Hematology M & Ms: Morphology and Mystery (Case Studies)
Karen A. Brown, MS, MASCP, MLS(ASCP)CM
Adjunct Professor
Department of Pathology
University of Utah School of Medicine
and ARUP Laboratories
Salt Lake City, Utah
California Association for Medical Technology
Spring Seminar South Series
North Hollywood, CA
March 15, 2020
2
Workshop Description
Hematology instrumentation has advanced to now routinely include a five-part
differential and, in some laboratories, automated cell image analysis. Yet, a manual
examination of the blood smear is still an essential procedure that provides valuable
diagnostic information. This session will use case studies to define important
morphologic variations and physiologic processes in selected disease conditions.
At the conclusion of this workshop, participants will be able to accurately:
1. Morphologically differentiate abnormal variations in RBCs, WBCs, and platelets.
2. Explain underlying physiological processes for abnormal RBC, WBC, and
platelet morphology.
3. Describe the morphologic basis for distinguishing benign from malignant WBC
disorders.
4. Correlate abnormal cellular morphologic variations with selected case studies.
3
I. Introduction
II. Common RBC Morphologic Variations
Even with automated differentials, a review of the peripheral blood (PB) smear is
still very important! Many diseases/conditions result in normal blood counts but
abnormal cellular morphology when a smear is reviewed. Some examples:
malaria, hereditary spherocytosis, and infectious mononucleosis.
Key to morphologic review: A properly prepared, well-stained smear that is
reviewed in the optimum area of the slide. RBCs are usually evaluated for:
Size
Shape
Hemoglobin content
Distribution and
Inclusions
III. Leukocyte Identification Criteria
Again, a properly prepared, well-stained smear that is evaluated in the optimum
area of the smear is key to a morphologic review of WBCs.
A. Characteristics of Normal Cells
1. Overall cell size
-immature cell usually larger
2. Nuclear/Cytoplasmic ratio
-nuclear size decreases as cell matures
3. Nucleus
(a) shape
-lobes may develop as cell matures
(b) color
-changes from pinkish purple to dark purple
(c) chromatin pattern
-condenses as cell matures
(d) presence/absence of nucleoli
-nucleoli usually associated with immaturity
4. Cytoplasm
(a) color
-immature cytoplasm stains a deep blue
(b) presence/absence of granules
(c) size and color of granules
4
B. Identification Criteria – Malignant Cells
1. Cellular
(a) size
-abnormally large or abnormally small
(b) clonality
-all abnormal cells appear similar
2. Nuclear
(a) shape
(1) clefting
(2) contortions
(3) pseudo-Pelger-Huët
(b) size
-multinuclearity
(c) chromatin pattern
(d) nucleoli
giant or prominent
(e) megaloblastoid features
– nuclear/cytoplasmic asynchrony
– unresponsive to B12 or folate
(f) increase in mitotic figures
3. Cytoplasmic
(a) granulation
(1) Auer rods
(2) mixed, basophilic and eosinophilic
(3) decreased (hypogranulation)
(b) increased fragility
-cytoplasmic fragmentation
IV. Platelets
Platelets are also evaluated on the peripheral blood smear for numbers and
for size. Platelets as large as RBCs are considered to be “giant”. Generally,
enlarged and giant platelets represent younger cells.
5
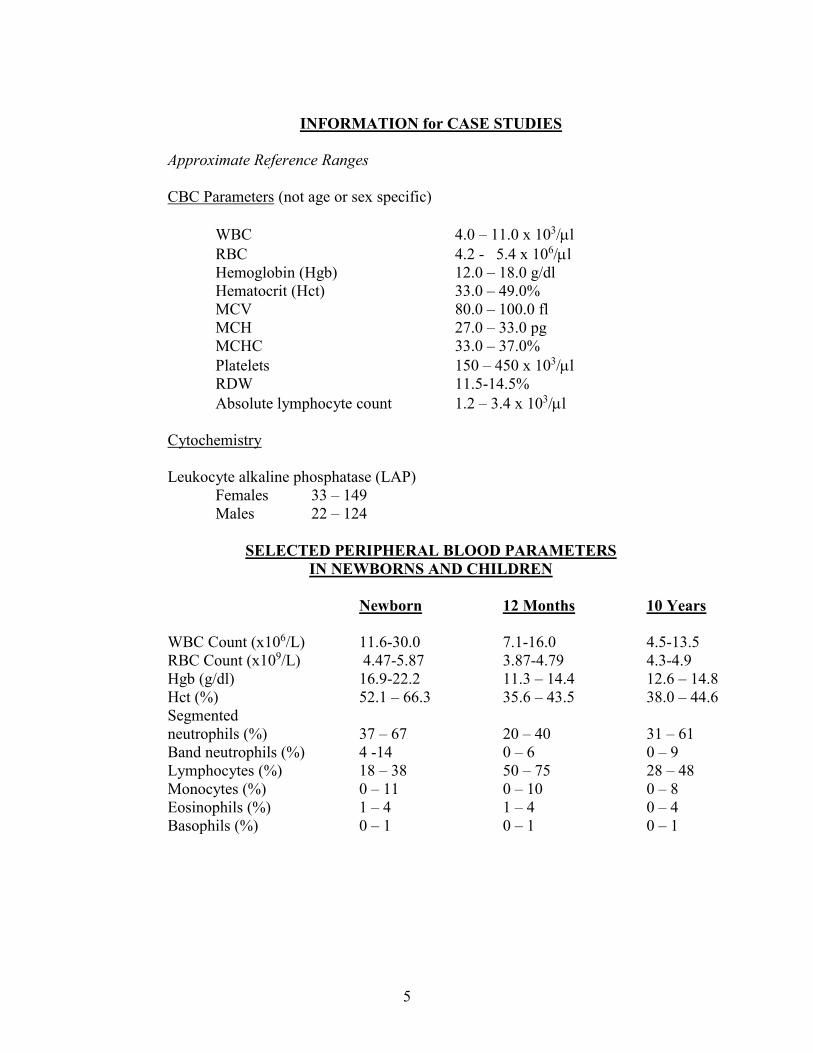
INFORMATION for CASE STUDIES
Approximate Reference Ranges
CBC Parameters (not age or sex specific)
WBC 4.0 – 11.0 x 103/l
RBC 4.2 - 5.4 x 106/l
Hemoglobin (Hgb) 12.0 – 18.0 g/dl
Hematocrit (Hct) 33.0 – 49.0%
MCV 80.0 – 100.0 fl
MCH 27.0 – 33.0 pg
MCHC 33.0 – 37.0%
Platelets 150 – 450 x 103/l
RDW 11.5-14.5%
Absolute lymphocyte count 1.2 – 3.4 x 103/l
Cytochemistry
Leukocyte alkaline phosphatase (LAP)
Females 33 – 149
Males 22 – 124
SELECTED PERIPHERAL BLOOD PARAMETERS
IN NEWBORNS AND CHILDREN
Newborn 12 Months 10 Years
WBC Count (x106/L) 11.6-30.0 7.1-16.0 4.5-13.5
RBC Count (x109/L) 4.47-5.87 3.87-4.79 4.3-4.9
Hgb (g/dl) 16.9-22.2 11.3 – 14.4 12.6 – 14.8
Hct (%) 52.1 – 66.3 35.6 – 43.5 38.0 – 44.6
Segmented
neutrophils (%) 37 – 67 20 – 40 31 – 61
Band neutrophils (%) 4 -14 0 – 6 0 – 9
Lymphocytes (%) 18 – 38 50 – 75 28 – 48
Monocytes (%) 0 – 11 0 – 10 0 – 8
Eosinophils (%) 1 – 4 1 – 4 0 – 4
Basophils (%) 0 – 1 0 – 1 0 – 1
6
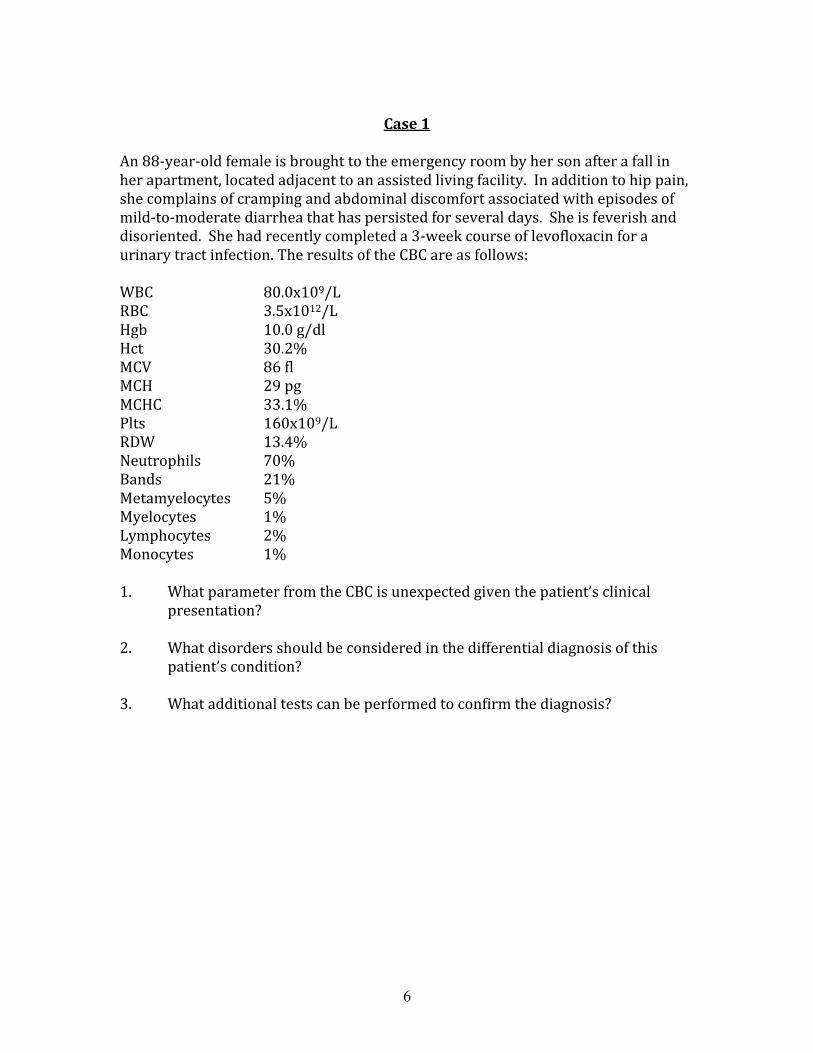
Case 1
An 88-year-old female is brought to the emergency room by her son after a fall in her apartment, located adjacent to an assisted living facility. In addition to hip pain, she complains of cramping and abdominal discomfort associated with episodes of mild-to-moderate diarrhea that has persisted for several days. She is feverish and disoriented. She had recently completed a 3-week course of levofloxacin for a urinary tract infection. The results of the CBC are as follows: WBC 80.0x109/L RBC 3.5x1012/L Hgb 10.0 g/dl Hct 30.2% MCV 86 fl MCH 29 pg MCHC 33.1% Plts 160x109/L RDW 13.4% Neutrophils 70% Bands 21% Metamyelocytes 5% Myelocytes 1% Lymphocytes 2% Monocytes 1% 1. What parameter from the CBC is unexpected given the patient’s clinical
presentation? 2. What disorders should be considered in the differential diagnosis of this
patient’s condition? 3. What additional tests can be performed to confirm the diagnosis?
7
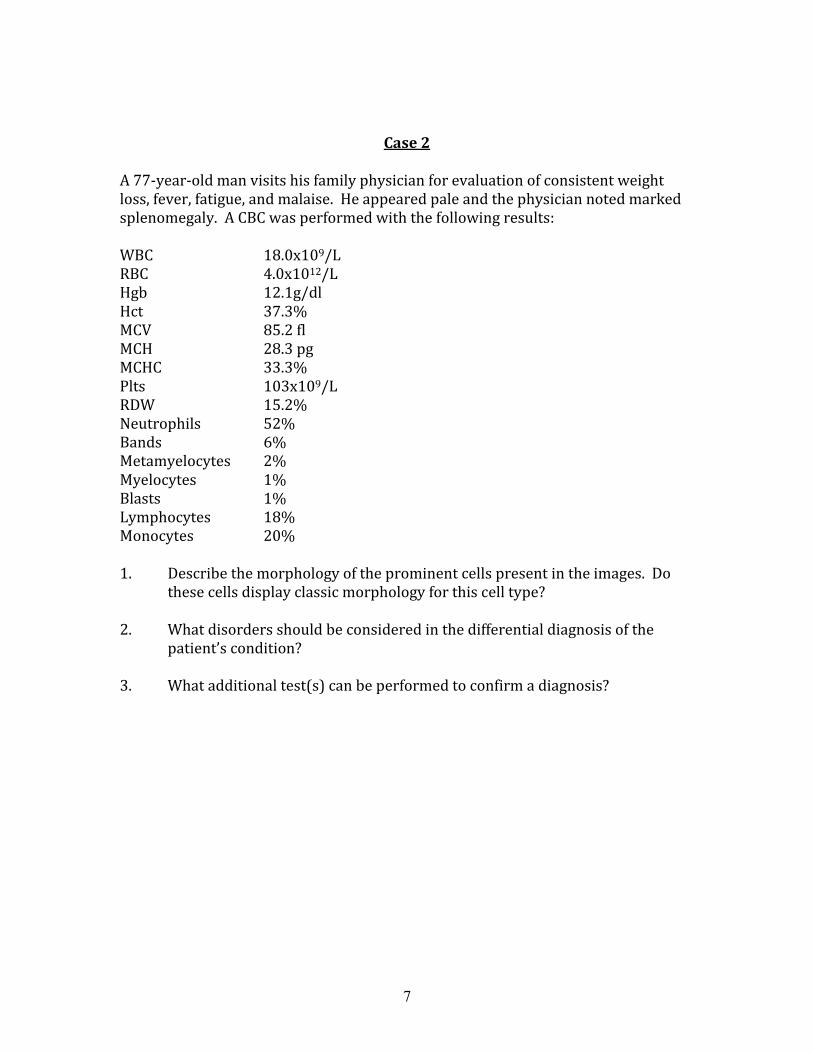
Case 2 A 77-year-old man visits his family physician for evaluation of consistent weight loss, fever, fatigue, and malaise. He appeared pale and the physician noted marked splenomegaly. A CBC was performed with the following results: WBC 18.0x109/L RBC 4.0x1012/L Hgb 12.1g/dl Hct 37.3% MCV 85.2 fl MCH 28.3 pg MCHC 33.3% Plts 103x109/L RDW 15.2% Neutrophils 52% Bands 6% Metamyelocytes 2% Myelocytes 1% Blasts 1% Lymphocytes 18% Monocytes 20% 1. Describe the morphology of the prominent cells present in the images. Do
these cells display classic morphology for this cell type? 2. What disorders should be considered in the differential diagnosis of the
patient’s condition? 3. What additional test(s) can be performed to confirm a diagnosis?
8
Case 3
This 60-year-old man presented to his physician complaining of fever, night sweats, fatigue, and weight loss. Physical examination revealed generalized lymphadenopathy and splenomegaly. He was admitted to a hospital for further evaluation. His hematologic results were reported as: WBC 78.4x109/L RBC 2.10x1012/L Hgb 6.7g/dl Hct 19.7% MCV 93.4 fl MCH 31.9 pg MCHC 34.1% Plts 55.0x109/L RDW 23.9% Neutrophils 2% Lymphocytes 2% Monocytes 2% Blasts 94% 1. What is unusual about the “blasts” reported on the manual differential cell
count? 2. Why is it significant to recognize the abnormal morphology of these cells? 3. Why is the patient neutropenic, anemic, and thrombocytopenic? 4. What contributions would immunophenotyping and cytogenetics make to
the diagnosis of this condition?
9
Case 4
A Caucasian male in his early thirties presented at the Emergency Room with a nosebleed that could not be controlled. He reported that similar episodes of epistaxis occurred through his childhood. Once, when he was a toddler, his parents panicked when mucosal bleeding became so severe it could not be stopped. They took him to the hospital where he received a blood transfusion. He did not need any transfusions in high school, but he was not permitted to play any contact sports. His bleeding episodes resumed after high school and he has been transfusion-dependent ever since, though only platelets are usually transfused now. In one year, he received five transfusions to support an uncontrolled bleeding event. The family history is negative and no other relatives are affected. A CBC showed the following:
WBC 9.6x109/L RBC 5.2x1012/L Hgb 15.0 g/dl Hct 46.1% MCV 90 fl MCH 32.3 pg MCHC 33% Plts 2.0x109/L RDW 12%
1. What results are abnormal from the data presented? 2. Identify any abnormal findings from the images of the peripheral blood. 3. What is a suggested diagnosis of this man’s condition? 4. What is the underlying defect that results in this condition? 5. What test(s) can be performed to confirm the diagnosis? 6. What is the explanation for a negative family history of this condition?
10
Case 5
A 40-year-old man with a history of glucose-6-phosphate dehydrogenase (GGPD) deficiency is admitted to University Hospital with recent onset of jaundice and fatigue. His medical history also included a splenectomy five years previously. The attending physician orders a CBC and reticulocyte count and results are listed below. WBC 9.2x109/L RBC 1.99x1012/L Hgb 8.1 g/dl Hct 24.5% MCV 122.9 fl MCH 40.9 pg MCHC 33.3% Plts 1108x109/L RDW 14.2% Retics 71.6% 1. What is the relationship between the elevated MCV and the reticulocyte count? 2. What effect does the patient’s splenectomy have on the RBC morphology noted
in the peripheral blood images? 3. What is the etiology and pathophysiology associated with G6PD? 4. What information from a patient history is needed to explain the acute hemolytic
episode?
11
Case 6
The parents of a 10-year-old girl take her to a pediatrician for evaluation of joint and abdominal pain. The young girl has complained of these symptoms for two weeks. The physician notices an enlarged spleen on physical examination and orders a CBC and results are as follows: WBC 44.1x106/L RBC 4.47x1012/L Hgb 11.7 g/dl Hct 31.4% MCV 70.2 fl MCH 26.0 pg MCHC 37.1% Plts 212x106/L RDW 19.8% 1. What abnormal RBC morphologies are present in the Wright-stained
peripheral blood? 2. What is the most likely diagnosis of this patient’s condition? 3. What additional test can be performed to confirm the diagnosis? 4. Is the elevated WBC significant in this disorder?
12
Case 7
An 8-year-old African-American girl was brought to her physician for evaluation of right upper quadrant pain. She has a lifelong history of hemolytic anemia. A CBC was performed and the results are as follows: WBC 8.2x109/L RBC 4.3x1012/L Hgb 10.7 g/dl Hct 29.2% MCV 67.9 fl MCH 24.8 pg MCHC 36.6% Plts 480x109/L RDW 16.2% 1. What abnormal RBC morphologies are present on the Wright-stained
peripheral blood smear represented in the pictures? 2. What disorders should be considered in a differential diagnosis? 3. What is the most likely explanation of this child’s condition?
Case 8
A 28-year-old man suffers from persistent and chronic diarrhea of approximately 2-months duration. He has also experienced abnormal cramps, fatigue, and weight loss. He is a Medical Laboratory Scientist and performs a CBC as a first step in the evaluation of his disorder. WBC 3.5x109/L RBC 5.4x1012/L Hgb 14.0 g/dl Hct 42.2% MCV 74.8 fl MCH 24.8 pg MCHC 33.1% Plts 304x109/L RDW 14.5% 1. What disorders should be considered in a differential diagnosis of this man’s
condition? 2. What is the most likely explanation of the man’s disorder? 3. What additional test should be performed to confirm a diagnosis?
13
Case 9
A 33-year-old female from Guyana has experienced chronic low-level bone and joint pain all her life. At times, she is also so tired and weak she can not get out of bed in the morning. These episodes of extreme weakness can last for several days. She visits her physician for a routine evaluation of her condition. Results of a CBC are as follows: WBC 17.5x109/L RBC 2.55x1012/L Hgb 7.2 g/dl Hct 23.5% MCV 89.5 fl MCH 28.9 pg MCHC 30.6% Plts 250x109/L RDW 18.1% 1. What abnormal morphologies are present in the Wright-stained peripheral
blood? 2. What is the diagnosis of this patient’s condition? 3. What is the relationship between the abnormally shaped erythrocytes and
the patient’s clinical symptoms?
Case 10
This patient was a previously healthy 18-year-old white female who initially presented to the
Emergency Room of a Montana hospital after a skiing accident in which she suffered abdominal
trauma. An abdominal CT scan showed a large hemoperitoneum while a resulting exploratory
laparotomy indicated a laceration of the left ovary. The injury was repaired, but the patient
received three units of autologous blood intraoperatively and two units packed red blood cells
postoperatively. The patient was stable until four days later, when she developed postoperative
bleeding, epistaxis, and vaginal bleeding.
She was subsequently transfused with significant amounts of packed red blood cells and fresh
frozen plasma, but the hemorrhaging continued. Therefore, five days later, she was transferred
to the University of Utah Medical Center for further evaluation and therapy.
14
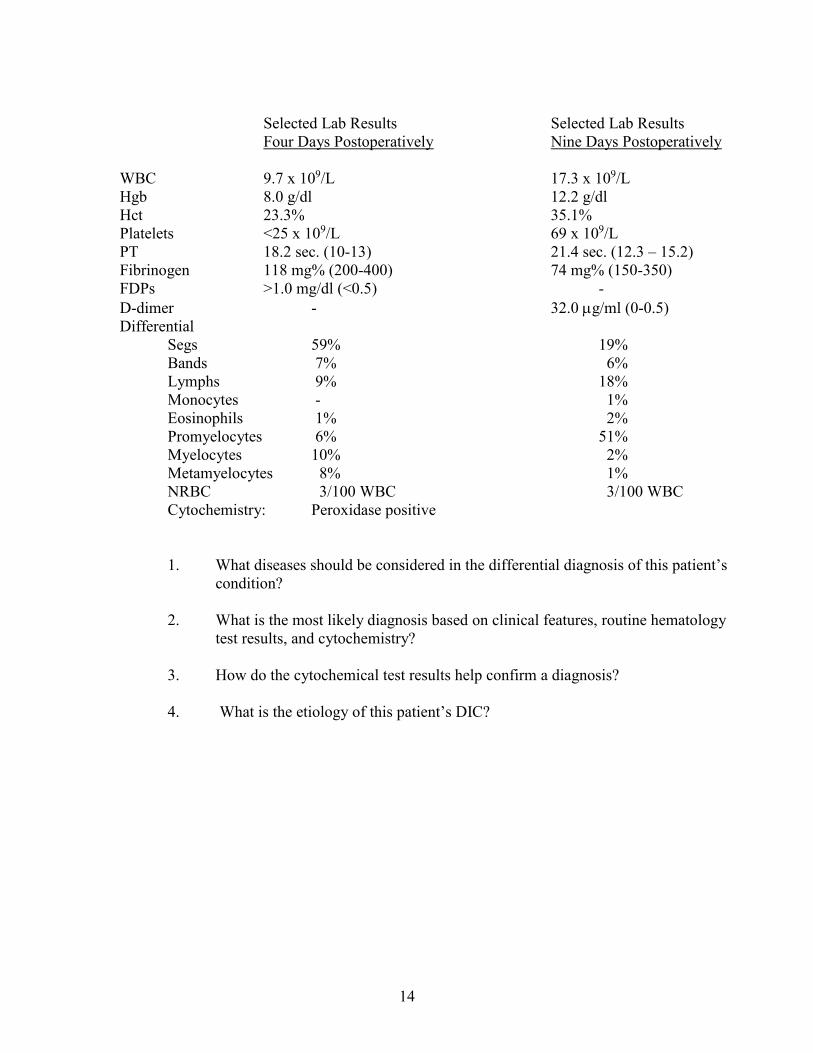
Selected Lab Results Selected Lab Results
Four Days Postoperatively Nine Days Postoperatively
WBC 9.7 x 109/L 17.3 x 109/L
Hgb 8.0 g/dl 12.2 g/dl
Hct 23.3% 35.1%
Platelets <25 x 109/L 69 x 109/L
PT 18.2 sec. (10-13) 21.4 sec. (12.3 – 15.2)
Fibrinogen 118 mg% (200-400) 74 mg% (150-350)
FDPs >1.0 mg/dl (<0.5) -
D-dimer - 32.0 g/ml (0-0.5)
Differential
Segs 59% 19%
Bands 7% 6%
Lymphs 9% 18%
Monocytes - 1%
Eosinophils 1% 2%
Promyelocytes 6% 51%
Myelocytes 10% 2%
Metamyelocytes 8% 1%
NRBC 3/100 WBC 3/100 WBC
Cytochemistry: Peroxidase positive
1. What diseases should be considered in the differential diagnosis of this patient’s
condition?
2. What is the most likely diagnosis based on clinical features, routine hematology
test results, and cytochemistry?
3. How do the cytochemical test results help confirm a diagnosis?
4. What is the etiology of this patient’s DIC?
15
Case 11
A 25-year-old female complained of headache, fatigue and shortness of breath for several days.
After developing a rash on her trunk and extremities, she was admitted to a local hospital. Three
days after admission, she developed a sore throat, enlarged lymph nodes, fluctuating fever and
enlarged spleen. Laboratory data are as follows:
WBC 8.1 x 103/l
Hemoglobin 13.0 g/dl
Hematocrit 39.0%
Segs 30%
Lymphs 60%
Monos 5%
Eosinophils 5%
1. What is the patient’s absolute lymphocyte count? Is this considered normal?
2. What disorders should be considered in the differential diagnosis of this patient’s
condition?
3. Is this case representative of a benign process or a malignant process? What is
the most probable diagnosis of this patient’s condition?
4. What additional tests should be performed to confirm a diagnosis?
16
Case 12
This adult male was evaluated in the outpatient hematology clinic for a possible anemia.
Results of a CBC are as follows:
WBC 4.8 x 103/µl
RBC 2.03 x 106/µl
Hgb 8.5 g/dl
Hct 24.8%
MCV 121.9 fl
MCH 42.1 pg
MCHC 34 .5%
Plts 107 x 103/µ1
What is the most probable diagnosis of this patient's condition?
Macrocytic anemias
Causes
Laboratory evaluation and results
Non-megaloblastic macrocytosis

17
REFERENCES
1. Carr, J. and Rodak, B., Clinical Hematology Atlas, third edition, W.B.
Saunders, 2009.
2. Clinical and Laboratory Standards Institute, Reference Leukocyte (WBC)
Differential Count (Proportional) and Evaluation of Instrumental Methods,
Approved Standard, 2nd edition, H20-A2, 2007.
3. Gulati, G. and Cara, J., Blood Cells Morphology & Clinical Relevance, second
edition, ASCP Press, 2014.
4. Harmening, D., Clinical Hematology and Fundamentals of Hemostasis, fifth
edition, F.A. Davis, 2009.
5. Kjeldsberg, C., and Perkins, S., editors, Practical Diagnosis of Hematologic
Disorders, fifth edition, ASCP Press, 2010.
6. McKenzie, S., Landis-Pinowar, K., and Williams, L., Clinical Laboratory
Hematology, fourth edition, Pearson, 2020.
7. Keohane, E., Otto, C., and Walenga, J., Rodak’s Hematology Clinical
Principles and Applications, Elsevier, 2020.
8. http://emedicine.medscape.com
2-15-14; 1-27-16; 4-3-18; 12-11-18; 1-15-20
Recommended