320 J Med Assoc Thai Vol. 92 No. 3 2009
Enhancing Limb Salvage by Non-Mobilized PeripheralBlood Angiogenic Cell Precursors Therapy in Patients
with Critical Limb Ischemia†
Pramook Mutirangura MD*,Chanean Ruangsetakit MD*, Chumpol Wongwanit MD*,
Khamin Chinsakchai MD*, Yael Porat PhD**,Adina Belleli PhD**, David Czeiger MD***
† ClinicalTrials.gov ID: NCT00523731* Vascular Surgery Unit, Department of Surgery, Faculty of Medicine Siriraj Hospital,
Mahidol University, Bangkok, Thailand** Theravitae Ltd. Nes Ziona, Israel
*** Ben-Gurion University, Beer Sheva, Israel
Background: Stem cell therapy has been proposed to enhance the salvage of critically ischemic limbs.Objective: Assess the efficacy and safety of the implantation of non-mobilized peripheral blood angiogeniccell precursors (NMPB-ACPs) in patients with critical limb ischemia (CLI) who were poor candidates forstandard revascularization treatment options.Material and Method: Six patients with CLI due to the infrapopliteal artery occlusive disease were includedin the present study. Intramuscular injections of NMPB-ACPs were administered in the ischemic limbs. Theefficacy was evaluated by clinical outcomes, ankle brachial index, toe brachial index, and computerizedtomographic angiography.Results: There was no evidence of local or systemic complication related to the procedure. Five patients(83.3%) had clinically significant improvement of adequate circulation at the distal limb for the completehealing. Four of them had complete healing of ischemic ulcers and stumps of toe amputation. However, onepatient with adequate granulation tissue at the stump of the left first toe amputation subsequently suffered fromsevere foot infection originating from the other toes and eventually underwent below knee amputation. Therewas no improvement of circulation at the distal limb after the administration of NMPB-ACPs in one patient(16.7%) who eventually underwent major amputation.Conclusion: The preliminary result of NMPB-ACPs therapy may be safe and provide benefits in the improve-ment of circulation in patients with CLI. A larger controlled trial is required to ascertain these preliminaryresults.
Keywords: Arterial occlusive diseases, Critical illness, Ischemia, Lower extremity, Peripheral blood stem celltransplantation, Stem cells
Correspondence to: Mutirangura P, Vascular Surgery Unit,Department of Surgery, Faculty of Medicine Siriraj Hospital,Mahidol University, Bangkok 10700, Thailand. Phone:0-2411-1808, Fax: 0-2412-9160. E-mail: [email protected], [email protected]
Critical limb Ischemia (CLI) is a serious problemof peripheral arterial occlusive disease due to the hightendency of major limb loss(1-3). The comorbidities of
ischemic heart disease and cerebrovascular disease arecommonly associated with this problem; resulting inhigh mortality and disability during the management(4-6).The primary treatments including arterial bypasssurgery, intervention and endovascular proceduresmay not succeed in many patients due to their poordistal artery run off and extensive calcification inlower extremity arteries. Major amputation therefore
J Med Assoc Thai 2009; 92 (3): 320-7Full text. e-Journal: http://www.mat.or.th/journal

J Med Assoc Thai Vol. 92 No. 3 2009 321
is inevitable in this situation(7-8). Autotransplantationof bone marrow cell(9,10) and granulocyte colonystimulating factor-mobilized peripheral bloodmononuclear cell demonstrated the improvement ofcirculation in critically ischemic limbs(11-15).
The authors recently reported the generationof enriched population of angiogenic progenitor cellsfrom human peripheral blood without the stimulationof bone marrow by granulocyte colony stimulatingfactor (G-CSF), called non-mobilized peripheral bloodangiogenic cell precursors (NMPB-ACPs)(16). Bonemarrow (BM) -derived stem/progenitor cells can beobtained by direct aspiration from the bone marrow,a procedure that entails pain and discomfort andrequires the use of anesthesia. An alternative methodof obtaining cells from the BM by pre-treating thepatient with G-CSF to induce migration of BM cells tothe peripheral blood (mobilized peripheral blood) mightresult in increased blood viscosity, metabolic demand,and platelet counts(17-20). To circumvent the risks anddiscomfort caused by either method. The authors optedto use cells harvested from non-mobilized peripheralblood as the raw material for ACP generation.
These cells simultaneously expressed Ulex-lectin and uptake of acetylated low density lipoprotein(Ac-LDL) as well as markers CD34, CD133, vascularendothelial growth factor (VEGF) receptor 2 (also knownas kinase domain region [KDR), Tie-2, CD144, vonWillebrand factor (vWF), and CD31. They also secretedinterleukine-8 (IL-8), VEGF, and angiogenin, and formedtube-like structures in vitro(16). However, the clinicalpotential of these cells is yet to be determined.
The objective of the present pilot study wasto assess the safety and efficacy of intra-muscularinjections of NMPB-ACPs in patients with critical limbischemia who were unresponsive to intensive medicaltherapy and unsuitable for revascularization procedure.
Material and MethodA pilot non-randomized, open-label study was
carried out in six patients with the permission of theEthics Committee, Faculty of Medicine Siriraj Hospital,Mahidol University, Bangkok, Thailand. The patientsunder the age of 85 years old with the symptoms ofcritical limb ischemia (Fontaine stage III and IV)(1)
such as ischemic rest pain, ischemic non- healed ulcerand digital gangrene together with hemodynamicassessment indicating limb threatening ischemia suchas ankle brachial index (ABI) below 0.4, or toe brachialindex (TBI) below 0.24 were enrolled in the presentstudy(21-23). The computerized tomographic angiography
(CTA) also demonstrated the site of arterial occlusionat the infrapopliteal level with poor distal artery run off.The patients suffering from stroke, valvular heartdiseases, cardiomyopathy, malignant diseases, chronicinfectious diseases such as AIDS and hepatitis as wellas those receiving blood transfusion within 4 weekspreceding the recruitment were excluded from thepresent study.
Cell Culture: Two hundred and fifty millilitersof blood were taken from the peripheral vein of thepatients in the present study, stored in a containerat the temperature of 2°C-8°C and transported to themanufacturing facility in Israel. The isolation andincubation of autologous ACPs were performed byTheravitae Co Ltd (Israel). Low-density synergeticcell populations (SCPs) were isolated as describedpreviously(16). To generate NMPB-ACPs, SCPs werecultured at a concentration of 1.5-3.0 x 106 cells/ml inX-vivo 15 serum-free medium (Cambrex, East Rutherford,NJ) supplemented with 10% autologous human serum,1-10 ng/ml VEGF(R&D Systems, Minneapolis, MN)and 5 IU/ml heparin (Kamada, Beit-Kama, Israel). Theprocess of obtaining the stem cell was performed forfive days.
Flow Cytometry: Prior to implantation, theNMPB-ACPs were harvested for analysis. The cellswere incubated in the dark, on ice, for 30 minutes, withspecific fluorochrome-conjugated CD34-APC (BDBiosciences, San Jose, CA) and CD31-PE (eBioscience,San Diego, CA), or with is otype-matched non-specificcontrols. To assess the cells potential to uptakeAc-LDL, NMPB-ACPs were loaded with 0.8 mg/mlDiO-Ac-LDL (BTI, Stoughton, MA,USA) for 15minutes at 37°C. Exclusion of dead cells from the finalanalysis was performed using 7-amino actinomycinD ([7-AAD], eBioscience) staining. Cell suspensiontriplicates of 500,000 cells each was stained, assessedby fluorescence-activated cell-sorting ([FACS],FACSCalibur, Becton Dickinson) and analyzed byCell Quest Pro software (Becton Dickinson). For eachreplication, at least 30,000 cells were acquired. Thepercentage of each marker was determined in eachtest tube. In addition, the mean and% coefficient ofvariance (%CV) were calculated for each marker. Theresults were reported as mean + standard error (SE) ofthe percentage of stained cells. The number of stainedcells was calculated by multiplying the number ofharvested cells with the staining percentagesobtained using the FACS.
ELISA assay for the detection of Inter-leukine-8 secretion: Samples of culture medium were

322 J Med Assoc Thai Vol. 92 No. 3 2009
collected from cells on the harvesting day. Secretion ofthe chemokines Interleukine-8 ([IL-8], also known asthe chemokine CXCL8) to the culture medium, wastested using commercial ELISA Kit (R&D systems Inc.MN, USA). Triplicates of standard curve consistingof seven dilutions and tested samples, each at fourdilutions, were analyzed. The intensity of the colorproportional to the IL-8 amount was measured using amicroplate reader (Multiskan EX) and Ascent Softwarefor Multiskan (Thermo Fisher Scientific, Inc, MA,USA). IL-8 concentration was determined relative tothe standard curve samples. The final concentrationwas expressed as IL-8 secreted per total cell dose.
The injection procedure was done in a proneposition with local anesthesia, sedation together withthe monitoring of vital signs, electrocardiography andoxygen saturation. The injection was performed intocalf muscles at 30 sites with one milliliter of stem cellsuspension for each site, which was 1.5 centimeterapart. After the procedure, the patient was observedin hospital for monitoring hemodynamic status andsystemic adverse events. Laboratory studies ofhematology, kidney, and liver function including thelevel of serum myoglobin were completely assessedbefore and after the procedure. The hemodynamicassessment of limb ischemia was performed by ABIand TBI at 1 and 3 months after the treatment. Theincrease of 0.15 of segmental pressure index wasconsidered significant improvement(24,25). The CTA wasrepeated 3 months post procedure. The assessment ofthe degree of collateral circulation and the evidenceof recanalization of the distal artery in CTA(26) wasperformed by the radiologist who was blinded to thepresent study. The primary end points of the clinicalefficacy assessment were absolute disappearance ofrest pain and complete healing of ischemic ulcer andstump of digital amputation. The follow up period wasat least 3 months post treatment.
ResultsSix male patients with the mean age of 65.5 +
14.7 (range 38.6-83.8) years were enrolled in the presentstudy. The clinical presentations were digital gangrenein four patients and ischemic ulcer in three patients(one patient had both gangrene and ulcer). One patientalso had limited intermittent claudication with 100 metermaximal walking distance (Table 1). All six patients inthe present study were classified as Fontaine stageIV(1). The average duration of clinical presentationswas 5.0 + 1.8 (range3.1-7.1) months. The risk factors ofatherosclerosis detected in this group were diabetes
mellitus in four (66.7%) patients, hypertension inthree (50%) patients, heavy smoking in three (50%)patients and hypercholesterolemia in one (16.7%)patient. Ischemic heart disease was found in three(50%) patients and two (33.3%) of them had previouscoronary bypass surgery. Prior to the present study,one patient had below the knee amputation on thecontralateral limb 5 years ago and the fifth toe amputa-tion on the affected limb one year ago. All six patientshad TBI below 0.24 and two patients had ABI at andbelow 0.4 (Table 1). CTA of the lower extremities alsodemonstrated poor distal artery run off which causedthe patients to be unsuitable for revascula-rization.Prior to the enrollment in the present study, ischemiculcer and distal gangrene in these patients were treatedfor at least two months without any improvement. Toeamputations were planned without the promisinglycomplete healing process. Below the knee amputationswere expected in all of them.
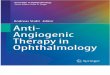
There was no change of hemodynamic statusafter taking 250 milliliters of peripheral blood from thepatients in the process of NMPB-ACPs production.The harvested cells, 54.5 x 106 + 10.2 x106 (mean + SE,n = 6) in number, were administered by thirty intra-muscular injections into the gastrocnemius muscle ofthe ischemic limb. The NMPB-ACPs were harvestedafter culturing exhibited high viability levels of 97.7%+ 0.6% (mean + SE, n = 6). Flow cytometry (FACS)assessment showed the expression of the stem cellmarkers CD34 in 19.0% + 2.4% (mean + SE, n = 6) ofthe cells, concomitant expression of CD31, uptake ofAc-LDL in 33.2% + 7.4% (mean + SE, n = 6) of the cellsand IL-8 ng/dose in 189.7% + 158.0% (mean + SE, n = 6)of the cells (Fig. 1).
In the immediate follow-up after the intra-muscular injection of NMPB-ACPs, five patients werehemodynamically stable. One patient developedthe symptoms of dyspnea during the night. Thesesymptoms were caused by fluid overload withimmediate response to diuretic therapy. Elevatedcardiac enzymes were detected even though thepatient had no symptom of angina. He refused toundergo the invasive evaluation of ischemic heartdisease. There were no abnormalities in the laboratorytests of hemotology, kidney and liver functionincluding the level of serum myoglobin. In the presentstudy, five patients (83.3%) had clinically significantimprovement of circulation at the distal limb adequatefor the complete healing (Table 1). Two of them hadthe complete healing of ischemic ulcer. Another twowith digital gangrene underwent toe amputation with

J Med Assoc Thai Vol. 92 No. 3 2009 323
Tabl
e 1.
Clin
ical
out
com
es, a
nkle
bra
chia
l ind
ex (A
BI)
, toe
bra
chia
l ind
ex (T
BI)
and
com
pute
rized
tom
ogra
phic
angi
ogra
phy
(CTA
) at b
asel
ine a
nd fo
llow
-up
No.
C
linic
al o
utco
mes
A
BI
T
BI
CTA
at 3
mon
thfo
llow
-up
visi
t
Bas
elin
e
3-6
mon
ths
Base
line
1 m
onth
3 m
onth
sBa
selin
e1
mon
th3
mon
ths
Incr
ease
dR
ecan
alisa
tion
colla
tera
lci
rcul
atio
n
1N
on-h
eale
d is
chem
ic u
lcer
atC
ompl
ete u
lcer
hea
ling
0.
77
0.92
*
0.85
0.
00**
0.
42*
0.
49*
+
+le
ft 1st
toe
2R
est p
ain
and
digi
tal g
angr
ene
Com
plet
e hea
ling
of
1.08
1.
09
0.92
0.
22
0.20
0.
46*
+
+at
righ
t 1st to
eto
e am
puta
tion
3D
igita
l gan
gren
e at r
ight
2nd
toe
Com
plet
e hea
ling
of
0.70
0.
70
0.90
*
0.10
0.
10
0.10
-
-to
e am
puta
tion
4N
on- h
eale
d Is
chem
ic u
lcer
atC
ompl
ete u
lcer
hea
ling
0.
55
0.80
*
0.89
*
0.22
0.
38*
0.
38*
-
+le
ft 1st t
oe a
nd li
mite
dIm
prov
emen
t of
inte
rmitt
ent c
laud
icat
ion
inte
rmitt
ent c
laud
icat
ion
(100
met
ers)
5D
igita
l gan
gren
e at l
eft 1
st toe
Sign
ifica
nt im
prov
emen
t
0.40
0.
40
NP
0.
00**
0.
00**
N
P
N
P
NP
of g
ranu
latio
n tis
sue
atba
se o
f toe
stu
mp
but
unde
rwen
t BK
A a
fter
infe
ctio
n du
e to
poo
rco
mpl
ianc
e6
Isch
emic
ulc
er an
d di
gita
lN
o im
prov
emen
t whi
ch
0.26
0.
31
0.31
0.
20
0.21
0.
21
-
-
gang
rene
at l
eft 5
th to
em
ight
rela
te to
cong
estiv
ehe
art f
ailu
re an
d fin
ally
unde
rwen
t BK
A
* Th
e inc
reas
e of 0
.15
of se
gmen
tal p
ress
ure i
ndex
was
cons
ider
ed si
gnifi
cant
impr
ovem
ent
** N
o flo
w, N
P: n
ot p
erfo
rmed
, BK
A: b
elow
kne
e am
puta
tion

324 J Med Assoc Thai Vol. 92 No. 3 2009
the complete healing of the stump. Among thesepatients, one also had an improvement of intermittentclaudication from 100 to 400 meters within threemonths and no symptom after six months. One patienthad significant improvement of healing with theadequate granulation tissue at the base of the first toestump (Fig. 2). Due to poor compliance and severefoot infection originated from the second and thirdtoes with septicemia, this patient subsequentlyunderwent below the knee amputation. On the contrary,one patient (16.7%) had no improvement after theadministration of NMPB-ACPs. The ischemic processof the affected limb was progressively worse, requiringbelow the knee amputation (Table 1). All patientssurvived the 6-month follow up period.
In hemodynamic assessment during the3-month follow up, two patients had an improvementin both ABI and TBI, one patient improved only inABI and another only in TBI. However, two patientshad no improvement in ABI or TBI. The CTA at threemonths post treatment demonstrated the recanalizationof distal artery in three patients and the increase ofcollateral circulation in two of them (Table 1). Fig. 3demonstrated the increase of collateral circulationand recanalization of the distal artery after theadministration of NMPB-ACPs.
DiscussionDespite technical advance in intervention and
surgical revascularization procedures, a substantialnumber of patients with peripheral arterial occlusivedisease and critical limb ischemia remain in whommajor amputation has to be considered the only finaloption(7). However, there were several studies of auto-transplantation of bone marrow origin cells(9,10) andG-CSF mobilized peripheral blood mononuclear cells inpatients with critical limb ischemia demonstrating theimprovement of ischemic status(11-15). Subsequently,these therapeutic modalities may enhance the oppor-tunity of limb salvage in those patients. Due to theharmful effect of G-CSF to cardiac patients(20), theuse of peripheral blood as raw material to provideangiogenic cell precursors without the stimulation ofbone marrow by injection of G-CSF is simpler, safer,and more suitable for the elderly patient with high-riskcomorbidities.
The present study illustrated that directintramuscular injection of NMPB-ACPs had improvedthe distal circulation in five patients (83.3%) with acritically ischemic limb by achieving complete ulceror toe stump healing in four (66.7%) patients and
Fig. 1 Representative illustration of flow cytometry(FACS) analysis performed on harvested NMPB-ACPs from one patient. (A) Cells size (assessedby Forward Scatter) and granularity (assessed bySide Scatter); (B) Concomitant expression of anti-CD31 and uptake of AC-LDL; (C and D) Matchedisotype control antibodies and specific anti-CD34expression
NMPB: ACPs: non-mobilized peripheral blood angiogeniccell precursors, AC-LDL: acetylated low density lipoprotein,FACS: fluorescence-activated cell-sorting
A B
C D
Fig. 2 The progression of left 1st toe status after the injec-tion of NMPB-ACPs in the fifth patient demon-strating the adequacy of granulation tissue at thebase of amputated wound for complete healing

J Med Assoc Thai Vol. 92 No. 3 2009 325
providing the adequate granulation tissue at the baseof first toe stump in one (16.7%) patient (Fig. 2). Theseresults indicated the efficiency of NMPB-ACPs incritical limb ischemia. Due to poor compliance andsubsequently extensive foot infection, below the kneeamputation was inevitable in the latter patient result-ing in the incomplete assessment of the healingprocess. The successful outcome was supported bythe improvement of ABI and/or TBI in four patientswho had complete ulcer and/or toe stump healing andthe evidence of CTA improvement in three patientswith increased collateral circulation and/or therecanalization in the distal artery. However, there wasno improvement of distal circulation in one patient(16.7%) who had dyspnea due to fluid overload afterthe injection. This clinical result was also confirmed byno change of ABI and TBI and no change in the degreeof collateral circulation and recanalization in CTA.The compromised cardiac status may play a role of theproliferation of injected progenitor cells. In addition,this patient had the most severe ischemia in this groupsuffering from both ischemic ulcer and digital gangrene.The ABI and TBI of this patient were also the lowest inthis group. It is worth identifying the level of ischemia
at which NMPB-ACPs is unable to improve the circula-tion. There was no abnormality in the laboratory studyof hematology, kidney, and liver function as well asthe level of serum myoglobin in all patients after thetreatment, indicating that the injection of NMPB-ACPswas safe for patients with critical limb ischemia.
In conclusion, intramuscular injection ofNMPB-ACPs may provide safety, and feasibility forthe enhancement of limb salvage in patients withcritical ischemic limb. The real efficacy of NMPB-ACPsfor ischemic limb requires randomized control trials ina larger series of such patients.
AcknowledgmentsThe authors thank Professor V. Thamlikitkul
for his advice and assistance, Asssociate ProfessorP. Vessakosol (PhD) and S. Tunpornpituk in thepreparation of this manuscript.
References1. Norgren L, Hiatt WR, Dormandy JA, Nehler
MR, Harris KA, Fowkes FG, et al. Inter-societyconsensus for the management of peripheralarterial disease. Int Angiol 2007; 26: 81-157.
2. Critical limb ischaemia: management and outcome.Report of a national survey. The Vascular SurgicalSociety of Great Britain and Ireland. Eur J VascEndovasc Surg 1995; 10: 108-13.
3. Mutirangura P, Ruangsetakit C, Wongwanit C,Sermsathanasawadi N, Chinsakchai K. Athero-sclerosis obliterans of the lower extremities in Thaipatients. J Med Assoc Thai 2006; 89: 1612-20.
4. Hertzer NR, Beven EG, Young JR, O’Hara PJ,Ruschhaupt WF 3rd, Graor RA, et al. Coronaryartery disease in peripheral vascular patients. Aclassification of 1000 coronary angiograms andresults of surgical management. Ann Surg 1984;199: 223-33.
5. Gentile AT, Taylor LM Jr, Moneta GL, Porter JM.Prevalence of asymptomatic carotid stenosis inpatients undergoing infrainguinal bypass surgery.Arch Surg 1995; 130: 900-4.
6. Turnipseed WD, Berkoff HA, Belzer FO. Post-operative stroke in cardiac and peripheral vasculardisease. Ann Surg 1980; 192: 365-8.
7. Nehler MR, Hiatt WR, Taylor LM Jr. Isrevascularization and limb salvage always thebest treatment for critical limb ischemia? J VascSurg 2003; 37: 704-8.
8. Nehler MR, Wolford H. Natural history andnonoperative treatment of chronic lower extremity
Fig. 3 Demonstration of the increase of collateral circula-tion and recanalization of the distal artery beforeand after the administration of NMPB-ACPs inthe second patient (Arrow: recanalisation of rightperoneal artery)

326 J Med Assoc Thai Vol. 92 No. 3 2009
ischemia. In: Rutherford RB, editor. Vascularsurgery. 6th ed. Philadelphia: Elsevier Saunders;2005: 1083-5.
9. Saigawa T, Kato K, Ozawa T, Toba K, Makiyama Y,Minagawa S, et al. Clinical application of bonemarrow implantation in patients with arterio-sclerosis obliterans, and the association betweenefficacy and the number of implanted bonemarrow cells. Circ J 2004; 68: 1189-93.
10. Tateishi-Yuyama E, Matsubara H, Murohara T,Ikeda U, Shintani S, Masaki H, et al. Therapeuticangiogenesis for patients with limb ischaemia byautologous transplantation of bone-marrow cells:a pilot study and a randomised controlled trial.Lancet 2002; 360: 427-35.
11. Arai M, Misao Y, Nagai H, Kawasaki M, NagashimaK, Suzuki K, et al. Granulocyte colony-stimulatingfactor: a noninvasive regeneration therapy fortreating atherosclerotic peripheral artery disease.Circ J 2006; 70: 1093-8.
12. Fadini GP, Avogaro A. Autologous transplantationof granulocyte colony-stimulating factor-mobilizedperipheral blood mononuclear cells improvescritical limb ischemia in diabetes. Diabetes Care2006; 29: 478-9.
13. Lenk K, Adams V, Lurz P, Erbs S, Linke A, Gielen S,et al. Therapeutical potential of blood-derivedprogenitor cells in patients with peripheral arterialocclusive disease and critical limb ischaemia. EurHeart J 2005; 26: 1903-9.
14. Kawamura A, Horie T, Tsuda I, Abe Y, Yamada M,Egawa H, et al. Clinical study of therapeutic angio-genesis by autologous peripheral blood stem cell(PBSC) transplantation in 92 patients with criticallyischemic limbs. J Artif Organs 2006; 9: 226-33.
15. Ishida A, Ohya Y, Sakuda H, Ohshiro K,Higashiuesato Y, Nakaema M, et al. Autologousperipheral blood mononuclear cell implantationfor patients with peripheral arterial diseaseimproves limb ischemia. Circ J 2005; 69: 1260-5.
16. Porat Y, Porozov S, Belkin D, Shimoni D, Fisher Y,Belleli A, et al. Isolation of an adult blood-derivedprogenitor cell population capable of differentiation
into angiogenic, myocardial and neural lineages.Br J Haematol 2006; 135: 703-14.
17. Losordo DW, Schatz RA, White CJ, Udelson JE,Veereshwarayya V, Durgin M, et al. Intramyocardialtransplantation of autologous CD34+ stem cellsfor intractable angina: a phase I/IIa double-blind,randomized controlled trial. Circulation 2007; 115:3165-72.
18. Fukumoto Y, Miyamoto T, Okamura T, Gondo H,Iwasaki H, Horiuchi T, et al. Angina pectorisoccurring during granulocyte colony-stimulatingfactor-combined preparatory regimen for auto-logous peripheral blood stem cell transplantationin a patient with acute myelogenous leukaemia.Br J Haematol 1997; 97: 666-8.
19. Hill JM, Syed MA, Arai AE, Powell TM, Paul JD,Zalos G, et al. Outcomes and risks of granulocytecolony-stimulating factor in patients with coronaryartery disease. J Am Coll Cardiol 2005; 46: 1643-8.
20. Matsubara H. Risk to the coronary arteries ofintracoronary stem cell infusion and G-CSFcytokine therapy. Lancet 2004; 363: 746-7.
21. Yao ST. Haemodynamic studies in peripheralarterial disease. Br J Surg 1970; 57: 761-6.
22. Vollrath KD, Salles-Cunha SX, Vincent D, TowneJB, Bernhard VM. Noninvasive measurement oftoe systolic pressure. Bruit 1980; 4: 27-30.
23. Zierler RE, Sumner DS. Physiologic assessment ofperipheral arterial occlusive disease. In: RutherfordRB, editor. Vascular surgery. 6th ed. Philadelphia:Elsevier Saunders; 2005: 197-222.
24. Baker JD, Dix DE. Variability of Doppler anklepressures with arterial occlusive disease: anevaluation of ankle index and brachial-anklepressure gradient. Surgery 1981; 89: 134-7.
25. Johnston KW, Hosang MY, Andrews DF.Reproducibility of noninvasive vascular labora-tory measurements of the peripheral circulation. JVasc Surg 1987; 6: 147-51.
26. Sun Z. Diagnostic value of color duplex ultra-sonography in the follow-up of endovascularrepair of abdominal aortic aneurysm. J Vasc IntervRadiol 2006; 17: 759-64.
Recommended