C
Hn
Ba
b
c
a
ARAA
KHHHT
PTHNG
I
alctfi
mn
0d
Rev Esp Med Nucl. 2011;30(5):317–319
linical note
ashimoto’s thyroiditis and severe hypothyroidism, associated with a single hotodule
. Zantoura,∗, M.H. Sfara, W. Alayaa, W. Chebbia, K. Chattib, and S. Jerbi c
Department of Endocrinology and Internal Medicine, Tahar Sfar Hospital, Hiboune, Mahdia, TunisiaDepartment of Nuclear Medicine, Sahloul Hospital, Sousse, TunisiaDepartment of Radiology, Tahar Sfar Hospital, Hiboune, Mahdia, Tunisia
r t i c l e i n f o
rticle history:eceived 2 September 2010ccepted 20 October 2010vailable online 20 February 2011
eywords:ashimoto’s thyroiditisypothyroidismot nodulehyroid scintigraphy
a b s t r a c t
We report the case of a 27 year-old man with symptoms of severe hypothyroidism that have evolvedsince his adolescence. He was found to have an 11 mm right lobe thyroid nodule. On thyroid ultrasound,the nodule was solid, heterogeneous with markedly atrophic hypoechoic surrounding tissue. Thyroidscintigraphy revealed increased 99mTc pertechnetate and 131I uptake, with persistence of 131I hyper-fixation after 24 h. There was no fixation of the radiotracer in the remaining tissue. Thyroid functiontests found TSH > 100 mIU/l, free thyroxine level 0.9 pmol/l (normal values 11.5-21.8), anti-thyroid per-oxydase antibodies strongly positive > 1,000 IU/ml, and anti-thyroglobulin antibodies negative. One yearafter levothyroxine therapy, the nodule decreased to 40% of its original size.
Hashimoto’s thyroiditis may present as a single hot nodule and severe hypothyroidism. Data of reportedcases suggest that the hot nodule corresponds to a localized hyperplasia of the less diseased portions ofthe thyroid. Chronic stimulation by TSH may have promoted nodular growth and isotopes uptake.
© 2010 Elsevier España, S.L. and SEMNIM. All rights reserved.
Tiroiditis de Hashimoto e hipotiroidismo severo, asociado con un solo nódulocaliente
alabras clave:iroiditis de Hashimotoipotiroidismoódulo calienteammagrafía tiroidea
r e s u m e n
Se presenta el caso de un hombre de 27 anos de edad con síntomas de hipotiroidismo severo en evolucióndesde la adolescencia, y un nódulo tiroideo de 11 mm en el lóbulo derecho. En la ecografía del tiroides,el nódulo era sólido, heterogéneo y con un tejido notablemente atrófico hipoecoico alrededor. La gam-magrafía tiroidea reveló un aumento en la captación en el nódulo tanto del 99mTc-pertecnetato como del131I, con persistencia de la captación de 131I en la imagen de 24 h. No se observó fijación del radiotrazadoren el resto de la glándula. Los análisis mostraron unos niveles séricos de TSH > 100 mUI/l, tiroxina libre0,9 pmol/l (11,5-21,8), anticuerpos antitiroperoxidasa positivo > 1.000 UI/ml y anticuerpos antitiroglob-
ulina negativos. Un ano después del tratamiento con levotiroxina, el nódulo redujo en un 40% su tamanooriginal.La tiroiditis de Hashimoto puede presentarse como un solo nódulo caliente e hipotiroidismo severo.Datos reportados sugieren que el nódulo caliente corresponde a una hiperplasia localizada de las por-ciones menos danadas del tiroides. La estimulación crónica por TSH puede haber favorecido el crecimientonodular y la captación de los isótopos.
ntroduction
Hashimoto’s thyroiditis (HT) is a chronic thyroid disorder char-cterized by autoimmune destruction of the thyroid, resulting inymphocyte infiltration, goiter, and eventually hypothyroidism. Inhildren and adolescents, it’s the most common thyropathy and ishe main cause of goiter.1 Hypothyroidism is the result of severebrous destruction at an advanced stage of the disease.1
The scintigraphic findings of HT are highly variable and canimic several thyroid disorders including diffuse hyperplasia,
odular goiter, cold nodules, and rarely hot nodules.2 Association of
∗ Corresponding author.E-mail address: [email protected] (B. Zantour).
212-6982/$ – see front matter © 2010 Elsevier España, S.L. and SEMNIM. All rights reseroi:10.1016/j.remn.2010.10.011
© 2010 Elsevier Espana, S.L. and SEMNIM. Todos los derechos reservados.
solitary hot nodule with hypothyroidism is a rare condition, it hasbeen previously reported in few cases, all female, 28 to 60 yearsold.3–6
Herein, we report a male patient presenting with severehypothyroidism evolving since adolescence, associated to a singlehot pertechnetate and iodine 131 thyroid nodule.
Case report
A 27-year-old man was referred to our endocrinology unit forshort stature, decreased skin pilosity, pallor and asthenia. He was
living in an area of iodine sufficiency. His mother had primaryhypothyroidism treated by Levothyroxine since 15 years. He wasborn at term of a normal pregnancy. He had a normal psychomotordevelopment. He went to school for 9 years and was unable to finishved.

318 B. Zantour et al / Rev Esp Med Nucl. 2011;30(5):317–319
THYROIDE
22. 5mm 11. 3mm 32. 2mm 6. 9mm
THYROIDE LD
A B
F hete1
cgaH
mntffit
wl6mk(
wm1>
swhttiah
uitht
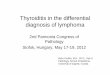
igure 1. A) Thyroid ultrasonography before levothyroxine therapy: 11.3 mm solidyear levothyroxine therapy, thyroid nodule decreased to 6.9 mm.
ollege. He was working as a carpenter. At the age of 13 years, hisrowth rate decreased. Pubertal development was initiated at thege of 17 years, but he had no facial nor pubic hair development.e had no neck surgical intervention or irradiation.
Clinical examination found a height 149 cm, weight 47 kg, bodyass index 21.77 kg/m2, blood pressure 110/60 mmHg. There was
o facial, body or axillary hair, with a sparse pubic hair, normalestis and penis volume. He had a dry, rough and pale skin, puffyace, cold extremities, husky voice and slow speech, thin brittlengermails and macroglossia. There was a single 1 cm nodule inhe right lobe of the thyroid.
Biological exams revealed normocytic normochromic anemiaith hemoglobin level 9 g/dl, normal white blood cells and patelets
evel, glycemia 3.56 mmol/l (normal values 3.9-5.5), cholesterol.7 mmol/l (normal values: < 5.18), triglycerides 1.8 mmol/l (nor-al values: < 1.69), natremia 134 mmol/l (normal values: 136-146),
alemia 3.9 mmol/l (normal values: 3.5-5.1), creatinine 77 �mol/lnormal values: 62-115), a normal sedimentation rate.
Thyroid function tests showed a severe primary hypothyroidismith a thyroid stimulating hormone level (TSH) > 100 mUI/l (nor-al values 0.2-4.2), a free thyroxine level 0.9 pmol/l (normal values
1.5-21.8), anti-thyroid peroxydase antibodies strongly positive1,000 UI/ml, anti-thyroglobulin antibodies negative.
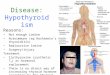
Thyroid ultrasonography found a small thyroid, 3 ml volume,olid heterogeneous nodule, 11.3 mm diameter, in the right lobe,ell demarcated from the surrounding tissue which was markedlyypoechoic (fig. 1A). Thyroid scintigraphy with 99mTc pertechne-ate revealed a hot area in the right thyroid nodule corresponding tohe nodule in the same localization, without uptake in the remain-ng tissue. 131I scintigraphy was performed the same day and afterdelay of 24 h. The nodule was hot with 131I, with persistence ofyper-fixation after 24 h (figs. 2A, 2B and 2C).
Levothyroxine substitution therapy was progressively initiatedntil a dose of 150 �g/day to normalize TSH level. We noted an
mprovement of all clinical signs of hypothyroidism, normaliza-ion of hemoglobin and lipid levels. The diameter of the nodulead diminished to 6.9 mm on the control ultrasound at one year ofherapy (Fig. 1B).
rogeneous right lobe thyroid nodule with hypoechoic surrounding tissue. B) After
Discussion
We report a case of solitary hot nodule associated with HTand hypothyroidism. This association has been described in a totalof 13 cases through the literature, all adult middle aged femalepatients. Thyroid nodule had an increased uptake of both 99mTcpertechnetate and iodine,4,6 or iodine when only iodine scintig-raphy was performed.7,8 A discrepancy between 99mTc and 131Iuptake on thyroid scan has been reported in two cases.3,5 Decreasediodine uptake with aspect of cold iodine thyroid nodule wasexplained by an organification defect with large intra-thyroid inor-ganic iodide pool.3,9 In the remaining cases and in our case, therewas an increased iodine uptake on thyroid scan.
Functional nodules in HT can be observed in early stage of thedisease or in advanced destruction stages according to the aspectof the surrounding tissue on thyroid scan and ultra-sonography.In the first form, the surrounding tissue was plainly visualized,follicular cells destruction and fibrosis are slight and left suffi-ciently normal thyroid tissue, inefficient hormone production iscaused mainly by abnormalities of iodine metabolism rather thana destructive process.10 In the second form, there was a severediminished uptake of the remaining thyroid tissue, the functionalnodules being the solely areas of uptake.8 In this case, histologicalexam showed HT of the nodule, with an extensive destruction ofthe remaining gland.8 Our patient had clearly this second form ofhot nodule. Hashimoto’s disease diagnosed at 27 years was evolvingsince adolescence, as attested by decreasing growth rate at 13 yearswith a final short stature, clinical signs of severe hypothyroidismand very low thyroidal hormones. The hot nodule was surroundedby atrophic non-functioning thyroid tissue. Chronic stimulation byTSH contributed to the increased ability of the nodular tissue toconcentrate isotopes.3,4
In our case as in the cases reported by Mousavi et al,4 and Zengiet al,6 thyroid nodules have diminished 40 to 60% in volume with
thyroid hormone replacement. This observation strengthens thehypothesis that the lesion presenting as a hot nodule is a localizedhyperplasia of the less diseased area secondary to stimulation byTSH.6
B. Zantour et al / Rev Esp Med Nucl. 2011;30(5):317–319 319
A B
C
F delay
rdtp
R
igure 2. Thyroid scans using 99mTc pertechnetate (A), 131I (B) and 131I after a 24 h
In conclusion, our case illustrates the great variability of thy-oid scan in HT and outlines the pathogenetic complexity of thisisease. Chronic stimulation by TSH may play an important role inhyroid hot nodules formation in patients with hypothyroid HT, byromoting nodular growth and increasing isotopes uptake
eferences
1. Radetti G, Gottardi E, Bona G, Corrias A, Salardi S, Loche S, et al. Thenatural history of euthyroid Hashimoto’s thyroiditis in children. J Pediatr.2006;149:827–32.
2. Yarman S, Mudun A, Alagol F, Tanakol R, Azizlerli H, Oguz H, et al. Scintigraphic
varieties in Hashimoto’s thyroiditis and comparison with ultrasonography.Nucl Med Commun. 1997;18:951–6.3. Boughattas S, Arifa N, Kacem M, Chatti K, Riahi N, Hassine H, et al.Hypothyroidism presenting as a hot pertechnetate nodule. Ann Nucl Med.2003;17:495–8.
(C): Hot nodule in the right lobe without uptake of the remaining thyroid tissue.
4. Mousavi Z, Zakavi SR, Farid NR. Hashimoto’s thyroiditis presenting as singlehot nodule and hypothyroidism. J Endocrinol Invest. 2002;25:643–5.
5. Boi F, Piga M, Loy M, Mariotti S. Hypothyroid Hashimoto’s thyroiditis withscintigraphic and echo-color Doppler features mimicking autonomous ade-noma. J Endocrinol Invest. 2002;25:469–72.
6. Zengi A, Karadeniz M, Demirpolat G, Akgun A, Karakoze S, Yilmaz C. Hypothy-roid Hashimoto’s thyroiditis with scintigraphic and color flow Dopplersonography features mimicking a hot nodule. Inter Med. 2009;48:231–4.
7. Hoogenberg K, Van Tol KM. Hashimoto’s thyroiditis presenting as functioningadenoma. Thyroid. 2001;11:893.
8. Bialas P, Marks S, Dekker A, Field JB. Hashimoto’s thyroiditis presentingas a solitary functioning thyroid nodule. J Clin Endocrinol Metab. 1976;43:1365–9.
9. Thrall JH, Burman KD, Wartofsky L, Corcoran RJ, Johnson MC, Gillin MT. Discor-
dant imaging of a thyroid nodule with 131I and 99mTc: concordance of 131I andfluorescent scans. Radiology. 1978;128:705–6.10. Amino N, Tada H, Hidaka Y. Chronic (Hashimoto’s) thyroiditis (Chapter 103).In: De Groot LJ, Jameson JL, editors. Endocrinology.. 4th ed. Philadelphia: W. B.Saunders Company; 2001. p. 1471–80.
Recommended