Functional Neurosurgery:Epilepsy Surgery
Functional Neurosurgery:Epilepsy Surgery
Kim J. Burchiel, M.D., F.A.C.S.Department of Neurological Surgery
Oregon Health and Science University
Kim J. Burchiel, M.D., F.A.C.S.Department of Neurological Surgery
Oregon Health and Science University

Epilepsy SurgeryEpilepsy Surgery
• 2 million in US have epilepsy• 400,000-600,000 medically intractable
– 25% candidates for epilepsy surgery• 1500 epilepsy surgery procedures done
in US per year• Cost of epilepsy surgery << lifetime
disability from epilepsy
• 2 million in US have epilepsy• 400,000-600,000 medically intractable
– 25% candidates for epilepsy surgery• 1500 epilepsy surgery procedures done
in US per year• Cost of epilepsy surgery << lifetime
disability from epilepsy

Epilepsy SurgeryEpilepsy Surgery
• J.E. Engle, M.D., Ph.D. (UCLA)– “In all of modern medicine, few generally
accepted therapeutic interventions are as underutilized as surgical treatment for epileptic seizures.”
• J.E. Engle, M.D., Ph.D. (UCLA)– “In all of modern medicine, few generally
accepted therapeutic interventions are as underutilized as surgical treatment for epileptic seizures.”

Epilepsy Surgery: HistoryEpilepsy Surgery: History
• Dr Benjamin Dudley– Trephinated 5 patients for focal motor seizures
(Transylvania Univ - Kentucky 1818-1827)• All 5 lived• 3 became seizure-free
• Hughings Jackson – Convinces Sir Victor Horsley to operate on 3
patients with post-traumatic seizures (National Hospital - London 1886)
• 2 became seizure-free
• Dr Benjamin Dudley– Trephinated 5 patients for focal motor seizures
(Transylvania Univ - Kentucky 1818-1827)• All 5 lived• 3 became seizure-free
• Hughings Jackson – Convinces Sir Victor Horsley to operate on 3
patients with post-traumatic seizures (National Hospital - London 1886)
• 2 became seizure-free

Epilepsy Surgery: HistoryEpilepsy Surgery: History
• Frederic and Erma Gibbs working with Percival Bailey (U. of Illinois 1947)– Temporal lobectomy
• Clinical localization
• Herbert Jasper and Wilder Penfield (Montreal Neurological Institute)– Temporal lobectomy
• Visible pathology– Epilepsy and the Functional Anatomy of the
Human Brain
• Frederic and Erma Gibbs working with Percival Bailey (U. of Illinois 1947)– Temporal lobectomy
• Clinical localization
• Herbert Jasper and Wilder Penfield (Montreal Neurological Institute)– Temporal lobectomy
• Visible pathology– Epilepsy and the Functional Anatomy of the
Human Brain

Epilepsy Surgery?
Medically Refractory Seizures
MRI
Video EEGWada TestNeuropsych
PETSPECT

Temporal LobectomyTemporal Lobectomy


Mesial Temporal SclerosisMesial Temporal Sclerosis

Mesial Temporal SclerosisMesial Temporal Sclerosis


Engel’s Classification System for Postoperative Seizure
Outcome
Engel’s Classification System for Postoperative Seizure
Outcome
• Class I: Free of disabling seizures• Class II: Rare disabling seizures• Class III Worthwhile improvement (>90%
seizure reduction)• Class IV No worthwhile improvement (< 90%
reduction or not improved)
• Class I: Free of disabling seizures• Class II: Rare disabling seizures• Class III Worthwhile improvement (>90%
seizure reduction)• Class IV No worthwhile improvement (< 90%
reduction or not improved)

Wiebe et al NEJM 2001Wiebe et al NEJM 2001
• 80 patients– Uncontrolled seizures
• > monthly• “strong temporal lobe semiology”• > one year• >2 drugs – Inc. DPH, CBZ, VPA
• 80 patients– Uncontrolled seizures
• > monthly• “strong temporal lobe semiology”• > one year• >2 drugs – Inc. DPH, CBZ, VPA

– Excluded patients• Brain lesions requiring urgent surgery• Progressive CNS disorders• Active psychosis• Pseudoseizures• FSIQ < 70• Previous epilepsy surgery• Focal extra-temporal EEG spikes/slowing • MRI evidence extra-temporal epileptogenic lesion• Bilateral temporal lobe pathology
– Excluded patients• Brain lesions requiring urgent surgery• Progressive CNS disorders• Active psychosis• Pseudoseizures• FSIQ < 70• Previous epilepsy surgery• Focal extra-temporal EEG spikes/slowing • MRI evidence extra-temporal epileptogenic lesion• Bilateral temporal lobe pathology
Wiebe et al NEJM 2001Wiebe et al NEJM 2001

• Randomized controlled trial– Mesial temporal lobe surgery (n=40)– Antiepileptic drug therapy (n=40)
• Evaluated by two blinded neurologists– Record review only
• Randomized controlled trial– Mesial temporal lobe surgery (n=40)– Antiepileptic drug therapy (n=40)
• Evaluated by two blinded neurologists– Record review only
Wiebe et al NEJM 2001Wiebe et al NEJM 2001

• Primary outcome measure– Freedom from seizures impairing
awareness (Engle class I)• Complex partial or generalized
• Primary outcome measure– Freedom from seizures impairing
awareness (Engle class I)• Complex partial or generalized
Wiebe et al NEJM 2001Wiebe et al NEJM 2001

• Four patients assigned to surgery did not undergo surgery (intent to treat paradigm)– 1: declined surgery, 2: data inconsistent, 1:
no seizures during monitoring• Six patients had subdural electrode
recording
• Four patients assigned to surgery did not undergo surgery (intent to treat paradigm)– 1: declined surgery, 2: data inconsistent, 1:
no seizures during monitoring• Six patients had subdural electrode
recording
Wiebe et al NEJM 2001Wiebe et al NEJM 2001

• Surgical morbidity– 1 thalamic infarct (sens loss in thigh)– 1 infection– 2 decline in verbal memory
• Asymptomatic VF deficits in 22 (55%)– Superior quadrantanopsia
• No surgical mortality– 1 death in medical arm (sudden, unexplained)
• Surgical morbidity– 1 thalamic infarct (sens loss in thigh)– 1 infection– 2 decline in verbal memory
• Asymptomatic VF deficits in 22 (55%)– Superior quadrantanopsia
• No surgical mortality– 1 death in medical arm (sudden, unexplained)
Wiebe et al NEJM 2001Wiebe et al NEJM 2001

• Primary outcome (Engle class I)– Surgical group – 58%
• 64% in group actually having surgery– Medical group – 8%
• Quality of life– Significantly higher in surgical group
• Employment and school attendance– Strong trend in data favoring surgery
• Primary outcome (Engle class I)– Surgical group – 58%
• 64% in group actually having surgery– Medical group – 8%
• Quality of life– Significantly higher in surgical group
• Employment and school attendance– Strong trend in data favoring surgery
Wiebe et al NEJM 2001Wiebe et al NEJM 2001

Wiebe et al NEJM 2001Wiebe et al NEJM 2001

Wiebe et al NEJM 2001Wiebe et al NEJM 2001

Wiebe et al NEJM 2001Wiebe et al NEJM 2001

• Engle editorial– “Even if referrals for surgery for epilepsy
increase, successful outcomes with respect to seizures may not have a maximal beneficial effect on patients’ lives until referring physicians stop considering intervention for seizures a last resort.”
• Engle editorial– “Even if referrals for surgery for epilepsy
increase, successful outcomes with respect to seizures may not have a maximal beneficial effect on patients’ lives until referring physicians stop considering intervention for seizures a last resort.”
Wiebe et al NEJM 2001Wiebe et al NEJM 2001

• What is it?• How effective is it?• Is it better or worse than Anterior Temporal
Lobectomy?– Seizure outcome– Neuropsychological outcome– Other
• When should its use be considered?
• What is it?• How effective is it?• Is it better or worse than Anterior Temporal
Lobectomy?– Seizure outcome– Neuropsychological outcome– Other
• When should its use be considered?
AmygdalohippocampectomyAmygdalohippocampectomy

Epilepsy SurgeryEpilepsy Surgery

Why Should AH be Considered?
Why Should AH be Considered?
• Preserve temporal neocortex in well-defined cases of mesial TL epilepsy
• Preserve neuropsychological functionfollowing epilepsy surgery– Avoid deficits– Maximize improvements
• Seizure free outcome must be comparable
• Preserve temporal neocortex in well-defined cases of mesial TL epilepsy
• Preserve neuropsychological functionfollowing epilepsy surgery– Avoid deficits– Maximize improvements
• Seizure free outcome must be comparable

Amygdalohippocampectomy: Surgical Approaches
Amygdalohippocampectomy: Surgical Approaches
• Transcortical• Trans-sylvian• Subtemporal
• Transcortical• Trans-sylvian• Subtemporal

Selective Amygdalohippocampectomy
Selective Amygdalohippocampectomy

Anterior Temporal LobectomyAnterior Temporal Lobectomy

• What it is• How effective it is• When its use should be considered• Potential Advantages over Anterior
Temporal Lobectomy
• What it is• How effective it is• When its use should be considered• Potential Advantages over Anterior
Temporal Lobectomy
AmygdalohippocampectomyAmygdalohippocampectomy

Epilepsy SurgeryEpilepsy Surgery

Does Smaller = Better?ATL v AH
Does Smaller = Better?ATL v AH
• What we want:– Large– Randomized– Contemporary– Single Center– Well defined selection criteria and pathology– Comprehensive standardized neuropsychological
battery and outcome measurements
• What we want:– Large– Randomized– Contemporary– Single Center– Well defined selection criteria and pathology– Comprehensive standardized neuropsychological
battery and outcome measurements

• What we have– Variable size– Non-randomized– Non-contemporary– Various inclusion criteria– Varied neuropsychological assessments at
variable time points
• What we have– Variable size– Non-randomized– Non-contemporary– Various inclusion criteria– Varied neuropsychological assessments at
variable time points
Does Smaller = Better?ATL v AH
Does Smaller = Better?ATL v AH

AH vs ATL: Seizure outcomeAH vs ATL: Seizure outcome
• N=74 consecutive, non-lesional cases– 37 AH– 37 ATL
• One year followup• Single center• Similar demographics, MRI features
• N=74 consecutive, non-lesional cases– 37 AH– 37 ATL
• One year followup• Single center• Similar demographics, MRI features
Arruda et al Ann Neurol 1996;40:446-50Arruda et al Ann Neurol 1996;40:446-50

Outcome by Procedure and Imaging Findings
Outcome by Procedure and Imaging Findings
% Seizure Free% Seizure FreeArruda et al Ann Neurol 1996;40:446-50Arruda et al Ann Neurol 1996;40:446-50

AH vs ATL: Seizure OutcomeAH vs ATL: Seizure Outcome
• Total N=321– AH = 138– ATL = 98– Lateral neocortical = 58– Lesion + Hippocampus = 27
• Retrospective• Non-randomized• Non-contemporary• Mean follow-up 38 months
• Total N=321– AH = 138– ATL = 98– Lateral neocortical = 58– Lesion + Hippocampus = 27
• Retrospective• Non-randomized• Non-contemporary• Mean follow-up 38 months
Clusmann J Neurosurg 2002; 97:1131-41Clusmann J Neurosurg 2002; 97:1131-41

AH vs. ATL: ResultsAH vs. ATL: Results
• Overall Outcome– 71% Class I– 11% Class II – 82% “satisfactory”
• Predictive factors– Clear MRI lesion– No history of status– MRI suggesting ganglioglioma or DNET– Concordant lateralized memory deficit– Absence of Dysplasia
• Overall Outcome– 71% Class I– 11% Class II – 82% “satisfactory”
• Predictive factors– Clear MRI lesion– No history of status– MRI suggesting ganglioglioma or DNET– Concordant lateralized memory deficit– Absence of Dysplasia
Clusmann J Neurosurg 2002; 97:1131-41Clusmann J Neurosurg 2002; 97:1131-41

“Satisfactory” Outcome by Procedure
“Satisfactory” Outcome by Procedure
%
NS NS
Clusmann J Neurosurg 2002; 97:1131-41Clusmann J Neurosurg 2002; 97:1131-41

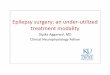
AH vs ATL: Seizure outcomeAH vs ATL: Seizure outcome
• N= 161 (80 ATL, 81 AH)• Single Center• Single Pathology (HS)• Non-randomized• Non-contemporary• Mean followup 5.8 years
• N= 161 (80 ATL, 81 AH)• Single Center• Single Pathology (HS)• Non-randomized• Non-contemporary• Mean followup 5.8 years
Paglioli et al J Neurosurg 2006;104:70-78Paglioli et al J Neurosurg 2006;104:70-78

Outcome by Surgical Procedure
Outcome by Surgical Procedure
Paglioli et al J Neurosurg 2006;104:70-78Paglioli et al J Neurosurg 2006;104:70-78

Visual FunctionVisual Function
• Risk of contralateral quadrantanopsia• VFD 10% from center
– 7% ATL– 28% AH
• VFD 40% from center– 74% ATL– 78% AH
• Risk of contralateral quadrantanopsia• VFD 10% from center
– 7% ATL– 28% AH
• VFD 40% from center– 74% ATL– 78% AH
Egan et al Neurology 55:1818-22, 2000

Should AH Result in Better Postoperative Cognitive Function?
Should AH Result in Better Postoperative Cognitive Function?
Perforant Path
Mossy FibersSchaffer Collaterals
Alveolar Path

Should AH Result in Better Postoperative Cognitive Function?
Should AH Result in Better Postoperative Cognitive Function?
• Less tissue is resected• Anterior Temporal Neocortex has a role in
– Language• Ojemann J Neurosurg 71:316-326, 1989• Hamberger et al.
– Neurology 56:56-61, 2001– Neurology 60:1478-83, 2003– Brain 128:2742-9, 2005
– Memory• Bayley et al Neuron 46:799-810
• Commissural pathways may connect operated side neocortex to opposite hipppocampus
• Less tissue is resected• Anterior Temporal Neocortex has a role in
– Language• Ojemann J Neurosurg 71:316-326, 1989• Hamberger et al.
– Neurology 56:56-61, 2001– Neurology 60:1478-83, 2003– Brain 128:2742-9, 2005
– Memory• Bayley et al Neuron 46:799-810
• Commissural pathways may connect operated side neocortex to opposite hipppocampus

Should AH Result in Better Postoperative Cognitive
Function?
Should AH Result in Better Postoperative Cognitive
Function?
• Disconnection of temporal neocortex• Preserved temporal neocortex is
hypometabolic– “Is amygdalohippocampectomy really selective in
medial temporal lobe epilepsy?” (Dupont et al Epilepsia 42:731-40, 2001)
• Disconnection of temporal neocortex• Preserved temporal neocortex is
hypometabolic– “Is amygdalohippocampectomy really selective in
medial temporal lobe epilepsy?” (Dupont et al Epilepsia 42:731-40, 2001)

AH vs. ATL: Cognitive Outcomes are Equivalent
AH vs. ATL: Cognitive Outcomes are Equivalent
• Montreal (ATL) n=23• Zurich (AH) n=25• Dublin (neocortical resection) n=23• Administered Verbal and Visuospatial
memory tests postoperatively (vs. controls)• Conclusion: Performance varied by side of
surgery not procedure
• Montreal (ATL) n=23• Zurich (AH) n=25• Dublin (neocortical resection) n=23• Administered Verbal and Visuospatial
memory tests postoperatively (vs. controls)• Conclusion: Performance varied by side of
surgery not procedure
Jones-Gotman Neuropsychologia 1997;35:963-73

Cognitive Outcomes Not Equivalent: Are the Data
Convincing?
Cognitive Outcomes Not Equivalent: Are the Data
Convincing?• Non-randomized, non-contemporary• N=49
– 17 ATL, 32 AH• Seizure free outcomes equivalent• IQ: Both groups gained 6-7 points postop.• Memory
– ATL: worsened non-verbal memory with R ATL– ATL: much worsened verbal memory with L ATL– AH: better memory following R AH– AH: smaller decrease in VM following L AH
• Non-randomized, non-contemporary• N=49
– 17 ATL, 32 AH• Seizure free outcomes equivalent• IQ: Both groups gained 6-7 points postop.• Memory
– ATL: worsened non-verbal memory with R ATL– ATL: much worsened verbal memory with L ATL– AH: better memory following R AH– AH: smaller decrease in VM following L AH
Morino ‘06

Neuropsychological OutcomesNeuropsychological Outcomes
• Paglioli et al (n=161 AH vs. ATL)– Many neuropsychological outcomes similar– With left sided surgery:
• 29% AH patients had improved verbal memory• 8% ATL patients had improved verbal memory• p=.05
• Clusmann et al (n=321, mostly AH and ATL)– Outcomes in AH superior for
• Verbal Memory• Attention• Total Neuropsychological performance
• Paglioli et al (n=161 AH vs. ATL)– Many neuropsychological outcomes similar– With left sided surgery:
• 29% AH patients had improved verbal memory• 8% ATL patients had improved verbal memory• p=.05
• Clusmann et al (n=321, mostly AH and ATL)– Outcomes in AH superior for
• Verbal Memory• Attention• Total Neuropsychological performance

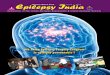
ATL vs. AH: Effects on Verbal Memory by AgeATL vs. AH: Effects on Verbal Memory by Age
Selective Amygdalo-HippocampectomySelective Amygdalo-Hippocampectomy
Anterior TemporalLobectomy
Anterior TemporalLobectomy
ControlsControlsControls ControlsControlsControls
Pre-opPrePre--opop Pre-opPrePre--opop
Post-opPostPost--opopPost-opPostPost--opop
Helmstaedter et al 2002, 2003Helmstaedter et al 2002, 2003
AgeAge AgeAge
P<0.01P<0.01
Ver
bal M
emor
yV
erba
l Mem
ory

Does AH Result in Better Postoperative Cognitive
Function?
Does AH Result in Better Postoperative Cognitive
Function?• Yes
– Paglioli ’06– Morino ‘06– Gleissner ’02, ’04– Hori ’03, ‘07– Clusmann ’02– Pauli ‘99– Helmstaedter ‘96, ’97, ‘02– Wieser ’91 ‘98
• Yes– Paglioli ’06– Morino ‘06– Gleissner ’02, ’04– Hori ’03, ‘07– Clusmann ’02– Pauli ‘99– Helmstaedter ‘96, ’97, ‘02– Wieser ’91 ‘98
• No/Maybe/Equivocal– Jones-Gotman ’97– Wolf ‘93– Goldstein ’93
• No/Maybe/Equivocal– Jones-Gotman ’97– Wolf ‘93– Goldstein ’93

What can guide optimal selection of candidates for
AH?
What can guide optimal selection of candidates for
AH?
• Imaging• Electrophysiology• Clinical Factors• Alternative Imaging Techniques
• Imaging• Electrophysiology• Clinical Factors• Alternative Imaging Techniques

Factors Predictive of AH Failure
Factors Predictive of AH Failure
Abosch ‘02Abosch ‘02
%

Is Type of AH Important?Is Type of AH Important?
• Transcortical vs Transsylvian AH– Transsylvian: avoids neocortical resection but
transects ~20% of anterior temporal stem of superior temporal gyrus and risks vascular injury
– Transcortical: dissect lateral temporal neocortexand traverse WM
• N=140• Randomized• No time, selection, center bias
• Transcortical vs Transsylvian AH– Transsylvian: avoids neocortical resection but
transects ~20% of anterior temporal stem of superior temporal gyrus and risks vascular injury
– Transcortical: dissect lateral temporal neocortexand traverse WM
• N=140• Randomized• No time, selection, center bias
Lutz ‘04Lutz ‘04

Is Type of AH important?Is Type of AH important?
Lutz ‘04Lutz ‘04

Amygdalohippocampectomy: The OHSU Experience
Amygdalohippocampectomy: The OHSU Experience
• 68 consecutive patients with well-defined medial temporal lobe epilepsy and with at least 1 year follow-up
• Most had radiological evidence of mesial temporal sclerosis
• Ages 15-56
• 68 consecutive patients with well-defined medial temporal lobe epilepsy and with at least 1 year follow-up
• Most had radiological evidence of mesial temporal sclerosis
• Ages 15-56

Preoperative MRIPreoperative MRI

AmygdalohippocampectomyAmygdalohippocampectomy

AmygdalohippocampectomyAmygdalohippocampectomy

AmygdalohippocampectomyAmygdalohippocampectomy

How small can it go?How small can it go?

AmygdalohippocampectomyAmygdalohippocampectomy

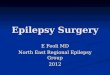
Amygdalohippocampectomy: Surgical Outcome OHSU
Amygdalohippocampectomy: Surgical Outcome OHSU
%
Engel ClassificationEngel Classification

ConclusionsConclusions• Temporal lobe surgery superior to continued BMT for
medically-intractable Temporal Lobe Epilepsy (Class I evidence).
• Outcome of Amygdalohippocampectomy (AH) equivalent and Anterior Temporal Lobectomy (ATL) are equivalent (Class II)
• AH may be superior to ATL– Cognitive outcome (Class III)
• Transcortical AH may be superior to transsylvian AH– Language function (Class III)
• Temporal lobe surgery superior to continued BMT for medically-intractable Temporal Lobe Epilepsy (Class I evidence).
• Outcome of Amygdalohippocampectomy (AH) equivalent and Anterior Temporal Lobectomy (ATL) are equivalent (Class II)
• AH may be superior to ATL– Cognitive outcome (Class III)
• Transcortical AH may be superior to transsylvian AH– Language function (Class III)

Recommended