Histology Pattern Recognition Software in Investigative Pathology
J. Webster, DVM, PhD, DACVP Laboratory of Cancer Biology and Genetics
National Cancer Institute, Bethesda, MD
Pathology Visions 2011 November 1, 2011

Outline
• Introduction – Pattern recognition image analysis
• Evaluation of pattern recognition image analysis – Tissue feature quantification
– Segmentation of morphologically complex tissues
– Observations and personal experiences
• Applications and Integration
• Conclusions
Whole Slide Digital Imaging: Revolutionary Transformation in Pathology
• Diagnostic pathology – Enhanced telepathology – Real-time consultations
• Education – Specimen preservation – Uniform lesion display – Conferencing
• Investigative pathology – Quantitative morphometric image analysis
Morphometric Image Analysis
• Quantify immunohistochemical reactions
• Quantify histochemical stains
• Quantify tissue feature areas
• Identify regions of interest
• Screen for histologic lesions
Morphometric Image Analysis
• Advantages – Increased data acquisition – Decreased subjectivity – Decreased observer variability – Whole-slide image analysis
• Limitations – Few well-developed protocols for applications – Sensitivity to processing and handling – Two-dimensional analysis
Pattern Recognition Image Analysis
• Advantages – Improved analysis throughput – Reproducible, quantitative analysis – Decreased intra-/ inter-observer bias
• Specific Applications – Quantifying metastatic lesions
• Pre-clinical therapeutic models • Tumor transplantation models
– Identifying regions of Interest • Immunohistochemistry quantification
– Diagnostic screening
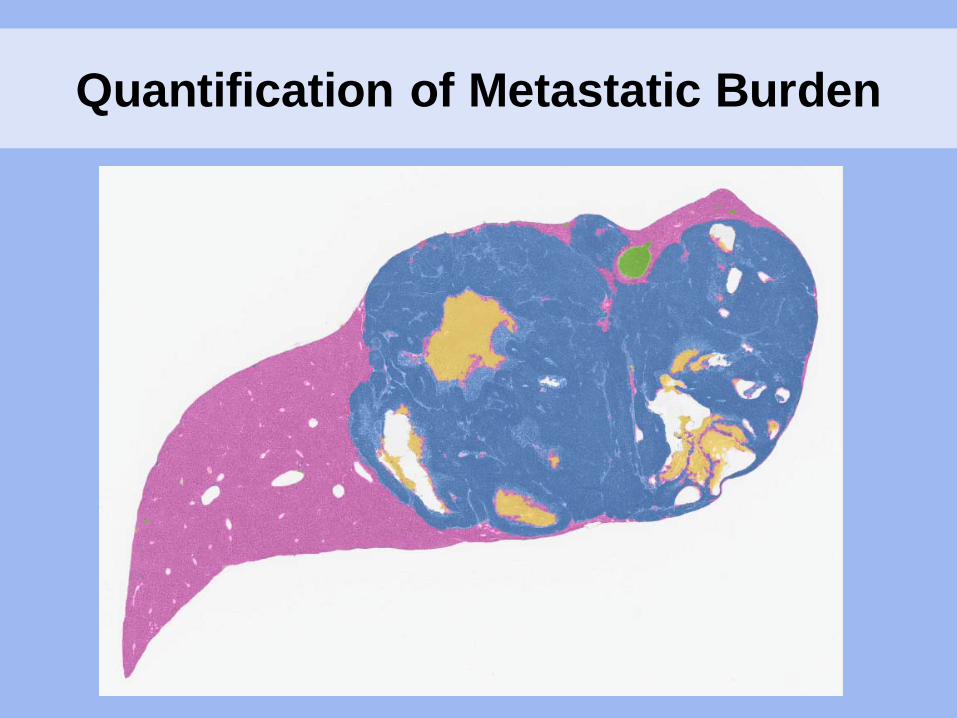
Quantification of Metastatic Burden
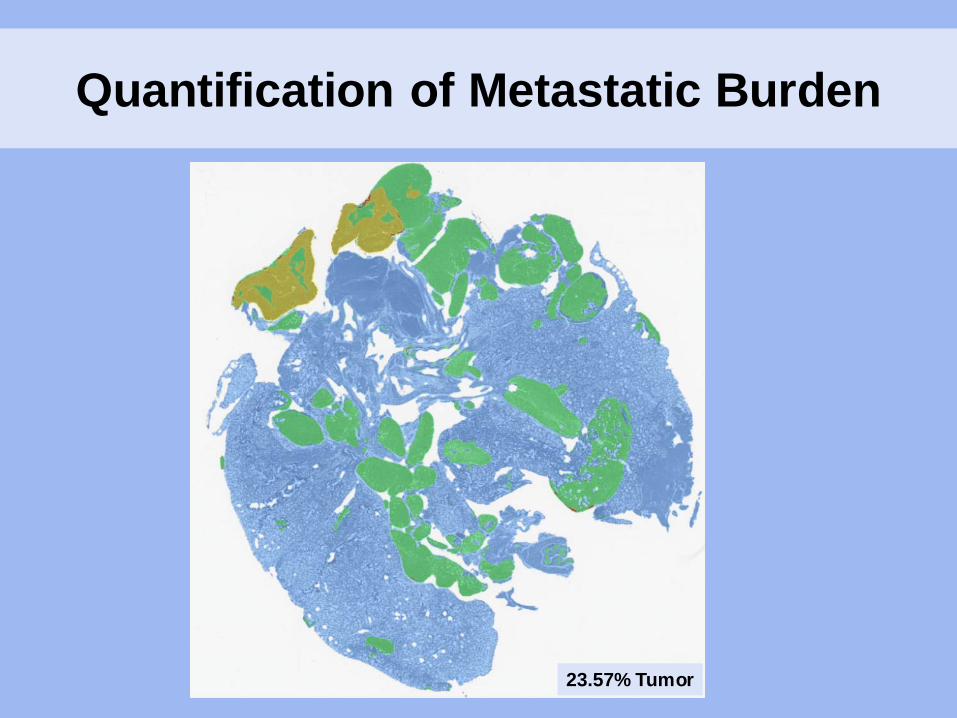
Quantification of Metastatic Burden
23.57% Tumor

Identification of Regions of Interest: Immunohistochemistry Quantification
Pattern Recognition Image Analysis: Persistent Questions
• How accurate are PRIA measurements?
• How reproducible are PRIA measurements?
• Can PRIA software be used for diagnostic screening?
• How can we best employ PRIA software?
• How well does 2-D PRIA represent 3-D lesions?
Evaluation of Pattern Recognition Image Analysis (PRIA)
• Comparison to established morphometric measurements – Quantification of pulmonary metastatic tumor burden – PRIA vs. manual segmentation
• Assessment of performance during segmentation of morphologically complex tissues – Identification of 3 ontogenic germ layers in stem cell-
derived teratomas
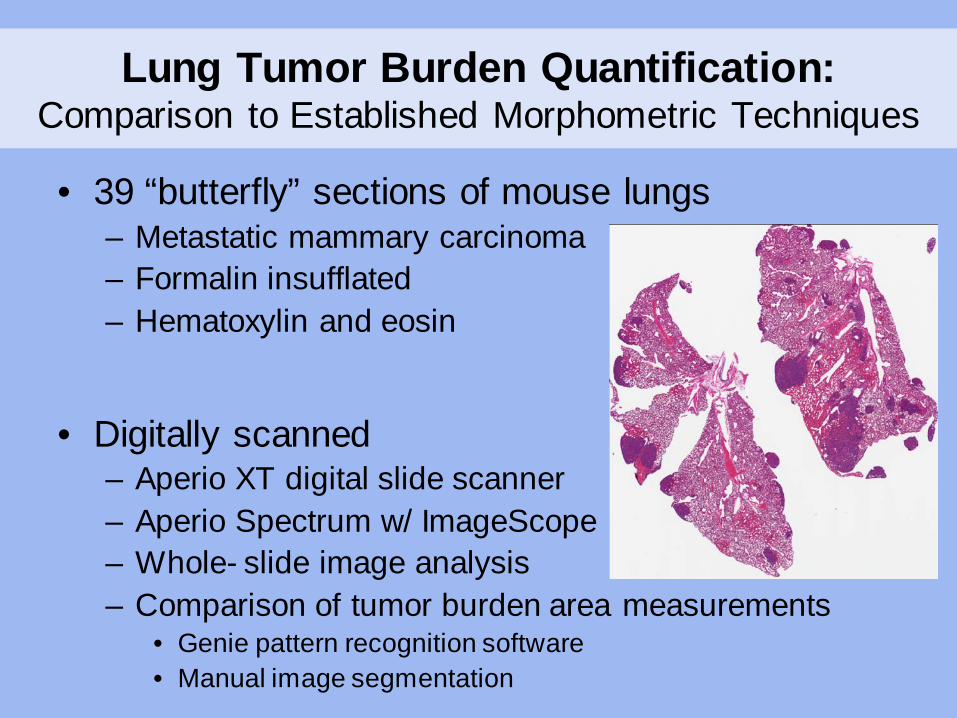
Lung Tumor Burden Quantification: Comparison to Established Morphometric Techniques
• 39 “butterfly” sections of mouse lungs – Metastatic mammary carcinoma – Formalin insufflated – Hematoxylin and eosin
• Digitally scanned
– Aperio XT digital slide scanner – Aperio Spectrum w/ ImageScope – Whole- slide image analysis – Comparison of tumor burden area measurements
• Genie pattern recognition software • Manual image segmentation
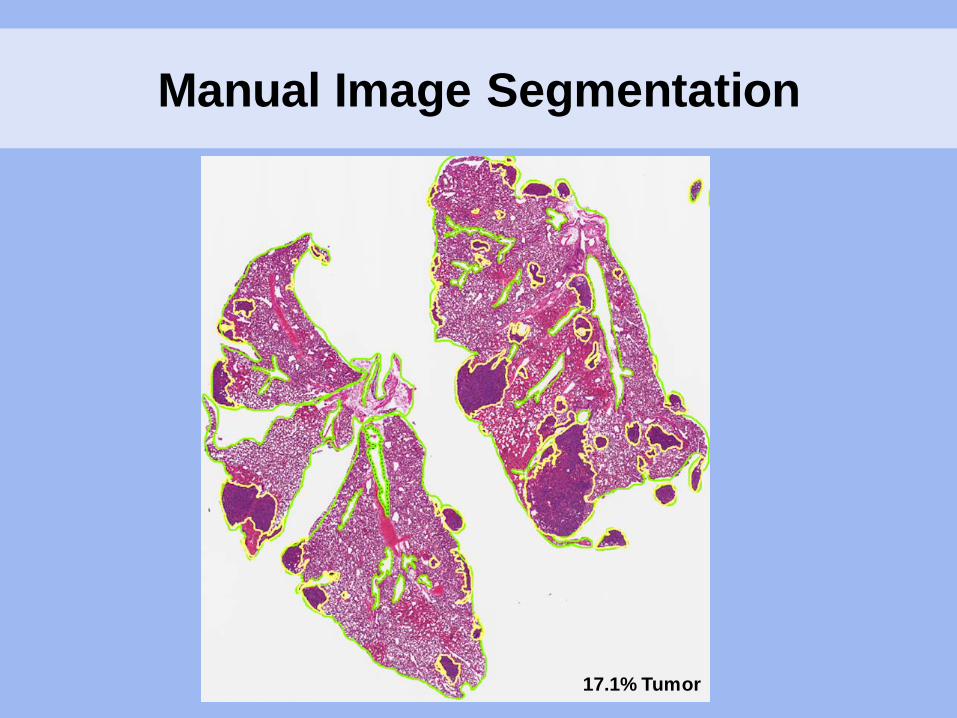
Manual Image Segmentation
17.1% Tumor
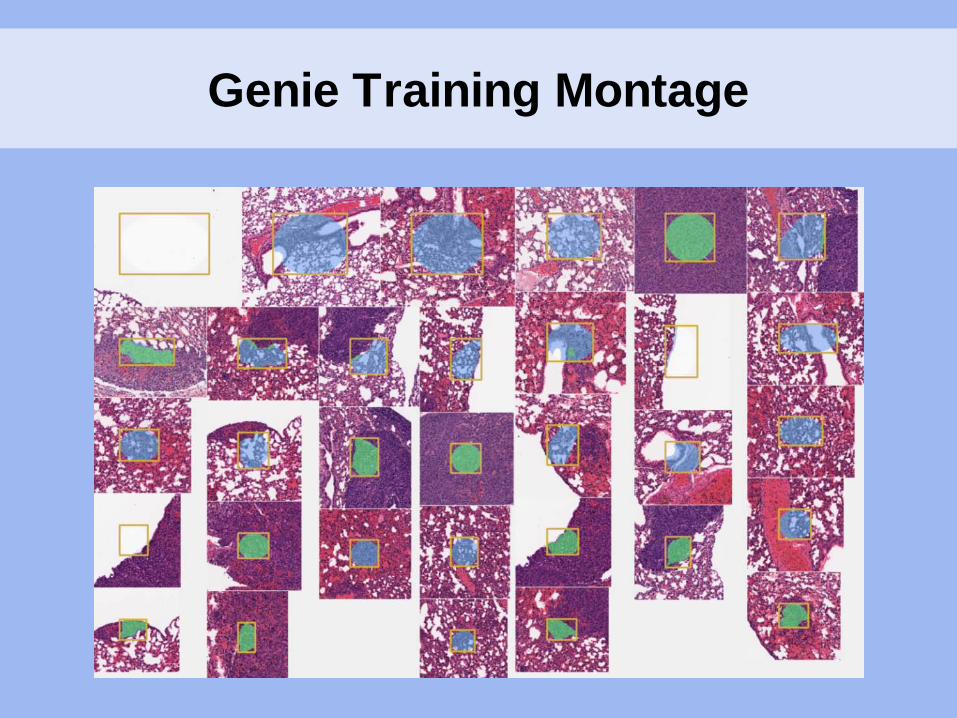
Genie Training Montage
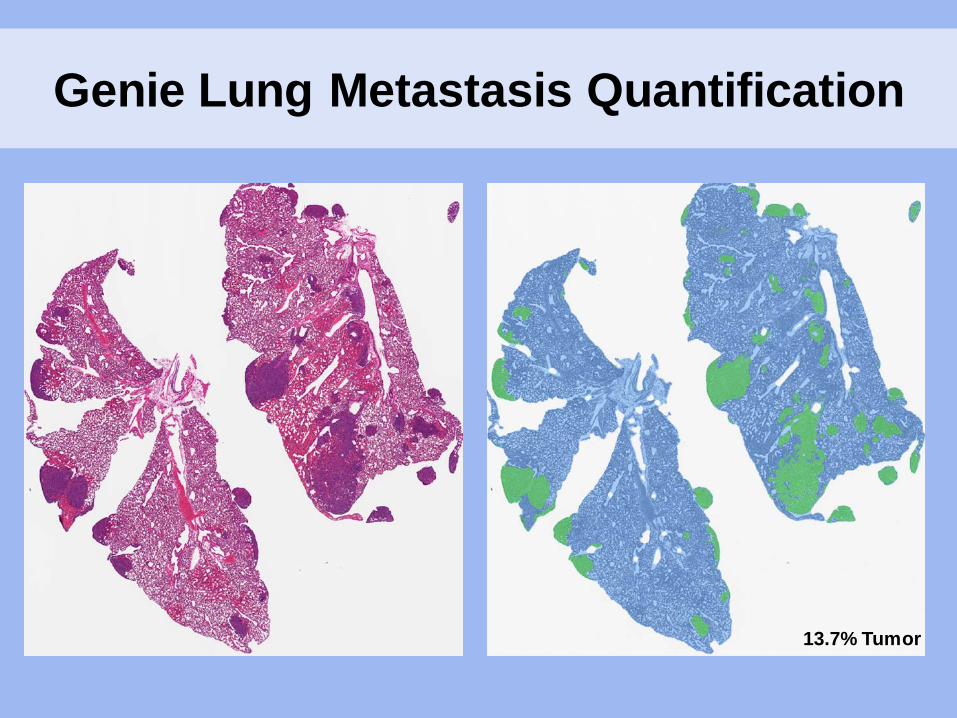
Genie Lung Metastasis Quantification
13.7% Tumor
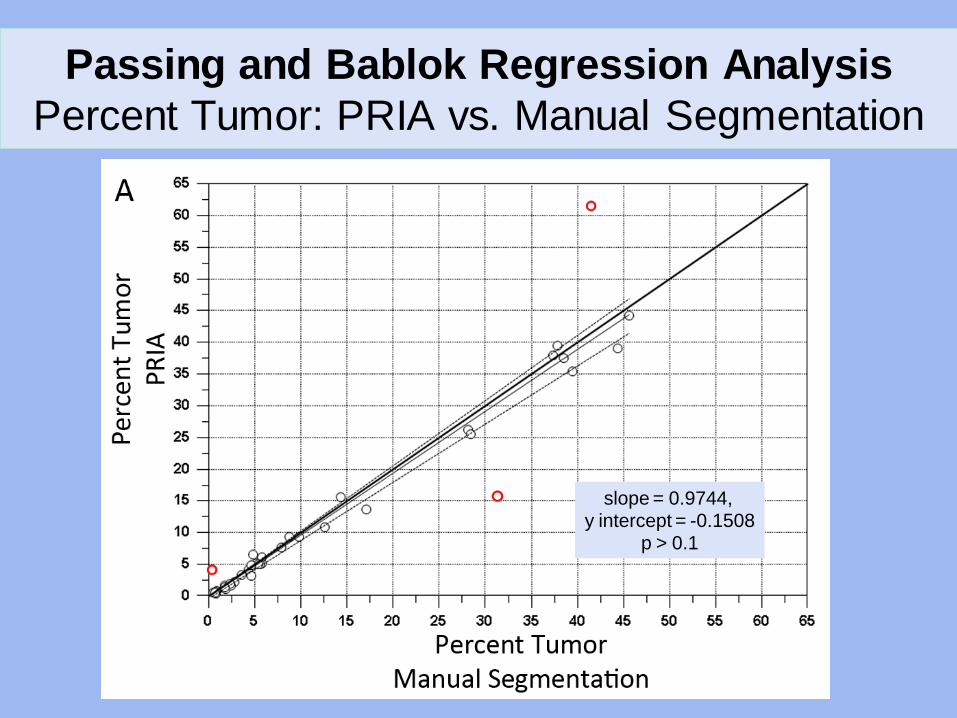
Passing and Bablok Regression Analysis Percent Tumor: PRIA vs. Manual Segmentation
slope = 0.9744, y intercept = -0.1508
p > 0.1
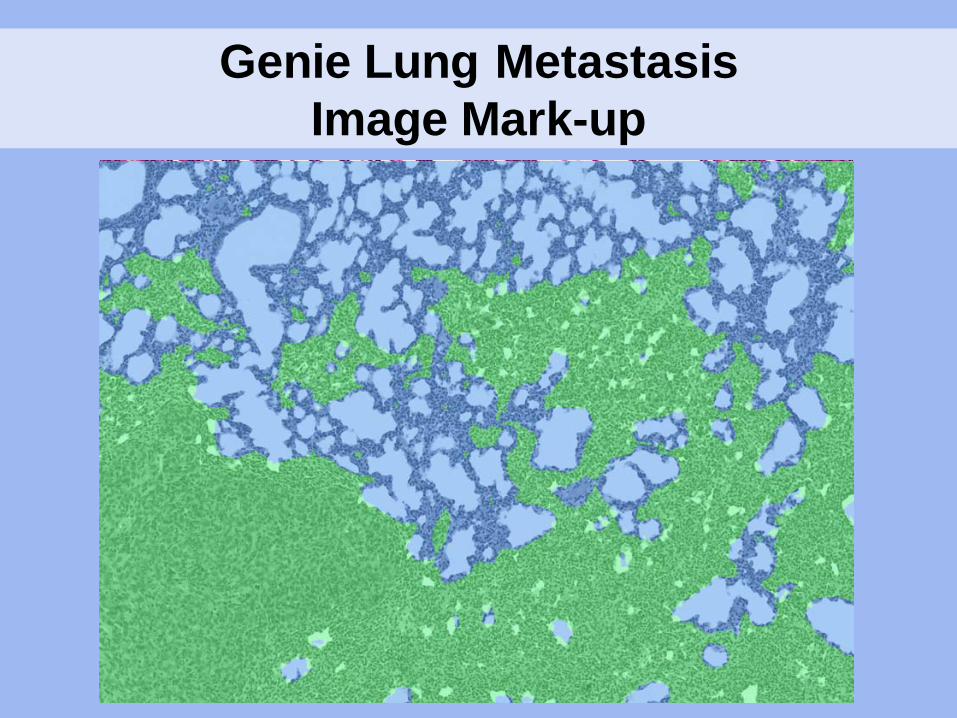
Genie Lung Metastasis Image Mark-up
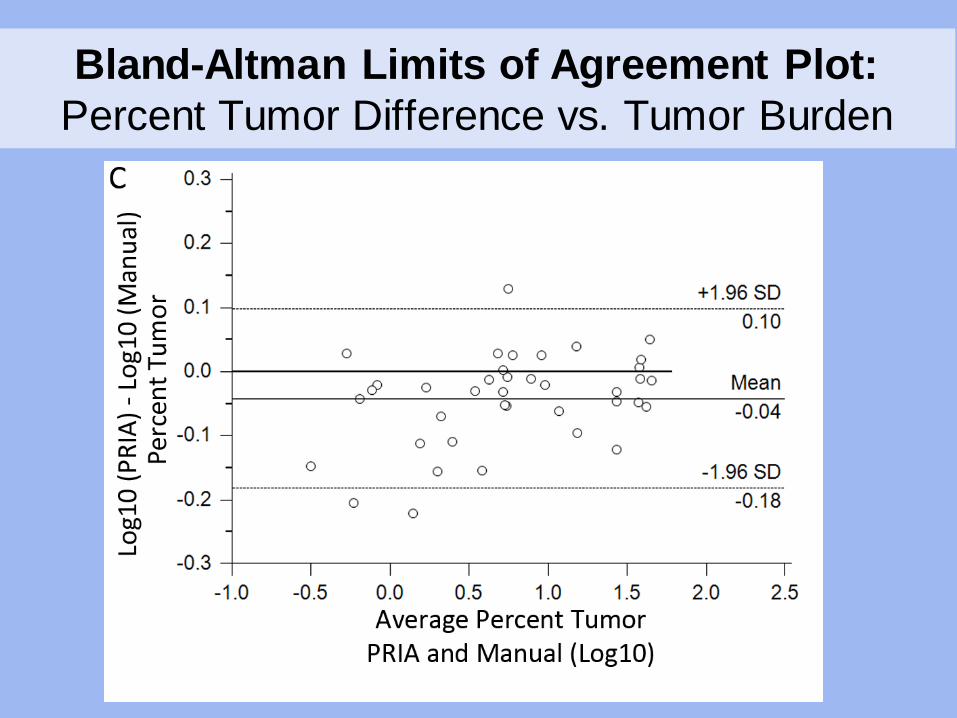
Bland-Altman Limits of Agreement Plot: Percent Tumor Difference vs. Tumor Burden
Lung Tumor Burden Quantification: Conclusions
• Commensurate percent tumor measures – PRIA tended to be < 9% less than Manual
• Differences between methods are uniform across samples
• Consistent inaccuracies – Mostly tolerable – Tangential bronchioles and atelectasis
• Algorithms are sensitive to variations in – Tissue handling – Processing – Staining
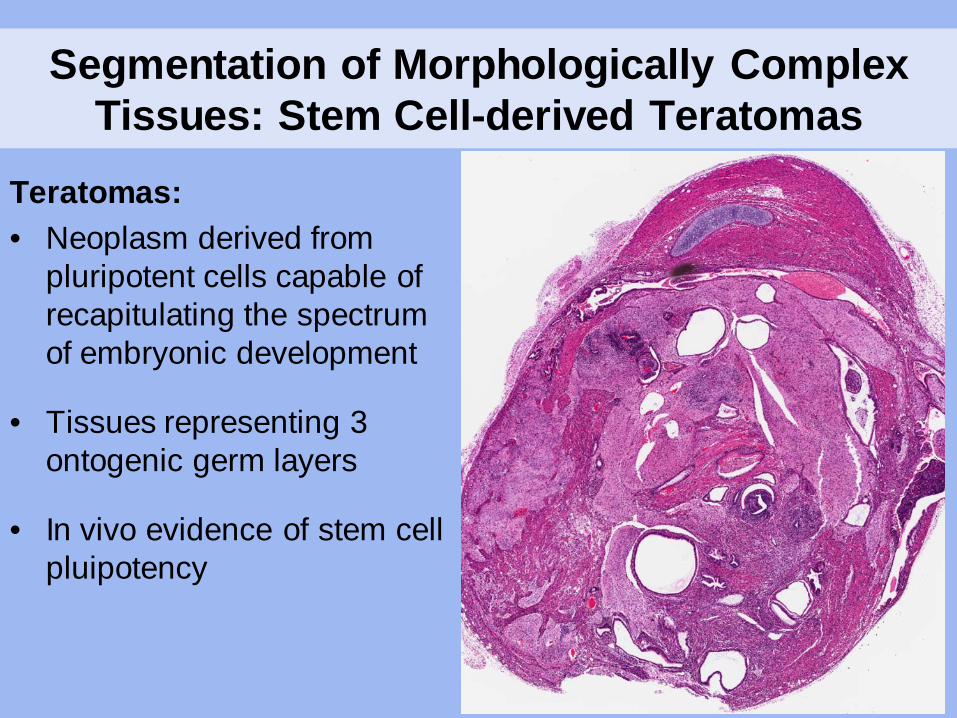
Segmentation of Morphologically Complex Tissues: Stem Cell-derived Teratomas
Teratomas: • Neoplasm derived from
pluripotent cells capable of recapitulating the spectrum of embryonic development
• Tissues representing 3 ontogenic germ layers
• In vivo evidence of stem cell pluipotency
Stem Cell Derived Teratomas
• Samples: – 26 Teratomas
• Mouse – 10 Embryonic stem cell/ 2 induced pluripotent stem cell
• Human – 8 Embryonic stem cell/ 6 induced pluripotent stem cell
• 10 more differentiated
• 16 less differentiated
• Formalin fixed, hematoxylin and eosin stained

Genie Training Montage
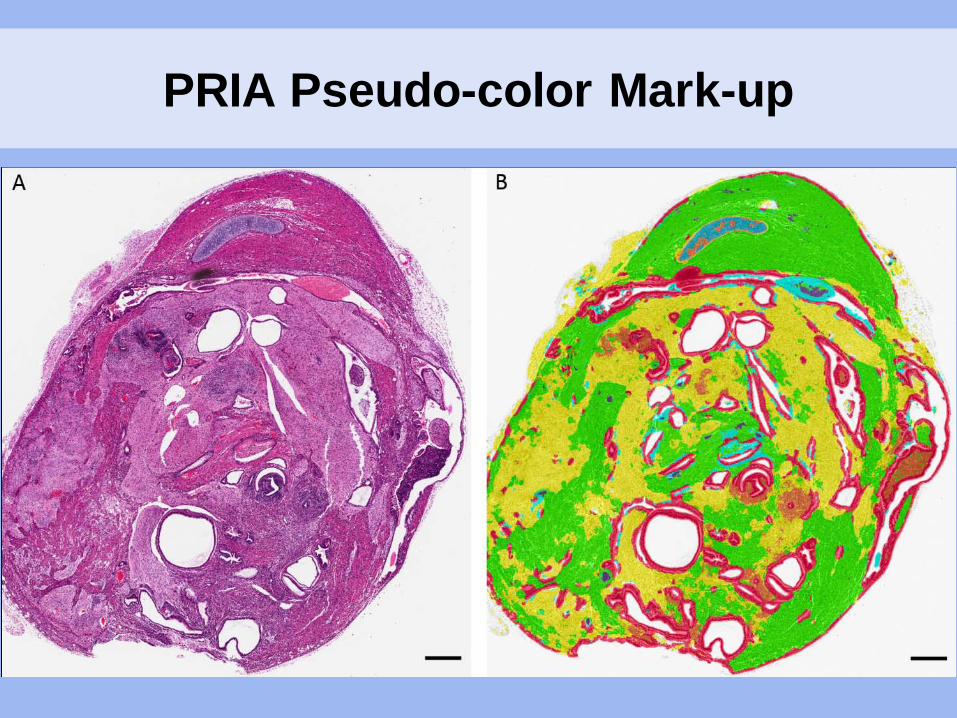
PRIA Pseudo-color Mark-up
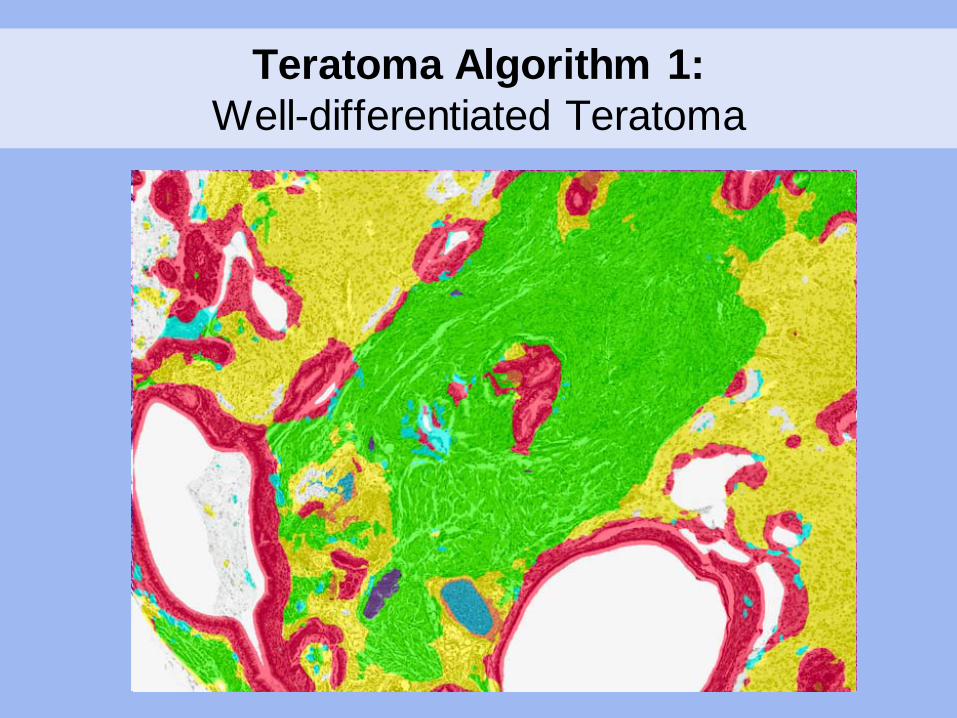
Teratoma Algorithm 1: Well-differentiated Teratoma
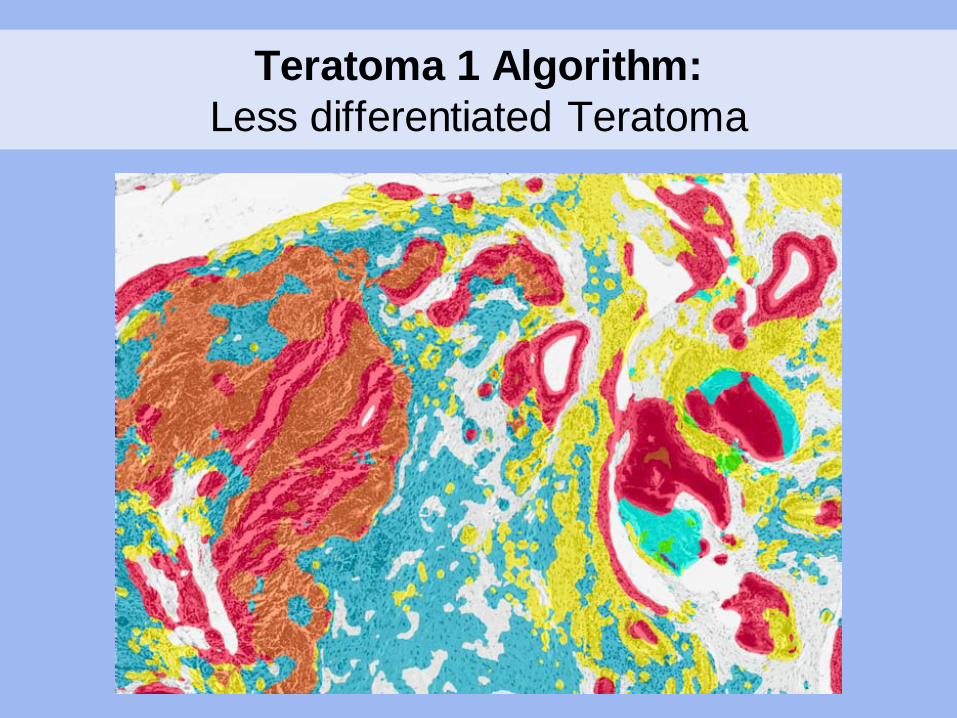
Teratoma 1 Algorithm: Less differentiated Teratoma
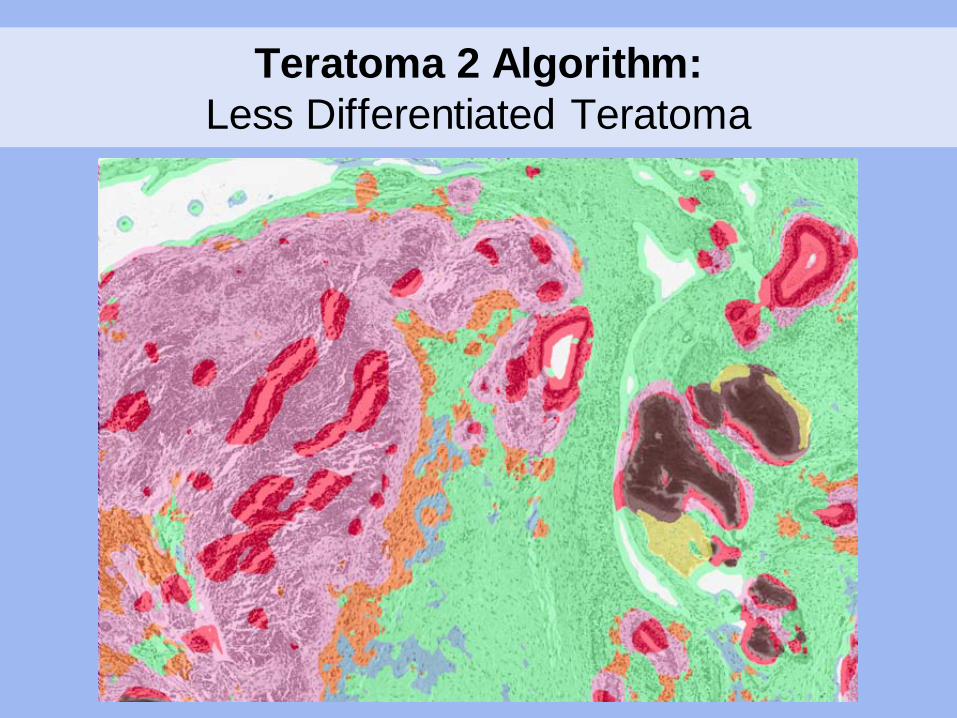
Teratoma 2 Algorithm: Less Differentiated Teratoma
Segmentation of Complex Tissues: Conclusions
• Challenging to account for all tissue classes in a single montage – Montage size limits – Broad spectrum of spatial-spectral features – Overlapping spatial-spectral features
• Overcoming some challenges – Development of multiple algorithms – Consider limitations – Ask appropriate questions

Perceived Limitations Based on Experience
• Preferential reliance on spectral features
• Sensitivity to specimen handling, processing, staining
• Limited contextual understanding – Restriction to a single magnification
• Repetitive difficulties in segmenting necrosis

Preferential Reliance on Spectral Features
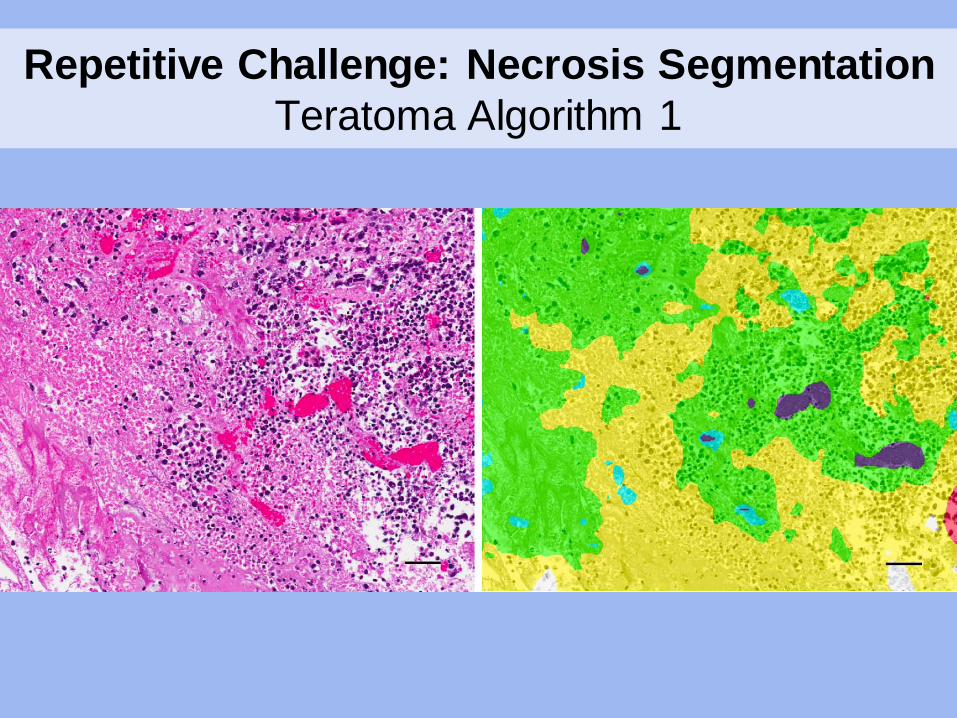
Repetitive Challenge: Necrosis Segmentation Teratoma Algorithm 1
PRIA Application: Tissue Biobank Quality Assurance
• Tissue biobanking – Essential for translational biomedical research – Reliant on high-quality, well-annotated specimens
• Need for quality assurance pathology review
• Traditional quality assurance pathology review – Confirmation of disease – Subjective assessment of percent tumor – Single or multiple staff pathologists
• Goal: – Utilize PRIA to reproducibly and consistently quantify
tumor percentages in biobank specimens
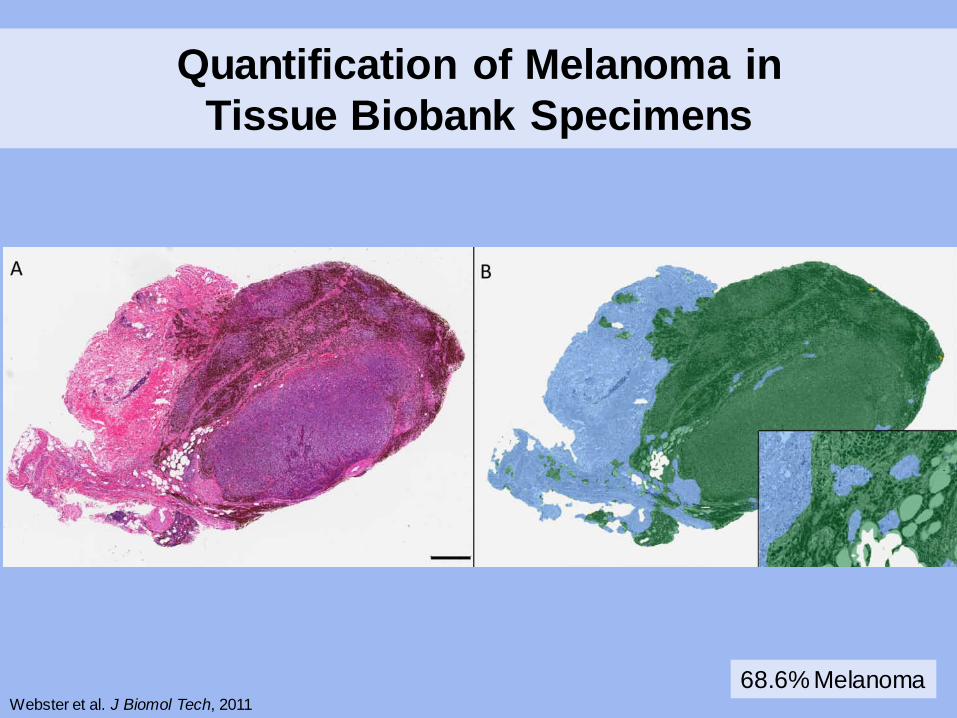
Quantification of Melanoma in Tissue Biobank Specimens
68.6% Melanoma Webster et al. J Biomol Tech, 2011
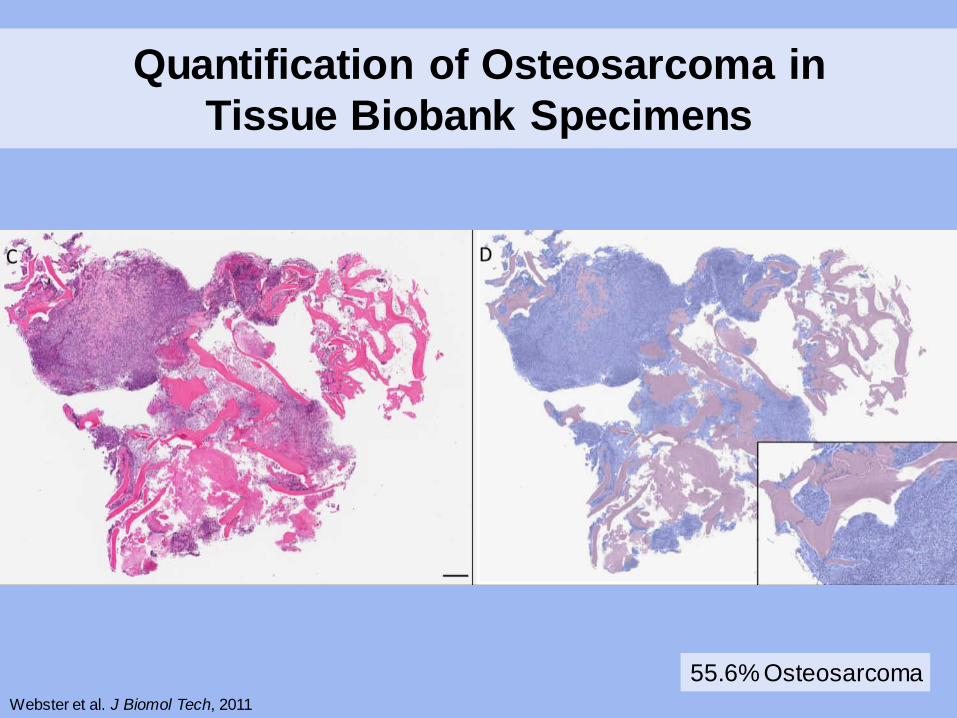
Quantification of Osteosarcoma in Tissue Biobank Specimens
55.6% Osteosarcoma Webster et al. J Biomol Tech, 2011
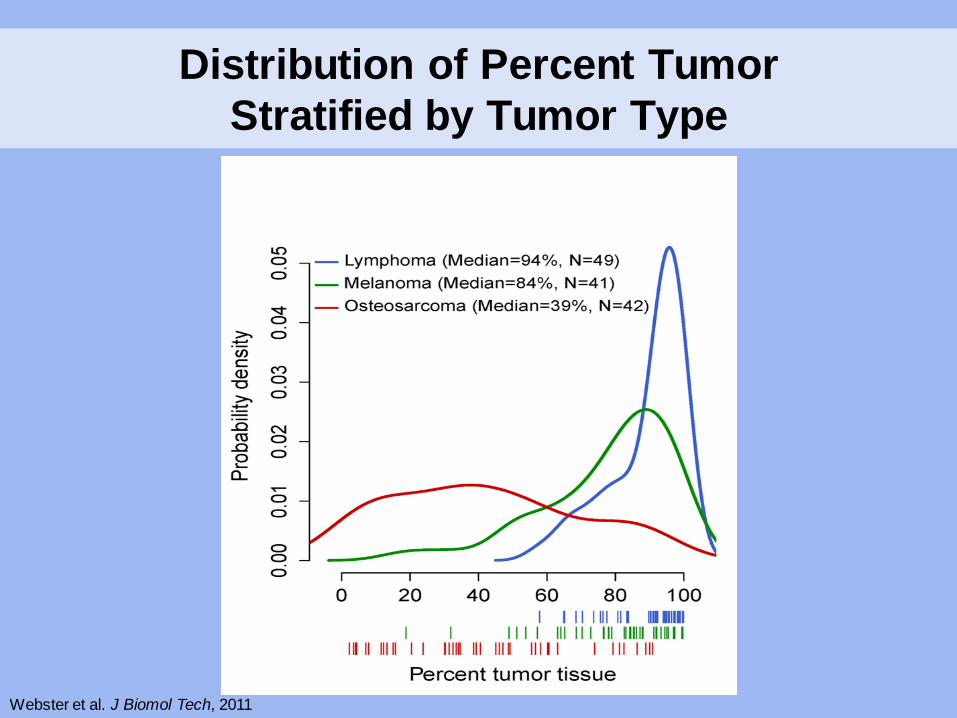
Distribution of Percent Tumor Stratified by Tumor Type
Webster et al. J Biomol Tech, 2011
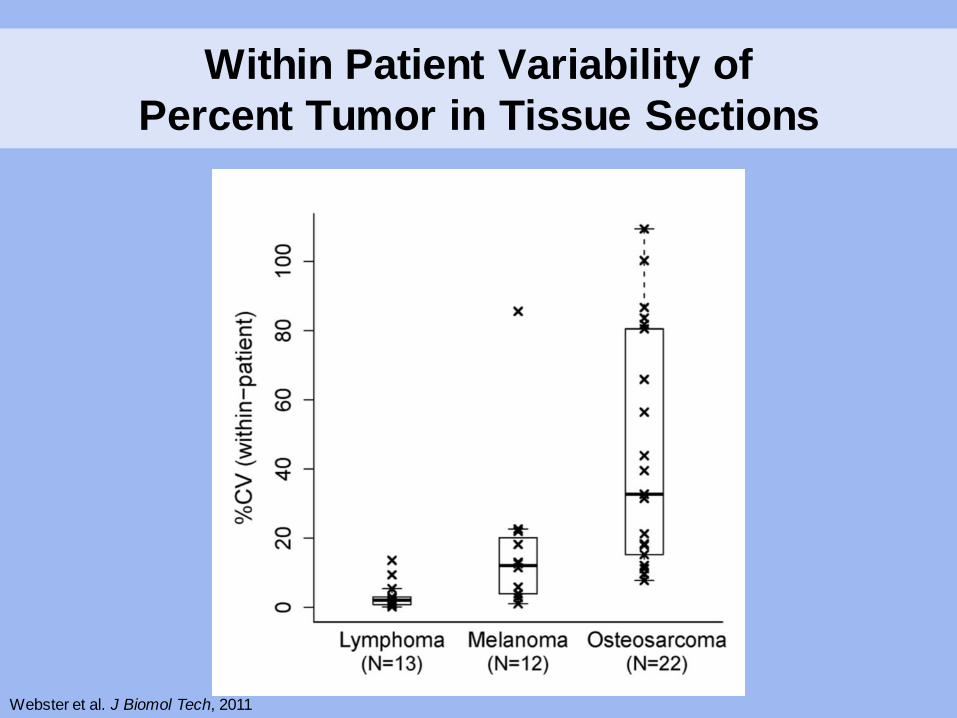
Within Patient Variability of Percent Tumor in Tissue Sections
Webster et al. J Biomol Tech, 2011
2-Dimensional Analysis of 3-Dimensional Lesions
• Questions: – Are single sections representative? – How many step sections are representative?
• What thicknesses?
• Evaluations: – Comparison to in vivo bioluminescence imaging – Comparison to advanced imaging modalities
• MRI • CT scan
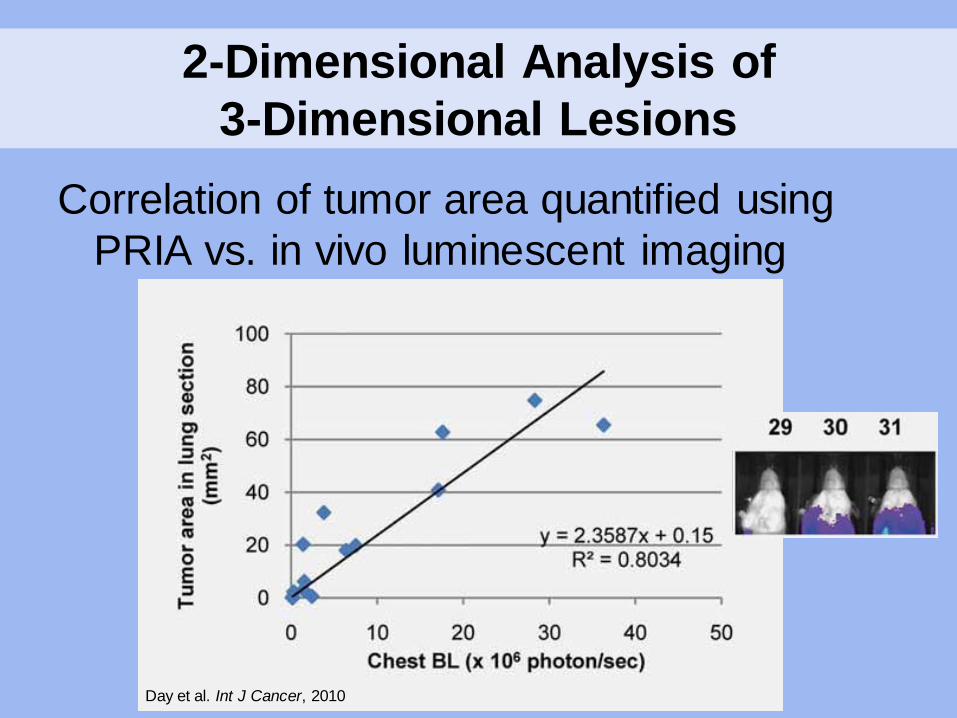
2-Dimensional Analysis of 3-Dimensional Lesions
Correlation of tumor area quantified using PRIA vs. in vivo luminescent imaging
Day et al. Int J Cancer, 2010
Conclusions
• Histologic PRIA software allows for – Reproducible tissue quantification – Decreased intra-/ inter-observer variability – Decreased subjectivity – Increased throughput
• Limitations must be considered – Difficulty segmenting complex tissues – Sensitivity to variations in tissue processing – Preferential reliance on spectral features

Conclusions
• PRIA is optimally utilized when – Tissues are uniformly handled/ processed
– Algorithms are simplified
– Application to appropriate questions
– Quality assurance is uniformly applied
– Pathologist oversight is included in PRIA applications
Acknowledgments • NCI Molecular Pathology Unit
– Mark Simpson – Jennifer Dwyer – Kara Corps – Shelley Hoover – Bih-Rong Wei – John Hickerson
• NCI Laboratory of Cancer
Biology and Genetics – Lalage Wakefield – Yu-an Yang – Christie Tomlinson – Jeff Green – Jing Huang
• National Institute of Aging – Minoru Ko – Yuhki Nakatake
• Johns Hopkins University
– Tarja Juopperi – Hongjun Song
Recommended