THE COMMONWEALTH
FUND
Health Care Reform Proposals of Health Care Reform Proposals of the 2008 Presidential Electionthe 2008 Presidential Election
Sara R. Collins, Ph.D. Sara R. Collins, Ph.D. Assistant Vice PresidentAssistant Vice President
The Commonwealth FundThe Commonwealth FundThe National Congress on the Un and Under InsuredThe National Congress on the Un and Under Insured
Washington, D.C.Washington, D.C.December 11, 2007December 11, 2007

THE
COMMONWEALTH FUND
2Why Does the Current Health Insurance System Why Does the Current Health Insurance System Fail to Promote High Performance? Fail to Promote High Performance?
• Access to care is unequal• Poor access to care is linked to poor
quality• Care delivery is inefficient• Fragmented health insurance system
makes it difficult to control costs• Financing of care for uninsured and
underinsured families is inefficient• Positive incentives in benefit design and
insurance markets are lacking

THE
COMMONWEALTH FUND
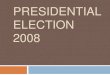
3Employers Provide Health Benefits to More than Employers Provide Health Benefits to More than 160 Million Working Americans and Family Members160 Million Working Americans and Family Members
Source: S. R. Collins, C. White, and J. L. Kriss, Whither Employer-Based Health Insurance? The Current and Future Role of U.S. Companies in the Provision and Financing of Health Insurance (New York: The Commonwealth Fund, Sept. 2007).Data: Current Population Survey, Mar. 2007.
Uninsured47.0
(16%) Employer 163.3(55%)
Numbers in millions, 2006
Medicaid27.9(9%)
Medicare39.1
(13%)
Total population = 296.7 Under-65 population = 260.7
Employer 160.8(62%)
Uninsured46.4
(18%)
Medicaid27.9
(11%)
Medicare6.4
(2%)
Military3.4
(1%)Military
3.4(1%)
Individual16.0(5%) Individual
15.8(6%)

THE
COMMONWEALTH FUND
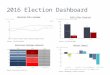
4Employer-Provided Health Insurance, Employer-Provided Health Insurance, by Income Quintile, 2000–2006by Income Quintile, 2000–2006
88% 88% 87% 87% 87% 87% 86%86% 85% 84% 84% 83% 82% 82%77% 77% 75% 74% 74% 72% 72%
62% 60% 57% 55% 54% 54% 53%
22%29% 26% 25% 23% 23% 22%
0%10%20%30%40%50%60%70%80%90%
100%
2000 2001 2002 2003 2004 2005 2006
HighestQuintile
Fourth
Third
Second
Lowestquintile
Percent of population under age 65 with health benefits from employer
Source: E. Gould, The Erosion of Employment-Based Insurance: More Working Families Left Uninsured,EPI Briefing Paper No. 203 (Washington, D.C.: Economic Policy Institute, Nov. 2007).

THE
COMMONWEALTH FUND
5
0
50
100
150
200
250
300
350
Tenn
esse
eN
orth
Dak
ota
Mon
tana
Sout
h C
arol
ina
Alas
kaId
aho
Neb
rask
aO
klah
oma
Ore
gon
Wis
cons
inAl
abam
aAr
izon
aAr
kans
asC
olor
ado
Del
awar
e
Dis
trict
of C
olum
bia
Flor
ida
Illin
ois
Indi
ana
Iow
aKa
nsas
Kent
ucky
Loui
sian
aM
aine
Mic
higa
nM
issi
ssip
piN
evad
aN
orth
Car
olin
aO
hio
Penn
sylv
ania
Sout
h D
akot
aTe
xas
Uta
hVi
rgin
iaW
yom
ing
Wes
t Virg
inia
Geo
rgia
New
Mex
ico
Cal
iforn
iaN
ew Y
ork
Rho
de Is
land
Was
hing
ton
Min
neso
taC
onne
ctic
utH
awai
iM
aryl
and
Mas
sach
uset
tsM
isso
uri
New
Ham
pshi
reVe
rmon
tN
ew J
erse
y
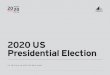
States’* Medicaid/SCHIP eligibility levels for children (% of federal poverty level)
Source: Kaiser Family Foundation, “Income Eligibility Levels for Children’s Separate SCHIP Programs, 2006” available online at http://www.statehealthfactsonline.org, accessed on February 9, 2007.
States’ Income Eligibility Levels for Medicaid/SCHIP States’ Income Eligibility Levels for Medicaid/SCHIP for Childrenfor Children

THE
COMMONWEALTH FUND
6
0
50
100
150
200
250
300
350
Arka
nsas
Loui
sian
aAl
abam
aIn
dian
aTe
xas
Virg
inia
Mis
siss
ippi
Kans
asW
est V
irgin
iaM
isso
uri
Idah
oO
klah
oma
Nor
th C
arol
ina
Geo
rgia
New
Ham
pshi
reW
yom
ing
Flor
ida
Neb
rask
aSo
uth
Dak
ota
Mic
higa
nM
onta
naN
ew M
exic
oN
orth
Dak
ota
Kent
ucky
Col
orad
oTe
nnes
see
Alas
kaN
evad
aO
hio
Sout
h C
arol
ina
Haw
aii
Ore
gon
Cal
iforn
iaD
elaw
are
New
Jer
sey
Mar
ylan
dN
ew Y
ork
Uta
hC
onne
ctic
utIll
inoi
sR
hode
Isla
ndVe
rmon
tW
isco
nsin
Airz
ona
Iow
aPe
nnsy
lvan
iaW
ashi
ngto
n
Dis
trict
of C
olum
bia
Mai
neM
inne
sota
Mas
sach
uset
ts
States’* Medicaid/SCHIP eligibility levels for parents (% of federal poverty level)
Source: Kaiser Family Foundation, “Income Eligibility for Parents applying for Medicaid, 2006” available online at http://www.statehealthfactsonline.org, accessed on February 9, 2007.
States’ Income Eligibility Levels for Medicaid/SCHIP States’ Income Eligibility Levels for Medicaid/SCHIP for Parentsfor Parents

THE
COMMONWEALTH FUND
7
050
100150200250300350
Alab
ama
Alas
kaAr
kans
asC
alifo
rnia
Col
orad
oC
onne
ctic
utFl
orid
aG
eorg
iaId
aho
Illin
ois
Indi
ana
Kans
asKe
ntuc
kyLo
uisi
ana
Mis
siss
ippi
Mis
sour
iM
onta
naN
ebra
ska
Nev
ada
New
Ham
pshi
reN
ew M
exic
oN
orth
Car
olin
aN
orth
Dak
ota
Ohi
oO
klah
oma
Rho
de Is
land
Sout
h C
arol
ina
Sout
h D
akot
aTe
nnes
see
Texa
sVi
rgin
iaW
est V
irgin
iaW
isco
nsin
Wyo
min
gM
ichi
gan
Ariz
ona
Del
awar
eH
awai
iM
aine
New
Jer
sey
New
Yor
kO
rego
nM
aryl
and
Uta
hVe
rmon
tM
inne
sota
Dis
trict
of C
olum
bia
Iow
aPe
nnsy
lvan
iaW
ashi
ngto
nM
assa
chus
etts
States’* Medicaid/SCHIP eligibility levels for non-parent adults (% of federal poverty level)
Source: State Coverage Initiatives, current as of October 2006.
States’ Income Eligibility Levels for Medicaid/SCHIP States’ Income Eligibility Levels for Medicaid/SCHIP for Non-Parent Adultsfor Non-Parent Adults

THE
COMMONWEALTH FUND
8
Adults ages 19–64 with individual coverage or who thought about or tried to buy it in past 3 years who: Total
Health Problem
No Health
Problem<200% Poverty
200%+ Poverty
Found it very difficult or impossible to find coverage they needed
34% 48% 24% 43% 29%
Found it very difficult or impossible to find affordable coverage
58 71 48 72 50
Were turned down or charged a higher price because of a pre-existing condition
21 33 12 26 18
Never bought a plan 89 92 86 93 86
Individual Market Is Not an Affordable Option Individual Market Is Not an Affordable Option for Many Peoplefor Many People
Source: S.R. Collins, J.L. Kriss, K. Davis, M.M. Doty, A.L. Holmgren, Squeezed: Why Rising Exposure to Health Care Costs Threatens the Health and Well-being of American Families, The Commonwealth Fund, September 2006.

47 Million Uninsured in 2006, Increase of 8.6 Million Since 2000, Adults Under-65 Accounted for Most of the Increase
WA
ORID
MT ND
WY
NV
CAUT
AZ NM
KS
NE
MN
MO
WI
TX
IA
ILIN
AR
LA
AL
SCTN
NCKY
FL
VA
OH
MI
WV
PA
NY
AK
MD
MEVTNH
MARI
CT
DE
DC
HI
CO
GAMS
OK
NJ
SD
WA
ORID
MT ND
WY
NV
CAUT
AZ NM
KS
NE
MN
MO
WI
TX
IA
ILIN
AR
LA
AL
SCTN
NCKY
FL
VA
OH
MI
WV
PA
NY
AK
ME
DE
DC
HI
CO
GAMS
OK
NJ
SD
19%–22.9%
Less than 14%14%–18.9%
23% or more
1999–2000 2005–2006
MARI
CT
VTNH
MD
NH
Source: J. C. Cantor, C. Schoen, D. Belloff, S. K. H. How, and D. McCarthy, Aiming Higher: Results from a State Scorecard on Health System Performance (New York: The Commonwealth Fund, June 2007).Updated Data: Two-year averages 1999–2000, updated with 2007 CPS correction, and 2005–2006 from the Census Bureau’s March 2000, 2001 and 2006, 2007 Current Population Surveys.
U.S. Average: 20.1%U.S. Average: 17.3%

Source: J. C. Cantor, C. Schoen, D. Belloff, S. K. H. How, and D. McCarthy, Aiming Higher: Results from a State Scorecard on Health System Performance (New York: The Commonwealth Fund, June 2007).Updated Data: Two-year averages 1999–2000, updated with 2007 CPS correction, and 2005–2006 from the Census Bureau’s March 2000, 2001 and 2006, 2007 Current Population Surveys.
WA
ORID
MT ND
WY
NV
CAUT
AZ NM
KS
NE
MN
MO
WI
TX
IA
ILIN
AR
LA
AL
SCTN
NCKY
FL
VA
OH
MI
WV
PA
NY
AK
MD
MEVTNH
MARI
CT
DE
DC
HI
CO
GAMS
OK
NJ
SD
10%–15.9%
Less than 7%7%–9.9%
16% or more
1999–2000
DE
MARI
WA
ORID
MT ND
WY
NVUT
KS
NE
MN
MO
WI
TX
IA
ILIN
LA
AL
SCTN
NCKY
FL
VA
OH
MI
WV
PA
NY
AK
ME
DC
HI
CO
GAMS
NJ
SD
2005–2006
CT
VTNH
MD
AR
CA
AZ NMOK
U.S. Average: 11.3%U.S. Average: 12.0%
Percent of Uninsured Children DeclinedSince Implementation of SCHIP, But Gaps Remain


THE
COMMONWEALTH FUND
12Adults Without Insurance Are Less LikelyAdults Without Insurance Are Less Likelyto Be Able to Manage Chronic Conditions to Be Able to Manage Chronic Conditions
161827
58
35
59
0
25
50
75
Skipped doses or did not fillprescription for chronic condition
because of cost
Visited ER, hospital, or both for chroniccondition
Insured all year Insured now, time uninsured in past year Uninsured now
Percent of adults ages 19–64 with at least one chronic condition*
*Hypertension, high blood pressure, or stroke; heart attack or heart disease; diabetes; asthma, emphysema, or lung disease. Source: S. R. Collins, K. Davis, M. M. Doty, J. L. Kriss, A. L. Holmgren, Gaps in Health Insurance: An All-American Problem, Findings from the Commonwealth Fund Biennial Health Insurance Survey (New York: The Commonwealth Fund) Apr. 2006.

THE
COMMONWEALTH FUND
13Previously Uninsured Medicare Beneficiaries With History of Previously Uninsured Medicare Beneficiaries With History of Cardiovascular Disease or Diabetes Have Much Higher Self-Reported Cardiovascular Disease or Diabetes Have Much Higher Self-Reported Hospital Admissions After Entering Medicare Than Previously InsuredHospital Admissions After Entering Medicare Than Previously Insured
Source: J. M. McWilliams, et al., “Use of Health Services by Previously Uninsured Medicare Beneficiaries,” NEJM 357;2, Jul 12 2007.
Number of hospital admissions per 2-year period
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
58 60 62 64 66 68 70 72
Uninsured before age 65 Continuously insured before age 65

THE
COMMONWEALTH FUND
14Cost-Related Access Problems, by DeductibleCost-Related Access Problems, by Deductible
168 11 12
252212
17 19
312719
26 24
44
0
25
50
75
Did not fill aprescription
Did not seespecialist when
needed
Skippedrecommended
test, treatment,or follow-up
Had medicalproblem, did not
see doctor orclinic
Any of the fouraccess
problems
<$500 $500–$999 $1,000+
Percent of adults ages 19–64 insured all year with private insurance
Source: S.R. Collins, et al., Squeezed: Why Rising Exposure to Health Care Costs Threatens the Health and Well-being of American Families, The Commonwealth Fund, September 2006.

THE
COMMONWEALTH FUND
15Many Americans Have Problems Many Americans Have Problems Paying Medical Bills or Are Paying Off Medical DebtPaying Medical Bills or Are Paying Off Medical Debt
3421
141323 26
1898
16
53
292626
42
0
25
50
75
Not able to paymedical bills
Contacted bycollectionagency*
Had to changeway of life to pay
medical bills
Medicalbills/debt being
paid off overtime
Any medical billproblem or
outstanding debt
Total Insured all year Uninsured during the year
Percent of adults ages 19–64 who had the following problems in past year:
*Includes only those who had a bill sent to a collection agency when they were unable to pay it.Source: S. R. Collins, K. Davis, M. M. Doty, J. L. Kriss, and A. L. Holmgren, Gaps in Health Insurance: An All-American Problem, The Commonwealth Fund, April 2006.

THE
COMMONWEALTH FUND
16
Percent of adults reporting: Total Insured all year
Insured now, time uninsured
during yearUninsured
now
Unable to pay for basic necessities (food, heat or rent) because of medical bills
26% 19% 28% 40%
Used up all of savings 39 33 42 49Took out a mortgage against your home or took out a loan
11 10 12 11
Took on credit card debt 26 27 31 23
One-Quarter of Adults With Medical Bill Burdens One-Quarter of Adults With Medical Bill Burdens and Debt Were Unable to Pay for Basic Necessitiesand Debt Were Unable to Pay for Basic Necessities
Source: S. R. Collins, K. Davis, M. M. Doty, J. L. Kriss, and A. L. Holmgren, Gaps in Health Insurance: An All-American Problem, The Commonwealth Fund, April 2006.
Percent of adults ages 19–64 with medical bill problems or accrued medical debt:

Americans Spend More Out-of-Pocket on Health Care Expenses
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$0 $100 $200 $300 $400 $500 $600 $700 $800 $900
a2003b2003 Total Health Care Spending, 2002 OOP Spending
ba
United States
OECD Median
New Zealand
Netherlands
Japan
GermanyFrance Canada Australia
a
Source: The Commonwealth Fund, calculated from OECD Health Data 2006.
Total health care spending per capita
Out-of-pocket spending per capita

18
THE COMMONWEALTH
FUND
16 Million Adults Under Age 65 16 Million Adults Under Age 65 Were Underinsured in 2005Were Underinsured in 2005
Uninsuredduring the year
47.8(28%)
Insured, notunderinsured
108.6(63%)
Underinsured16.1(9%)
Adults 19–64
Note: Underinsured defined as having any of three conditions: 1) annual out-of-pocket medical expenses are 10% or more of income; 2) among low-income adults, out-of-pocket medical expenses are 5% or more of income; 3) health plan deductibles are 5% or more of income.Source: Michelle M. Doty, Analysis of the Commonwealth Fund Biennial Health Insurance Survey (2005).

19
THE COMMONWEALTH
FUND
Roadmap to Health Insurance for All: Principles for Reform
• Builds an essential foundation for quality and efficiency as well as access
• Benefits cover essential services with financial protection• Premiums/deductibles/out of pocket costs affordable• Coverage is automatic, stable, seamless• Choice of health plans or care systems• Broad health risk pools; competition based on
performance, not risk or cost shift• Simple to administer: lowers overhead costs
providers/payers• Minimizes dislocation• Financing adequate/fair/shared across stakeholders

20
THE COMMONWEALTH
FUND
Health Reform and the Presidential Candidates• Leading Democrats:
– Mixed private-public group insurance– Shared financial responsibility (government, employers, households),
employer & individual mandate– Medicaid/SCHIP expansion– New group insurance “connectors” with private & public plan options
like Medicare– Insurance market regulations against risk selection– HIT, prevention, chronic care management, comparative
effectiveness, pay for performance, transparency– Finance with repeal/expiration of high-income tax breaks and system
reforms
• Leading Republicans:– Tax incentives for purchase of individual insurance– Make employer health insurance contributions taxable income to
employee– Buy insurance from any state– Greater state flexibility to reallocate Medicaid/SCHIP dollars– Tort reform, transparency, IT, pay for performance, prevention

21Features of Candidates’ Approaches to Health Care ReformFeatures of Candidates’ Approaches to Health Care ReformSenator Clinton
Senator Edwards
Senator Obama
Mayor Giuliani
Senator McCain
Governor Romney
Individual Mandate X X
Children up to age 25 only No No No
Employer Shared Responsibility
TK% of payroll, small
businesses exempt 6% of payroll TK% of payroll No No No
Subsidies for Low-income Uninsured
Tax credit for premium >TK%
of income
Refundable tax credit on sliding
scale
Sliding scale premium subsidies
Health insurance
credit for low-income
Tax credit $2,500 for
individuals, $5,000 for families
Premium subsidies
Medicaid/ SCHIP expansion X
Parents/ children up to 250% FPL; childless adults up to 100% FPL X No No No
Risk pooling
Private Health Choices Menu
through FEHBP & public
insurance plan option modeled after Medicare
Regional health markets with
private & public plan options
National Health Insurance
Exchange with private & public
plan options
Purchase private
insurance in any state
Purchase private
insurance in any state
Incentives to states to
deregulate private
insurance markets
Quality and Efficiency Measures
HIT, Transparency,
P4P, Prevention, Comparative effectiveness,
Chronic disease management, Disparities, Malpractice
reform
HIT, Transparency,
P4P, Prevention, Comparative effectiveness,
Chronic disease management, Disparities, Malpractice
reform
HIT, Transparency,
P4P, Prevention, Comparative effectiveness,
Chronic disease management, Disparities, Malpractice
reform
HIT, Transparency,
Prevention, Malpractice
reform
HIT, Transparency,
P4P, Prevention, Chronic disease
management, Malpractice
reform
HIT, Transparency,
Malpractice reform

22Candidates’ Agreement on Health Care Reform FeaturesCandidates’ Agreement on Health Care Reform FeaturesSenator Clinton
Senator Edwards
Senator Obama
Mayor Giuliani
Senator McCain
Governor Romney
Candidates From Both Parties Agree
Expanding coverage X X X X X X
Health IT X X X X X X
Transparency X X X X X X
Malpractice reform X X X X X X
Some Candidates Agree
Pay for performance X X X No X No
Prevention X X X X X No
Candidates DifferUniversal coverage X X X No No No
Individual mandate X X All children No No No
Employer pay or play X X X No No No
Changes to employer benefit tax exemption X No No X No Unclear
Regulation of insurance markets X X X No No No

THE
COMMONWEALTH FUND
23Design Matters: How Well Do Different StrategiesDesign Matters: How Well Do Different StrategiesMeet Principles for Health Insurance Reform?Meet Principles for Health Insurance Reform?
Principles for Reform
Tax Incentives and Individual Insurance
Markets
Mixed Private-Public Group Insurance with Shared Responsibility
for Financing Public Insurance
Covers Everyone 0 + +Minimum Standard Benefit Floor – + +Premium/Deductible/Out-of-Pocket CostsAffordable Relative to Income
– + +
Easy, Seamless Enrollment 0 + ++Choice + + +Pool Health Care Risks Broadly – + ++Minimize Dislocation, Ability to Keep Current Coverage + ++ –Administratively Simple – + ++Work to Improve Health Care Quality and Efficiency 0 + +
0 = Minimal or no change from current system; – = Worse than current system; + = Better than current system; ++ = Much better than current systemSource: S.R. Collins, et al., A Roadmap to Health Insurance for All: Principles for Reform, Commission on a High Performance Health System, The Commonwealth Fund, October 2007.

THE
COMMONWEALTH FUND
24Why Not the Best?Why Not the Best?
• Current directions absent policy change:– Costs expected to go to 20% of GDP and
uninsured to move up the economic ladder
• Aiming higher: Why not the best?– U.S. has the resources and technology– Facing facts can help build consensus

25
THE COMMONWEALTH
FUND
Related Commonwealth Fund Reports• A High Performance Health System for the United States: An Ambitious
Agenda for the Next President, The Commonwealth Fund Commission on a High Performance Health System, November 2007.
• S. R. Collins, C. Schoen, K. Davis, et al., A Roadmap to Health Insurance for All: Principles for Reform, The Commonwealth Fund Commission on a High Performance Health System, October 2007.
• C. Schoen, R. Osborn, M. M. Doty, et al., “Toward Higher-Performance Health Systems: Adults’ Health Care Experiences in Seven Countries, 2007,” Health Affairs Web Exclusive, October 31, 2007.
• S. R. Collins, C. White, and J. L. Kriss, Whither Employer-Based Health Insurance? The Current and Future Role of U.S. Companies in the Provision and Financing of Health Insurance, The Commonwealth Fund, September 2007.
• J. C. Cantor, D. Bellof, C. Schoen, et al., Aiming Higher: Results from a State Scorecard on Health System Performance, The Commonwealth Fund Commission on a High Performance Health System, June 2007.
Visit the Fund at: www.commonwealthfund.org

26
THE COMMONWEALTH
FUND
Acknowledgements
Jennifer L. Kriss,Program AssociateThe Commonwealth Fund
Karen Davis,PresidentThe Commonwealth Fund
Cathy Schoen,Senior Vice President for Research and EvaluationThe Commonwealth Fund
Recommended