
George LAU
Hepatitis B e antigen positive patients:Why do I treat my patient with pegylated
interferon?2nd Hepatitis Paris conference
George KK Lau, M.D.
The University of Hong Kong

What do we want to achieve in treating HBeAg+ CHB patients?
HBeAg seroconversion
Disease remission (↓ HBV DNA; ↓ ALT)
HBsAg loss/seroconversion
Prevention of HCC and cirrhosis
Increased survival
Hoofnagle et al. Ann Intern Med 1981; Fattovich et al. Hepatology 1986; Di Bisceglie et al. Gastroenterology 1987; Niederau et al. NEJM 1996; Chu et al. Gastroenterology 2002; van Zonneveld et al. Hepatology 2004
HBeAg loss
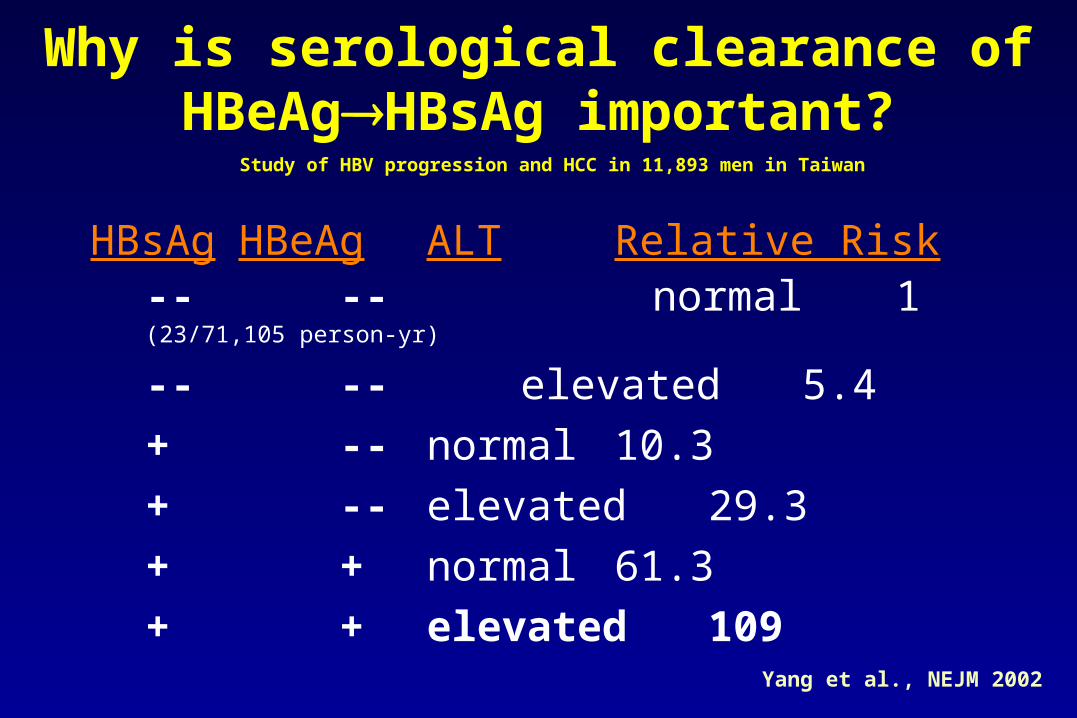
Why is serological clearance of HBeAgHBsAg important?
HBsAg HBeAg ALT Relative Risk-- -- normal 1 (23/71,105 person-yr)
-- -- elevated 5.4
+ -- normal 10.3
+ -- elevated 29.3
+ + normal 61.3
+ + elevated 109
Yang et al., NEJM 2002
Study of HBV progression and HCC in 11,893 men in Taiwan

Registered treatment of chronic hepatitis B-2007
Immune therapy (finite)
Conventional IFN-Pegylated IFN-2a
Anti-viral (life-long)
Lamivudine
Adefovir dipivoxil
Entecavir
LdT
Clevudine (Korea)
Immune control,
no antiviral drugs
Continued need for
antiviral drugs
Aim for sustained remission Suppression of viral replication ? Immune recovery
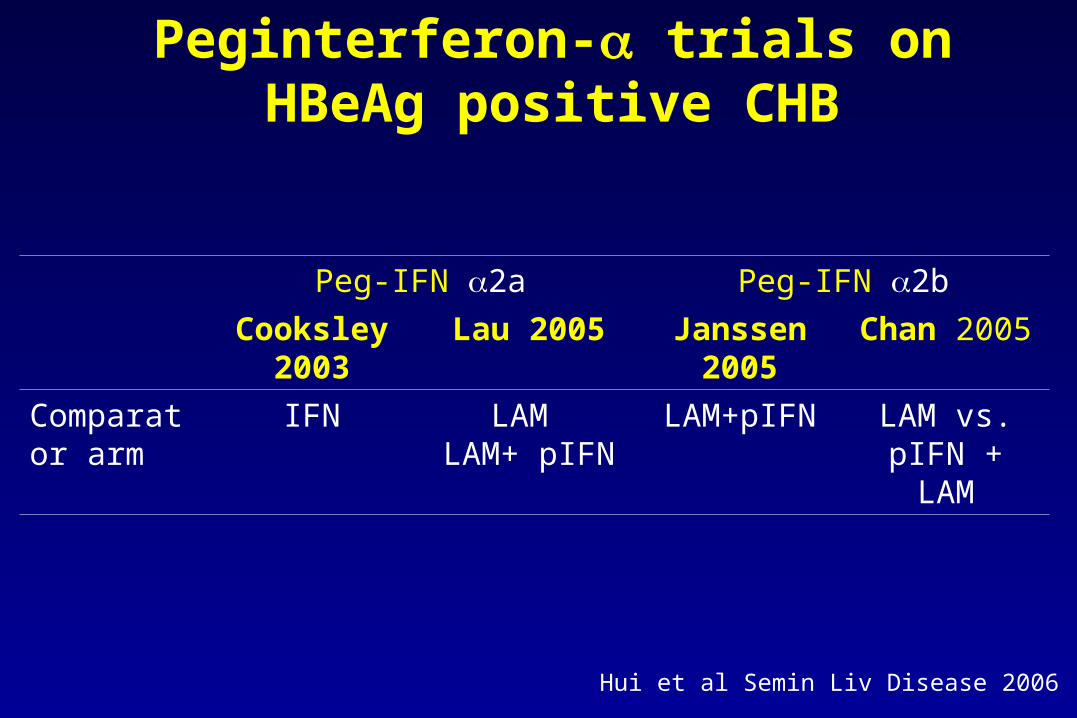
Peg-IFN 2a Peg-IFN 2b
Cooksley 2003 Lau 2005 Janssen 2005 Chan 2005
Comparator arm
IFN LAM LAM+ pIFN
LAM+pIFN LAM vs. pIFN + LAM
Peginterferon- trials on HBeAg positive CHB
Hui et al Semin Liv Disease 2006
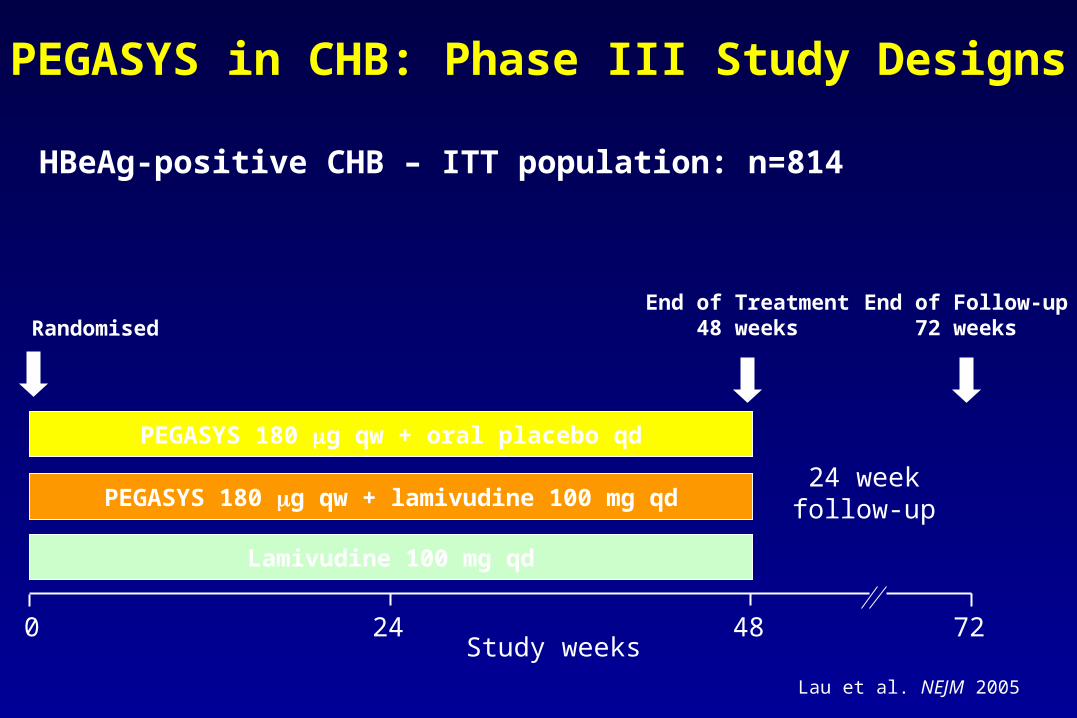
PEGASYS in CHB: Phase III Study Designs
HBeAg-positive CHB – ITT population: n=814
Lamivudine 100 mg qd
PEGASYS 180 g qw + lamivudine 100 mg qd
PEGASYS 180 g qw + oral placebo qd
0 24 48
24 weekfollow-up
72Study weeks
RandomisedEnd of Treatment
48 weeksEnd of Follow-up
72 weeks
Lau et al. NEJM 2005

HBV DNA Levels Over Time plus HBeAg Seroconversion at End of Follow-up
12
*all numbers shown are log10 reduction from baseline
On-treatment Follow-up
Mea
n H
BV
DN
A (
log
10 c
op
ies/
mL
)
2
4
6
8
10
0 6 12 18 24 30 36 42 48 54 60 66 72
-4.5*
-5.8*
-2.0
-7.2*
-2.6
-2.4
32%
27%
19%
P=0.023
P<0.001
HBeAg Seroconversion Rates at End of Follow-up
PEGASYS
n=271 n=271 n=272
PEGASYS+ LAM
LAM
Study week

HBV DNA Suppression in Patients Achieving HBeAg Seroconversion
On-treatment Follow-up
Study week
Mea
n H
BV
DN
A (
log
10 c
op
ies/
mL
)
3.3
0
2
4
6
8
10
12
0 6 12 18 24 30 36 42 48 54 60 66 72
10,000 cp/mL
patients with HBeAg seroconversion maintained DNA levels <10,000 cp/mL
Fried et al. EASL 2005

0
5
10
15
20
1.37
12.17
3.57
14.89
1.30
Incidence of Hepatocellular Carcinoma (HCC) by HBV DNA Level
Chen et al. JAMA 2006
Cu
mu
lati
ve In
cid
enc
e o
f H
CC
(%
)*
≥106104–105<104PCR negative
Level of HBV DNA (cp/mL)
*at the end of the 19th year of follow-up
105–106

21
1820
24
27
22
25
0
5
10
15
20
25
30
354 355 272 271 271 136 130
69% 38% 40% 69% 25% 10% 33%
Chang NEJM 2006 Lau NEJM 2005
(%)
Janssen Lancet 2005
ETV LAM Peg-2a + LAM
LAM Peg-2a Peg-2b + LAM
Peg-2b
No
DNA <400cp/ml
HB
eAg
ser
oco
nve
rsio
n
at e
nd
of
trea
tmen
t (%
)End of Treatment HBeAg seroconversion in Relation to
Extent of HBV DNA Suppression

Serological clearance of HBsAg with current treatment (~1 yr)
% Lam1 ADV2 LdT3 ETV4 Pegasys5
Adoptive immune transfer6
HBeAg 18 12 25* 21 32 -
HBsAg 0 0 0 0 3 65
*HBeAg loss
Spontaneous HBsAg clearance in Chinese-0.1-0.8%/yr
1Lai et al NEJM 1998, 2Marcellin et al NEJM 2003, 3Poynard et al. J Hepatol 2004, 4Chang et al. Hepatology 2004, 5Lau et al. NEJM 2005, 6 Lau et al Gastroenterology 2002
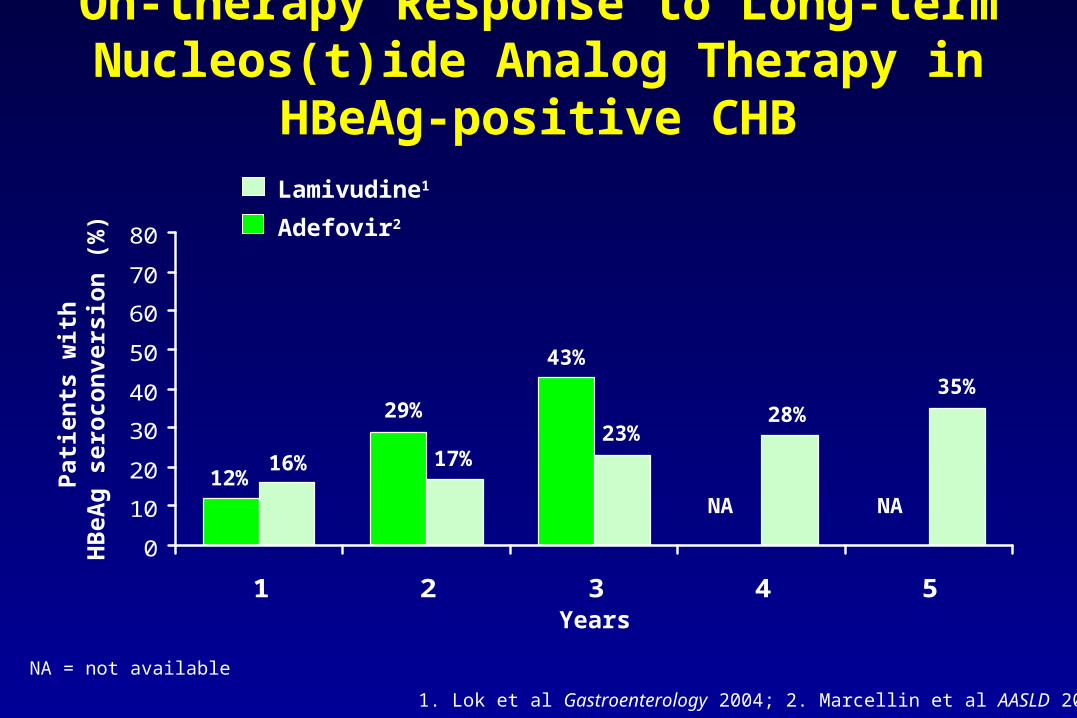
0
10
20
30
40
50
60
70
80
1 2 3 4 5
Pat
ien
ts w
ith
H
BeA
g s
ero
con
vers
ion
(%
)
Lamivudine1
1. Lok et al Gastroenterology 2004; 2. Marcellin et al AASLD 2004
Adefovir2
Years
16% 17%23%
28%35%
12%NA NA
NA = not available
On-therapy Response to Long-term Nucleos(t)ide Analog Therapy in HBeAg-positive CHB
29%
43%
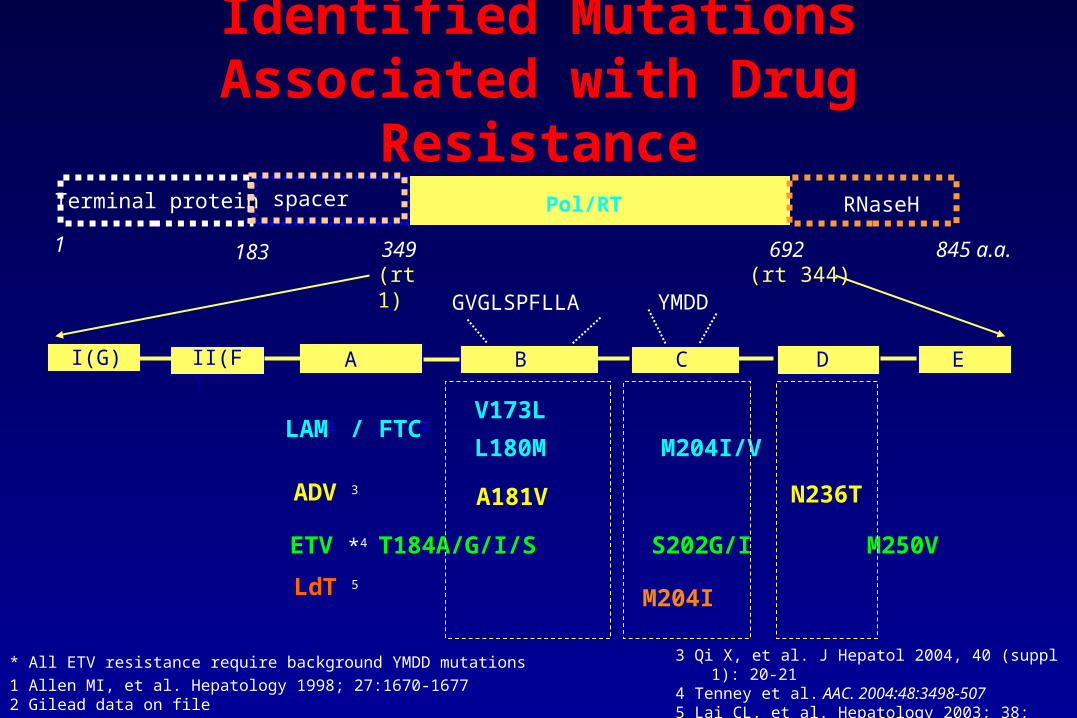
845 a.a.
Terminal protein Pol/RT RNaseH
A B C ED
1 183 349 692
YMDD
V173L
L180M M204I/V
GVGLSPFLLA
I(G) II(F)
(rt1) (rt 344)
Identified Mutations Associated with Drug Resistance
LAM1 / FTC2
ETV *4 T184A/G/I/S S202G/I M250V
ADV 3 A181V N236T
LdT 5
M204I
* All ETV resistance require background YMDD mutations
1 Allen MI, et al. Hepatology 1998; 27:1670-16772 Gilead data on file
3 Qi X, et al. J Hepatol 2004, 40 (suppl 1): 20-214 Tenney et al. AAC. 2004:48:3498-5075 Lai CL, et al. Hepatology 2003; 38: 262A6 Soriano V et al, AASLD 2004
spacer
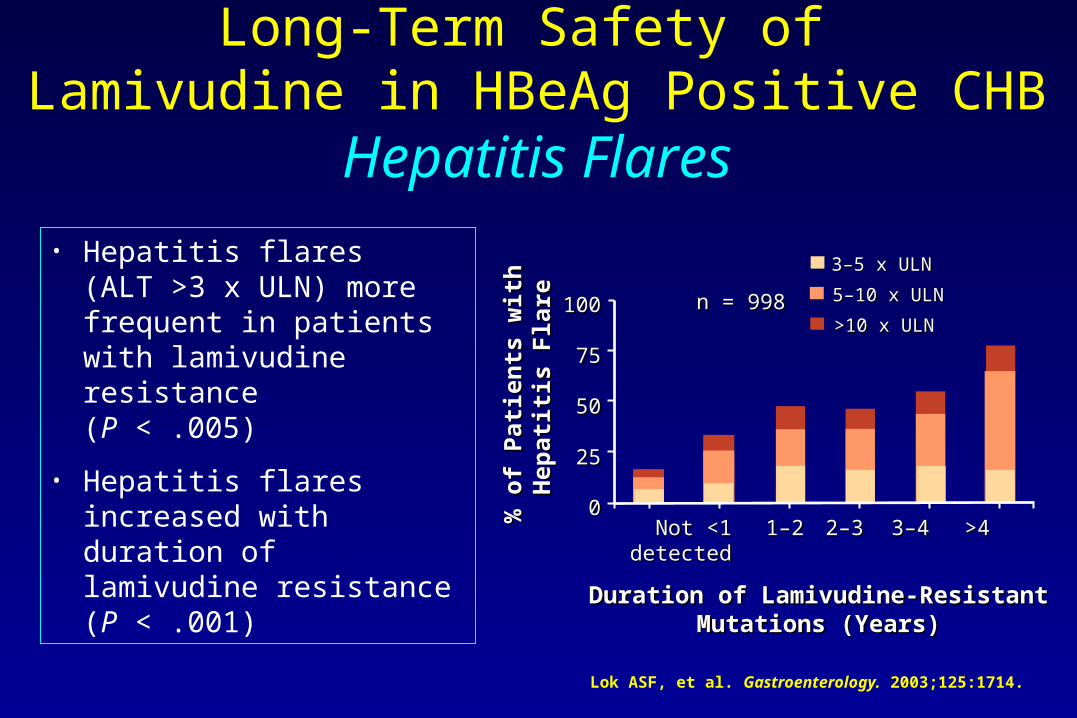
Duration of Lamivudine-ResistantDuration of Lamivudine-ResistantMutations (Years)Mutations (Years)
% o
f P
atie
nts
wit
h
% o
f P
atie
nts
wit
h
Hep
atit
is F
lare
Hep
atit
is F
lare
100100
7575
5050
2525
00 Not Not <1 <1 1–2 1–2 2–3 2–3 3–4 3–4 >4>4
detecteddetected
3–5 x ULN3–5 x ULN
n = 998n = 998
Long-Term Safety of Lamivudine in HBeAg Positive CHB
Hepatitis Flares
• Hepatitis flares(ALT >3 x ULN) more frequent in patients with lamivudine resistance (P < .005)
• Hepatitis flares increased with duration of lamivudine resistance (P < .001)
5–10 x ULN 5–10 x ULN
>10 x ULN>10 x ULN
Lok ASF, et al. Gastroenterology. 2003;125:1714.

HBeAg Relapse Following Lamivudine and IFN
Cu
mu
lati
ve %
rel
apse
of
HB
eAg
sero
con
vers
ion
0 26 52 78 104 130 156
10
20
30
40
50
60
70
80
90
100
Time (weeks) after the end of therapy
LAM
IFN
van Nunen et al. Gut 2003
Cumulative rate of relapse in patients who had achieved HBeAg seroconversion by end of treatment
54%
32%
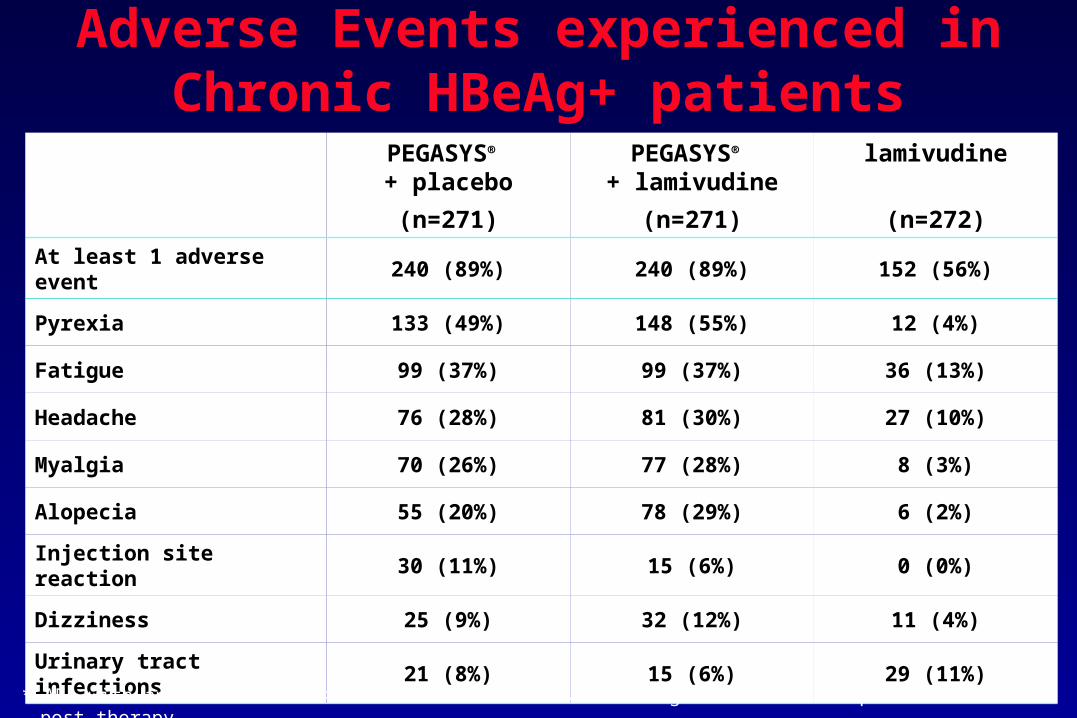
Adverse Events experienced in Chronic HBeAg+ patients
PEGASYS® + placebo
(n=271)
PEGASYS® + lamivudine
(n=271)
lamivudine
(n=272)
At least 1 adverse event 240 (89%) 240 (89%) 152 (56%)
Pyrexia 133 (49%) 148 (55%) 12 (4%)
Fatigue 99 (37%) 99 (37%) 36 (13%)
Headache 76 (28%) 81 (30%) 27 (10%)
Myalgia 70 (26%) 77 (28%) 8 (3%)
Alopecia 55 (20%) 78 (29%) 6 (2%)
Injection site reaction 30 (11%) 15 (6%) 0 (0%)
Dizziness 25 (9%) 32 (12%) 11 (4%)
Urinary tract infections 21 (8%) 15 (6%) 29 (11%)
* AEs with an incidence of >10% in one treatment arm during treatment and up to 8 weeks post-therapy
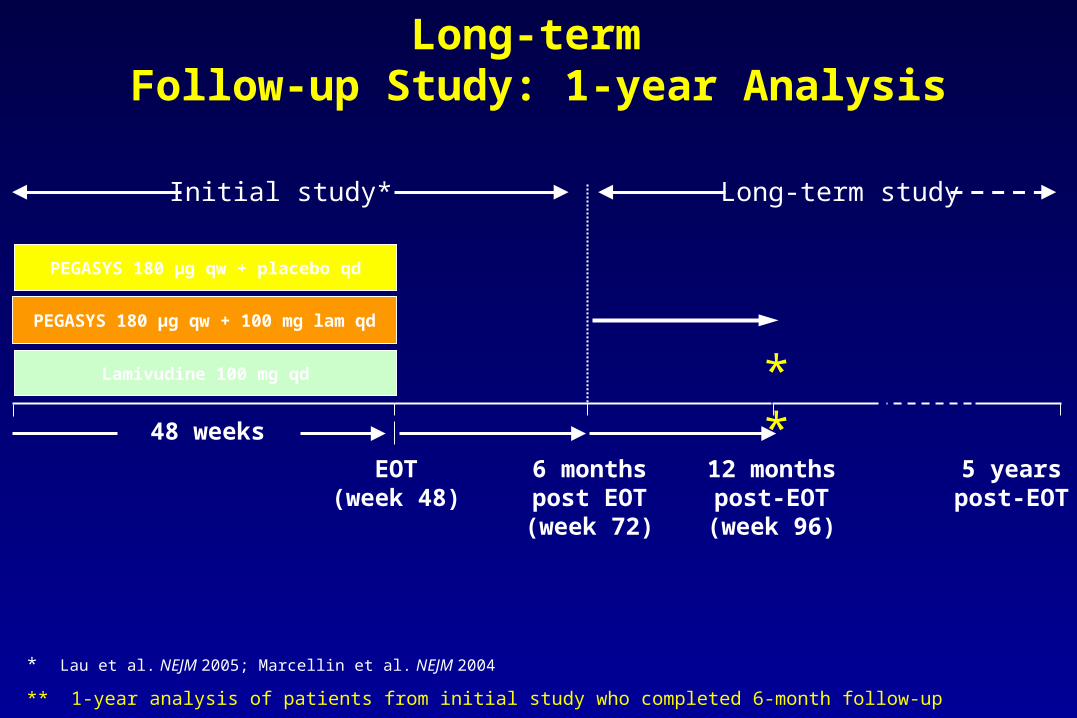
Long-term Follow-up Study: 1-year Analysis
* Lau et al. NEJM 2005; Marcellin et al. NEJM 2004
** 1-year analysis of patients from initial study who completed 6-month follow-up
Lamivudine 100 mg qd
PEGASYS 180 μg qw + 100 mg lam qd
PEGASYS 180 μg qw + placebo qd
48 weeks
12 monthspost-EOT(week 96)
5 yearspost-EOT
**
Initial study*
EOT(week 48)
6 monthspost EOT(week 72)
Long-term study
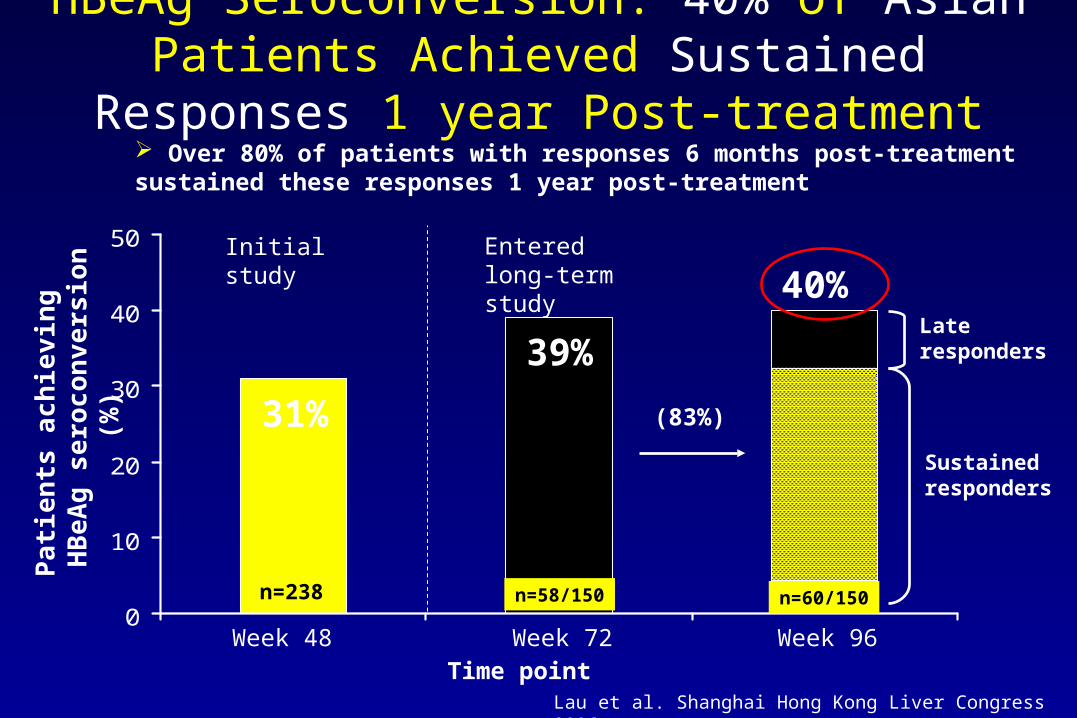
0
10
20
30
40
50
40%
39%
HBeAg Seroconversion: 40% of Asian Patients Achieved Sustained Responses 1 year Post-treatment
31%
Pa
tie
nts
ac
hie
vin
g
HB
eA
g s
ero
co
nve
rsio
n (
%)
n=238 n=58/150 n=60/150
Week 48 Week 72 Week 96Time point
Lau et al. Shanghai Hong Kong Liver Congress 2006
Initial study Entered long-term study
Over 80% of patients with responses 6 months post-treatment sustained these responses 1 year post-treatment
(83%)
Late responders
Sustained responders
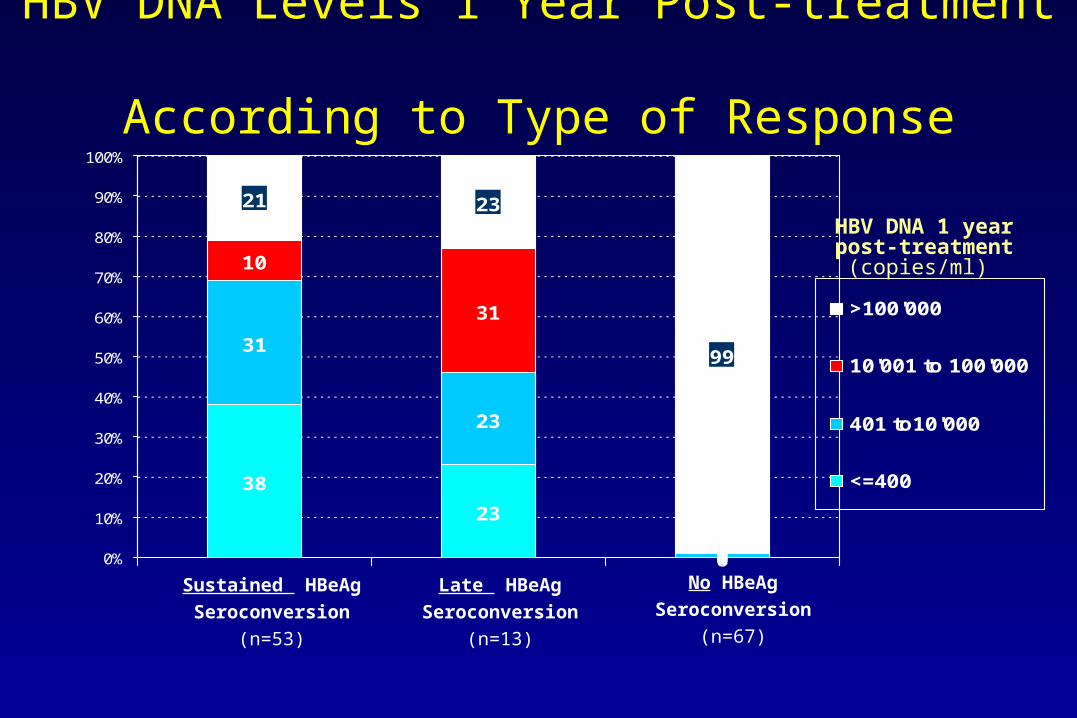
38
23
0
31
23
1
10
31
0
21 23
99
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
>100'000
10'001 to 100'000
401 to10'000
<=400
No HBeAg
Seroconversion
(n=67)
HBV DNA Levels 1 Year Post-treatment According to Type of Response
HBV DNA 1 year post-treatment
(copies/ml)
Sustained HBeAg
Seroconversion
(n=53)
Late HBeAg
Seroconversion
(n=13)
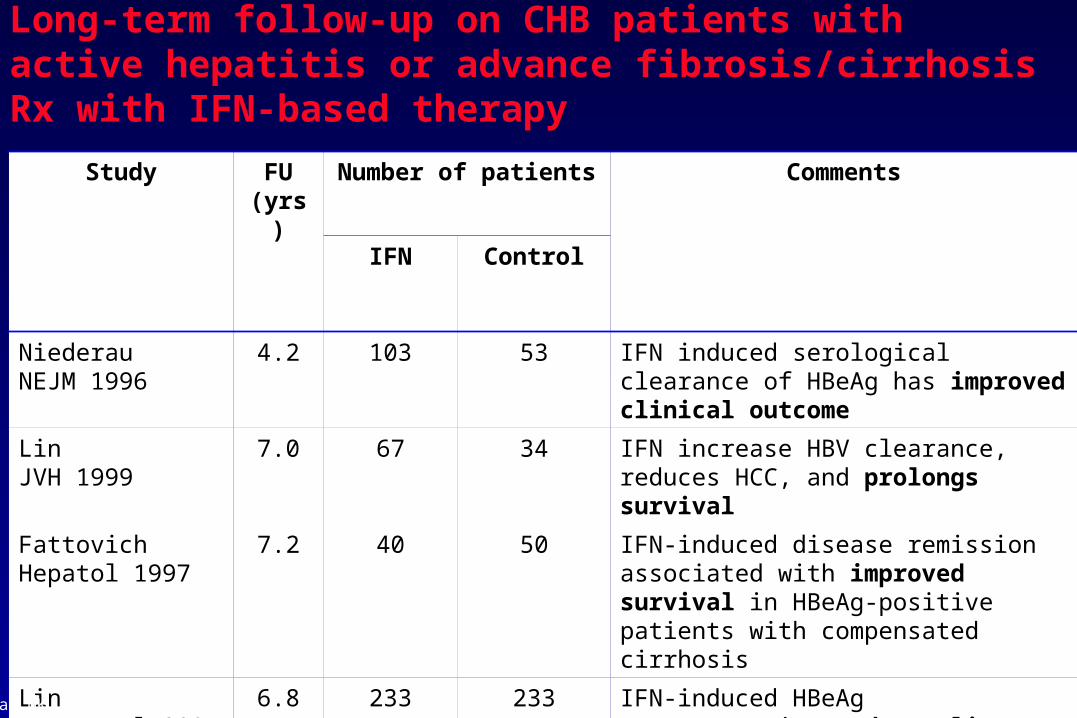
Study FU (yrs)
Number of patients Comments
IFN Control
Niederau NEJM 1996
4.2 103 53 IFN induced serological clearance of HBeAg has improved clinical outcome
Lin JVH 1999
7.0 67 34 IFN increase HBV clearance, reduces HCC, and prolongs survival
Fattovich Hepatol 1997
7.2 40 50 IFN-induced disease remission associated with improved survival in HBeAg-positive patients with compensated cirrhosis
Lin J Hepatol 2007
6.8 233 233 IFN-induced HBeAg seroconversion reduces liver cirrhosis and cancer
Long-term follow-up on CHB patients with active hepatitis or advance fibrosis/cirrhosis Rx with IFN-based therapy
Lau GK. J Hepatol 2007
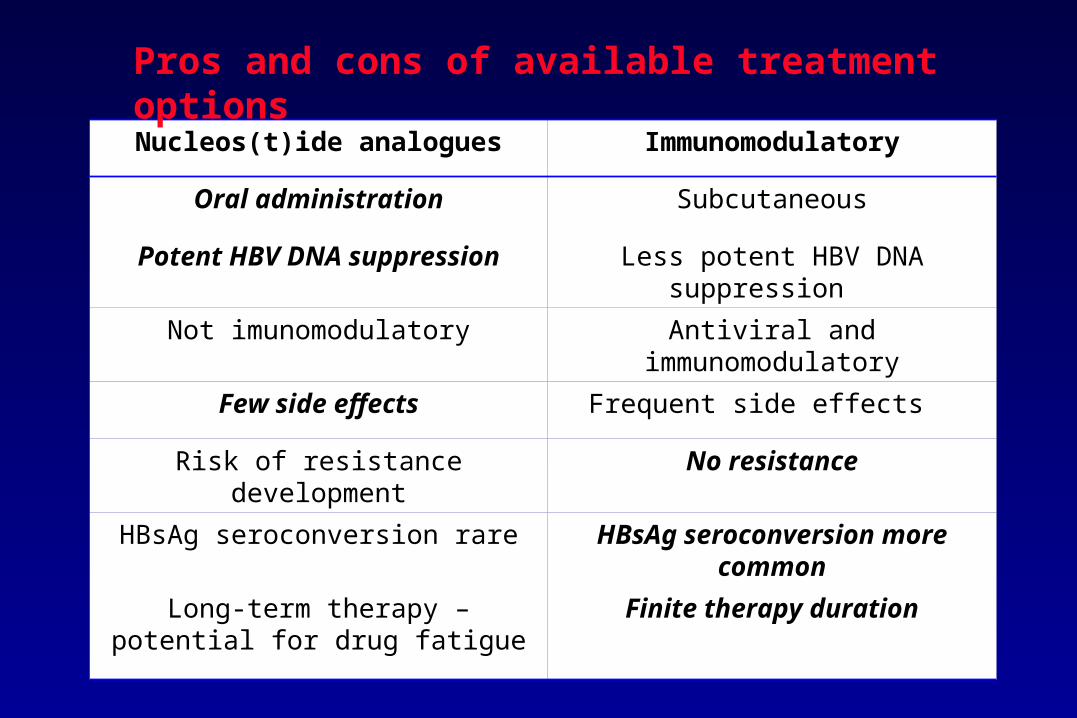
Nucleos(t)ide analogues Immunomodulatory
Oral administration Subcutaneous
Potent HBV DNA suppression Less potent HBV DNA suppression
Not imunomodulatory Antiviral and immunomodulatory
Few side effects Frequent side effects
Risk of resistance development No resistance
HBsAg seroconversion rare HBsAg seroconversion more common
Long-term therapy – potential for drug fatigue
Finite therapy duration
Pros and cons of available treatment options
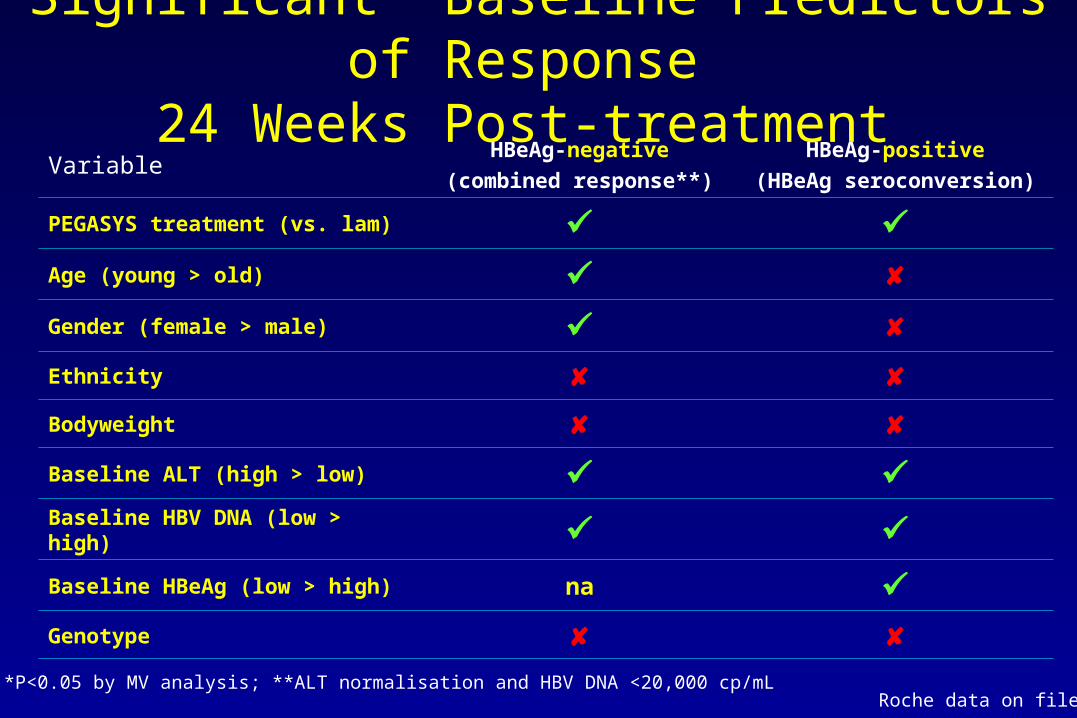
Significant* Baseline Predictors of Response 24 Weeks Post-treatment
VariableHBeAg-negative
(combined response**)
HBeAg-positive
(HBeAg seroconversion)
PEGASYS treatment (vs. lam) Age (young > old) Gender (female > male) Ethnicity Bodyweight Baseline ALT (high > low) Baseline HBV DNA (low > high) Baseline HBeAg (low > high) na Genotype
*P<0.05 by MV analysis; **ALT normalisation and HBV DNA <20,000 cp/mL Roche data on file

HBsAg-seroconversion by Genotype
1 Flink, Am J Gastroenterol 2006; 2 Hadziyannis, EASL 2005
PEG-IFN α-2b 1
0
3
6
9
12
15
A n=47
5%
8%
0%
Bn=12
C n=21
D n=51
1815%
Per
cen
tag
e o
f p
atie
nts
(%
) 21
24
HBV genotype
PEG-IFN α-2a 2
22%
0
3
6
9
12
15
A n=23
2%0% 0%
Bn=76
C n=162
D n=9
18
Per
cen
tag
e o
f p
atie
nts
(%
) 21
24
HBV genotype
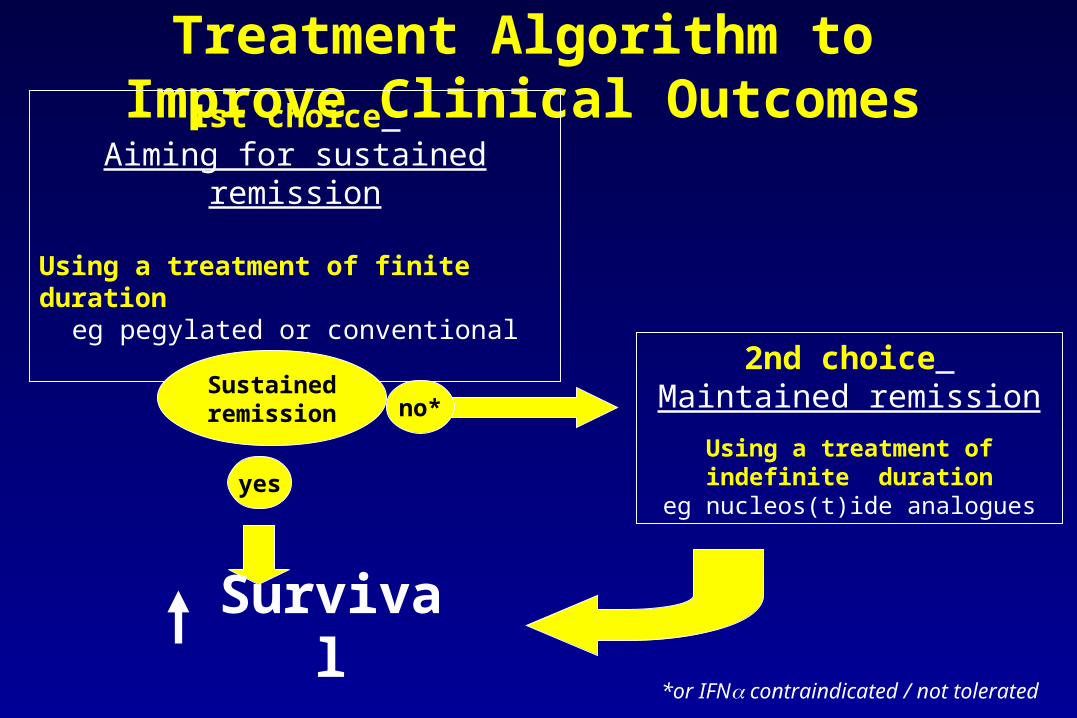
Treatment Algorithm to Improve Clinical Outcomes
1st choice Aiming for sustained remission
Using a treatment of finite durationeg pegylated or conventional IFN
Sustainedremission
yes
no*
2nd choice Maintained remission
Using a treatment of indefinite duration
eg nucleos(t)ide analogues
*or IFN contraindicated / not tolerated
Survival
Recommended

















