Goldenhar Syndrome
Presented by Lori Kingsbury & Jennifer Klundt
DCOM 732 Craniofacial Anomalies Summer 2010

Goldenhar SyndromeAKA Oculo-auriculo-vertebral
dysplasia (OAV) First described in 1952 by
Maurice GoldenharAssociated with anomalous
development of the first branchial arch and second branchial arch

EtiologiesEtiology is unclear; one possible etiology
suggested is that there seems to be a deficiency in mesodermal formation or defective interaction between neural crest and the mesoderm.
Some factors are believed to be related to the development of the disease. These may include:Drug ingestion (cocaine, thalidomide, retinoic
acid and tamoxifen)Environmental factors (insecticides and
herbicides)Maternal diabetes

Prevalence•1 in 5,000 – 25,000 live births
•Male prevalence
•Most cases are sporadic
•1-2% of cases report autosomal dominant transmission
•A few families consistent with autosomal recessive have been reported
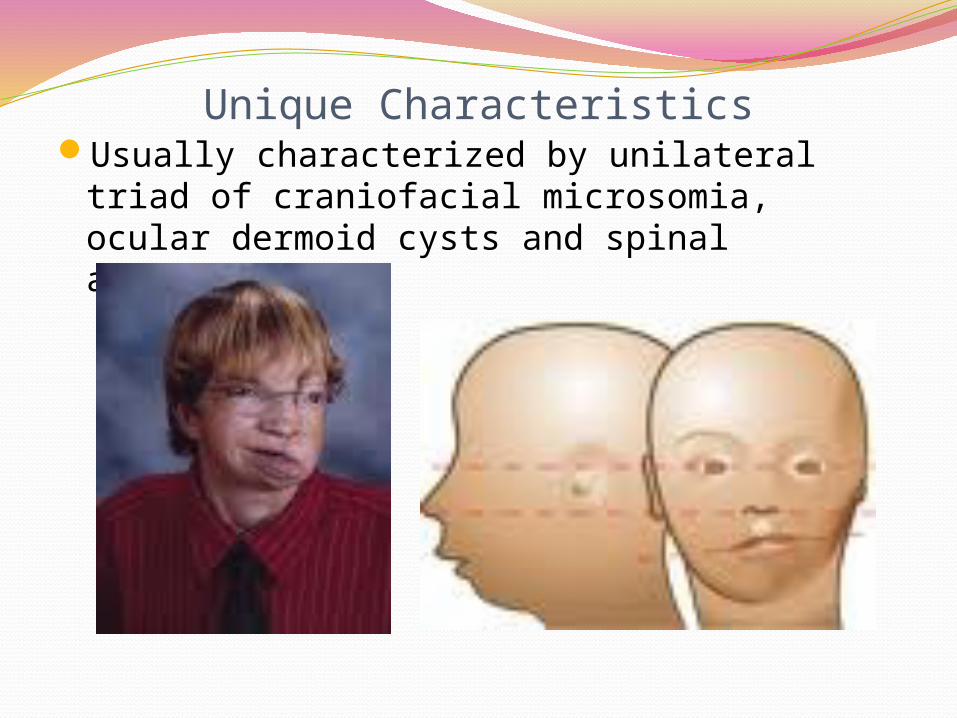
Unique CharacteristicsUsually characterized by unilateral triad of
craniofacial microsomia, ocular dermoid cysts and spinal abnormalities
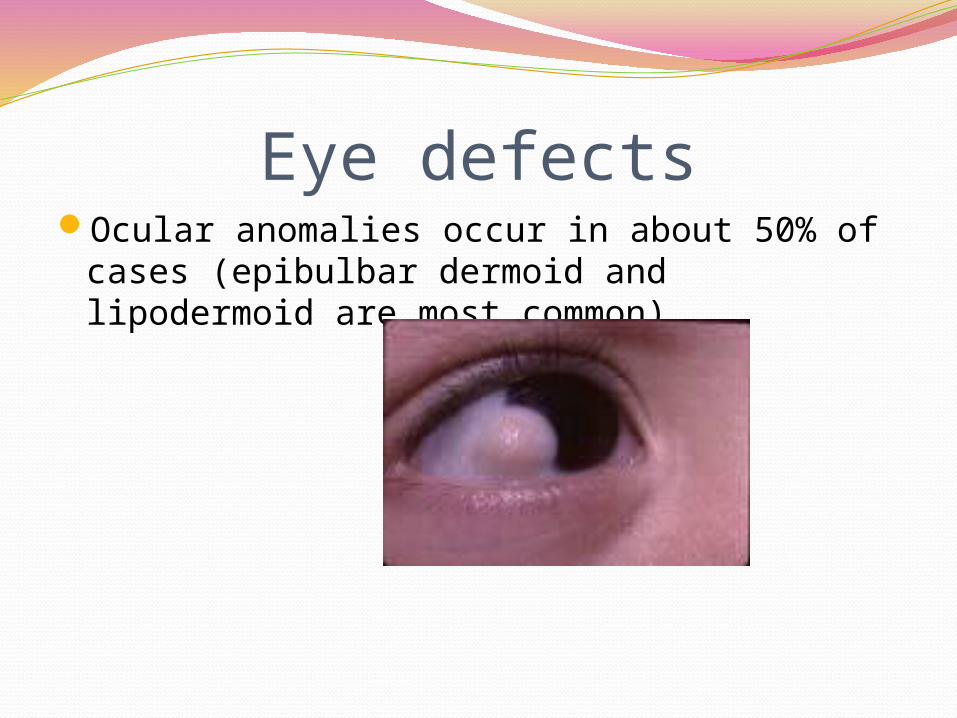
Eye defectsOcular anomalies occur in about 50% of
cases (epibulbar dermoid and lipodermoid are most common)

Ear defectsAuricular defects are reported in 65% of
cases (preauricular tags, microtia, anotia, conductive hearing loss

Vertibral defectsVertibral anomolies including absence of
vertibrae, hemivertebrae, fused ribs, kyphosis & scoliosis.

Facial Features

Physical Signs/SymptomsUnilateral or bilateral Hemifacial microsomia
(HFM)Microtia; chin may be closer to the affected
earMicrognathiaFacial cleftingCleft lip/palateHearing lossMissing eye or benign growths of the eye

Other Health IssuesHeart, kidney, and lung problems are also
common in individuals with Goldenhar syndrome. These typically involve one side of the organ being underdeveloped or missing.

Speech/Language Characteristics Highly VariableLanguage problems – associated with hearing
lossSpeech problems –tongue shape, jaw shape
and mobility, weakness or difficulty moving side that is smaller
Hyponasality – clefting of lip and/or palate Swallowing problems – lack of saliva, tongue
shape or use Abnormal airways

DiagnosisNo Genetic Test
Through identification of physical anomalies
Appearance, Skeletal Formations, Hearing Deficits
Professionals in pediatric medicine, radiology, ophthalmology, otolaryngology, odontology, and neurology contribute to the diagnosis

TreatmentLowering of jaw on affected side
Lengthening jaw
Addition of bone to build up cheeks
Soft tissue may be added to face
3 to 4 operations to rebuild ear

TreatmentTreatment of hearing loss or deafness
Speech therapy
Managing feeding problems
Orthodontics
Treating associated problems like heart or kidney issues

Prognosis
VERY GOOD
Normal Lifespan Normal Intelligence

Videoshttp://www.youtube.com/watch?v=YctDsa
VLLLY&feature=youtube_gdatahttp://www.youtube.com/watch?v=hkSyKk
q9fmshttp://www.youtube.com/watch?v=zWz06
w4Cerl

Referenceshttp://www.ccakids.com/Syndrome/Hemifacia
lMicrosomia.pdfhttp://www.healthline.com/galecontent/golde
nhar-syndromehttp://www.orpha.net/consor/cgi-bin/oc_Exp.p
hp?Lng=GB&Expert=374http://righthealth.com/topic/Goldenhar_Syndr
omes

Multiple Choice Exam QuestionsQuestion #1 Goldenhar Syndrome is characterized by:
A. Craniofacial microsomiaB. Ocular dermoid cystsC. Spinal abnormalitiesD. All of the above

Multiple Choice Exam QuestionsQuestion #2Which of the following is NOT a characteristic
of Goldenhar Syndrome?A. MicrotiaB. Facial CleftingC. MacrognathiaD. Hearing loss

Multiple Choice Exam QuestionsQuestion #3Which of the following is NOT a treatment
associated with Goldenhar Syndrome?A. Plastic SurgeryB. Aural RehabilitationC. Behavior ModificationsD. Managing Feeding Issues
Recommended