EPILEPSY
Mid-16th century term.
French word epilēpsia "seizure"
Greek epilambanein "seize" < lambanein "grasp”
“ TO BE POSSESSED BY”

Epilepsy: epidemiology• Incidence: Developed countries: 40-70 per one lacDeveloping countries: 100-190 per one lac• Prevalence:Developed countries: 4-10 per 10,000Developing countries: 57 per 10,000• Partial seizures with or without gen.most common• Bimodal age distribution: < 1year and > 60. Less sharp in developing countriesCommon causes: Perinatal disorders asstd. with CP and
MR, Head trauma, CNS infections, Stroke, Brain tumours, Alcohol and other drugs
Men affected 1-2.4 times comp. to women

What is a seizure?
Seizure A transient neurological dysfunction due to an abnormal transient hypersynchronous firing of cerebral neurons, which may or may not have a clinical manifestation – Electrical or Clinical seizure
.

What is Epilepsy?
• Epilepsy A clinical paroxysmal disorder of recurring seizures
• Epileptic Syndrome A well recognised disease-complex characterised by epilepsy

Basic pathophysiology?
I. Neuronal hyperexcitability
“Paroxysmal Depolarisation Shift (PDS)”


II. Hypersynchrony of neuronal firing
Simultaneous firing due to inhibition of collateral inhibitory neurons
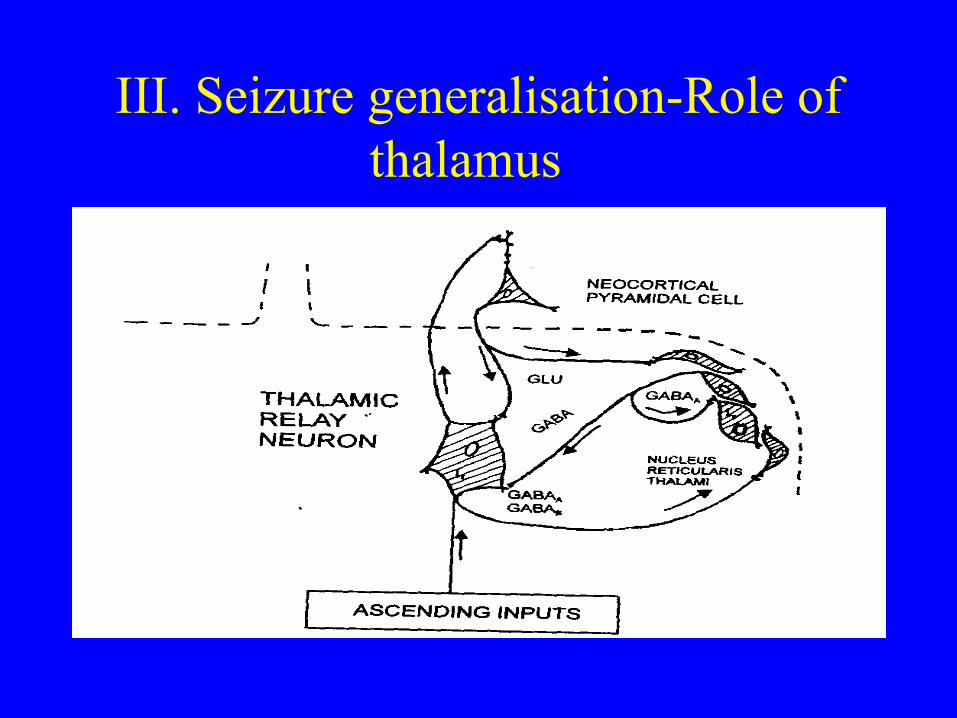
III. Seizure generalisation-Role of thalamus

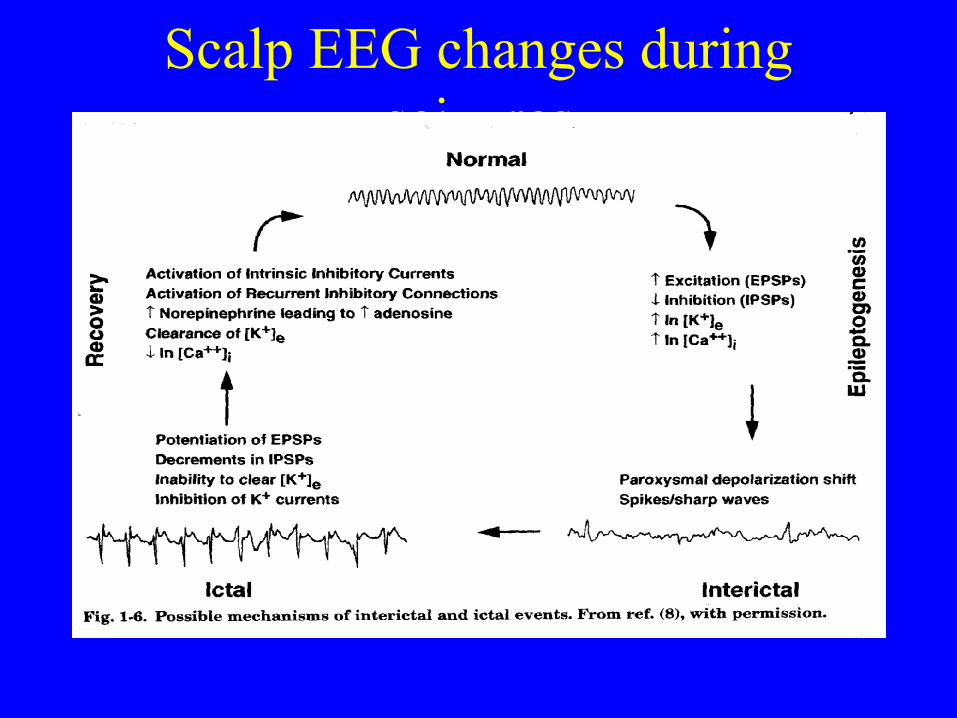
Scalp EEG changes during seizures

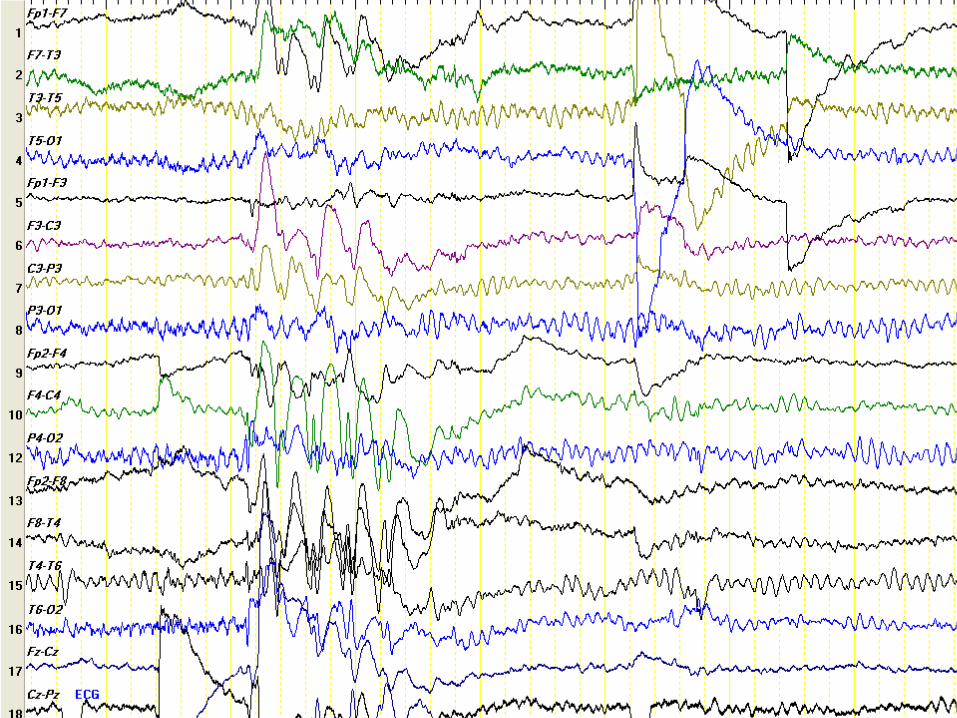
How does an EEG page look?

Scalp EEG record during a seizure

EEG of a “ bad and epileptic brain”-Hypsarrythmia











PLEDS
Types of seizures and related terms
• Myoclonus A single abrupt shock like extensor movement of a limb. myoclonic seizures.
• Petit Mal The French term used in the 1800's to describe a small spell. Still used today to describe absence seizures as well as atypical absence.
• Tonic Sustained contraction of one or more muscle groups, independent of position (i.e. can be flexed, extended, or opisthotonic).
• Convulsion Tonic, clonic or tonic-clonic seizure• Aura A generic term for a warning. A colloquial term
for simple partial seizure.

Automatism A purposeful, but irrelevant activity during or shortly following a seizure. The spectrum of these activities is wide, but follow general rules of stereotypy and short
duration. Not premeditated, or requiring higher cognitive functions. Not directed violence.
Status A pathological state different from a single seizure by the Epilepticus absence or reduction of inhibitory processes to terminate
the seizure. Applies to any seizure type. The length of time required to differentiate seizure from status is both empirical and practical.
Convulsive, myoclonic status: 10-30 minutes. Longer in complex partial or "absence" status since the diagnosis is dependent on clinical suspicion and EEG.

Classification of seizures
• Convulsive/non-convulsive (Major/minor)
• Focal or non-focal
• Acute symptomatic/remote symptomatic/ idiopathic or cryptogenic

Revised ILAE SEIZURE Classification
• 1. Classification of seizures• 2. Classification of epilepsies and
epileptic syndromes

Revised ILAE SEIZURE Classification
1. PARTIAL (FOCAL, LOCAL) SEIZURES
2. GENERALIZED SEIZURES (CONVULSIVE OR NONCONVULSIVE)
3. UNCLASSIFIED EPILEPTIC SEIZURES

Revised ILAE classification of epilepsies and epileptic syndromes
• 1. Localisation related epilepsies and syndromes
• 2. Generalised Epilepsies and Syndromes
• 3. Epilepsies and syndromes (focal/generalised of undetermined aetiology)

Revised ILAE SEIZURE Classification
1. PARTIAL (FOCAL, LOCAL) SEIZURES
2. GENERALIZED SEIZURES (CONVULSIVE OR NONCONVULSIVE)
3. UNCLASSIFIED EPILEPTIC SEIZURES

Revised ILAE SEIZURE Classification
1. PARTIAL (FOCAL, LOCAL) SEIZURES
• A. Simple partial seizures
• B. Complex partial seizures
• C. Partial seizures evolving to generalized tonic-clonic convulsions (GTC

Revised ILAE SEIZURE Classification:
2. Generalised seizures• A. Absence seizures
• B. Myoclonic seizures
• C. Clonic seizures
• D. Tonic seizures
• E. Tonic-clonic seizures
• F. Atonic seizures (astatic)

Revised ILAE SEIZURE Classification
3. UNCLASSIFIED EPILEPTIC SEIZURES• Includes all seizures that cannot be classified
because of inadequate or incomplete data and some that defy classification in hitherto described categories.
• This includes some neonatal seizures, e.g., rhythmic eye movements, chewing, and swimming movements.

REVISED ILAE SEIZURE CLASSIFICATION
I. PARTIAL (FOCAL, LOCAL) SEIZURES- 3 Main types
A. Simple partial seizures
B. Complex partial seizures
1. With impairment of consciousness at onset
2. Simple partial onset followed by impairment of consciousness
C. Partial seizures evolving to generalized tonic-clonic convulsions (GTC)
1. Simple evolving to GTC
2. Complex evolving to GTC (including those with simple partial onset)

Clinical seizure types
A. Simple partial seizures (consciousness not impaired)
1. With motor signs
a. focal motor without march
b. focal motor with march (Jacksonian)
c. versive
d. postural
e. phonatory (vocalization or arrest of speech)
2. With somatosensory or special-sensory symptoms (simple
hallucinations, e.g.,tingling, light flashes, buzzing)
a. somatosensory
b. visual
c. auditory
d. olfactory
e. gustatory

Clinical seizure types
A. Simple partial seizures (continued)
3. With autonomic symptoms or signs (including epigastric sensation, pallor, sweating, flushing, piloerection, and pupillary dilatation)
4. With psychic symptoms (disturbance of higher cerebral function).
a. dysphasic
b. dysmnesic (e.g., d‚j… vu)
c. cognitive (e.g., dreamy states, distortions of time sense)
d. affective (fear, anger, etc.)
e. illusions (e.g., macropsia)
f. structured hallucinations (e.g., music, scenes)

B. Complex partial seizures (with impairment of consciousness;
may sometimes begin with simple symptomatology)
1. Simple partial onset followed by impairment of consciousness
a. with simple partial features (A.1.-A.4.) followed by impaired
consciousness
b. with automatisms
2. With impairment of consciousness at onset
a. with impairment of consciousness only
b. with automatisms
C. Partial seizures evolving to secondarily generalized seizures
(This may be generalized tonic-clonic, tonic, or clonic.)
1. Simple partial seizures (A) evolving to generalized seizures
2. Complex partial seizures (B) evolving to generalized seizures
3. Simple partial seizures evolving to complex partial seizures
evolving to generalized seizures

II. GENERALIZED SEIZURES (CONVULSIVE OR NONCONVULSIVE)
• The first clinical changes indicate initial involvement of both hemispheres.
• Consciousness may be impaired and this impairment may be the initial manifestation.
• Motor manifestations are bilateral.
• The ictal electroencephalographic patterns initially are bilateral and presumably reflect neuronal discharge which is widespread in both hemispheres.

II. GENERALIZED SEIZURES
• A. 1. Absence seizures• a. impairment of consciousness only
• b. with mild clonic components
• c. with atonic components• d. with tonic components• e. with automatisms• f. with autonomic components
• (b through f may be used alone or in combination)
• 2. Atypical absence May have:• a. changes in tone that are more pronounced than in A.1• b. onset and/or cessation that is not abrupt
• B. Myoclonic seizures Myoclonic jerks (simple or multiple)
• C. Clonic seizures
• D. Tonic seizures• E. Tonic-clonic seizures• F. Atonic seizures (astatic)
• Combinations of the above may occur, e.g., B and F, B and D.
Revised ILAE SEIZURE Classification
3. UNCLASSIFIED EPILEPTIC SEIZURES• Includes all seizures that cannot be classified
because of inadequate or incomplete data and some that defy classification in hitherto described categories.
• This includes some neonatal seizures, e.g., rhythmic eye movements, chewing, and swimming movements.

Revised ILAE classification of epilepsies and epileptic syndromes
• 1. Localisation related epilepsies and syndromes
• 2. Generalised Epilepsies and Syndromes
• 3. Epilepsies and syndromes (focal/generalised of undetermined aetiology)
Revised ILAE classification of epilepsies and epileptic syndromes
1.Localisation related epilepsies and syndromes
A.Idiopathic age related syndromes:
1)Benign rolandic epilepsy
2)Benign occipital epilepsy
B.Symptomatic: Syndromes of great individual Variability.
1)Tuberous sclerosis 2)Heterotopia
3)Cavernous hemangioma 4)ganglioneroma
5)Granuloma 6)Glioma
Revised ILAE classification of epilepsies and epileptic syndromes (Contd)
2. Generalised Epilepsies and SyndromesA.Idiopathic age related
– Benign neonatal familial convulsions– Benign neonatal convulsions– Benign myoclonic epilepsy of infancy– Childhood absence epilepsy– Juvenile myoclonic epilepsy– Epilepsy with grandmal on awakeningB. Symptomatic Non-specific cause. Early myoclonic encephalopathy Specific syndromes: Epileptic states complicating many disease states:[Phenyl Ketonuria,Porphyrias, Tay-Sachs, NCL, Pyridoxine deficiency, MERRF]
C. Idiopathic, symptomatic or both o West syndrome } PKU, Tay Sachs, TORCH inf.o Lennox-Gastout syndrome } o Epilepsy with myoclonic-astatic seizureso Epilepsy with myoclonic absences

Revised ILAE classification of epilepsies and epileptic syndromes
(Contd)3.Epilepsies and syndromes focal/generalised of undetermined aetiology
A.With both focal and generalised seizures• Neonatal seizures• Severe myoclonic epilepsy in infancy• Epilepsy with continuous spike-wave during slow-
wave sleep• Acquired epileptic aphasia (Landou-Kleffner)
B.quivocal of focal or generalised nature: LGS
Revised ILAE classification of epilepsies and epileptic syndromes
(Contd)
4. Special syndromesA. Situation related seizures:Febrile seizures
Cataminial seizures
Drug induced, alcohol induced or sleep deprived seizures
B. Reflex epilepsies: Eating, reading, hotwater epilepsies
C. Chronic progressive epilepsia partialis continua
D. Apparently unprovoked isolated epileptic events
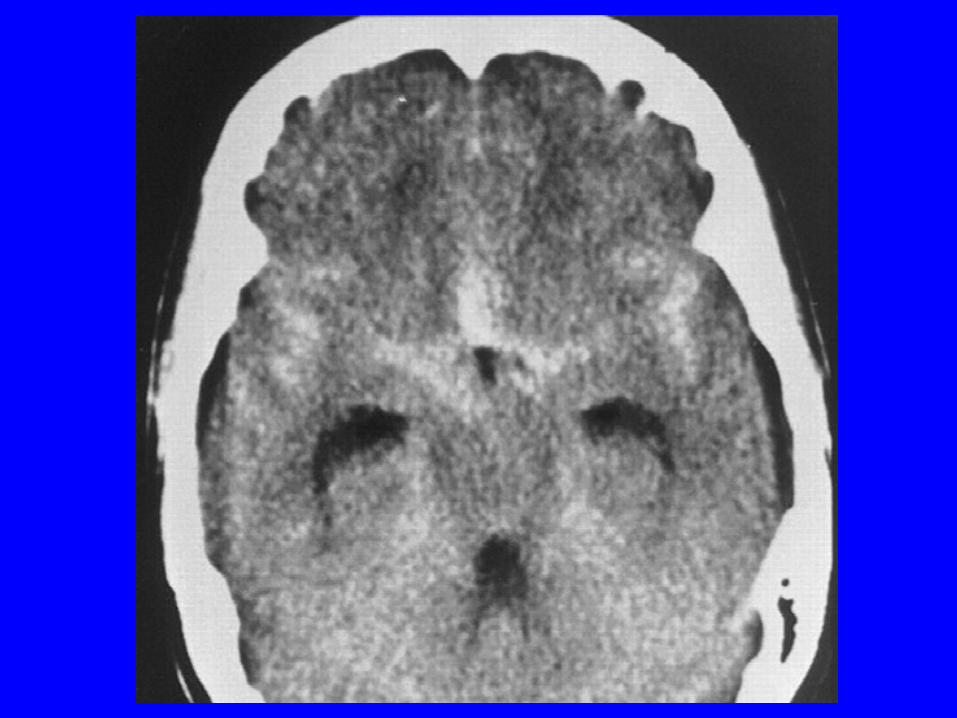
Aetiopathogenesis - I
Acquired Focal:
• Cerebral granuloma
• Brain abscess
• Mesial temporal sclerosis



Aetiopathogenesis - II
Acquired Diffuse cerebral lesions:
• Cerebral edema
• Encephalitis
• Subarachnoid hemorrhage

Aetiopathogenesis-III
Normal brain in acquired abnormal milieu interior as in
• Renal
• Hepatic
• Respiratory failure
• Poisoning
• Septicemia

Aetiopathogenesis-IV
Developmentally abnormal neuronal pools due to chromosomal or other genetic
anomalies
• Heterotopia
• Lissencephaly

Aetiopathogenesis - V
Developmentally abnormal neuronal membranes or circuits- intrauterine or
peripartum insults
• Neonatal HIE
• Intrauterine infections
• Aminoacidurias
• Phacomatoses
Aetiopathogenesis - VI
Genetic epilepsies: Due to abnormal expression of synaptic membrane channel
or receptor proteins
• Childhood Absence seizures
• Juvenile myoclonic epilepsy
Seizure- Videos

Eating-(Reflex) Epilepsy

Temporal lobe type Complex partial seizures with secondary
generalisation

Frontal lobe type Complex Partial Seizures- Adversive/gyratory
Seizure
Gyratory Seizure: Temporal lobe type Complex Partial Seizures-

Sleep associated complex partial seizures

Myoclonic seizure

Reflex Temporal lobe Complex partial seizure- vacuum cleaner sound


Pharmacotherapy of Epilepsy


Primary AEDs» Initial Usual
Dose Increment Maximum
• Diphenylhydantoin 300 mg OD 50-100 mg/1-2week 400 mg
• Phenobarbitone 90 mg OD 30 mg/2 wks 180 mg
• Carbamazepine 200 mg tid 200 mg/3 days 1200 mg
• Ethosuximide 250 mg tid 250 mg/2 wks 1500 mg • Valproate 200 mg tid 200 mg/3 days 1500 mg

Phenobarbitone
• Cheap, Long half life;
• But hyperactivity, sedation, cognitive side effects

Diphenyl Hydantoin
• Long half life.
• Good for focal and generalised epilepsies.
• Side effects too many: Hirsuitism, acne, gingival hyperplasia, megaloblastic anemia, osteoporosis, foetal hydantoin syndrome
• Long acting IM preps. Available now

Sodium Valproate
• Drug of choice for primary Generalised epilepsy, Works in focal too, Skin rashes rare (aliphatic)
• 3 to 4 times dosage• Hepatotoxicity, alopecia, tremor, weight gain,
Foetal valparin syndrome • IV prep. Available. Useful in SE.
• Long acting once daily oral prep also abvailable
Carbamazepine
• Most used drug for all partial seizures. Works in generalised too.
• Positive cognitive effects. Safer drug in pregnancy.
• Rashes common. 3-4 times dosage. No parenteral prep.
• Longer acting preparations available now

Oxcarbamazepine
• Lesser frequency- twice only
• Rashes occur but less
• Hyponatremia on long term use
• Decrease OCP levels

Lamotrigine
• Useful add on for both primary generalised and partial seizures.
• Very useful in LGS, Intractable JME etc.
• Rashes can be a major problem
• VPA doubles but CBZ, DPH, PB reduces blood levels---Caution with polytherapy
Vigabatrin
• Very Useful drug in myoclonic seizures
• Increases the blood level and reduces the need of VPA
• Drug interactions minimum.
• Hallucinations can occur

Levetiracetam
• Extremely useful drug in complex partial seizures
• Remarkably free from all side effects
• Negligible drug interactions

Anti-epileptic drug Selection• Correct diagnosis of the type of epilepsy influences treatment,
prognosis and genetic counseling.• Use the least expensive AED (all things being equal, like efficacy).• Prefer AEDs which can be taken once daily over bid/tid as this
improves compliance. AEDs almost never need qid dosing• For absence epilepsy (petit mal), ethosuximide is the AED of
choice. Valproate is equally effective--BUT--fatal complications (rare) make it an unacceptable first choice.
• Use valproate for absence plus myoclonic/clonic/tonic/atonic.• Phenytoin, carbamazepine Phenobarbital and primidone are all
equally effective against partial/complex partial seizures.• Valproate, clonazepam are only second line drugs for partial seizures.• Newer is not better, and almost certainly more expensive but drug
interactions much less for most

Monotherapy
• One best drug to fit the fit and Fit the patient; Sequential monotherapy
• Start with one AED and push the dose to clinical toxicity or seizure control.
• Withdraw AEDs that are not effective.

Polypharmacy
• Never have a patient on more than three (3) AED's.
• Don't use combinations meds (e.g., Dilantin with phenobarbital).
• No good study has been done to prove that multiple AEDs are synergistic in the treatment of epilepsy.
• Polypharmacy is expensive, increases side effects and increases the complexity of adjusting AEDs in the refractory patient.
Status Epilepticus-Definition 1. Major motor (convulsive) status is 3
seizures uninterrupted by consciousness or a single prolonged seizure greater than 1/2 hour.
2. Spike wave stupor (Absence or Petit mal) and complex partial (psychomotor) status are prolonged alterations of consciousness verified by EEG as epileptic.
3. Epilepsia partialis continua is focal motor status (rarely sensory).
Status Epilepticus- Causes• Outpatient -- patient presents to hospital already in
status.
• a. Anticonvulsant withdrawal
• b. Alcohol withdrawal
• c. Hysterical
• d. Tumor
• e. Others i.Vascular--stroke, hemorrhage, aneurysm,
• ii Infectious -- bacterial, viral
•
Status Epilepticus- TreatmentImmediate treatment • 1. Start IV, draw bloods (including
anticonvulsant levels), push 50 cc 10% glucose and 100 mg thiamine; In neonates, calcium and pyridoxine too
• 2. Monitor vital signs. • 3.Examine patient. • 4. Protect patient from external injury, never
leave patient alone
• 5. Intubate all patients if first line drugs fail.

Status Epilepticus-Definitive Treatment • a. Diazepam- fast acting, short lasting• i. Good results, easy to administer.• ii. 10 mg IV push over 30 seconds, may be
repeated. If two doses fail to stop status, then further doses probably won't work either.
• iii. Side effects -- hypotension, bradycardia, respiratory depression,cardiac arrest, depresses mental status.
• b. Lorazepam - fast acting, medium lasting.• i. Similar to diazepam in most ways.• ii. 4 mg IV push may be repeated.• Respiratory depression only in the extubated patient.
Status Epilepticus-Definite Treatment c. IV Phenytoin - fast and long acting. i. Presently used concomitantly with a benzodiazepine
as the long lasting drug, half-life 20 hours.12-20mg/kg IV ii. Must be given as close to the vein as possible since it
precipitates out in the line. It's pH is 12, all i.v. fluids are pH 4-6.
d. IV Valproate -fast acting, long acting. i. Generally not used because of lack of experience.
Good results in both major motor and absence status. ii. 25 mg/kg IV push, may repeat. iii. Far less side effects than Diazepam and dilantin.
especially in unstable cardiac status, hypotension, hepatic failure etc.

Management of Medically refractory epilepsy- Localisation
of seizure focus
• Video-EEG
• MRI seizure protocol
• SPECT scan/ PET scan
• Invasive (subdural) EEG
• Psychometry
• Wada’s test

Management of Medically refractory epilepsy
• If MTS, Anterior temporal lobectomy
• In GTCS, subpial resection, callosotomy, commissurotomy,
• Sturge-Weber, Rasmussen’s etc.hemispherectomy
• Ketogenic diet
• Vagal stimulation

Brain Mapping

Epileptics in special situations in life
• Marriage• Pregnancy• Driving • No to some Jobs: Piloting, Firemen, Diving,
Mining, hiking, Space exploration. Night duties• Associated mental retardation and other
disabilities
• Psychiatric comorbidity

THANK YOU
Recommended