EXAMINATION OF THE EYES
WHY TO EXAMINE EYES?
Eye tests are important for the detection of many common eye infections and diseases.
Eyes are also an important indicator to detect chronic systemic diseases like Hypertension and Diabetes.
Must after maxillofacial trauma to rule out any near and late complications emerging for the eyes.
APPROACHES TO EYE EXAMINATIONThere are two perspectives for examining
the eyes :
1. Ophthalmic Perspective – because eyes are prone to many infections, diseases and conditions.
2. Maxillofacial Perspective – because the eyes and the orbit forms an integral component of facial and mid-facial fractures and trauma.
OCULAR TRAUMA Blunt ocular trauma can cause both
structural and functional damage to the eyes.
Ocular trauma should reveal all the SEVEN CLASSIC RINGS of eye injuries. The eye examination should focus on these signs.
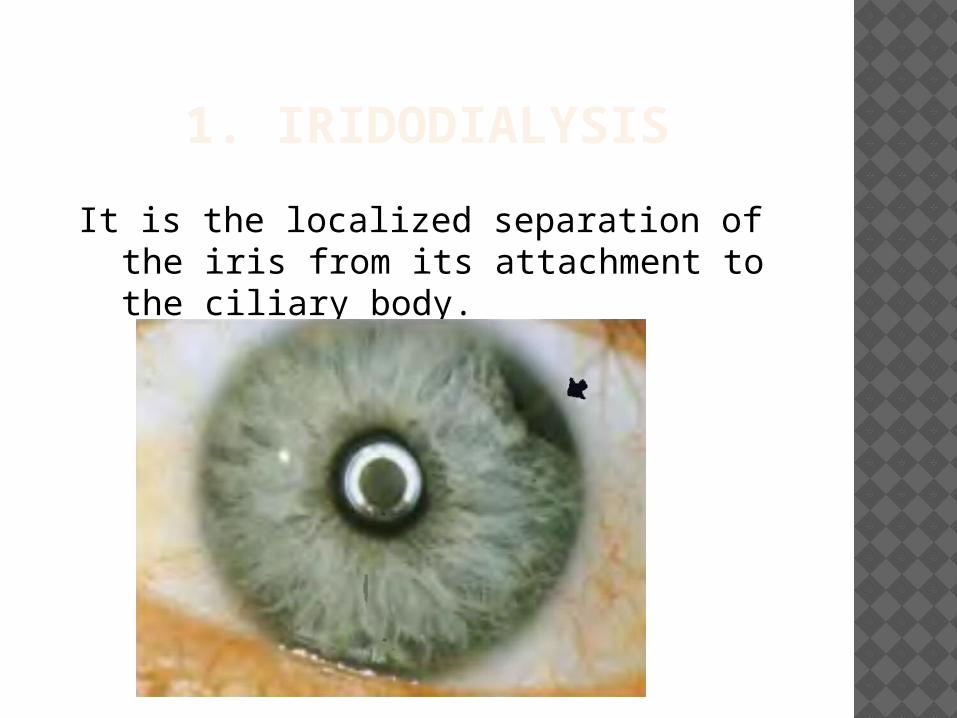
1. IRIDODIALYSIS
It is the localized separation of the iris from its attachment to the ciliary body.
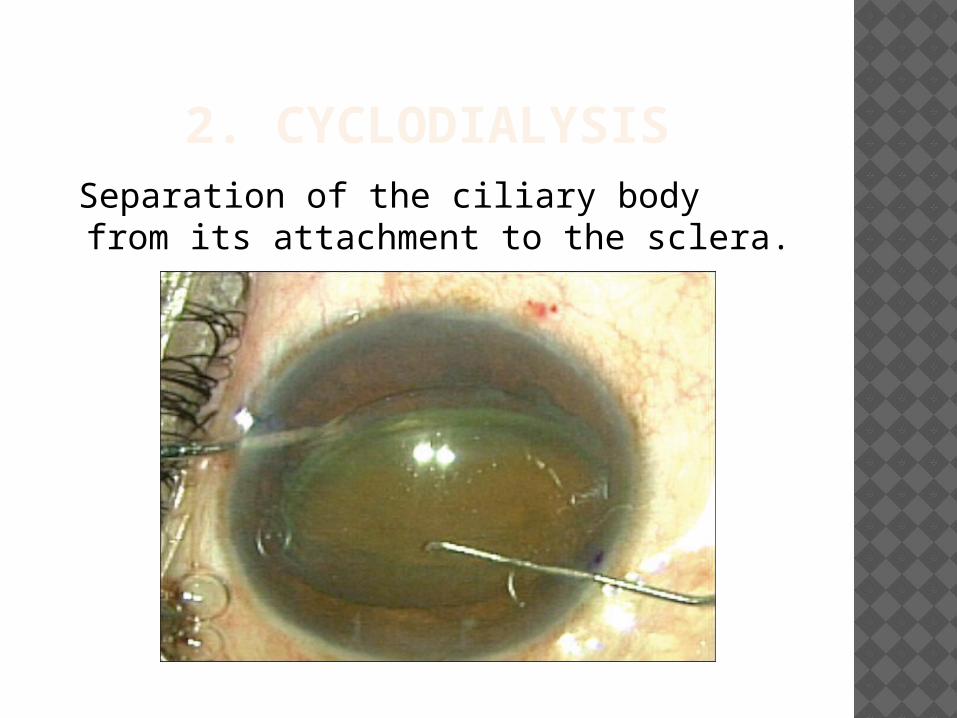
2. CYCLODIALYSIS Separation of the ciliary body from its
attachment to the sclera.
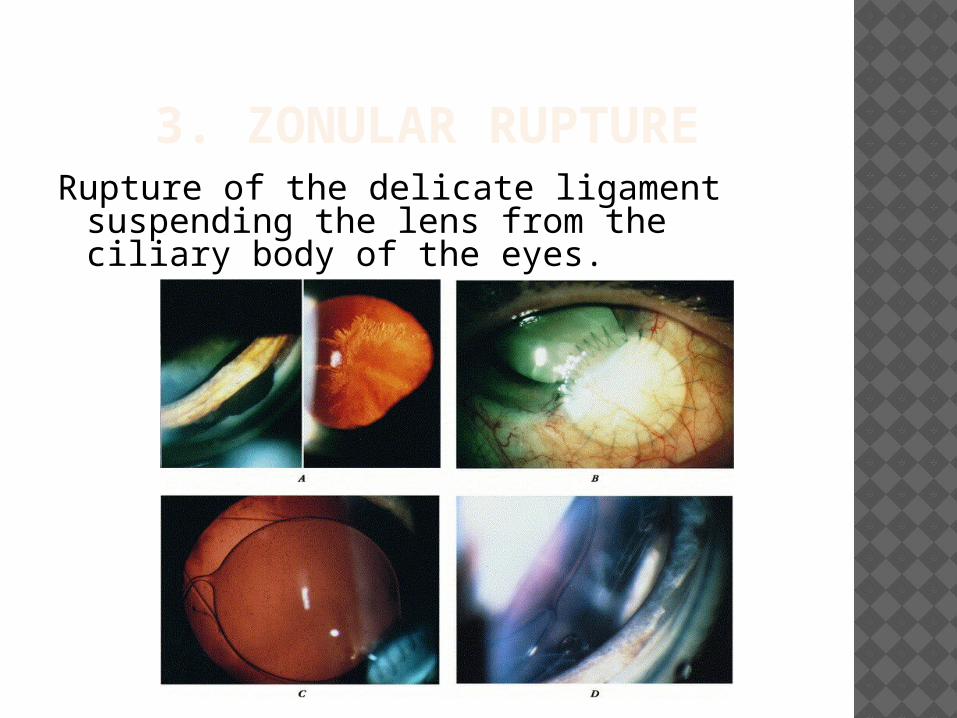
3. ZONULAR RUPTURERupture of the delicate ligament
suspending the lens from the ciliary body of the eyes.
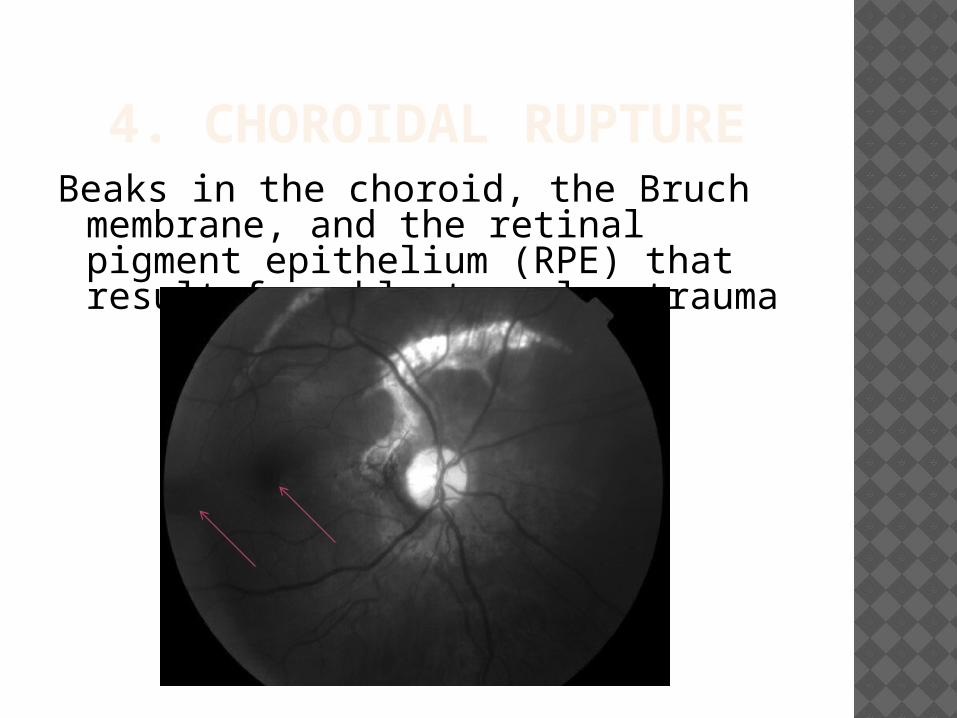
4. CHOROIDAL RUPTUREBeaks in the choroid, the Bruch
membrane, and the retinal pigment epithelium (RPE) that result from blunt ocular trauma
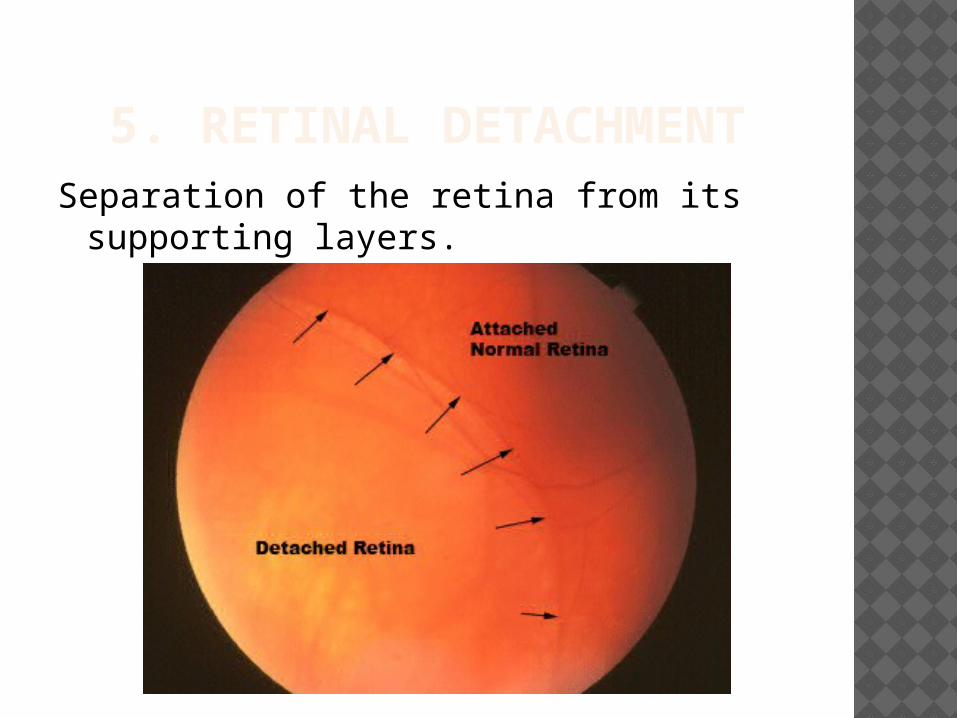
5. RETINAL DETACHMENTSeparation of the retina from its
supporting layers.
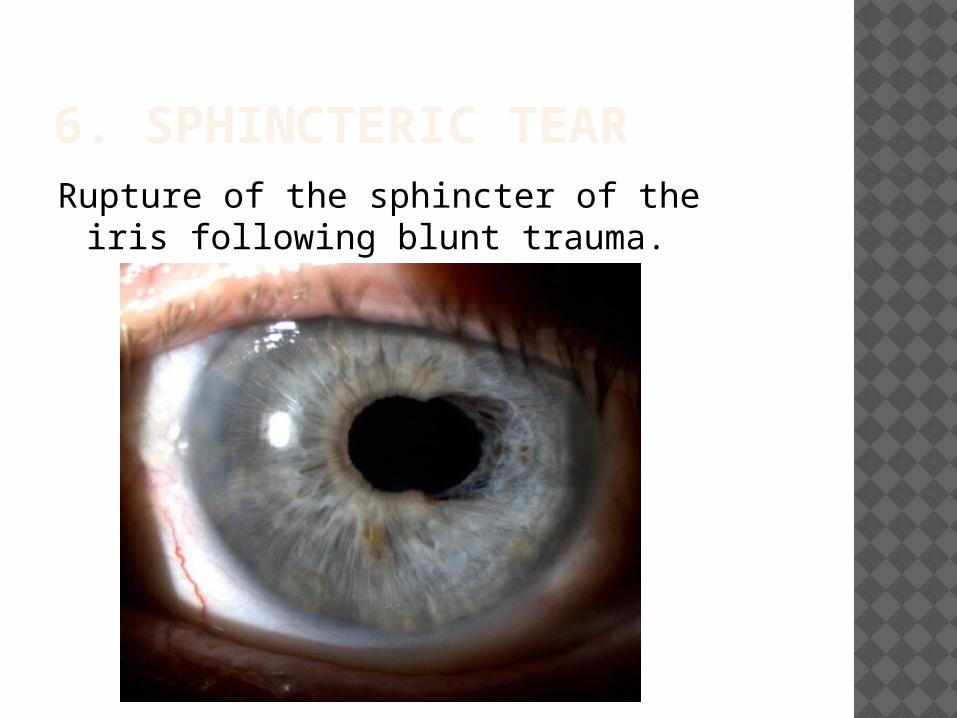
6. SPHINCTERIC TEARRupture of the sphincter of the iris
following blunt trauma.
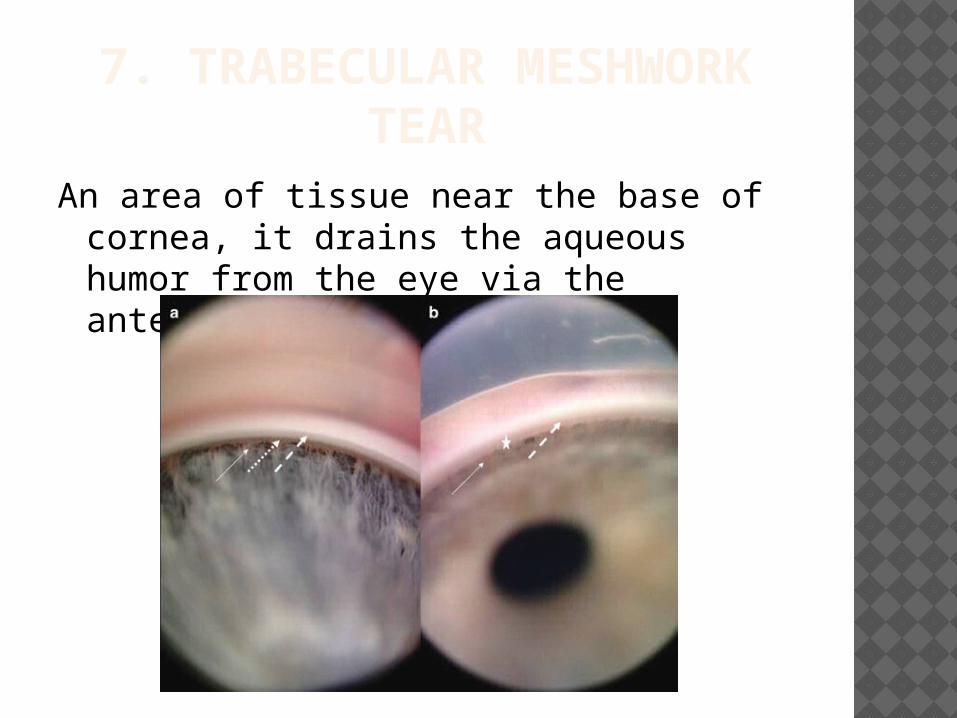
7. TRABECULAR MESHWORK TEAR
An area of tissue near the base of cornea, it drains the aqueous humor from the eye via the anterior chamber.
IMMEDIATE GOALS FOLLOWING OCULAR TRAUMA Protection of intact portions of the visual
system and avoidance of any further injury to the undamaged portions.
Accurate assessment of the extent of injury.
Institution of therapeutic measures that first achieve optimal function, and secondarily achieve optimal cosmetic results.
FREQUENCY AND INCIDENCE OF OCULAR TRAUMA
A few studies have been done to assess the frequency and incidence of ocular trauma.
1. Frequency and characteristics of ocular trauma in an urban population–Wilson, Wooten, and Williams
(Journal of the national medical association, Vol. 83, NO. 8,1991).
The brief findings of this study were : The study was a prospective analysis of 514
consecutive patients with direct ocular trauma. Males ( 3.5%) outnumbered the Females ( 1%). Bilateral injuries were encountered in 35 (27.6%)
The most common etiologic reasons were –Blunt Objects, Sharp Objects, Chemical, Radiation.
The factors associated with visual impairments were – poor initial visual acuity, Hyphema, Optic nerve trauma, retinal detachment and vitreous haemorrhage.
35 (27.6%) had bilateral injuries. One hundred sixty eyes were involved; 40 (25%) injuries were to the right eye only and 50 (31.37%) were to the left eye only.
2. Study of ocular trauma in an urban slum population in Delhi – Vats, Murthy, Chandra, Gupta and Gogoi.
(Indian Journal of Ophthalmology, Vol.56, Aug 2008 )
The study which was done in a slum, 163 episodes of ocular trauma were reported by 158 participants.
Mean age of trauma was 24.2 years. Males were significantly more affected
than females. Blunt Trauma was the commonest mode
of injury (41.7%). Blindness resulted in 11.4% of injured
eyes. A significant association was noted
between ocular trauma and workplace ( 43.80%).
TYPES OF EYE INJURIES1.Closed Globe injury / Non Penetrating
Trauma2. Penetrating Trauma3. Perforating Trauma
4. Blow-Out Fracture of the Orbit
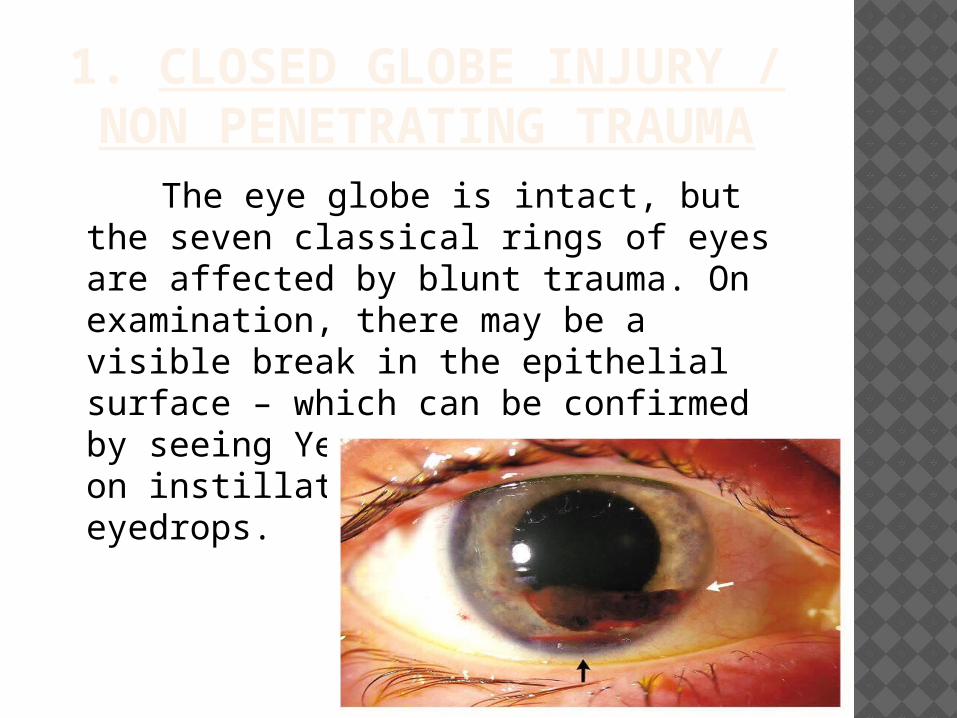
1. CLOSED GLOBE INJURY / NON PENETRATING TRAUMA The eye globe is intact, but the seven
classical rings of eyes are affected by blunt trauma. On examination, there may be a visible break in the epithelial surface – which can be confirmed by seeing Yellowish-Green staining on instillation of Flourescein eyedrops.
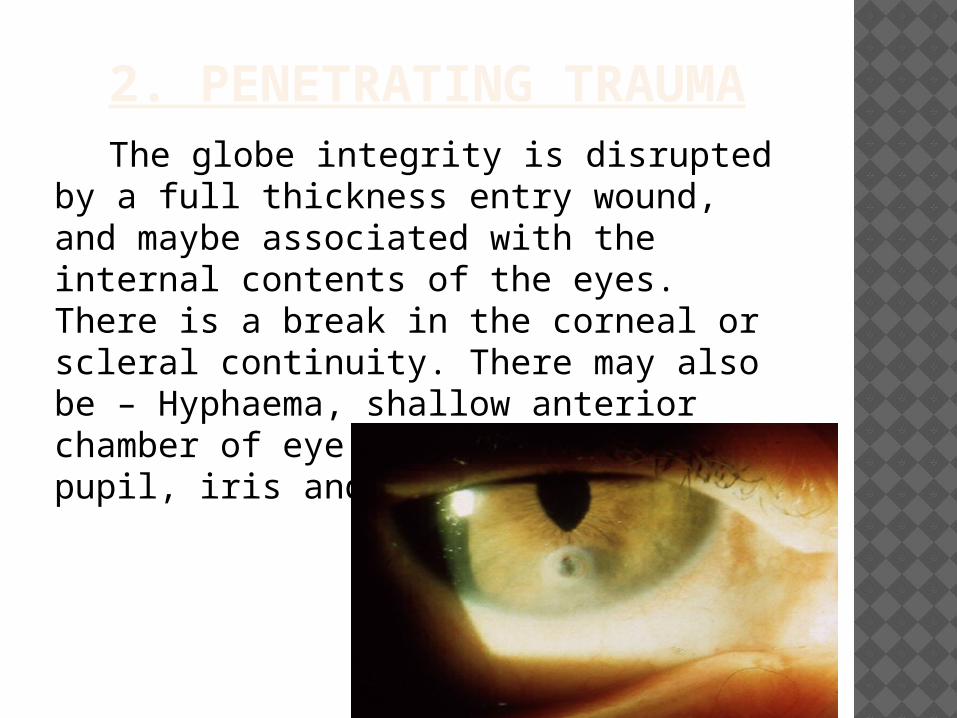
2. PENETRATING TRAUMA The globe integrity is disrupted by a full
thickness entry wound, and maybe associated with the internal contents of the eyes. There is a break in the corneal or scleral continuity. There may also be – Hyphaema, shallow anterior chamber of eye, distortion of pupil, iris and lens damage.
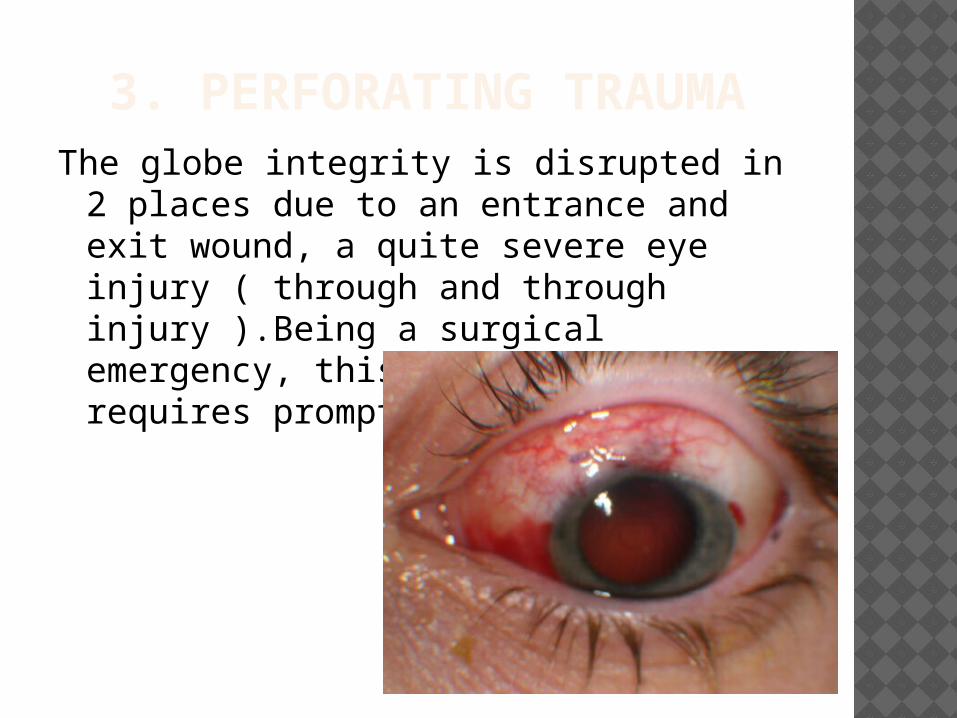
3. PERFORATING TRAUMAThe globe integrity is disrupted in 2
places due to an entrance and exit wound, a quite severe eye injury ( through and through injury ).Being a surgical emergency, this type of trauma requires prompt referral.
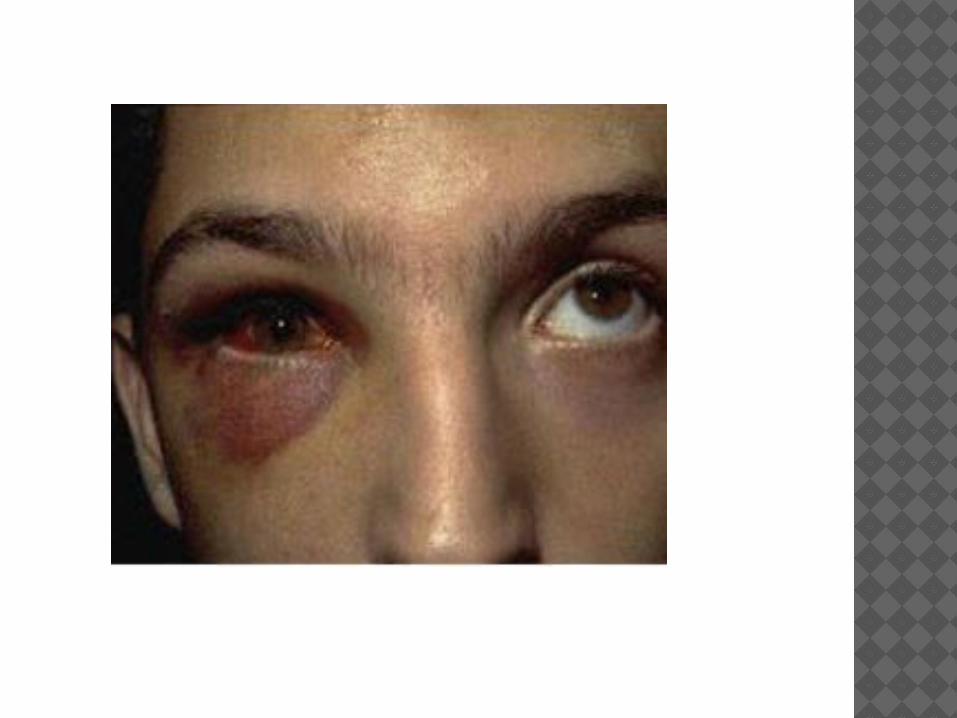
4. BLOW-OUT FRACTURE OF THE ORBIT
This is caused by blunt trauma, leading to fracture of the floor or medial wall of the orbit – due to sudden increased pressure on orbital contents and rise in infra-orbital pressure. The patient may have – periocular ecchymosis and edema, subcutaneous emphysema, decreased ocular mobility, enophthalmus, anaesthesia of cheek, diplopia, hyphaema and subconjunctival haemorrhage.
CLINICAL FEATURES IN OCULAR TRAUMA
The clinical features of eye injuries vary with type and severity of trauma, ranging from irritating pain to traumatic destruction of the globe.
1. Swelling of the eyelids and conjunctiva – can produce temporary vision impairment.
2. Damage to the cornea – swelling of the corneal tissues, can be present with hyphaema.
3. Damage to the sclera – can be non-penetrating, penetrating, perforating or blow-out.
4. Damage to iris and supporting structures- can cause Miosis and Mydriasis. Iridodialysis can give the appearance of a secondary pupil. It can also cause Photophobia and blurred vision.
5. Lens damage - can cause Cataract formation or total dislocation.
6. Retinal damage – can cause damage to the Choroid and hemorrhage into the Vitreous Humor.
7. Optic nerve injury – can cause partial to total vision impairment.
8. Damage to external muscles of eyes – results in diplopia and reduced eye movement.
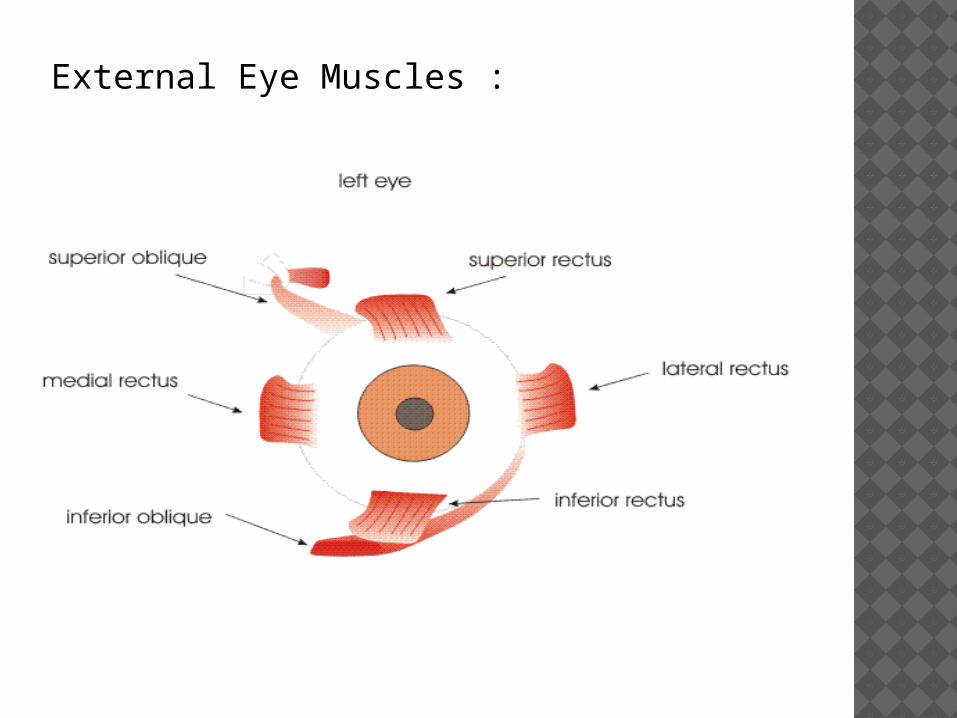
External Eye Muscles :
9. Damage to Ophthalmic and Maxillary divisions of Trigeminal Nerve – impairs sensations in the eyelids, the conjunctiva and cornea.
10. Damage to Lacrimal Gland – impairs production of tears.
11. Damage to Infra-orbital blood vessels and nerve – may result in substantial displacement and distortion of the eyes.
EXAMINATION OF EYE INJURIES
Clinical Assessment
History of Injury
External examination of eye
Ocular surface examination
Orbital examination
Examination for Visual Field
Pupil examination
CLINICAL ASSESSMENTThe aim in assessing the patient with eye
trauma is to determine : What the injury is ? Identify associated injuries ? Identify factors that could potentially
make it worse ? Decide whether it can be managed by
yourself or whether it needs referring after first treatment is administered ?
HISTORY OF INJURY Time of injury ? Nature of injury – - physical v/s chemical - blunt v/s penetrating - speed of impact
Possible entrance of any foreign body ? Previous acuity, eye problems and medical
history ? Circumstances of the injury – important for
medico legal considerations.
VISUAL ACUITY Before the external examination of eye is
started, the visual acuities in both eyes should be checked.
Usually, this involves the use of the Snellen eye chart. During a maxillofacial examination in a dental clinic, it may not be possible to use this chart.
An alternative is – by simply asking the patient to identify an item you hold up, like your watch or pen.
A 20/20 score or a 6/6 vision indicates clearness of vision.
EXTERNAL EXAMINATION OF EYE
1. Examination of Orbit and Eyelids - eyelid is evaluated for excessive skin, herniated orbital fat, abnormal eyelid creases, ptosis, retraction, and prolapse of the lacrimal gland.
Look for lacerations, bruising and oedema.
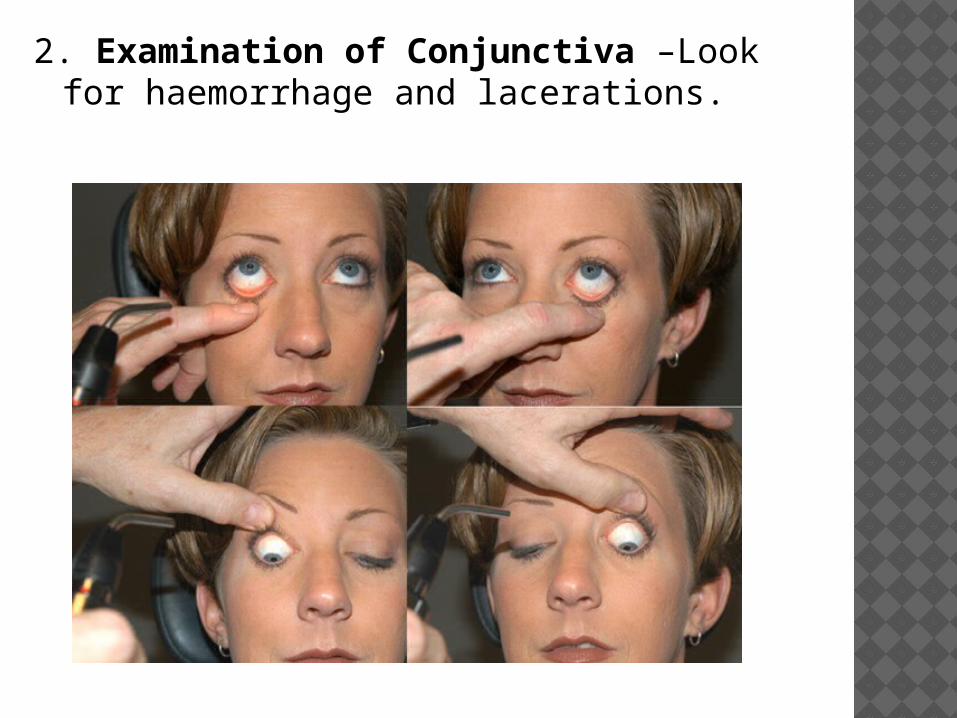
2. Examination of Conjunctiva –Look for haemorrhage and lacerations.

3. Examination of Cornea –Look for corneal abrasions using Slit Lamp technique.
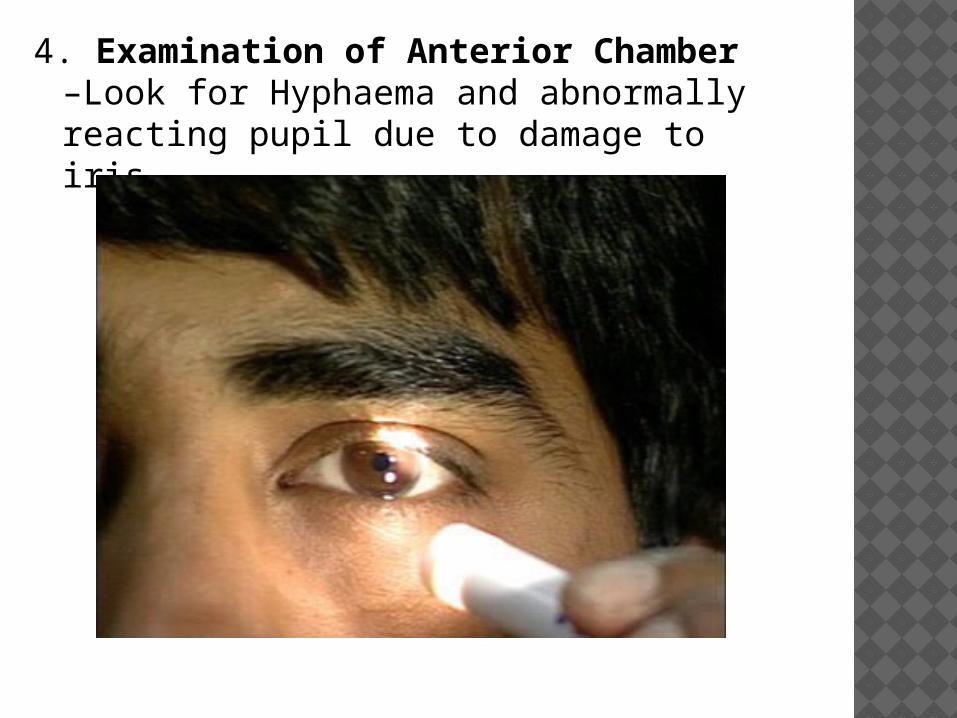
4. Examination of Anterior Chamber –Look for Hyphaema and abnormally reacting pupil due to damage to iris.
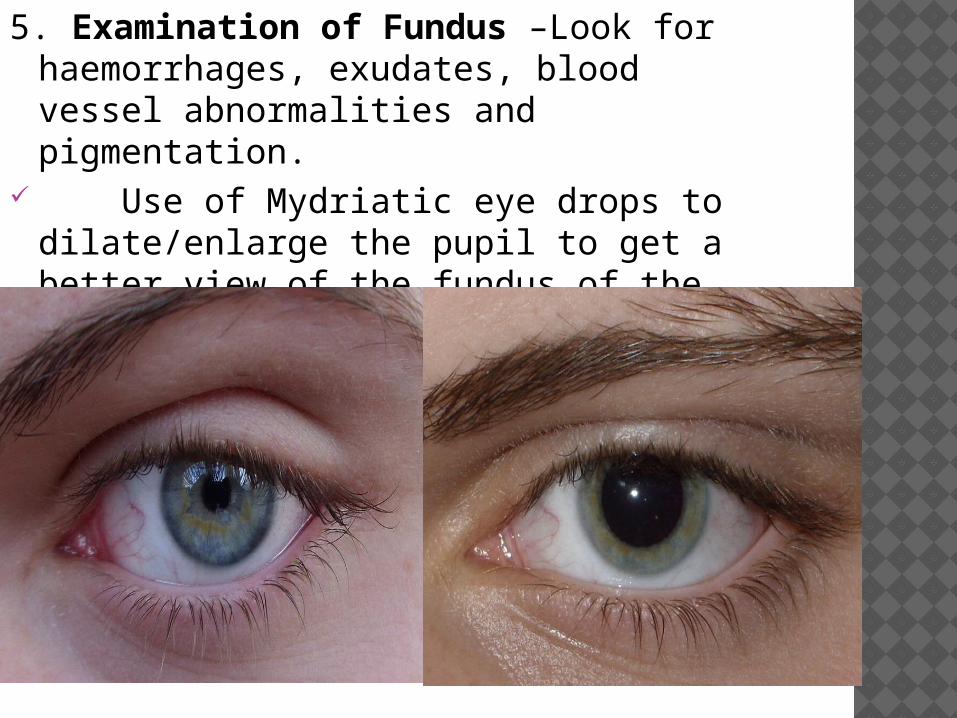
5. Examination of Fundus –Look for haemorrhages, exudates, blood vessel abnormalities and pigmentation.
Use of Mydriatic eye drops to dilate/enlarge the pupil to get a better view of the fundus of the eye.
OCULAR SURFACE EXAMINATION
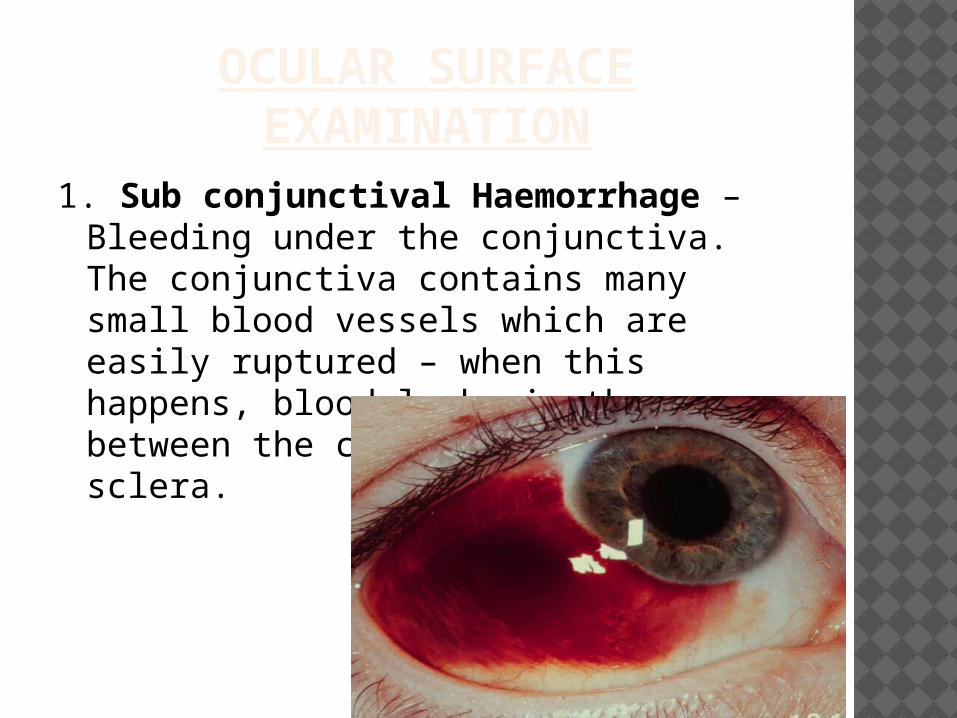
1. Sub conjunctival Haemorrhage – Bleeding under the conjunctiva. The conjunctiva contains many small blood vessels which are easily ruptured – when this happens, blood leaks in the space between the conjunctiva and sclera.
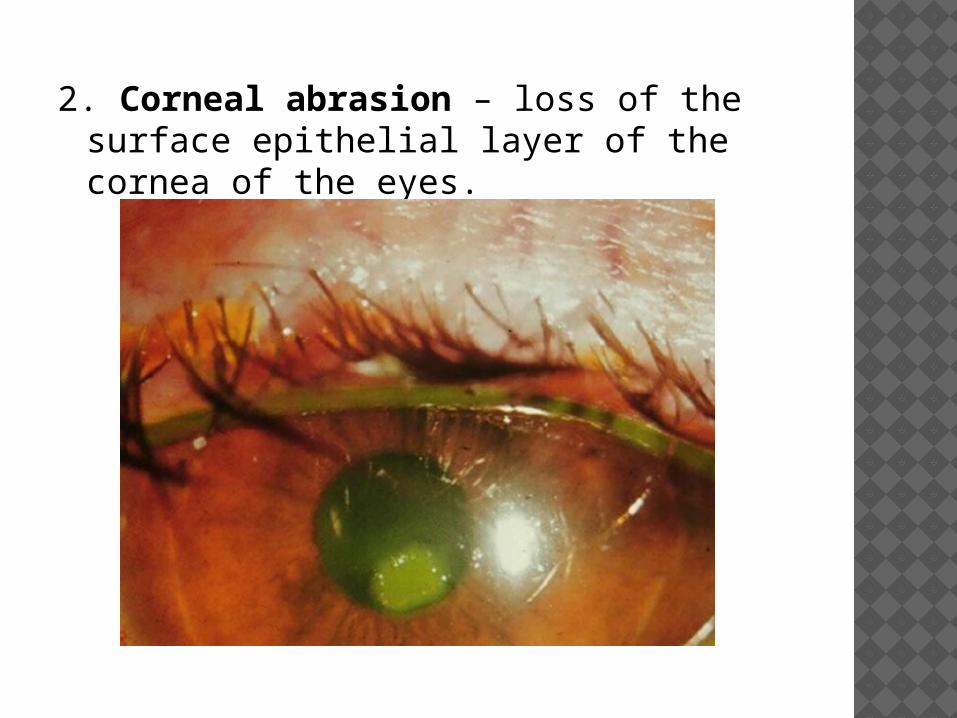
2. Corneal abrasion – loss of the surface epithelial layer of the cornea of the eyes.
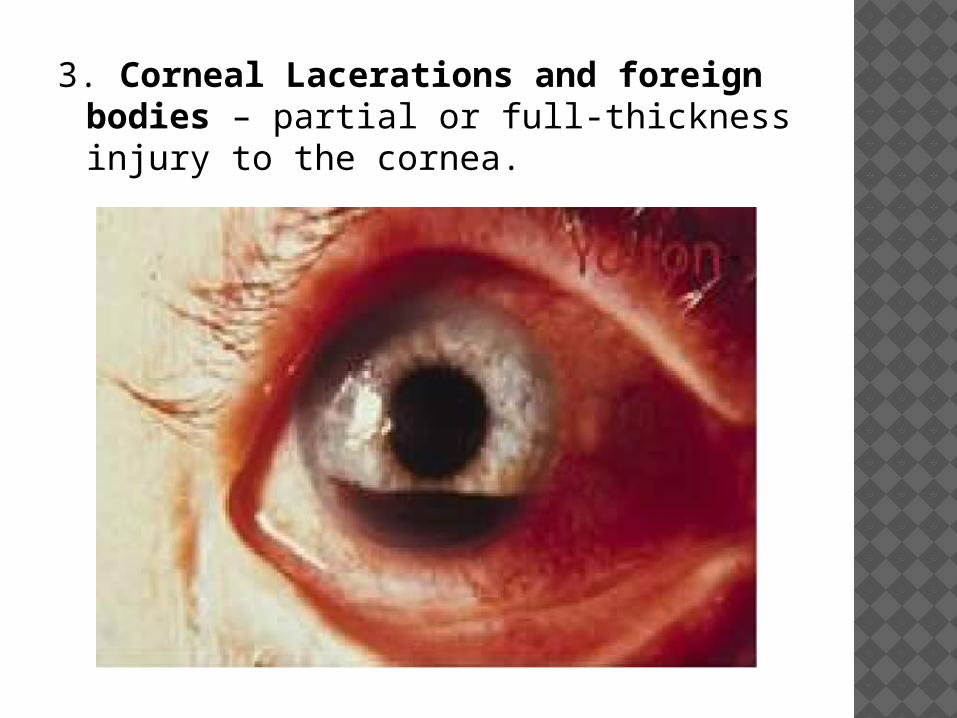
3. Corneal Lacerations and foreign bodies – partial or full-thickness injury to the cornea.
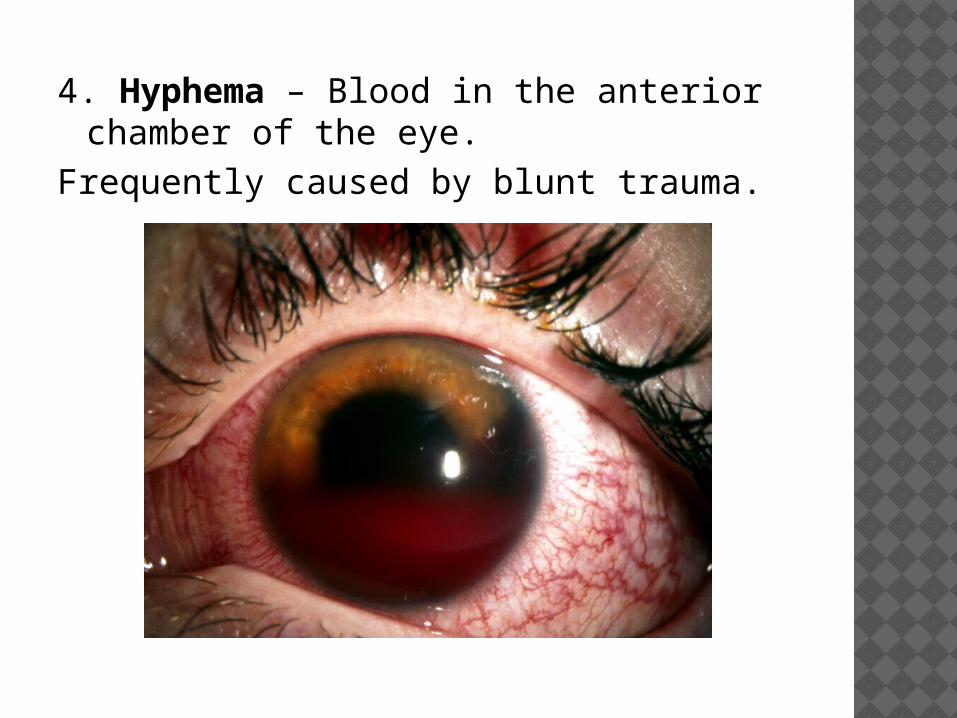
4. Hyphema – Blood in the anterior chamber of the eye.
Frequently caused by blunt trauma.
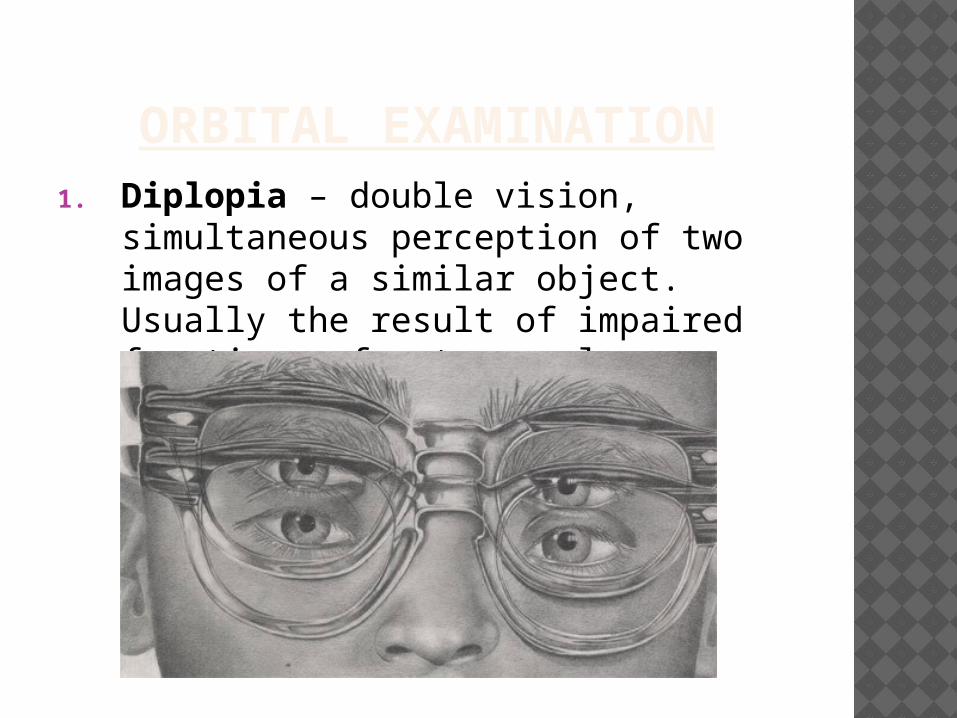
ORBITAL EXAMINATION1. Diplopia – double vision,
simultaneous perception of two images of a similar object. Usually the result of impaired functions of extra ocular muscles.
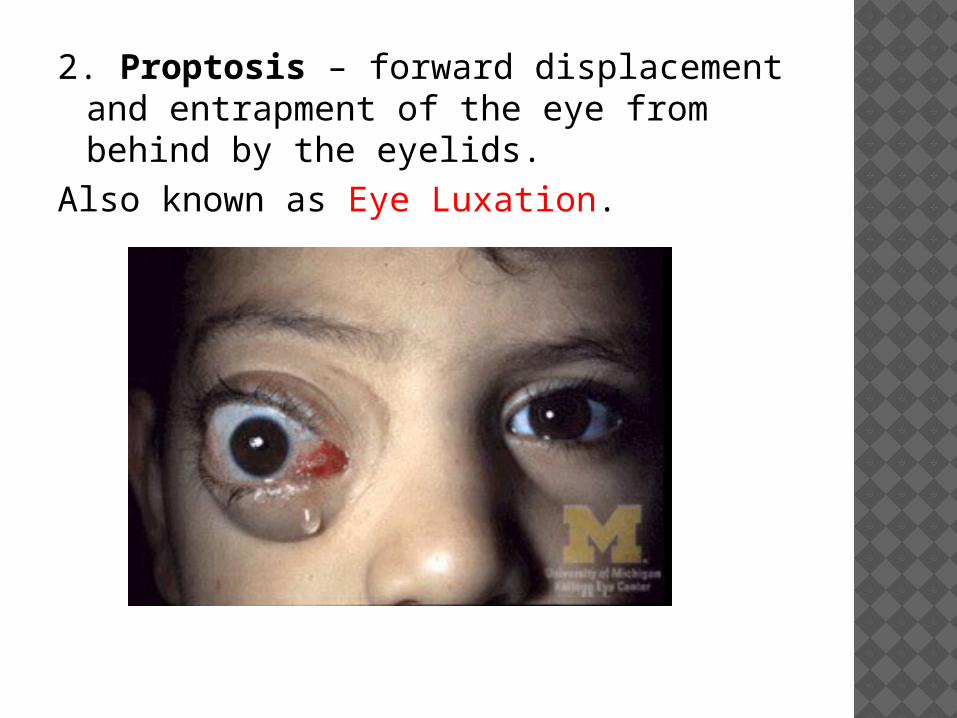
2. Proptosis – forward displacement and entrapment of the eye from behind by the eyelids.
Also known as Eye Luxation.
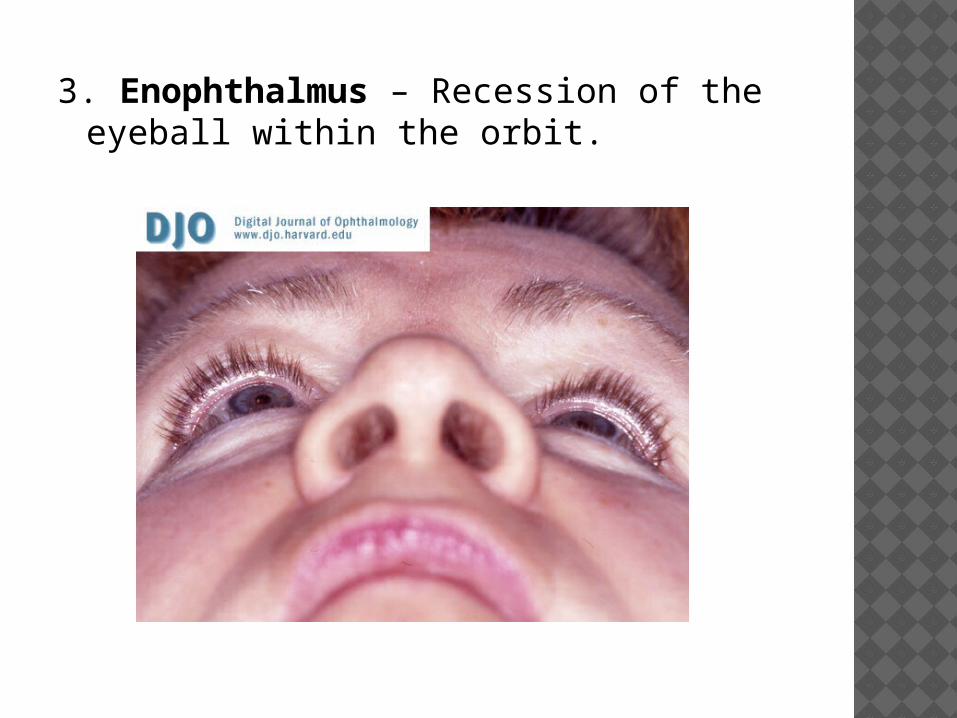
3. Enophthalmus – Recession of the eyeball within the orbit.
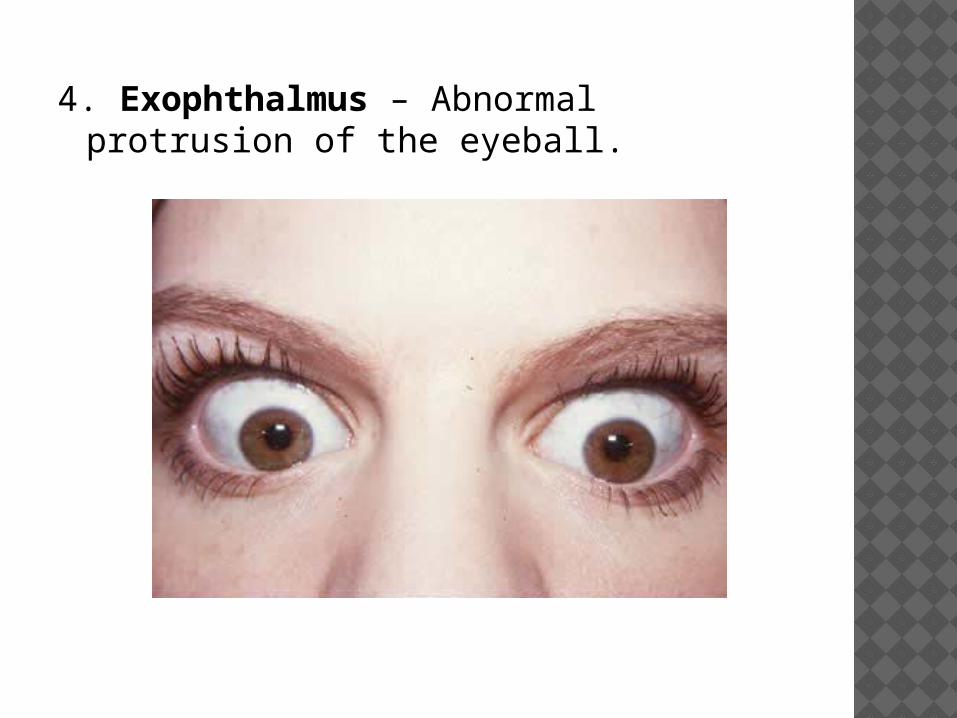
4. Exophthalmus – Abnormal protrusion of the eyeball.
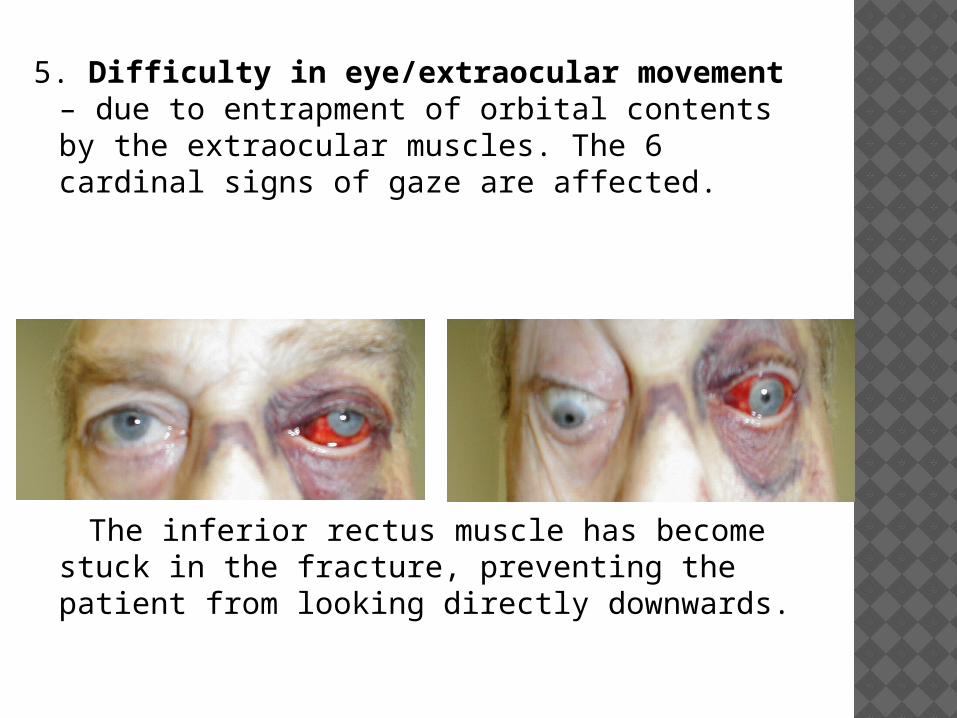
5. Difficulty in eye/extraocular movement – due to entrapment of orbital contents by the extraocular muscles. The 6 cardinal signs of gaze are affected.
The inferior rectus muscle has become stuck in the fracture, preventing the patient from looking directly downwards.
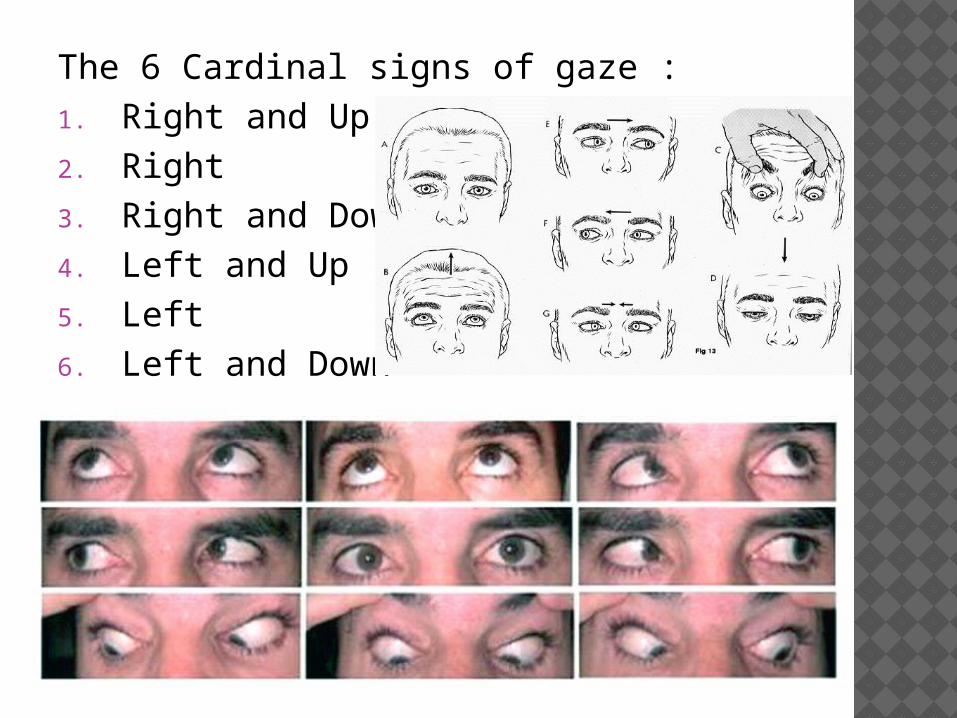
The 6 Cardinal signs of gaze : 1. Right and Up2. Right3. Right and Down4. Left and Up5. Left6. Left and Down
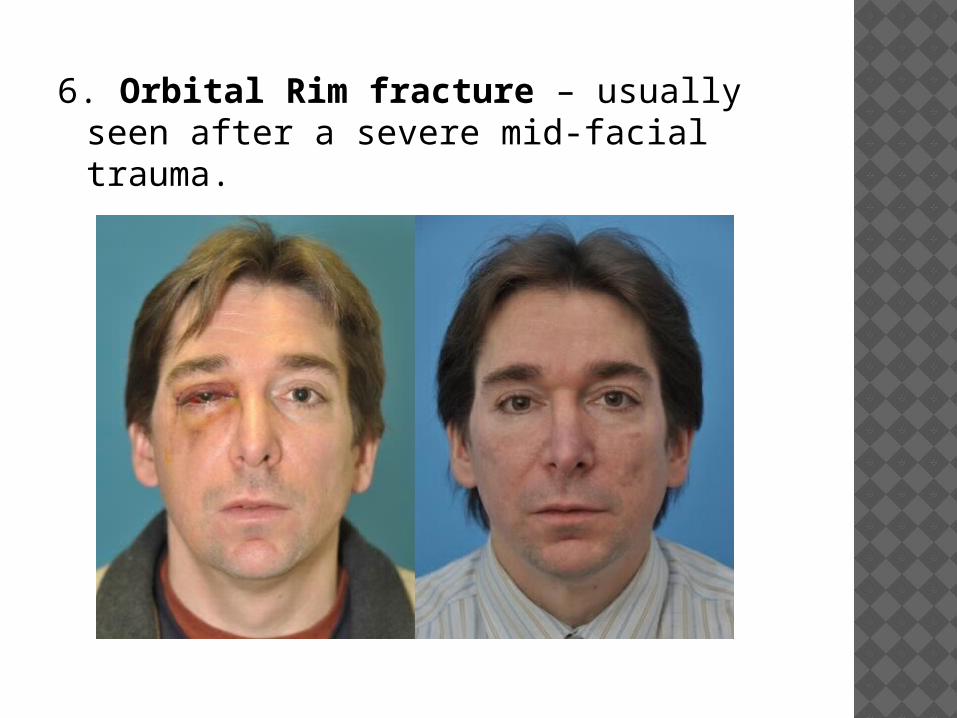
6. Orbital Rim fracture – usually seen after a severe mid-facial trauma.
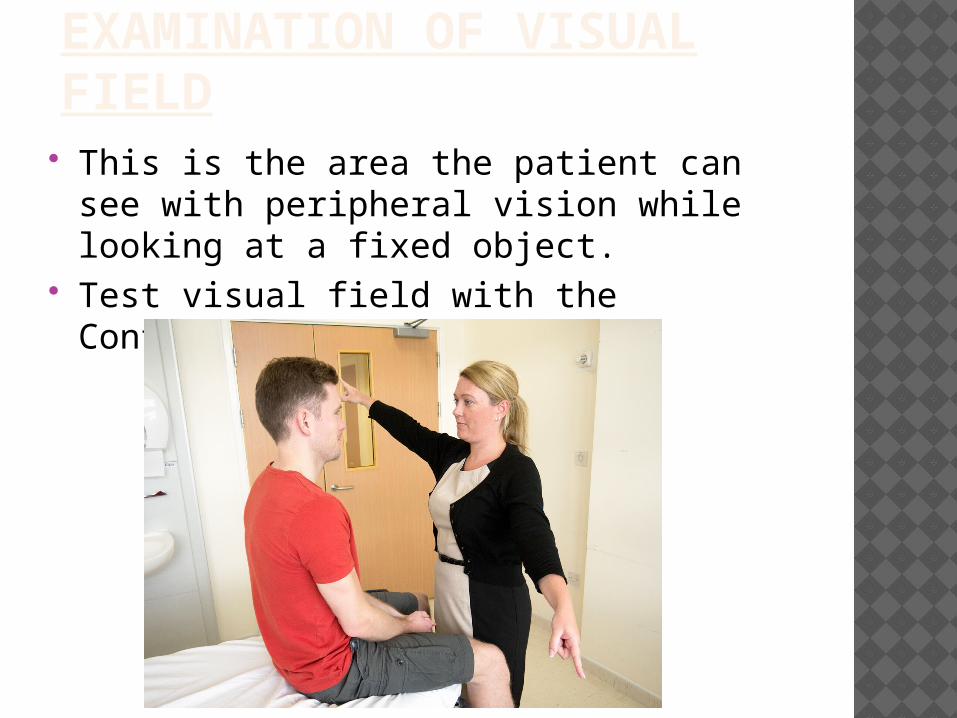
EXAMINATION OF VISUAL FIELD
This is the area the patient can see with peripheral vision while looking at a fixed object.
Test visual field with the Confrontation Test.
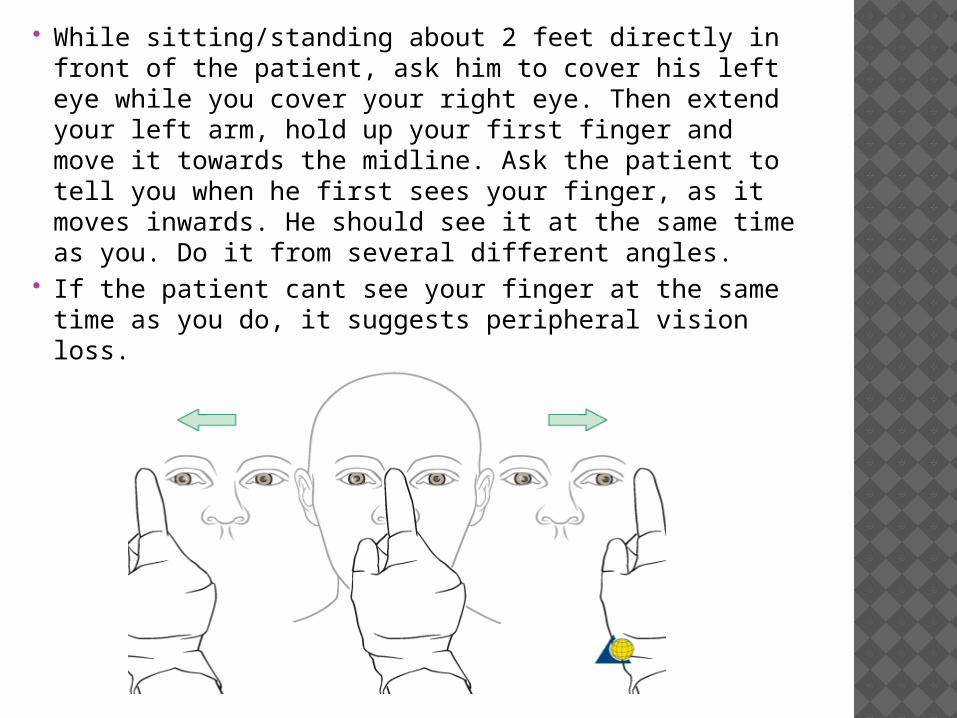
While sitting/standing about 2 feet directly in front of the patient, ask him to cover his left eye while you cover your right eye. Then extend your left arm, hold up your first finger and move it towards the midline. Ask the patient to tell you when he first sees your finger, as it moves inwards. He should see it at the same time as you. Do it from several different angles.
If the patient cant see your finger at the same time as you do, it suggests peripheral vision loss.
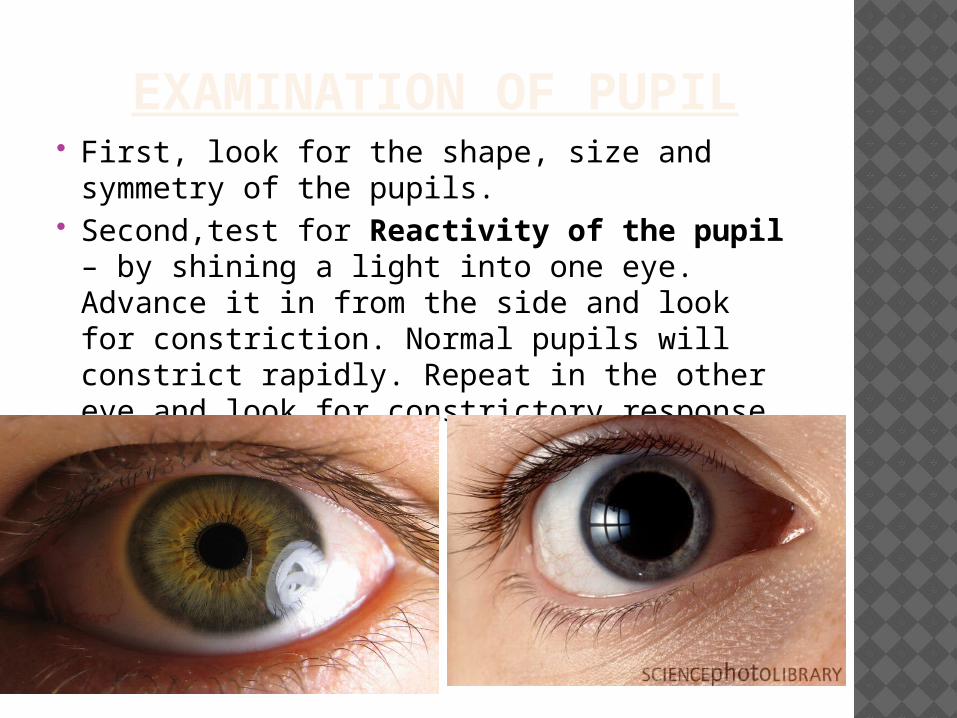
EXAMINATION OF PUPIL First, look for the shape, size and symmetry
of the pupils. Second,test for Reactivity of the pupil –
by shining a light into one eye. Advance it in from the side and look for constriction. Normal pupils will constrict rapidly. Repeat in the other eye and look for constrictory response.
Third, test for Accommodation. Ask the patient to focus on a distant object, and then on your finger – as you move it from a distance to the bridge of his nose. When he focuses on the distant object, his pupils should dilate, but as he focuses on the closer object, they should constrict.
Lastly, check for the Ocular muscle response. Have the patient follow your finger in a H pattern. Normal eye movements should be conjugate, or together and smooth. Jerky eye movements (Nystagmus) maybe indicative of other conditions. These tests the 6 cardinal fields of gaze.
THANK YOUSanchit Goyal
PG Trainee OMFS
Recommended



![EYES : Meningitis, eyes, inflamed, wild, staring, pupils ...homoeopathybooks.com/Repertory of Concomitant... · Difficult, breathing, closing, eyes, on : Carb-v., Carb-an. EYES :[CONSTITUTION]](https://img.pdfslide.us/doc/110x75/5a9a0bd77f8b9aba4a8d6b57/eyes-meningitis-eyes-inflamed-wild-staring-pupils-of-concomitantdifficult.jpg)