5-10-2014
1
Professor Bastiaan R. BloemParkinson Center Nijmegen (ParC)
Radboud University Nijmegen Medical Center
@BasBloem
Gait, freezing, postural instability and FALLS
Falls typically have a single cause
Most falls are environmental
Falls are mainly motor disorders
Falls cannot be prevented
Falls have relatively little importance for patients
The windmills
5-10-2014
2
Why are falls so
important?
Importance of falls
… and immediately decides to retire!
5-10-2014
3
The best predictor offalls is a prior fall
(but falls predict much more …)
“Take home” message!
1967
5-10-2014
4
Scientific confirmation
1999
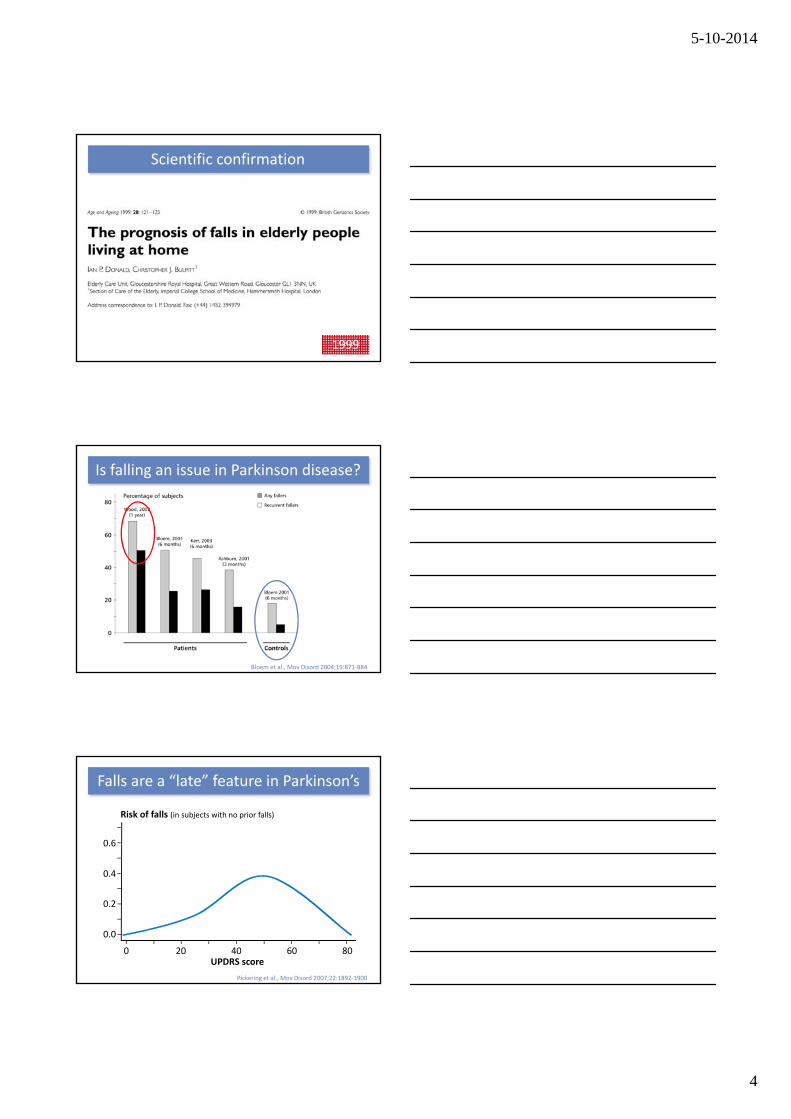
Bloem et al., Mov Disord 2004;19:871‐884
Is falling an issue in Parkinson disease?
Falls are a “late” feature in Parkinson’s
UPDRS score80
Risk of falls (in subjects with no prior falls)
0.6
0.4
0.2
0.0
6040200
Pickering et al., Mov Disord 2007;22:1892‐1900
5-10-2014
5
But when falls do occur ...
Fear of falling
Fewer falls is not necessarily better!
“Take home” message!
5-10-2014
6
I will never fall again!
Fear also leads to inactivity
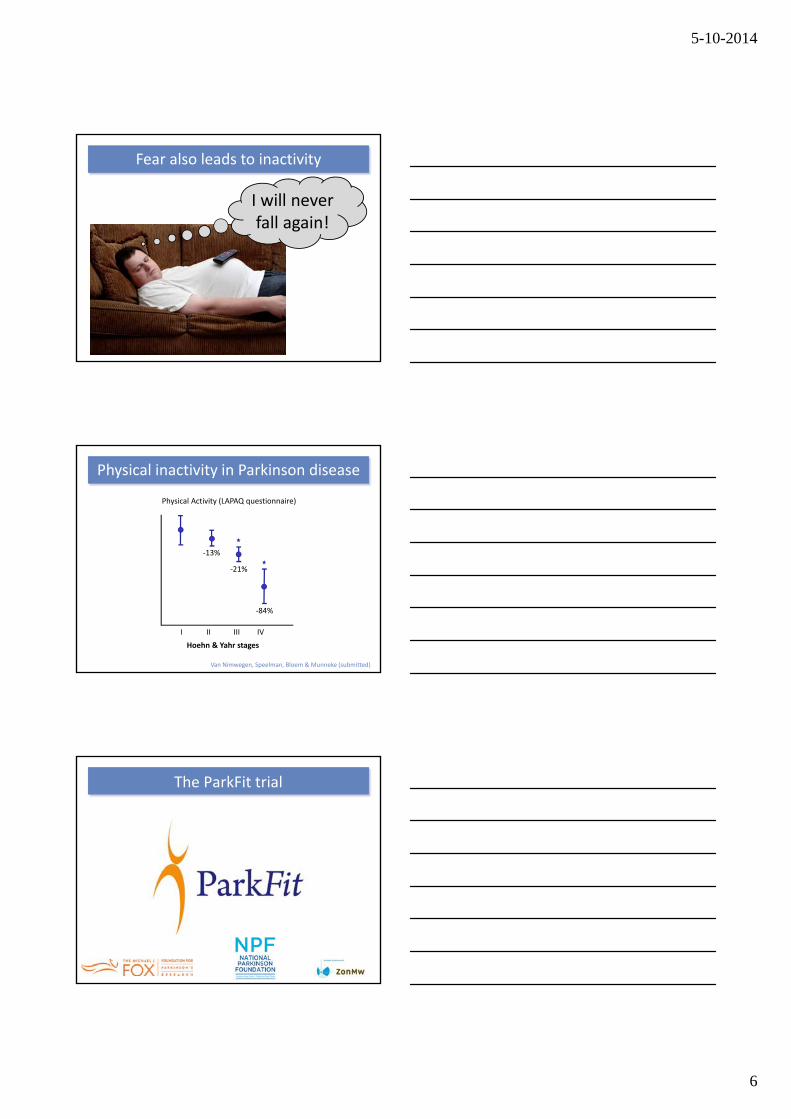
Van Nimwegen, Speelman, Bloem & Munneke (submitted)
Physical inactivity in Parkinson disease
‐13%
‐21%
‐84%
IVIIIIII
Hoehn & Yahr stages
Physical Activity (LAPAQ questionnaire)
The ParkFit trial

5-10-2014
7
Signing up is not enough!
Prevention of physical inactivity
5-10-2014
8
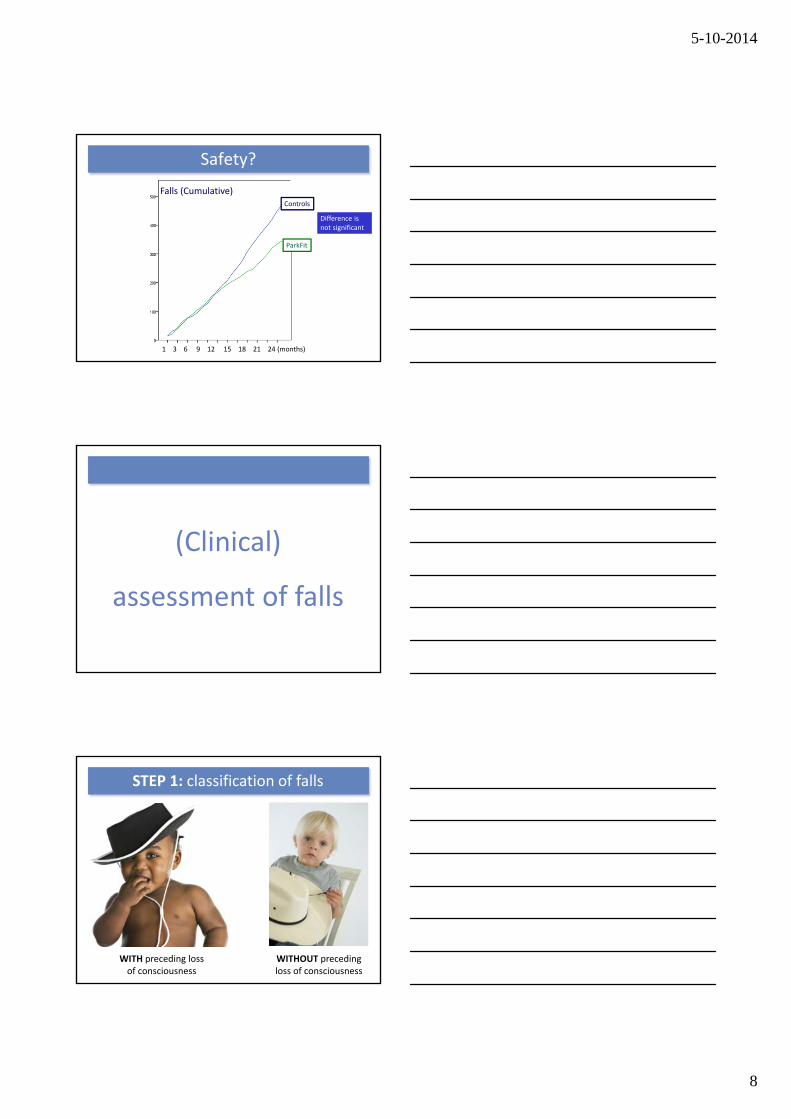
Falls (Cumulative)
1 3 6 9 12 15 18 21 24 (months)
Controls
ParkFit
Safety?
Difference is not significant
(Clinical)
assessment of falls
STEP 1: classification of falls
WITH preceding loss of consciousness
WITHOUT preceding loss of consciousness
5-10-2014
9
Useful tips & tricks
! Contact moment with the floor !
! Nature of the injuries !
Further classification of falls
Intrinsic falls Extrinsic falls
Analysis of security videos
5-10-2014
10
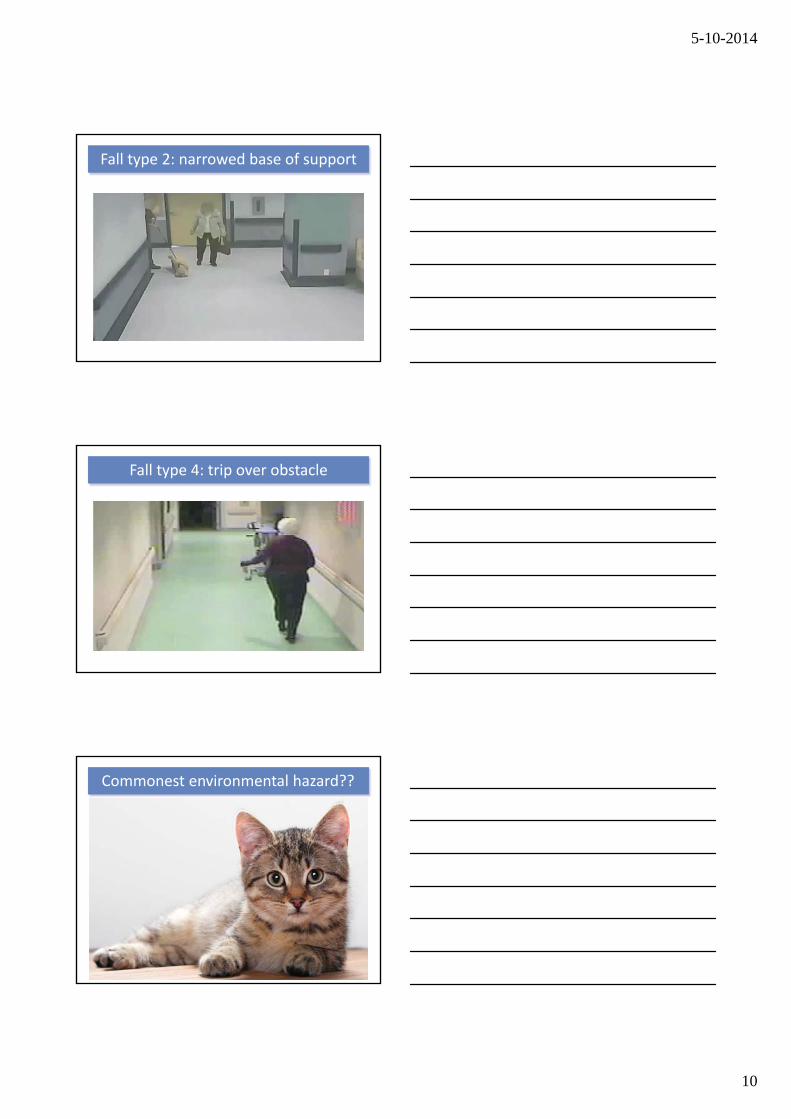
Fall type 2: narrowed base of support
Fall type 4: trip over obstacle
Commonest environmental hazard??
5-10-2014
11
Most falls in Parkinson’s disease are intrinsic
Treat the patient, not the environment
“Take home” message!
STEP 2: prior falls yes or no?
The falls telephone
5-10-2014
12
Automated falls detection
• 3 linear accelerometers• 1 altitude sensor• Validated algorithms
Is my patient likely
to fall (again)?
5-10-2014
13
Intoxications
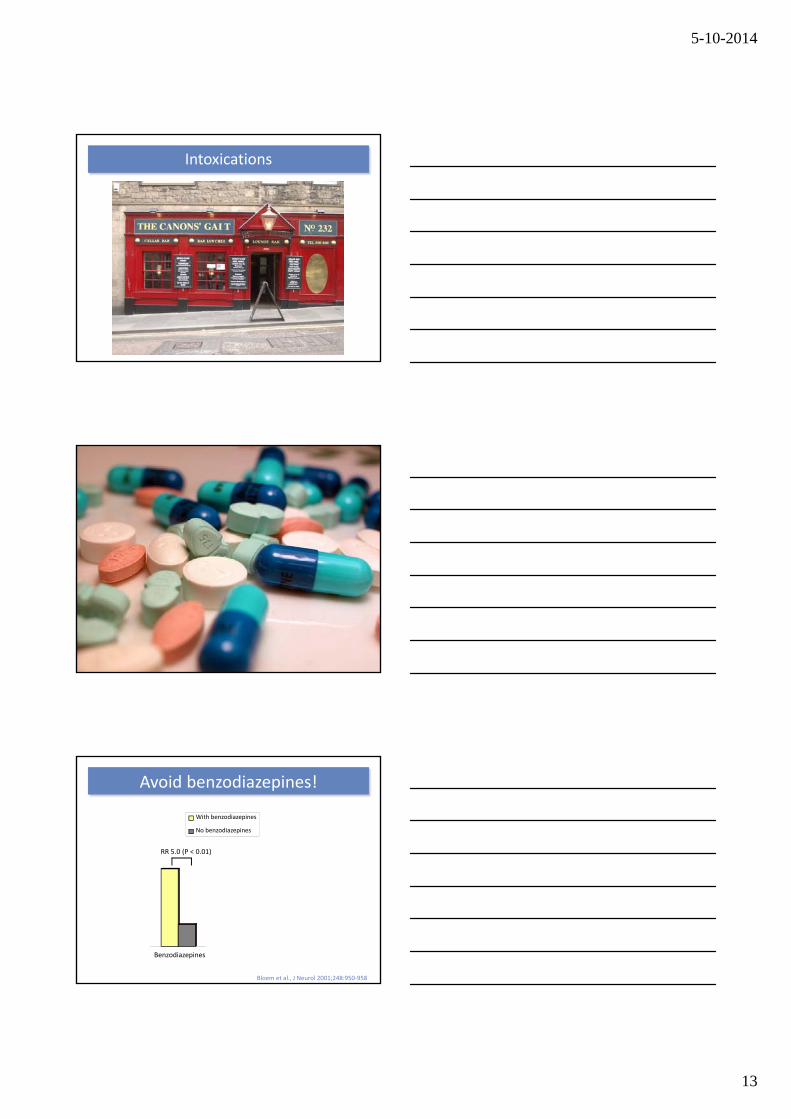
Avoid benzodiazepines!
Benzodiazepines
With benzodiazepines
No benzodiazepines
RR 5.0 (P < 0.01)
Bloem et al., J Neurol 2001;248:950‐958
5-10-2014
14
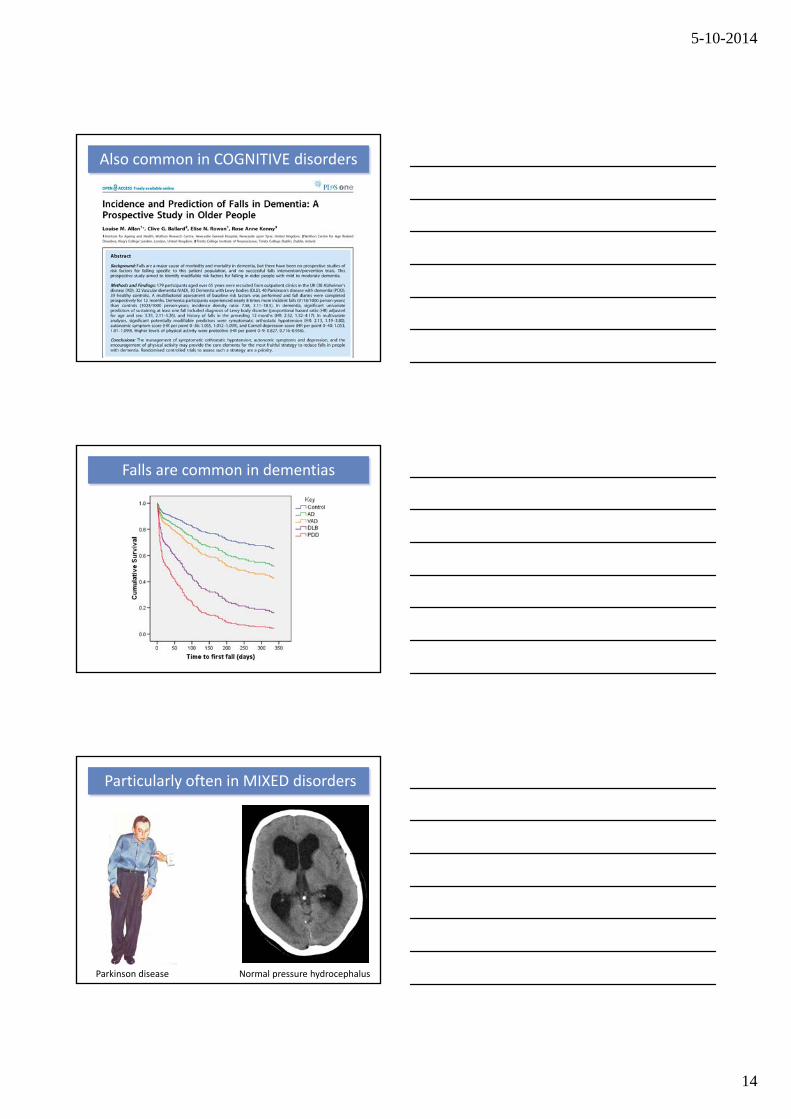
Also common in COGNITIVE disorders
Falls are common in dementias
Particularly often in MIXED disorders
Normal pressure hydrocephalusParkinson disease
5-10-2014
15
‘Spot’ diagnosis
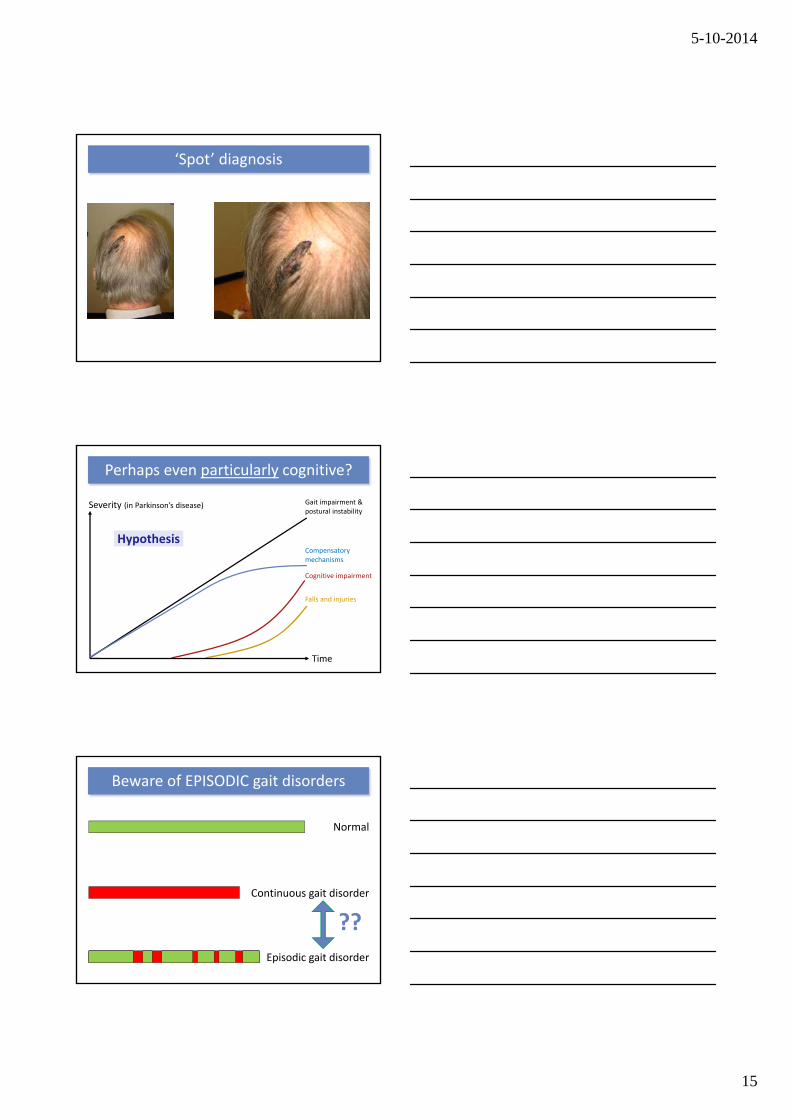
Perhaps even particularly cognitive?
Severity (in Parkinson’s disease)
Time
Gait impairment & postural instability
Compensatory mechanisms
Falls and injuries
Cognitive impairment
Hypothesis
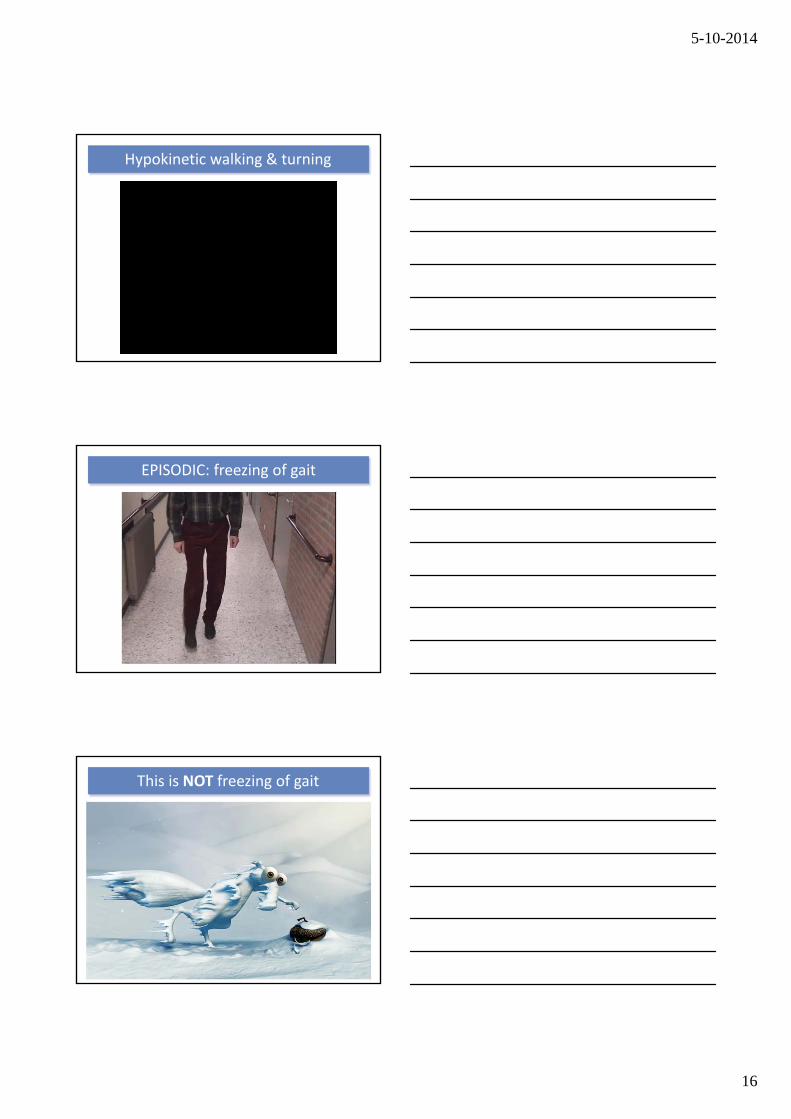
Beware of EPISODIC gait disorders
Continuous gait disorder
Episodic gait disorder
??
Normal
5-10-2014
16
Hypokinetic walking & turning
EPISODIC: freezing of gait
This is NOT freezing of gait
5-10-2014
17
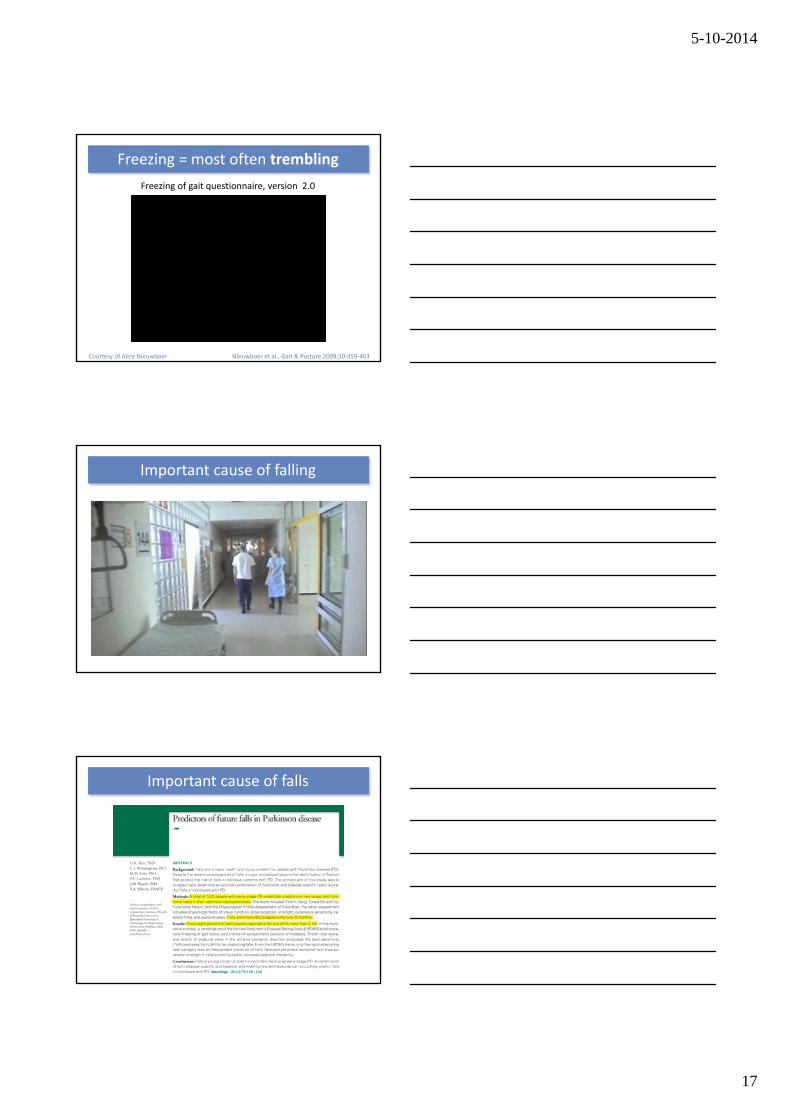
Freezing = most often trembling
Nieuwboer et al., Gait & Posture 2009;30:459‐463
Freezing of gait questionnaire, version 2.0
Courtesy of Alice Nieuwboer
Important cause of falling
Important cause of falls
5-10-2014
18
Falls in Parkinson’s disease = freezing!
“Take home” message!
Absent when being examined
A good illustration
5-10-2014
19
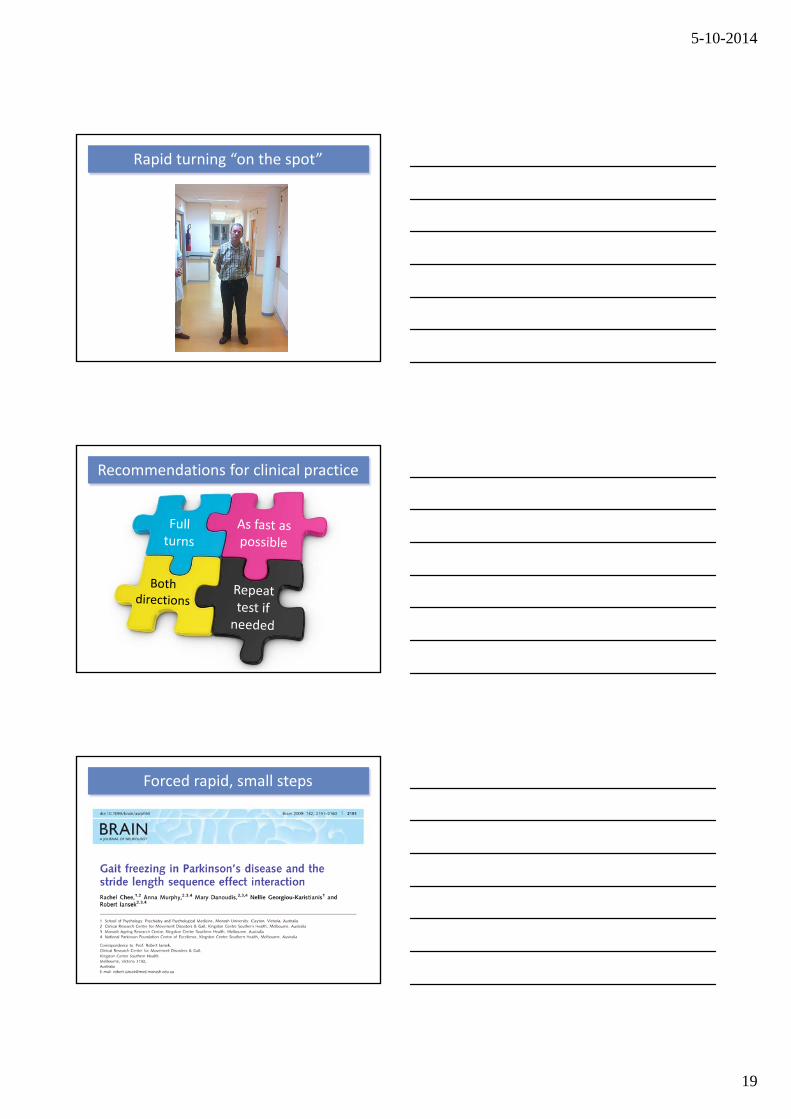
Rapid turning “on the spot”
Recommendations for clinical practice
Forced rapid, small steps
5-10-2014
20
Forced rapid, small steps
Analysis of security videos
Fall type 1: turning (& freezing?)
5-10-2014
21
Consider freezing of gait when patients
• Fall forward
• Claim “spontaneous” falls
• Fall while turning around
Some rules of thumb
Freezing in other species
Treatment of freezing
5-10-2014
22
Dopaminergic abnormalities
Dopa‐induced abnormalities
Non‐dopaminergic abnormalities
Clinical state while freezing
Increaselevodopa
“OFF” period freezing
Courtesy of Alberto Albanese Albanese et al., Neurology 2005;64:1958‐1960
Dopa‐responsive freezing
Threshold to treat freezing of gait
Pseudo ON state freezing
Freezing of gait
Dose of antiparkinson med
ication
Threshold for treatment response
Appendicular symptoms & signs
Dose of antiparkinson med
ication
OFF state
ON state
Threshold for treatment response
OFF state freezing
ON state freezing
My private hypothesis
5-10-2014
23
Dopaminergic abnormalities
Dopa‐induced abnormalities
Non‐dopaminergic abnormalities
Clinical state while freezing
“OFF” period freezing
Decreaselevodopa
Decreaseagonist
ON state freezing of gait
Espay et al., Neurology 2012;78:454‐457
What is this?
Růžička, Nutt and Bloem, Mov Disord, in press
5-10-2014
24
Looks just like …
Dopaminergic abnormalities
Dopa‐induced abnormalities
Non‐dopaminergic abnormalities
Clinical state while freezing
Idazoxan?“Non‐dopaminergic”
freezing?L‐threo‐DOPS?
Duloxetine?
5-10-2014
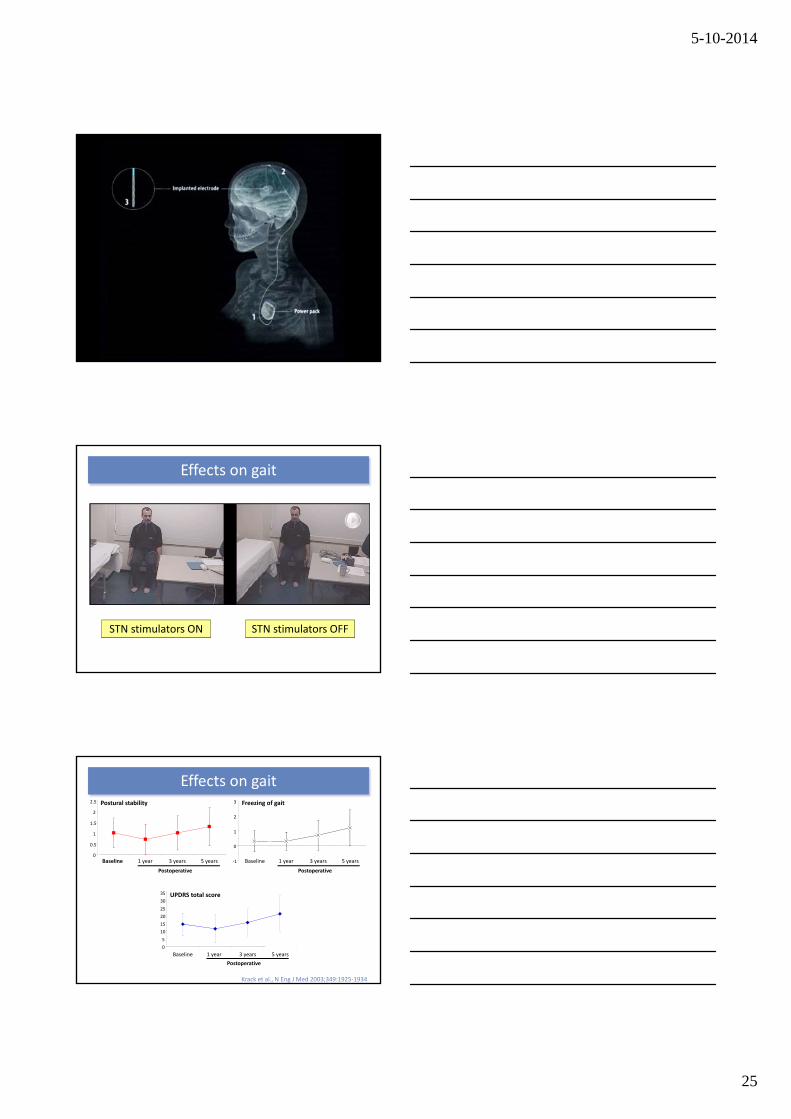
25
STN stimulators ON STN stimulators OFF
Effects on gait
Krack et al., N Eng J Med 2003;349:1925‐1934
0
0.5
1
1.5
2
2.5
Baseline 1 year 3 years 5 years
Postural stability
Postoperative
‐1
0
1
2
3
Baseline 1 year 3 years 5 years
Freezing of gait
Postoperative
0
5
10
15
20
25
30
35
Baseline 1 year 3 years 5 years
UPDRS total score
Postoperative
Effects on gait
5-10-2014
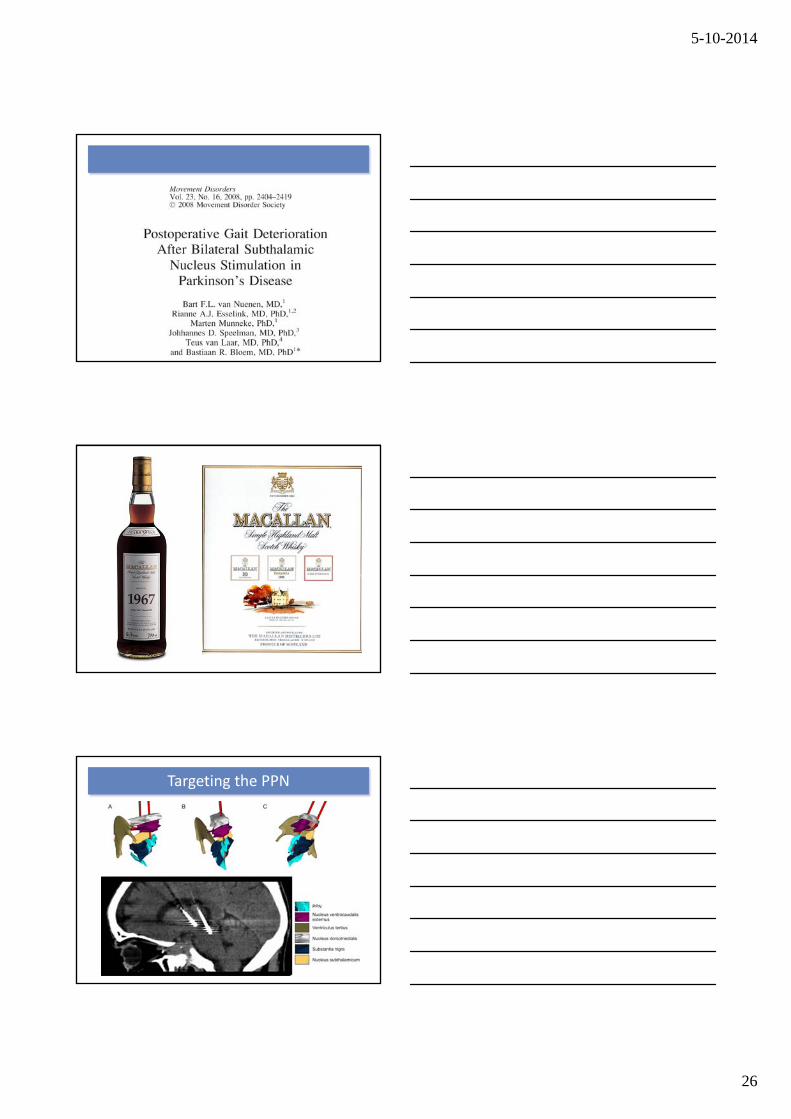
26
Targeting the PPN
5-10-2014
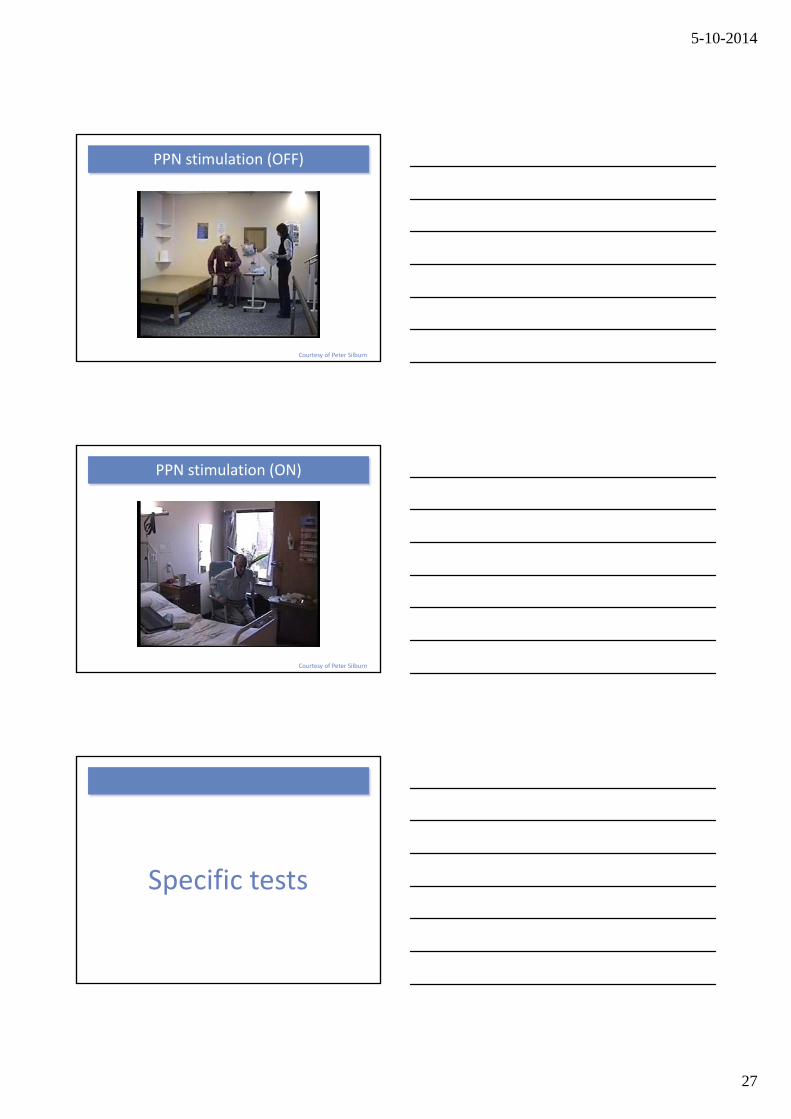
27
PPN stimulation (OFF)
Courtesy of Peter Silburn
PPN stimulation (ON)
Courtesy of Peter Silburn
Specific tests
5-10-2014
28
Traditional testing
Real life example
5-10-2014
29
Real life example
0
10
20
30
40
50
60
70
80
Patients
PercentageP = 0.001
Bloem et al, J Neurol 2001;87:950‐958
Controls
Multiple tasking and falls in PD
Parkinson MSA
Tandem gait testing
5-10-2014
30
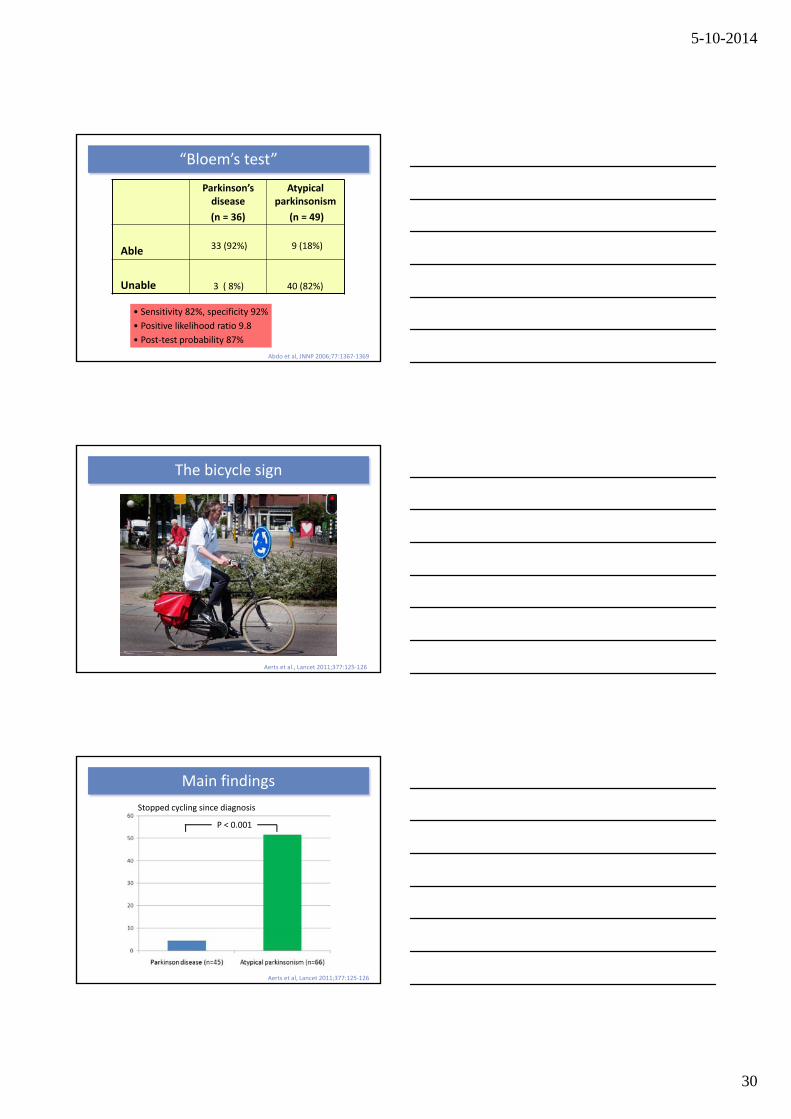
Parkinson’s disease
(n = 36)
Atypical parkinsonism
(n = 49)
Able
Unable
33 (92%)
3 ( 8%)
9 (18%)
40 (82%)
• Sensitivity 82%, specificity 92%
• Positive likelihood ratio 9.8
• Post‐test probability 87%
Abdo et al, JNNP 2006;77:1367‐1369
“Bloem’s test”
The bicycle sign
Aerts et al., Lancet 2011;377:125‐126
Stopped cycling since diagnosis
P < 0.001
Aerts et al, Lancet 2011;377:125‐126
Main findings

5-10-2014
31
Even in Japanese Alps (and Korean mountains?!)
Miwa and Kondo, J Parkinson’s Disease 2012;1:167‐168
Tandem gait and cycling are easy ways to differentiate Parkinson disease
from atypical parkinsonism
“Take home” message!
Freezing in vascular parkinsonism
5-10-2014
32
Under recognized?!
Under recognized?!
Main results
305 consecutive Parkinson patients
• Dizziness Handicap Inventory• Dix‐Hallpike manoeuvre• Test for orthostatic hypotension
Not dizzy (n=154, 51%)Dizzy (n=151, 49%)
Orthostatic hypotension(n=57, 38%)
Classical BPPD(n=12, 8%)
Atypical BPPD(n=4, 3%)
• Symptom free (n=10, 63%)• Improved (n=3)• No improvement (n=3)
• Canalith‐reposition manoeuvre• 3‐month follow‐up
5-10-2014
33
Benign paroxysmal positional vertigo is
common, under recognized but treatable
“Take home” message!
Falls are NOT untreatable
Some rules of thumb
5-10-2014
34
Thank you
Recommended