
© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 1
IDSA Treatment Guidelines for IDSA Treatment Guidelines for Candidiasis and Invasive Candidiasis and Invasive
AspergillosisAspergillosisOut with the old and in with the new!Out with the old and in with the new!
Dr. Dawn WarkentinDr. Dawn WarkentinB.Sc (Pharm), PharmDB.Sc (Pharm), PharmDPharmacotherapeutic Specialist Heme/OncPharmacotherapeutic Specialist Heme/OncCSU Pharmaceutical Sciences, VGHCSU Pharmaceutical Sciences, VGHClinical Associate Professor, Clinical Associate Professor, Faculty of Pharmaceutical Sciences, UBCFaculty of Pharmaceutical Sciences, [email protected]@vch.ca

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 2
IDSA Treatment Guidelines for Candidiasis and IDSA Treatment Guidelines for Candidiasis and Invasive Aspergillosis: Out with the old and in with Invasive Aspergillosis: Out with the old and in with the new!the new!
Outline:Outline:Review significant changes in guidelines inReview significant changes in guidelines intreatment of invasive aspergillus and candidiasistreatment of invasive aspergillus and candidiasis
–– Supporting evidenceSupporting evidence–– Diagnostic testingDiagnostic testing–– Therapeutic drug monitoringTherapeutic drug monitoring
Review available antifungal agentsReview available antifungal agents–– Differences in spectrum of activityDifferences in spectrum of activity–– Differences in pharmacokinetics, ADRs, drug Differences in pharmacokinetics, ADRs, drug
interactions, and cost interactions, and cost

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 3
The Old…The Old…

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 4
Quality of EvidenceQuality of Evidence

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 5
Incidence of Invasive MycosisIncidence of Invasive Mycosis
US National Hospital Discharge Survey statisticsCandida species is 4th leading cause of nosocomial bloodstream infections

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 6
Mortality from Invasive MycosisMortality from Invasive Mycosis

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 7
Expansion of Antifungal Expansion of Antifungal ArmamentariumArmamentarium
New AzolesPosaconazole (2007)
Ravuconazole
New EchinocandinsMicafungin (2007)
Anidulafungin (2007)

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 8
2008 IDSA Guidelines: Management of 2008 IDSA Guidelines: Management of Invasive Aspergillosis (IA)Invasive Aspergillosis (IA)
Invasive pulmonary aspergillosisInvasive pulmonary aspergillosis–– DiagnosisDiagnosis–– Available antifungal agentsAvailable antifungal agents
•• Therapeutic drug monitoringTherapeutic drug monitoring–– Primary therapyPrimary therapy–– Salvage therapySalvage therapy–– ProphylaxisProphylaxis–– Combination therapyCombination therapy–– Adjunctive therapyAdjunctive therapy
•• SurgerySurgery•• ImmunomodulationImmunomodulation
Extrapulmonary aspergillosisExtrapulmonary aspergillosisChronic,saprobic, and allergic formsChronic,saprobic, and allergic forms
Walsh et al. Treatment of Aspergillosis: Clinical Practice Guidelines of the Infectious DiseaseSociety of America. CID 2008;46:327-60.

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 9
Advances in diagnosis of IAAdvances in diagnosis of IADiagnosis should be aggressively Diagnosis should be aggressively pursued whenever possiblepursued whenever possible
–– EORTC definition(EORTC definition(European Organization for European Organization for Research in Treatment of Cancer Research in Treatment of Cancer –– Invasive Fungal Invasive Fungal Infection Cooperative Group)Infection Cooperative Group)
–– Diagnostic imagingDiagnostic imaging•• Halo sign and airHalo sign and air--crescent sign by CTcrescent sign by CT
–– NonNon--culture based diagnosisculture based diagnosis•• Galactomannan Antigen EIAGalactomannan Antigen EIA•• Used in combination with CT findings for Used in combination with CT findings for
early initiation of therapy and to assess early initiation of therapy and to assess responseresponse
–– Not HC approvedNot HC approved–– Promising but remains investigationalPromising but remains investigational–– Surrogate markerSurrogate marker–– Be aware of false positive results (PT, Be aware of false positive results (PT, plasmalyteplasmalyte))

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 10
Recommended approach for Recommended approach for therapeutic drug monitoring (TDM)therapeutic drug monitoring (TDM)
Rationale:Rationale:–– Evidence shows patient to patient variability in Evidence shows patient to patient variability in
pharmacokinetics of triazolespharmacokinetics of triazoles–– Absorption (itra and posa), drug interactions (all), and Absorption (itra and posa), drug interactions (all), and
pharmacogenetics (vori).pharmacogenetics (vori).Not enough data to generate consensus or specific Not enough data to generate consensus or specific recommendations recommendations
Recommend TDM when evaluating reasons for Recommend TDM when evaluating reasons for therapeutic failure or toxicity (Btherapeutic failure or toxicity (B--III)III)

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 11
Therapeutic Drug Monitoring Therapeutic Drug Monitoring (TDM)(TDM)
What the guidelines say:What the guidelines say:–– Itraconazole:Itraconazole:
•• Measure levels to document absorption (BMeasure levels to document absorption (B--II)II)•• Limited evidence but >250ng/ml Limited evidence but >250ng/ml –– more favorable more favorable
outcomeoutcome–– VoriconazoleVoriconazole
•• Measure levels especially with oral therapyMeasure levels especially with oral therapy–– Potential toxicityPotential toxicity–– Document adequate response (BDocument adequate response (B--III)III)
–– PosaconazolePosaconazole•• Limited data, one study observed an association Limited data, one study observed an association
between concentration and response in salvage between concentration and response in salvage invasive aspergillosisinvasive aspergillosis

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 12
Other recent publications of Other recent publications of TDMTDM
Target RangeTarget Range CommentCommentItraconazoleItraconazole Trough >0.5 mcg/mLTrough >0.5 mcg/mL After 7days on therapy After 7days on therapy
to ensure absorptionto ensure absorption
VoriconazoleVoriconazole Trough >2mcg/mLTrough >2mcg/mLPeak <6mcg/mLPeak <6mcg/mLAvg. 1.25mcg/mLAvg. 1.25mcg/mL
After 7days on therapyAfter 7days on therapyEfficacy, toxicityEfficacy, toxicity
PosaconazolePosaconazole Level TBDLevel TBD Average >1.25 mcg/mL Average >1.25 mcg/mL assoc with responseassoc with response
FlucytosineFlucytosine <100 mcg/mL<100 mcg/mL Obtain 2hr after oral Obtain 2hr after oral dose; toxicity seen with dose; toxicity seen with >100mcg/mL>100mcg/mL
Dodds Ashley ES, et al. Clin Infect Dis 2006;43:S28-39. Goodwin ML, et al.J Antimicrob Chemother 2007;61:17-25.
TDM not recommended for amphotericin B, fluconazole, or echinocandins

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 13
Voriconazole TDMVoriconazole TDMFungus Testing LaboratoryFungus Testing LaboratoryUniversity of Texas Health University of Texas Health
Science CenterScience Center7703 Floyd Curl Drive7703 Floyd Curl DriveSan Antonio, Texas 78284San Antonio, Texas 78284Contact: Gennenthel PennickContact: Gennenthel [email protected]@uthscsa.edu
Focus TechnologyFocus Technology5785 Corporate Ave.5785 Corporate Ave.Cypress, California 90630Cypress, California 90630Contact: Dr. Howard EnglerContact: Dr. Howard Englerphph--714714--220220--20652065faxfax--714714--484484--12961296email:hengler@focusanswersemail:hengler@focusanswers
.com.com

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 14
Recommended approach for Recommended approach for primary therapy of IAprimary therapy of IA
Early initiation of therapy (AEarly initiation of therapy (A--I)I)
Voriconazole IV (AVoriconazole IV (A--1)1)
Dose: Dose: •• 6mg/kg IV q12h X 2 then 4mg/kg IV q12h6mg/kg IV q12h X 2 then 4mg/kg IV q12h•• Step down to 200mg PO BID (maximize oral dose by Step down to 200mg PO BID (maximize oral dose by
using 4mg/kg)using 4mg/kg)Consider drug interactions, ADR’s, dosing issues, Consider drug interactions, ADR’s, dosing issues,
renal function with IV renal function with IV

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 15
Voriconazole vs Amphotericin B for Primary Voriconazole vs Amphotericin B for Primary Therapy of Invasive AspergillosisTherapy of Invasive Aspergillosis
Herbrecht R et al. N Engl J Med 2002;347:408-15.
Randomized, unblinded, MC trial
Definite or probable aspergillosis
Voriconazole 6mg/kg IV BID X1 daythen 4mg/kg IV BID X ≥7 days
then 200mg PO BID
Amphotericin B 1-1.5mg/kg/day

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 16
Voriconazole vs Amphotericin B for Primary Voriconazole vs Amphotericin B for Primary Therapy of Invasive AspergillosisTherapy of Invasive Aspergillosis
Authors conclusions: This study shows the superiority of voriconazole over amphotericin B as initial therapy for invasive aspergillosis, in terms of response rate, survival rate, and safetyHerbrecht R et al. N Engl J Med 2002;347:408-15.
Survival at 12 wk in MITT groupVori: 70.8%AmB: 57.9%
10 d77 days

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 17
What is an alternate agent for What is an alternate agent for primary therapy?primary therapy?
Lipid formulation of amphotericin B (ALipid formulation of amphotericin B (A--I)I)–– Dose: 3Dose: 3--5mg/kg/day IV 5mg/kg/day IV
Randomized trial looking at two doses of LRandomized trial looking at two doses of L--amphotericin Bamphotericin B–– 3 mg/kg/day was as effective and less toxic than 3 mg/kg/day was as effective and less toxic than
10mg/kg/day for first 14 days*10mg/kg/day for first 14 days*
e.g. patients where there is contraindication to voriconzolee.g. patients where there is contraindication to voriconzole
* Cornely OA, et al. Liposomal amphotericin B as initial therapy for invasive mold infection: a randomized trial comparing a high-loading dose regimen with standard dosing. Clin Infect Dis 2007;44:1289-97.

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 18
What is an another alternate agent What is an another alternate agent for primary therapy?for primary therapy?
“Amphotericin B “Amphotericin B deoxycholate may be deoxycholate may be the only agent and the only agent and should be considered should be considered standard of care”standard of care”$53/day$53/day
ResourceResource--limited limited settingssettings

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 19
Recommended approach for Recommended approach for salvage therapy of IAsalvage therapy of IA
Include the following:Include the following:–– Lipid formulations of Lipid formulations of
amphotericin B (LFAB)amphotericin B (LFAB)–– ItraconazoleItraconazole–– PosaconazolePosaconazole–– CaspofunginCaspofungin–– MicafuginMicafugin
Refractory to Refractory to Voriconazole?Voriconazole?–– Paucity of dataPaucity of data
Change of class of Change of class of agents and/or agents and/or combinationcombination

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 20
Recommended approach for Recommended approach for combination therapy in IAcombination therapy in IA
Not wellNot well--controlled clinical trials for controlled clinical trials for routine administration for primary routine administration for primary therapytherapy–– potential role in salvage therapypotential role in salvage therapy
Paramount is reversal of Paramount is reversal of immunosuppression or recovery from immunosuppression or recovery from neutropenianeutropenia

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 21
2008 Proposed IDSA Guidelines: 2008 Proposed IDSA Guidelines: Management of Candida InfectionsManagement of Candida Infections
Pappas PG et al. 2007 IDSA Annual Meeting

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 22
Recommended approach for treatment Recommended approach for treatment of candidemia/invasive candidiasisof candidemia/invasive candidiasis
UncomplicatedUncomplicated
NonNon--neutropenicneutropenicHemodynamically stableHemodynamically stableNo recent azole exposureNo recent azole exposure
Not colonized with C. glabrata or kruseiNot colonized with C. glabrata or krusei
↓↓
Start IV fluconazoleStart IV fluconazole
800mg IV x1 800mg IV x1 →→400mg IV qday 400mg IV qday →→ POPO

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 23
Recommended approach for treatment Recommended approach for treatment of candidemia/invasive candidiasisof candidemia/invasive candidiasis
ComplicatedComplicatedNeutropenicNeutropenic
Hemodynamically unstableHemodynamically unstableRecent azole exposureRecent azole exposure
Colonized with C. glabrata or kruseiColonized with C. glabrata or krusei
↓↓
Start EchinocandinStart Echinocandin•• Caspo 70mg LD Caspo 70mg LD →→50mg IV qday or50mg IV qday or
•• Mica 100mg IV qday orMica 100mg IV qday or•• Anidula 200mg LD Anidula 200mg LD →→100mg IV qday100mg IV qday
OR LFAB 3mg/kg/dayOR LFAB 3mg/kg/day
Transition to PO fluco/vori only if sensitivities Transition to PO fluco/vori only if sensitivities knownknown

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 24
Which agent to use for invasive Which agent to use for invasive candida candida -- EchinocandinsEchinocandins
–– MIC and pharmacokinetic differences smallMIC and pharmacokinetic differences small–– More experience with CaspofunginMore experience with Caspofungin–– Micafungin dose is determined (100mg)Micafungin dose is determined (100mg)–– Caspo/mica equivalentCaspo/mica equivalent–– No future studies likelyNo future studies likely
–– Consider all three therapeutically equivalentConsider all three therapeutically equivalent

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 25
What is about in resourceWhat is about in resource--limited limited settings when echinocandins or settings when echinocandins or
LFAB are unavailable?LFAB are unavailable?
“Amphotericin B “Amphotericin B deoxycholate 0.5deoxycholate 0.5--1.0mg/kg/day should 1.0mg/kg/day should be considered standard be considered standard of care”of care”Transition to Transition to fluconazole when you fluconazole when you have an isolate with have an isolate with predictable sensitivitiespredictable sensitivities

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 26
Recommended approach for treatment Recommended approach for treatment of candidemia/invasive candidiasisof candidemia/invasive candidiasis
VoriconazoleVoriconazole–– Offers little advantage over fluconazole as Offers little advantage over fluconazole as
primary therapyprimary therapy–– Limited to transition to PO in selected cases Limited to transition to PO in selected cases
(e.g.. (e.g.. C. kruseiC. krusei))Intravenous catheter removal recommendedIntravenous catheter removal recommendedDuration or therapyDuration or therapy–– Candidemia: at least 2 weeks after last positive Candidemia: at least 2 weeks after last positive
culture and resolution of symptomsculture and resolution of symptoms–– Candidiasis: not studiedCandidiasis: not studied

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 27
When are the echinocandins NOT When are the echinocandins NOT the drug of first choice?the drug of first choice?
Sanctuary SitesSanctuary Sites–– Endophthalmitis?Endophthalmitis?–– Endocarditis?Endocarditis?–– CNS infections?CNS infections?–– CandiduriaCandiduria
C. Parapsilosis in C. Parapsilosis in complicated situations complicated situations such as endocarditis or such as endocarditis or osteomyelitisosteomyelitis

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 28
Quality Improvement MeasuresQuality Improvement Measures
Fundoscopic exam on all patients with Fundoscopic exam on all patients with proven invasive candidiasisproven invasive candidiasisStart antifungal agents within 24 hours of Start antifungal agents within 24 hours of positive culturepositive cultureConfirmatory negative cultures (i.e.. get Confirmatory negative cultures (i.e.. get follow up cultures to document clearance)follow up cultures to document clearance)

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 29

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 30
2008 Proposed IDSA Guidelines: 2008 Proposed IDSA Guidelines: Management of Candida InfectionsManagement of Candida Infections
Major changes from 2004Major changes from 2004
–– EmphasisEmphasis on fluconazole and echinocandins as the on fluconazole and echinocandins as the “preferred choices” for proven/suspected cases“preferred choices” for proven/suspected cases
–– DeDe--emphasisemphasis on AmB and LFAB under most on AmB and LFAB under most circumstancescircumstances
–– Concept of Concept of stepstep--downdown therapy is strongly encouragedtherapy is strongly encouraged–– Voriconazole generally advised as stepVoriconazole generally advised as step--down therapy for down therapy for
selected isolated (e.g. selected isolated (e.g. c. krusei c. krusei and other isolates with and other isolates with known susceptibility dataknown susceptibility data))
–– More emphasis on species identification and More emphasis on species identification and susceptibilitysusceptibility

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 31
2008 Proposed IDSA Guidelines: 2008 Proposed IDSA Guidelines: Management of Candida InfectionsManagement of Candida Infections
Major changes from 2004Major changes from 2004
–– Little distinction made between echinocandinsLittle distinction made between echinocandins–– Fluconazole prophylaxis in neonatal units limited to high Fluconazole prophylaxis in neonatal units limited to high
risk sitesrisk sites–– Consideration of resourceConsideration of resource--limited environmentslimited environments

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 32
Review of currently available Review of currently available antifungal agentsantifungal agents
AvailabilityAvailability POPO IVIVAzolesAzoles
itra, fluco, voriitra, fluco, vori ++ ++
posaconazoleposaconazole ++ --PolyenesPolyenes
amphotericin B deoxycholate amphotericin B deoxycholate and lipid formulations of and lipid formulations of amphotericin B (LFAB)amphotericin B (LFAB)
-- ++
EchinocandinsEchinocandins
caspofungin, micafungin, caspofungin, micafungin, anidulafunginanidulafungin -- ++

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 33
Recent advances in susceptibility Recent advances in susceptibility testing for testing for AspergillusAspergillus sp.sp.
Development of standardized susceptibility testing Development of standardized susceptibility testing for for AspergillusAspergillus species. species. AspergillusAspergillus spp. sent to reference lab in Edmontonspp. sent to reference lab in Edmonton–– Some clinical correlation with azoles and amphotericinSome clinical correlation with azoles and amphotericin
Interpretive breakpoints not established for any Interpretive breakpoints not established for any antifungal agents against filamentous fungi.antifungal agents against filamentous fungi.NonNon--aspergillus molds difficult to interpret MIC dataaspergillus molds difficult to interpret MIC dataOften data from animal models do not correlate Often data from animal models do not correlate clinicallyclinically

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 34
Recent advances in susceptibility Recent advances in susceptibility testing for testing for CandidaCandida sp.sp.
Clinical and Laboratory Standards Institute (CLSI) Clinical and Laboratory Standards Institute (CLSI) has developed reproducible standardized testing of has developed reproducible standardized testing of azoles against azoles against CandidaCandida spp.spp.–– Clinical correlation best for patients with Clinical correlation best for patients with
oropharyngeal/esophageal candidiasis and C. oropharyngeal/esophageal candidiasis and C. albicansalbicans–– Not as good correlation with systemic infections and Not as good correlation with systemic infections and
other yeastsother yeastsCLSI developed standardized testing and CLSI developed standardized testing and determined MIC’s for echinocandins but poor determined MIC’s for echinocandins but poor clinical correlationclinical correlation

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 35
Spectrum of ActivitySpectrum of Activity

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 36
Spectrum of Activity: Spectrum of Activity: EchinocandinsEchinocandins
ActivityActivity SpeciesSpeciesHighly ActiveHighly ActiveLow MIC, fungicidalLow MIC, fungicidal
C. albicans, glabrata, tropicalis, C. albicans, glabrata, tropicalis, krusei, kefyrkrusei, kefyrP. jeroviciP. jerovici
Very ActiveVery ActiveLow MIC without fungicidal Low MIC without fungicidal activity mostlyactivity mostly
C. parapsilosis, guilliermondii, C. parapsilosis, guilliermondii, lusitaniaelusitaniaeA. fumigatus, flavus, terreusA. fumigatus, flavus, terreus
Some ActivitySome ActivityMight have therapeutic Might have therapeutic potential (?combination)potential (?combination)
Coccidioides immitis, B. dermatitidis, Coccidioides immitis, B. dermatitidis, Scedosporium spp, P. variotii, H. Scedosporium spp, P. variotii, H. capsulatumcapsulatum
InactiveInactive Zygomycetes, Cryptococcus Zygomycetes, Cryptococcus neoformans, Fusarium, neoformans, Fusarium, TrichosporonTrichosporon

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 37
Echinocandin’s spectrum of Echinocandin’s spectrum of activity activity -- summarysummary
No consistent relevant differences between No consistent relevant differences between echinocandinsechinocandinsMIC’s in vitro studies vary depending on MIC’s in vitro studies vary depending on center and mediumcenter and mediumC. parapsilosis C. parapsilosis -- MIC in all 3 but ? clinical MIC in all 3 but ? clinical relevance relevance For candida and aspergillus infections: For candida and aspergillus infections: choice of agent is not species drivenchoice of agent is not species driven

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 38
Pharmacokinetic considerationsPharmacokinetic considerations
© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 39
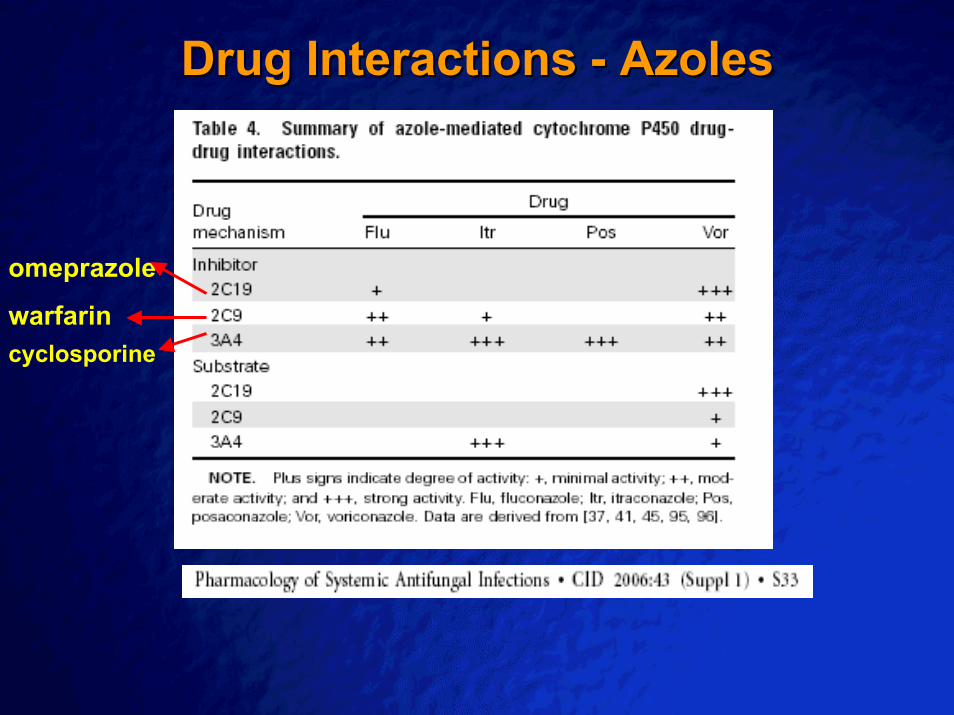
Drug Interactions Drug Interactions -- AzolesAzoles
cyclosporine
omeprazole
warfarin

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 40
Drug Interactions Drug Interactions -- EchinocandinsEchinocandins
CaspofunginCaspofungin–– ↑↑ Caspo by Caspo by CSACSA (33%) (33%) –– controversialcontroversial–– ↓↓ AUC AUC tacrolimustacrolimus by 20%by 20%–– ↓↓ Caspo by P450 inducers such as Caspo by P450 inducers such as rifampin, rifampin,
phenytoin, carbamezapime, nelfinavir, efavirenzphenytoin, carbamezapime, nelfinavir, efavirenz•• ((↑↑ dose from 50 mg to 70mg/day)dose from 50 mg to 70mg/day)
MicafunginMicafungin–– ↑↑ AUC of AUC of nifedipinenifedipine and and sirolimussirolimus
Anidulafungin Anidulafungin –– No interactions reportedNo interactions reported
© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 41
Common Drug ToxicitiesCommon Drug Toxicities
Amphotericin B and LFABAmphotericin B and LFAB–– NephrotoxicityNephrotoxicity–– Electrolyte abnormalitiesElectrolyte abnormalities–– InfusionInfusion--related reactionsrelated reactions
AzolesAzoles–– LFT elevations, rashLFT elevations, rash–– Itra: GI disturbanceItra: GI disturbance–– Vori: visual changes and hallucinationsVori: visual changes and hallucinations
EchinocandinsEchinocandins–– Generally well toleratedGenerally well tolerated–– No major or significant difference between three No major or significant difference between three
drugsdrugs

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 42
Relative “Econotoxicities”Relative “Econotoxicities”
2186 77
220180 201
420
95
188
735
0
100
200
300
400
500
600
700
800FlucoPOFlucoIVAmpho B CaspoMicaAnidulaVori IVVori POPosa POLamB
Daily acquisition cost ($) for treatment of invasive fungal infections

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 43
In conclusion…..In conclusion…..
IDSA Primary treatment of IAIDSA Primary treatment of IA–– Voriconazole or LFABVoriconazole or LFAB–– Resource limited: Amphotericin B deoxycholateResource limited: Amphotericin B deoxycholateIDSA Primary treatment of IC or candidemiaIDSA Primary treatment of IC or candidemia–– Stable patient: fluconazoleStable patient: fluconazole–– Unstable patient: echinocandin or LFABUnstable patient: echinocandin or LFAB
•• Resource limited: Amphotericin B deoxycholateResource limited: Amphotericin B deoxycholate
Consider: species and location of infection, Consider: species and location of infection, organ function, pharmacokinetics, ADR’s organ function, pharmacokinetics, ADR’s and drug interactionsand drug interactions

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 44
Treatment Protocol for Probable/Proven Treatment Protocol for Probable/Proven Invasive Invasive Aspergillosis (IA)Aspergillosis (IA) InfectionInfection
Proven/Probable Aspergillosis
Low risk for developing renal dysfunctionAmphotericin B Deoxycholate
CrCL>50mL/min and high risk for developing renal dysfunction(e.g. allogeneic HSCT and MM, ICU with↓ urine output)Voriconazole (PO if possible)
Consider potential drug interactions with VoriconazoleStep down to PO Voriconazole as soon as safely possible
In Amphotericin B resistant organism (Aspergillus terreus) use Voriconazole or Caspofungin
Marked infusion-related toxicity OR renal dysfunction
CrCL<50mL/min AND 1. Able to take POVoriconzole PO
2. Unable to take POAmbisome
Voriconazole (PO if possible)
Walsh et al. Treatment of Aspergillosis: Clinical Practice Guidelines of the Infectious Disease Society of America. CID 2008;46:327-60

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 45
Treatment Protocol for Probable/Proven Treatment Protocol for Probable/Proven Invasive Invasive Candida (IC)Candida (IC) InfectionInfection
Yeast in blood (species unknown)
Uncomplicated patient(all of the following)Non neutropenicHemodynamically stableNo recent azole exposureNot colonized with C. glabrata or kruseiFluconazole
Complicated patient(any of the following)Neutropenic or major immunodeficiencyHemodynamically unstableRecent azole exposureColonized with C. glabrata or krusei
CaspofunginAmphotericin Bdeoxycholate
Low risk for developing renal dysfunction
CrCL<50mL/min OR high risk for developing renal dysfunction (e.g.allogeneic HSCT and MM, ICUwith↓ urine output)
Pappas PG et al. 2007 IDSA Annual Meeting
Once species identified and sensitivities determined, tailor therapy.See table on next page

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 46

© 2001 By Default!
A Free sample background from www.pptbackgrounds.fsnet.co.uk
Slide 47
Recommended

















