Int. Rehabil. Med., 7, 93-98 0 Eular Publishers
Original Paper
Exercise testing of leg amputees and the result of prosthetic training
J. A. VAN ALSTB, H. E. P. CRUTS~, K. H U I S M A N ~ and J. DE V R I E S ~
Twente University of Technology; a ‘t Roessingh Rehabilitation Centre; bde Stadsmaten Hospital: Enschedc: The Netherlands
Revised piqier uccvpted.for publication: May 1985. Correspondence 10: Dr. J. ‘4. van AlstC, Twente University of Technology, Dept. of Electrical Engineering.
Biomedical Engineering Division. PO Box 2 17, 7500 AE Enschede, The Netherlands.
Key words disease.
Arm exercise - Cardiac condition - Exercise testing - Exercise electrocardiography - Leg amputees - Peripheral vascular
Summary Thirty-nine patients undergoing rehabilitation following leg amputation were examined to determine cardiac status, which included clinical examination and a graded exercise ECG test, using an arm ergometer. Results were compared to final walking ability. I t was found that the cardiac status of these patients was generally poor and that the exercise ECG results did co-relate to walking ability.
Resume ‘Trente-neuf patients en reeducation fonctionnelle apres avoir subi I’amputation d’une jambe ont ete evalues sur le plan cardiaque. Ce bilan comportait un examen clinique et un ECG a l’effort a I’aide d’un ergometre adapte au membre superieur. Les resultats enregistrb ont ete confrontes a la capacite de marche de chaque sujet en fin de la periode d’entrahement. On a constate que la plupart de ces patients presentaient des fonctions cardiaques alterkes et que I’ECG a I’effort etait un bon reflet de la capacite residuelle de marche.
Zusammenfassung 39 Patienten wurden wahrend ihrer Rehabilitation nach Beinamputation auf ihren Herzbefund untersucht. Diese Untersuchung bestand in einer klinischen Befundaufnahme und in einer Ergometrie, wobei ein Arm-Ergometer benutzt wurde. Die Ergebnissc wurden verglichen mit der Gehfahigkeit beim Austritt. Es wurde festgestellt, dass der kardiale Status dieser Patienten im allgemeincn zu wiinschen iibrig l i e s und dass die Resultate der Ergometrie mit der Gehfahigkeit korrelierten.
Resumen Se exaniinaron treinta y nueve pacientes sometidos a rehabilitacidn tras una amputacion de pierna, con vistas a determinar su estado cardiaco. Ello incluyo un reconocimiento clinico y la prueba del ejercicio graduado con ECG, empleando un ergdmetro de brazo. Los resultados se compararon con la capacidad final para caminar. Se encontro que el estado cardiac0 de estos pacientes era generalmente malo, y 10s resultados del ejercicio en el ECG estuvieron correlacionados con la capacidad para caminar.
Introduction
Eighty to ninety per cent of the some 2000 leg amputations performed annually in the Netherlands are because of cir- culatory problems caused by peripheral atherosclerosis I. Combined with the relatively high age of the patients with a vascular indicated leg amputation (50-90 years) this gives rise to the expectation that the cardiac condition is dimin- ished in a significant number of them.
Despile this expectation quantitative data on the cardiac condition of this population are scarce. To our knowledge only Kavanagh? reported on the cardiac condition of a group of elderly Canadian amputees which he investigated by exercise testing. He reported a history of heart trouble in almost half of the patients and found a substantial depres- sion of the ST-T segment of the electrocardiogram (ECG) during exercise testing in two-thirds of the group. He stated that more attention should be paid to the cardiac problems of the elderly amputee.
It is important to detect subjects with a poor cardiac condition before starting a prosthetic rehabilitation pro- gramme aimed at the restoration of the walking ability. A poor cardiac condition may both (a) influence the progress
Acknowledgment This work has been supported by a grant from the Nederlandse Hartstichtung (The Dutch Heart Foundation).
of the rehabilitation and (b) increase the risk of coronary problems during the rehabilitation process 3 .4 . These as- pects are in addition interrelated; a high coronary risk imposes, or possibly should impose, certain restrictions in the rehabilitation programme in order to remain within safety limits. Patients with a poor cardiac condition are possibly less inclined to exert themselves to the same degree as non-cardiac subjects.
As preliminary results of a study5 we observed relatively high cardiac loads during walking exercises by “vascular” amputees. This was not unexpected in view of the follow- ing.
(a) Comparison of trained amputees with leg prostheses with non-amputees walking at the same speed showed a higher energy consumption ranging from 10% in unilat- eral below-knee amputees to 40- 100°/o in unilateral above-knee amputees6. 7 .
(b) An even higher energy consumption should be expected when untrained amputees are learning to walk again, while the uncoordinated gait pattern accomplished by fewer muscles requires additional effort.
(c) In the period before and after leg amputation the sub- jects have led a sedentary life which has diminished their physical condition *.
Since information concerning the vascular leg amputees is scanty, it was decided to evaluate the cardiac condition of
93
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
6/14
For
pers
onal
use
onl
y.

Int. Rehabil. Med., 1985. vol. 7 . no. 3
this group and to relate it to the degree of prosthetic walking attained at the end of the rehabilitation process, expressed in a three-level scale.
Graded exercise testing has been used with increasing frequency in the diagnosis of coronary artery disease. Exer- cise tests performed according to a suitable protocol provide valuable diagnostic information about the functional capac- ity of the cardiovascular system and form a rational basis for recommendations on physical activities in these pa- tients’, l o . In this study we subjected all vascular leg ampu- tees admitted to our rehabilitation centre during a certain period to graded exercise testing in order to obtain an impression of their cardiac condition and physical work capacity.
Accordingly we defined cardiac condition as the maxi- mum heart rate obtained during graded exercise testing wilhout objective (as observed on the ECG) or subjective (as stated by the patient) cardiac problems. The heart rate is considered to be a good index of the myocardial oxygen consumption“, and can therefore be used as an index for the cardiac energetic load. As a corollary the maximum heart rate is an index for the maximum cardiac load. By adopting the heart rate as reflecting cardiac energetic load we are able to make an explicit distinction between the cardiac and the total energetic load of the body. The latter can be calculated from the oxygen consumption.
The measure used for maximum physical work capacity was the maximum work load obtained during the test. There is no evidence of a linear relation between work load and heart rate in elderly leg amputees performing rowing ergo- metry (see Methods), as there is in bicycle ergometry in healthy subjects. Therefore we used both measures for eval- uation.
However, we were primarily interested in the cardiac load rather than in the patient’s physical work capacity.
The group of vascular leg amputees was examined in order to obtain an impression of
(a) the cardiac condition of amputees novitiating in a pros-
(b) the exercise-induced cardiac problems as visualized on
(c) the maximum heart rate provoked by exercise testing as
(d) the applicability of graded exercise testing in these
thetic rehabilitation programme;
the ECG;
a measure of the cardiac condition;
patients.
The level of prosthetic walking attained at the conclusion of the rehabilitation programme was established. The reha- bilitation result was compared with the findings of the exercise test performed at the initiation of the rehabilitation programme. This comparison was an attempt to correlate a patient’s exercise test performance at the beginning to the prosthetic walking result at the end of the rehabilitation programme.
Knowledge of a patient’s cardiac condition, and of the cardiac loads as induced by specific exercises, can be useful for the physiotherapist to keep the patient within safe levels of activity, while optimizing therapeutical intensity.
Methods
Patients The Roessingh Rehabilitation Centre in Enschede, The Netherlands, admits leg amputees for prosthetic rehabilita- tion programmes after their discharge from the hospital where they underwent amputational surgery. All patients with a leg amputation ensuing from peripheral vascular
disease who started a prosthetic rehabilitation programme at the Centre in the period January 1982-May 1983 were included in this study. The population consisted of 28 men and 11 women with a mean age of 67.4 years (range 43 to 92).
The level of the unilateral leg amputations in men (wom- en) was in seven (six) cases above-knee amputations, in nine (two) cases through-knee, and in eight (two) cases below- knee amputations. Of four male bilateral leg amputees two patients had both through-knee amputations, one patient had two below-knee and one patient had one above-knee and one below-knee amputation. One female patient had two below-knee amputations.
Additional diagnosis included 18 cases of diabetes melli- tus. Other non-cardiac factors present that could adversely affect the prosthetic rehabilitation were: cerebral vascular accident (three patients), blindness (two), deafness (one), arthritis (one), lung embolism (one), and Parkinson’s dis- ease (one). A standard 12-lead ECG was obtained imme- diately before the exercise test.
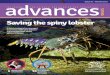
The exercise test The graded exercise test was performed on a specially designed ergometerI*, as shown in Fig. 1. It consists of a load unit on which the seated patient exercises by turning two cranks against an adjustable torque. Both cranks point in the same direction so the patient pushed or pulled with both arms simultaneously during exercise. The resul ting rotation permitted coordinated trunk movement with the use of large body muscles. We called the apparatus provi- sionally a rowing ergometer.
Figure 1 The rowing ergometer in operation.
The patient was seated on the ergometer chair which was positioned at wheelchair height. The patient was secured with a hip seat belt and swivelled into the exercise position. The height of the chair was adjusted and fixed so that the fulcrum of the cranks was at shoulder height and the load- unit position was adjusted to the length of the patient’s arm. The patients were asked to maintain a speed of 50 revolu- tions per minute although the load controlled by the load unit (Lode instruments, type Angio) is in a wide range independent of the rotational speed. Speed was indicated by means of a green lamp (when within the accepted h i t s , 4 6 - 5 4 revolutions per minute) and two red lamps (when outside these limits). This speed indication was also easily interpreted by patients who were visually handicapped.
The test protocol was as follows. First the load was sct at
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
6/14
For
pers
onal
use
onl
y.

VAN ALSTE et a/.: Exercise testing of lee. amDutees
zero to allow the rotating parts of the ergometer to attain working speed, followed by an initial load value of 30 W. The load was increased every minute by 10 W until the patient was unable to continue the exercise or the physician stopped the test.
The electrocardiogram was recorded using the bipolar leads CC5 and CM5 1 3 . The baseline wander, as well as signal and noise components over 100 Hz, were removed by a hardware linear phase bandpass filter
As stated before we used the ECG to detect an upper limit in the attainable cardiac load. If a significant ST-segment depression or rhythm disturbance occurred, the heart rate involved was considered the maximum cardiac load. The detection of ST segment depression, abnormal beats and rhythms were required for this analysis of the ECG. If no ECG abnormalities were encountered, maximum cardiac load was identified as the heart rate obtained at maximum work load. The patient was then unable to continue the test, as a result of general or local fatigue, dyspnoea, etc.
A specially developed hardware device detected QRS complexes and measured interbeat intervals which were transmitted to an Apple-I1 computer. The computer also controlled the ergometer work load protocol and recorded and displayed the heart rate versus work load. The comput- er programme was written in Basic. The unfiltered and filtered ECGs were recorded on a Siemens Elema Oscillom- ink for 10 seconds every minute, also under computer control.
Arterial blood pressure was measured before and within 15 seconds after conclusion of the exercise. The tests were performed under supervision of a cardiologist, who also took the patient’s history, performed the physical examina- tion and judged the rest and exercise ECG.
Quantitative evaluation of the electrocardiogram Besides the simple on-line processing and monitoring as described previously, the ECG was further analysed from an analog recording. The processing was performed by a PDP 11/23 computer system extended with a special-purpose processor called VIPERiJ for some time-consuming mathe- matical operations. It consisted of digital filtering, for removal of base wander, line frequency disturbances and componcnts over 100 Hz. All ECG beats were detected and then classified according to their morphology. This was done by continously calculating the correlation coefficient R(t) between the incoming ECG and a number of templates representing the actual QRS morphologies. When R(t)>0.92, then the ECG beat was assigned to the appro- priate beatclass and the point of time t where R(r) was maximum, was used as fiducial point for averaging. As known from a pilot study”, ectopic beats are often present in the E(’Gs of elderly leg amputees. Averaged beats were obtained from each morphological class in order to remove noise duc to exercise, and updated” to enable measurement of morphological parameters throughout the test. The heart rate was plotted versus exercise time, as was the percentage of ECG heats incorporated in a specific morphological beat class. Morphological and time parameters were plotted after computer measurement from the most prominent beat class, containing the “normal” beats (by definition). Fig. 2 shows a typical example of averaged beats and presents the morphological development of a beat class with the exercise time. The morphological parameters were measured on this type of averaged beat.
Prosthetic rehabilitation result The result of the completed rehabilitation programme was classified according to the level of walking quality attained with a leg prosthesis. We distinguished three levels:
c l a s s 0 c l a s s I c l a s s 2
I 1 I 1
0.5 min
I It.0::b:o new, 54
Figure2 Typical example of averaged ECG beats (left CC5, right CM5 lead) presenting the morphological development of beat classes during exercise testing. Class: the class number; time: the time in minutes after the start of the test: New: the number of new beats incorporated in the class.
Level 1 : Completion of rehabilitation without any leg pros- thesis.
Level 2: Ability to walk with a leg prosthesis with the help of a walking frame. A radius of action of less than 40 m, and only suitable for walking indoors.
Level 3: Ability to walk with a leg prosthesis for more than 40 m, with or without the use of a walking stick or crutches. also outdoors.
Results
History, rest-ECG findings Past myocardial infarction documented by history and characteristic evolutionary changes on the rest ECG were observed in nine patients. Further cardiac problems included four cases of left ventricular hypertrophy, three of bundle-branch block, three of essential hypertension, four of atrial fibrillation, and one of mitral insufficiency. These cardiac problems were diagnosed in 2 1 of the 39 subjects. Thirteen patients were on digoxin therapy and eight patients used beta-blocking agents. This medication was continued during the test period.
Graded exercise test findings Of the 39 patients, two were unable to perform the test, that is they were unable to continue the rowing exercise at the initial load value of 30 W for more than Y2 min: one because of anaemia and the other because of polyneuropathy. The maximum performance in the exercise test in terms of
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
6/14
For
pers
onal
use
onl
y.

Ini. Rehahil. Med.. 1985, vol. 7, no. 3 -
16
14
12
10
a - 6 -
4 -
2 -
maximum work load and maximum heart rate are shown in the histograms of Fig. 3. The mean maximum work load was 63 W _+ 3.4 (SEM) and the mean maximum heart rate was 124 min-l f 3.6 (SEM). The shaded part of Figure 3 shows that an appreciable part of this group of patients had cardiac problems as indicated by history and rest ECG.
The mean of the increase in heart rate between rest and maximum was 43 min-l? 3.0 (SEM). This figure did not change when the subjects using beta-blocking agents were excluded. The mean slope of the increase of heart rate versus the increase in work load during exercise was 0.72 f 0.05 (SEM) min-I W-I.
n m +
Y
B
kl
L
0
5
t
- - r-
- -
- - -
o r
100 115 120 145 160 175
-+- Max. Heart Rate I min-’I - Max. Work Load (watt1
Figure3 Histograms of maximum performance during graded exercise testingofa group of 37 patientsas described. Shaded = past myocardial infarction, left ventricular hypertrophy, atrial fibrill- ation. or bundle branch block.
In fourteen patients ST-segment depressions of more than 1 mm horizontal or down-sloping were seen in the ECG at maximum work load, leading to early termination ofthe test in one patient. Of these patients five also showed a similar ST-segment depression at rest, previous to the exercise test. Digoxin therapy was used by eight of the fourteen patients, which made it uncertain whether the ST-depression was of ischaemic origin or not. In Fig. 4 these findings are specified in relation to maximum work load and maximum heart rate.
Ectopic beats were seen in three patients during exercise, in one patient the number being more than 10% ofall beats in a 30s period. Four patients had ectopic beats within 5 min after termination of the exercise with a maximum ranging from 8 to 12%. One patient showed ectopic beats during exercise, with a maximum of l6%, and after the exercise with a maximum of 13%, but also showed ventric- ular extrasystoles at rest. The presence of ectopic beats caused no early termination of the test.
-+- M o x . Heart Rate Imin-’I - Max. Work Load l w a t t l
K,A ST-segment depression a t rest &J on digoxin therapy
both
Figure4 Histogram of a group of 14 patients who had more than I mm ST-segment depression during maximum exercise, arranged in classes of maximum heart rate and maximum work load.
In the patients who terminated the exercise test this was in 59% of the cases due to general fatigue, in 18% to arm muscle fatigue, and in 23% to inability to maintain the rotational speed. No patient terminated the test because of chest pain. The individual test data in terms of maximum heart rate versus maximum work load are presented in Fig. 5. In this figure the patients who used digoxin or beta- blocking agents are indicated.
lE01 160 O 1 140 t 0
0 D no cardiac medicat ion m O D
o digoxin 1 0-blocking agent
bo th digoxin and P-blocking agent
I , y ; , , I
80
0 0 20 40 60 80 loo 120
--+ Max. Work Load (watt1
Figure5 Individual exercise test data. Patients who used digoxin or beta-blocking agents are indicated.
The maximum heart rate of our patient group could not be compared with values of normal subjects of the same age since no data of this age group are available. Therefore the equations of Calvert16 were used, which relate maximum heart rate with age in normal subjects from 16 to 62 years performing graded bicycle exercise:
fmax = a - b ’ A
wheref,,, is the maximum heart rate (min-I) and A is the age (years).
for males: a = 201 min-I, b= 0.6 min-I . year-I (standard error Offma, is 1 1 min-I).
b= 0.7 min-I year-’ (standard error off,,, is 12 min-I).
for females: a = 192 min-I,
Our patient group reached a mean value of 80% f 2.3 (SEM) of the predicted maximum heart rate, which is significantly lower than the value predicted for normal subjects (Student t-test, pt0.05). A histogram of the distribution of these percentages is shown in Fig. 6.
4 Percentage of Max Heart Rote predicted for age
Figure6 Histogram of the percentage of maximum heart rate in vascular leg amputees (achieved during rowing exercise) of the maximum heart rate predicted according to Calvert
96
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
6/14
For
pers
onal
use
onl
y.

VAN ALSTE et a/.; Exercise testing of leg amputees
Prosthetic rehabilitation result Of the bilateral leg amputees the prosthetic rehabilitation result of three of them was classified at level 1, one at level 2 , and one has not yet completed rehabilitation after 8 months of treatment.
The thirty-four unilateral leg amputees all completed their prosthetic rehabilitation. Two of them were classified at level I, one ofwhom suffered a cerebral vascular accident during the rehabilitation period, eleven at level 2, and the other twenty-one at level 3.
Relation between rehabilitation result and exercise test In Fig. 7 the results of the completed rehabilitation pro- grammes of unilateral amputees were classified in the three- level scale and arranged in histograms according to maxi- mum heart rate and maximum work load. Figure 7b shows that subjects who achieved a peak work load of more than 60 W all attained the highest rehabilitation level.
sx 1G y. ec 70 80 )90 - max work load l uo t t l
n mote
,emole
Figure7 Histograms ofthe number of unilateral amputees achiev- ing a specific level of prosthetic walking at the end of the rehabil- itation programme: 1 = no prosthesis, 2 = prosthesis with use indoors only, and 3 = prosthesis with use outdoors. The bars indi- cate the Icvel ofprosthetic walking and are arranged according to (a) the maximum heart rate and (b) the maximum work load achieved during the exercise testing at the start of the rehabilitation pro- gramme.
The mean performances or unilateral amputees during the exercise test were significantly different for the ten subjects who achieved prosthetic walking level 2 from those twenty-one who achieved level 3 (Student t-test, pt0.05). Their mean maximum heart rates were 1 13 * 7 (SEM) and 130 f 4 (SEM) min -I, respectively. Their mean maximum work loads were 44 k 3 (SEM) and 7 I ~t 4 (SEM) W, respec- tively.
Discussion
Cardiac problems are indeed common in elderly vascular leg amputees, as shown in this study. Although these find- ings are not compared with a normal group of the same age, the information is of importance because the amputees are initiating a programme of rehabilitation exercises known to provoke high heart rates.
More than half of the amputees had a history of myocar- dial infarction or an abnormal rest ECG. Half of the patients received digoxin and/or beta-blocking agents. Electrocar-
diography during exercise testing added previously unrec- ognized cardiac problems indicated by ST-segment depres- sion and the presence of aberrant beats. From these findings a cardiologist can determine a safe maximum heart rate for a specific patient while exercising, thus providing a guide- line for the physiotherapist.
Because of the subjectivity of the endpoint criterion of the test in patients who reached their maximum heart rate trouble-free, this may not be the maximum attainable.
From experiences of a pilot study in trained vascular leg amputees presented in Ref. 12 and the cardiac performance during exercise testing reported by Kavanagh a consider- ably greater number of ST-segment depressions and rhythm disturbances during exercise testing was expected. Prelimi- nary results obtained during repeated exercise testing in the course of the rehabilitation programme revealed a decrease in heart rate at rest and an increase of cardiac arrhyth- mias5.
The maximum work capacity as indicated by the mean maximum work load during rowing exercise was 63 W. This value seems low, indicating a poor physical condition. Com- parison with a normal group of a similar age, however, is lacking.
In spite of their poor cardiac and physical condition, of the thirty-four unilateral amputees all but two were able to walk with a leg prosthesis at the end of the rehabilitation programme. A global comparison between the initial exer- cise test findings and the rehabilitation results shows that patients with a maximum work capacity of more than 60 W achieved the ability to walk outdoors with a prosthesis. Thirty-eight per cent of the patients with a lower work capacity achieved the same rehabilitation level.
Rowing exercise with ECG recording is an applicable way of exercise testing in vascular leg amputees. It provides measures for the cardiac condition and physical work capac- ity. The findings can be used to advise heart-rate limits for rehabilitation exercises, preventing exercise-induced car- diac problems becoming dominant. A good performance during the initial exercise test indicated by a high maximum work load and a high maximum heart rate increases the chance of a good prosthetic rehabilitation result.
References
1 Poulssen MGN Verandering en verschuiving(in Dutch). Thesis 1979. Maastricht
2 Kavanagh T and Shephard RJ. The application of cxcrcisc testing to the elderly amputee. CMA J. 1973; 108: 314-317
3 Hamilton EA and Nichols PJR. Rehabilitation of the elderly lower-limb amputee. Br Mer/.J 1972; 2: 95-99
4 Peizer E. On the energy requirements for prosthesis usc by geriatric amputees. Nat. Academy of Sciences - Nat. Research Council. Conference on the geriatric amputee (Publ. 9 19). Washington, I96 1 ; 146- I 50
5 Cruts HEP, Alste JA van, Huisman K and Vries J de. Cardiac loads during prosthetic training in leg amputees. Proceedings 01‘ the eighth international symposium on external control of‘ human extremities, Dubrovnik, Yugoslavia, 1984; pp. 269- 280
6 Corcoran PJ. Energy expenditure during ambulation. P h p Basis Rehabrl Med 197 1 : 10: 185- 198
7 Erdman WJ, Hettinger Th and Saez F. Comparative work stress for above-knee amputees using artificial legs or crutches. Arrr .I Phys Med 1960; 39: 225-232
8 Nichols PJR Rehabilitation Medicine. The iClanu,q~tnetrt 41’ Physical Disabilities, chap. 1 I . The elderly amputee, Butter- worth, London. 1976: 228-253
9 Blomqvist CG. Use of exercise testing for diagnostic and func- tional evaluation of patients with atherosclerotic hear1 disease. Circulation 197 1 : 44: I 120
97
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
6/14
For
pers
onal
use
onl
y.

In t . Rehahil. Mtid., 1985, vol. 7, no. 3
I 0 Clausen JP. Circulatory adjustments to dynamic exercise and effect of physical training in normal subjects and patients with coronary artery disease. In: Sonnenblick, EH and Lesch M (eds.) Exercise and Jfca?t Diseuse. Grune & Stratton, New York, 1977, 39-75
I 1 Gobcl FL, Nordstrom, KA, Nelson RR, Jorgensen CR and Wang Y. The rate-pressure product as an index of myocardial oxygcn consumption during exercise in patients with angina pectoris. Circulation 1978; 57: 549-556
I2 Alste JA van. Haye MW la. Huisman K, Vries J de and Boom H BK. Exercise electrocardiography using rowing ergometry suitable for leg amputees. f n i Rehabil Med 1985; 7: 1-5
I 3 Ascoop CA, Distelbrink CA and Lang PA de. Clinical value of
quantitative analysis of ST-slope during exercise. Br tle(wt .I
I4 Alste JA van and Luursema ED. VIPER: a powerful tool for the real-time calculation of inner products for biomedical signal processing. Med Biol Eng Conlput 1985; 23: 74-76
15 AlstC JA van, Luursema ED, Cruts HEP and Herrmann OE. Beat-to-beat analysis of waveshape and rhythm in XECG using inner vector product hardware. IEEE C017?pU1~raF i n Curdio/o,qr, Seattle, 1982; 355 - 358
16 Calvert AF, Bernstein LB and Bailey IK. Physiological responses to maximal exercise in a normal Australian popula- tion - comparative values in patients with anatomically defined coronary artery disease. Ausfr N Z J Med 1977: I : 497-506
1977; 39: 212-217
-
_. Book reviews -
A text or a history?
Therapeutic Exrrcrse. 4th edition, by J. V. Basmajian. Williams & Wilkins, Baltimore. 622 pages, 161 illustrations. E31. ISBN 0- 683 -00434- 4.
‘I%erapwtic Excrcise is one volume of the Rehabilitation Medicine Library Series and was originally published as part of the Physical Medicine Library edited by Sidney Licht. The change ofname from Physical Medicine to Rehabilitation, which occurred to reflect a different attitude and scope in medical practice, is not reflected in this book. The 4th edition has grown very considerably in content since the 3rd edition. Growth in size would appear to have created editorial problems, so that no single area is dealt with in any depth and, as a result, there are serious omissions. The reviewer wonders for whom the text is written, as it would seem to fall between a number of stools and, at times, appears primarily to be a memento to a group of distinguished physicians. It is a pity that in a book entitled Therapeutic Exercise in a Rehabilitation Series there is so little input from the physiotherapist, especially at a time when an increasing number of therapists are carrying out original research and possess journalistic capability. The omissions on rehabilitation are serious in what is supposed to be a comprehensive text, and seem to have been made at the expense of long chapters on history and physiological principles which might be better published as a separate volume or volumes, where relevant anatomy and physiol- ogy could be dealt with in greater depth, I t is unfortunate that some sections are dealt with in the barest of outline, such as the chapter entitled ‘Exercise in pulmonary disease’. Though there are chapters on cerebral palsy, paraplegia, hemiplegia, multiple sclerosis, and lower motor neuron lesions, there is no chapter on Parkinson’s disease or any aspect of neurosurgery and head injury. There are no chapters on traumatology and scant alluding to orthopaedics, though the chapter on scoliosis by Caillet is of anticipated high quality. There is no content on geriatrics or gerontology as a specialty, no dermatology, no chapter on plastic surgery or burns, and so on. In principles of exercise the omission of a section on balance. for example, is both serious and puzzling.
Harris’s chapter on facilitation techniques gives a very compre- hensive overview ofa number oftechniques, includingP N F, Rood and Bobath. Wynn Parry’s short chapter on vicarious or trick movements is an excellent concise chapter dealing with this diffi- cult topic about which little is understood. He helps to emphasize and widen the appreciation of this subject. In the chapter on clinical
The science of multiple sclerosis
lrnmiinologicul and Clinical Aspects ofMultiple Sclerosis. Edited by R. E. Gonsette and P. Delmotte. MTP, Lancaster, f39.95. 492 pages, 105 illus., ISBN 0-85200-762-0.
This book contains a number of short papers, abstracts and descriptions of posters relating to the 25th anniversary symposium of the Belgian Research Group for MS. As such its coverage of the field is both repetitive and patchy with many contributions being of
assessment of joint motion, Moore gives a detailed account of measurement with a standard goniometer. However, such informa- tion has long been available in the booklet of the American Acad- emy of Orthopaedic Surgeons, Joint Motion, Method qf Measrrritig and Recording, and thus with limited space, other methods might have been described usefully in more detail. Similar comment could be made of Schram’s chapter on resistance exercise with no mention of myometers, MacQueen’s method or the Oxford scale. In their chapter on crutch and cane use, Hoberman and Basmajian spend valuable space describing methods of aid measurement. notoriously useful only as a starting point yet, in a text for students, give no mention to well-documented dangers of incorrect crutch size or to reasons for correct height. There is no mention of elbow crutches, gutter crutches, frames, tripods or other modifications. Hydrotherapy is almost dismissed, occupying 5 pages. one of which is taken up by pictures and diagrams. Approaches to treatment of cerebral palsy have changed and widened in the last decadc. yet there is no reference to therapists, such as Levitt or Finnie. Onc has become used to full and detailed references at the end of each chapter (243 for Chapter II), yet there are all too few from the late 1970s and early 1980s.
It is unfortunate to entitle a chapter ‘Therapeutic exercise for back pain’ and devote almost the entire section to TMS, at the expense of other definitive diagnoses. Most of the chapters devoted to specific pathologies have suffered from the editorial hand, so that only the briefest of discussion and treatment method can be given. In some chapters the situation has been devised by giving details of non-specific tables of exercise; these tend to be taken as sacrosanct by the less able student. Having been somewhat critical, there are. nevertheless, excellent and welcome chapters: Biofeedback; Excr- cise in peripheral vascular disease (rarely granted space): Exercise in coronary artery disease; Brief isometric exercise, and Gait and gait retraining.
In a way the book is a memento to the work of people such as Licht and Basmajian, who have done so much to bring the attention of the public and the medical profession to the importance of rehabilitation, physiotherapy, and other allied medical professions. Such has been the expansion of the field that the days of being able to produce an all-encompassing single volume have passed. I t would be difficult to recommend this book as a “bible” Ibr all therapists, though no doubt it will find its place on the refcrence library shelf. PAUL S. WAGSTAFF
rather dubious standard while others are of considerable scientific interest. This format is really unsuitable as a reference work either in clinical or scientific studies of MS, as important scientific and clinical advances are bound to be published with more detail and i n a more authoritative form elsewhere. Publications of this kind are really little more than a souvenir for those who attendcd thc meeting and I do not think that the price of the book would recommend it to other readers. D.L. MCLELLAN
98
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Frei
e U
nive
rsita
et B
erlin
on
11/0
6/14
For
pers
onal
use
onl
y.
Recommended