquired thrombophilia was seen in N-PVT patients (26%), there was no sta-
49
Table 10. Systemic risk factors in Portal vein thrombosis (n=173). Patients can have more than one factor.

Results and Discussion
42
tistically significant difference compared to C-PVT (17%) and M-PVT (18%) patients.
New insights in the aetiology of PVT have revealed the presence of more than one risk factor in a high proportion of patients (Denninger et al. 2000; Janssen et al. 2001; Amitrano et al. 2007; Sogaard et al. 2007). This was con-firmed in our study with 23% having a combination of a local and a systemic risk factor compared to 16% in a study from the Netherlands (Janssen et al. 2001). Moreover, almost half of the patients (46%) had two or more risk factors (regard-less of if local or systemic). However, in reports from the East (e.g. India) the presence of thrombophilia and multiple risk factors have been less evident (Jain and Nijhawan 2007; Dutta et al. 2008).
In an Italian single centre study of non-cirrhotic non-malignant patients with thrombosis confined to the splanchnic veins, the occurrence of two or more risk factors was 27% (Amitrano et al. 2007) compared to 37% in our N-PVT patients. These findings suggest that a thorough diagnostic work-up in order to optimise the management of patients is warranted irrespective of the presence of a local precipitating factor.
Medical treatment and interventions
Details of interventions performed at diagnosis and during follow-up are given in Table 11. Of the 116 anticoagulated patients, 94 had an acute thrombo-sis, 15 chronic thrombosis and in seven the nature of the thrombosis was not specified. The median duration of anticoagulant therapy was 6.4 (range 0.1-114) months and the mean duration was 16 months.
50

Results and Discussion
43
Table 11. Interventions in 173 patients with portal vein thrombosis.
At
diagnosis During
follow-up n % n %
Anticoagulants 113 65 116 67
Heparin/LMWH 102 103
Coumarin derivatives 63 70
Thrombolysis 6 3 6 3
Acetylsalicylic acid 11 6 14 8
Other antiplatelet drugs 2 1 2 1
Diuretics 64 37 71 41
Betablockers 64 37 72 42
Isosorbide mononitrate 11 6 13 8
Band ligation 26 15 36 21
Sclerotherapy 20 12 23 13
TIPS or surgical shunting 3 2 5 3
Liver transplantation* 1 1 8 5
Splenectomy 0 0 5 3
Bowel resection 4 2 6 3
*Due to underlying liver disease
FU, Follow-up; LMWH, low-molecular-weight heparin; TIPS, transjugular intrahepatic portosystemic shunting.
Anticoagulation was more common in N-PVT patients (85%) than those with C-PVT (70%) or M-PVT (50%), (p=0.004) while diuretics were less frequent in N-PVT patients (p<0.001). All six patients (4%) given thrombolysis (one local and five systemically) were non-malignant and non-cirrhotic. Three patients (2%) with an underlying liver disease underwent TIPS at diagnosis. In two patients (both N-PVT) surgical shunting procedures were performed during the first or the third year after diagnosis due to GI-bleeding and varices. Eight patients (5%) underwent liver transplantation secondary to their underlying liver disorder, of whom one ultimately died, six days after transplantation. Six patients (3%) un-derwent bowel resection due to ischemia.
Information on recanalisation was available in 61 patients (35%). Partial or complete recanalisation was seen in 70% during the first year of follow-up and 72% at the last follow-up visit. 36 of 44 patients (82%) with recanalisation had received anticoagulation. An increased obstruction in the portal venous tract was
51

Results and Discussion
44
observed in 7% and remained unchanged in 21%. Recanalisation frequencies did not seem to differ between N-PVT (68%, n=40), C-PVT (83%, n=12) and M-PVT (78%, n=9) patients (NS).
Due to the lack of randomized controlled trials, the best treatment for PVT is empirical (de Franchis 2005; Chawla et al. 2009; DeLeve et al. 2009; de Franchis 2010; Tsochatzis et al. 2010). Partly based on retrospective studies from France, in which 90% achieved partial or complete recanalisation 23 without an in-creased risk of bleeding (Condat et al. 2001), anticoagulant therapy has been ad-vocated for patients with acute nonmalignant and noncirrhotic PVT (de Franchis 2005). Recanalisation was, however, achieved only in 66% (31% partial and 34% complete) of our N-PVT patients during the first year after diagnosis, with a mi-nor increase to 68% when analysing the total follow-up period. Although these results must be interpreted with caution as data on recanalisation were limited, they are consistent with a retrospective Italian series in which 45% of N-PVT patients achieved complete recanalisation (Amitrano et al. 2007). However, find-ings in a prospective study of anticoagulated patients have furthermore indicated a limited recanalisation rate of 38% (Plessier et al. 2010), negatively influenced by the presence of ascites and concomitant splenic vein obstruction at diagnosis. These results have not altered the current guidelines for early treatment with anti-coagulants (DeLeve et al. 2009; de Franchis 2010). In PVT with cirrhosis, there is no consensus on the indication for anticoagulant therapy (DeLeve et al. 2009; de Franchis 2010). After initiating prophylactic therapy for variceal bleeding the use of anticoagulants have been reported by some groups (Francoz et al. 2005; Tsochatzis et al. 2010) and TIPS has been successful in other series (Bauer et al. 2006; Han et al. 2011).
To treat selected patients with an acute, extensive, symptomatic thrombosis who are eligible for or already listed for liver transplantation is suggested.
Survival
Cause of death
A total of 74 patients (43%) died during a median follow-up was 2.5 years (range 0–9.7). The causes of death are listed in Table 12. We had two deaths due to variceal bleeding in patients who had not been anticoagulated. Death due to in-testinal ischemia occurred in only one (0.6%) patient.
52

Results and Discussion
45
Table 12. Cause of deaths and survival rates in two large portal vein thrombosis cohorts.
Rajani et al, 2010,
n=173 Janssen et al, 2001,
n=172
Deaths 74 43% 67 39%
Cause of deaths
Malignancy 31 42 30 45
Intra-abdominal 28 18
Other 3 12
Liver failure 16 22 10 15
Cardiac failure 9 12 9 13
Multiorgan failure 6 8 - -
Infection 4 5 4 6
Variceal bleeding 2 3 4 6
Intestinal ischemia 1 1 - -
Other, non-liver related 5 7 7 10
Unknown 0 3 4
Survival rate
Overall at 1/5/10 year 69/54/- 70/61/54
Tx-free at 1/5/10 year 92/76/-* 95/89/81**
* No cancer, no cirrhosis
** No cancer, no cirrhosis, no mesenteric vein thrombosis
Survival rates
The overall survival at 1 and 5 years was 69% (95% CI 61–76) and 54% (95% CI 46–62), respectively (Figure 6). The rates were consistent with the findings in a similar multicentre series from the Netherlands (Janssen et al. 2001), being 69% vs. 70%, and, 54% vs. 61% (Table 12). A slightly lower survival in our study is tentatively attributed to a higher frequency of concomitant mesenteric vein thrombosis (31% vs. 11%), which has been associated with decreased survival (Janssen et al. 2001; Kumar et al. 2001; Orr et al. 2007). However, this was not evident in our univariate analysis.
53

Results and Discussion
46
Figure 6. Overall survival rates for all patients with portal vein thrombosis, for patients with non-malignant, non-cirrhotic portal vein thrombosis, N-PVT, for patients with cir-rhosis, but no malignancy, C-PVT, and for patients with malignancy with or without cirrhosis, M-PVT.
In N-PVT (n=89) the survival at 1 and 5 years was 92% (95% CI 86–98) and 76% (95% CI 66–86), respectively, and similar to findings in previous series (Janssen et al. 2001; Amitrano et al. 2007). However, the 5-year survival for such patients was higher in an Italian cohort being 93% (Amitrano et al. 2007) compared to 76% in our study. A more favourable outcome could be explained by their single tertiary referral centre holding a liver transplantation unit, and by a uniform management strategy in younger patients (median age at diagnosis was 45 years compared to 54 years in our study).
For C-PVT (n=38) the survival at 1 and 5 years was 53% (95% CI 37–69) and 38% (95% CI 19–58), respectively and for those with M-PVT (n=46) 37% (95% CI 23–51) and 24% (95% CI 11–37), respectively. Reports comparing the survival in cirrhotic patients with and without PVT are lacking in the literature. The median one-year cumulative survival for C-PVT was 53% in our study, i.e. worse than the 78% reported for cirrhotic patients in general (D'Amico et al. 2006).
54

Results and Discussion
47
Multivariate analysis
The results of a multivariate analysis (Table 13) showed that age, bilirubin, cir-rhosis and malignancy independently influenced survival (p<0.001) consistent with a previous report (Janssen et al. 2001) in which survival was primarily re-lated to the underlying disorder.
Table 13. Multivariate survival analysis of characteristics at diagnosis in 173 patients with portal vein thrombosis. Relative risk (RR) of death is given for the total cohort and separately for those with non-malignant portal vein thrombosis (n=127).
PVT (n=173) Non-malignant PVT (n=127)
RR 95% CI p RR 95% CI p
Age
<=50 1.0 1.0
51-60 1.9 0.8 - 4.3 0.14 2.9 1.0 - 8.4 0.06
> 60 4.2 2.0 - 8.6 <0.001 12.0 4.1 - 34.9 <0.001
Sex
Female 1.0 1.0
Male 1.9 1.1 - 3.5 0.03 1.1 0.6 - 2.3 0.72
Bilirubin (μmol/L)
<= 20 1.0 1.0
> 20 4.8 2.6 - 8.8 <0.001 3.8 1.7 - 8.6 0.00
Albumin (g/L)
<= 30 1.0 31 7.90 - 1.0 31 7.90
> 30 0.9 0.5 - 1.5 0.58 1.2 0.5 - 2.8 0.62
Mesenteric vein thrombosis
Absent 1.0 1.0
Present 1.2 0.7 - 2.2 0.55 0.8 0.4 - 1.8 0.61
Cirrhosis
Absent 1.0 1.0
Present 2.7 1.6 - 4.7 <0.001 7.3 2.9 - 18.3 <0.001
Abdominal inflammation
Absent 1.0 1.0
Present 0.5 0.2 - 1.2 0.11 1.1 0.3 - 3.7 0.88
Malignancy
Absent 1.0
Present 3.5 1.9 - 6.6 <0.001
55

Results and Discussion
48
Similar to other reports (Kiladjian et al. 2008), the presence of thrombophilia and MPD at diagnosis did not significantly affect survival in analysis.
Although the use of anticoagulants during the first year after diagnosis was high (65%) compared to 25-34% in previous studies (Janssen et al. 2001; Amitrano et al. 2004), we did not observe an increased survival with anticoagula-tion, nor has this been evident in other studies with the exception of one study in chronic portomesenteric thrombosis patients (Orr et al. 2007). In that report, mortality was more frequently caused by variceal bleeding (38%) than in our study (3%).
Thrombophilic factor VIII in BCS and PVT
In Paper III we explored the role of procoagulant factor VIII in primary BCS and non-malignant PVT as no obvious risk factors were observed in up to 23% of patients (Paper I and II).
We found significantly increased plasma levels of coagulant factor VIII both in BCS and PVT patients with or without cirrhosis as compared to healthy con-trols (p < 0.001) (Table 14).
Table 14. Factor VIII levels in patients with portal vein thrombosis (PVT), Budd-Chiari syndrome (BCS), cirrhosis without thrombosis, deep vein thrombosis (DVT) and con-trols. Mean (standard deviation).
Factor VIII, kIE/L
P vs. controls
P vs. DVT
P vs. cirrhosis
PVT (all, n=83) 1.90
(0.67) < 0.001 < 0.001 NS
PVT (without cirrhosis, n=62) 1.87
(0.67) < 0.001 < 0.001 NS
PVT (with cirrhosis, n=21) 1.97
(0.68) < 0.001 < 0.001 NS
BCS (n=19) 1.63
(0.63) < 0.001 NS <0.01
Cirrhosis (n=26) 2.22
(0.66) < 0.001 < 0.001 -
DVT (n=95) 1.41
(0.44) < 0.001 -
Controls (n=17) 1.04
(0.07) -
P; P-values as per ANOVA. NS; not significant.
56

Results and Discussion
49
Increased factor VIII levels have not previously been reported in BCS apart from a case study in which familial elevated levels were observed in two patients (Koshy 2004). For PVT, the present study confirms previous results from case series (Brandenburg et al. 2001; Fimognari et al. 2005; Shah et al. 2005) and a small case-control study (n=32) (Koshy and Jeyakumari 2007) in which high fac-tor VIII levels were found employing another assay.
Our patients were sampled beyond the acute incident. A possible influence of an acute phase reaction was further investigated by correlating factor VIII re-sults to hs-CRP in the non-acute phase (i.e. > 3 months after diagnosis). A weak correlation was seen only in PVT without cirrhosis not excluding factor VIII ele-vation as an independent risk factor in primary PVT.
Recently, a case-control study (n=85) (Martinelli et al. 2009) similar to ours, albeit from a single tertiary referral centre, demonstrated an odds ratio of 10.5 for PVT without and 6.0 with PVT cirrhosis, when factor VIII exceeded the 66th per-centile of the levels in healthy controls. Using the 95th percentile the odds ratio was 3.1 for PVT (without cirrhosis). However, these findings were partly due to an acute phase reaction as 64% of their PVT patients were tested within three months after diagnosis, which resulted in lower odds ratios when excluding these patients from the analysis.
Factor VIII activity was higher in both cirrhotic (1.97 kIE/L) and non-cirrhotic PVT (1.87 kIE/L) compared to DVT (1.41 kIE/L) patients (p < 0.001); however for BCS (1.63 kIE/L) the results were not statistically significant (p = 0.87), suggesting that reduced flow in the portal vein may influence the circulat-ing factor VIII concentration. Using an upper reference range limit (1.80 kIE/L) of the assay as cut-off, elevated levels were found in high proportions of patients with PVT and in cirrhotic patients without thrombosis (Figure 7.) These findings suggest that a reduced flow in the portal vein may influence the circulating factor VIII concentration.
57

Results and Discussion
50
Figure 7. Percentage of patients with elevated plasma levels of factor VIII (>1.80 kIE/ml).
* Chi-squared test p-value < 0.05, ** < 0.01, *** < 0.001.
Established prothrombotic risk factors were not detected in 21% of non-cirrhotic PVT, in 48% of cirrhotic PVT or in 11% of BCS patients. In these patients an elevated factor VIII concentration was present in 85%, 70% and 50%, respec-tively. These findings could explain a majority of PVT and BCS cases previously denoted as being idiopathic.
In line with previous publications (DeLeve et al. 2009; Shetty and Ghosh 2010) the frequency of prothrombin gene mutation in PVT was higher (5%) and factor V Leiden (as well as antiphospholipid syndrome) lower (8%) compared to in BCS patients (although not statistically significant). In Sweden the prevalence of these genetic mutations in the normal population is 1-2% for the prothombin gene and 8-14% for factor V Leiden (Lindahl et al. 1999; Bjorkman et al. 2005). Therefore, in our PVT patients (with and without cirrhosis), the prevalence ap-pears to be increased for the prothrombin gene mutation, but not for factor V Leiden. This is similar to non-cirrhotic PVT data from a large Italian case-control study (Primignani et al. 2005), however, in contrast to results from the Nether-lands (Janssen et al. 2000). For cirrhotic PVT patients, disparities exist on the presence of genetic thrombophilic risk factors (Amitrano et al. 2000; Amitrano et al. 2004; Mangia et al. 2005). Possible explanations could be different frequen-cies of coagulation disorders in the background populations, as well as patient selection criteria since cirrhotic patients are not routinely screened. Furthermore, reduced portal flow velocity (Zocco et al. 2009) could be a confounding factor by influencing impairing the synthesis and clearance of coagulation factors.
48
71
21
81
18
0
10
20
30
40
50
60
70
80
90
100
PVT (withoutcirrhosis, n=62)
PVT (withcirrhosis, n=21)
BCS (n=19) Cirrhosis (n=26) DVT (n=95)
%
***
****
**
**
58

Results and Discussion
51
JAK 2 46/1 haplotype and V617F mutation in BCS and PVT In Paper IV, we found a high occurrence of the JAK2 46/1 haplotype in BCS (53%) and PVT (36%) patients compared to controls (27%) p=0.02 (OR=3.0; 95% CI 1.5-5.9) and p=0.02 (OR=1.5; 95% CI 1.1-2.1), respectively (Table 15). The association remained significant when adjusting for age and gender. In PVT patients the JAK2 haplotype was highly enriched in non-cirrhotic patients (41%) (p <0.01 ; OR=1.8; 95% CI 1.2-2.6) but not in cirrhotic patients (23%)(p=0.53; OR= 0.8; 95% CI 0.4-1.7) relative to population controls.
Table 15. Association between JAK2 46/1 haplotype and JAK2 V617F mutation status in 19 patients with Budd-Chiari syndrome (BCS) and 91 patients with portal vein thrombosis (PVT). Haplotype frequencies in patients were compared to the frequency in 283 controls from a background population.
N
JAK 2 46/1 Haplotype'
frequency (%)
P-value vs. con-
trols Odds Ratio (95% CI) Odds Ratio (95% CI)* Controls 283 27 All patients 110 39 <0.01 1.7 (1.2-2.3) 1.6 (1.1 - 2.2) JAK2 V617F + 25 66 <0.01 5.5 (2.8 - 10.7) 5.2 (2.6 - 10.5) JAK2 V617F - 85 31 0.30 1.2 (0.8 - 1.8) 1.2 (0.8 - 1.7) BCS 19 53 0.02 3.0 (1.5 - 5.9) 2.5 (1.2 - 5.2) JAK2 V617F + 12 63 <0.01 4.6 (1.9 - 10.9) 3.8 (1.5 - 9.5) JAK2 V617F - 7 36 0.5 1.5 (0.5 - 4.6) 1.4 (0.4 - 4.3) All PVT 91 36 0.02 1.5 (1.1 - 2.1) 1.46 (1.0 - 2.1) JAK2 V617F + 13 69 <0.01 6.5 (2.6 - 16.2) 5.8 (2.3 - 14.6) JAK2 V617F - 78 31 0.37 1.2 (0.8 - 1.7) 1.1 (0.8 - 1.7) Non-cirrhotic PVT 69 41 <0.01 1.8 (1.2 - 2.6) 1.8 (1.2 - 2.6) JAK2 V617F + 13 69 <0.01 6.5 (2.6 - 16.2) 5.8 (2.3 - 14.6) JAK2 V617F - 55 34 0.15 1.4 (0.9 - 2.1) 1.3 (0.8 - 2.0) Cirrhotic PVT 22 23 0.53 0.8 (0.4 - 1.7) 0.8 (0.4 - 1.6) JAK2 V617F + 0 JAK2 V617F - 22 23 0.53 0.8 (0.4 - 1.7) 0.8 (0.4 - 1.6)
' Tagged by the C-allele of SNP rs12343867 and G-allele of SNP rs12340895. Linkage disequilibrium (d=0.2091, d'=0.9998 and r=0.9914).
* Adjusted for sex and age.
CI, confidence interval; SNP, single-nucleotide polymorphism.
59

Results and Discussion
52
The JAK 2 46/1 haplotype enrichment was evident in JAK2 V617F mutation positive patients, being nearly 5-fold in BCS and 6-fold in non-cirrhotic PVT. We also found that one of two (50%) V617F negative PVT patients carried the specific haplotype.
Prior to our study the prevalence of JAK2 V617F-mutation has not been known in Swedish BCS and PVT patients. We observed a very high occurrence in our BCS patients (63%) (Figure 8).
Figure 8. Percentage myeloproliferative disorders (MPD) and JAK2-mutation in pa-tients with Budd-Chiari syndrome (BCS) and Portal vein thrombosis (PVT).
Previous series have reported frequencies between 40-50% (Shetty and Ghosh 2010), however, in the most recent large multicentre prospective BCS study the prevalence was not more than 29% (Darwish Murad et al. 2009). A recent meta-analysis including ten studies found the pooled prevalence to be 37% (95% CI 25-51%) for the JAK2 V617F mutation in BCS. The variation was remarkably large, varying from 9% to 70% (Qi et al. 2011). The lowest prevalence was re-ported from India. This could indicate different frequencies of the acquired JAK2 V617F mutation in Western compared to Eastern BCS patients which needs to be addressed in future studies. Moreover, different inclusion criteria, number of pa-tients studied (Qi et al. 2011), the sensitivity of the assays used to detect JAK2 V617F (Xu et al. 2007) and publication bias (Dentali et al. 2009) may also ex-plain these discrepancies.
In PVT the JAK2 V617 mutation was found in 14% without cirrhosis, a fre-quency lower than previous series 20-40% (Plessier et al. 2010; Shetty and Ghosh 2010) and meta-analysis prevalence of 24% (95% CI 18-31%) (Qi et al. 2011).
Interestingly, 1/22 (5%) of the cirrhotic PVT patients (all JAK2 V617F nega-tive) had a bone marrow histology verified essential thrombocythaemia. This pa-
6863
105
15 14
2 10
10
20
30
40
50
60
70
80
MPD JAK2 positive JAK2 negative,MPD
JAK2 positive,MPD not known
%BCS (n=19)
PVT (n=91)
60

Results and Discussion
53
tient did not carry the 46/1 allele. Previously, the JAK 2 46/1 haplotype fre-quency has not been investigated in cirrhotic PVT and V617F mutation data have so far been published in two reports (Colaizzo et al. 2008; Xavier et al. 2010). A meta-analysis of these two studies demonstrated that approximately 7% (95% CI: 2.6–11.9) of cirrhotic patients with PVT carried the mutation, suggesting a poten-tial for routine screening in these patients too (Qi et al. 2010). However, none of our cirrhotic PVT patients were V617F positive and an association with the 46/1 haplotype was not found. The diagnostic and prognostic value of JAK2 haplo-type and V617F mutation testing in cirrhotic patients needs to be clarified by fur-ther investigations.
We could not confirm the findings by Colaizzo et. al (Colaizzo et al. 2010) suggesting the 46/1 haplotype was overrepresented in JAK2 V617F negative PVT patients without MPD. The disparity could be explained by different control groups (n=283 population controls in our study compared to n=181 hospital em-ployees not being in Hardy-Weinberg equilibrium).
The European Network for Vascular Disorders of the Liver (EN-Vie) study group (Smalberg et al. 2011) has very recently reported increased erythrocytosis in newly diagnosed BCS and PVT patients carrying the JAK2 46/1 haplotype without the JAK2 V617F mutation. We could not confirm this finding in our pa-tient cohort (data not shown), nor has it been observed in previous studies ana-lysing a possible association between clinical and laboratory characteristics and the JAK2 46/1 haplotype in MPD patients (Jones et al. 2009; Andrikovics et al. 2010; Pardanani et al. 2010; Tefferi et al. 2010).
In line with previous publications (Patel et al. 2006; Primignani et al. 2006; Kiladjian et al. 2008; Orr et al. 2010; Xavier et al. 2010; Smalberg et al. 2011) there was an clear association between JAK2 V617F mutation and erythrocytosis (Patel et al. 2006; Primignani et al. 2006; Kiladjian et al. 2008; Orr et al. 2010; Xavier et al. 2010; Smalberg et al. 2011) splenomegaly (Patel et al. 2006; Primignani et al. 2006; Kiladjian et al. 2008; Smalberg et al. 2011), increased ALT (Kiladjian et al. 2008; Smalberg et al. 2011) and worse prognostic scores (Kiladjian et al. 2008; Smalberg et al. 2011).
We did not explore other MPD associated mutations e.g. in JAK2 exon 12 (Scott et al. 2007) and MPL, a thrombopoietin receptor gene, (Pardanani et al. 2006; Pikman et al. 2006) as they were not detected in a large (n=241) European BCS and PVT study (Kiladjian et al. 2008).
In all, V617F negative MPD were seen in 10% of BCS and 2% of PVT cases (Figure 8). Conversely, JAK2-mutation positive subjects without previously di-agnosed MPD were found in 5% of BCS and 1% of PVT patients.
Thus, analysing JAK2 V617F mutation should be considered in the diagnos-tic work-up of primary BCS and PVT, however, a negative result dose not rule out MPD.
61

Results and Discussion
54
General discussion There are some limitations and strengths to our studies. In Sweden, patient care during the study period was virtually almost exclusively public and based on geographical grounds i.e. patients are referred to specific hospitals according to council of residence. Reporting ICD diagnose codes to patient registers is manda-tory, and 99% of all hospitalisations are registered (Patientregistret 1998). To assure full catchment of all cases, analysis of epidemiology was restricted to pri-mary catchment area patients centres which had used both in- and outpatient reg-isters to identify patients. Although a thorough search was performed sampling error could have occurred; if so, asymptomatic BCS or PVT (with cirrhosis) and patients with advanced malignancy would most probably have been missed. At the time of our epidemiological studies (Paper I and II), screening for hepatocel-lular carcinoma was not routinely performed in the participating centres. Thus, the incidence and prevalence rates of PVT reported here are possibly underesti-mated.
The studies are a retrospective analysis of a heterogeneous, although large nationwide patient cohort, and a standardised initial diagnostic workup had not been applied. Thus, it is possible that some prothrombotic factors in our BCS and PVT patients went undetected.
To exclude an undue selection and referral bias as much as possible, we in-cluded all patients treated at both academic and non-academic hospitals. Follow-up and outcome endpoints, i.e. death and causes of death, can accurately be as-certained using the national citizen registration number for register search.
Treatment bias is possibly reduced by a recent study period during which dramatic changes in therapeutic options have evolved.
In Papers III and IV the DVT group and population controls, respectively, were large and population-based. The healthy control sample was small, however reference values have been well established for factor VIII.
62

Conclusion
55
CONCLUSIONS
BCS is a rare disorder; the mean age-standardised incidence and prevalence rates in Sweden 1990-2001 were 0.8 per million inhabitants per year and 1.4 per mil-lion inhabitants respectively.
Due to the low incidence, a high level of suspicion of BCS is necessary in pa-tients presenting with any of, or a combination of, unexplained ascites, abdomi-nal pain and hepatomegaly in order to confirm this condition early with the aim to improve the outcome of patients.
The incidence and prevalence rates of PVT were higher 0.7 per 100 000 inhabi-tants per year and 3.7 per 100 000 inhabitants, respectively.
The clinical features of PVT are diverse and represent a patient population with different underlying aetiologies.
In BCS the transplantation-free survival was poor, whereas in PVT the survival was good in the absence of cirrhosis and cancer, which were the most common underlying risk factors. Mortality due to intestinal infarction was low and less than 1% in our PVT cohort.
Concurrent prothrombotic risk factors were present in almost half of BCS and PVT patients, underlining the concept of multiple causes in the aetiology of these disorders. These findings suggest that a thorough diagnostic work-up to optimize the management is warranted irrespective of the presence of one precipitating factor.
Patients with PVT and BCS have elevated plasma levels of coagulation factor VIII. Prospective studies are needed to investigate if factor VIII levels can pre-dict thrombosis formation, especially in patients with liver cirrhosis, and if meas-uring the levels can be of value in the management of these patients.
The prevalence of the somatic (acquired) JAK2 V617F mutation was high in our cohort and associated with the presence of a germline (inherited) JAK2 46/1 hap-lotype.
63

Conclusion
56
64

Acknowledgements
57
ACKNOWLEDGEMENTS
I would like to express my sincere gratitude to all those who directly and indi-rectly supported me in making this thesis possible. In particular I would like to thank:
All patients, your intriguing and challenging disease got my tutor and all the rest of us on this endeavour!
Sven Almer, my tutor and research guru. For taking me on and introducing me to the world of research. For your support at all times and sharing experiences be-yond p-values. Pranam.
Tomas Lindahl, my co-tutor for sharing your knowledge and laboratory resources in venous thrombosis during the second part of this work.
All my co-authors: Annika Bergquist, Einar Björnsson, Ulrika Broomé (de-ceased), Åke Danielsson, Inga-lill Friis-Liby, Olof Grip, Anders Gustavsson, Sofie Haglund, Cecilia Jennersjö, Marjo Kapraali, Stergios Kechagias, Lars Lööf, Tor Melin, Per Sangfelt, Hans Svensson, Hans Verbaan and Sven Wallerstedt, for enrolment of patients and sound advice.
SILK, a network of hepatologists at all Swedish university hospitals, for believing in the project, and providing the necessary infrastructure for conducting liver studies with large patient cohorts in a relatively small country.
Björn Tavelin, for statistical help with epidemiology and survival rate calcula-tions; and his colleagues at NSCRI/A+Science (Umeå) for database support.
Lena Svensson, for her excellent assistance in the lab and keeping the spirits high with coffee and cakes during meetings. Gratitude also to Kerstin Gustavsson.
Peter Söderkvist, for providing population controls from the DNA-bank.
Mårten Werner, for enrolment of patients.
65

Acknowledgements.
58
Christer Grännö, my mentor and brilliant clinical supervisor for laying the path, and brightening up work, whenever needed, with crazy jokes and a lot of fun.
Past and present heads of department: Leif Ockander, Staffan Schön and Agneta Ståhl (Jönköping); Rolf Hultcrantz and co-heads Hans Törnblom and Peter Thelin Schmidt (Stockholm); Henrik Hjortswang (Linköping); for providing the necessary facilities and resources to complete this thesis.
All my collegues at the departments of Medicine (Ryhov) and Gastroenterology & Hepatology (Karolinska), for enduring an increased work load during my ab-sence.
Nurses, secretaries and other staff members at all participating hospitals for help in collecting blood samples and retrieving archived medical records. You know who you are.
All my friends for making life more fun. You mean a lot!
Mum, Dad, Tina, Niteen and charming Veer for their endless support, encour-agement and love. Finally, Ranu, my love, for supporting me in finishing this thesis. Pay back time, I guess…
This thesis was supported by unrestricted grants from Futurum - the academy of healthcare, County Council of Jönköping; The County council of Östergötland (ALF-grants); The Medical Research Council of Southeast Sweden (FORSS) and The Swedish Society of Medicine (Bengt Ihre-fonden and Gastroenterologisk fond).
66

References.
59
REFERENCES
Abdel-Wahab, O (2011). Genetics of the myeloproliferative neoplasms. Curr Opin Hematol 18(2): 117-23.
Almdal, TP and Sorensen, TI (1991). Incidence of parenchymal liver diseases in Denmark, 1981 to 1985: analysis of hospitalization registry data. The Danish Association for the Study of the Liver. Hepatology 13(4): 650-5.
Amarapurkar, DN, Punamiya, SJ and Patel, ND (2008). Changing spectrum of Budd-Chiari syndrome in India with special reference to non-surgical treatment. World J Gastroenterol 14(2): 278-85.
Amitrano, L, Brancaccio, V, Guardascione, MA, Margaglione, M, Iannaccone, L, D'Andrea, G, et al. (2000). Inherited coagulation disorders in cirrhotic patients with portal vein thrombosis. Hepatology 31(2): 345-8.
Amitrano, L, Guardascione, MA, Brancaccio, V, Margaglione, M, Manguso, F, Iannaccone, L, et al. (2004). Risk factors and clinical presentation of portal vein thrombosis in patients with liver cirrhosis. J Hepatol 40(5): 736-41.
Amitrano, L, Guardascione, MA, Scaglione, M, Pezzullo, L, Sangiuliano, N, Armellino, MF, et al. (2007). Prognostic factors in noncirrhotic patients with splanchnic vein thromboses. Am J Gastroenterol 102(11): 2464-70.
Andrikovics, H, Nahajevszky, S, Koszarska, M, Meggyesi, N, Bors, A, Halm, G, et al. (2010). JAK2 46/1 haplotype analysis in myeloproliferative neoplasms and acute myeloid leukemia. Leukemia 24(10): 1809-13.
Austin, SK and Lambert, JR (2008). The JAK2 V617F mutation and thrombosis. Br J Haematol 143(3): 307-20.
Baccarani, M, Cortes, J, Pane, F, Niederwieser, D, Saglio, G, Apperley, J, et al. (2009). Chronic myeloid leukemia: an update of concepts and management recommendations of European LeukemiaNet. J Clin Oncol 27(35): 6041-51.
Balfour, GW and Stewart, TG (1869). Case of enlarged spleen complicated with ascites both depending on varicose dilatation and thrombosis of the portal vein. Edinburgh Med J 14: 589-98.
Baron, JA, Gridley, G, Weiderpass, E, Nyren, O and Linet, M (1998). Venous thromboembolism and cancer. Lancet 351(9109): 1077-80.
Bauer, J, Johnson, S, Durham, J, Ludkowski, M, Trotter, J, Bak, T, et al. (2006). The role of TIPS for portal vein patency in liver transplant patients with portal vein thrombosis. Liver Transpl 12(10): 1544-51.
Baxter, EJ, Scott, LM, Campbell, PJ, East, C, Fourouclas, N, Swanton, S, et al. (2005). Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet 365(9464): 1054-61.
67

References
60
Bjorkman, A, Burtscher, IM, Svensson, PJ, Hillarp, A, Besjakov, J and Benoni, G (2005). Factor V Leiden and the prothrombin 20210A gene mutation and osteonecrosis of the knee. Arch Orthop Trauma Surg 125(1): 51-5.
Brancatelli, G, Vilgrain, V, Federle, MP, Hakime, A, Lagalla, R, Iannaccone, R, et al. (2007). Budd-Chiari syndrome: spectrum of imaging findings. AJR Am J Roentgenol 188(2): W168-76.
Brandenburg, VM, Frank, RD, Wasmuth, HE and Gartung, C (2001). Elevated levels of factor VIII:C as a possible risk factor for portal, splenic, and mesenteric vein thrombosis. Gastroenterology 120(6): 1563-4.
Budd, G (1845). On diseases of the liver. 146. Campbell, PJ and Green, AR (2006). The myeloproliferative disorders. N Engl J
Med 355(23): 2452-66. Chait, Y, Condat, B, Cazals-Hatem, D, Rufat, P, Atmani, S, Chaoui, D, et al.
(2005). Relevance of the criteria commonly used to diagnose myeloproliferative disorder in patients with splanchnic vein thrombosis. Br J Haematol 129(4): 553-60.
Chawla, Y, Duseja, A and Dhiman, RK (2009). Review article: the modern management of portal vein thrombosis. Aliment Pharmacol Ther 30(9): 881-94.
Chiari, H (1899). Ueber die selbstandige phlebitis obliterans der hauptstamme der venae hepaticae als todesursache. Beitr Z Pathol Anat 26: 1-18.
Colaizzo, D, Amitrano, L, Guardascione, MA, Balzano, A and Margaglione, M (2008). Janus kinase-2 mutation, cirrhosis and splanchnic vein thrombosis. Eur J Gastroenterol Hepatol 20(3): 245-6.
Colaizzo, D, Tiscia, GL, Bafunno, V, Amitrano, L, Vergura, P, Grandone, E, et al. (2010). The JAK2 rs12343867 CC genotype frequently occurs in patients with splanchnic venous thrombosis without the JAK2V617F mutation: a retrospective study. J Thromb Haemost 8(2): 413-6.
Condat, B, Pessione, F, Hillaire, S, Denninger, MH, Guillin, MC, Poliquin, M, et al. (2001). Current outcome of portal vein thrombosis in adults: risk and benefit of anticoagulant therapy. Gastroenterology 120(2): 490-7.
Condat, B, Vilgrain, V, Asselah, T, O'Toole, D, Rufat, P, Zappa, M, et al. (2003). Portal cavernoma-associated cholangiopathy: a clinical and MR cholangiography coupled with MR portography imaging study. Hepatology 37(6): 1302-8.
D'Amico, G, Garcia-Tsao, G and Pagliaro, L (2006). Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol 44(1): 217-31.
Dahlback, B (2005). Blood coagulation and its regulation by anticoagulant pathways: genetic pathogenesis of bleeding and thrombotic diseases. J Intern Med 257(3): 209-23.
Dahlback, B (2008). Advances in understanding pathogenic mechanisms of thrombophilic disorders. Blood 112(1): 19-27.
68

References.
61
Darwish Murad, S, Plessier, A, Hernandez-Guerra, M, Fabris, F, Eapen, CE, Bahr, MJ, et al. (2009). Etiology, management, and outcome of the Budd-Chiari syndrome. Ann Intern Med 151(3): 167-75.
de Bruijne, EL, Darwish Murad, S, de Maat, MP, Tanck, MW, Haagsma, EB, van Hoek, B, et al. (2007). Genetic variation in thrombin-activatable fibrinolysis inhibitor (TAFI) is associated with the risk of splanchnic vein thrombosis. Thromb Haemost 97(2): 181-5.
de Franchis, R (2005). Evolving consensus in portal hypertension. Report of the Baveno IV consensus workshop on methodology of diagnosis and therapy in portal hypertension. J Hepatol 43(1): 167-76.
de Franchis, R (2010). Revising consensus in portal hypertension: report of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension. J Hepatol 53(4): 762-8.
De Stefano, V, Za, T, Rossi, E, Vannucchi, AM, Ruggeri, M, Elli, E, et al. (2008). Recurrent thrombosis in patients with polycythemia vera and essential thrombocythemia: incidence, risk factors, and effect of treatments. Haematologica 93(3): 372-80.
DeLeve, LD, Valla, DC and Garcia-Tsao, G (2009). Vascular disorders of the liver. Hepatology 49(5): 1729-64.
Deltenre, P, Denninger, MH, Hillaire, S, Guillin, MC, Casadevall, N, Briere, J, et al. (2001). Factor V Leiden related Budd-Chiari syndrome. Gut 48(2): 264-8.
Denninger, MH, Chait, Y, Casadevall, N, Hillaire, S, Guillin, MC, Bezeaud, A, et al. (2000). Cause of portal or hepatic venous thrombosis in adults: the role of multiple concurrent factors. Hepatology 31(3): 587-91.
Dentali, F, Galli, M, Gianni, M and Ageno, W (2008). Inherited thrombophilic abnormalities and risk of portal vein thrombosis. a meta-analysis. Thromb Haemost 99(4): 675-82.
Dentali, F, Squizzato, A, Brivio, L, Appio, L, Campiotti, L, Crowther, M, et al. (2009). JAK2V617F mutation for the early diagnosis of Ph- myeloproliferative neoplasms in patients with venous thromboembolism: a meta-analysis. Blood 113(22): 5617-23.
Dhiman, RK, Behera, A, Chawla, YK, Dilawari, JB and Suri, S (2007). Portal hypertensive biliopathy. Gut 56(7): 1001-8.
Dutta, AK, Chacko, A, George, B, Joseph, JA, Nair, SC and Mathews, V (2008). Risk factors of thrombosis in abdominal veins. World J Gastroenterol 14(28): 4518-22.
Eapen, CE, Velissaris, D, Heydtmann, M, Gunson, B, Olliff, S and Elias, E (2006). Favourable medium term outcome following hepatic vein recanalisation and/or transjugular intrahepatic portosystemic shunt for Budd Chiari syndrome. Gut 55(6): 878-84.
Elliott, MA and Tefferi, A (2005). Thrombosis and haemorrhage in polycythaemia vera and essential thrombocythaemia. Br J Haematol 128(3): 275-90.
69

References
62
Enstrom, C, Osman, A and Lindahl, TL (2007). A genotyping method for VKORC1 1173C>T by Pyrosequencing((R)) technology. Scand J Clin Lab Invest: 1-4.
Fimognari, FL, De Santis, A, Piccheri, C, Moscatelli, R, Gigliotti, F, Vestri, A, et al. (2005). Evaluation of D-dimer and factor VIII in cirrhotic patients with asymptomatic portal venous thrombosis. J Lab Clin Med 146(4): 238-43.
Fisher, NC, Wilde, JT, Roper, J and Elias, E (2000). Deficiency of natural anticoagulant proteins C, S, and antithrombin in portal vein thrombosis: a secondary phenomenon? Gut 46(4): 534-9.
Francoz, C, Belghiti, J, Vilgrain, V, Sommacale, D, Paradis, V, Condat, B, et al. (2005). Splanchnic vein thrombosis in candidates for liver transplantation: usefulness of screening and anticoagulation. Gut 54(5): 691-7.
Garcia-Pagan, JC, Heydtmann, M, Raffa, S, Plessier, A, Murad, S, Fabris, F, et al. (2008). TIPS for Budd-Chiari syndrome: long-term results and prognostics factors in 124 patients. Gastroenterology 135(3): 808-15.
Hadengue, A, Poliquin, M, Vilgrain, V, Belghiti, J, Degott, C, Erlinger, S, et al. (1994). The changing scene of hepatic vein thrombosis: recognition of asymptomatic cases. Gastroenterology 106(4): 1042-7.
Han, G, Qi, X, He, C, Yin, Z, Wang, J, Xia, J, et al. (2011). Transjugular intrahepatic portosystemic shunt for portal vein thrombosis with symptomatic portal hypertension in liver cirrhosis. J Hepatol 54(1): 78-88.
Henderson, JM, Gilmore, GT, Mackay, GJ, Galloway, JR, Dodson, TF and Kutner, MH (1992). Hemodynamics during liver transplantation: the interactions between cardiac output and portal venous and hepatic arterial flows. Hepatology 16(3): 715-8.
Hernandez-Guerra, M, Turnes, J, Rubinstein, P, Olliff, S, Elias, E, Bosch, J, et al. (2004). PTFE-covered stents improve TIPS patency in Budd-Chiari syndrome. Hepatology 40(5): 1197-202.
Hoekstra, J, Guimaraes, AH, Leebeek, FW, Darwish Murad, S, Malfliet, JJ, Plessier, A, et al. (2010). Impaired fibrinolysis as a risk factor for Budd-Chiari syndrome. Blood 115(2): 388-95.
Hollestelle, MJ, Geertzen, HG, Straatsburg, IH, van Gulik, TM and van Mourik, JA (2004). Factor VIII expression in liver disease. Thromb Haemost 91(2): 267-75.
Horton, JD, San Miguel, FL and Ortiz, JA (2008). Budd-Chiari syndrome: illustrated review of current management. Liver Int 28(4): 455-66.
Jain, P and Nijhawan, S (2007). Portal vein thrombosis: etiology and clinical outcome of cirrhosis and malignancy-related non-cirrhotic, non-tumoral extrahepatic portal venous obstruction. World J Gastroenterol 13(39): 5288-9.
James, C, Ugo, V, Le Couedic, JP, Staerk, J, Delhommeau, F, Lacout, C, et al. (2005). A unique clonal JAK2 mutation leading to constitutive signalling causes polycythaemia vera. Nature 434(7037): 1144-8.
70

References.
63
Janssen, HL, Garcia-Pagan, JC, Elias, E, Mentha, G, Hadengue, A and Valla, DC (2003). Budd-Chiari syndrome: a review by an expert panel. J Hepatol 38(3): 364-71.
Janssen, HL, Meinardi, JR, Vleggaar, FP, van Uum, SH, Haagsma, EB, van Der Meer, FJ, et al. (2000). Factor V Leiden mutation, prothrombin gene mutation, and deficiencies in coagulation inhibitors associated with Budd-Chiari syndrome and portal vein thrombosis: results of a case-control study. Blood 96(7): 2364-8.
Janssen, HL, Wijnhoud, A, Haagsma, EB, van Uum, SH, van Nieuwkerk, CM, Adang, RP, et al. (2001). Extrahepatic portal vein thrombosis: aetiology and determinants of survival. Gut 49(5): 720-4.
Johansson, P, Kutti, J, Andreasson, B, Safai-Kutti, S, Vilen, L, Wedel, H, et al. (2004). Trends in the incidence of chronic Philadelphia chromosome negative (Ph-) myeloproliferative disorders in the city of Goteborg, Sweden, during 1983-99. J Intern Med 256(2): 161-5.
Jones, AV, Chase, A, Silver, RT, Oscier, D, Zoi, K, Wang, YL, et al. (2009). JAK2 haplotype is a major risk factor for the development of myeloproliferative neoplasms. Nat Genet 41(4): 446-9.
Kiladjian, JJ, Cervantes, F, Leebeek, FW, Marzac, C, Cassinat, B, Chevret, S, et al. (2008). The impact of JAK2 and MPL mutations on diagnosis and prognosis of splanchnic vein thrombosis: a report on 241 cases. Blood 111(10): 4922-9.
Kiladjian, JJ, Cervantes, F, Leebeek, FW, Marzac, C, Cassinat, B, Chevret, S, et al. (2008). The impact of JAK2 and MPL mutations on diagnosis and prognosis of splanchnic vein thrombosis: a report on 241 cases. Blood 111(10): 4922-9.
Kilpivaara, O, Mukherjee, S, Schram, AM, Wadleigh, M, Mullally, A, Ebert, BL, et al. (2009). A germline JAK2 SNP is associated with predisposition to the development of JAK2(V617F)-positive myeloproliferative neoplasms. Nat Genet 41(4): 455-9.
Koshy, A (2004). Familial high factor VIII level associated with hepatic vein thrombosis. J Clin Gastroenterol 38(8): 723.
Koshy, A and Jeyakumari, M (2007). High FVIII level is associated with idiopathic portal vein thrombosis in South India. Am J Med 120(6): 552 e9-11.
Koster, T, Blann, AD, Briet, E, Vandenbroucke, JP and Rosendaal, FR (1995). Role of clotting factor VIII in effect of von Willebrand factor on occurrence of deep-vein thrombosis. Lancet 345(8943): 152-5.
Kraaijenhagen, RA, in't Anker, PS, Koopman, MM, Reitsma, PH, Prins, MH, van den Ende, A, et al. (2000). High plasma concentration of factor VIIIc is a major risk factor for venous thromboembolism. Thromb Haemost 83(1): 5-9.
71

References
64
Kralovics, R, Passamonti, F, Buser, AS, Teo, SS, Tiedt, R, Passweg, JR, et al. (2005). A gain-of-function mutation of JAK2 in myeloproliferative disorders. N Engl J Med 352(17): 1779-90.
Kumar, S, Sarr, MG and Kamath, PS (2001). Mesenteric venous thrombosis. N Engl J Med 345(23): 1683-8.
Landgren, O, Goldin, LR, Kristinsson, SY, Helgadottir, EA, Samuelsson, J and Bjorkholm, M (2008). Increased risks of polycythemia vera, essential thrombocythemia, and myelofibrosis among 24,577 first-degree relatives of 11,039 patients with myeloproliferative neoplasms in Sweden. Blood 112(6): 2199-204.
Langlet, P, Escolano, S, Valla, D, Coste-Zeitoun, D, Denie, C, Mallet, A, et al. (2003). Clinicopathological forms and prognostic index in Budd-Chiari syndrome. J Hepatol 39(4): 496-501.
Levine, RL, Wadleigh, M, Cools, J, Ebert, BL, Wernig, G, Huntly, BJ, et al. (2005). Activating mutation in the tyrosine kinase JAK2 in polycythemia vera, essential thrombocythemia, and myeloid metaplasia with myelofibrosis. Cancer Cell 7(4): 387-97.
Lindahl, TL, Lundahl, TH, Nilsson, L and Andersson, CA (1999). APC-resistance is a risk factor for postoperative thromboembolism in elective replacement of the hip or knee--a prospective study. Thromb Haemost 81(1): 18-21.
Lisman, T and Leebeek, FW (2007). Hemostatic alterations in liver disease: a review on pathophysiology, clinical consequences, and treatment. Dig Surg 24(4): 250-8.
Ludvigsson, JF, Welander, A, Lassila, R, Ekbom, A and Montgomery, SM (2007). Risk of thromboembolism in 14,000 individuals with coeliac disease. Br J Haematol 139(1): 121-7.
Lunde, AS, Lundeborg, S, Lettenstrom, GS, Thygesen, L and Huebner, J (1980). The person-number systems of Sweden, Norway, Denmark, and Israel. Vital Health Stat 2(84): 1-59.
Mahmoud, AE, Elias, E, Beauchamp, N and Wilde, JT (1997). Prevalence of the factor V Leiden mutation in hepatic and portal vein thrombosis. Gut 40(6): 798-800.
Mahmoud, AE, Helmy, AS, Billingham, L and Elias, E (1997). Poor prognosis and limited therapeutic options in patients with Budd-Chiari syndrome and portal venous system thrombosis. Eur J Gastroenterol Hepatol 9(5): 485-9.
Mangia, A, Villani, MR, Cappucci, G, Santoro, R, Ricciardi, R, Facciorusso, D, et al. (2005). Causes of portal venous thrombosis in cirrhotic patients: the role of genetic and acquired factors. Eur J Gastroenterol Hepatol 17(7): 745-51.
Martinelli, I, Primignani, M, Aghemo, A, Reati, R, Bucciarelli, P, Fabris, F, et al. (2009). High levels of factor VIII and risk of extra-hepatic portal vein obstruction. J Hepatol 50(5): 916-22.
72

References.
65
Mentha, G, Giostra, E, Majno, PE, Bechstein, WO, Neuhaus, P, O'Grady, J, et al. (2006). Liver transplantation for Budd-Chiari syndrome: A European study on 248 patients from 51 centres. J Hepatol 44(3): 520-8.
Moller, S, Dumcke, CW and Krag, A (2009). The heart and the liver. Expert Rev Gastroenterol Hepatol 3(1): 51-64.
Montano-Loza, AJ, Tandon, P, Kneteman, N, Bailey, R and Bain, VG (2009). Rotterdam score predicts early mortality in Budd-Chiari syndrome, and surgical shunting prolongs transplant-free survival. Aliment Pharmacol Ther 30(10): 1060-9.
Moucari, R, Rautou, PE, Cazals-Hatem, D, Geara, A, Bureau, C, Consigny, Y, et al. (2008). Hepatocellular carcinoma in Budd-Chiari syndrome: characteristics and risk factors. Gut 57(6): 828-35.
Murad, SD, Kim, WR, de Groen, PC, Kamath, PS, Malinchoc, M, Valla, DC, et al. (2007). Can the model for end-stage liver disease be used to predict the prognosis in patients with Budd-Chiari syndrome? Liver Transpl 13(6): 867-74.
Murad, SD, Valla, DC, de Groen, PC, Zeitoun, G, Haagsma, EB, Kuipers, EJ, et al. (2006). Pathogenesis and treatment of Budd-Chiari syndrome combined with portal vein thrombosis. Am J Gastroenterol 101(1): 83-90.
Murad, SD, Valla, DC, de Groen, PC, Zeitoun, G, Hopmans, JA, Haagsma, EB, et al. (2004). Determinants of survival and the effect of portosystemic shunting in patients with Budd-Chiari syndrome. Hepatology 39(2): 500-8.
Nonami, T, Yokoyama, I, Iwatsuki, S and Starzl, TE (1992). The incidence of portal vein thrombosis at liver transplantation. Hepatology 16(5): 1195-8.
Nordic MPD study group (NMPD). Guidelines for the diagnosis and treatment of patients with polycythemia vera, essential thrombocythemia and primary myelofibrosis. (2009). from http://www.nmpn.org/guidelines.shtml.
Ogren, M, Bergqvist, D, Bjorck, M, Acosta, S, Eriksson, H and Sternby, NH (2006). Portal vein thrombosis: prevalence, patient characteristics and lifetime risk: a population study based on 23,796 consecutive autopsies. World J Gastroenterol 12(13): 2115-9.
Ogren, M, Bergqvist, D, Bjorck, M, Acosta, S and Sternby, NH (2007). High incidence of concomitant venous thromboembolism in patients with portal vein thrombosis: a population study based on 23 796 consecutive autopsies. J Thromb Haemost 5(1): 198-200.
Ohnishi, K, Okuda, K, Ohtsuki, T, Nakayama, T, Hiyama, Y, Iwama, S, et al. (1984). Formation of hilar collaterals or cavernous transformation after portal vein obstruction by hepatocellular carcinoma. Observations in ten patients. Gastroenterology 87(5): 1150-3.
Okuda, H, Yamagata, H, Obata, H, Iwata, H, Sasaki, R, Imai, F, et al. (1995). Epidemiological and clinical features of Budd-Chiari syndrome in Japan. J Hepatol 22(1): 1-9.
73

References
66
Okuda, K (2002). Inferior vena cava thrombosis at its hepatic portion (obliterative hepatocavopathy). Semin Liver Dis 22(1): 15-26.
Okuda, K, Ohnishi, K, Kimura, K, Matsutani, S, Sumida, M, Goto, N, et al. (1985). Incidence of portal vein thrombosis in liver cirrhosis. An angiographic study in 708 patients. Gastroenterology 89(2): 279-86.
Olcaydu, D, Harutyunyan, A, Jager, R, Berg, T, Gisslinger, B, Pabinger, I, et al. (2009). A common JAK2 haplotype confers susceptibility to myeloproliferative neoplasms. Nat Genet 41(4): 450-4.
Olsen, RJ, Tang, Z, Farkas, DH, Bernard, DW, Zu, Y and Chang, CC (2006). Detection of the JAK2(V617F) mutation in myeloproliferative disorders by melting curve analysis using the LightCycler system. Arch Pathol Lab Med 130(7): 997-1003.
Orloff, MJ, Daily, PO, Orloff, SL, Girard, B and Orloff, MS (2000). A 27-year experience with surgical treatment of Budd-Chiari syndrome. Ann Surg 232(3): 340-52.
Orr, DW, Harrison, PM, Devlin, J, Karani, JB, Kane, PA, Heaton, ND, et al. (2007). Chronic mesenteric venous thrombosis: evaluation and determinants of survival during long-term follow-up. Clin Gastroenterol Hepatol 5(1): 80-6.
Orr, DW, Patel, RK, Lea, NC, Westbrook, RH, O'Grady, JG, Heaton, ND, et al. (2010). The prevalence of the activating JAK2 tyrosine kinase mutation in chronic porto-splenomesenteric venous thrombosis. Aliment Pharmacol Ther 31(12): 1330-6.
Panis, Y, Belghiti, J, Valla, D, Benhamou, JP and Fekete, F (1994). Portosystemic shunt in Budd-Chiari syndrome: long-term survival and factors affecting shunt patency in 25 patients in Western countries. Surgery 115(3): 276-81.
Pardanani, A, Lasho, TL, Finke, CM, Gangat, N, Wolanskyj, AP, Hanson, CA, et al. (2010). The JAK2 46/1 haplotype confers susceptibility to essential thrombocythemia regardless of JAK2V617F mutational status-clinical correlates in a study of 226 consecutive patients. Leukemia 24(1): 110-4.
Pardanani, AD, Levine, RL, Lasho, T, Pikman, Y, Mesa, RA, Wadleigh, M, et al. (2006). MPL515 mutations in myeloproliferative and other myeloid disorders: a study of 1182 patients. Blood 108(10): 3472-6.
Patel, RK, Lea, NC, Heneghan, MA, Westwood, NB, Milojkovic, D, Thanigaikumar, M, et al. (2006). Prevalence of the activating JAK2 tyrosine kinase mutation V617F in the Budd-Chiari syndrome. Gastroenterology 130(7): 2031-8.
Patientregistret 1987-1996 Kvalitet och innehåll (1998). Epidemiologiskt Centrum, Socialstyrelsen. Stockholm.
Perello, A, Garcia-Pagan, JC, Gilabert, R, Suarez, Y, Moitinho, E, Cervantes, F, et al. (2002). TIPS is a useful long-term derivative therapy for patients with Budd-Chiari syndrome uncontrolled by medical therapy. Hepatology 35(1): 132-9.
74

References.
67
Pikman, Y, Lee, BH, Mercher, T, McDowell, E, Ebert, BL, Gozo, M, et al. (2006). MPLW515L is a novel somatic activating mutation in myelofibrosis with myeloid metaplasia. PLoS Med 3(7): e270.
Pirisi, M, Avellini, C, Fabris, C, Scott, C, Bardus, P, Soardo, G, et al. (1998). Portal vein thrombosis in hepatocellular carcinoma: age and sex distribution in an autopsy study. J Cancer Res Clin Oncol 124(7): 397-400.
Plessier, A, Darwish-Murad, S, Hernandez-Guerra, M, Consigny, Y, Fabris, F, Trebicka, J, et al. (2010). Acute portal vein thrombosis unrelated to cirrhosis: a prospective multicenter follow-up study. Hepatology 51(1): 210-8.
Plessier, A, Sibert, A, Consigny, Y, Hakime, A, Zappa, M, Denninger, MH, et al. (2006). Aiming at minimal invasiveness as a therapeutic strategy for Budd-Chiari syndrome. Hepatology 44(5): 1308-16.
Poddar, U, Thapa, BR, Rao, KL and Singh, K (2008). Etiological spectrum of esophageal varices due to portal hypertension in Indian children: is it different from the West? J Gastroenterol Hepatol 23(9): 1354-7.
Primignani, M, Barosi, G, Bergamaschi, G, Gianelli, U, Fabris, F, Reati, R, et al. (2006). Role of the JAK2 mutation in the diagnosis of chronic myeloproliferative disorders in splanchnic vein thrombosis. Hepatology 44(6): 1528-34.
Primignani, M, Martinelli, I, Bucciarelli, P, Battaglioli, T, Reati, R, Fabris, F, et al. (2005). Risk factors for thrombophilia in extrahepatic portal vein obstruction. Hepatology 41(3): 603-8.
Qi, X, Han, G and Fan, D (2010). The preferable treatment for cirrhotic portal vein thrombosis: anticoagulation or transjugular intrahepatic portosystemic shunt? Hepatology 51(2): 713-4.
Qi, X, Yang, Z, Bai, M, Shi, X, Han, G and Fan, D (2011). Meta-analysis: the significance of screening for JAK2V617F mutation in Budd-Chiari syndrome and portal venous system thrombosis. Aliment Pharmacol Ther 33(10): 1087-103.
Rautou, PE, Moucari, R, Escolano, S, Cazals-Hatem, D, Denie, C, Chagneau-Derrode, C, et al. (2009). Prognostic indices for Budd-Chiari syndrome: valid for clinical studies but insufficient for individual management. Am J Gastroenterol 104(5): 1140-6.
Rosendaal, FR (1999). Venous thrombosis: a multicausal disease. Lancet 353(9159): 1167-73.
Rossle, M, Olschewski, M, Siegerstetter, V, Berger, E, Kurz, K and Grandt, D (2004). The Budd-Chiari syndrome: outcome after treatment with the transjugular intrahepatic portosystemic shunt. Surgery 135(4): 394-403.
Sarin, SK, Sollano, JD, Chawla, YK, Amarapurkar, D, Hamid, S, Hashizume, M, et al. (2006). Consensus on extra-hepatic portal vein obstruction. Liver Int 26(5): 512-9.
75

References
68
Scott, LM, Tong, W, Levine, RL, Scott, MA, Beer, PA, Stratton, MR, et al. (2007). JAK2 exon 12 mutations in polycythemia vera and idiopathic erythrocytosis. N Engl J Med 356(5): 459-68.
Segev, DL, Nguyen, GC, Locke, JE, Simpkins, CE, Montgomery, RA, Maley, WR, et al. (2007). Twenty years of liver transplantation for Budd-Chiari syndrome: a national registry analysis. Liver Transpl 13(9): 1285-94.
Serra, J, Sales, M, Chitolie, A, Domenech, P, Rossi, E, Borrell, M, et al. (2002). Multicentre evaluation of IL Test Free PS: a fully automated assay to quantify free protein S. Thromb Haemost 88(6): 975-83.
Shah, SR, DasGupta, A, Sharma, A, Joshi, A, Desai, D, Abraham, P, et al. (2005). Thrombophilic conditions in non-cirrhotic portal vein thrombosis. Indian J Gastroenterol 24(5): 205-10.
Sharma, S, Texeira, A, Texeira, P, Elias, E, Wilde, J and Olliff, SP (2004). Pharmacological thrombolysis in Budd Chiari syndrome: a single centre experience and review of the literature. J Hepatol 40(1): 172-80.
Shetty, S and Ghosh, K (2010). Thrombophilic dimension of Budd chiari syndrome and portal venous thrombosis - A concise review. Thromb Res.
Shrestha, SM, Okuda, K, Uchida, T, Maharjan, KG, Shrestha, S, Joshi, BL, et al. (1996). Endemicity and clinical picture of liver disease due to obstruction of the hepatic portion of the inferior vena cava in Nepal. J Gastroenterol Hepatol 11(2): 170-9.
Smalberg, JH, Koehler, E, Darwish Murad, S, Plessier, A, Seijo, S, Trebicka, J, et al. (2011). The JAK2 46/1 haplotype in Budd-Chiari syndrome and portal vein thrombosis. Blood.
Smalberg, JH, Murad, SD, Braakman, E, Valk, PJ, Janssen, HL and Leebeek, FW (2006). Myeloproliferative disease in the pathogenesis and survival of Budd-Chiari syndrome. Haematologica 91(12): 1712-3.
Sogaard, KK, Astrup, LB, Vilstrup, H and Gronbaek, H (2007). Portal vein thrombosis; risk factors, clinical presentation and treatment. BMC Gastroenterol 7: 34.
Sogaard, KK, Horvath-Puho, E, Gronbaek, H, Jepsen, P, Vilstrup, H and Sorensen, HT (2009). Risk of venous thromboembolism in patients with liver disease: a nationwide population-based case-control study. Am J Gastroenterol 104(1): 96-101.
Sole, X, Guino, E, Valls, J, Iniesta, R and Moreno, V (2006). SNPStats: a web tool for the analysis of association studies. Bioinformatics 22(15): 1928-9.
Sozer, S, Fiel, MI, Schiano, T, Xu, M, Mascarenhas, J and Hoffman, R (2009). The presence of JAK2V617F mutation in the liver endothelial cells of patients with Budd-Chiari syndrome. Blood 113(21): 5246-9.
Tanaka, M and Wanless, IR (1998). Pathology of the liver in Budd-Chiari syndrome: portal vein thrombosis and the histogenesis of veno-centric cirrhosis, veno-portal cirrhosis, and large regenerative nodules. Hepatology 27(2): 488-96.
76

References.
69
Tefferi, A, Lasho, TL, Patnaik, MM, Finke, CM, Hussein, K, Hogan, WJ, et al. (2010). JAK2 germline genetic variation affects disease susceptibility in primary myelofibrosis regardless of V617F mutational status: nullizygosity for the JAK2 46/1 haplotype is associated with inferior survival. Leukemia 24(1): 105-9.
Tripodi, A, Primignani, M, Chantarangkul, V, Dell'Era, A, Clerici, M, de Franchis, R, et al. (2009). An imbalance of pro- vs anti-coagulation factors in plasma from patients with cirrhosis. Gastroenterology 137(6): 2105-11.
Tsochatzis, E, Venerito, M, Papatheodoridis, GV, Archimandritis, AJ, Monkemuller, K, Malfertheiner, P, et al. (2006). Hepatobiliary and pancreatic: spontaneous splenorenal shunts in portal hypertension. J Gastroenterol Hepatol 21(7): 1214.
Tsochatzis, EA, Senzolo, M, Germani, G, Gatt, A and Burroughs, AK (2010). Systematic review: portal vein thrombosis in cirrhosis. Aliment Pharmacol Ther 31(3): 366-74.
Valla, D (2004). Hepatic venous outflow tract obstruction etiopathogenesis: Asia versus the West. J Gastroenterol Hepatol 19: 204-211.
Valla, D, Casadevall, N, Lacombe, C, Varet, B, Goldwasser, E, Franco, D, et al. (1985). Primary myeloproliferative disorder and hepatic vein thrombosis. A prospective study of erythroid colony formation in vitro in 20 patients with Budd-Chiari syndrome. Ann Intern Med 103(3): 329-34.
Valla, D, Le, MG, Poynard, T, Zucman, N, Rueff, B and Benhamou, JP (1986). Risk of hepatic vein thrombosis in relation to recent use of oral contraceptives. A case-control study. Gastroenterology 90(4): 807-11.
Valla, DC (2009). Primary Budd-Chiari syndrome. J Hepatol 50(1): 195-203. Wanless, IR (2002). Anatomy, histology, embryology and developmental
anomalies of the liver. Sleisenger & Fordtran's Gastrointestinal & Liver Disease M. Feldman, L. S. Friedman and M. Sleisenger, W.B. Saunders Company; 7th edition. 2: 1195-1201.
Vardiman, JW, Thiele, J, Arber, DA, Brunning, RD, Borowitz, MJ, Porwit, A, et al. (2009). The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood 114(5): 937-51.
Vinazzer, H and Pangraz, U (1987). Protein C: comparison of different assays in normal and abnormal plasma samples. Thromb Res 46(1): 1-8.
Virchow, RLK (1856). Virchow RLK. Phlogose und thrombose im Gefäßsystem. Gesammelte Abhandlung zur Wissenchaftlichen Medizin. Frankfurt, Germany.
Xavier, SG, Gadelha, T, Pimenta, G, Eugenio, AM, Ribeiro, DD, Gomes, FM, et al. (2010). JAK2V617F mutation in patients with splanchnic vein thrombosis. Dig Dis Sci 55(6): 1770-7.
77

References
70
Xu, X, Zhang, Q, Luo, J, Xing, S, Li, Q, Krantz, SB, et al. (2007). JAK2(V617F): Prevalence in a large Chinese hospital population. Blood 109(1): 339-42.
Zeitoun, G, Escolano, S, Hadengue, A, Azar, N, El Younsi, M, Mallet, A, et al. (1999). Outcome of Budd-Chiari syndrome: a multivariate analysis of factors related to survival including surgical portosystemic shunting. Hepatology 30(1): 84-9.
Zhang, CQ, Fu, LN, Xu, L, Zhang, GQ, Jia, T, Liu, JY, et al. (2003). Long-term effect of stent placement in 115 patients with Budd-Chiari syndrome. World J Gastroenterol 9(11): 2587-91.
Zhao, R, Xing, S, Li, Z, Fu, X, Li, Q, Krantz, SB, et al. (2005). Identification of an acquired JAK2 mutation in polycythemia vera. J Biol Chem 280(24): 22788-92.
Zocco, MA, Di Stasio, E, De Cristofaro, R, Novi, M, Ainora, ME, Ponziani, F, et al. (2009). Thrombotic risk factors in patients with liver cirrhosis: correlation with MELD scoring system and portal vein thrombosis development. J Hepatol 51(4): 682-9.
The Truth Is Out There!
The X files
78
Recommended