Federally Qualified Health Center Look-Alike Program Overview and Initial
Designation Application Process
Jennifer Joseph, PhD, MSEdChief, Strategic Operations Branch
U.S. Department of Health and Human ServicesHealth Resources and Services Administration
Bureau of Primary Health Care

Agenda
• FQHC Definitions, Principles, Benefits and Eligibility
• Program Administration• Application Process• Application Components/Content Overview• Application Submission Information• Review Timelines• Tips for Preparing a Successful Application• Technical Assistance Resources• Questions and Answers
2

What is an FQHC?
Medicare and Medicaid statutes define a provider type: “Federally Qualified Health
Center” (FQHC) – Respectively, Social Security Act §1861(aa)(4) and §1905(l)(2)(B)
• Entity that receives a grant under section 330 of the Public Health Service Act – Health Center Program.
• Entity that is determined by DHHS to meet requirements to receive funding without actually receiving a grant (i.e., FQHC Look-Alike).
• Entities that are outpatient health programs or facilities operated by a tribe or tribal organization under the Indian Self-Determination Act or by an Indian organization receiving funds under Title V of the Indian Health Care Improvement Act.
3

Fundamental Principles
• Private non-profit or public entities that serve a high-need community or population
• Governed by a community board of which at least a majority are health center patients who represent the patient population served
• Provide comprehensive primary care and enabling and supporting services
• Services are available to all, with fees adjusted based upon ability to pay
• Meet all performance and accountability requirements for administrative, clinical and financial operations 4

Benefits
Benefit Health Center Grantees
FQHC Look-Alikes
Health Center Program grant funding YES NOEligible for Medicaid Prospective Payment System (PPS)
YES YES
Eligible for Medicare cost-based reimbursement
YES YES
Access to 340B drug pricing YES YESEligible for Federal Tort Claims Act medical malpractice insurance
YES NO
Automatic Health Professional Shortage Area (HPSA) Designation
YES YES
Vaccines for Children YES YESEligible for supplemental Health Center Program funding
YES NO
5

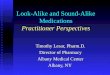
Growth of FQHC Look-Alike Program
1991 20110
20
40
60
80
100
120
28
112
FQHC Look-Alike Organizations
6

Eligibility
Eligibility Requirement Health Center Grantees
FQHC Look-Alikes
Must be a private, charitable, tax-exempt nonprofit organization OR public entity (direct or co-applicant arrangement).
YES YES
Must serve a medically underserved area (MUA) or medically underserved population (MUP) designated by DHHS.
YES YES
Must not be owned, controlled or operated by another entity.
NO YES
Must be operational and providing primary care services at the time of application submission.
NO YES
7

Look-Alike Program Administration
• The FQHC Look-Alike Program is operated under an intra-agency agreement between HRSA and CMS
• HRSA is responsible for:– Assuring compliance with requirements under section
330 of the Public Health Service Act– Making a recommendation to CMS for designation as
a Look-Alike• CMS is responsible for:
– Designating an organization as a Look-Alike– This designation makes the organization eligible to
apply for Medicaid and Medicare reimbursement under the FQHC payment methodologies and to enroll in the 340B drug program 8

Program Administration
• HRSA staff are responsible for:– Developing the application instructions– Providing technical assistance to applicants
and existing FQHC Look-Alikes– Reviewing all initial designation, renewal of
designation, and annual certification applications
– Monitoring continued compliance with program requirements
9

Application Process: Grantee and Look-Alike Comparison
Application Health Center Grantees
FQHC Look-Alikes
Application opportunities for new organizations
New Access Point Rolling
HRSA Electronic Handbook (EHB) application and data reporting
YES YES, as of 2011-2012
10

FQHC Look-Alike Application Types
Application Type Description
Initial Designation Comprehensive application required for organizations seeking initial FQHC Look-Alike designation
Renewal of Designation
Comprehensive application required for existing Look-Alike organizations to renew their FQHC Look-Alike designation after an initial two-year designation period, and thereafter, typically every five-years.
Annual Certification An annual program update submitted by existing FQHC Look-Alikes.
11

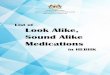
Initial Designation Application Process
Application submitted
HRSA reviews for completeness and
eligibility
Disapproval
HRSA reviews for compliance
HRSA sends recommendatio
n to CMS
Request for changes and TA
Disapproval
CMS designates organization and
informs HRSA
CMS sends recommendation to CMS regional office and State Medicaid
agency
HRSA sends Notice of Look-
Alike Designation
Newly designated FQHC Look-Alike applies to CMS and State Medicaid
agency for FQHC Medicare and Medicaid numbers

Enrolling for FQHC Medicare and Medicaid Reimbursement
• FQHC Look-Alike designation establishes eligibility to enroll in Medicare as an FQHC and for enrollment in State Medicaid program as an FQHC provider.
• Each organization must:– Prepare and submit a Medicare Enrollment
application for each permanent and seasonal site and ensure that it has received the appropriate approvals prior to billing under the FQHC benefit
– Enroll in their State Medicaid program as an FQHC provider 13

Application Overview
The Initial Designation application demonstrates compliance with the requirements of section 330 of the PHS Act, including evidence that the organization: 1. Serves populations in high-need areas2. Will maintain or increase access to primary care
health services, improve health outcomes, and reduce health disparities
3. Provides ready access to the full range of required primary, preventive, enabling and supplemental health care services to all persons in the target population

Application Overview
4. Has a collaborative and coordinated delivery system for the provision of health care to the underserved
5. Has a sound and complete plan that is clearly responsive to identified health care needs of the target population
6. Has a reasonable and accurate budget7. Is already operational and providing primary,
preventive, enabling and supplemental services in the community

Application Components
• Program Narrative– Need– Response – Collaboration– Evaluative measures– Resources/capabilities– Governance
• Forms and Documents• Attachments
16

Forms and Documents
Initial Designation Application Content TypeCover Page FormForm 1A: General Information Worksheet FormTable of Contents DocumentProject Abstract DocumentProject Narrative DocumentClinical Performance Measures FormFinancial Performance Measures FormForm 2: Staffing Profile FormForm 3: Income Analysis Form DocumentForm 3A: FQHC Look-Alike Budget FormForm 4: Community Characteristics FormForm 5A: Services Provided FormForm 5B: Service Sites FormForm 5C: Other Activities/Locations (if applicable) FormForm 6A: Current Board Member Characteristics FormForm 6B: Request for Waiver of Governance Requirements FormForm 8: Health Center Agreements FormForm 9: Need for Assistance FormForm 10: Annual Emergency Preparedness and Management Report FormForm 12: Contacts Information Form

Attachments
Initial Designation Application Content TypeAttachment 1: Patient Origin Study DocumentAttachment 2: Service Area Map DocumentAttachment 3: Current or Requested MUA/MUP Designation DocumentAttachment 4: Governing Board Bylaws DocumentAttachment 5: Governing Board Meeting Minutes DocumentAttachment 6: Co-Applicant Agreement for Public Centers (if applicable) DocumentAttachment 7: Affiliation, Contract, and/or Referral Agreements (if applicable) DocumentAttachment 8: Articles of Incorporation DocumentAttachment 9: Evidence of Non-Profit or Public Agency Status DocumentAttachment 10: Medicare and Medicaid Provider Documentation DocumentAttachment 11: Organizational Chart DocumentAttachment 12: Position Descriptions for Key Personnel DocumentAttachment 13: Resumes for Key Personnel DocumentAttachment 14: Schedule of Discounts/Sliding Fee Scale DocumentAttachment 15: Most Recent Independent Financial Audit DocumentAttachment 16: Letters of Support DocumentAttachment 17: Floor Plans DocumentAttachment 18: Other Information Document

Application Submission
• Applications must be submitted through the HRSA EHB– Refer to HRSA’s Electronic Submission User Guide,
available online at http://bphc.hrsa.gov/about/lookalike/index.html for detailed application and submission instructions.
• Once the Initial Designation application process is started in the EHB system, it must be completed and submitted in a maximum of 90 calendar days.
• Applications that are ineligible or not completed within 90 days will not be considered for designation. 19

Registering in the EHB
• Step one: Create individual system accounts for each individual who will assist in the application preparation, including the following roles: Authorizing official (AO); Business official (BO); Other employee (project directors, assistant staff)
• Step two: Associate individuals with the appropriate organization.
• For assistance in registering with HRSA EHBs, call 877-GO4-HRSA (877-464-4772) or 301-998-7373 between 9:00 am to 5:30 pm ET or email [email protected]
20

Estimated Timelines
21
Responsible Entity
Step in Process Number of Days
Applicant Development and submission of application once the application process has been initiated in the EHB.
90
HRSA Initial review of the application once received in EHB.
105
Applicant Response to any follow-up information requested by HRSA.
30
HRSA HRSA review of applicant response to requested follow-up information.
45
CMS CMS review and approval process 30
Estimated time from application submission to CMS approval for an application with no follow-up information requested by HRSA: Up to 135 days
Estimated time from application submission to CMS approval for an application requiring follow-up information: Up to 210 days

Preparing for a Successful Application
• Perform a thorough needs assessment early• Request technical assistance from your PCA/PCO
or other experienced health centers• Ensure that the organization is operating in full
compliance with each program requirement, including active involvement and oversight of a governing board
• Ensure that all application forms, attachments, and program narrative provide consistent information
• Take advantage of technical assistance resources

23
Avoiding Common Mistakes
Common mistakes in applications:• Organization did not meet the eligibility
requirements• Organization did not demonstrate compliance
with all program requirements• Inconsistencies between the program narrative
and data forms• Application did not include all required forms and
attachments• Applicant did not correctly complete required
forms

Avoiding Common Mistakes: Eligibility
• Organization was owned, operated, or controlled by another entity
• Organization did not have non-profit status• Organization was not serving, in whole or in part,
a MUA/MUP
24

Avoiding Common Mistakes: Need
• Organization’s service area was not clearly defined
• Service area overlap existed with an existing FQHC
• Application contained no discussion of other providers or did not include letters of support from other providers (or an explanation for why they were not included)
• Application data tables did not align with the program narrative and/or organizational chart
25

Avoiding Common Mistakes: Health Services
• Organization did not have after-hours coverage• Organization did not have a sliding fee scale or
the sliding fee scale was not based on the most recent FPL
• Organization did not have admitting privileges or document a continuity of care plan, including discharge planning
26

Avoiding Common Mistakes: Management and Finance
• Organization did not comprehensively discuss lines of authority
• Organization’s organizational chart lacked the names and FTEs of staff or was not aligned with the narrative
• Application did not contain a recent audit• Organization did not have Medicare and Medicaid
provider numbers by site to demonstrate its operational status
27

Avoiding Common Mistakes: Governance
• Organization’s governing board had non-compliant bylaws
• Public entity organization’s co-applicant agreement was not clearly written
• Governing board bylaws did not contain a conflict of interest policy
• The governing board included employees of the organization
• The governing board did not meet at least monthly
28

Key Resources for Application Development
• FQHC Look-Alike Application Instructions 2011-2012 and EHB System User Guides: http://bphc.hrsa.gov/about/lookalike/index.html
• Service Area Overlap: Policy and Process (PIN 2007-09) for guidance on preparing a service area overlap analysis
• Health Center Program Requirements: http://bphc.hrsa.gov/about/requirements/index.html
• FQHC Look-Alike Application Resources document under “Application Help” on the TA page
29

Questions
30

Contact Information
Jennifer JosephChief, Strategic Operations Branch
Telephone: 301-594-4300E-mail: [email protected]
31
Recommended