Gout
Gout
Deposits of sodium urate crystals in articular, periarticular, and subcutaneous tissues
May be primary or secondary Primary – hereditary error of purine metabolism Secondary – drugs that inhibit uric acid excretion or
another acquired disorder
Incidence and Risk Factors
Primary gout accounts for 90% of cases
Affects primarily middle aged men
Risk factors: obesity, HTN, thiazide diuretics, excess alcohol use
Pathophysiology
Uric acid is end product of purine metabolism and is excreted by the kidneys
Hyperuricemia results from Increase in uric acid production Underexcretion of uric acid by kidneys Both
Diet high in purines will not cause gout, but may trigger an attack in a susceptible person
Clinical Manifestations
Gouty arthritis in one or more joints (but less than four
Great toe joint most common first manifestation; other joints may be the foot, ankle, knee, or wrist
Joints are tender & cyanotic May be precipitated by trauma, surgery, alcohol
ingestion, or infection
Clinical Manifestations
Onset usually nocturnal, with sudden swelling and excruciating pain
May have low grade fever Usually subsides within 2-10 days Joints are normal, with no symptoms between
attacks
Complications
Joint deformity Osteoarthritis Tophi may produce draining sinuses that may
become infected Renal stones, pyelonephritis, obstructive renal
disease
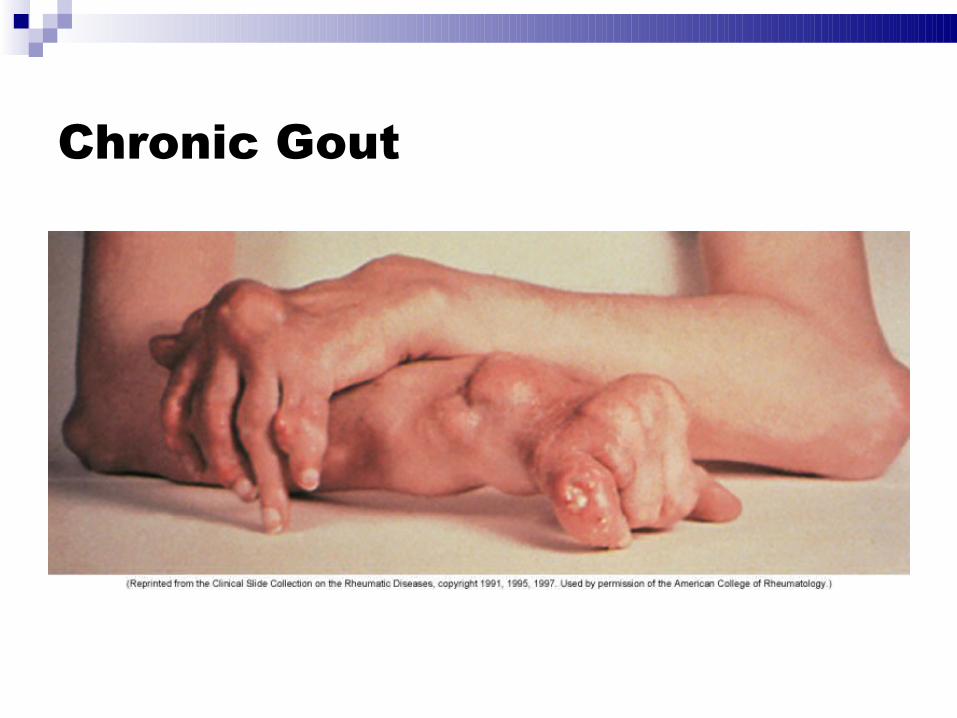
Chronic Gout
Diagnosis
History & physical examination
Family history of gout
Diagnostic studies
Diagnostic Studies Serum uric acid levels > 6 mg/dl
May be caused by other factors
24 hour urine uric acid levels Synovial fluid aspiration contains uric acid crystals
Seldom necessary, as diagnosis based on clinical symptoms possible in 80% of cases
X-rays appear normal in early stages; tophi appear as eroded areas of bone
Collaborative Care
Acute attack Colchicine produces dramatic antiiflammatory
effects with relief within 24-48 hours NSAIDs for additional pain relief Corticosteroids (po or intraarticular) Adrenocorticotropic hormone (ACTH) Joint aspiration to decompress
Collaborative Care
Prevention of acute attacks
Colchicine combined with: allopurinol (Zyloprim, Alloprim) – blocks production of
uric acid probenecid (Benemid), sulfinpyrazone (Anturane) –
inhibit tubular reabsorption of uric acid febuxostat (Uloric) – inhibits xanthine oxidase, recently
shown to reduce serum uric acid levels
Collaborative Care
Dietary measures Weight reduction Avoidance of alcohol Avoidance of foods high in purines
High: Sardines, anchovies, herring, mussels, liver, kidney, goose, venison, meat soups, sweetbreads, beer & wine
Moderate: Chicken, salmon, crab, veal, mutton, bacon, pork, beef, ham
Collaborative Care
Prevention of renal stones Increase fluid intake to maintain adequate urine
output Allopurinol ACE inhibitor losartin (Cozar) – promotes urate
diuresis
Nursing Care
Acute gouty arthritis – pain control Gentle, supportive care of affected joints Immobilize and rest affected joints – bed rest or
NWB Cradle or footboard to prevent pressure from
bedcovers Monitor ROM and degree of pain
Nursing Care Patient/Family teaching
Gout is a chronic disease Drug teaching Need to monitor serum uric acid levels Precipitating factors
Excess calorie intake, alcohol intake, purine rich foods Fasting Niacin, ASA, diuretics Surgery or major medical event such as MI
Learning Objectives : Learning Objectives Classify the drugs commonly
used in the treatment of gout. Mention the indications, side effects, dosage and toxicities of drugs used in the treatment of gout Design a plan for treatment of gout. Prescribe the appropriate treatment for different cases of gout. Enumerate the tests required for monitoring of the therapy of gout
Gout :
Gout Metabolic disorder Characterized by hyperurecamia (normal plasma urate 1-4mg/dl) Acute gout: sudden onset of severe inflammation in the small joint due to precipitation of urate crystals in the joint space. Chronic gout: pain and stiffness persist in the joint between attacks.
Classification of drugs for the treatment of Acute Gout. : Classification of drugs for the treatment of Acute
Gout. NSAIDs Colchicine Corticosteroid In acute attack arthritis is treated first and Hyperuricemia later
Drugs for Chronic gout : Drugs for Chronic gout Uricosuric Drugs:
Probenecid Sulfinpyrazone Uric acid synthesis inhibitor Allopurinol
Non-steroidal Anti-inflammatory agents (NSAIDs) : Non-steroidal Anti-inflammatory agents
(NSAIDs) Strong anti-inflammatory agent: (Indomethacin, Naproxen, Piroxicam, Diclofenac or Etoricoxib) Given in relatively high and quickly repeated dose. Effective in terminating the acute attack (but my take 12-24hours) Naproxen, Piroxicam also inhibits chemotactic migration of leukocytes into the inflamed joint. Once acute attack is over, reduce the dose and continue the drug for 3-4 weeks.
Dose of NSAIDs for acute attack of gout : NSAIDs in high doses taken with food are:
Naproxen: 750 mg immediately, then 500 mg every 8-12 hours Diclofenac: 75—100 mg immediately, then 50 mg every 6-8 hours Indomethacin: 75 mg immediately, then 50 mg every 6-8 hours. After 24-48 hours, reduced doses are given for a further week. Contraindications: active peptic ulcer disease/ impaired renal function/ allergy to NSAIDs. Dose of NSAIDs for acute attack of gout
Colchicine :
Colchicine Alkaloid from Colchicum autumnale. Suppresses gouty inflammation Neither analgesic nor anti-inflammatory. No effect on blood uric acid level. Acts by binding to microtubules of neutrophils/ monocytes destroy microtubule loss of movement and phagocytosis by the leucocytes. ADRs: GI upset/ bloody diarrhea/ abd.pain/ hematological disorders/loss of hair/ sometimes motor paralysis.
Uses:
Treatment of Acute attack: effective within first 24h of attack. A small dose (0.5 -1.5mg) taken at first symptom of attack abort it. Dose:1mg PO followed by 0.25mg 1-3 hourly till the acute attack is over or total dose of 6mg is given or diarrhea starts. Maintenance dose 0.5-1mg/day for 4-8 weeks. Prophylaxis of gout: 0.5 -1mg/day (prevents further attack) Doses should be decreased in renal and hepatic dysfunction
Corticosteroid :
Corticosteroid Gives dramatic symptomatic relief. Used if NSAIDs are contraindicated. If Gout is monoarticular: intra-articular administration (e.g. triamcinolone, 10-40mg depending of size of joint) For Polyarticular gout: IV or Orally Methylprednisolone 40mg/day IV tapered over 7 days. Prednisolone 40-60mg/day orally tapered over 7 days
Chronic gout :
Chronic gout Pain and stiffness persist in between attack. Hyperuricaemia Tophi Urate stone in kidney Progressive disability. Tophi
Uricosuric Drugs :
Uricosuric Drugs Uricosuric drug enhances uric acid excretion via kidney Uricosuric drugs are similar to urate in structure Blocks the tubular reabsorption of filtered urate thereby reducing metabolic urate pool and preventing formation of new Tophi and reduce the size of those already present. When given with Colchicine, they lessen the frequency of recurrences of acute gout.
Indications: Increasing frequency or severity of acute attacks.
Precautions with uricosuric drugs: (to reduce precipitation of uric acid in urinary tract) Maintain daily urinary output of 2 liters or more. Maintain urinary pH above 6.0 (give potassium citrate 30-80mEq/d) Uricosuric drugs are avoided in patients with history of uric acid nephrolithiasis. Aspirin in Moderate doses (<3g/d) antagonizes the action of uricosuric agents and aggravates hyperuricemia.
Probenecid : Probenecid Uses: Chronic gout and
hyperuricaemia: (2nd line/ adjuvant drug) 0.5g/day initially, with gradual increase to 1-2g daily. It gradually lowers blood urate level. Ineffective in the presence of renal insufficiency (serum creatinine >2mg/dl) Adverse effects: rashes, allergic dermatitis, upper GIT irritation, and drowsiness. Inhibits excretion of penicillin, dapsone indomethacin, and acetazolamide.
Sulfinpyrazone : Sulfinpyrazone Uses: In chronic gout: start with
100-200mg BD, gradually increase according to response (Max. dose 800mg/d) Uricosuric action is additive with probenecid but antagonized by Salicylates. It inhibits platelet aggregation. Adverse effects: gastric irritation/rashes/ hypersensitivity reaction.
Uric acid synthesis inhibitor(Allopurinol) Hypoxanthine Xanthine Uric Acid Xanthineoxidase Xanthineoxidase Allopurinol -ve -ve
Competitive inhibitor of uric acid synthesis by
inhibiting xanthine oxidase. Xanthine oxidase is involved in the metabolism of hypoxanthine and xanthine to uric acid. Promptly lowers plasma urate and urinary uric acid concentration and facilitates tophus mobilization. Allopurinol is very effective in uric acid overproducers.
Dose: initially 100mg/d of allopurinol is given for 1
week, the dose is increased to 200 – 300mg/d, if serum uric acid is still high. ADRs: precipitation of acute gouty arthritis in the initial month of therapy /GI upset/ skin rash/ alopecia. Probenecid increases the excretion of allopurinol If patient taking both Probenecid and allopurinol than ↑dose of allopurinol and ↓ dose of Probenecid
Treatment plan for acute attack of Gout : Treatment plan for acute attack of Gout Treatment
is given for symptomatic relief only As the attack is self-limited and resolve spontaneously Toxicity of therapy must be considered in each patient. Arthritis is treated first and hyperuricemia later. NSAIDs: treatment of choice when not contraindicated.
Treatment plan of Acute Gout : Treatment plan of Acute Gout NSAIDs
Contraindicated? Renal insufficiency Peptic ulcer disease Congestive heart failure NSAID intolerance Are Corticosteroids Contraindicated? NSAIDs Antiinflamatory doses Corticosteroids Oral Colchicine Oral or Intraarticular Steroid Intraarticular PO Steroid
Indomethacin: 75 mg immediately, then 25-50 mg every 8 hours
till the symptoms resolves (usually 5-10days) Glucocorticoids are useful when NSAIDs are contraindicated Monarticular Gout: intra-articular triamcinolone, 10–40 mg. Polyarticular gout:Methylprednisolone 40 mg/d I.V tapered over 7 days or Prednisone, 40–60 mg/d orally tapered over 7 days.
Management of gout in between attack : Management of gout in between attack Low-
purine diet: Lose weight Less meat and seafood consumption Higher intake of dairy products A high liquid intake (daily urinary output of 2 L or more) Avoidance of hyperuricemic medications: (Thiazide and loop diuretics and low dose Aspirin)
Drug Treatment of Chronic gouty arthritis : Indication: > 2-3 attacks/year initiate
prophylaxis. Uricosuric: for under-excretors Probenicid: Sulfinpyrazone: toxic side effects Avoid with renal disease Consider NSAIDs to avoid exacerbation of gout Indications for Allopurinol Tophaceous deposites Uric acid consistently >9mg/dl Impaired renal function Prophylaxis for tumor-lysis syndrome Consider NSAID’s to avoid exacerbation Drug Treatment of Chronic gouty arthritis
Tests required for monitoring of the therapy of gout : Tests required for monitoring of the therapy of
gout After the acute phase is over take steps to see Blood uric acid level is normalized. Tophis if present is are reversed. Nephropathy if present is reversed or at least halted.
Pseudogout :
Pseudogout Deposition of calcium containing salts in articular surface. Occurs in many diseases e.g. hyperperathyroidism, diabetes, wilson’s disease etc. Ocurs in persons >60years. Characterized by acute and recurrent arthritis involving large joints (knee and wrist) Treatment: NSAIDs/ intraarticular glucocorticoid/ colchicines.


Recommended