GHANA HEALTH SERVICE
2010 ANNUAL REPORT

2010 Annual Report Ghana Health Service
Page 1 of 76
FOREWORD
In 2010, the Ghana Health Service reviewed its working strategies under the five health sector objectives
as a result of the development of a new Health Sector Medium Term Development Plan. The new strategic
objectives that guided the implementation of services during the year 2010 were:
1. Bridge the equity gaps in access to health care and nutrition services and ensure sustainable
financing arrangements that protect the poor
2. Improve governance and strengthen efficiency in health service delivery, including medical
emergencies.
3. Improve access to quality maternal, neonatal, child and adolescent health services.
4. Intensify prevention and control of communicable and non-communicable diseases and promote
healthy lifestyles
5. Improve institutional care including mental health service delivery
This 2010 report outlines the GHS‟ experiences in implementing the strategies under the planned action of
work. It also highlights some overarching issues that require attention in the near future, these include;
Delays and inadequacy of funds given to the Districts
Inadequate numbers of skilled personnel particularly, midwives and medical assistants
The decline in EPI coverage for all the antigens
Despite these drawbacks a lot of progress has been made in the fight to eradicate Guinea worm disease. In
the year under review, only eight cases of Guinea worm were reported. They were all contained. The
country is on the verge of eradicating Guinea worm.
Our goal towards eradicating Polio is also on course, during the year under review no case of wild polio
virus was isolated.
I wish to acknowledge the effort that all the staff of the Ghana Health Service, especially those working in
very difficult circumstances has contributed to realizing the goals of the Health Sector.
Our commitment towards achieving the Global targets for health remains unwavering.
With our experiences in these four years of implementing our strategic health plan, and as we move into
the final year, I believe that we have been able to not only develop a deeper understanding of some of the
complexities and challenges of our health sector, but also prepared our minds and hearts towards a greater
commitment, coordination and participation in order that we may harness the benefits and richness of
quality and accessible healthcare for all Ghanaians.
Thank you.

2010 Annual Report Ghana Health Service
Page 2 of 76

2010 Annual Report Ghana Health Service
Page 3 of 76
EXECUTIVE SUMMARY
The Ghana Health Service (GHS) is the largest autonomous national executive body responsible for
implementing all national health policies in Ghana. Established in 1996, the GHS in liaison with the
Ministry of Health (MOH) is dedicated to bringing quality health care and services to every door step and
household with the commitment to achieve optimum quality of life in every community in Ghana. The
GHS Annual Review of 2010 and the annual report, summarizes the Service‟s operations and performance
in 2010 under the revised five health sector objectives under the health sector Medium Term Development
Plan:
To accelerate the push towards achieving the MDGs 5 and to some extent 4, the MDG 5 Accelerated
Framework (MAF) document was developed during the year under review. An Emergency Obstetric and
Neonatal care facility survey was also undertaken.
During the year under review, the GHS initiated the development and use of information technology to
improve information management and service delivery. Infrastructure for health has been expanded to
support effective and efficient services delivery. Strategic direction for District Health Systems
Strengthening Initiatives was provided (UWR CHPS Initiative, GEHIP, MoTeCH and GAVI). Selected
activities outlined in the GAVI HSS project were carried out to improve service delivery in the districts.
Work on reviewing the District Health Information Management System (DHIMS) was initiated. The
improvement in the health workforce and distribution continued during the year under review. However,
the numbers of midwives and medical assistants are still not adequate in most districts.
With regards to CHPS implementation, there has been an increase in the numbers of functional CHPS
zones. This has been driven mainly by the increasing availability of community health nurses. The number
of functional CHPS zones increased from 868 in 2009 to 1,023 in 2010.
All the service indicators showed some improvement. The nurse-to-patient population ratio has improved
to 1: 955 in 2010 in comparison to 1:1079 in 2008 and to 1:971 in 2009. OPD per capita also increased to
0.91 in 2010 following similar increases over previous years (0.77 in 2008 and 0.81 in 2009). TB
treatment success rate increased from 85.5% in 2008 to 87.0% in 2009. Antenatal coverage increased
marginally from 92.1% to 92.2%. Skilled delivery rate improved nationally from 45.6% in 2009 to 48.9%
in 2010 and Institutional Maternal Mortality Ratio decreased from 169.9/100,000LB in 2009 to
163.2/100,000LB in 2010. Guinea worm cases fell from 242 in 2009 to 8 in 2010.
Despite these positive achievements,immunization coverage declined in all the antigens compared to the
previous year 2009. Family planning coverage fell from 31.1% in 2009 to 23.8% in 2010.
Funds flow for district level activities continue to be erratic. Although total funding appears to have
increased, the increase has been for earmarked funding.

2010 Annual Report Ghana Health Service
Page 4 of 76
The year under review saw an improvement in the reimbursement of facilities by the National Health
Insurance Authority. There is now a lag period for payment of on the average of three months compared to
about six months previously.
The challenges facing the service are in the area of ensuring adequate and timely funding for district level
activities. The inadequate numbers and mal-distribution of critical staff like midwives and medical
assistants continue to affect service delivery.
There is the need for strategies to improve on the equitable distribution of critical health staff and improve
the quality of care at all levels.

2010 Annual Report Ghana Health Service
Page 5 of 76
LIST OF TABLES
Table 1: Trend of OPD per capita by Regions………………………………………………… 31
Table 2: Trend in Doctor Population ratio by Regions (2007-2010)……………………………… 31
Table 3: Trend in Nurse Population ratio by Region (2007-2010)……………………………. 32
Table 4: Progress in the implementation of CHPS by Regions (2008-2010)…………………….. 33
Table 5: Percentage of facilities given provisional accreditation by NHIA by Regions…………. 34
Table 6: Trend in Health Sector Budget for the period (2007-2010)………………………….. 35
Table 7: Statement of Receipts and Expenditures for GHS 2010…………………………………. 36
Table 8: GHS Fleet size as at December 2010……………………….. …………………… 37
Table 9: Key Sector performance indicators (2006-2010)……………………………………… 38
Table 10: Trend of skilled Delivery by Regions……….. ………………………………….. 39
Table 11: Trend of Penta 3 coverage by Regions ……. …………………………………….. 39
Table 12: Summary of core surveillance indicators Jan- Dec 2010……………………………. 42
Table 13: Distribution of H1N1 vaccination and AEFI by Regions……………………………. 43
Table 14: Top 3 agents involved in poisoning in 2010………… …………………………… 46
Table 15: Top 10 Diseases from OPD 2010……. ………………………………………….. 48
LIST OF FIGURES
Fig 1: Trend in functional CHPS zones………………….………………………………….. 32
Fig 2: Accredited facilities by grades……….………………………………………………. 34
Fig 3: Trend of early child hood mortalities in Ghana (DHS) ……………………………………. 40
Fig 4: Trend of notified cases TB 2005-2010 ……………………………………………………. 41
Fig 5: Proportion of OPD cases attributed to Malaria 2006-2010……………………………… 44
Fig 6: Proportion of Total cases and deaths attributed to Malaria……………………………….. 45
Fig 7: Under five malaria case fatality rate ……………………………………………………… 45
Fig 8: Reported Poisoning Trends by Agents………………………………………………………46
Fig 9: Male Female distribution among cases of Hypertension seen in health facilities…………...47
Fig 10: Age Distribution of Hypertension cases seen at OPD………………………………………47
2010 Annual Report Ghana Health Service
Page 6 of 76
CONTENTS
FOREWORD .................................................................................................... 1
EXECUTIVE SUMMARY ................................................................................. 3
LIST OF TABLES ............................................................................................. 5
LIST OF FIGURES ........................................................................................... 5
CONTENTS ...................................................................................................... 6
ACRONYMS & ABBREVIATIONS ................................................................... 9
INTRODUCTION ............................................................................................ 11
PERFORMANCE BY OBJECTIVES ................................................................ 12
HO1: Bridge Equity Gaps in access to health care and nutrition services and ensure sustainable financing
arrangements that protect the poor .............................................................................. 12
Access to Health Care .............................................................................................. 12
Human Resources Planning, Recruitment, Deployment Retention and Management 12
Gender and Equity .................................................................................................... 14
National Health Insurance Scheme ........................................................................... 14
HO2: IMPROVE GOVERNANCE AND STRENGTHEN EFFICENCY IN HEALTH SERVICE
DELIVERY, INCLUDING MEDICAL EMERGENCIES .......................................... 16
Information Technology to Improve Health Information Management and Service Delivery 16
eHealth ..................................................................................................................... 16
ICT Governance-GHS ICT Enterprise Architecture (EA) ......................................... 16
ICT Training ............................................................................................................ 16
Financing Mechanism and Financial Management Systems ...................................... 16
Management Systems and Scale-up leadership Training ............................................ 17
Infrastructure to Support Effective and Efficient Service Delivery ............................. 17
HO3: IMPROVED ACCESS TO QUALITY MATERNAL, NEONATAL, CHILD AND
ADOLESCENT HEALTH SERVICES ...................................................................... 19
Access to Quality Maternal Newborn and Reproductive Health Services .................. 19
HO4: INTENSIFY PREVENTION AND CONTROL OF COMMUNICABLE AND NON-
COMMUNICABLE DISEASES AND PROMOTE HEALTHY LIFESTYLES ......... 21
Health Promotion and Awareness Creation of Risk Factors ...................................... 21
Non-Communicable Diseases ................................................................................... 21
Malaria ..................................................................................................................... 22
HIV/AIDS ................................................................................................................ 22
Tuberculosis (TB) .................................................................................................... 23

2010 Annual Report Ghana Health Service
Page 7 of 76
Yaws ........................................................................................................................ 24
Guinea Worm ........................................................................................................... 24
Buruli Ulcer ............................................................................................................. 24
H1N1 Influenza ........................................................................................................ 25
Disease Surveillance, Emergency Preparedness and Response .................................. 25
Environmental And Occupational Health And Safety ............................................... 26
Occupational health .................................................................................................. 26
Environmental health ............................................................................................... 26
Poison control programme .........................................................................................27
Research and development ........................................................................................27
HO-5 IMPROVE INSTITUTIONAL CARE, INCLUDING MENTAL HEALTH SERVICE
DELIVERY ................................................................................................................ 29
KEY PERFORMANCE INDICATORS BY OBJECTIVES ................................. 31
TABLES AND FIGURES .................................................................................. 31
HEALTH OBJECTIVE ONE: Bridge Equity Gaps in access to health care and nutrition services and
ensure sustainable financing arrangements that protect the poor .................................. 31
Outpatient Attendance ............................................................................................. 31
Community Based Health Planning and Services ..................................................... 32
National Health Insurance Scheme. .......................................................................... 34
HEALTH OBJECTIVE TWO: IMPROVE GOVERNANCE AND STRENGTHEN EFFICENCY IN
HEALTH SERVICE DELIVERY, INCLUDING MEDICAL EMERGENCIES .......... 35
Financing mechanism and financial management systems ......................................... 35
HEALTH OBJECTIVE THREE: IMPROVE ACCESS TO QUALITY MATERNAL, NEONATAL,
CHILD AND ADOLESCENT HEALTH SERVICES ................................................ 38
Institutional Maternal Mortality ratio ........................................................................ 38
Ante natal Care ........................................................................................................ 38
Skilled Delivery ....................................................................................................... 39
Immunization ........................................................................................................... 39
HEALTH OBJECTIVE FOUR: INTENSIFY PREVENTION AND CONTROL OF COMMUNICABLE
AND NON-COMMUNICABLE DISEASES AND PROMOTE HEALTHY LIFESTYLES 41
Selected core surveillance indicators: ....................................................................... 42
HEALTH OBJECTIVE FIVE: IMPROVE INSTITUTIONAL CARE, INCLUDING MENTAL
HEALTH SERVICE DELIVERY .............................................................................. 48
CHALLENGES ............................................................................................... 49
Objective 1: Bridge gaps in access to health care and nutrition services and ensure sustainable financing
arrangements that protects the poor ............................................................................. 49
Human Resource ...................................................................................................... 49

2010 Annual Report Ghana Health Service
Page 8 of 76
Objective 2: Improve governance and strengthen efficiency in health service delivery, including medical
emergencies. ............................................................................................................... 49
Objective 3: Improve access to quality maternal, neonatal, child and adolescent health services 50
Objective 4: Intensify prevention and control of communicable and non-communicable diseases and
promote healthy lifestyles. .......................................................................................... 50
Objective 5: Improve institutional care including mental health service delivery .......... 51
THE WAY FORWARD FOR 2010 .................................................................... 52
Objective 1:Bridge the equity gaps in access to health care and nutrition services and ensure sustainable
financing arrangements that protect the poor. .............................................................. 52
Objective 2:Improve governance and strengthen efficiency in health service delivery, including medical
emergencies. ............................................................................................................... 52
Objective 3:Improve access to quality maternal, neonatal, child and adolescent health services. 53
Objective 4:Intensify prevention and control of communicable and non-communicable diseases and
promote healthy lifestyles. ........................................................................................... 53
Objective 5: Improve institutional care including mental health service delivery. ........ 54
ANNEXES: TRENDS IN SECTOR INDICATORS ............................................ 56
Doctor to Population Ratio ......................................................................................... 56

2010 Annual Report Ghana Health Service
Page 9 of 76
ACRONYMS & ABBREVIATIONS ACCPAC- Accounting Package
ADB - Agricultural Development Bank
ANC - Ante Natal Care
BCC - Behavior Change Communication
BMCs - Budget Management Centers
CHEW - Community Health Extension Worker
CHO - Community Health Officer
CHPS - Community Health Planning Service
DC - Disease Control
DDHS - District Director of Health Services
DFID - Department for International Development
DHIMS - District Health Information Management Systems
DISHOP - District Health System Operationality
EMD - Estate Management Department
EPI - Expanded Programme on Immunization
FDB - Food and Drugs Board
GAIN - Global Alliance for Improved Nutrition
GAVI - Global Alliance for vaccines and Immunization
GHS - Ghana Health Service
GIS - Geographical Information System
GOG - Government of Ghana
GRB - Gender Responsive Budgeting
GSCP - Ghana Sustainable Change Project
GTZ - German Technical Cooperation
HASS - Health Administrative Support Services
HI - Health Information
HIRD - High Impact Rapid Delivery
HIV - Human Immune Deficiency Virus
HIV/AIDS - Human Immune Virus/ Acquired Immune Deficiency Syndrome
HR - Human Resource
HRD - Human Resource Division
ICD - Institutional Care Division
ICT - Information Communication Technology
IDSR - Integrated Disease Surveillance and Response
IEC - Information Education & Communication
IGF - Internally Generated Funds
IMCI - Integrated Management of Childhood Illness
IPT - Intermittent Preventive Treatment
IRS - Indoor Residual Spraying
IST - In Service Training
KATH - Komfo Anokye Teaching Hospital
KNUST - Kwame Nkrumah University of Science and Technology
KRHTS - Kintampo Rural Health Training School
Lab - Laboratory
LDP - Leadership Development Program
MAF - MDG 5 Accelerated Framework.
MDAs - Ministries Department and Agencies

2010 Annual Report Ghana Health Service
Page 10 of 76
MDBS - Multi-Donor Budget Support
MDG - Millennium development Goal
MHAPP - Mental Health and Poverty Project
MoH - Ministry of Health
MTT - Multidisciplinary Ministerial Task Team
NACP - National Aids Control Programme
NGOs - Non-Governmental Organizations
NHI - National Health Insurance
NHIS - National Health Insurance Scheme
NHRC - Navrongo Health Research Centre
NMCCSP - Nutrition and Malaria Control for Child Survival Project OHS - Occupational health Strategy
OI/ART.STI- Anti Retroviral Therapy/ Sexually Transmitted Infections
OPD - Out Patient Department
PMTCT - Prevention of Mother to Child Transmission
PPM - Planned Preventive Maintenance
PPME - Policy Planning Monitoring and Evaluation
QA - Quality Assurance
QHP - Quality Health Partners
RHS - Regional Health Service
SBS - Sector Budget Support
ToTs - Training of Trainers
U5 - Under Fives
UNICEF - United Nations International Children‟s Emergency Fund.
WAWI - West African Water Initiative
WVI - World Vision International

2010 Annual Report Ghana Health Service
Page 11 of 76
INTRODUCTION
The Ghana Health Service (GHS) 2010 Annual Report details the activities of its fourth-year program of
work (4th
/ 5YPOW) which overlaps the health sector Medium Term Development Plan. Thus 2010 report
has been restructured to reflect changes in the health sector performance objectives as captured in the
Health Sector Medium Term Development Plan (2010-2013). The report covers all the various activities
undertaken during the year 2010 and how these activities have contributed to the much needed boost in the
quality of life of the Ghanaian.
The new five health sector objectives around which this report was written are:
1. Bridge equity gaps in access to health care and nutrition services and ensure sustainable
financing arrangements that protect the poor;
2. Improve governance and strengthen efficiency in health service delivery, including medical
emergencies;
3. Improve access to quality maternal, neonatal, child and adolescent health services;
4. Intensify prevention and control of communicable and non-communicable diseases and
promote healthy lifestyles;
5. Improve institutional care including mental health service delivery.

2010 Annual Report Ghana Health Service
Page 12 of 76
PERFORMANCE BY OBJECTIVES
HO1: Bridge Equity Gaps in access to health care and nutrition services
and ensure sustainable financing arrangements that protect the poor
Access to Health Care
The increase in OPD per capita continued for the year 2010. From 0.49 in 2001, it has increased to 0.77 in
2008 and 0.81 in 2010. In 2010 it rose to 0.91. The main drivers for this trend appear to be the health
insurance and the improvement in the spread of health infrastructure. The National Health Insurance
addresses financial accessibility whilst the improvement in the spread of health infrastructure addresses
the geographical accessibility, which are the main challenges to access to health care in Ghana.
Human Resources Planning, Recruitment, Deployment Retention and Management
To ensure that the Human Resource Development Division delivers on its mandate, the division in 2010
introduced some interventions to improve the human resource management.
Key Activities undertaken were:
Compilation and update of GHS Headquarters staff database covering seven out of the ten
Directorates at GHS HQ were covered.
Compilation and update of nominal roll for GHS. The total staff population for GHS according to
the nominal roll was 33,426 as at August 2010. This represented 0.08% increase over the 2009
figure of 33,169.
Appointments made during the year under review: 54 officers were appointed into various senior
management positions; 3,075 newly qualified nursing staff (including general nurses, midwives,
community Health Nurses, Psychiatric Nurses, Enrolled Nurses); 167 contract appointments; 241
Technical and Support Service Staff and 257 replacements.
Implementation of policy on the three-year continuous service eligibility for promotion after first
appointment (1st level promotion). Officers who had first appointment between 1
st January, 2004
and 31st December 2006 were interviewed for promotion to the next grade. Promotion interviews
for the last two grades of the HND class were also decentralized to the regions. Overall, promotion
of 419 staff, comprising 215 nursing staff and 204 non-nursing staff were approved by GHS
Council in 2010.
Approval of staff grade conversions and Upgrading. A total of 305 applications were approved for
conversion and 209 for upgrading. The approval was based on the consideration of the additional
academic qualifications and the programme of study of the applicants.

2010 Annual Report Ghana Health Service
Page 13 of 76
Processing of Applications of 1014 disengaged staff. This comprised retirement (816); vacation of
post (107); resignation (52) and death (39).
Approval of 358 Leave applications. This comprised study leave with pay (186), study leave
without pay (78) and leave of absence (94).
Revision of existing staff appraisal form. The new appraisal form was disseminated and circulated
for use at the various institutions and service levels.
The GHS in conjunction with the MOH engaged the Fair Wages and Salary Commission to
undertake re-evaluation of the health sector jobs and devise a means of determining market
premium for health workers.
The Leadership Development Programme (LDP), which is intended to strengthen the capacity of
healthcare managers in leadership and management, was rolled out at GHS Headquarters and in
the following regions - Ashanti, Volta, Greater Accra and Western Regions. Overall, 276 officers
benefited from the programme.
The GHS in conjunction with the Human Resource for Health Division (HRHD) of the Ministry of
Health (MoH) made a submission to the Fair Wages Commission in respect of internal relativity
distortions created by the proposed Single Spine Salary Structure. The Ministry is currently
engaging the Commission to address the concerns raised.
The GHS assisted with the development of curriculum for training of Nurse Aneasthetists at Ridge
Hospital. The training programme commenced in October 2010 with 25 students.
The GHS in conjunction with the School of Public Health, University of Ghana, organized a
training programme aimed at Improving Management of Public Health Interventions (IMPHI). A
total of 11 senior managers from GHS benefited from the training.
The GHS collaborated with GIMPA to organize a four week course in Health Administration and
Management for selected staff in GHS. Two sessions were organized in March and July 2010. A
total of 157 senior health managers drawn from public, quasi-governmental, private and Christian
Health Association of Ghana (CHAG) institutions attended the training programme.
The Service also supported in the development and review of training curriculum for pre-service
training institutions.
Observations from the Payroll Data Analysis
The overall number of health workforce on the Ministry of Health payroll as at December 2010 was
50,206 compared to 49,318 in 2009 with corresponding monthly wage bill of GH¢ 31,088,770 in GH₵
27,129,935.92. There was an increase of 12.73% in the December 2010 monthly wage bill over the

2010 Annual Report Ghana Health Service
Page 14 of 76
December 2009 monthly wage bill of. In terms of numbers, the total figure increased by 1.8% from the
2009 figure of 49,318 to 50,206 in 2010.
The distribution of the health workforce on the payroll by agencies was as follows: the GHS (72%),
Christian Health Association of Ghana – CHAG (15%), Korle-Bu Teaching Hospital (6%), Komfo
Anokye Teaching Hospital (5%) and Tamale Teaching Hospital (2%).
The analysis of the payroll data further indicated that overall, 61.53% of the health workforce as at
December 2010 were females. For Doctors, about 27% constituted females while the remaining 73% were
males. The analysis also showed that health workers aged between 25 and 34 years constituted about
37.1% (18,611) of the total workforce. This implies that over one-third of the total health workforce is
made up of quite young workers. However, it is important to note that workers aged between 55 and 60
formed about 15% (7,520). This relatively high proportion of health workers would be moving out of the
Service in the next 5 years. Management staff constituted 9% (2,768) of this age segment. Within the
same age bracket (i.e. 55 – 60 yrs), nurses constitute about 46.8% (3,520) with about half of them (1,531)
being midwives.
Gender and Equity
Special efforts were made within the year to ensure gender mainstreaming within programs and activities
of the GHS. The GHS undertook a rapid appraisal of the current gender mainstreaming approaches. The
aim was to assess progress, understand the challenges of implementation and allow for correction to better
consolidate gender mainstreaming in the GHS.
The Ghana Health Service assessed equity of enrollment in the NHIS and looked at community
perceptions vis-à-vis schemes, providers as well as community attitudes and beliefs. A household survey
was conducted in the Central and Eastern Regions of Ghana. The results were translated into a set of clear
policy recommendations.
National Health Insurance Scheme
At the end of the year 2010, 65% of GHS facilities had been accredited. Most passed, but only a few were
given grade A. About 20% failed and will need to be assisted to pass. The major reasons for failing
included; inadequate staffing, poor infrastructure/equipment and poor management. Some GHS facilities
have not applied for accreditation. Poor management control systems within the GHS accounts for these
refusals.
Upper West Region presented the lowest number of facilities for accreditation with the NHIA. None of
the GHS facilities that applied for accreditation failed. However, some facilities were given provisional
accreditation .Upper West had the highest proportion of facilities accredited grade A followed by Greater
Accra and Northern regions whilst Volta, Ashanti and Brong Ahafo regions had the highest proportion of
facilities awarded grade D.
The NHIA conducted clinical audits around the country and some deductions to the submitted claims were
made. Major reasons for the deductions included poor folder retrieval, poor hand writing, diagnosis not

2010 Annual Report Ghana Health Service
Page 15 of 76
matching with treatment, poly pharmacy (in the prescription of antibiotics) and up coding. Although some
facilities were assisted to retrieve some of the funds, many could not retrieve them.
.
The GHS supported the work towards the Capitation Pilot Payment in the Ashanti Region. Work was not
completed to enable the pilot to take off. Work is still on-going.
GHS contributed to the draft review of the NHIS law which was completed and submitted to MOH and
the Attorney General Department.
A Health providers‟ forum has been formed and two meetings have been held. The group proposed that
GHS conduct some sample costing of the health services that is provided by Regional and District
Hospitals, Health Centres and CHPS before the review of tariffs. This will ensure that GHS negotiates for
the new tariffs with empirical evidence.

2010 Annual Report Ghana Health Service
Page 16 of 76
HO2: IMPROVE GOVERNANCE AND STRENGTHEN EFFICENCY IN
HEALTH SERVICE DELIVERY, INCLUDING MEDICAL
EMERGENCIES
Information Technology to Improve Health Information Management and Service Delivery
The GHS has initiated the development and use of information technology to improve information
management and service delivery. It is collaborating with other partners to improve the collection,
collation, analysis and reporting of health information.
Some of the key activities undertaken to improve the health information management system were:
Deployment of and provision of technical support for iHOST (electronic medical records) in some
Hospitals.
Deployment f smart phones for collecting service data in Kintampo South and Asuogyaman as part
of GAVI HSS
Replication of MOTECH in Senya Breku district in the Central Region.
Initiation of transition from DHIMS to web-based DHIMS 2 is ongoing.
Initiation of Management processes to ensure local managers validate and use the data that they
generate.
eHealth
As a follow up to the launch of the eHealth Policy by the Ministry of Health, meetings were held during
the year to set the platform for implementing the policy.
ICT Governance-GHS ICT Enterprise Architecture (EA)
The GHS continued to work with the National Information and Telecommunication Authority (NITA) in
the area of ICT governance. NITA during the year under review initiated the deployment of the fibre optic
backbone that Ministry, Departments and Agencies (MDAs) are going to be linked onto. The Ghana
Health Service has strategically placed itself in a position to benefit from this roll-out.
ICT Training
There was capacity building in ICT across various levels of the service. Teams from the ICT department
and Centre for Health Information Management (CHIM) attended trainings on Free Open Source Software
(FOSS), Networking, Google applications and DHIS 2. The Bachelor of Science program in Health
Informatics was started at the School of Public Health, Legon.
Financing Mechanism and Financial Management Systems
A strategic plan was developed for the Finance Division for the Service. The GHS prepared its
consolidated financial statement for 2010 on time. Two review meetings were held with the Regional

2010 Annual Report Ghana Health Service
Page 17 of 76
Finance officers. Quarterly financial data validation and consolidation were carried out in all ten (10)
regions. The GHS Headquarters was linked to the MOFEP in readiness for GIFMIS Roll-out. Finance
and Non Finance Managers in all ten (10) Regions were trained in the revised ATF. The Service coordinated the ten (10) year audit of Global Fund by the Office of the Inspector General (OIG).
Management Systems and Scale-up leadership Training
Based on recommendations made after the assessment of the performance review of 2008, the conduct of
performance review has been restructured to reflect organizational accountability.
Key activities undertaken under management system:
Coordinated GHS Retreats and Performance Reviews of 2009 POW
Produced the 2008 GHS Annual Report
Produced “Facts and Figures 2009”
Supported the development of Monitoring & Supervision Checklists including one for NHIS)
Reviewed the National Malaria M&E plan
Developed SOPs: Programmes for monitoring, improved data collection and feedback systems
To improve performance within the Service, management systems were strengthened by building capacity
of various professionals.
In the area of improving financial management and accountability, the leadership and management of the
GHS carried out the following activities:
a. Developed 2009 policies and priorities for GHS
b. Championed stakeholder fora to discuss HSS issues -including the review of the policy on CHPS
c. Coordinated development of 2009 MTEF plans and budgets and collated this into a national plan.
Infrastructure to Support Effective and Efficient Service Delivery
The GHS with funding through the NACP and EPI constructed three incinerators in selected districts.
Installation of emergency obstetric equipment in Ashanti, Western, Northern and Brong-Ahafo Regions
was completed.
The Service initiated the procurement, delivery and distribution of emergency obstetric equipment in
Central, Eastern and Upper East Regions
A nationwide needs assessment for the development phase of the ORIO grant to improve TB case
detection in Ghana was conducted. To improve the quality of service delivery, a number of equipment were repaired in various facilities.
Among the equipment repaired were: One defective operating table for Tema General Hospital and

2010 Annual Report Ghana Health Service
Page 18 of 76
defective x-ray equipment donated by General Electric (GE) at Axim and Apam Hospitals. X-ray
equipment at Bole, Kintampo and Ashanti Mampong Hospitals are awaiting spare parts for repairs.
New fleet of vehicles were procured: 332 Great Wall pick-ups, 13 Hover SUV vehicles and GAVI funded
pick-ups,
The proportion of pick-ups to 4-wheel vehicles has increased from 57% in 2000 to 79% in 2010. The
growth corresponds to expansion of services such EPI, TB, HIV, new districts and upgrading of health
centers to hospitals.
The national average age of vehicles has reduced from 7.8 years in 2008 to 5.6 years in 2010. Similarly,
the national average age of motorcycles has reduced from 6.6 years in 2008 to 2.8 years in 2010.
The service procured back-up spare parts for vehicles and bikes deployed into the system. Each RHD is
required to establish a Revolving Fund using the spare parts as seed-capital.
Data on health facilities in all the then regions have been updated.
The service undertook a survey of all uncompleted GHS/ MoH projects in all the ten regions (excluding
the Teaching Hospitals) to ascertain their actual number, stage of completion and the cost of outstanding
works. The report was accepted by MoH for implementation.
Proposed Capital Budget for the year 2010 amounted to GH¢ 19.5m. The priority areas included the
completion/rehabilitation of health facilities, staff accommodation and CHPS facilities
101 out of the 120 projects planned in the 2010 Capital budget were procured or considered on-going.
However, actual work took place on only 24 project sites.
In spite of allocation of funds in the approved 2010 budget, there were practically no funds available to
pay contractors and consultants. Many contractors therefore, pulled out of most of the project sites due to
lack of payment of outstanding claims. The outcome was the submission of a small number of certificates
by the regions for processing in 2010.
The Ghana Health Service submitted entries on Corporate Innovations to the African Union for
consideration of awards. The Service also submitted its proposal on Boat Operations (The Hardest-to-
Reach) in response to a call for papers to an International Development and Innovations conference in
Yale University. The proposal was also accepted for presentation in 2011.
2010 Annual Report Ghana Health Service
Page 19 of 76
HO3: IMPROVED ACCESS TO QUALITY MATERNAL, NEONATAL,
CHILD AND ADOLESCENT HEALTH SERVICES
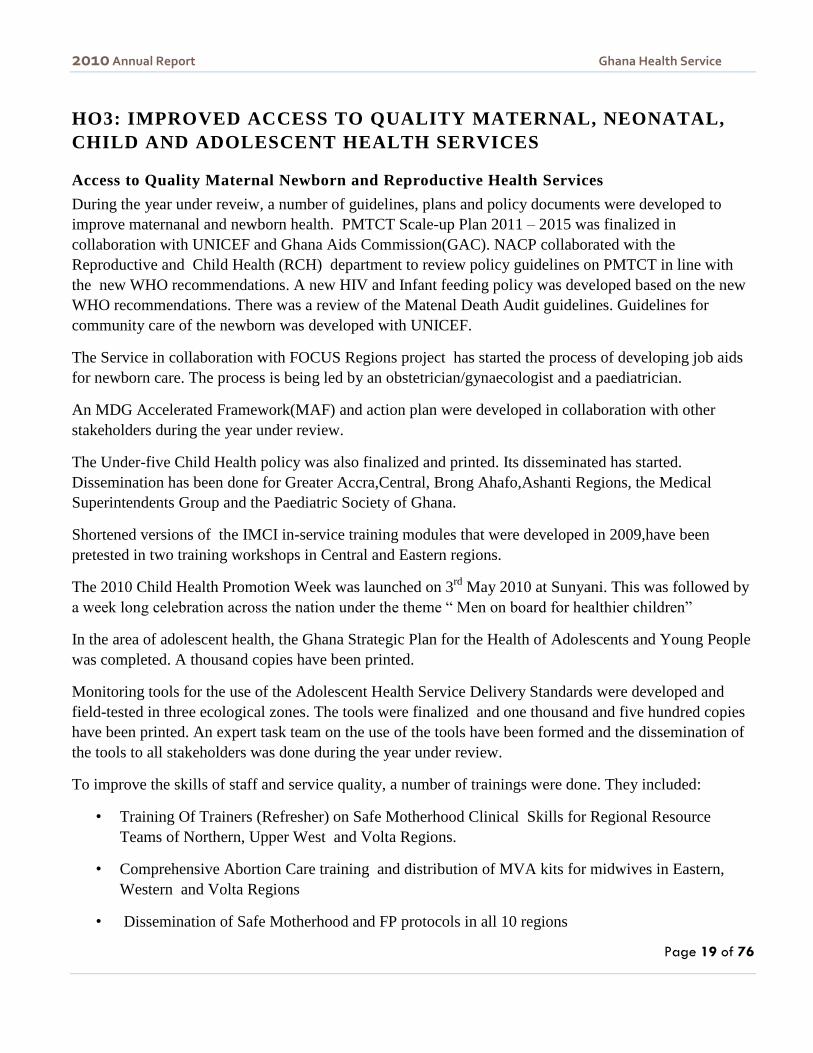
Access to Quality Maternal Newborn and Reproductive Health Services
During the year under reveiw, a number of guidelines, plans and policy documents were developed to
improve maternanal and newborn health. PMTCT Scale-up Plan 2011 – 2015 was finalized in
collaboration with UNICEF and Ghana Aids Commission(GAC). NACP collaborated with the
Reproductive and Child Health (RCH) department to review policy guidelines on PMTCT in line with
the new WHO recommendations. A new HIV and Infant feeding policy was developed based on the new
WHO recommendations. There was a review of the Matenal Death Audit guidelines. Guidelines for
community care of the newborn was developed with UNICEF.
The Service in collaboration with FOCUS Regions project has started the process of developing job aids
for newborn care. The process is being led by an obstetrician/gynaecologist and a paediatrician.
An MDG Accelerated Framework(MAF) and action plan were developed in collaboration with other
stakeholders during the year under review.
The Under-five Child Health policy was also finalized and printed. Its disseminated has started.
Dissemination has been done for Greater Accra,Central, Brong Ahafo,Ashanti Regions, the Medical
Superintendents Group and the Paediatric Society of Ghana.
Shortened versions of the IMCI in-service training modules that were developed in 2009,have been
pretested in two training workshops in Central and Eastern regions.
The 2010 Child Health Promotion Week was launched on 3rd
May 2010 at Sunyani. This was followed by
a week long celebration across the nation under the theme “ Men on board for healthier children”
In the area of adolescent health, the Ghana Strategic Plan for the Health of Adolescents and Young People
was completed. A thousand copies have been printed.
Monitoring tools for the use of the Adolescent Health Service Delivery Standards were developed and
field-tested in three ecological zones. The tools were finalized and one thousand and five hundred copies
have been printed. An expert task team on the use of the tools have been formed and the dissemination of
the tools to all stakeholders was done during the year under review.
To improve the skills of staff and service quality, a number of trainings were done. They included:
• Training Of Trainers (Refresher) on Safe Motherhood Clinical Skills for Regional Resource
Teams of Northern, Upper West and Volta Regions.
• Comprehensive Abortion Care training and distribution of MVA kits for midwives in Eastern,
Western and Volta Regions
• Dissemination of Safe Motherhood and FP protocols in all 10 regions

2010 Annual Report Ghana Health Service
Page 20 of 76
• A 5 day training of trainers (T.O.T.) workshop on Lactation Management was organized for 28
participants from Northern, Upper East, Upper West, Brong Ahafo and Ashanti Regions in April
2010. The training was held in Sunyani.

2010 Annual Report Ghana Health Service
Page 21 of 76
HO4: INTENSIFY PREVENTION AND CONTROL OF
COMMUNICABLE AND NON-COMMUNICABLE DISEASES AND
PROMOTE HEALTHY LIFESTYLES
Health Promotion and Awareness Creation of Risk Factors
The GHS carried out educational campaign through the mass media on Regenerative Health, the
prevention of cholera and the H1N1 outbreaks. Special activities were carried out on the launch of the
World Diabetes day.
Non-Communicable Diseases
Draft document on the Strategic framework for controlling and managing NCD has been completed.
Strategic document on Sickle cell disease and cancers are currently being finalised
There was a consultative meeting to look at Policy guidelines for managing breast cancer. An alcohol
policy development working group was also formed.
One of the key interventions in the control of non-communicable diseases is health promotion.
Some key Health promotion activities carried out were:
Celebration of world and national events – tobacco, diabetes, heart, cancer, Sickle cell disease
Making of some Press releases - cancer, healthy lifestyles
Organisation of Radio talk shows on various NCDs at all levels
Launching of “Good Life. Live it Well” Campaign in Nov 2010 in collaboration with John
Hopkins University.
Organization of GHS Health Promotion Seminar in Feb 2010 - „Diet and physical activity‟
Promotion of Health walks – It is now becoming a part of celebration of several national events
and anniversary of several companies and churches
An agency with the support of the MOH launched an SCD project on April 23, 2010
Started developing posters on cancers in late 2010
With regards to cancer screening early detection and management the following activities were held:
Acquisition of a GoG loan of $700,000 to support cancer prevention, early detection and palliative
care.
Provision of HPV vaccination (Cervarix) at Ridge Hospital
Organization of meetings on the introduction of HPV vaccine.

2010 Annual Report Ghana Health Service
Page 22 of 76
The following studies on NCDs were completed during the year under review:
1. Prevalence of risk factors for NCDs among patients reporting to KBTH
2. Prevalence of Risk factors for Cardiovascular Diseases among students in University of Ghana
3. WHO Study on global AGEing and adult health (SAGE) nationwide study in 5,573 adults and
elderly (18 years +)
4. Systematic review of hypertension in Ghana
Malaria
The Ghana Health Service has been implementing strategies to improve on malaria case management.
After successfully changing and revising the Anti-Malaria Drug Policy, focus has been on early case
detection and prompt treatment at all levels, with emphasis on cases in the most vulnerable groups,
children under five, non-immune visitors and pregnant women. In a bid to equip health workers with the
most current knowledge and skills, treatment guidelines and training manuals were revised and printed.
During the period under review, both public and private facilities throughout the country were supplied
with Artesunate-Amodiaquine tablets for the treatment of uncomplicated malaria. A total of 600,000 Rapid
Diagnostic Test (RDT) kits were also supplied to the health facilities to help with the laboratory
confirmation of cases.
In Ghana, the diagnosis of malaria has been predominantly clinical. However, with the rapid scale up of
proven interventions and their possible impact on malaria epidemiology, expert advice through the WHO
recommends a parasitological confirmation of all cases prior to treatment. There has therefore been the
need to scale up laboratory diagnosis either by microscopy or RDTs. To ensure that malaria cases are lab
confirmed before management is started, the training of laboratory staff on diagnosis which commenced in
the previous year was continued with the training of 373 peripheral health workers on laboratory diagnosis
(microscopy/RDTs). The USAID/PMI IMad project also conducted onsite training and supportive
supervision for lab technicians on microscopy. Sixty health facilities (60) including regional and district
hospitals as well as health centres with labs were visited and given technical support in lab diagnosis of
malaria in the first phase of the programme.
The total number of malaria cases seen at the OPD showed an upward trend from 3,694,671 in 2009 to
3,740,055 for the year under review. The proportion of malaria to total OPD also increased from 32.5% to
34% during the same period. Overall case fatality for malaria also worsened from 1.22% in 2009 to 1.44%
in 2010. Admissions for malaria however declined during the same period.
HIV/AIDS
In 2010, the GHS supervised the establishment of seven hundred and seventy four (774) testing centers
compared to two hundred and eighty-four (284) for the year 2009.

2010 Annual Report Ghana Health Service
Page 23 of 76
Ghana adopted the combination antiretroviral therapy, as a policy since 2006, for PMTCT.
In 2010, five hundred and twenty thousand, nine hundred (520,900) pregnant women got to know their
HIV status compared to the three hundred and eighty-one thousand, eight hundred and seventy-four
(381,874) pregnant women got to know their HIV sero-status in 2009. Ten thousand, nine hundred and
eighty four (10,984) were positive (2.9%) compared to six thousand six hundred thirty-four (6,634)
representing 1.7% who were found to be positive among the pregnant women tested in 2009. Out of these
positive pregnant women, 55% were given Anti-retroviral (ARVs) as prophylaxis. The rest were not
eligible to receive their ARVs and they were subsequently lost to follow-ups.
Tuberculosis (TB)
In 2010, the National TB Programme entered its final year of successful implementation of the Global
Fund Round 5 Grant.
TB control activities continued to be integrated into the GHS structure at primary, secondary, and tertiary
levels of care.
In 2010, a total of 15,145 cases of TB were registered representing a case notification rate of 62%
compared to a total number of 15,286 registered in 2009 (64%). Fifty-five per cent (55%) of all registered
TB patients were pulmonary smear positive TB cases while 30% and 10% were pulmonary smear negative
and extra pulmonary TB (EPTB) cases respectively. Since 2004, the proportion of EPTB cases has gone
up by 52%.
TB treatment success rate however showed an upward trend reaching 87.0% for the 2009 cohort compared
to 85.1% for the 2008 cohort. For the 2009 cohort, 79.1% were cured compared to 77.9% cured for the
2008 cohort.
Some of the activities undertaken during the year:
Conduction of a National Stakeholders Review Meeting;
Organized an International conference on Improving TB case detection in Ghana.
Implemented a new intervention for improving TB case finding as a pilot in Accra Metropolitan Area with
support from CIDA and WHO.
Developed the National Infection Prevention and Control Policy in collaboration with the Institutional
Care Division of Ghana Health Service;
Developed Standard Operating Procedures for Intensified TB case finding at the facility level;
Conducted supervisory visits to regional and district levels to monitor TB activities;
Coordinated meetings of various sub-groups and the National TB Advisory Board.
Received technical assistance missions from various partner agencies such as WHO, KNCV, MSH and
TB CAP.

2010 Annual Report Ghana Health Service
Page 24 of 76
Mobilized resources by developing grant proposals for Global Fund National Strategic Approach and
Round 9 call for proposals and WHO/CIDA call for proposals on implementing innovations to improve
TB case detection.
Conducted advocacy, communication and social mobilization activities for TB control.
Conducted operational research towards improved programme management.
Yaws
Support visits were made to 9 regions during the year under review.
In the area of capacity building, 35 core Regional Health Directorate members were trained on yaws
diagnosis (picture cards), elimination strategies and data tools for routine and baseline data collection.
Central Region DHA and the DDHS group in Volta Region had training in yaws diagnosis and
management. Some of the consumables distributed by the National Program to the Districts included:
100,000 data collection tools (TS, ADR, Reg), 3,500 picture cards, 1.549 million vials of BP (1.2 MU)
and 28,000 (2.4 MU) (1.5 million vials 1.2 MU taken at end of year)
The number of cases of Yaws detected during the year under review was 9,778 which was far below the
2009 cases of 36,328 and 28,080 in 2008. The drop in the cases detected can be attributed to the decrease
in the surveillance for Yaws in some of the districts and poor reporting. The current national prevalence of
yaws is approximately 700 cases per 100,000 in the population under 15 years (2008 Rapid Survey by
National Yaws Elimination Program).
Guinea Worm
Major advancement was made during the year to finally eradicate guinea worm in Ghana. For the year
under review, only eight (8) cases were reported. All of them were detected before the worms emerged
and were treated in the case containment center, leaving no room for them to contaminate water sources.
The last case was on 11th May, 2010, and since then no case has been detected in the country. There are
only four currently endemic villages located in three districts all in the Northern region of the country. The
National reward scheme was launched in July 2010 followed by vigorous sensitization across the country.
However, no report has been made yet. Two hotline numbers were made available for reporting rumors;
12 rumors /suspected cases were notified through the lines: from the Northern Region (7), Volta Region
(2), Western Region (2) and Central Region (1). All were promptly investigated and discarded as not
being guinea worm disease. The National Certification Committee was inaugurated in July 2010 and has
since visited three (3) regions. Namely Northern Region, Brong Ahafo Region and WesternRegion.
Buruli Ulcer
Strategies were put in place to ensure early case detection. For the year under review, 1,005 cases were
reported. This ranged from 124 cases in Ashanti Akim North alone followed by Ga West with 121 cases.
The National case detection rate is 1.16/100,000. The programme collaborated with some research centers

2010 Annual Report Ghana Health Service
Page 25 of 76
including Noguchi to improve the diagnosis of Buruli ulcer using Polymerase Chain Reactions (PCRs).
Case management using antibiotics was strengthened through training of health workers. Surgical
outreach services were organized to support some districts to manage their cases.
H1N1 Influenza
Following the high incidence rate of Pandemic Influenza H1N1 in 2009, some measures were taken to reduce the
impact of the pandemic on health and minimize disruption to society and the economy. Among these were the
development of a National Action Plan, technical support visits and training of regional and district teams in
surveillance and management of the disease. The most prominent measure, however, was the deployment of
2,300,000 doses of PandemrixTM Pandemic Influenza Vaccine to priority groups of the population. The vaccination
campaign was undertaken to protect the public - reduce morbidity and mortality and the transmission of the virus
within communities.
Disease Surveillance, Emergency Preparedness and Response
Key activities undertaken under Disease Surveillance included:
Installation of Data entry templates for all regions
On-site orientation of staff on use of Epi-Info in managing IDSR data (weekly and monthly
reports)
Printing of 12,300 copies of CBS Registers (support from WHO)
Production of weekly and monthly bulletins on priority diseases and provision of feedback;
o Weekly - 43 / 52 (82.6%)
o Monthly – August produced / October
Completion of Yellow Fever risk assessment
Evaluation of IDSR (by Email)
Creation of Cholera awareness and improvement surveillance on diarrhoeal diseases in coastal
regions; Volta Central, Greater Accra, Western
Response to Cholera Outbreaks
Technical Support visit to the 3 Northern regions & BAR on meningitis
Supported- investigations into Meningitis Outbreaks in Jirapa & Bongo Districts
Initiation of assessment of core capacities –IHR
Carrying out of Port Health Activities

2010 Annual Report Ghana Health Service
Page 26 of 76
Holding of quarterly NPEC and NCC meetings were held during the period under review
Provision of Guinea Worm technical support to Eastern, Volta, Western and Greater Accra
Regions
Conduction of Local STOP activities
Sensitization of clinicians on selected priority diseases (Polio, Measles, Yellow fever, Pandemic
Influenza, Meningitis etc)
Supported Records review in some health facilities.
Environmental And Occupational Health And Safety
The Occupational and Environmental Health Unit has three (3) technical areas, namely Occupational
Health, Environmental Health and Poison Control.
Occupational health
Key Activities
Dissemination of Occupational Health and Safety Policy
Orientation of Regional, Institutional and District focal persons in Batanya, in the Central Region
Environmental health
Key Activities :
Conducted monitoring visits to Healthcare Waste Management (HCWM) in pilot project in
Swedru Hospital and Kwanyako Health Centre
Scoping exercise done for Strategic Health Impact Assessment for Oil & Gas sector carried out
with technical support from WHO
Completion of draft report on Situational Analysis & Needs Assessment (SANA) on the Strategic
health & environment alliance as part of implementation of the Libreville Declaration.

2010 Annual Report Ghana Health Service
Page 27 of 76
Poison control programme
Key Activities
• Responded to enquiries on poisoning; managed 24 patients with poisoning.
• Trained various staff on basic toxicology awareness and prevention of poisoning as well as first aid
for poisoning: Seventy two (72) community health nursing staff and 4 public health nursing staff
from 49 polyclinics, 4 hospitals, 4 reproductive and child health units, 2 maternity homes and 1
municipal health directorate within the Accra Metropolitan and Ledzokuku-Krowor Municipal
District of the Greater Accra Region.
• Trained Seventy-nine (79) farm workers from Ga East & Dangme West in safe handling of
chemicals.
• Trained some farmers, Agriculture Extension Officers, Environmental Protection Agency (EPA)
staff, pesticides dealers and health workers on recognition of effects of poisoning
Research and development
The Research and Development Division of the GHS became operational in January 2009 with the
mandate to generate information through relevant research, strengthen decision- making, fine-tune and set
health priorities
For the year 2010, the division;
conducted two supervisory visits to three (3) centres, - Navrongo, Kintampo and Dodowa,
Organized eight (8) local scientific meetings
Participated in five (5) international research output presentations.
Communication amongst the research centers and the international research community was ensured by
the effective and efficient maintenance of internet connectivity and access to HINARI, AGORA and
OARE.
Capacity development activities in the year comprised of:
training of a librarian in computer indexing to strengthen the documentation centre and support
provision of support to staff (4) to attend short courses
The GHS Ethical Review Committee reviewed 207 proposals within the year and approved of 152 for
implementation.
Some of the current research activities in the division include:

2010 Annual Report Ghana Health Service
Page 28 of 76
Strategies for Health Insurance for Equity in less Developed Countries (SHIELD) which aims at
evaluating existing inequities in health care and the extent to which health insurance mechanisms
could address equity challenges
ABBA, which aims to determine impact of scaling-up HIV/AIDS interventions on human
resources by identifying the health services most severely affected by HIV/AIDS and proposing
relevant health service indicators to inform sector needs.
2010 Annual Report Ghana Health Service
Page 29 of 76
HO-5 IMPROVE INSTITUTIONAL CARE, INCLUDING MENTAL
HEALTH SERVICE DELIVERY
Some of the activities undertaken in institutional care included
The GHS introduced a customer care program with support from Ecobank. The Bank supported the
development and launching of handbooks and posters on Customer Care. A video on customer care was
also developed and trainers for all the Regions were trained using the same support.
40 pharmacist, obstetricians and other health staff were trained on the pharmaceutical management of
uterotonics and a stakeholders meeting on the use of uterotonics was held.
Outreach services in Oral health and Eye Care were targeted at deprived areas .
The number of cataract surgeries done per one million population increased from 600 to 713. Although
this figure is still below the actual service need of 2,500 surgeries per million population, it is an
indication of our collective resolve to work harder to clear cataract cases which contributes about 45% to
the burden of blindness in Ghana.
A study to assess the quality of care for sick children in hospitals in selected hospitals was carried out as
part of the Better Medicine for children‟s project. The key findings were as follows:
Generally hospital support systems were adequate (running water, electricity, backup generator, soap etc)
Laboratory support was also good and laboratory results could be obtained in reasonable time: within two
hours, although some hospitals did not carry out cerebrospinal fluid microscopy
Drugs needed for management was most often available at the pharmacy but emergency drugs were not
readily available on the wards and emergency areas
There was shortage of professional nurses and in most of the facilities sick children were cared for by
student nurses, health care assistants and ward aides who had inadequate skills and knowledge to do this
job
There were gaps in the case management of common childhood illnesses, especially the management of
diarrhoea and malnutrition. Case management protocols and guidelines were most often not available.
Best practice was observed in the management of children with HIV/AIDS where there were protocols
and staff had been trained in their use.
The GHS signed a cooperative agreement with CDC aimed at strengthening clinical laboratories.
Activities under the agreement include;
Development of National Strategic Plan and Policy
Establishment of quality management systems
Preparation of selected labs for WHO accreditation
2010 Annual Report Ghana Health Service
Page 30 of 76
Piloting of Lab health information management system
Other partners who supported the laboratory services are IMAD, JSI/ DELIVER
The Taylor and Taylor project is ongoing and in 2010, the company started the replacement of laboratory
equipment that was supplied in the first phase projected
Mental Health
The poor quality of mental health at Accra Psychiatry hospital was brought to public domain in a
documentary by a Ghanaian journalist. As a result of which several interventions were put in place to
improve quality of care; some of these include
Provision of bore holes
Decongestion by discharging patients who have been stabilized and have been on admission for more than
5 years
Disciplinary measures against those who were found to have breeched regulations and rules
Security beefed up with 24hr security at the hospital
Seminars on medico legal issues, code of conduct and disciplinary procedures and quality assurance
Procurement of food supplies was streamlined

2010 Annual Report Ghana Health Service
Page 31 of 76
KEY PERFORMANCE INDICATORS BY OBJECTIVES
TABLES AND FIGURES
HEALTH OBJECTIVE ONE: Bridge Equity Gaps in access to health care
and nutrition services and ensure sustainable financing arrangements
that protect the poor
Outpatient Attendance
OPD attendance nationally has generally increased
significantly since 2008 from 0.77 to 0.98. Three
regions, Brong-Ahafo, Volta Region and Eastern
Region which showed a decline in OPD per capita in
2009 all showed increases in 2010. All the Regions
showed increase in OPD per capita. Upper East region
continue to show a consistent improvement in per
capita OPD attendance since 2006 when it recorded
0.55, and subsequently increasing to an OPD per capita
of 1.47 in 2010. Northern Region with its large land
mass and few facilities present a challenge to access
and this is shown in the low OPD per capita. Volta
Region is also similarly challenged, with its high patient to doctor ratio in comparison to the other regions
The doctor population ratio for Ghana, looking
at doctors on the government payroll improved
from 1 doctor to 11,929 to 1 doctor to 10,423.
Northern Region showed remarkable
improvement from one doctor to 50,751 in
2009to one doctor to 18,257 in 2010. The
improvement is due mainly to the efforts of the
Chief Executive of the Tamale Teaching
Hospital to attract doctors to the Hospital. There
is the need for the service to look at the
strategies that was used in Tamale to see how
REG 2007 2008 2009 2010
ASH 0.72 0.73 0.89 1.04
BAR 1.02 1.30 1.15 1.25
CR 0.70 0.68 0.71 0.81
ER 0.94 0.97 0.95 1.04
GAR 0.60 0.51 0.51 0.97
NR 0.31 0.49 0.53 0.54
UER 0.69 1.01 1.37 1.47
UWR 0.65 0.70 0.72 0.91
VR 0.51 0.73 0.69 0.76
WR 0.72 0.86 0.99 1.16
National 0.69 0.77 0.81 0.98
Region 2007 2008 2009 2010
ASH 10,667 9,537 8,288 7,184
BAR 22,479 21,475 16,919 22,967
CR 29,260 26,140 22,877 18,218
ER 18,141 17,571 16,132 15,801
GAR 5,202 4,959 5,103 4,099
NR 92,046 68,817 50,751 18,257
UER 30,111 33,475 35,010 31,214
UWR 43,265 43,988 47,932 27,050
VR 28,269 27,959 26,538 32,605
WR 33,794 31,745 33,187 31,190
National 12,591 12,713 11,929 10,423
TABLE 1: TREND OPD PER CAPITA BY REGION (2007-2010)
TABLE 2: TREND IN DOCTOR POPULATION RATIO BY REGION (2007-2010)

2010 Annual Report Ghana Health Service
Page 32 of 76
replicable this can be in other regions. With this improvement in Northern Region‟s doctor to population,
Volta Region now has the worst doctor patient ratio (1:32,190)
Compared to the previous year there appear
to be a worsening of the nurse to population
ratio. This may be due to the source of data
that was used in the previous years. The
number of midwives have been taken out of
the total number of nurses for the year 2010
resulting a lower total number of general
nurses. Unfortunately correction could not be
done for the previous years to make it
comparable. Overall however, there has
been improvement in the ratio as a result of
increase production and reduction in the
brain drain.
Community Based Health Planning and Services
39 55 84190 270 345 409
8681034
0200400600800
10001200
2002 2003 2004 2005 2006 2007 2008 2009 2010
Num
ber
of fu
ncti
onal
CH
PS
zone
s
Years
Fig 1. Trends in Functional CHPS Zones (2002-2010)
Region 2007 2008 2009 2010
ASH 2,028 1,336 1,173 1,156
BAR 1,964 1,140 993 1,245
CR 1,476 895 811 1,200
ER 1,175 959 832 953
GAR 979 881 874 800
NR 1,953 1,534 1,367 1,426
UER 1,132 956 805 926
UWR 1,209 870 750 842
VR 1,266 892 800 1,090
WR 2,004 1,413 1,213 1,398
National 1,342 1,079 971 1,077
TABLE 3: TREND IN NURSE POPULATION RATIO BY REGION (2007-2010)

2010 Annual Report Ghana Health Service
Page 33 of 76
There have been an increase in community health officers in all districts; most of them have already had
training in CHPS service delivery as part of their pre-service training. To make use of the increase
availability of trained Community Health Officers, many districts have taken the advantage to expand
CHPS in their districts. Functional CHPS have increased from 345 in 2007 to 1,034 in 2010. A functional
CHPS zone being defined as a geographically well defined area within a sub-district, which has been
assigned to a CHO, who has started offering service by home visits to clients in the zone, although one or
more key milestones like provision of a compound has not been achieved. The population covered by
CHPS moved from 15.3% in 2009 to 18.7% in 2010.
Table 4: Progress in the Implementation of CHPS by Region, 2008-2010
Region
2008 2009 2010
Funct
Funct
Funct
Ashanti 8 8 36
B/Ahafo 9 62 46
Central 46 68 93
Eastern 86 298 315
G/ Accra 5 20 83
Northern 39 75 78
U/ East 88 104 96
U/ West 41 85 93
Volta 42 50 71
Western 45 114 123
Totals 409 868 1034

2010 Annual Report Ghana Health Service
Page 34 of 76
National Health Insurance Scheme.
Upper west region presented the lowest number of facilities the NHIA for accreditation. None of the GHS
facilities failed, however facilities given provisional accreditation were in the following regions
Table 5. Percentage of facilities given provisional accreditation by Regions(Round2)
Region % facilities that were assessed and given
provisional accreditation
Brong Ahafo 19
Upper East 2
Volta 19
Western 2
Upper West had the highest proportion of facilities accredited grade A, followed by Greater Accra and
Northern regions whilst Volta, Ashanti and Brong Ahafo regions had the highest proportion of facilities
awarded grade D.
Fig 2. Accredited Facilities by grades (all facilities types) National Health Insurance

2010 Annual Report Ghana Health Service
Page 35 of 76
HEALTH OBJECTIVE TWO: IMPROVE GOVERNANCE AND
STRENGTHEN EFFICENCY IN HEALTH SERVICE DELIVERY,
INCLUDING MEDICAL EMERGENCIES
Financing mechanism and financial management systems
Table 6: Trends in Health Sector Budget for the period 2007-2010
TOTAL HEALTH SECTOR
BUDGET 2007 2008 2009
2010
SOURCE
BUDGET
(000) BUDGET BUDGET
BUDGET
(„000)
GOG
248,190.00
268,517.00
344,398.00
400,451.00
HEALTH FUND/SBS
18,900.00
126,731.00
63,981.00
79,823.00
EARMARKED FUNDS
78,583.50
92,191.00
18,602.00
243,294.00
IGF
52,100.00
115,070.00
108,312.00
208,180.00
NHIF
175,909.70
235,430.00
462,940.00
480,908.00
HIPC
9,500.00
6,485.00
11,427.00
8,000.00
TOTAL HEALTH SECTOR
BUDGET
583,183.20
844,424.00
1,009,660.00
1,420,656.00
The overall budget for health increased for the year 2010. Most of the increase however, was in IGF with
an increase of 92.2%. The shift of source of funding from GOG to internally generated fund is shifting
funds from public health to clinical care. The public health units at the District level do not generate any
IGF. They depend heavily on the GOG to run their activities. The present situation is making it very
difficult for District Health Directorates to implement their planned activities for the year. The increase in
the earmarked funding from 18,602 Ghana cedis to 243,294 Ghana cedis inhibits district initiatives for

2010 Annual Report Ghana Health Service
Page 36 of 76
service delivery as the earmarked funds are allocated to very specific activities at the District level which
might not be the priority of the district.
Table7: Statement of Receipts and expenditure for GHS for the Year 2010
Statement of Income and Expenditure
Source Receipt Exp % diff
GoG 5,916,700.99 14,977,067.50 -153.1%
IGF 219,719,142.10 217,488,775.18 1.01%
SBS 3,104,377.79 2,874,417.02 7.4%
Programme 86,924,059.95 72,021,992.64 17.1%
Total 315,664,280.83 307,362,252.34 2.6%
For the total non-wage recurrent receipts, 69.6% of total receipts for the year 2010 came from internally
generated funds. The decrease in receipts from GOG is a source of concern. GOG constitute only 1.9% of
total receipts for the year 2010. The over expenditure for the GOG for the year 2010 was as a result of
money received in late 2009 that was used in the early part of 2010.

2010 Annual Report Ghana Health Service
Page 37 of 76
There was an improvement in the fleet size of the service, with the introduction of the facilities vehicle
hire purchase schemes. Other programs also procured vehicles for both the Regions and Districts. More
motorbikes were also provided for the districts.
Table 8: GHS FLEET SIZE AS AT DEC 2010
REGION VEHICLE MOTORBIKE
ASHANTI 120 532
BRONG-AHAFO 150 764
CENTRAL 109 457
EASTERN 170 756
GREATER ACCRA 127 340
NORTHERN 183 871
UPPER EAST 131 640
UPPER WEST 102 582
VOLTA 130 696
WESTERN 94 627
HEADQUARTERS 225 47
TOTAL 1,541 6,312

2010 Annual Report Ghana Health Service
Page 38 of 76
HEALTH OBJECTIVE THREE: IMPROVE ACCESS TO QUALITY
MATERNAL, NEONATAL, CHILD AND ADOLESCENT HEALTH
SERVICES
TABLE 9: KEY SECTOR PERFROMANCE INDICATORS (2006-2010)
Indicator
2007 2008 2009 2010
Institutional MMR (per 1000 live births) 224 200 169.9 163.2
HIV prevalence among pregnant women 15-24 yrs 2.6% 2.2% 2.9% 2.0
ANC coverage 91.1% 97.4% 92.1% 93.3%
% Deliveries attended by a trained
Health worker
32.1% 44.2% 45.6% 49.5%
PNC coverage 56.7% 57.5% 56.0% 61.6%
FP Acceptor Rate 23.2% 33.8% 31.1% 24.9%
Penta 3 coverage 87.8% 86.6% 89.3% 87.1%
Measles coverage 88.6% 86.5% 89.1% 87.7%
Institutional Maternal Mortality ratio
There has been a gradual decrease in the institutional maternal mortality ratio. It has reduced from
169.9/100,000LB to 163.2LB. Although the decreases have not been so significant, it is a reflection of all
the interventions that have been put in place towards achieving MDG5. Volta Region has a high maternal
mortality ratio(209.6/100,000LB) compared to the other Region with Northern Region recording lowest
Institutional Maternal mortality ratio of 137.2/100,000LB. One of the factors that influence Institutional
Maternal mortality ratio is the utilization of facilities, Northern Region with its low skilled delivery of
36.8%, need to ensure that women are not dying within the communities
Ante natal Care
Efforts to provide quality maternal care services continue to be high priority in the GHS. This focus is
yielding positive results in the coverage of skilled attendance across the country. There was a marginal
increase in the ANC coverage an improvement over the previous year when there was a decrease. Efforts
in addressing the MDG5 through the posting and training of midwives to health centers and CHPS
compounds may be responsible for this trend.

2010 Annual Report Ghana Health Service
Page 39 of 76
Skilled Delivery
Skilled delivery rate improved nationally from 45.6%2009 to
49.5%2010. However, there are inter-regional variations: Upper
East, Western, Northern, Ashanti and Brong Ahafo Region
have all shown consistent increase in skilled delivery from the
year 2008. Greater Accra recovered from the drop in 2009 and
increase coverage to 54.4% this may be a reflection of
improvement in data collection from the private sector. There
has been a reduction in coverage in the Volta and Eastern
Region. Skilled delivery coverage which is delivery made by a
trained health worker is dependent on the distribution of these
staff. Volta Region has seen a worsening in the midwife to
population ratio during the year 2010. Also most of their
nurses are old, so they are not practicing.
Immunization
General performance in immunization as
measured by Penta III coverage dropped from
89.3%2009 to 87.1 %2010. The drop in coverage
was in all the regions with the exception of
Ashanti Region. Several factors are
contributing to this decline. Some of the
reasons are: Poor data capture especially in the
Greater Accra Region. Inadequate and delays
in the release of funds for district activities
also affected the outreach services organized
by district to provide immunization service for
hard to reach communities resulting in low
coverage. Funds for district service activities
were released to the Districts in late May 2010.
The best time for immunization activities is during the dry season from January to April, when most
communities are accessible.
SUP-DEL 2007 2008 2009 2010
ASH 26.7 35.0 42.4 53.4
BAR 34.5 49.8 53.7 54.0
CR 22.3 56.3 52.5 51.6
ER 43.1 48.0 52.1 48.2
GAR 43.1 50.2 47.9 54.4
NR 27.7 26.0 36.1 36.8
UER 43.5 40.4 52.6 59.7
UWR 32.9 40.6 36.7 46.5
VR 33.3 37.5 39.4 36.9
WR 17.6 39.1 42.6 49.6
National 32.1 42.2 45.6 49.5
Region 2007 2008 2009 2010
ASH 72.0 76.8 83.7 86.5
BAR 100.0 97.3 95.0 94.3
CR 93.0 92.2 96.6 94.3
ER 93.0 93.0 94.5 93.6
GAR 68.0 68.3 72.7 70.1
NR 124.0 114.5 123.0 109.2
UER 102.0 94.8 106.0 83.1
UWR 94.0 87.5 90.1 81.7
VR 84.0 83.8 82.9 81.4
WR 93.0 89.0 88.6 86.4
National 87.8 86.6 89.3 87.1
TABLE 11: TREND OF PENTA III COVERAGE BY REGION
(2006-2009)
TABLE 10: TREND SKILLED DELIVERY BY REGION (2006-2010)

2010 Annual Report Ghana Health Service
Page 40 of 76
Figure 3 TREND OF EARLY CHILDHOOD MORTALITIES IN GHANA
The trend in early child mortalities in Ghana has
shown a gradual decline in neonatal, infant and under-five mortality. This augurs well for the country‟s
bid to achieve the MDG4. There have been no deaths from measles in Ghana for the past seven years.
Most of the decline in childhood mortality has been in the under five, where immunization has contributed
greatly to reducing preventable deaths. Neonatal mortality has however shown little decline and there is
the need to concentrate efforts in reducing this further.

2010 Annual Report Ghana Health Service
Page 41 of 76
HEALTH OBJECTIVE FOUR: INTENSIFY PREVENTION AND
CONTROL OF COMMUNICABLE AND NON-COMMUNICABLE
DISEASES AND PROMOTE HEALTHY LIFESTYLES
FIGURE 4 TREND OF NOTIFIED CASES OF TB (2005 -2009)
The Service is not doing too well with regards to TB case notification. After the increase from 2007 of
57/100,000 population to 64/100,000 in 2009, there was a decline to 63/100,000 pop in 2010. This might
be partly due to low level of suspicion of TB by prescribers and the low numbers of Laboratories to do the
sputum microscopy for the diagnosis.

2010 Annual Report Ghana Health Service
Page 42 of 76
Table 12: Summary of core surveillance indicators, Jan – Dec 2008 - 2010
Indicator Target 2008 2009 2010
Timeliness of Monthly ≥ 80% 74 92 86
Annualized non polio AFP rate per
100,000 Pop chn. < 15yrs.
≥ 2.0 2.24 2.53 1.82
% Adequacy of stool ≥80% 78.0 75.3
% of Districts reporting at least
one suspected case of measles
investigated with blood specimen
≥80% 90.6 81.1 80.5
% of Districts reporting at least
one suspected case of yellow fever
investigated with blood specimen
≥80% 59.0 48.0 59.4
Meningitis case fatality rate ≥10% 21.4 18.8 >10
Cholera case fatality rate (%) ≥1% 1.7 0.7 1.8
Selected core surveillance indicators:
Focal Outbreaks of H1N1 occurred mostly in schools – Eastern, Volta and Brong Ahafo Region
All regions reported suspected cases; Upper East Region did not confirm any suspected H1NI cases. There
were 75% of Confirmed cases in Greater Accra Region and 5.5% in Eastern.

2010 Annual Report Ghana Health Service
Page 43 of 76
Table 13 Distribution of H1NI vaccination and AEFI by Regions.
Regions Total
Population
Target 10% of total
population
Total
Vaccinated Coverage Total AEFI
Ashanti 5,014,536 501,454 288,454 57.5 29
Brong-Ahafo 2,323,878 232,388 108,357 46.6 14
Central 1,961,997 196,200 135,700 69.2 60
Eastern 2,420,925 242,093 156,918 64.8 172
Greater Accra 4,469,506 446,951 280,804 62.8 455
Northern 2,399,912 239,991 163,505 68.1 -
Upper East 1,026,458 102,646 77,099 75.1 28
Upper West 682,452 68,245 52,605 77.1 2
Volta 1,974,112 197,411 142,864 72.4 54
Western 2,637,135 263,713 171,737 65.1 11
National 24,910,911 2,491,091 1,578,043 63.3 825
Cholera and Meningitis: A review of the core surveillance indicators in 2010 showed that cholera case
fatality rate increased from 0.7 in 2009 to 1.8 in 2010 whereas that of meningitis decreased from 18.8 in
2009 to just above 10% in 2009.
More need to be done on the clinical management of meningitis, although the case fatality have reduced
from 18.8 to just above 10%, it is still unacceptably high. Late reporting of cases to facilities also
contributes to the poor outcomes.

2010 Annual Report Ghana Health Service
Page 44 of 76
FIGURE 5. PROPORTION OF OPD CASES ATTRIBUTED TO MALARIA (2006 -2010)
The proportion of total OPD attributed to malaria continues to increase. With the introduction of the rapid
diagnostic tests (RDTs) for malaria it was believed that the proportion of OPD attributed to malaria was
going to decrease. Unfortunately this has not happened, and for the 2010 year there was actually an
increase. It has been found that there is the need to train clinicians and prescribers on how to manage cases
with fever as most diagnose anyone with fever as having malaria and treating them as such. This has been
found to be the case even when RDTs are used and the results have been negative for malaria parasites.

2010 Annual Report Ghana Health Service
Page 45 of 76
FIGURE 6: PROPORTION OF TOTAL CASES AND DEATHS ATTRIBUTED TO MALARIA, 2006-2010
34.10 of total admissions in health facilities were attributed to malaria and 19% of total deaths in health
facilities were also attributed to malaria( Fig 6). The results shows an increasing trend in the admissions
and death attributed to malaria. This is in contrast to the decreasing malaria case fatality rate in children
under five years. There is the need for a study to ascertain whether these admissions and deaths attributed
were really malaria cases.
FIGURE 7: UNDER 5YRS MALARIA CASE FATALITY RATE 2002-2010
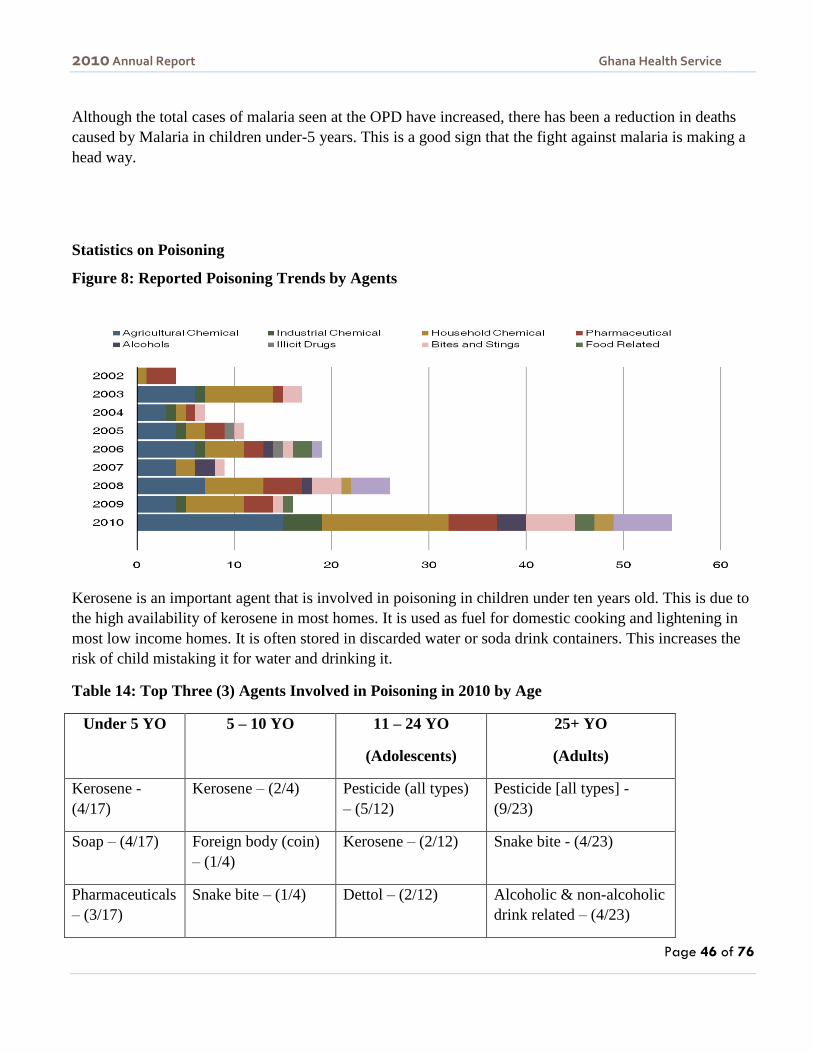
2010 Annual Report Ghana Health Service
Page 46 of 76
Although the total cases of malaria seen at the OPD have increased, there has been a reduction in deaths
caused by Malaria in children under-5 years. This is a good sign that the fight against malaria is making a
head way.
Statistics on Poisoning
Figure 8: Reported Poisoning Trends by Agents
Kerosene is an important agent that is involved in poisoning in children under ten years old. This is due to
the high availability of kerosene in most homes. It is used as fuel for domestic cooking and lightening in
most low income homes. It is often stored in discarded water or soda drink containers. This increases the
risk of child mistaking it for water and drinking it.
Table 14: Top Three (3) Agents Involved in Poisoning in 2010 by Age
Under 5 YO 5 – 10 YO 11 – 24 YO
(Adolescents)
25+ YO
(Adults)
Kerosene -
(4/17)
Kerosene – (2/4) Pesticide (all types)
– (5/12)
Pesticide [all types] -
(9/23)
Soap – (4/17) Foreign body (coin)
– (1/4)
Kerosene – (2/12) Snake bite - (4/23)
Pharmaceuticals
– (3/17)
Snake bite – (1/4) Dettol – (2/12) Alcoholic & non-alcoholic
drink related – (4/23)

2010 Annual Report Ghana Health Service
Page 47 of 76
Non communicable Diseases – Hypertension
Analysis of 2010 morbidity data indicates that there were twice as many female cases of hypertension than
men. This could be due to that fact that more females attend hospitals than men.
Fig 9: Male female distribution among cases of Hypertension seen in health facilities
Source CHIM
The age distribution for all cases (Males and females) showed a fairly even distribution among ages above
35yrs age groupings. Slightly higher percentage was observed in the 70+ age group which is to be
expected but for the younger age groups 35-49 the proportion of cases being similar to the older
populations is of concern which requires further investigation.
Fig 10: Age Distribution – Hypertension cases OPD Morbidity 2010 CHIM
Source CHIM

2010 Annual Report Ghana Health Service
Page 48 of 76
HEALTH OBJECTIVE FIVE: IMPROVE INSTITUTIONAL CARE,
INCLUDING MENTAL HEALTH SERVICE DELIVERY
Malaria was the commonest condition seen at the OPD accounting for about 44% of all
conditions seen.
Table15: Top Ten Diseases seen at the OPD
Malaria
All Other Diseases
Other ARI(Acute Respiratory
Infection)
Skin Diseases & Ulcers
Diarrhoea Diseases
Hypertension
Rheumatism and Joint Paints
Intestinal worms
Acute Eye infection
Anaemia
Pregnancy and Related
Complications
Acute Urinary Tract Infection
Typhoid/Enteric Fever

2010 Annual Report Ghana Health Service
Page 49 of 76
CHALLENGES
Objective 1: Bridge gaps in access to health care and nutrition services
and ensure sustainable financing arrangements that protects the poor
Human Resource
Lack of updated and comprehensive HR database
Swelling health sector wage bill
Inequitable distribution of available staff
Poor monitoring system to track disengaged staff
High attrition rates
Delayed promotions
Inadequate support from Regional and Divisional Directors on HR activities particularly the
updating and submission of nominal rolls on quarterly basis.
Objective 2: Improve governance and strengthen efficiency in health
service delivery, including medical emergencies .
Lack of payment for vehicle maintenance services which is threatening to collapse the Central
Mechanical Workshop
Blatant disregard for GHS Capital Investment Plan by MoH
Lack of spare parts particularly for corrective maintenance of laundry equipment
Inadequate number and aging artisans
Lack of commitment on the part of some institutional managers to commit funds and logistics
towards maintenance of health infrastructure
Poor coordination in the supply and installation of medical equipment by various programme,
donors and BEU
2010 Annual Report Ghana Health Service
Page 50 of 76
Objective 3: Improve access to quality maternal, neonatal, child and
adolescent health services
Inadequate numbers and poor distribution of midwives to provide deliveries by skilled attendants.
Lack of Blood bank facilities in most Hospitals
Inadequate medical equipment.
Inadequate resources for in-service training, fellowship and other management and leadership
training
Out-dated staffing norms for facilities, making re-distribution of essential health staff difficult.
Objective 4: Intensify prevention and control of communicable and non -
communicable diseases and promote healthy lifestyles .
• Delays in getting results of YF investigations from Institute de Pasteur (Dakar)
• Erratic supply of yellow fever reagents to the NPHRL
• Inadequate reporting during outbreaks including observance of daily reporting
• Poor use of existing case definition
• There is little idea about index of suspicion of cholera cases
• Vehicle for Rapid Response activities not performing optimally
• Inadequate documentation of surveillance activities
Non-use of outbreaks/rumour logbooks.
General low awareness on NCDs
Inappropriate care behaviour – low utilization, late reporting
General lack of national screening programmes for NCDs
Limited diagnostic or screening equipment for NCDs
Inadequate or absent treatment guidelines for NCDs
Counselling at health facilities for NCDs – weak, or not well done
Limited palliative services
2010 Annual Report Ghana Health Service
Page 51 of 76
Objective 5: Improve institutional care including mental health service
delivery
Compliance to national guidelines is low especially at the lower level where clinical care structures
are very weak , this coupled with non availability in most of the facilities
Inadequate Staffing in health facilities coupled with maldistribution and poor attitude affect
quality of services
In the earlier part of the year delayed payment of claims by NHIA affected service provision
The coverage of Clinical care interventions (IPC, Patient Safety, Customer Care) is very low and
thus their impact cannot be felt
Poor quality of some of the clinical care data

2010 Annual Report Ghana Health Service
Page 52 of 76
THE WAY FORWARD FOR 2010
Objective 1:Bridge the equity gaps in access to health care and nutrition
services and ensure sustainable financing arrangements that protect the
poor.
Scale out standard HR tool (WAHO HRIS Software) to support HR Planning and budget at National
and Regional Level.
Forecast HR needs of the GHS.
Complete reviewing staffing norms
Production of HR Bulletin (Newsletter)
Updating of Nominal Roll
Headquarters levels
Regional Levels
Reconciliation of Nominal roll with Payroll
Provide Technical Support to other HR Units and Regions Scale out standard HR tool (WAHO HRIS
Software) to support HR Planning and budget at National and Regional Level.
Forecast HR needs of the GHS.
Complete reviewing staffing norms
Production of HR Bulletin (Newsletter)
Updating of Nominal Roll
Headquarters levels
Regional Levels
Reconciliation of Nominal roll with Payroll
Provide Technical Support to other HR Units and Regions
Objective 2:Improve governance and strengthen efficiency in health
service delivery, including medical emergencies .
Undertake Planned Preventive and Corrective Maintenance Programmes – transport, equipment
and buildings
Promote the use of Standard Designs and Specifications for construction of various types of health
facilities
Develop criteria for prioritization of infrastructure development
Healthcare Waste Management programme – conduct regional trainings with EHCU and construct
13 incinerators in selected health facilities.
2010 Annual Report Ghana Health Service
Page 53 of 76
Collate information and monitor civil works procurement plans of all RHDs and GHS HQ
Pursue the Completion of the GHS Hq. Rehabilitation Project including the construction of access
road to the 28th February crossing road
Implement GHS Capital Plan and provide technical support for ADB PIU, OPEC PIU,
Bolgatanga Regional Hospital PIU
Revamp the Boat Management System
Develop Standard Transport Operating Procedures (STOPs) also known as Transport Manual to
guide the operational management of transport resources
Sustain new initiative for vehicle replacement – Hire Purchase Scheme.
Work towards strengthening Procurement and Logistics systems in the GHS.
Liaise with PPA in the training of the ETC Members and Practitioners.
Advocate for establishment of the Central Procurement Account.
Objective 3:Improve access to quality maternal, neonatal, child and
adolescent health services.
• Improve on Monitoring & Supervision (maternal, newborn & nutrition surveillance)
• Implement EMONC Assessment recommendations
• Provide modern equipment – sonicaid, portable Ultrasound, CTG Monitors for health facilities
• Build Capacity of Staff to offer quality care.
• Improve on Technical support to Regions, Districts, Division, Programmes and Partner agencies
• Strengthen Health Promotion Department & Resource Centre to provide materials for behaviour
change communication.
Objective 4:Intensify prevention and control of communicable and non -
communicable diseases and promote healthy lifestyles.

2010 Annual Report Ghana Health Service
Page 54 of 76
Strengthen the skills and practices of health personnel in the core surveillance functions through
structured and integrated in-service training and enhanced facilitative supervisory support visits
Complete adaptation of Second Edition of IDSR Technical Guidelines and its Training Modules to
address declining core functions
Print and distribute 400 copies of revised IDSR technical guidelines
Organize zonal surveillance review meetings for District Surveillance Officers
Installation of Data entry templates for all regions and on-site orientation of staff on the use of
Epi-Info in managing IDSR data (weekly and monthly reports)
Update database (inventory) for Community Based Surveillance
Produce weekly and quarterly bulletins on priority diseases and provide feedback to the regions.
This would be done in collaboration with Program managers and Center for Health Information
Management in this direction.
Expand screening centres for cervical cancer
Strengthen cancer registration, early detection, palliative care
Scale up newborn screening SCD
Continue advocacy for more NCDCP staff and Regional Focal Persons
Objective 5: Improve institutional care including mental health service
delivery.
The will be steps to initiate the establishment of the District Clinical care teams as defined in the
Act 525.
Some of Gaps identified in the quality of care for sick children in hospitals will be addressed
through the provision of clinical care guidelines, engaging the Paediatric Society, collaborating
with the better Medicine for Children‟s project a
Improving collaboration between public health and clinical care at all level should be placed on
GHS agenda
The Impact of clinical care interventions will be felt if there is scaling up to all health facilities
such as infection prevention and control, patient safety, customer care, accidents and emergency,
data quality audit, clinical audit In this regard, performance of health facility managers must be
linked to the implementation of clinical care interventions
National clinical lab will be strengthened to enable it coordinate the implementation of GHS CDC
cooperative and other lab agreements

2010 Annual Report Ghana Health Service
Page 55 of 76
Continue collaboration with NHIA in the accreditation program. In addition GHS facilities that fail
or awarded provisional accreditation will be supported to gain accreditation
Introduce clinical data quality audit
Complete draft clinical care guidelines and disseminate
Continue specialist outreach service
Intensify clinical supervision
Undertake research on neonatal care and baseline A and E services
Contribute to programs that will improve maternal health and make blood available and safe

2010 Annual Report Ghana Health Service
56
ANNEXES: TRENDS IN SECTOR INDICATORS
Doctor to Population Ratio
2010 2009 2008
Number of Doctors Doctors Population
ratio Number of Doctors
Doctor Population
Ratio Number of Doctors
Doctor Population
Ratio
ASHANTI 684 7,184 589 8,288 495 9,537
BRONG AHAFO 99 22,967 134 16,919 103 21,475
CENTRAL 113 18,218 84 22,877 72 26,140
EASTERN 163 15,801 148 16,132 134 17,571
GREATER CCRA 935 4,099 839 5,103 827 4,959
NORTHERN 134 18,257 46 50,751 33 68,817
UPPER EAST 33 31,214 29 35,010 30 33,475
UPPER WEST 25 27,050 14 47,932 15 43,988
VOLTA 64 32,605 73 26,538 68 27,959
WESTERN 75 31,190 77 33,187 78 31,745
TOTAL 2,325 10,423 2,033 11,929 1,855 12,713

2010 Annual Report Ghana Health Service
57
Nurse to Population Ratio
Region
2010 2009 2008
Number of nurses Nurse population
ratio Number of Nurses
Nurse Population
Ratio Number of Nurses
Nurse Population
Ratio
ASHANTI 4,252 1,156 4,161 1,173 3533 1,336
BRONG AHAFO 1,826 1,245 2,283 993 1940 1,140
CENTRAL 1,715 1,200 2,369 811 2104 895
EASTERN 2,703 953 2,871 832 2454 959
GREATER CCRA 4,793 800 4,897 874 4656 881
NORTHERN 1,716 1,426 1,708 1,367 1480 1,534
UPPER EAST 1,112 926 1,262 805 1051 956
UPPER WEST 803 842 895 750 758 870
VOLTA 1,914 1,090 2,421 800 2132 892
WESTERN 1,673 1,398 2,107 1,213 1753 1,413
TOTAL 22,507 1,077 24,974 971 21,861 1,079

2010 Annual Report Ghana Health Service
58
Hospital Bed Utilization Statistics
Region Percentage Occupancy Average Length of Stay
2010 2009 2008 2010 2009 2008
ASHANTI 69.4 65.5 63.3 3.9 4.0 4.2
BRONG AHAFO 62.2 57.9 60.5 3.8 3.5 3.9
CENTRAL 50.5 51.4 52.5 3.6 3.5 4.0
EASTERN 57.4 55.9 55.6 4.2 4.2 4.4
GREATER CCRA 86.1 78.3 72.0 6.4 6.0 6.4
NORTHERN 71.0 59.1 61.3 3.0 2.2 2.7
UPPER EAST 52.5 49.7 42.2 2.7 2.8 2.9
UPPER WEST 66.1 62.1 59.4 3.5 3.5 3.4
VOLTA 52.9 54.1 51.1 4.2 4.5 4.9
WESTERN 53.8 52.0 51.5 3.3 3.3 3.7
TOTAL 63.2 59.8 58.3 3.9 3.8 4.2

2010 Annual Report Ghana Health Service
59
Region
Turnover Per Bed Turnover Interval
2010 2009 2008 2010 2009 2008
ASHANTI 64.6 59.7 54.7 1.7 2.1 2.5
BRONG AHAFO 60.5 59.8 56.6 2.3 2.6 2.6
CENTRAL 51.0 54.2 47.9 3.5 3.3 3.6
EASTERN 49.7 49.0 46.1 3.1 3.3 3.5
GREATER CCRA 49.5 47.3 41.4 1.0 1.7 2.5
NORTHERN 87.8 98.2 81.6 1.2 1.5 1.7
UPPER EAST 72.0 65.0 52.8 2.4 2.8 4.0
UPPER WEST 68.9 64.0 63.2 1.8 2.2 2.4
VOLTA 46.3 44.1 38.4 3.7 3.8 4.7
WESTERN 60.3 57.0 50.6 2.8 3.1 3.5
TOTAL 58.8 57.1 51.1 2.3 2.6 3.0
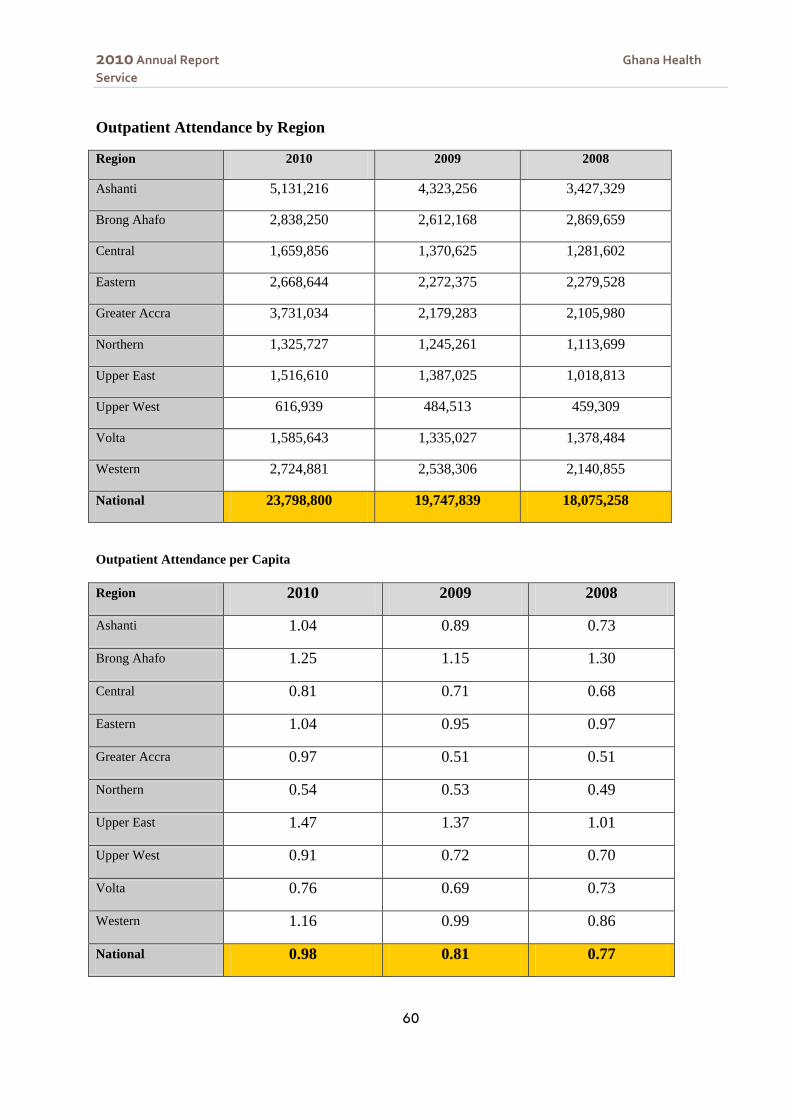
2010 Annual Report Ghana Health
Service
60
Outpatient Attendance by Region
Region 2010 2009 2008
Ashanti 5,131,216 4,323,256 3,427,329
Brong Ahafo 2,838,250 2,612,168 2,869,659
Central 1,659,856 1,370,625 1,281,602
Eastern 2,668,644 2,272,375 2,279,528
Greater Accra 3,731,034 2,179,283 2,105,980
Northern 1,325,727 1,245,261 1,113,699
Upper East 1,516,610 1,387,025 1,018,813
Upper West 616,939 484,513 459,309
Volta 1,585,643 1,335,027 1,378,484
Western 2,724,881 2,538,306 2,140,855
National 23,798,800 19,747,839 18,075,258
Outpatient Attendance per Capita
Region 2010 2009 2008
Ashanti 1.04 0.89 0.73
Brong Ahafo 1.25 1.15 1.30
Central 0.81 0.71 0.68
Eastern 1.04 0.95 0.97
Greater Accra 0.97 0.51 0.51
Northern 0.54 0.53 0.49
Upper East 1.47 1.37 1.01
Upper West 0.91 0.72 0.70
Volta 0.76 0.69 0.73
Western 1.16 0.99 0.86
National 0.98 0.81 0.77

2010 Annual Report Ghana Health
Service
61
Inpatient Admissions by Region
Region 2010 2009 2008
Ashanti 225,629 207,089 145,316
Brong Ahafo 123,187 111,521 104,976
Central 79,562 77,620 60,658
Eastern 139,159 127,050 121,985
Gr. Accra 132,975 112,314 79,974
Northern 118,499 116,818 66,146
Upper East 66,538 56,324 48,507
Upper West 51,605 44,287 42,061
Volta 101,653 93,829 83,093
Western 121,263 115,246 94,037
National 1,160,070 1,062,098 846,753
Hospital Admission Rate
Region 2010 2009 2008
Ashanti 45.92 42.42 30.78
Brong Ahafo 54.18 49.19 47.46
Central 38.65 40.39 32.23
Eastern 54.03 53.21 51.81
Greater Accra 34.69 26.23 19.50
Northern 48.44 50.04 29.13
Upper East 64.60 55.48 48.30
Upper West 76.31 66.00 63.75
Volta 48.71 48.43 43.71
Western 51.84 45.10 37.98
National 47.87 43.79 35.91

2010 Annual Report Ghana Health
Service
62
PUBLIC HEALTH SERVICES
HIV Prevalence among pregnant women attending ANC clinics by Region
Region 2010 2009 2008
Ashanti 3.0 3.9 3.0
Brong Ahafo 2.0 2.9 2.6
Central 1.7 3.0 2.0
Eastern 3.2 4.2 4.5
Greater Accra 2.6 3.2 3.0
Northern 0.7 2.0 1.1
Upper East 2.4 2.2 2.0
Upper West 1.7 3.1 1.6
Volta 1.8 2.6 1.7
Western 2.5 3.1 2.9
National 2.0 2.9 2.2
HIV Prevalence among pregnant women by Age Groups
Age Group 2010 2009 2008
15 – 19 Yrs 1.1 1.9 1.2
20 – 24 Yrs 1.7 2.2 2.3
25 – 29 Yrs 2.5 3.7 3.0
30 – 34 Yrs 2.8 3.4 2.8
35 – 39 Yrs 2.8 3.6 2.9
40 – 44 Yrs 2.1 4.0 1.8
45 – 49 Yrs 2.7 1.8 2.6
15 – 24 Yrs 1.5 2.1 1.9

2010 Annual Report Ghana Health
Service
63
Guinea Worm Cases
Region 2010 2009 2008
Ashanti 0 2 5
Brong Ahafo 0 2 11
Central 0 0 1
Eastern 0 1 2
Greater Accra 0 0 0
Northern 8 237 479
Upper East 0 0 1
Upper West 0 0 1
Volta 0 0 1
Western 0 0 0
National 8 242 501

2010 Annual Report Ghana Health
Service
64
Tuberculosis Cure Rate
Region 2009 2008 2007
Ashanti 77.4 81.4 82.3
Brong Ahafo 71.3 70.9 64.1
Central 86.3 87.1 81.8
Eastern 73.8 75.5 72.9
Greater Accra 81.7 81.5 82.5
Northern 79.3 74.8 76.3
Upper East 88.3 72.2 75.0
Upper West 54.6 42.1 44.5
Volta 90.7 88.0 79.8
Western 77.6 73.5 74.2
National 79.1 77.9 77.5
Tuberculosis Success Rate
Region 2009 2008 2007
Ashanti 88.8 90.3 90
Brong Ahafo 78.9 82.3 77
Central 90.4 89.8 87
Eastern 80.5 82.0 79
Greater Accra 87.5 84.4 87
Northern 84.5 87.8 83
Upper East 89.1 76.9 79
Upper West 73.6 61.8 71
Volta 97.1 93.4 87
Western 90.9 86.5 86

2010 Annual Report Ghana Health
Service
65
National 87.0 85.5 84
Expanded Program on Immunization
Measles Immunization Coverage Rate
REGION 2010 2009 2008
Ashanti 87.8 87.1 80.7
Brong Ahafo 95.5 93.9 96.6
Central 97.4 98.1 94.4
Eastern 96.0 94.0 95.1
Greater Accra 71.2 74.0 67.3
Northern 107.1 119.7 109.2
Upper East 83.6 105.9 93.1
Upper West 82.0 90.5 90.0
Volta 78.4 78.3 78.8
Western 85.7 85.1 87.5
National 87.7 89.1 86.5
Penta 3 Immunization Coverage Rate
REGION 2010 2009 2008
Ashanti 86.5 83.7 76.8
Brong Ahafo 94.3 95.0 97.3
Central 94.3 96.6 92.2
Eastern 93.6 94.5 93.0
Greater Accra 70.1 72.7 68.3
Northern 109.2 123.0 114.5
Upper East 83.1 106.0 94.8
Upper West 81.7 90.1 87.5

2010 Annual Report Ghana Health
Service
66
Volta 81.4 82.9 83.8
Western 86.4 88.6 89.0
National 87.1 89.3 86.6
OPV 3 Immunization Coverage Rate
REGION 2010 2009 2008
Ashanti 86.3 83.6 76.7
Brong Ahafo 94.1 93.8 97.2
Central 92.9 93.7 90.9
Eastern 93.1 94.2 92.7
Greater Accra 70.3 72.3 68.4
Northern 109.0 122.1 114.2
Upper East 82.8 105.4 89.2
Upper West 81.7 89.3 87.4
Volta 81.5 83.1 83.8
Western 86.0 88.0 88.4
National 86.8 88.7 86.1

2010 Annual Report Ghana Health
Service
67
BCG Immunization Coverage Rate
REGION 2010 2009 2008
Ashanti 105.5 101.6 95.7
Brong Ahafo 111.6 111.1 111.6
Central 120.5 123.9 118.6
Eastern 114.3 114.2 111.7
Greater Accra 78.8 75.6 76.4
Northern 126.8 139.5 131.0
Upper East 91.3 123.5 107.3
Upper West 92.3 104.6 105.2
Volta 94.1 94.5 98.1
Western 99.0 100.7 103.0
National 102.1 103.8 102.6
Tetanus Toxoid Immunization Coverage Rate
REGION 2010 2009 2008
Ashanti 78.0 83.1 80.2
Brong Ahafo 84.9 82.2 89.8
Central 94.3 89.6 93.2
Eastern 83.6 85.1 80.7
Greater Accra 67.4 66.8 59.6
Northern 93.5 108.0 97.9
Upper East 63.8 85.5 66.2
Upper West 69.4 71.2 71.6
Volta 60.8 63.9 63.7

2010 Annual Report Ghana Health
Service
68
Western 62.8 62.6 62.7
National 76.2 78.6 76.3
Yellow Fever Immunization Coverage Rate
REGION 2010 2009 2008
Ashanti 87.4 86.8 80.4
Brong Ahafo 95.1 94.0 94.8
Central 95.1 96.8 91.3
Eastern 95.9 94.2 95.4
Greater Accra 43.2 73.2 66.8
Northern 106.0 118.7 107.6
Upper East 81.5 107.5 84.8
Upper West 82.6 89.5 88.0
Volta 78.5 78.2 79.0
Western 85.5 84.7 93.1
National 87.5 88.8 86.0
AFP Non - Polio Rate
REGION 2010 2009 2008
Ashanti 1.48 2.1 1.35
Brong Ahafo 2.40 3.6 4.22
Central 1.38 3.8 2.00
Eastern 1.60 4.0 2.70
Greater Accra 0.95 1.0 1.06
Northern 2.20 2.4 3.40
Upper East 2.00 5.3 4.50
Upper West 4.00 4.0 3.33

2010 Annual Report Ghana Health
Service
69
Volta 3.13 2.3 1.63
Western 2.18 1.5 2.10
National 1.82 2.5 2.24
Reproductive Health Services
ANTENATAL COVERAGE SUPERVISED DELIVERY
REGION 2010 2009 2008 2010 2009 2008
Ashanti 84.7 80.7 86.1 53.4 42.4 35.0
Brong Ahafo 82.3 97.9 102.1 54.0 53.7 49.8
Central 106.1 109.1 115.5 51.6 52.5 56.3
Eastern 84.8 93.4 98.2 48.2 52.1 48.0
Greater Accra 89.5 77.4 85.2 54.4 47.9 50.3
Northern 120.9 120.8 127.7 36.8 36.1 26.0
Upper East 92.5 100.1 102.1 59.7 52.6 40.4
Upper West 88.8 88.9 93.5 46.5 36.7 40.6
Volta 81.0 88.9 93.4 36.9 39.4 37.5
Western 109.8 93.5 98.8 49.6 42.6 39.1
National 93.3 92.1 97.8 49.5 45.6 42.2
REGION
POST NATAL CARE FAMILY PLANNING
2010 2009 2008 2010 2009 2008
Ashanti 52.6 38.4 51.6 17.6 17.5 15.7
Brong Ahafo 59.2 53.7 57.2 33.0 43.4 36.3
Central 66.8 71.4 77.6 25.1 33.1 33.0
Eastern 64.5 67.0 61.5 31.5 32.9 33.1
Greater Accra 57.7 51.7 48.7 31.6 32.6 63.9
Northern 88.9 84.9 80.7 21.5 28.9 26.0
Upper East 76.2 77.8 57.3 24.3 33.0 26.2

2010 Annual Report Ghana Health
Service
70
Upper West 68.4 64.9 68.7 49.2 56.5 59.8
Volta 50.1 47.3 50.5 22.5 27.5 21.6
Western 54.4 49.5 45.6 13.0 18.9 19.6
National 61.6 56.4 57.5 24.9 31.1 33.8
Institutional Maternal Mortality Ratio
Region 2010 2009 2008
Maternal
Deaths
Maternal
Mortality
Ratio
Maternal
Deaths
Maternal
Mortality
Ratio
Maternal
Deaths
Maternal
Mortality
Ratio
Ashanti 165 149.6 177 215.1 222 252.6
Brong Ahafo 73 138.7 94 194.4 81 185.3
Central 82 149.0 69 129.4 92 223.2
Eastern 115 191.6 82 135.5 98 170.7
Greater Accra 169 181.5 166 197.1 167 194.3
Northern 84 137.2 96 147.4 91 175.9
Upper East 37 137.9 30 130.9 27 152.2
Upper West 26 157.7 41 266.7 22 120.6
Volta 82 209.6 55 146.0 52 144.7
Western 99 176.1 79 148.2 101 269.5
National 932 163.2 889 169.9 953 199.7

2010 Annual Report Ghana Health
Service
71

2010 Annual Report Ghana Health
Service
72
Trend of OPD attendance per Capita 2001-2010
0.49 0.49 0.50 0.52
0.54 0.55
0.69
0.77 0.81
0.98
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1.1
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
NU
MB
ER
OF
OP
D V
ISIT
S P
ER
CA
PIT
A
TREND IN OPD ATTENDANCE PER CAPITA (Ghana, 2001 - 2010)
Trend of Hospital Admissions(per 1,000pop) 2001-2010
34.9 34.1
36.0 35.3
36.9
33.6
39.3
35.9
43.8
47.9
20
25
30
35
40
45
50
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
NU
MB
ER
(P
ER
10
00
PO
PU
LA
TIO
N)
TREND IN HOSPITAL ADMISSIONS (PER 1,000 POPULATION) 2001-2010

2010 Annual Report Ghana Health
Service
73
DOCTOR POPULATION RATIO (2001-2010)
20,036 18,274
16,759 17,733 17,929
14,732
12,529 12,713 11,929
10,423
-
5,000
10,000
15,000
20,000
25,000
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Doctor Population Ratio, 2001-2010
NURSE POPULATION RATIO (2001-2010)
1,728 1,675 1,649 1,510 1,508 1,537
1,342
1,079 971
1,077
-
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Nurse Population Ratio, 2001-2010

2010 Annual Report Ghana Health
Service
74
6.4
5.5
4.64.4
4.0
0.0
2.0
4.0
6.0
8.0
1988 1993 1998 2003 2008
Total Fertiltity Rate - Ghana1988 - 2008
Trend of Institutiona Maternal Mortality Ratio(2001-2010)
255.7
204.4 204.5 186.0
196.8 187.2
230.2
199.7
169.9 163.2
0.0
50.0
100.0
150.0
200.0
250.0
300.0
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Institutional Maternal Mortality Ratio 2001-2010

2010 Annual Report Ghana Health
Service
75
76.3 78.1
76.0 76.0
83.0 84.2
87.8 86.6
89.3
87.1
60.0
65.0
70.0
75.0
80.0
85.0
90.0
95.0
100.0
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
PE
RC
EN
TA
GE
CO
VE
RA
GE
PENTA 3 COVERAGE 2001 TO 2010
Trend of Supervised Delivery (2001-2010)
49.3 52.6 52.1 53.4
54.2
44.5
32.1
42.2 45.6
49.5
0
10
20
30
40
50
60
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
PE
RC
EN
TA
GE
CO
VE
RA
GE
COVERAGE OF SUPERVISED DELIVERY (2001-2010)
Recommended