FFY 2014 – Inpatient Medicare PPS Proposed Rule Summary
May 10, 2013 FR
Presented by Lisa Ellis and Yolanda Chin
May 10, 2013
1

AGENDA
Inpatient PPS Update Factors DRG Rate Calculation Example Wage Index Changes Market Basket DSH Payment Changes DGME Changes Critical Access Hospitals (CAHs) Medicare Dependent Hospital (MDH) Designation Low-Volume Hospitals Sole Community Hospitals (SCH) Value-Based Purchasing Program Hospital Readmission Reduction Program (HRRP) Hospital IQR Program Admission and Medical Review Criteria for Inpatient Services Clarified Proposals for Future Years
2
3
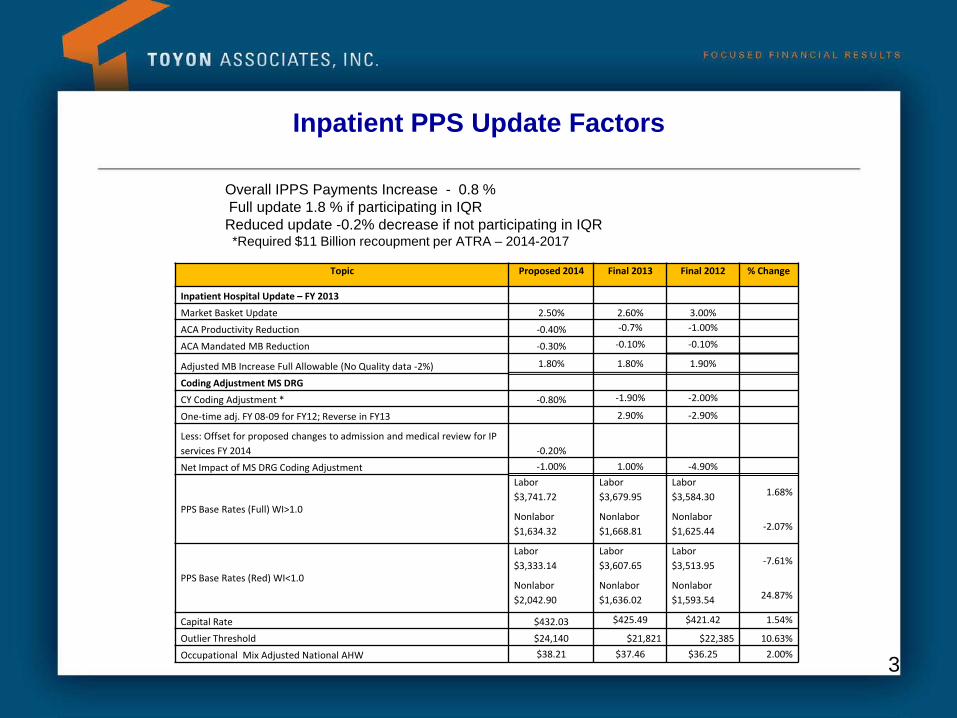
Inpatient PPS Update Factors
Topic Proposed 2014 Final 2013 Final 2012 % Change
Inpatient Hospital Update – FY 2013
Market Basket Update 2.50% 2.60% 3.00%
ACA Productivity Reduction -0.40% -0.7% -1.00%
ACA Mandated MB Reduction -0.30% -0.10% -0.10%
Adjusted MB Increase Full Allowable (No Quality data -2%) 1.80% 1.80% 1.90%
Coding Adjustment MS DRG
CY Coding Adjustment * -0.80% -1.90% -2.00%
One-time adj. FY 08-09 for FY12; Reverse in FY13 2.90% -2.90%
Less: Offset for proposed changes to admission and medical review for IP services FY 2014 -0.20%
Net Impact of MS DRG Coding Adjustment -1.00% 1.00% -4.90%
PPS Base Rates (Full) WI>1.0
Labor $3,741.72
Labor $3,679.95
Labor $3,584.30 1.68%
Nonlabor $1,634.32
Nonlabor $1,668.81
Nonlabor $1,625.44 -2.07%
PPS Base Rates (Red) WI<1.0
Labor $3,333.14
Labor $3,607.65
Labor $3,513.95 -7.61%
Nonlabor $2,042.90
Nonlabor $1,636.02
Nonlabor $1,593.54 24.87%
Capital Rate $432.03 $425.49 $421.42 1.54%
Outlier Threshold $24,140 $21,821 $22,385 10.63% Occupational Mix Adjusted National AHW $38.21 $37.46 $36.25 2.00%
Overall IPPS Payments Increase - 0.8 % Full update 1.8 % if participating in IQR Reduced update -0.2% decrease if not participating in IQR *Required $11 Billion recoupment per ATRA – 2014-2017
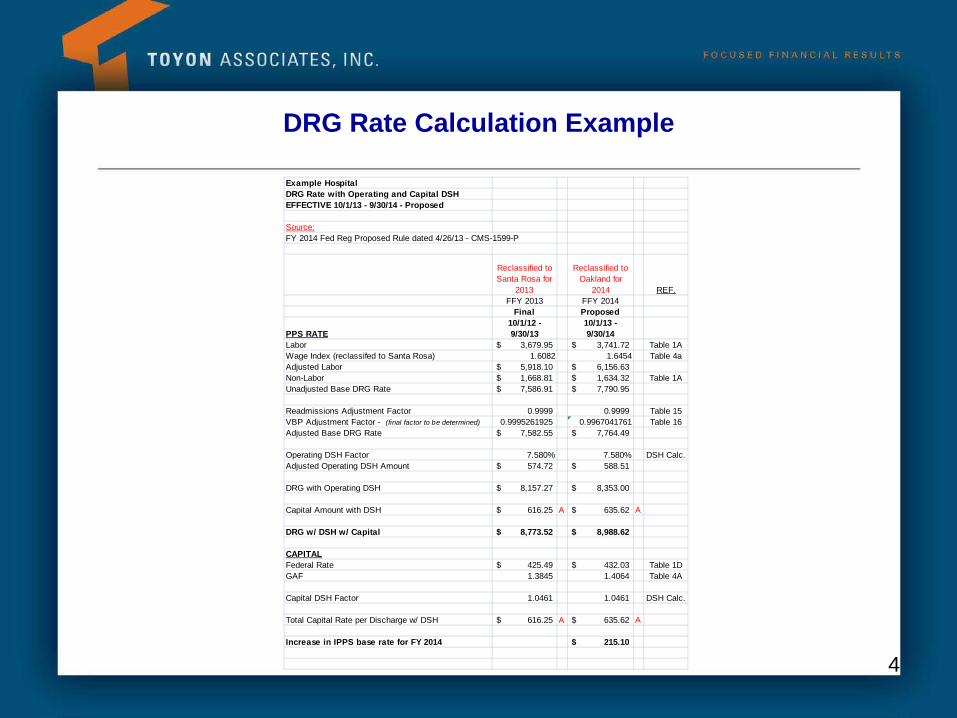
DRG Rate Calculation Example
4
Example HospitalDRG Rate with Operating and Capital DSHEFFECTIVE 10/1/13 - 9/30/14 - Proposed
Source:FY 2014 Fed Reg Proposed Rule dated 4/26/13 - CMS-1599-P
Reclassified to Santa Rosa for
2013
Reclassified to Oakland for
2014 REF.FFY 2013 FFY 2014
Final Proposed
PPS RATE10/1/12 - 9/30/13
10/1/13 - 9/30/14
Labor 3,679.95$ 3,741.72$ Table 1AWage Index (reclassifed to Santa Rosa) 1.6082 1.6454 Table 4aAdjusted Labor 5,918.10$ 6,156.63$ Non-Labor 1,668.81$ 1,634.32$ Table 1AUnadjusted Base DRG Rate 7,586.91$ 7,790.95$
Readmissions Adjustment Factor 0.9999 0.9999 Table 15VBP Adjustment Factor - (final factor to be determined) 0.9995261925 0.9967041761 Table 16Adjusted Base DRG Rate 7,582.55$ 7,764.49$
Operating DSH Factor 7.580% 7.580% DSH Calc.Adjusted Operating DSH Amount 574.72$ 588.51$
DRG with Operating DSH 8,157.27$ 8,353.00$
Capital Amount with DSH 616.25$ A 635.62$ A
DRG w/ DSH w/ Capital 8,773.52$ 8,988.62$
CAPITALFederal Rate 425.49$ 432.03$ Table 1DGAF 1.3845 1.4064 Table 4A
Capital DSH Factor 1.0461 1.0461 DSH Calc.
Total Capital Rate per Discharge w/ DSH 616.25$ A 635.62$ A
Increase in IPPS base rate for FY 2014 215.10$
5
Wage Index Changes
CMS currently uses Office of Management and Budget (OMB) statistical areas to define areas
On February 28, 2013 OMB announced revisions to these statistical areas based on 2010 census, but there was not sufficient time to implement changes
Changes based on 2010 census expected to be proposed for FY 2015
CMS has proposed to extend rural floor through FFY 2014
6
Market Basket
Now rebased to 2010 – will use FY 2010 cost reports for relative portion of base-year cost weights – instead of FY 2006 data
Labor-related share increased to 69.6 percent from 68.8 percent. For hospitals with wage indices of less than 1.0, labor-related share will remain at 62 percent
Market Basket update is 2.5%
7
DSH Payment Changes
New Medicare DSH Payment Method
Changes per ACA Section 1886(r)
Effective FFY 2014
New DSH payment rules do not revise or replace capital DSH payment
Two payment components:
25% of what hospital would have been paid under existing DSH formula - “empirically justified DSH payments”
75% of previous DSH entitlements will be placed in a pool and the new payments based in part on uncompensated care - “uncompensated care DSH payments”
8
DSH 25% of Existing DSH Payment
(“empirically justified DSH payments”)
Still paid on interim payment basis, per discharge
Changes will need to be made to hospital cost report
More detailed operational and cost report instructions will follow the final rule
DSH Eligibility for Uncompensated Care Payment
(“uncompensated care DSH payments”) Subsection (d) hospitals – PPS hospitals that qualify for existing DSH based
on their “disproportionate patient percentage” or Pickle percentage CMS is proposing to exclude:
Sole community hospitals (SCH) that are paid based on their hospital specific payment rate
Maryland hospitals paid under a waiver
Hospital participating in Rural Community Hospital Demonstration
Critical Access Hospitals (CAH)
9
DSH Three Factors Used to Calculate Uncompensated Care Payment
1) CMS estimate of 75% of amount of Medicare DSH payments for FY 2014 (otherwise would have been paid under existing DSH methodology)
2) Adjustment for percent change in national uninsured rate (persons under 65) from a base 2013 rate
3) Each eligible hospital’s estimated uncompensated care amount relative to the estimated uncompensated care amount for all hospitals that are eligible to receive the standard DSH payment
10
DSH Factor 1 – 75% of Aggregate Amount under Old DSH
CMS will estimate the pool in advance of each year – 2014 estimate is
$12.338 billion
75% of that amount would be $9.2535 billion for 2014
This estimate based on February 2013 estimate from Office of the Actuary
Final estimate would be based on July 2013 estimate from Office of the Actuary
11
DSH
Factor 2 – Uninsured Rate Change
Estimated uninsured rate for 2013 is 18% from a Congressional Budget
Office (CBO) letter from 2010
Estimated uninsured rate for 2014 is 16% from a CBO report issued February 5, 2013
Calculation of percent change in uninsured rate:
1 – [(0.16 – 0.18)/0.18] = 1 – 0.111 = .889 (88.9 percent)
This must be reduced per statute by a reduction of 0.1 percentage points for 2014 – 88.9 percent – 0.1 percentage points = 88.8 percent
12
DSH Adjusted Uncompensated Care Pool for 2014 = $8.217 Billion
$9.2535 x 88.8 percent = $8.217 billion
Note – this amount is not based on real data for either 2013 or 2014
CMS is not expecting to reconcile this amount at a later date for actual experience
13
DSH Factor 3 – Uncompensated Care Cost
CMS is proposing to use alternate data to measure uncompensated care cost for
FY 2014, and possibly additional years
FY 2014 proposal to use Medicaid patient days + Medicare SSI patient days from a prior period (2010/2011)
Concerns regarding standardization and completeness of Worksheet S-10 data
For 2014, each hospital’s percent-to-total of uncompensated care cost will be estimated using a proxy:
1. Medicaid days from most recently available cost report (2010/2011)
2. Medicare-SSI days from most recently available SSI ratios (FFY 2010 available now, FFY 2011 available Spring 2013)
Medicare Advantage (Part C) days will be included in SSI fraction (diluting it)
14
DSH Payments for DSH
CMS issued a Medicare Supplementary table containing calculation of allocation percentages.
Each hospital identified as “projected to receive DSH for FY 2014” has been given a “Proposed Factor 3.”
This percentage is then multiplied by $8.217 billion to determine what each hospital will receive for uncompensated care costs.
If a hospital is NOT expected to qualify for standard DSH payment for a fiscal year: No interim payments for Standard DSH or additional payment for uncompensated care If ultimately qualifies for standard payment at cost report settlement, CMS would pay 25
percent and new payment for uncompensated care at that time
If a hospital IS expected to qualify for standard DSH payment for a fiscal year: Interim DSH payments (25 percent) on a discharge basis New uncompensated care payments made periodically but not per discharge If hospital is found not to be eligible at cost report settlement, CMS will recoup interim
payments
15
DSH Uncompensated Care Payments
Uncompensated care payment will be paid on Federal Fiscal Year basis
CMS proposes “to reconcile that amount in the cost reporting period that begins in the respective Federal fiscal year” – 12/31/14 cost report will start receiving uncompensated care costs in fall of 2013
CMS proposes all three factors determined prospectively and not reconciled at cost report settlement
CMS may decide to reconcile factor 3 based on more recent cost report data
16
DSH Sole Community Hospitals
Uncompensated care payments would not be accounted for in determining whether an SCH is paid the higher of the Federal rate or the hospital-specific rate
CMS is proposing to exclude sole community hospitals paid under their hospital specific rate “from the application of section 1886 (r) of the Act” (i.e., no DSH payment or new uncompensated care payment)
17
DSH Medicare Advantage (Part C) Days
CMS proposing to adopt the policy change first announced in 2004:
Include Medicare Advantage days in the SSI fraction – will dilute it
Exclude Medicaid-eligible portion of these days from numerator of Medicaid fraction – will dilute it
This is CMS’ response to the district court decision in the Allina case, where they were ruled against because they did not give required notice-and-comment rulemaking procedure
Going forward, effective 10/1/13, CMS is giving notice of the treatment of Medicare Advantage days
18
DGME Changes
DGME
Proposal to include labor and delivery (L&D) IP days in the Medicare Utilization Ratio (numerator and denominator)
Would require changes to cost report worksheets – WS S-3, Part I
CMS recognizes that this will reduce GME payments, as the denominator will be increased greater than numerator
Reduction in IPPS payments by $15 million in FY 2014
INFLATION UPDATE FREEZE FOR HIGH PER RESIDENT AMOUNTS (PRAs)
Freeze for PRAs that exceed ceiling expires beginning in FY 2014
Cost reporting periods beginning on or after 10/1/13 – apply full CPI-U update for GME payment
19
Critical Access Hospitals (CAHs)
For DGME or IME, a hospital may not claim FTE resident training that occurred at a CAH
CAH can include costs of training these residents when they rotate to the CAH
Also, proposal clarifies COP (Conditions of Participation) – must provide IP care on site
20
Medicare Dependent Hospital (MDH) Designation
MDH designation extended by Section 606 of American Taxpayer Relief Act
(ATRA) for one additional year, through FY 2013
Proposed FY 2014 rule included expiration of MDH payment designation, effective for discharges after 10/1/13. These hospitals will then be paid for inpatient services based on the Federal rate
MDHs can apply for SCH status but must apply by 8/31/13 in order to be paid as SCH at 10/1/13
21
Low-Volume Hospitals
Temporary changes to low volume definition and payment adjustment
methodology that was provided by ACA and ATRA for FY 2011 – FY 2013 are expiring
Return to the definition and payment method in place prior to FY 2011:
Effective for FY 2014 and subsequent years, in order to qualify as a low-volume hospital, a subsection (d) hospital must be more than 25 road miles from another subsection (d) hospital and have less than 200 discharges (that is, less than 200 discharges total, including both Medicare and non-Medicare discharges) during the fiscal year. Under existing policy, effective for FY 2014 and subsequent years, qualifying hospitals would receive the low-volume hospital payment adjustment of an additional 25 percent for discharges occurring during the fiscal year.
22
New Sole Community Hospital (SCH) Applicants
Including labor and delivery days as inpatient days could affect a hospital’s eligibility for SCH status
Total inpatient days of SCH applicant compared to nearby hospital to determine if it is a “like” hospital (SCH must be more than 35 miles from “like” hospital)
Total inpatient days of nearby hospital must be >8% of applicant’s total inpatient days
23
Value-Based Purchasing Program
Would reduce base operating DRG payment amounts by 1.25 percent in FY 2014
Estimated $1.1 billion available for value-based incentive payments for FY 2014
Program is budget neutral
FY 2016 – CMS proposes to remove 3 clinical process of care measures from program and add 3 measures
FY 2017 - 2 additional measures added
24
Hospital Readmissions Reduction Program (HRRP)
Began 10/1/12
FY 2014 maximum penalty increases to 2 percent (ACA requirement)
Three 30-day readmissions measures:
Pneumonia, acute myocardial infarction, and heart failure
Proposal modifies three 30-day readmissions measure to exclude planned readmissions
AHA - “While the AHA welcomes the planned readmissions exclusions, we are disappointed that CMS has not yet excluded readmissions unrelated to the initial reason for admission, as the ACA requires.”
Proposal to add two 30-day readmissions measures beginning in FY 2015 – chronic obstructive pulmonary disease, and total hip/knee arthroplasties
25
Hospital IQR Program
IPPS Hospitals that do not participate in submitting quality data –
receive a negative .2 percent update
Greater than 99% participation now
FY 2014 – 57 quality measures (10 quality measures in 2004)
26
Admission and Medical Review Criteria for Inpatient Services Clarified
Hospitals have needed guidance on when a patient is appropriately treated and paid by Medicare as an inpatient
Supposedly would help patients who have been having longer stays as outpatients because of the hospitals’ uncertainties about payment if patient is admitted
Presumption is that a patient should be admitted if:
• Hospital inpatient admissions spanning at least two midnights (at least more than one Medicare utilization day), will presumptively qualify as appropriate for payment under Medicare Part A.
• Patient requires procedure that is specified as inpatient-only
Presumption can be overcome by medical record documentation if physician admits the patient but the patient stays less than expected time. However, the physician must support their original expectation with medical documentation.
CMS estimate – proposed policy would increase IP PPS expenditures by $220 million.
CMS will permanently and prospectively reduce standardized amount, SCHs’ and MDHs’ hospital-specific rates, and Puerto Rico-specific amount each by 0.2 percent.
AHA – “We are concerned that this proposed policy would continue to allow CMS contractors to second guess physicians’ judgment. We are also very disappointed that CMS is proposing to cut inpatient payments by 0.2 percent to offset the estimated $220 million in additional inpatient PPS expenditures it believes will be associated with this proposed policy.”
FR – “These additional expenditures result from an expected net increase in hospital inpatient encounters due to some encounters spanning more than 2 midnights moving to the IPPS from the OPPS, and some encounters of less than 2 midnights moving from the IPPS to the OPPS.” 27
Proposals for Future Years
2015 – HAC – Hospital-acquired Conditions Effective FY 2015, ACA requires a 1percent reduction in Medicare payment to hospitals in bottom 25 percentile
of national HAC rates Eight quality measures grouped into two domains to determine payment penalties Domain 1 – claims-based Patient Safety Indicators (PSIs) Domain 2 – healthcare-associated infection (HAI) measures – two HAI measures for FY 2015 CMS will calculate a “total HAC score” – higher score indicates worse performance 2016 - IQR PROGRAM To meet FY 2016 IQR reporting requirements, CMS proposes that hospitals have the option to report one
quarter of data for 16 quality measures using electronic health records (EHRs) certified in the meaningful use program. The agency strongly encourages participation in the voluntary election as a precursor to a required electronic reporting requirement of measures. The electronic reporting option would allow hospitals to meet both their FY 2016 IQR reporting requirement for those 16 measures, as well as fulfill the electronic quality measure reporting requirements in the meaningful use program.
AHA – “The AHA is concerned about the substantial differences between EHR-based and manual chart
abstraction methodologies that result in variation in the performance results. We also continue to be concerned that quality measures reported via certified EHRs have not been adequately validated.”
For FY 2016, CMS proposes to remove eight measures from the IQR program. For FY 2016, the agency proposes to add five measures to the IQR program.
28
Recommended


![FY 2020 Inpatient Rehabilitation Facility PPS Final Rule ... · Medicare Inpatient Rehabilitation Facility Prospective Payment System for FY 2020 [CMS-1710-F] Summary of Final Rule](https://img.pdfslide.us/doc/110x75/5e152d886e3b54465b2e79a7/fy-2020-inpatient-rehabilitation-facility-pps-final-rule-medicare-inpatient.jpg)














