Hemimegalencephaly in an adult with normal intellectual functionand mild epilepsy
ISABELLE BEAULIEU-BOIRE1 | ANNE LORTIE2 | JOHANNE BISSONNETTE3 | SYLVAIN PREVOST4 |DENIS BERGERON5 | CHRISTIAN BOCTI1,6
1 Division of Neurology, Department of Medicine, Centre Hospitalier Universitaire de Sherbrooke, Universit� de Sherbrooke, Sherbrooke, QC. 2 Division of Neuropediatry,Department of Pediatrics, Centre Hospitalier Universitaire Sainte-Justine, Montreal, QC. 3 Division of Neuropediatry, Department of Pediatrics, Centre Hospitalier Universitaire deSherbrooke, Universit� de Sherbrooke, Sherbrooke, QC. 4 Division of Nuclear Medicine and Radiobiology, Centre Hospitalier Universitaire de Sherbrooke, Universit� deSherbrooke, Sherbrooke, QC. 5 Division of Diagnostic Radiology, Centre Hospitalier Universitaire de Sherbrooke, Universit� de Sherbrooke, Sherbrooke, QC. 6 Research Centre onAging, University Institute of Geriatrics of Sherbrooke, Sherbrooke, QC, Canada.
Correspondence to Dr Isabelle Beaulieu-Boire at Division of Neurology, Centre Hospitalier Universitaire de Sherbrooke, 3001 12e Avenue Nord, Sherbrooke, QC, Canada J1H 5N4.E-mail: [email protected]
PUBLICATION DATA
Accepted for publication 26th July 2011.Published online 21st December 2011.
ABBREVIATIONFDG-PET Fluorodeoxyglucose positron
emission tomography
Hemimegalencephaly is a rare congenital brain malformation, usually associated with mental
retardation,* refractory epilepsy, and progressive neurological deficits. We report the case of a
19-year-old female with de novo diagnosis of right hemimegalencephaly, normal intellectual
function, and history of non-refractory epilepsy. She presented with weakness and paraesthesia of
the left leg. Extensive evaluation was negative for other causes for the weakness, which was attrib-
uted to progressive neurological damage secondary to long-standing subclinical epileptic activity
in the hemimegalencephalic hemisphere. This patient underwent a cerebral fluorodeoxyglucose
positron emission tomography that demonstrated near-normal cortical metabolism. Formal
neuropsychological evaluation revealed mild deficits in the affected hemisphere, but preserved
general intellectual function. This case illustrates the wide phenotypic variations in this condition
and raises questions about prenatal counselling for hemimegalencephaly.
CASE REPORTAn otherwise healthy 19-year-old female presented to ourneurology clinic with paresis of the left leg. She experienced rel-atively sudden weakness and numbness of her left leg when shestood up after a prolonged period of sitting 5 days previously.Further questioning raised the possibility of clonic movementsin the period just preceding the appearance of weakness. Thepatient was still able to ambulate even though the symptomspersisted. Her neurological examination showed mild distalweakness of the left lower limb (Medical Research CouncilGrade 4)1 slowed alternate rapid movements on the left sidealong with hyperreflexia, mild spastic hypertonia, and an exten-sor plantar response. Her sensory examination and her visualfields were normal. Her gait appeared spastic with mild stiffnessand circumduction of the left leg. The patient gave written con-sent for the publication of her case.
She had no significant medical history, with unremarkableprenatal and perinatal periods. Her psychomotor develop-ment, including motor milestones, was also normal. Shereported three episodes suggestive of complex partial seizuresin a period of a few months before we assessed her, and neverconsulted a physician for these episodes. She never sufferedfrom a seizure in her childhood. Her family history was
non-contributive. When she presented to us, she was studyingliterature at college and her academic performance wasexcellent. She mentioned difficulties with mathematics andvisuospatial orientation, but performed high above average inforeign languages classes.
Computed tomography revealed hypertrophy of the righthemisphere with massive hypodensity of the white matter asso-ciated with enlargement of the right ventricular system. Brainmagnetic resonance imaging showed increased cortical thick-ness throughout the right hemisphere, with a diffuselyincreased T2-weighted signal of the white matter of the hemi-sphere consistent with gliosis (Figs. 1 and 2). There was bandheterotopia in the frontal region. No acute lesion was identi-fied. Diffusion-weighted imaging was negative. Spinal-cordmagnetic resonance imaging was normal. An electroencephalo-gram showed spikes in the right occipital region and general-ized diffuse slowing of the right hemisphere. A lumbarpuncture was performed and analysis of cerebrospinal fluid wasunremarkable. A fluorodeoxyglucose cerebral positron emis-sion tomography (FDG-PET) scan showed that the corticalglucose metabolism in the right hemisphere was slightlyreduced compared with the left hemisphere but not signifi-cantly decreased relatively to a normal database (Fig. 1).
A diagnosis of right hemimegalencephaly was made. Noconcomitant disease was found to explain the rapid onset of*UK usage: learning disability.
284 DOI: 10.1111/j.1469-8749.2011.04136.x ª The Authors. Developmental Medicine & Child Neurology ª 2011 Mac Keith Press
DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY CASE REPORT
paralysis of the left leg. She was started on carbamazepineconsidering the history of complex partial seizures and thepositive findings on electroencephalogram. She was sent homewith a reference in physiotherapy to improve her left legmotor function.
After discharge, the patient went through a standardizedneuropsychological evaluation, including Wechsler AdultIntelligence Scale 3rd edition, Rey figure, Delis-Kaplan Exec-utive Function System, Wechsler Memory Scale 3rd edition,California Verbal Learning Test 2nd edition, and HooperVisual Organisation Test. The results showed a global cogni-tive performance around average (42nd centile), with a smallbut non-significant difference between verbal (47th centile)and non-verbal (34th centile) performance. The evaluationalso demonstrated minimal slowing of visuoattentional pro-cesses and attention tasks, mild difficulty with visuospatialanalysis and integration, and excellent verbal memory.
At follow-up, her neurological deficits were stable. She hadstopped her antiepileptic medication on her own, but reportedepisodes suggestive of secondary generalized tonic–clonicseizures and was put back on carbamazepine, with subsequentseizure-free status after more than 1 year of follow-up. Con-trol magnetic resonance imaging did not show any significantchange.
DISCUSSIONHemimegalencephaly is a rare congenital brain malformationconsisting of abnormal migration and proliferation of neuronsand glial cells leading to hypertrophy of the cerebral hemi-sphere.2,3 This syndrome may occur in isolation, or in associa-
a b
Compressed 7:1IM: 13 SE: 8
Compressed 7:1IM: 11 SE: 7
cm
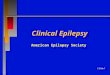
Figure 2: (a) Coronal real inversion recovery and (b) T2-weighted magnetic resonance imaging showing diffuse enlargement of the right cerebral hemi-sphere, right ventriculomegaly, enlarged perivascular spaces, and diffuse white matter anomalies.
–14.5mm –14.5mm –14.5mma b c
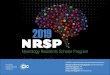
Figure 1: (a) Axial T2-weighted magnetic resonance imaging showing diffuse enlargement of the right cerebral hemisphere, right ventriculomegaly, anddiffuse white matter anomalies. (b) Axial view on the cerebral fluorodeoxyglucose positron emission tomography scan showing mildly reduced metabolism inthe right hemisphere cortex, but not statistically different from (c) a normal database, the significant deficits being limited to white matter.
What this paper adds• New insight into the phenotypic variability of hemimegalencephaly.• It is the first report of normal cortical function on fluorodeoxyglucose positron
emission tomography in hemimegalencephaly.
Case Report 285

tion with neurocutaneous syndromes or hemigigantism.3 It isusually associated with severe epileptic disorders, focal neuro-logical deficits, macrocrania, and mild to severe mental retar-dation.3 Seizures are usually refractory to medical treatmentand often necessitate surgical treatment consisting in hemi-spherectomy or hemispherotomy.4
To our knowledge, patients with hemimegalencephaly haverarely been reported to reach adulthood without necessitatingantiepileptic agents.4 In the case of our patient, she experi-enced a few complex partial seizures in her life, only in lateadolescence, but did not reach medical attention for this prob-lem. She responded well to carbamazepine with no recurrenceof seizures, which is quite surprising in the context ofhemimegalencephaly.
Very few cases of normal intellectual development in adultswith hemimegalencephaly have been described in the litera-ture.5 It is usually recognized that the extent of the malforma-tion is correlated with the degree of intellectual impairment.6
Interestingly, the neuropsychological evaluation did not revealsignificant differences between the functions classically associ-ated with right or left hemispheres, possibly reflecting com-pensation from neuronal plasticity in this long-standingmalformation. Also, preservation of near-normal metabolicfunction in the cortex, as demonstrated on FDG-PET scan,could explain that deficits were relatively mild on neuro-cognitive testing. To our knowledge, the only report of a PETscan in an adult with hemimegalencephaly demonstratedhypometabolism in the megalencephalic cortex; indeed, thispatient had mental retardation and drug-resistant epilepsy.7 Ina small series of children, normal metabolism in the affectedhemisphere was observed not so infrequently, however, inthree patients out of nine.8 Hemimegalencephaly in childrenwas reported to be associated not only with ipsilateral but alsocontralateral dysfunction on FDG-PET imaging.9 In thissame report, contralateral hypometabolism was related to aworse prognosis. This could suggest that cortical metabolism
on PET scan could be related to intellectual function inhemimegalencephaly.
The relatively sudden appearance of paresis of her left leg isalso an uncommon presentation in hemimegalencephaly. Noreports of association of hemimegalencephaly with vascularevents or demyelinating plaques have been described in theliterature. To our knowledge, this is the first reported case ofa sudden neurological deficit in an adult patient withhemimegalencephaly.Considering the fact that the neurologicaldeficit is concordant with the side of the hemimegalencephaly,with temporal coincidence with partial seizures of the same dis-tribution, it could be explained by repeated epileptic activityinducing permanent damage to cerebral structures. Anotherhypothesis is that the neurological deficit was perhaps alreadypresent in the past, but another process such as new-onset partialseizures resulted in a sudden awareness of the problem. This lastpossibility seems unlikely given the history of normal perfor-manceinphysical activitiesprevious to theacuteepisode.
In conclusion, hemimegalencephaly is a rare cerebral mal-formation usually associated with severe mental retardation,epilepsy, and progressive neurological deficits. The case of ourpatient, who had normal intellectual development, is quiteatypical for hemimegalencephaly, but has been described inprevious case reports and demonstrates the incredible pheno-typic variability in these patients. This raises an ethical issue asto prenatal counselling of mothers with hemimegalencephalyfound in the fetus, considering the occasional favourable evo-lution. This case is also the first demonstration of normalmetabolism of the cortex in hemimegalencephaly in an adultpatient. FDG-PET seems to be a valuable imaging procedurein hemimegalencephaly, and further reports should helpdefine the prognostic value in these patients.
ACKNOWLEDGEMENTSWe thank Marie Farmer, Division of Neuropediatry, Department of
Pediatrics, Centre Hospitalier Universitaire de Sherbrooke.
REFERENCES
1. Campbell WW, DeJong RN, Haerer AF. Motor strength
and power. In: Campbell W, editor. DeJong’s The Neuro-
logic Examination. 6th edn. Philadelphia, PA: Lippincott
Williams and Wilkins, 2005: 344–6.
2. Manoranjan B, Provias JP. Hemimegalencephaly: a fetal case
with neuropathological confirmation and review of the litera-
ture. Acta Neuropathol 2010; 120: 117–30.
3. Di Rocco C, Battaglia D, Pietrini D, Piastra M, Massimi L.
Hemimegalencephaly: clinical implications and surgical
treatment. Childs Nerv Syst 2006; 22: 852–66.
4. Ohtsuka Y, Ohno S, Oka E. Electroclinical characteristics of
hemimegalencephaly. Pediatr Neurol 1999; 20: 390–3.
5. Fusco L, Ferracuti S, Fariello G, Manfredi M, Vigevano F.
Hemimegalencephaly and normal intellectual development.
J Neurol Neurosurg Psychiatry 1992; 55: 720–2.
6. Civardi C, Vicentini R, Collini A, Boccagni C, Cantello R,
Monaco F. Motor cortical organization in an adult with
hemimegalencephaly and late onset epilepsy. Neurosci Lett
2009; 460: 126–9.
7. Hoffmann KT, Amthauer H, Liebig T, et al. MRI and 18F-
fluorodeoxyglucose positron emission tomography in
hemimegalencephaly. Neuroradiology 2000; 42: 749–52.
8. Uematsu M, Haginoya K, Togashi N, et al. Unique discrep-
ancy between cerebral blood flow and glucose metabolism in
hemimegalencephaly. Epilepsy Res 2010; 92: 201–8.
9. Rintahaka PJ, Chugani HT, Messa C, Phelps ME. Hemi-
megalencephaly: evaluation with positron emission tomogra-
phy. Pediatr Neurol 1993; 9: 21–8.
286 Developmental Medicine & Child Neurology 2012, 54: 284–286
Recommended
![E-ISSN: The antihyperglycemic, antioxidant and ... · Ehretia cymosa Thon. ... epilepsy, convulsions and spasm and toothache [15]. The sap from the fresh leaves is used as a mild](https://img.pdfslide.us/doc/110x75/5aeb12de7f8b9ac3618eaefb/e-issn-the-antihyperglycemic-antioxidant-and-cymosa-thon-epilepsy-convulsions.jpg)