GCIG Virtual Spring Meeting 2020
Some rules for the videoconference• Please keep yourself muted• Please, do not over-run your time• Please, do not speak at the same time• Questions must be submitted via the chat function• After each new concept questions will be addressed• For all other presentations questions will be taken at
the end of each session• After the presentation of new ideas, interested
groups should send an email to the presenter

Template
ENDOMETRIAL CANCER COMMITTEE TUESDAY, JUNE 2, 2020
Chair: Stefano Greggi Co-Chair: Carien Creutzberg Harmonization Liaisons: Karen Verhoeven (Ops); Dongsheng Tu/Andrew Embleton (Stats)
AGENDA
Welcome and Introductions: S. Greggi COI Disclosures: Approval of Report: November 2019 (posted on GCIG website) Motion: __________________________ Seconded: _____________________________ NEW PROPOSALS/CONCEPTS: BGOG: ENGOT-EN11/KEYNOTE-B21 (Toon v Gorp) ANZGOG: EN3 (Andreas Obermair) UDATE OF TRIALS IN DEVELOPMENT: CCTG: DOMINO (Stephen Welch) DGOG/GINECO/NCRI: RAINBO (Carien Creutzberg / Judith Kroep) NCI/ANZGOG: Phase III study of carboplatin/paclitaxel alone or combined with either trastuzumab or trastuzumab/pertuzumab in HER2 overexpressing EC (Matthew Powell) ONGOING TRIALS (maximum of 5 minutes each): NCI: NRG-GY-020. A phase III random. trial of RADIATION +/- MK-3475 (Pembrolizumab) FOR newly diagnosed EARLY Stage MSI+ EC (Matthew Powell) NCI: NRG-GY-018. (Matthew Powell) BGOG: ENGOT-EN5/SIENDO (Ignace Vergote) NSGO: ENGOT-EN6-NSGO/RUBY (Mansoor Mirza) AGO: AGO-OP.6 / ECLAT (Philipp Harter) MITO: ECCO, AEC (Stefano Greggi) COGI: SAVE (David Gaffney) DGOG: PORTEC-4a (Carien Creutzberg) MANGO: AtTEnd (Nicoletta Colombo) CLOSED/PUBLISHED STUDIES: S. Greggi
Discussion/Future Directions: Experience with COVID situation in Italy and consequences for trials – Stephano Greggi ADJOURN

EN Committee, May 2020
New proposals

ENDO-3A Phase III Randomised Clinical Trial Comparing Sentinel
Node Biopsy with No Retroperitoneal Node Dissection in
Apparent Early-Stage Endometrial Cancer
A Obermair, ANZGOG

Background
Is there value to patients of SLND for the surgical treatment of Endometrial Cancer (EC)?
Practice management guidelines of EC mandate surgical assessment of lymph nodes.
Research has been focussed on technique and accuracy of SLND (“Can it replace LND for staging?”).
Patient benefit of SLND has been argued (e.g., selection of treatment, survival) but is yet to be demonstrated.
Potential of patient detriment: In FIRES 12% of patients had positive LNs but 19 of 36 patients with positive LNs had (very-) low volume involvement.
ASTEC and Italian LND trials
No benefit of DFS or OS
Incidence of adverse events 3.5 times higher for LND
ASTEC trial
Italian trial

Trial design

Trial design
Phase 3 RCT to provide definitive evidence on value of SLND
Participants receive TH BSO with SNB
Participants receive TH BSO without retroperitoneal node dissection
Primary outcome is DFS at 4.5 years
Secondary outcomes: PROMS/QoL; perioperative outcomes; adverse events; lymphoedema, adjuvant treatment; cost/cost effectiveness; molecular.
Stage 1 – 444 participants using 1:1 randomisation
Stage 2 – Further 316 participants using 1:1 randomisation
Stratification by histological cell type (endometriodvs other), treatment centre, surgical approach (lap vs robot), BMI (<30, 30-45, >45) and age.
Adjuvant treatment: Based on uterine factors and ESMO risk stratification • Positive LN will be offered chemotherapy• ITC shall not be offered chemo• Micrometastasis (<0.2 mm) clinician’s discretion

Power Calculations
Primary Outcome Measure is DFS at 4.5 years
Estimated 4.5-yr DFS rate in the control group is 90%
A non-inferiority (NI) margin of 5% at 4.5 years would be clinically worthwhile in trading off the extra morbidity associated with SLND.
A sample size of 721 participants would have 80% power with 97.5% (one-sided) confidence to detect a 5% difference at 4.5 years assuming a 4-year accrual and minimum of 4-year follow-up time.
Allowing for a modest 5% loss to follow-up, the total sample size for the study would be 760 participants. This sample size will also have >90% power to detect a NI margin of at most 6% at 4.5 years.

Quality assurance
Surgeon accreditation
Provide evidence of 30 cases
Competency Assessment Tool (CAT) developed though 4-round Delphi process)
Surgeons need to perform SLND at least twice a month
SLN detected in at last 7 of the most recent 10 cases
Continuously, all SLND cases will be video-recorded and randomly assessed (CAT)
Independent Data Safety Management Committee
Recurrence adjudication committee

EN Committee, May 2020
Trials under development – status update

Resected stage III endometrioid endometrial cancerLND mandatory**Local d-MMR
Chemoradiotherapy*
RANDOMIZE
Stratify by:• ECOG PS• CRT regimen
*Chemoradiotherapy = Investigators’ choice (“sandwich” vs PORTEC3)**Sentinel LND allowed
CCTG Proposal: Durvalumab as part of Post-Operative Therapy for MIsmatch
Repair-deficient eNdOmetrial cancer(DOMINO)
1:1
Sample size =170 pts
Observation
Durvalumab1500 mg IV Q4W(max 12 months)
NED on CT
Contact: [email protected]

RAINBO umbrella program
Refining Adjuvant treatment IN endometrial cancer Based On molecular profile (RAINBO)
a TransPORTEC collaboration and initiativeDGOG, GINECO, NCRI, CCTG, ANZGOG
Carien Creutzberg and Judith Kroep for TransPORTEC Consortium

Vermij et al; Histopathology 2020
MMR proficientMMR deficient
p53 normal p53 abnormal
POLE pathogenic POLE wildtype or non-pathogenic POLE variant
EEC, NOSSEC, NOSCCC, NOSDEC, NOS
POLEmut EC MMRd EC NSMP EC p53mut EC
Endometrial CancerEndometrioid, Serous, Clear Cell, Dediff EC
Molecular testing notperformed OR inconclusive
Surrogate Marker Tests:
1. POLE sequencing
2. MMR-IHC
3. p53-IHC
Paradigm Shift in Endometrial Cancer Classification

PORTEC-3Molecular analysis successful in 97% of
samples
Molecular classification prognostic
PORTEC-3 HR-EC trial cohort N=410
32% NSMP
33% MMRd13% POLE
22% p53
Stelloo et al, Clinical Cancer Research 2016; Leon-Castillo et al, ESMO 2019; **Leon-Castillo et al, J Pathol 2020
Double classifiers reclassified**
N=410 (PORTEC-3)
POLE
NSMP
p53abn
MMRd

p=0.015, HR 0.50 (95%CI 0,28-0,88)
Creutzberg, Leon-Castillo et al, ESMO 2019 and Leon-Castillo et al, ESGO 2019
PORTEC-3
Molecular classification predictive of differential benefit from adj Ctx
p53abnPOLEmut MMRd NSMP
• P53abn: worst prognosis but greatest benefit from adj Ctx• POLEmut: does not relapse regardless of tx• MSI and NSMP: intermediate prognosis , but little benefit from Adj Ctx
No adj tx needed? Adj IO rather thanCtx?PARP as
maintenance?

• International program of personalized, molecular based, adjuvant treatment of pts with HREC to increase 5-yr RFS with less toxicity
• Patients will be centrally registered and after molecular classification be recruited into the international program and be allocated to one of the four subtrials: p53abn, MMRd, NSMP and POLEmut.
• Groups involved: DGOG, GINECO, NCRI, CCTG/PMH, ANZGOG
• Groups interested: ENGOT, EORTC, SAKK, CEEGOG, ….?
RAINBO: Refining Adjuvant treatment INendometrial cancer Based On molecular features

RAINBO: Refining Adjuvant treatment INendometrial cancer Based On molecular features
RAINBOSteering Committee*
RAINBOAdvisory Committee*
transPORTEC RAINBO Consortium
PI: Dr. A. LearyGINECO
PI: Dr. J. KroepDGOG
PI: Dr. M. PowellNCRI
PI: Dr. H. Mackay / K. HanCCTG/PMH
RAINBO PIs
RAINBOTranslational Research
Committee*
*RAINBO committees will include international experts on endometrial cancer management, oncologists, radiation oncologists, pathologists, statisticians and patient advocacy

Resected ECAll histologic subtypes
MolecularClassification
RAINBO umbrella program supported by GCIG and coordinated by TransPORTEC will allocate EC pts to 4 international academic sub-trials each led by one Gyn-Onc national clinical trial group
RCT/RT → PARPinhib
CT/RT
R
RT → aPD1
RT (RTCT for stage III allowed)
No Adj Tx
RRT → Hormonal Tx
CT/RT
RAINBO umbrella Program
N = 485GINECO
N = 300DGOG
N = 698NCRI
N = 100CCTG/PMH
Primary endpoint 5-yr RFS

RAINBO – protocol design and funding
RCT/RT → PARPinhib
CT/RT
R
RT → aPD1
RT (RTCT for stage III allowed)
No Adj Tx
RRT → Hormonal Tx
CT/RT
N = 485GINECO
N = 300DGOG
N = 698NCRI
N = 100CCTG/PMH
Protocol development ongoingAcademic trialsPharma support likelyCombined with DCS grant applicationCancer Research UK grant application
TAPER de-escalation trial

TAPER trial POLE (and p53wt) Trial – single arm
Inclusion criteriaEndometrial endometrioid adenocarinoma
Stages IA G3, IB, II (microscopic)POLEmut & p53wt EC
No adjuvant treatment for POLEmutDe-escalation of RT for p53wt
PI team : Canada – Han/McAlpine//Fyles/Mackay/WelchAim: Confirm safety of no additional or de-escalated treatment in POLEmut & p53wt ECPrevalence: POLEmut ~5-10% of EC; p53wt ~50%Single arm prospective phase II trial – assumption 3-year pelvic relapse < 4% - stopping rule when ≥ 4% relapse (2-stage design)
N= 276
Follow-up
Exclusion criteriaNon-pathogenic POLEmutMMRd, p53 abn

NRG UC1972HER2+ Serous Carcinomas
Trial setting: HER2 positive stage I-IV uterine serous carcinoma and
carcinosarcoma after primary surgery
Study Design: 3 Arm Randomized phase III trial carboplatin/paclitaxel
alone or combined with either trastuzumab or
trastuzumab/pertuzumab ;
Endpoints: primary: PFS Secondary: OS, RR, safety / tolerability
Sponsor(s): NCI
Planned No. of patients: 347
Current accrual: 0
Other important: Study design and inclusion in development
Proposed Trials – status update

NRG UC1972BACKGROUND- Breast/Gastric
• 15% of breast cancer HER2+ & US FDA approved Trastuzumab (T) in 1998
• HERA trial enrolled over 5,000 women early stage: One year of maintenance
DFS(HR 0.76, 95% CI 0.68-0.86) and death (0.74, 0.64-0.86). 10 year survival
improvement from 63% to 69%; two years maintenance did not improve
• Meta-analysis 1,400 patients with HER2-positive metastatic breast cancer, the
addition of T improved OS (HR 0.82, 95% CI 0.71-0.94) (Balduzzi 2014).
• Gastric cancer: ORR 35% to 47% and OS significantly improved with T (13.8
versus 11.1 months, HR 0.74, 95% CI 0.60-0.91).
• Pertuzumab (P) binds dimerization domain, inhibiting HER2 to other HER family
receptors (heterodimerization). Approved in MBC and EBC with APHINITY trial
n=4,804 HER2-positive early breast cancer: T+chemo +-T. DFS 7.1% with P and
8.7% in the placebo group (HR 0.82, P = .047).
Proposed Trials – status update

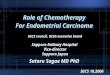
NRG UC1972BACKGROUND- RP2 trail
• RP2 Fader et al: randomized 61 patients 1:1 to receive carboplatin/paclitaxel
for 6 cycles ± trastuzumab followed by maintenance trastuzumab until
progression or toxicity.
• Benefit appeared to be primarily in the newly diagnosed patients (Stage III/IV)
PFS (9.0 versus 14.8 months, HR 0.393, 90% CI 0.203-0.758, p=0.0078)
OS (21.1 versus 31.9 months, HR 0.440 90% CI 0.219-0.882 p=0.0230)
Proposed Trials – status update
17 4 3 3 3 3 2 0
19 14 7 5 4 2 0
0 12 24 36 48 60 72 84
Months since on-treatment date
0.0
0.2
0.4
0.6
0.8
1.0
Pro
port
ion p
rogre
ssio
n-fre
e
NoYes
YesNoTrastuzumab
PFS vs Trastuzumab, Advanced (IIIC or IV)With Number of Subjects at Risk
17 4 3 3 3 3 2 0
19 14 7 5 4 2 0
0 12 24 36 48 60 72 84
Months since on-treatment date
0.0
0.2
0.4
0.6
0.8
1.0
Pro
port
ion p
rogre
ssio
n-fre
e
NoYes
YesNoTrastuzumab
● Censored
PFS vs Trastuzumab, Advanced (IIIC or IV)With Number of Subjects at Risk
17 13 8 3 3 3 2 0
19 19 14 7 6 4 0
0 12 24 36 48 60 72 84
Months from on-treatment date
0.0
0.2
0.4
0.6
0.8
1.0
Pro
port
ion A
live
NoYes
YesNoTrastuzumab
Overall Survival vs Trastuzumab, Advanced (IIIC or IV)With Number of Subjects at Risk
17 13 8 3 3 3 2 0
19 19 14 7 6 4 0
0 12 24 36 48 60 72 84
Months from on-treatment date
0.0
0.2
0.4
0.6
0.8
1.0
Pro
port
ion A
live
NoYes
YesNoTrastuzumab
● Censored
Overall Survival vs Trastuzumab, Advanced (IIIC or IV)With Number of Subjects at Risk

NRG UC1972BACKGROUND
Inclusion of Carcinosarcomas (UCS)?
• UCS frequently contains serous components and in a recent TCGA study, 78%
of the samples were considered “serous like” based on molecular analysis
(Cherniack et al). Serous histology drives outcome (Gotoh, Nature, 2019)
• UCS overexpress HER2: 13 of 80 patients (16%) were HER2 positive based on
IHC or FISH testing. All 13 of the positive cases had either serous or mixed
carcinoma component (Rottman et al, 2020).
• Targeting HER2 in vitro and in vivo had been demonstrated in UCS models, with
strong anti-tumor effects (Menderes et al).
• Carboplatin and paclitaxel is now considered the standard of care for all stage
of UCS (GOG 0261;Powell et al, ASCO 2019).
Proposed Trials – status update

NRG UC1972BACKGROUND
Inclusion of Early Stage?
• Treatment is controversial; Portec3 suggest ChemoRT; GOG258: serous I/II +cytology
• Her2 appears to be an important predictive biomarker for early stage serous patients:
• Erickson et (ASCO 2020): n=169; 44 (26%) were HER2+ and 125 (74%)HER2- neg
• Despite chemotherapy: 43 patients (25.4%) experienced relapse and HER+ tumors
were more likely to recur (50% vs 16.8%, p<0.001)
• Multivariate analysis, HER2+ was a strong independent risk factor for recurrence (aHR
3.50, 95% CI 1.84 – 6.67, p <0.001) and OS (aHR 2.00, 95% CI 1.04 – 3.88, p = 0.039)
Proposed Trials – status update

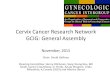
• All patients must have tumors that are HER2 positive as defined by ASCO/CAP 2018 guidelines (3+ IHC, 2+ IHC with positive FISH, or FISH positive) – Centralized pre-testing versus local testing with conformation??
• Sample size: PFS
• Concern about accrual
Given wide spread us of T in
USA for advanced staged
115 patients per arm:
-10/mo accrual time 35 mo
NRG UC1972BACKGROUND
Other considerations…
Proposed Trials – status update
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44
Prop
ortio
n Al
ive
With
out P
rogr
essio
n
Months from Randomization
Estimated PFS Distributions in the Reference Arm
Overall Early Stage Advanced Stage
Early Stage
OVERALL
Advanced Stage

EN Committee, May 2020
Ongoing Trials – status update

NRG GY-018
Trial setting: Measurable Stage III or IVA, Stage IVB or Recurrent
Endometrial Cancer
Study Design: A Phase III Randomized, Placebo-Controlled Study
Paclitaxel and Carboplatin +- Pembrolizumab to progression or 2 years
Sponsor(s): NCI (A)
Planned No. of patients: N: 590 pMMR; 220 dMMR = 810
Current accrual: 94
Other important: Centralized MMR/MSI testing.
Ongoing Trials – status update

NRG GY-018
Ongoing Trials – status update

NRG GY-020
Trial setting: High intermediate risk mismatch repair deficient (dMMR)
endometrioid endometrial cancer
Study Design: Randomized phase III trial of radiation +/-
pembrolizumab
Primary outcome: 3-year RFS
Sponsor(s): NCI (A)
Planned No. of patients: N: 168 (2:1 randomization)
Current accrual: 4
Other important: Considering addition of non-measurable stage III
patients.
Ongoing Trials – status update
PENDING:

NRG GY-020
- Arm 1: vaginal brachytherapy or pelvic radiation- Arm 2: vaginal brachytherapy or pelvic radiation with MK-3475
(pembrolizumab) every 3 weeks x 1 year (**Proposed amendment proposed to change to 400mg q 6 weeks)
- All patients will receive standard vaginal brachytherapy
- For patients with Stage IB grade 3 (≥ 50% myometrial invasion and grade 3) or Stage II, the treating physician may choose to prescribe pelvic external beam radiation (EBRT). This must be decided prior to randomization. All other patients will receive vaginal brachytherapy only
Ongoing Trials – status update
PENDING:

NRG GY-020
• Stage I endometrioid endometrial cancer and a combination of age and risk factors:
- Age >70 and ≥1 risk factor- Age 50-70 and 2 risks factors- Age <50 and 3 risk factorsRisk factors: - Myometrial invasion ≥ 50%
- Lymphovascular space invasion- Grade 2 or 3
• Stage II endometrioid endometrial cancer • Patients with isolated tumor cells in sentinel lymph nodes are
eligible (considered N0i) as long as there is no evidence of micro-or macro-metastases in any lymph nodes.
Ongoing Trials – status update
PENDING:
Key Eligibility Criteria

ENGOT-EN6 /NSGO - RUBY
Eligible SubjectsRecurrent or PrimaryAdvanced (stage III or IV) Endometrial Cancer or first recurrent endometrial cancer with a low potential for cure by radiotherapy or surgery alone or in combination
N = 470Randomization 1:1
Dostarlimab 500 mgCarboplatin AUC5mg/mL/minPaclitaxal 175 mg/m2
Q3W for 6 cycles
Dostarlimab 1.000 mgQ6W up to 3 years*
Follow-up
Stratification:
By microsatellite instability (MSI) status (MSI-high [MSI-H] or microsatellite stable [MSS]), prior external pelvic radiotherapy (yes or no), and disease status (recurrent, primary Stage III, or primaryStage IV).
PlaceboCarboplatin AUC5mg/mL/minPaclitaxal 175 mg/m2
Q3W for 6 cycles
PlaceboQ6W up to 3 years*
*Treatment ends after 3 years, progression of disease, toxicity, withdrawal of consent, Investigator’s decision, or death, whichever occurs first. Continued treatment with dostarlimab or placebo beyond 3 years may be considered following discussion between the Sponsor and the Investigator.
Principal Investigator: Mirza
Sponsor: Tesaro-GSK
Lead Group: NSGO

ECLAT - Endometrial Cancer
Lymphadenectomy Trial
AGO-OP.6
For further information, please contact: Philipp Harter ([email protected])
R
System. lymphadenectomy
⚫ pelvic
⚫ para-aortic
No lymphadenectomy
• histologically confirmed
endometrial cancer
• FIGO IB or FIGO II
(all subtypes)
• FIGO IA, G3 (Type I)
• FIGO IA (Type II)
• Absence of bulky nodes
• Age 18 - 75y
n=640
SLN in LNE arm as additional procedure allowed
Primary endpoint:
Overall Survival
Type I: endometrioid, endometrioid + squamous differentiation,
mucinous
Type II: serous, clear cell, carcinosarcoma

• Trial Model: Academic (A)
• Sponsor: Philipps-University Marburg / AGO Study Group
• Trial status: Recruiting
• Planned accrual: 640 patients in 5 years
• Current accrual: 173 patients randomized (Status May 14th, 2020)
• GCIG Groups involved: AGO, NOGGO, KGOG
Further groups are invited to join
• Other important information: None
ECLAT - Endometrial Cancer
Lymphadenectomy Trial
AGO-OP.6

E.C.Co. Endometrial Cancer Conservative treatment
A multicentre archive
Data collection is made by appropriate eCRFs via the Clinical Trials Unit of
National Cancer Institute of Naples (Study Data Center) website

PROJECT TYPE / DESIGN & TIME PERSPECTIVE
Observational / Patient archive, Prospective (a first phase of three years is planned, eventually followed by
further three years)
INCLUSION CRITERIA
- Conservatively treated endometrial cancer
- Informed consent to personal data processing
- Existence of an IRB-approved local protocol that allows conservative treatment to be performed (or statement
that such treatment is considered as a standard)
INTERVENTIONS & OUTCOME MEASURES
Data collection - PRIMARY OUTCOME MEASURES: proportion of complete regression, duration of response,
frequency and pattern of relapse, frequency of metachronous ovarian cancer, tumor-related deaths; SECONDARY
OUTCOME MEASURES: treatment related morbidity, frequency of spontaneous pregnancies, frequency of
pregnancies after ART, pattern of residual disease on definitive surgical specimens
TREATMENT
SINCE THIS IS A ARCHIVE, TREATMENT IS NOT DICTATED BY A PROTOCOL, HOWEVER, TREATMENT HAS TO BE
ADMINISTERED ACCORDING TO A IRB-APPROVED LOCAL PROTOCOL (except for the countries where conservative
treatment can be given outside a IRB-approved study because considered as a standard procedure)
E.C.Co. Endometrial Cancer Conservative treatment
A multicentre archive

Country Sites PI #pts registered
Naples, NCI Greggi S. 33
Rome, Catholic University Scambia G 19
Avellino, Malzoni Center Malzoni M. 10
Wien, University Polterauer S. 9
Milan, NCI Raspagliesi F. 7
Bergamo, ‘Papa Giovanni XXIII’ H Malandrino C. 6
Milan, ‘S. Raffaele’ H De Marzi P. 4
Naples, Ist University Zullo F. 3
Bari, ‘Giovanni Paolo II’ H Cormio G. 3
Parkville, Royal Women's H - 1
Fudan, University Chen X. -
Leiden, University - -
Rome, NCI Vizza E. -
Varese, F. Del Ponte H Ghezzi F. -
95
Participation (11.05.2020)
E.C.Co. Endometrial Cancer Conservative treatment
A multicentre archive

E.C.Co. Endometrial Cancer Conservative treatment
A multicentre archive
Fertility-sparing treatment for intramucous, moderately differentiated, endometrioid endometrial cancer:
A Gynecologic Cancer Inter-Group (GCIG) study
In press, Journal of Gynecologic Oncology (accepted, May 25, 2020)
Falcone F, Leone Roberti Maggiore U, Di Donato V, Perrone AM, Frigerio L, Bifulco G, Polterauer S, Casadio P, Cormio G, Masciullo V, Malzoni M, Greggi S
(Analysis on 23 patients)

CONTACT INFORMATION
STEFANO GREGGI, MD, PhD
Gynecologic Oncology Surgery,
Istituto Nazionale Tumori “Fondazione G. Pascale”
Via M. Semmola, 80131, Naples, Italy
Tel.: +39 0815903320; Fax: +39 0815903851
E‐mail: [email protected]
E.C.Co. Endometrial Cancer Conservative treatment
A multicentre archive

Cytoreductive Surgery in Advanced Endometrial Cancer
Multicenter Retrospective Study
Ongoing Trial – status update

Objectives
To explore the feasibility of a biomolecular grouping analysis (ProMisE
molecular classifier)*
*potential subsequent prospective phase to validate
To document the treatment strategy adopted in oncology reference
centers for patients with primary AEC;
To identify the predictors of survival;
To formulate a hypothesis for selection criteria/predictive factors for
successful CRS in AEC;
1
2
3
4
Cytoreductive Surgery in Advanced Endometrial Cancer
Multicenter Retrospective Study
Ongoing Trial – status update

Cytoreductive Surgery in Advanced Endometrial Cancer
Multicenter Retrospective Study
Ongoing Trial – status update
Eligibility
Patients with primary advanced endometrial cancer
treated during the period 2005 – 2015

Inclusion criteria
FIGO Stage: IIIA bulky*; IIIB; IIIC1 bulky*; IIIC2 bulky*; IVA; IVB intraabdominal
* diagnosed by pre-operative imaging techniques and/or intraoperatively
Exclusion criteria
- Age > 75;
- Performance Status (ECOG) >1;
- Patients treated for strictly palliative purposes;
- Patients with second malignancies who had been treated by laparotomy or
who had a therapy that could interfere with the treatment of AEC
Cytoreductive Surgery in Advanced Endometrial Cancer
Multicenter Retrospective Study
Ongoing Trial – status update

Participating site status 11.05.2020
Cytoreductive Surgery in Advanced Endometrial Cancer
Multicenter Retrospective Study
Ongoing Trial – status update
Country Sites Group Recruitment # pts registered
Naples, NCI MITO Active 35
Bari, NCI MITO Active 57
Parkville, The Royal Women's Hospital ANZGOG Active 17
Torino, S. Anna H MITO Active 16
Reggio Emilia, ‘S. Maria Nuova’ H MITO Active 15
Rome, S. Giovanni Addolorata H MITO Active 14
Herston, RBWH and Wesley H ANZGOG Active 8
Trieste, ‘Burlo Garofolo’ H MITO Active 7
Naples, Ist University MITO Active 1
Avellino, Malzoni Center MITO Active 0
Varese, F. Del Ponte H MITO Active 0
Bern, University SAKK Active 0
Bergamo, ‘Papa Giovanni XXIII’ H MITO Active 0
Milan, ‘S. Raffaele’ H MITO Active 0
Subiaco, St John of God Subiaco H ANZGOG Active 0
Westmead H ANZGOG Active 0
Fudan, University SGOG pending -
170

Contact Information
STEFANO GREGGI, MD, PhD
Gynecologic Oncology Surgery,
Istituto Nazionale Tumori di Napoli IRCCS “Fondazione G. Pascale”
Tel.: +39 0815903320; Fax: +39 0815903851
E‐mail: [email protected]
Cytoreductive Surgery in Advanced Endometrial Cancer
Multicenter Retrospective Study
Ongoing Trial – status update
Study package available on
http://www.usc-intnapoli.net

2 Fractions11 Gy at the surface
(7.3 Gy at ½ cm for a 3 cm cylinder)
Standard of care brachytherapy1. 7 Gy @ ½ cm x 32. 5-5.5 Gy @ ½ cm x 43. 6 Gy @ surface x 5
Short Course Adjuvant Vaginal Cuff Brachytherapy (VCB) in Early Endometrial Cancer Compared to Standard of Care (SAVE)
•Primary Objective:•Evaluate patient reported outcomes (PROs) using the Global Health Score from the QLQ30
•Secondary Objectives: •Evaluate cost effectiveness •Evaluate CTCAE v4 toxicities•Document any pattern of recurrence

Short Course Adjuvant Vaginal Cuff Brachytherapy (VCB) in Early Endometrial Cancer Compared to Standard of Care (SAVE)
53/108 accrued

PORTEC-4a
Trial setting: Stage I-II endometrial cancer - high-intermediate risk
Study Design: Randomised trial of molecular profile-based versus standard recommendations for adjuvant radiotherapy
Sponsor(s): LUMC; funding: Dutch Cancer Society
Planned No. of patients: 500
Current accrual: 212
Other important information: International participation : Belgium (Univ hospGhent), Germany (Tübingen, München, Essen, Lubeck), Cancer Trials Ireland; CEEGOG Prague; GINECO preparing activation; Vienna preparing activation
Ongoing Trials – status update
Inclusion criteria: FIGO 2009 – high intermediate risk endometrial cancer
• Stage IA (with invasion), any age with grade 3 • Stage IB, grade 1-2 and age > 60• Stage IB, grade 1-2 and LVSI+• Stage IB, grade 3 without LVSI• Stage II (microscopic), grade 1

PORTEC-4a
Ongoing Trials – status update
2 1 Standard treatment recommendation based on clinicopathological factors
Vaginal brachytherapy
Vaginal brachytherapy (~40%)
Observation (~55%)
External beam radiation therapy (~5%)
Follow-up and Quality of Life
Randomisation
Favourable
Intermediate
Unfavourable
Individual treatment recommendation based on
molecular pathology analysis

PORTEC-4a
Ongoing Trials – status update
Pilot phase (n=50) endpoints:
• Logistics of molecular analysis (< 2 wks)
• Patient acceptance
• Completed: 50 pts
PORTEC-4a study endpoints (n=500):
• Vaginal control and RFS
• Pelvic and distant recurrence and OS
• Quality of life and freedom from symptoms
• Costs and use of health care resources
• Current total: 327
➢ Requirement to determine profile within 2 working weeks➢ Participating groups: validation of molecular profile & logistics;
dummy run & QA procedure for brachytherapy
➢ Some delay in accrual due to COVID-19

Trial model: academic
Sponsor(s): MaNGO - Istituto di Ricerche Farmacologiche Mario Negri IRCCS - Milan
Principal Investigator: Nicoletta Colombo, Istituto Europeo di Oncologia - Milan
Planned No. of patients: 550
Paclitaxel 175mg/m2
carboplatin AUC 5 or 6 placebo
Maintenance placebo
Paclitaxel 175mg/m2
carboplatin AUC 5 or 6 atezolizumab 1200mg
Maintenance atezo 1200mg
Stage III/IV with residual disease or
recurrent endometrialcancer
Confirmed PD
R 1:2
Stratified by:
▪ Country
▪ Histological type
▪ Disease (recurrent disease vs advanced disease at primary
diagnosis)
▪ MS status
AtTEnd - Atezolizumab Trial in
Endometrial cancer

AtTEnd - Study Update
As of 22 May 2020
number of randomized patients: 183• Trial status: recruiting
• Accrual start: October 2018
• GCIG involved groups:
A-AGO, AGO, SAKK, NCRI,
JGOG, GEICO, ANZGOG
• Involved sites: 94
• Active sites: 62
• ANZGOG sites will be
opened by June 2020

EN Committee, May 2020
Closed Trials – status update

ENGOT-EN1/FANDANGO - Trial DesignA randomised double-blind placebo-controlled phase II trial of first line combination chemo-therapy
with Nintedanib/placebo for patients with advanced or recurrent endometrial cancer.
Stratification:• Stage of disease (stage 3C 2 vs. stage 4 vs. recurrent disease) • Prior adjuvant chemotherapy (yes/no) • Disease status (Measurable vs. non-measurable disease according to RECIST
1.1)
Ran
do
miz
atio
n 1
:1N
= 1
48
Primary end-point:Progression-Free Survival (PFS)
ENGOT model: A
Status: Randomization closedLast patient randomized: 25.01.2019Sponsor: NSGO-CTUNSGO-CTU PM: Mette Engell
Primary Endpoint (PFS) expected:
2021

ENGOT-EN2-DGCG - Trial DesignA phase II Trial of postoperative chemotherapy or no further treatment for patients with node-
negative stage I-II intermediate or high-risk endometrial cancer.
Supported by
n=240
Endometrioid:Stage I - G3; II
Non-endometrioid:Stage I-II
ChemotherapyCarboplatin-Paclitaxel x 6+ BrachytherapyObservation+ Brachytherapy
1:1 randomization
ENGOT model: A
Status: Randomization closedLast patient randomized: 23.04.2019Sponsor: DGCGNSGO-CTU PM: Joan Løhndorf
Primary end-point:Overall survival (OS)
Primary Endpoint (OS) expected:
2022/2023

Endometrial Cancer
Primary stage 4 or relapsed disease
ER positive endometrioid
adenocarcinoma
Randomize
Randomization: 1:1
N=78
ARM ALetrozole, 2.5mg d 1-28 every 28 daysPlacebo 125mg d 1-21 every 28 days
Until progression
ARM BLetrozole, 2.5mg d 1-28 every 28 days
Palbociclib 125mg d 1-21 every 28 days
Until progression
Stratification:• Number of prior lines (primary adv disease vs. 1st relapse vs. ≥2 relapses)• Measurable vs. evaluable disease• Prior use of MPA/Megace
ENGOT-EN3/NSGO-PALEO - Trial DesignA randomized, double-blind, placebo-controlled, phase II trial of Palbociclib in combination with Letrozole versus
Placebo in combination with Letrozole for patients with Estrogen Receptor Positive advanced or recurrent Endometrial
cancer.
ENGOT model: A
Status: Randomization closedLast patient randomized: 21.12.2018Sponsor: NSGO-CTU NSGO-CTU PM: Joan Løhndorf
Primary end-point: Progression-Free Survival (PFS)
Primary Endpoint (PFS):
ESMO 2020

Recommended