Endometrial Cancer: Current Status of
Radiation
William Small Jr., MD
Professor and Chairman
Loyola University, Chicago
Learning Objectives
Review the patterns of recurrence for
endometrial cancer.
Review the role and techniques of radiation for
early stage endometrial cancer.
Review the role of radiation in advanced stage
endometrial cancer.
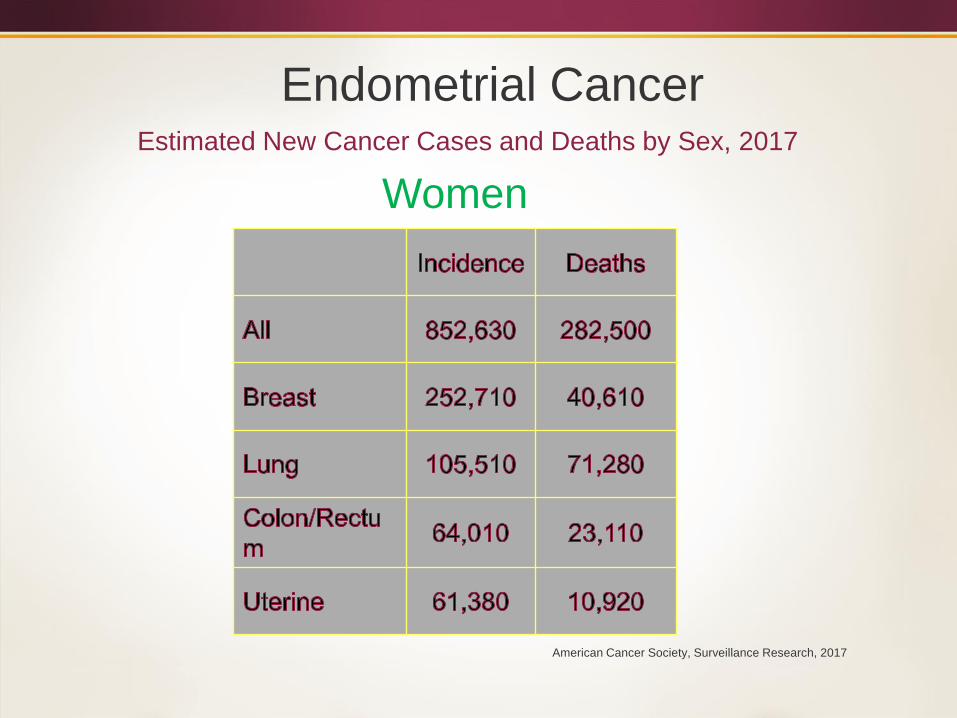
Estimated New Cancer Cases and Deaths by Sex, 2017
Endometrial Cancer
Women
American Cancer Society, Surveillance Research, 2017
“The reports of my death have
been greatly exaggerated.”
-Mark Twain
“There are three kinds of lies: Lies,
Damned Lies, and Statistics.”
-Benjamin Disraeli
-Mark Twain
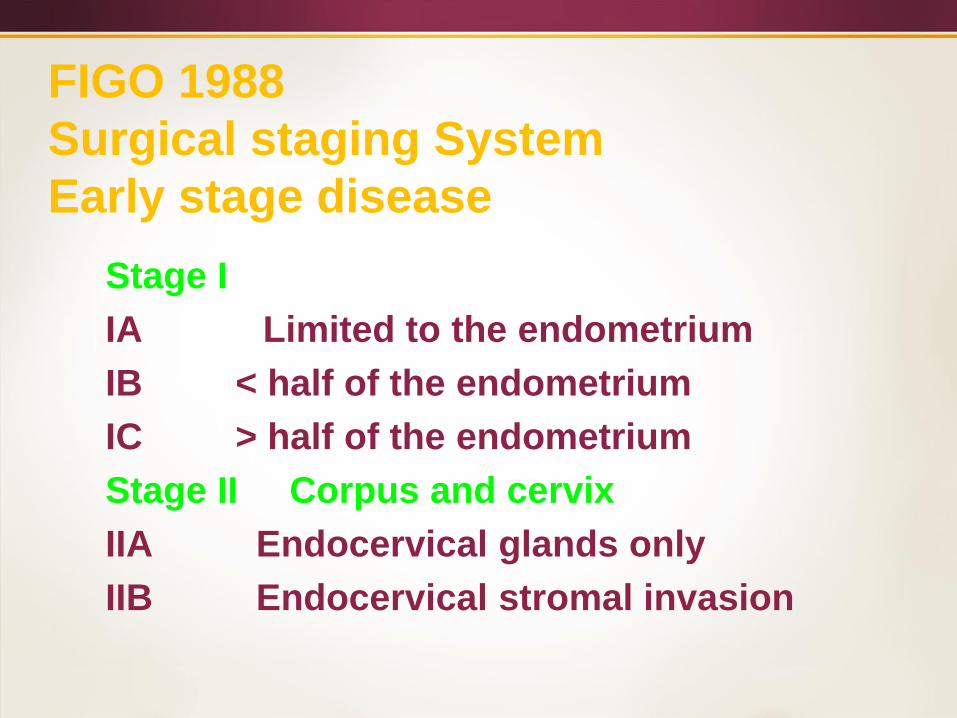
FIGO 1988
Surgical staging System
Early stage disease
Stage I
IA Limited to the endometrium
IB < half of the endometrium
IC > half of the endometrium
Stage II Corpus and cervix
IIA Endocervical glands only
IIB Endocervical stromal invasion
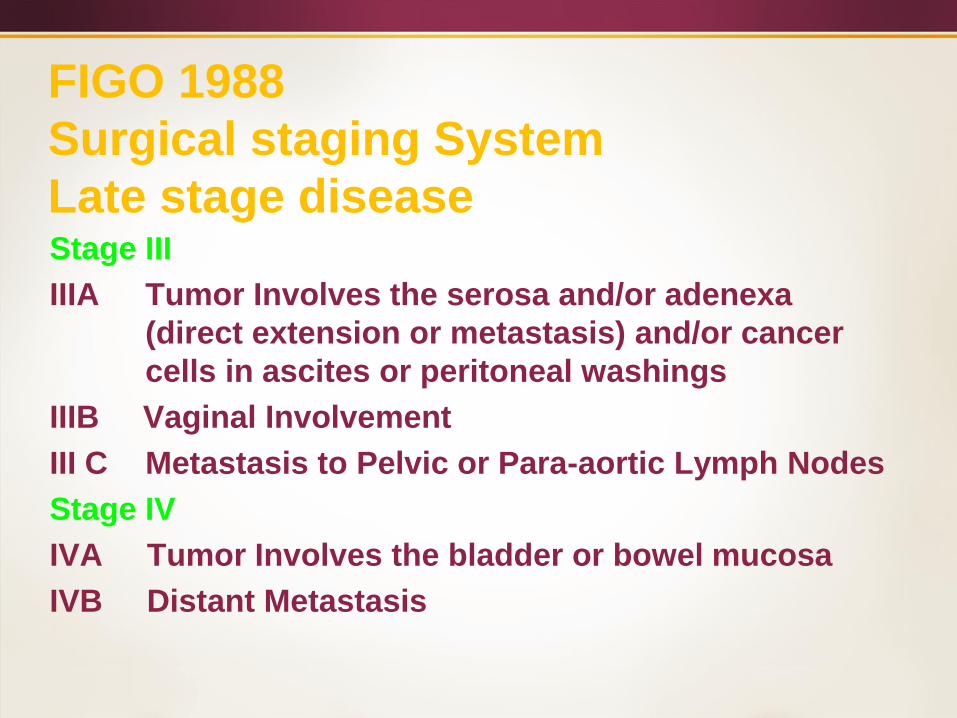
FIGO 1988
Surgical staging System
Late stage diseaseStage III
IIIA Tumor Involves the serosa and/or adenexa
(direct extension or metastasis) and/or cancer
cells in ascites or peritoneal washings
IIIB Vaginal Involvement
III C Metastasis to Pelvic or Para-aortic Lymph Nodes
Stage IV
IVA Tumor Involves the bladder or bowel mucosa
IVB Distant Metastasis
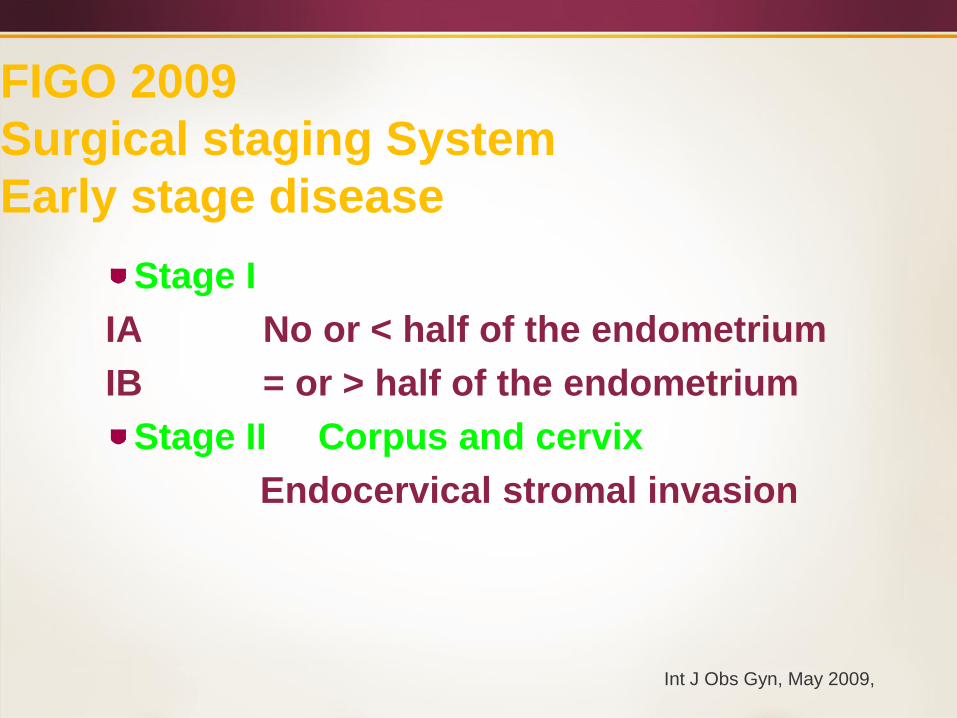
FIGO 2009
Surgical staging System
Early stage disease
Stage I
IA No or < half of the endometrium
IB = or > half of the endometrium
Stage II Corpus and cervix
Endocervical stromal invasion
Int J Obs Gyn, May 2009,
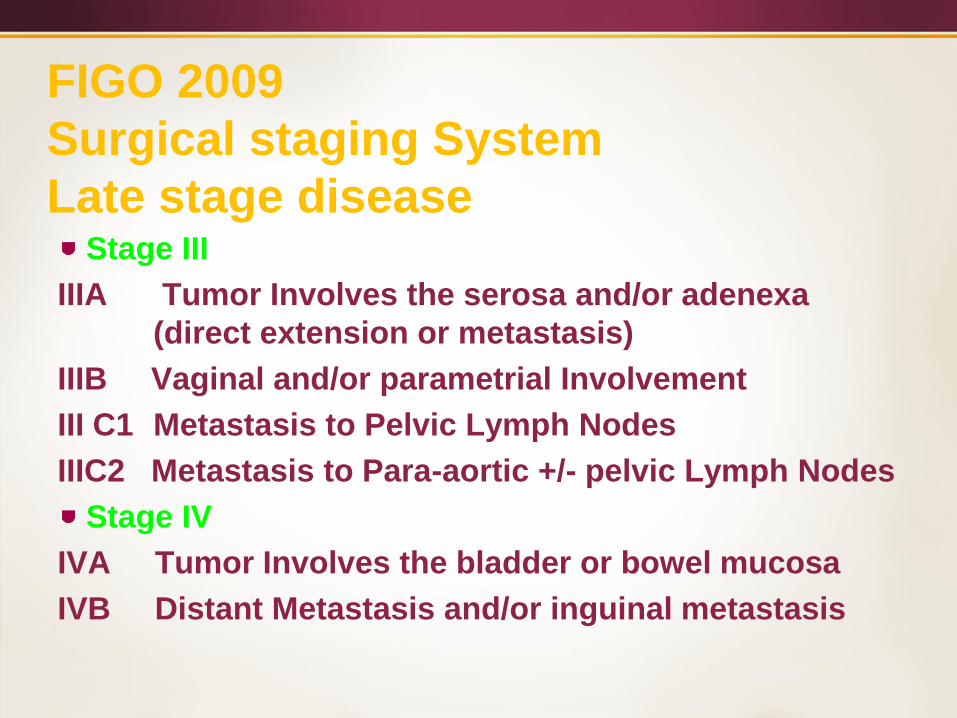
FIGO 2009
Surgical staging System
Late stage diseaseStage III
IIIA Tumor Involves the serosa and/or adenexa
(direct extension or metastasis)
IIIB Vaginal and/or parametrial Involvement
III C1 Metastasis to Pelvic Lymph Nodes
IIIC2 Metastasis to Para-aortic +/- pelvic Lymph Nodes
Stage IV
IVA Tumor Involves the bladder or bowel mucosa
IVB Distant Metastasis and/or inguinal metastasis
Post Operative Radiotherapy
Early Stage Disease
All Patients
Receive Adjuvant RT
Even Low Grade
Minimally Invasive
Tumors
Center A
No Patients
Receive adjuvant RT
Even High Grade
Deeply Invasive
Tumors
Center B
Very contentious Disease
Postoperative RT Rationale
Early stage patient with adverse pathologic features
are at risk for extra uterine disease and recurrence
Most commonly cited pathologic factors
-Myometrial Invasion (MI)
-Tumor Grade
-Cervical involvement
- Age
- LVSI
Importance demonstrated in GOG33
Unclear what these number would
be in the face of negative imaging
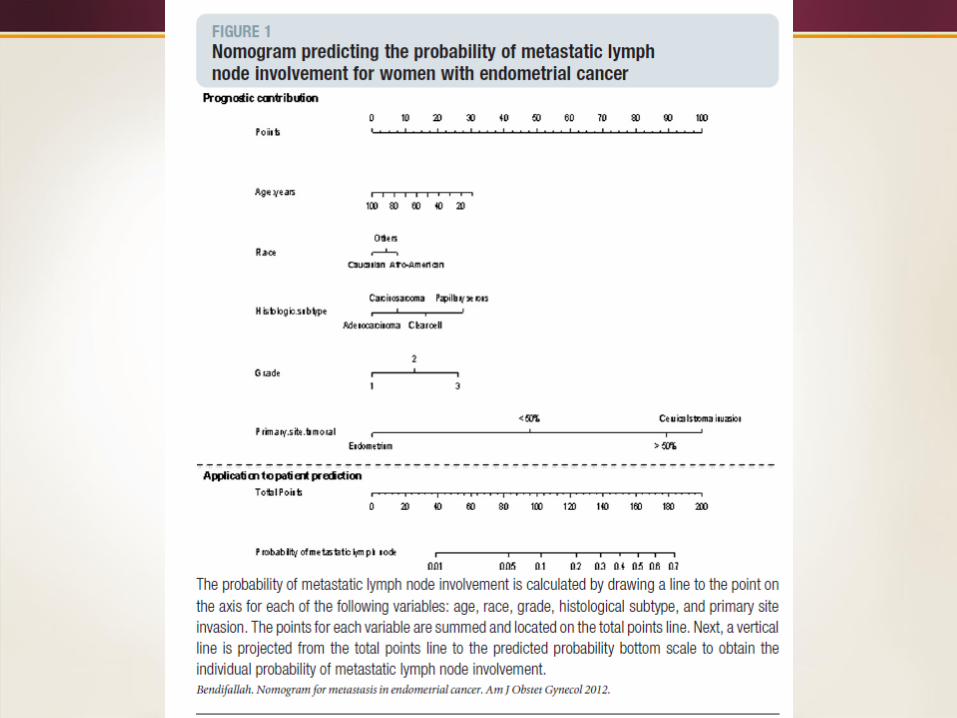
Predicting Lymph Node
Metastasis
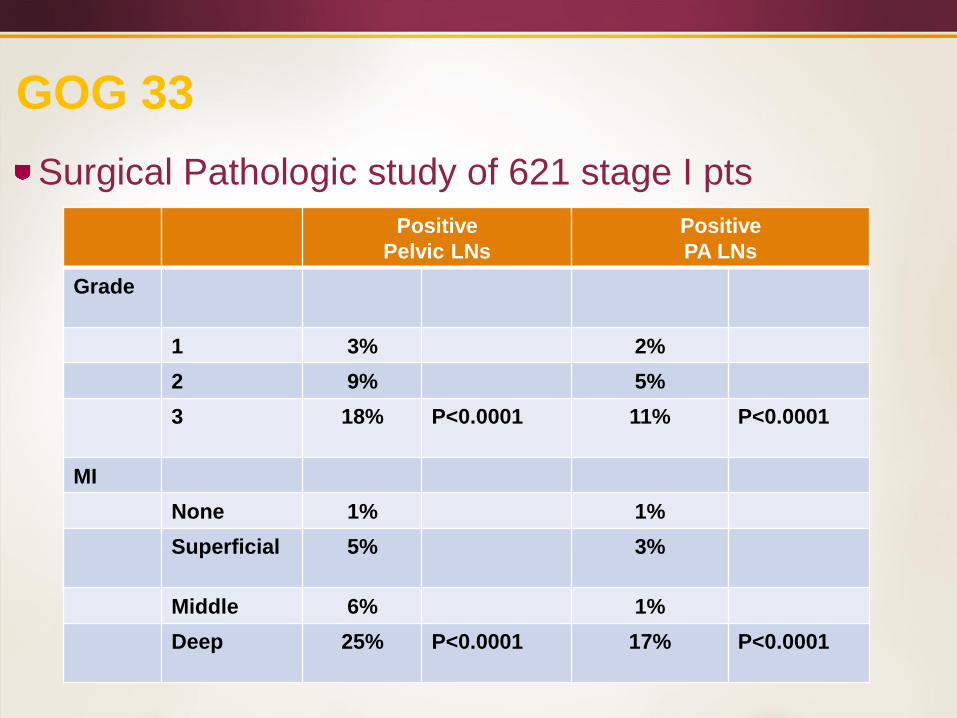
GOG 33
Surgical Pathologic study of 621 stage I pts
Positive
Pelvic LNs
Positive
PA LNs
Grade
1 3% 2%
2 9% 5%
3 18% P<0.0001 11% P<0.0001
MI
None 1% 1%
Superficial 5% 3%
Middle 6% 1%
Deep 25% P<0.0001 17% P<0.0001
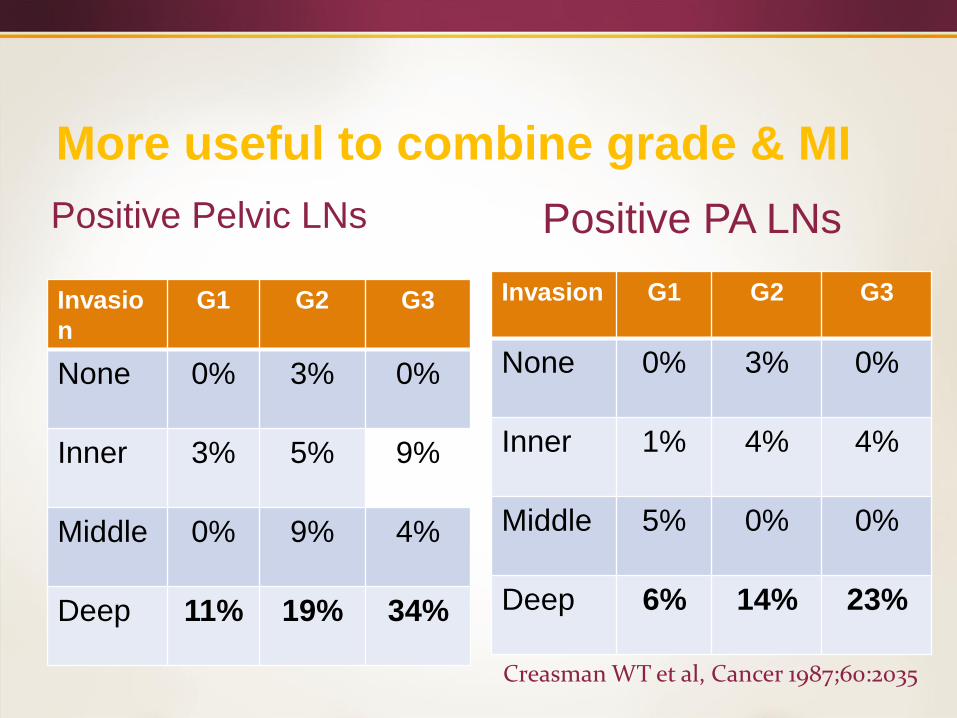
More useful to combine grade & MI
Positive Pelvic LNs
Invasio
n
G1 G2 G3
None 0% 3% 0%
Inner 3% 5% 9%
Middle 0% 9% 4%
Deep 11% 19% 34%
Invasion G1 G2 G3
None 0% 3% 0%
Inner 1% 4% 4%
Middle 5% 0% 0%
Deep 6% 14% 23%
Positive PA LNs
Creasman WT et al, Cancer 1987;60:2035
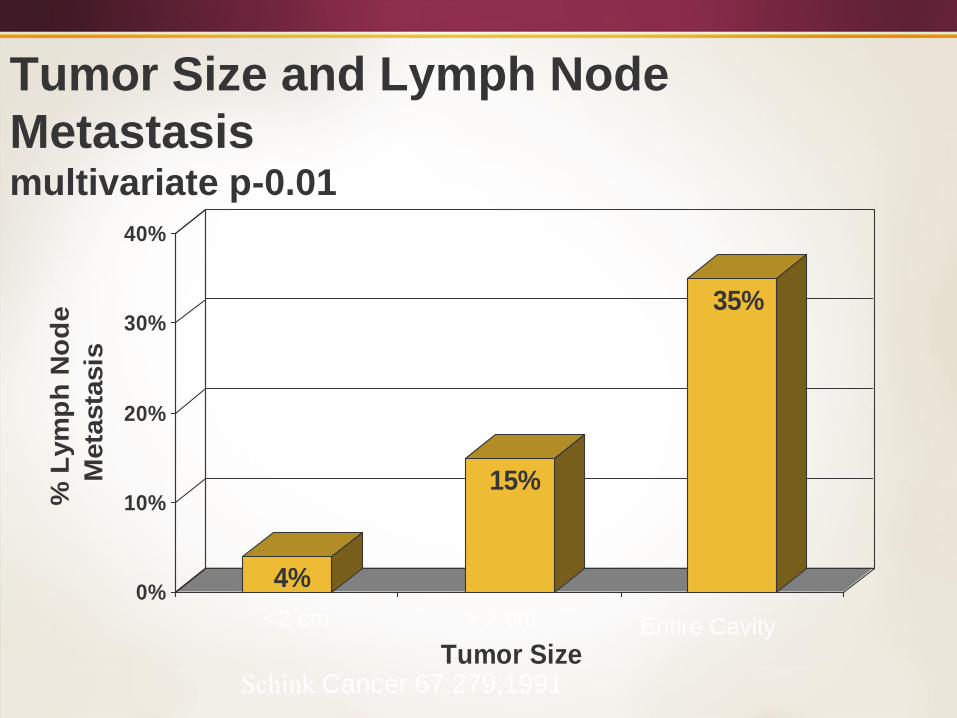
Tumor Size and Lymph Node
Metastasismultivariate p-0.01
4%
15%
35%
0%
10%
20%
30%
40%
% L
ym
ph
No
de
Meta
sta
sis
Tumor Size
<2 cm > 2 cm Entire Cavity
Schink Cancer 67:279;1991
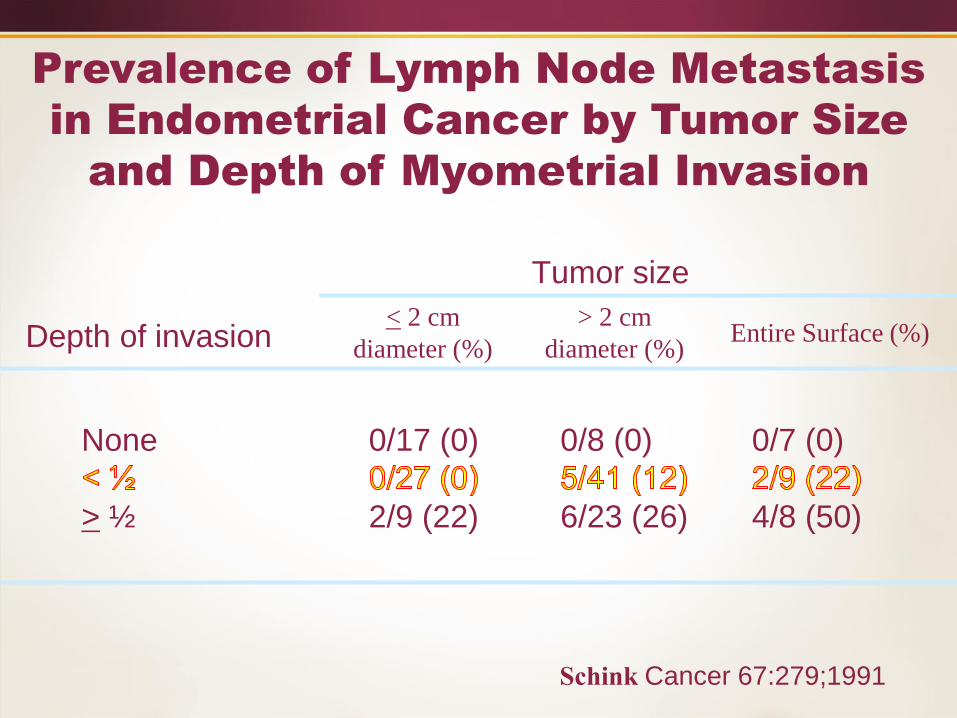
Tumor size
Depth of invasion
None 0/17 (0) 0/8 (0) 0/7 (0)
> ½ 2/9 (22) 6/23 (26) 4/8 (50)
Prevalence of Lymph Node Metastasis
in Endometrial Cancer by Tumor Size
and Depth of Myometrial Invasion
< 2 cm
diameter (%)
> 2 cm
diameter (%)
Schink Cancer 67:279;1991
Entire Surface (%)

Tumor size
Tumor Grade
I 1/27 (4) 1/26 (4) 0/7 (0)
II 0/19 (0) 5/28 (18) 2/4 (50)
III 1/7 (14) 5/18 (28) 4/6 (67)
< 2 cm
diameter (%)
> 2 cm
diameter (%)Entire Surface (%)
Schink Cancer 67:279;1991
Prevalence of Lymph Node Metastasis
in Endometrial Cancer by Tumor Size
and Grade
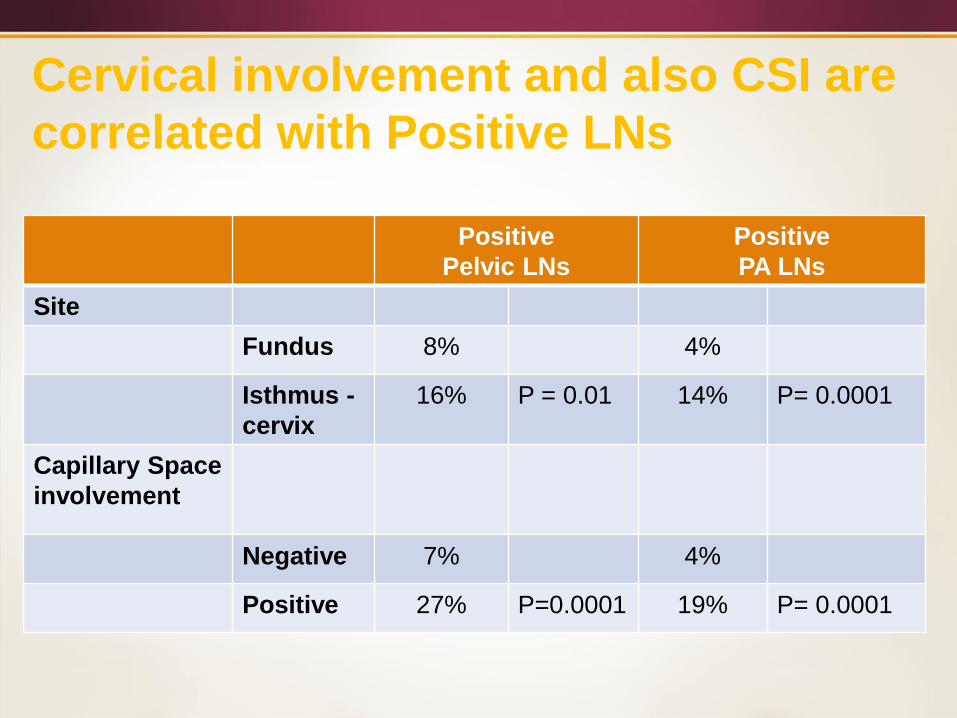
Cervical involvement and also CSI are
correlated with Positive LNs
Positive
Pelvic LNs
Positive
PA LNs
Site
Fundus 8% 4%
Isthmus -
cervix
16% P = 0.01 14% P= 0.0001
Capillary Space
involvement
Negative 7% 4%
Positive 27% P=0.0001 19% P= 0.0001
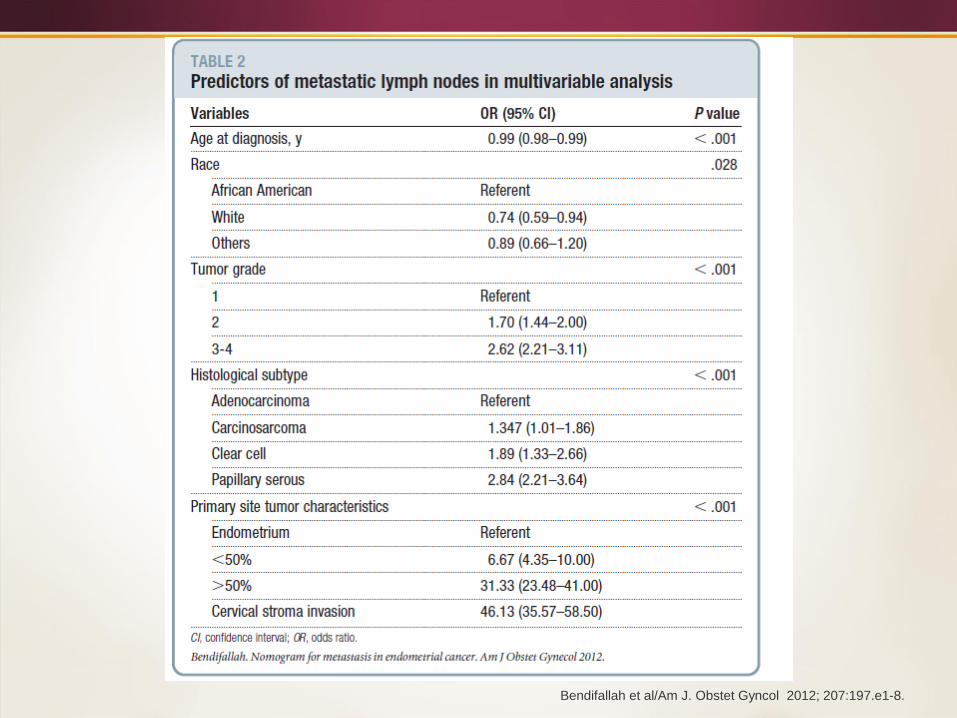
Bendifallah et al/Am J. Obstet Gyncol 2012; 207:197.e1-8.
What evidence supports the use of
Adjuvant Radiation Therapy in
Stage I & II Endometrial
Carcinoma ?
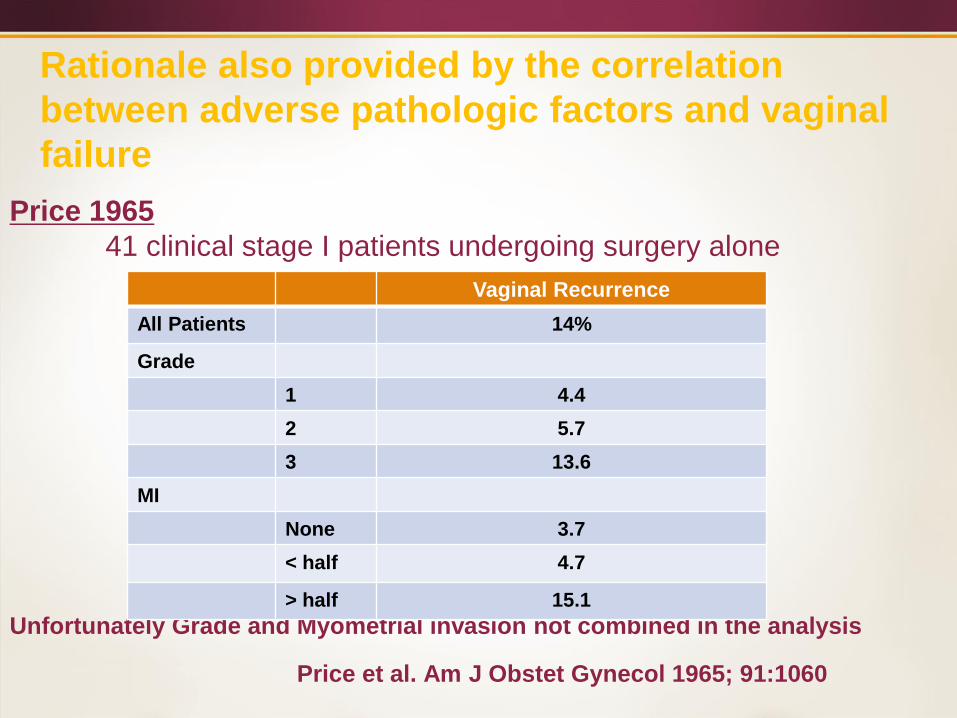
Rationale also provided by the correlation
between adverse pathologic factors and vaginal
failure
Price 1965
41 clinical stage I patients undergoing surgery alone
Unfortunately Grade and Myometrial invasion not combined in the analysis
Price et al. Am J Obstet Gynecol 1965; 91:1060
Vaginal Recurrence
All Patients 14%
Grade
1 4.4
2 5.7
3 13.6
MI
None 3.7
< half 4.7
> half 15.1
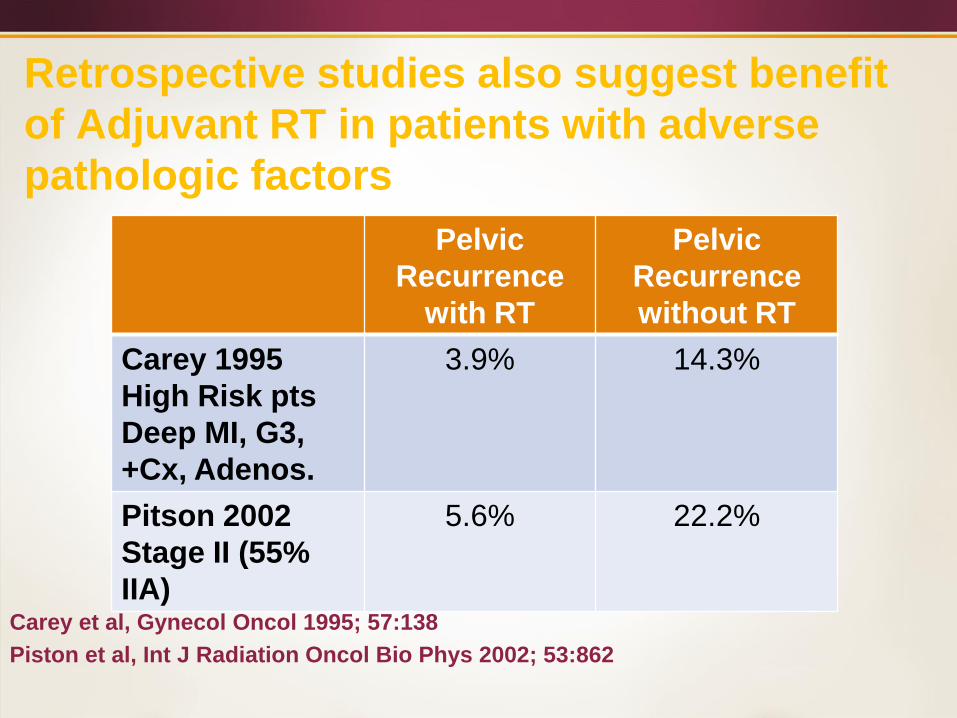
Retrospective studies also suggest benefit
of Adjuvant RT in patients with adverse
pathologic factors
Carey et al, Gynecol Oncol 1995; 57:138
Piston et al, Int J Radiation Oncol Bio Phys 2002; 53:862
Pelvic
Recurrence
with RT
Pelvic
Recurrence
without RT
Carey 1995
High Risk pts
Deep MI, G3,
+Cx, Adenos.
3.9% 14.3%
Pitson 2002
Stage II (55%
IIA)
5.6% 22.2%
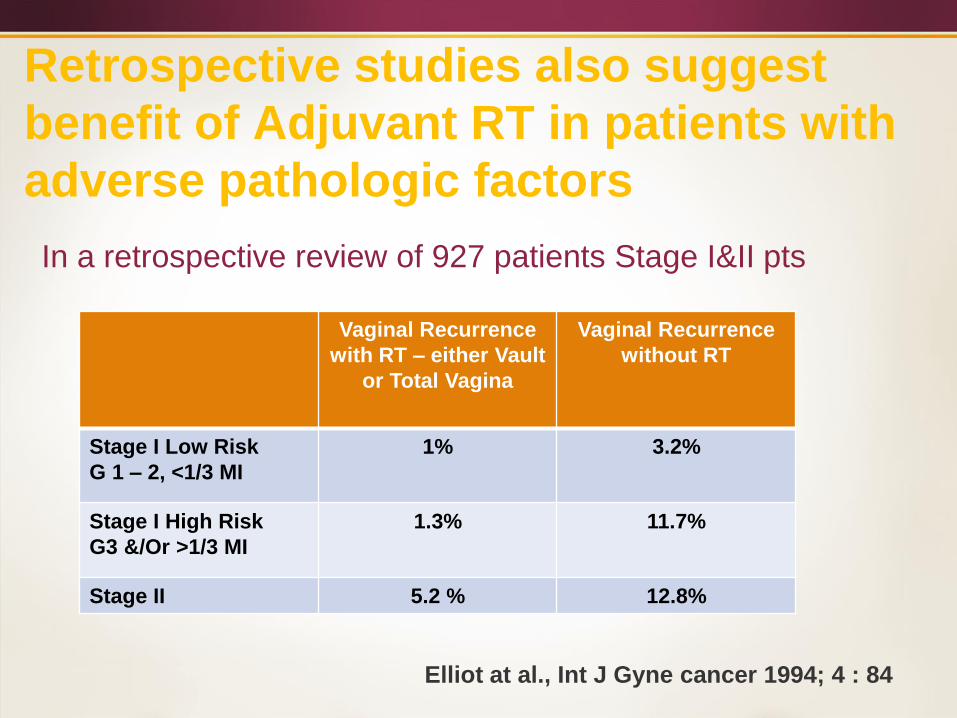
Retrospective studies also suggest
benefit of Adjuvant RT in patients with
adverse pathologic factors
In a retrospective review of 927 patients Stage I&II pts
Elliot at al., Int J Gyne cancer 1994; 4 : 84
Vaginal Recurrence
with RT – either Vault
or Total Vagina
Vaginal Recurrence
without RT
Stage I Low Risk
G 1 – 2, <1/3 MI
1% 3.2%
Stage I High Risk
G3 &/Or >1/3 MI
1.3% 11.7%
Stage II 5.2 % 12.8%
Post operative RT Stage I & II Disease
Five prospective randomized trials have been
conducted to evaluate post operative
radiotherapy in early stage disease
Norwegian Trial
PORTEC 1
GOG 99
ASTEC/EN 5
PORTEC 2
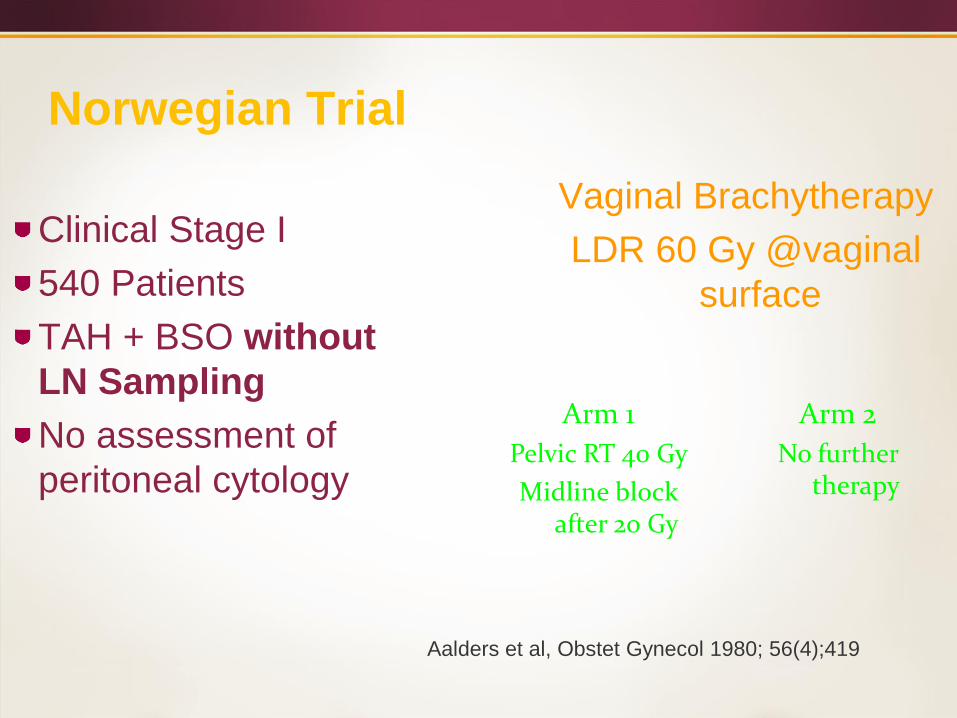
Norwegian Trial
Clinical Stage I
540 Patients
TAH + BSO without
LN Sampling
No assessment of
peritoneal cytology
Vaginal Brachytherapy
LDR 60 Gy @vaginal
surface
Arm 1
Pelvic RT 40 Gy
Midline block after 20 Gy
Arm 2
No further therapy
Aalders et al, Obstet Gynecol 1980; 56(4);419
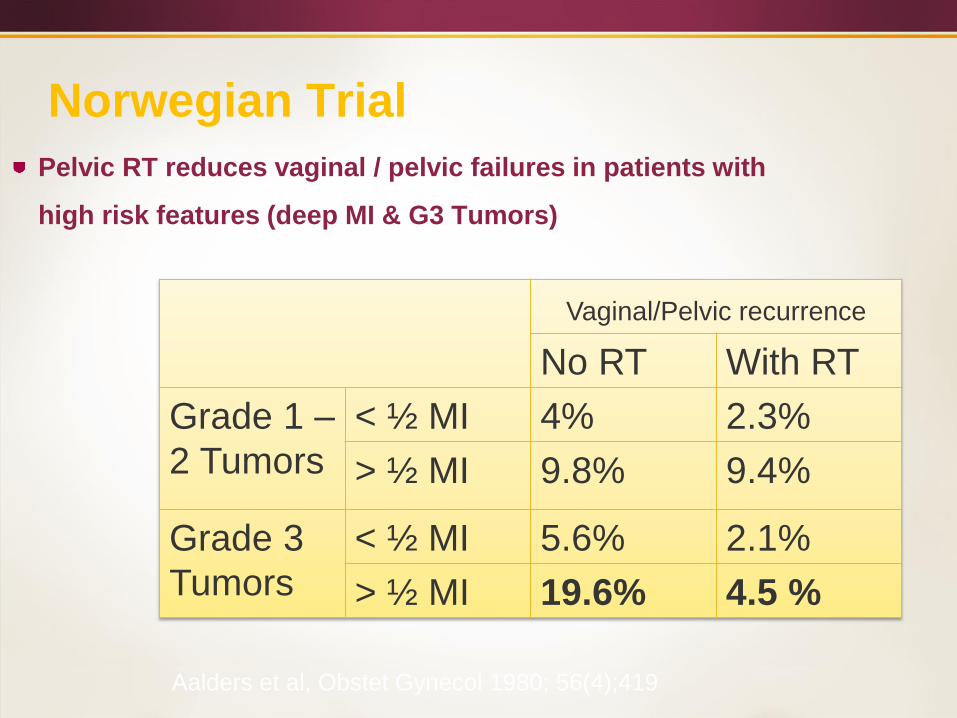
Norwegian Trial
Pelvic RT reduces vaginal / pelvic failures in patients with
high risk features (deep MI & G3 Tumors)
Vaginal/Pelvic recurrence
No RT With RT
Grade 1 –
2 Tumors
< ½ MI 4% 2.3%
> ½ MI 9.8% 9.4%
Grade 3
Tumors
< ½ MI 5.6% 2.1%
> ½ MI 19.6% 4.5 %
Aalders et al, Obstet Gynecol 1980; 56(4);419
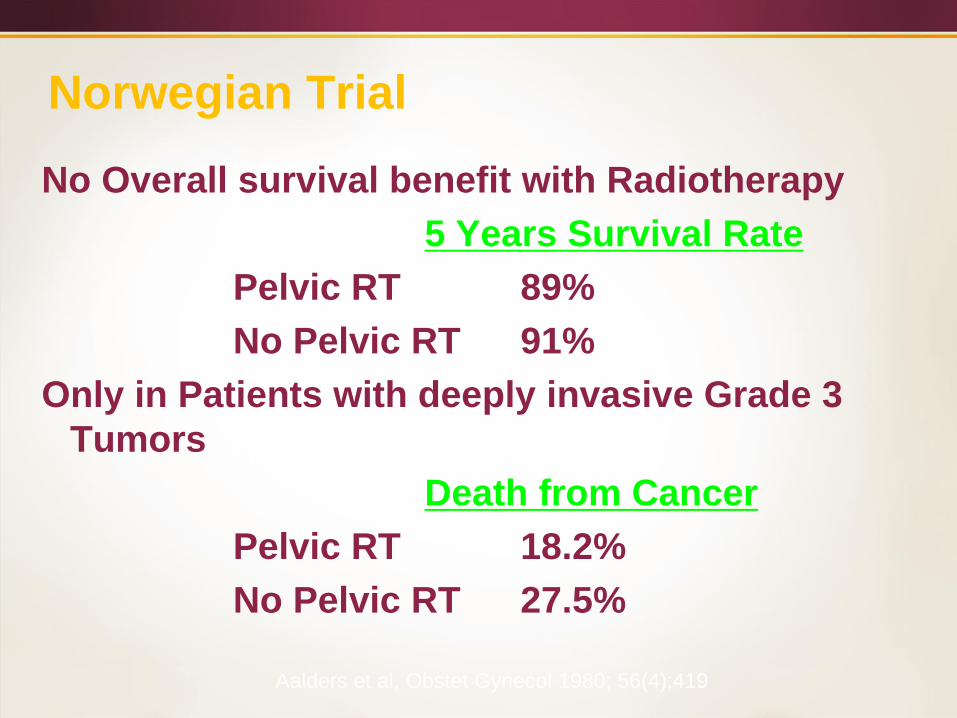
Norwegian Trial
No Overall survival benefit with Radiotherapy
5 Years Survival Rate
Pelvic RT 89%
No Pelvic RT 91%
Only in Patients with deeply invasive Grade 3
Tumors
Death from Cancer
Pelvic RT 18.2%
No Pelvic RT 27.5%
Aalders et al, Obstet Gynecol 1980; 56(4);419
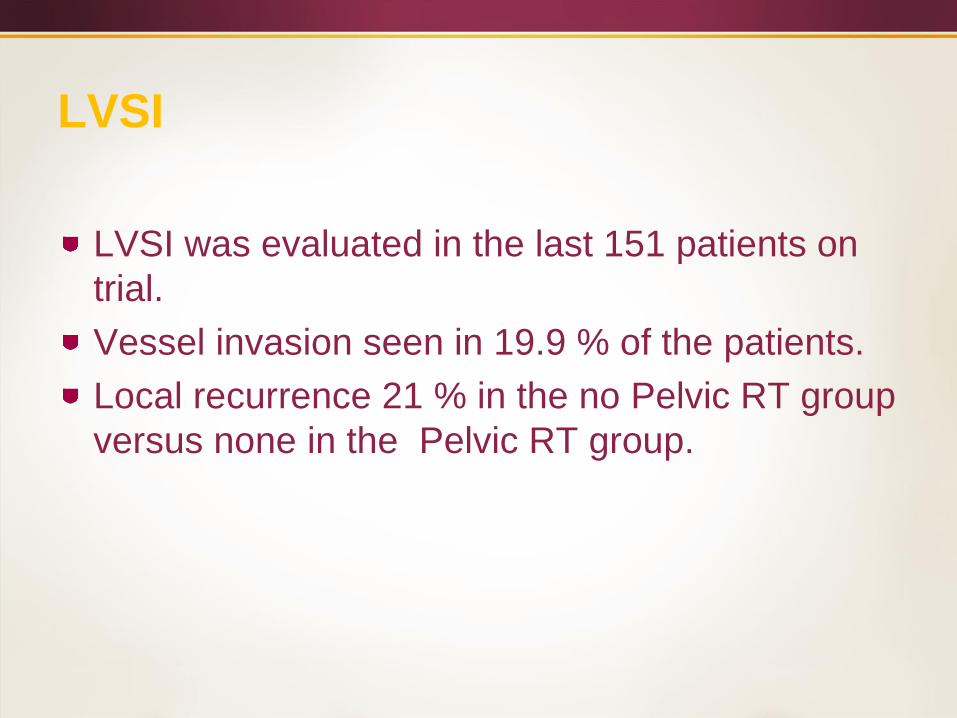
LVSI
LVSI was evaluated in the last 151 patients on
trial.
Vessel invasion seen in 19.9 % of the patients.
Local recurrence 21 % in the no Pelvic RT group
versus none in the Pelvic RT group.
Aadlers Trial: Conclusions
Grade 3> 50 % invasion – pelvic RT.
All patients with LVSI receive pelvic RT
All other patients with invasion receive
VBT.
PORTEC Trial
Post Operative Radiation Therapy in
Endometrial Carcinoma
Selected Clinical Stage I
Grade 1 > ½ MI
Grade 2 any MI
Grade 3 < ½ MI
715 Patients
TAH + BSO without LN
Sampling
All histologies
Regimen 1
Pelvic radiotheraoy
46 Gy / 23 Fractions
No Vaginal Brachytherapy
• Regimen 2
No further Treatment
HIR Definition
Age > 60
Grade 3
Invasion >50%
HIR defined as: 2 of those 3 factors present
(except for grade 3 with deep invasion = high
risk, eligible for PORTEC3)
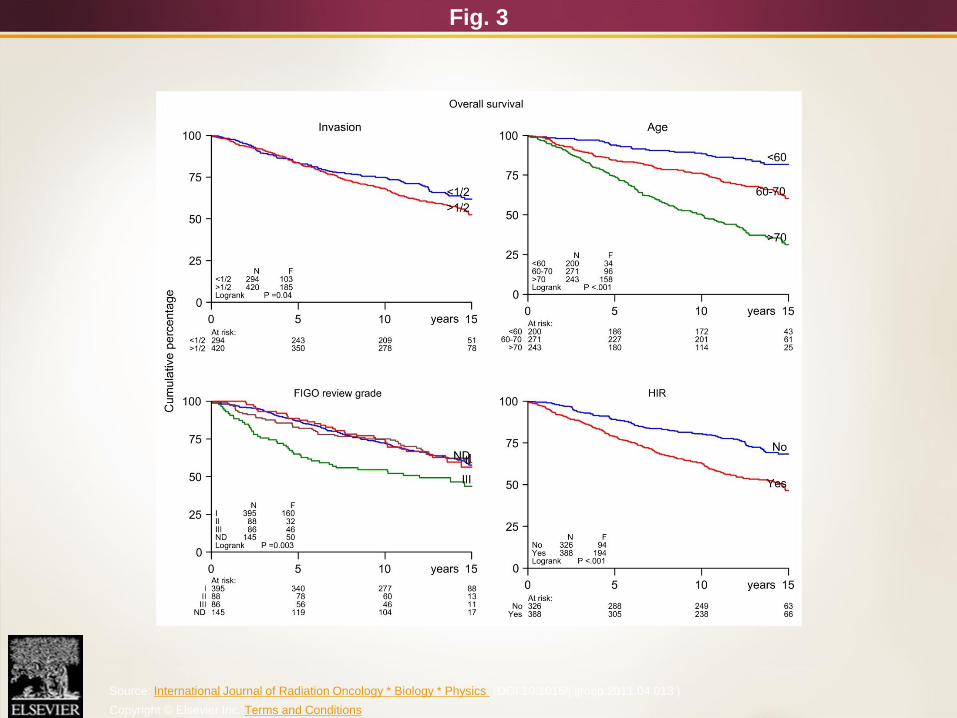
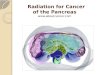
Fig. 3
Source: International Journal of Radiation Oncology * Biology * Physics (DOI:10.1016/j.ijrobp.2011.04.013 )
Copyright © Elsevier Inc. Terms and Conditions
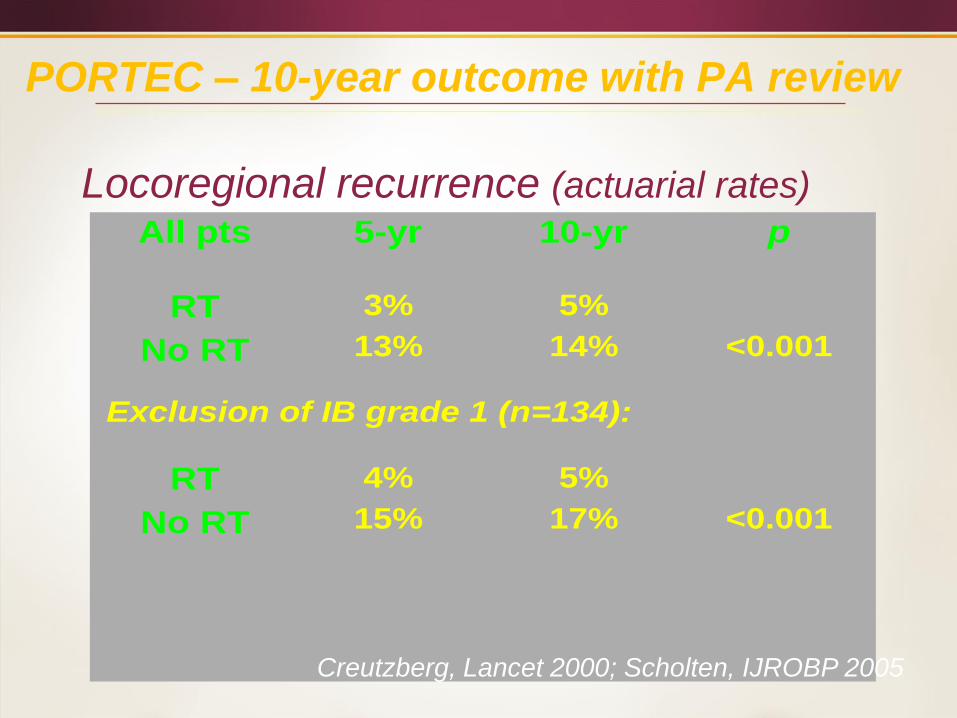
PORTEC – 10-year outcome with PA review
All pts 5-yr
10-yr p
RT
No RT
3%
13%
5%
14%
<0.001
Exclusion of IB grade 1 (n=134):
RT
No RT
4%
15%
5%
17%
<0.001
Locoregional recurrence (actuarial rates)
Creutzberg, Lancet 2000; Scholten, IJROBP 2005
PORTEC – 15-year outcome
( Median f/u: 13.3 Years)
Locoregional recurrence (actuarial rates)
5.8 % in the Radiotherapy Arm
15.5 % in the NAT Arm
Nout et al; JCO, 2011
Site of Loco-regional Recurrences
74% of the locoregional recurrences were isolated
vaginal recurrences.
Nout et al; JCO, 2011
GOG 99 Trial
Stage IB - II (Occult)
Pap/Serous-Clear Cell
Excluded
392 Patients
TAH + BSO with
selective Bilateral
Pelvic & Para- aortic
lymphadenectomy
Assessment of
peritoneal cytology
Regimen 1
Pelvic radiotheraoy
50.4 Gy / 1.8 Gy/ Fraction
No Vaginal Brachytherapy
• Regimen 2
No further Treatment
Keys et al. Gynecol Oncol 2004; 92;744
Overall Results
Median follow-up of surviving patients – 68 months.
The 24-month cumulative incidence of recurrence
(CIR) rate was 3% in the RT group and 12 % in the
no additional therapy group.
13 of the 18 loco-regional recurrences in the NAT
arm were in the vaginal vault (72%)
Overall Results
CIR at 24 months of isolated local (vagina or pelvic)
1.6% versus 7.4%
48 month Kaplan-Meier estimates for survival –
86% in the NAT group, 92 % in RT group (p=0.55).
The GI, GU, Cutaneous and Hematological side
effects were significantly higher in the RT group.
HIR group (GOG-99)
HIR (high intermediate risk):
at least 70 yr with any other risk factor
at least 50 yr with any 2 other risk factor
any age with all 3 other factors
Prognostic factors:
› advanced age
› high grade (2 or 3)
› outer 33% myometrial invasion
› lymph-vascular space invasion (LVI)
Keys, Gynecol Oncol 2004
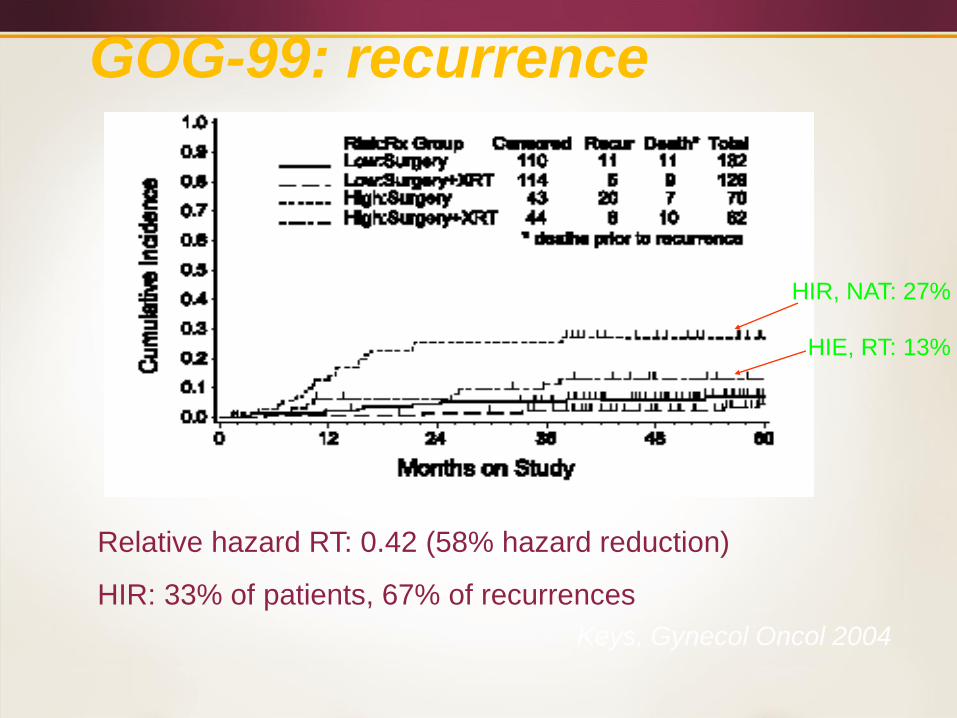
GOG-99: recurrence
Relative hazard RT: 0.42 (58% hazard reduction)
HIR: 33% of patients, 67% of recurrences
HIR, NAT: 27%
HIE, RT: 13%
Keys, Gynecol Oncol 2004
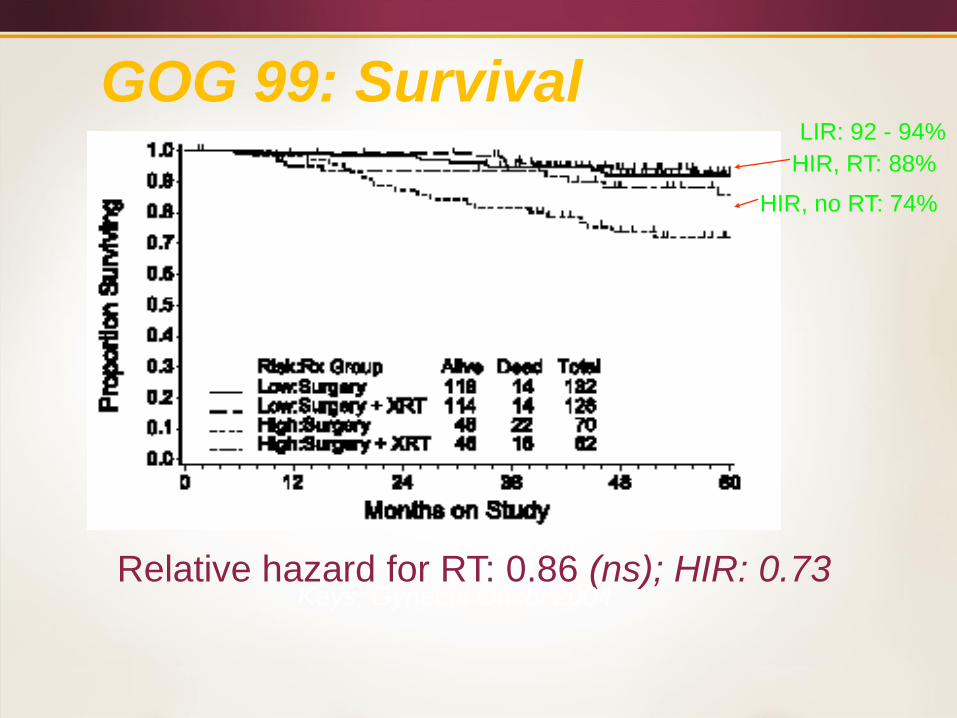
GOG 99: Survival
Relative hazard for RT: 0.86 (ns); HIR: 0.73
HIR, no RT: 74%
HIR, RT: 88%
LIR: 92 - 94%
Keys, Gynecol Oncol 2004
MRC ASTEC Radiotherapy and
NCIC EN.5 TrialAdjuvant external beam radiotherapy (EBRT) in the treatment of
endometrial cancer: results of the randomized MRC ASTEC and
NCIC CTG EN.5 trials
ASTEC ISRCTN 16571884
EN.5 clinicaltrials.gov NCT 00002807
Presented by
Jane Orton
On behalf of all ASTEC and EN.5 Collaborators
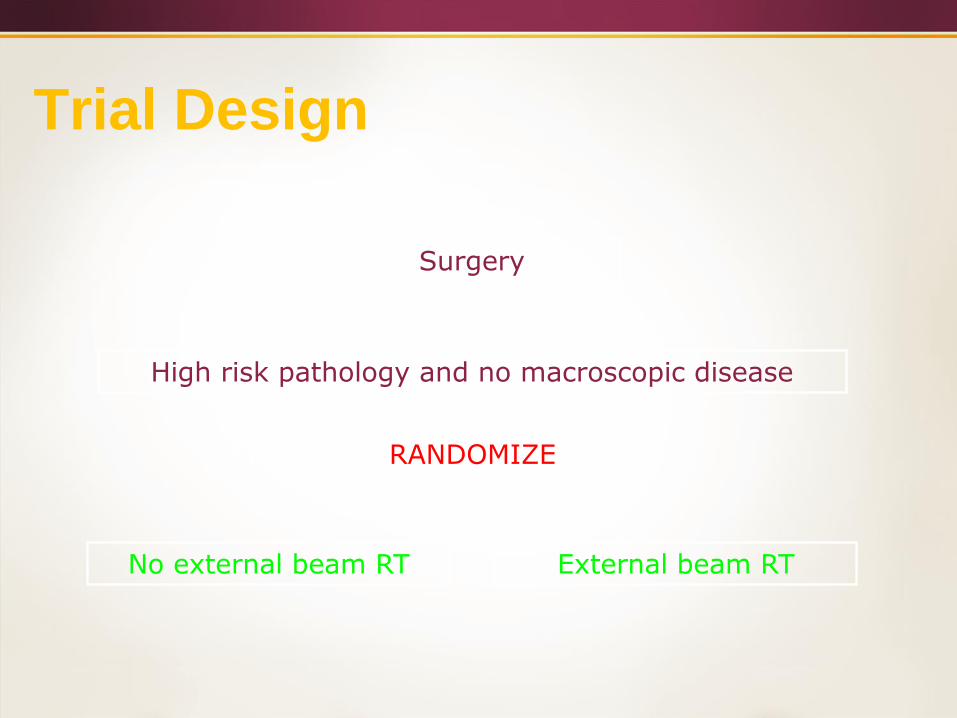
Trial Design
Surgery
High risk pathology and no macroscopic disease
RANDOMIZE
No external beam RT External beam RT
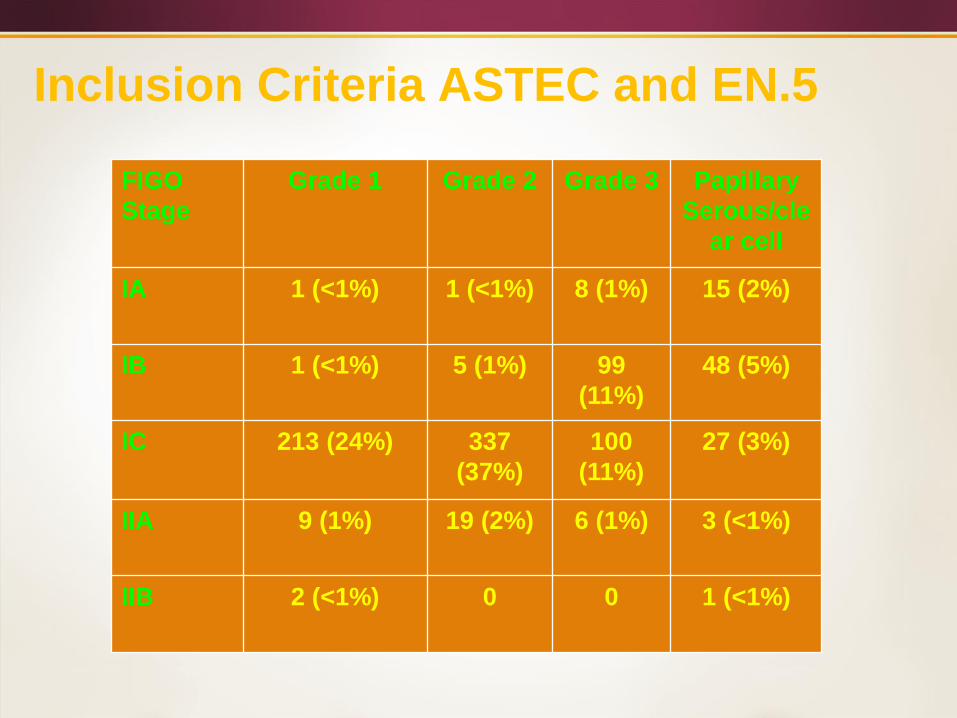
Inclusion Criteria ASTEC and EN.5
FIGO
Stage
Grade 1 Grade 2 Grade 3 Papillary
Serous/cle
ar cell
IA 1 (<1%) 1 (<1%) 8 (1%) 15 (2%)
IB 1 (<1%) 5 (1%) 99
(11%)
48 (5%)
IC 213 (24%) 337
(37%)
100
(11%)
27 (3%)
IIA 9 (1%) 19 (2%) 6 (1%) 3 (<1%)
IIB 2 (<1%) 0 0 1 (<1%)
Eligibility Criteria
Brachytherapy allowed if
centre policy
stated before randomisation
used in both arms
Positive para-aortic nodes an exclusion
Positive pelvic lymph nodes
Eligible for ASTEC
Ineligible for EN.5
Brachytherapy
In the ASTEC trial HDR: Two fractions of 4 Gy at
0.5 cm from the vaginal mucosa over 3-7 days
or LDR: 15 Gy – upper third of the vagina.
In the EN-5: Given in accordance with local
practice.
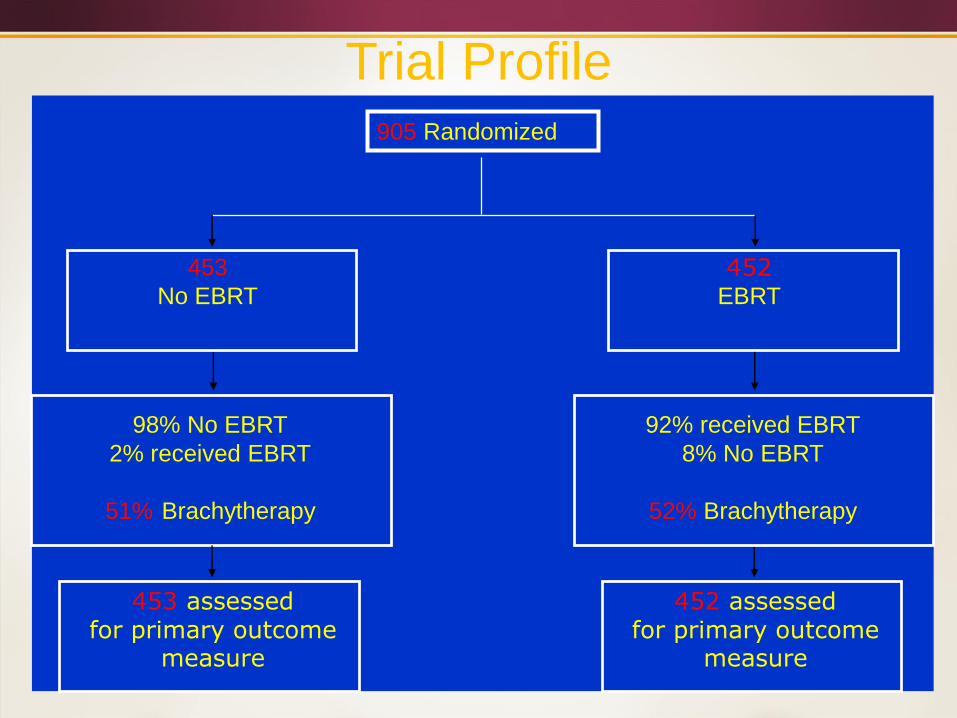
98% No EBRT
2% received EBRT
51% Brachytherapy
453
No EBRT
453 assessed for primary outcome
measure
452EBRT
92% received EBRT
8% No EBRT
52% Brachytherapy
452 assessed for primary outcome
measure
905 Randomized
Trial Profile
Patient Characteristics
Baseline characteristics balanced between treatment groups
median age 65 years
98 % performance status 0-1
83% endometrioid histology
25% lymphovascular space invasion
4% positive peritoneal cytology
Surgery received
71% TAH/BSO
29% TAH/BSO plus lymphadenectomy
4% of patients (with nodes harvested) had positive pelvic
nodes
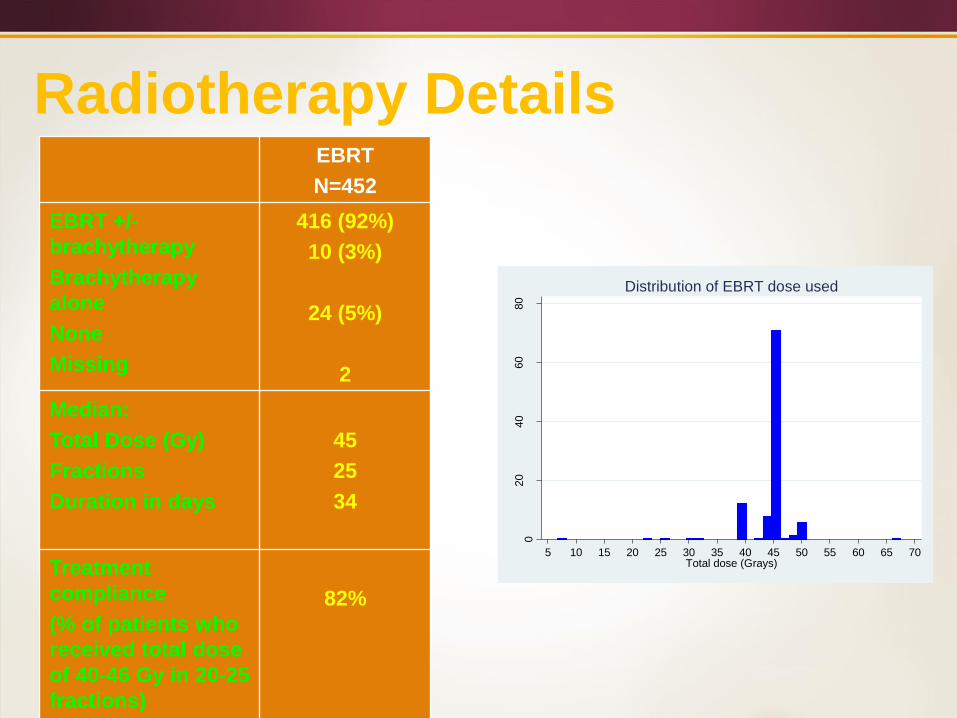
Radiotherapy DetailsEBRT
N=452
EBRT +/-
brachytherapy
Brachytherapy
alone
None
Missing
416 (92%)
10 (3%)
24 (5%)
2
Median:
Total Dose (Gy)
Fractions
Duration in days
45
25
34
Treatment
compliance
(% of patients who
received total dose
of 40-46 Gy in 20-25
fractions)
82%
020
40
60
80
Perc
enta
ge (
%)
5 10 15 20 25 30 35 40 45 50 55 60 65 70Total dose (Grays)
Distribution of EBRT dose used
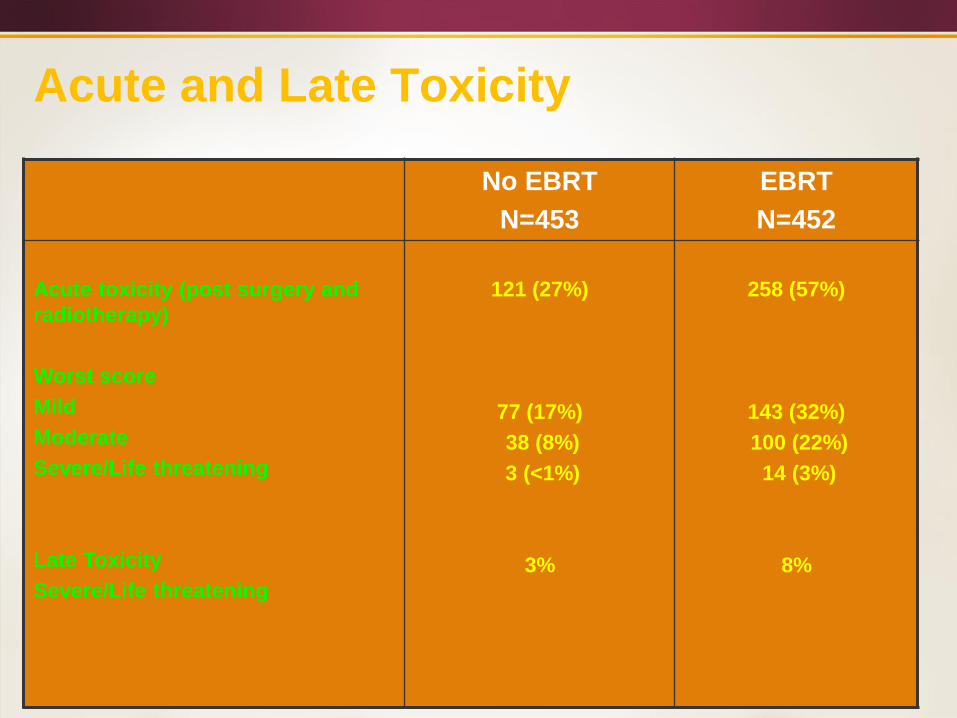
Acute and Late Toxicity
No EBRT
N=453
EBRT
N=452
Acute toxicity (post surgery and
radiotherapy)
Worst score
Mild
Moderate
Severe/Life threatening
Late Toxicity
Severe/Life threatening
121 (27%)
77 (17%)
38 (8%)
3 (<1%)
3%
258 (57%)
143 (32%)
100 (22%)
14 (3%)
8%
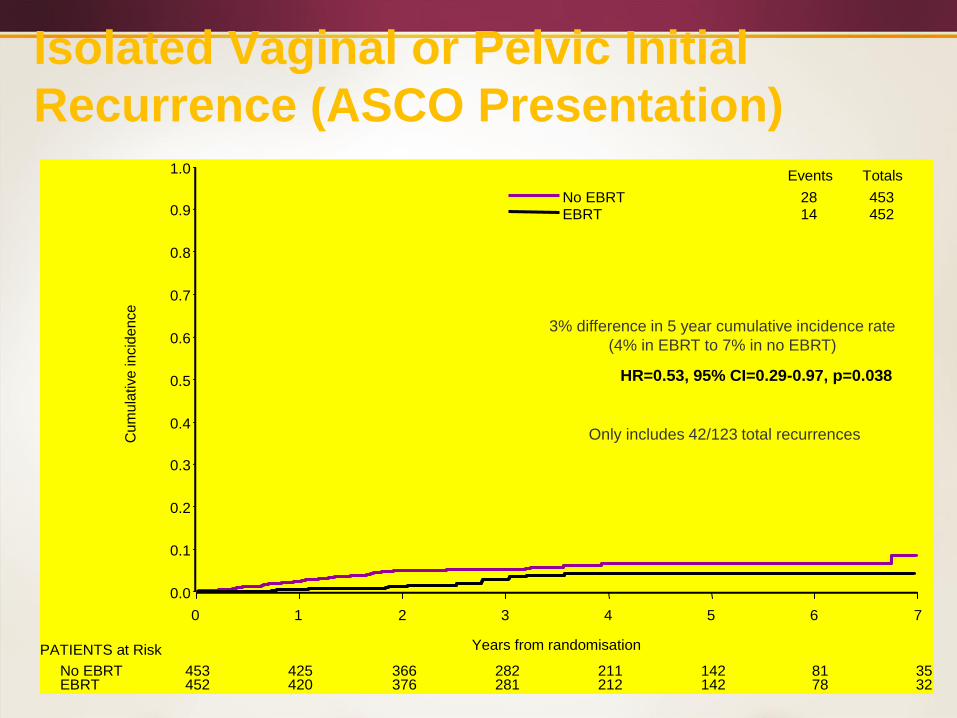
Isolated Vaginal or Pelvic Initial
Recurrence (ASCO Presentation)
28 45314 452
Events Totals
PATIENTS at Risk
No EBRTEBRT
453 425 366 282 211 142 81 35452 420 376 281 212 142 78 32
No EBRT EBRT
Cu
mu
lative
incid
en
ce
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Years from randomisation
0 1 2 3 4 5 6 7
HR=0.53, 95% CI=0.29-0.97, p=0.038
3% difference in 5 year cumulative incidence rate
(4% in EBRT to 7% in no EBRT)
Only includes 42/123 total recurrences
Isolated Vaginal or Pelvic Initial Recurrence
5-year cumulative incidence 6.1 % versus 3.2 %
(p=0.02)
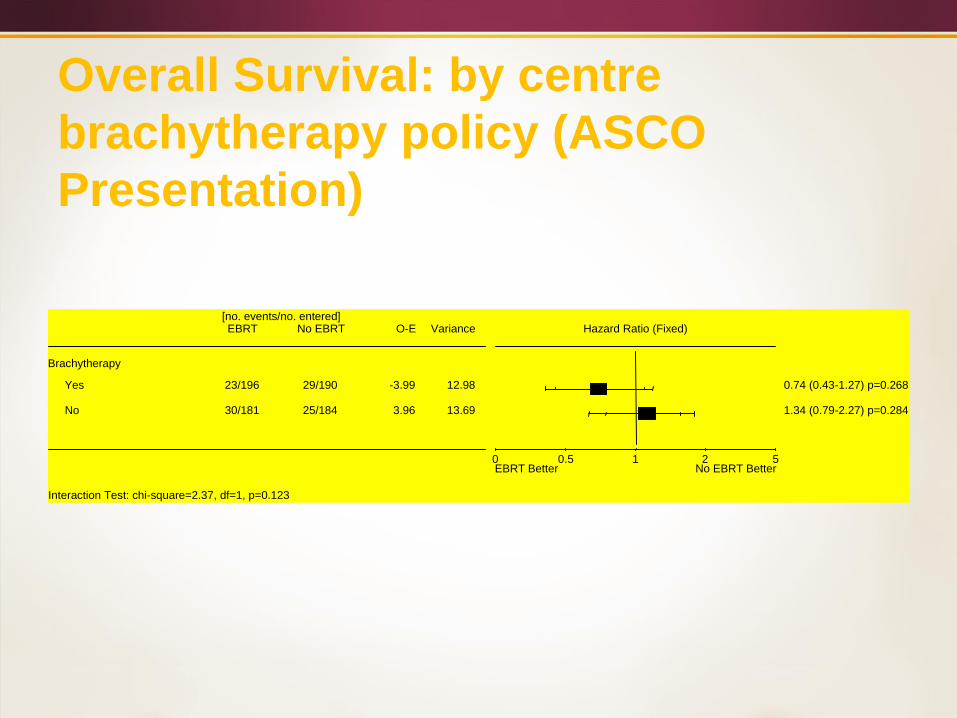
Overall Survival: by centre
brachytherapy policy (ASCO
Presentation)
Brachytherapy
Yes 23/196 29/190 -3.99 12.98
No 30/181 25/184 3.96 13.69
[no. events/no. entered]EBRT No EBRT O-E Variance Hazard Ratio (Fixed)
EBRT Better No EBRT Better0 1 50.5 2
0.74 (0.43-1.27) p=0.268
1.34 (0.79-2.27) p=0.284
Interaction Test: chi-square=2.37, df=1, p=0.123
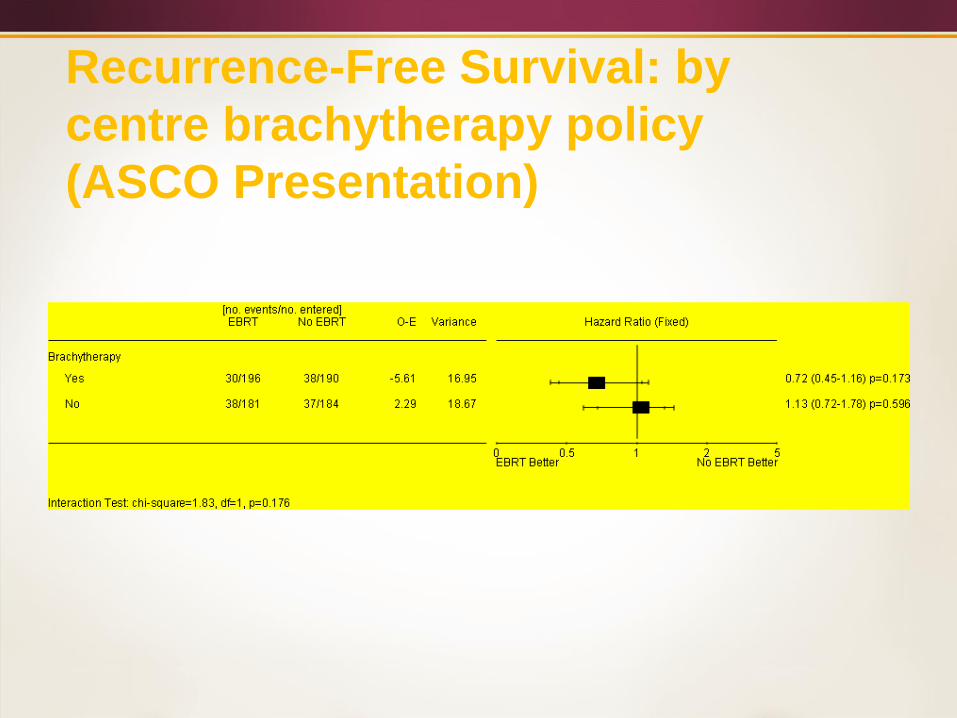
Recurrence-Free Survival: by
centre brachytherapy policy
(ASCO Presentation)
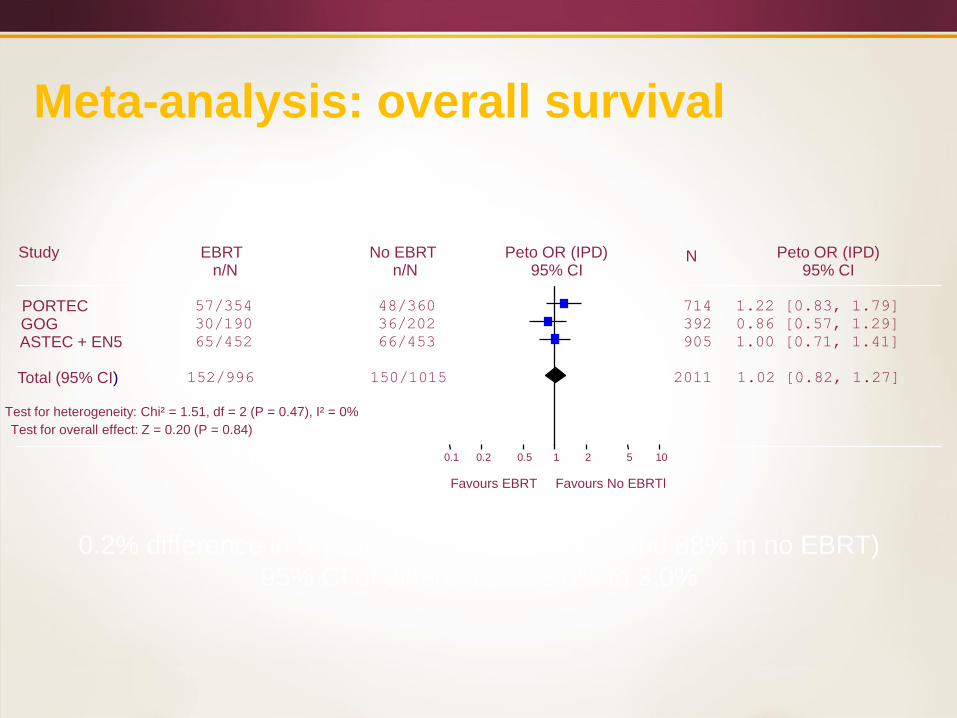
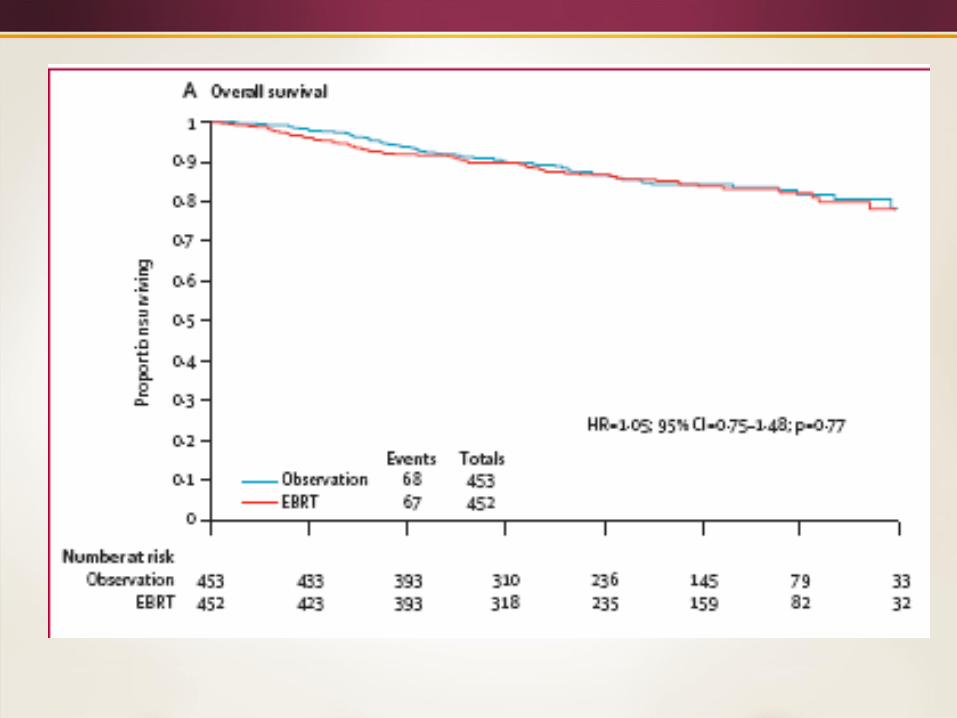
Meta-analysis: overall survival
Study EBRT No EBRT Peto OR (IPD) Peto OR (IPD)n/N n/N 95% CI
N95% CI
PORTEC 57/354 48/360 714 1.22 [0.83, 1.79]
GOG 30/190 36/202 392 0.86 [0.57, 1.29]
ASTEC + EN5 65/452 66/453 905 1.00 [0.71, 1.41]
Total (95% CI) 152/996 150/1015 2011 1.02 [0.82, 1.27]
Test for heterogeneity: Chi² = 1.51, df = 2 (P = 0.47), I² = 0%
Test for overall effect: Z = 0.20 (P = 0.84)
0.1 0.2 0.5 1 2 5 10
Favours EBRT Favours No EBRTl
0.2% difference in 5-year OS (87.8% in EBRT and 88% in no EBRT)
95% CI of difference = -2.0% to 3.0%
The “Myth” that Isolated Vaginal
Recurrences are Easily Salvageable
Accompanying editorial to GOG 99 by Michael Berman noted: “Yet vaginal recurrences usually are treated successfully with radiotherapy in patient not previously treated with adjunctive radiation”
The data from GOG 99 noted that 12 of 13 patients in the NAT arm were treated with salvage radiotherapy – crude observations noted 5 of these thirteen died of endometrial cancer.
Immediate versus delayed RT
Salvage rate may not be as high as those
commonly quoted.
> 70% results are typically quoted.
Most studies do not support this even in isolated
vaginal recurrences.
Survival typically range around 40 – 50 %.
Poorer outcomes in non-vaginal pelvic recurrences.
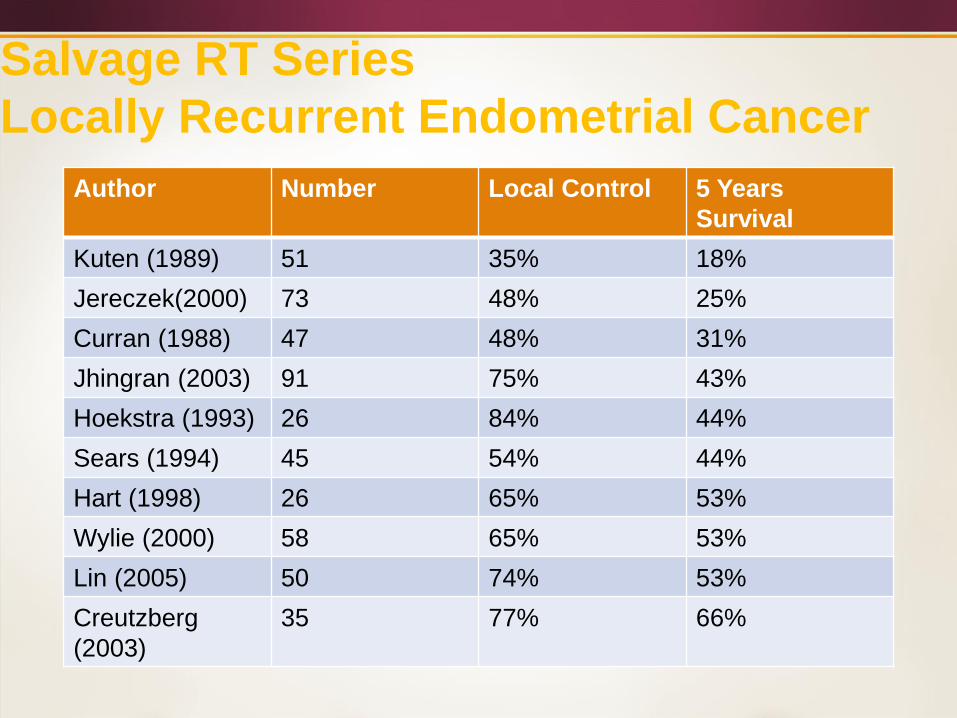
Salvage RT Series
Locally Recurrent Endometrial Cancer
Author Number Local Control 5 Years
Survival
Kuten (1989) 51 35% 18%
Jereczek(2000) 73 48% 25%
Curran (1988) 47 48% 31%
Jhingran (2003) 91 75% 43%
Hoekstra (1993) 26 84% 44%
Sears (1994) 45 54% 44%
Hart (1998) 26 65% 53%
Wylie (2000) 58 65% 53%
Lin (2005) 50 74% 53%
Creutzberg
(2003)
35 77% 66%

Salvage treatment with high-dose-rate brachytherapy for isolated vaginal endometrial
cancer recurrence
And the risk of toxicity should NOT be ignored
22 isolated vaginal recurrences
18 EBRT + HDR, 4 HDR alone
Median follow-up 32 month
18% grade 3-4 GI toxicity
50% grade 3 vaginal sequelae
Petignat et al. Gynecol Oncol 2006; 101:445
Population Based Data
SEER analysis: efficacy of RT
• SEER program (NCI), 10% US population
• 21.249 patients, 1988-2001
• 19% of patients had RT (82% EBRT)
• 43% had surgical node samplingLee et al, JAMA 295, 389-97, 2006
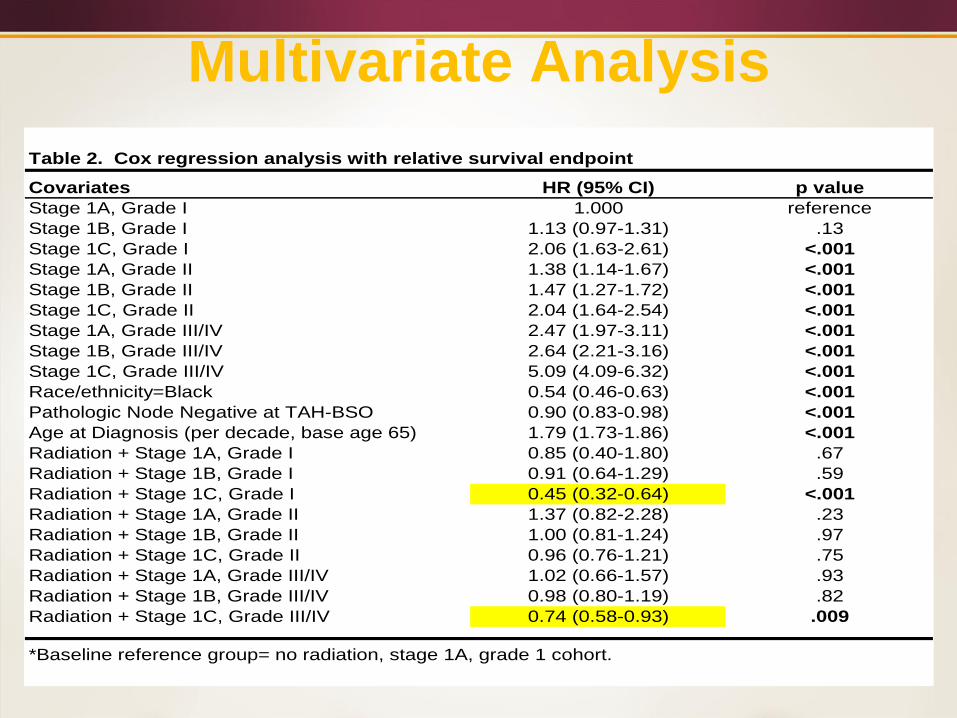
Multivariate Analysis
Table 2. Cox regression analysis with relative survival endpoint
Covariates HR (95% CI) p value
Stage 1A, Grade I 1.000 reference
Stage 1B, Grade I 1.13 (0.97-1.31) .13
Stage 1C, Grade I 2.06 (1.63-2.61) <.001
Stage 1A, Grade II 1.38 (1.14-1.67) <.001
Stage 1B, Grade II 1.47 (1.27-1.72) <.001
Stage 1C, Grade II 2.04 (1.64-2.54) <.001
Stage 1A, Grade III/IV 2.47 (1.97-3.11) <.001
Stage 1B, Grade III/IV 2.64 (2.21-3.16) <.001
Stage 1C, Grade III/IV 5.09 (4.09-6.32) <.001
Race/ethnicity=Black 0.54 (0.46-0.63) <.001
Pathologic Node Negative at TAH-BSO 0.90 (0.83-0.98) <.001
Age at Diagnosis (per decade, base age 65) 1.79 (1.73-1.86) <.001
Radiation + Stage 1A, Grade I 0.85 (0.40-1.80) .67
Radiation + Stage 1B, Grade I 0.91 (0.64-1.29) .59
Radiation + Stage 1C, Grade I 0.45 (0.32-0.64) <.001
Radiation + Stage 1A, Grade II 1.37 (0.82-2.28) .23
Radiation + Stage 1B, Grade II 1.00 (0.81-1.24) .97
Radiation + Stage 1C, Grade II 0.96 (0.76-1.21) .75
Radiation + Stage 1A, Grade III/IV 1.02 (0.66-1.57) .93
Radiation + Stage 1B, Grade III/IV 0.98 (0.80-1.19) .82
Radiation + Stage 1C, Grade III/IV 0.74 (0.58-0.93) .009
*Baseline reference group= no radiation, stage 1A, grade 1 cohort.
What is the “best” RT
It is clear that radiotherapy is indicated in high risk
early stage endometrial cancer.
Can VBT replace external beam for the majority of
these patients?
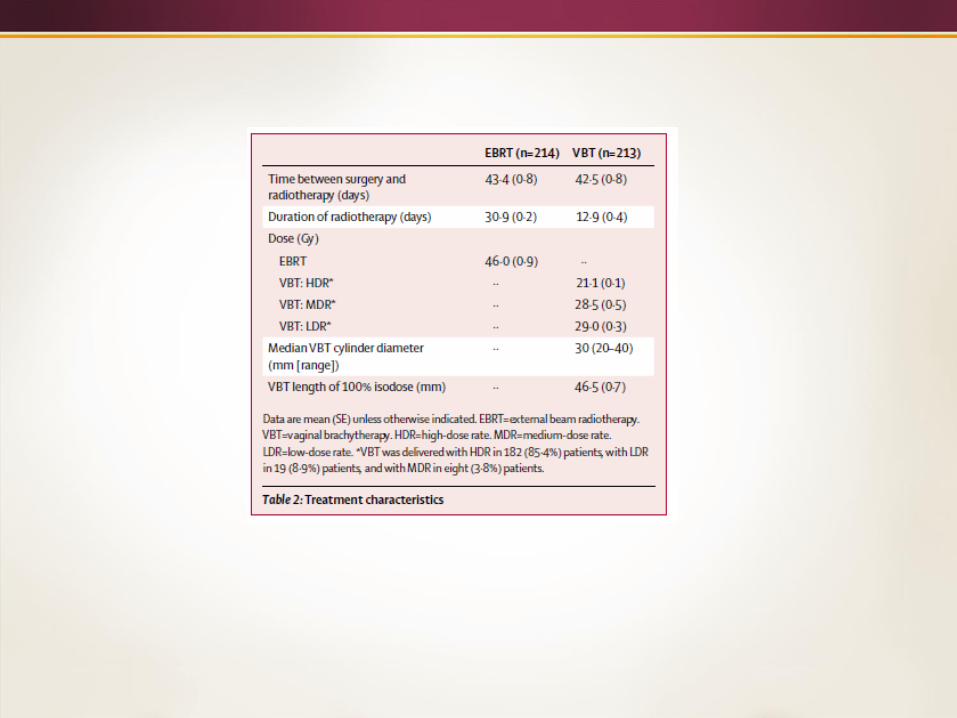
PORTEC - 2 trial (2002-2006)
Stage I-IIA endometrial carcinoma
• age > 60 and IC grade 1-2, or IB grade 3
• stage 2A (except grade 3 > 1/2)
• surgery: TAH-BSO
Rpelvic radiotherapy
vaginal brachytherapyUtrecht
Ijsselmeer
Groningen
DrentheNoord
Holland
Gelderland
Limburg
Flevoland
Zuid Holland
Noord Brabant
Zeeland
Overijssel
Friesland
Waddenzee
PORTEC-2
Randomized Between:
Pelvic Radiotherapy – 46 Gy in 23 fractions
VS
Vaginal Brachytherapy – 21 Gy HDR or 30 Gy LDR
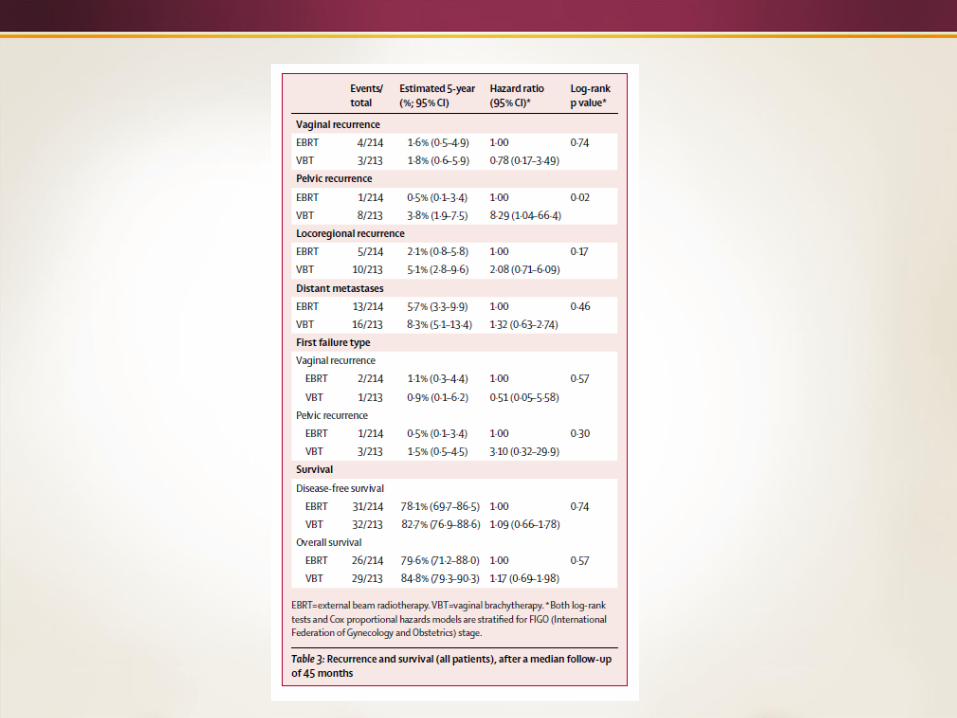
PORTEC-2 Author Conclusions
“Despite the slightly but significantly increased
pelvic failure rate in the VBT arm, DM, RFS and OS
were similar. As patient reported quality of life after
VBT was…better, VBT should be the treatment of
choice for patients with high-intermediate risk
endometrial cancer”
PORTEC- 4 and Patient Preference
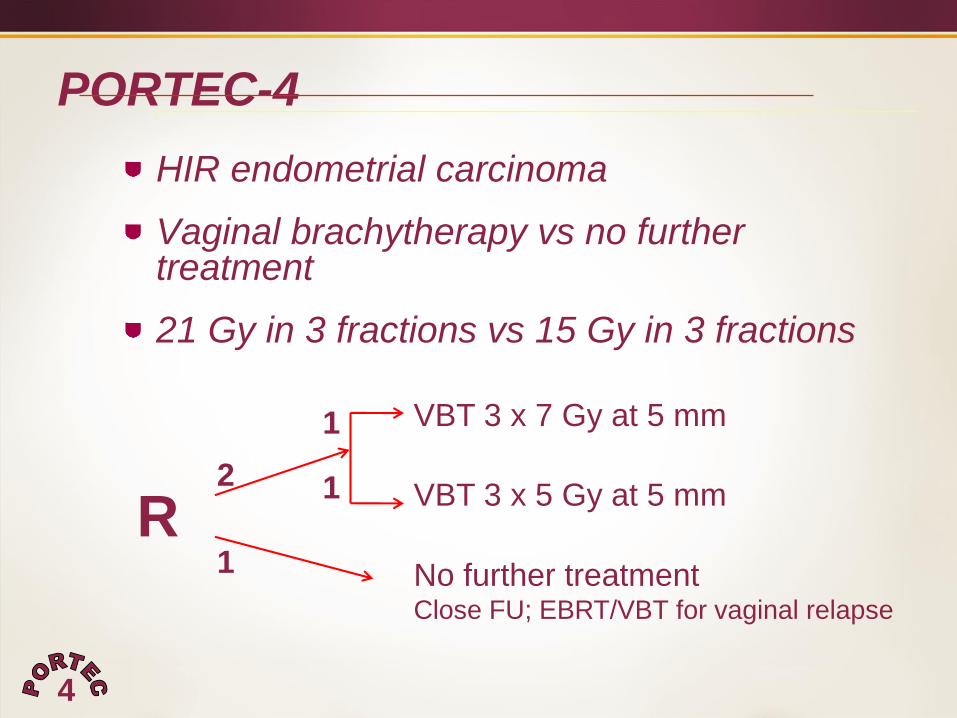
PORTEC-4
HIR endometrial carcinoma
Vaginal brachytherapy vs no further treatment
21 Gy in 3 fractions vs 15 Gy in 3 fractions
1
1
R
VBT 3 x 7 Gy at 5 mm
VBT 3 x 5 Gy at 5 mm
No further treatmentClose FU; EBRT/VBT for vaginal relapse
2 1
4
Kunneman, et.al/British Journal of Cancer, 2014, 1-6
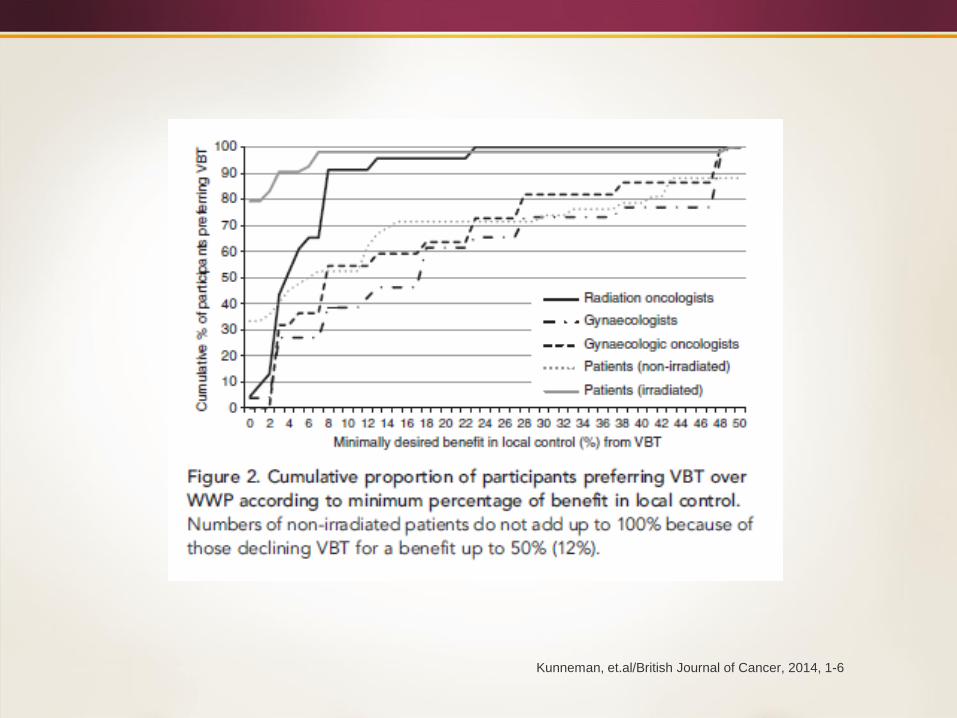
Kunneman, et.al/British Journal of Cancer, 2014, 1-6
How should you treat – so called –
intermediate risk patients?
The data on unselected patients consistently
shows a reduction in vaginal recurrences.
I believe the “best” technique is to look at all the
risk factors before deciding on an individual
patient.
Clinical Outcomes in International Federation of
Gynecology and Obstetrics Stage IA Endometrial Cancer
With Myometrial Invasion Treated With or Without
Postoperative Vaginal Brachytherapy
V. Diavolitsis, M.D.,1 * A. Rademaker, Ph.D.,2 J. Lurain, M.D.,3 A. Hoekstra,
M.D., M.P.H.,4 J. Strauss, M.D., M.B.A.,5 and W. Small, Jr., M.D.,*
Departments of Radiation Oncology, Preventive Medicine, and Obstetrics and
Gynecology, Division of Gynecologic Oncology, Robert H. Lurie Comprehensive
Cancer Center, Northwestern University Feinberg School of Medicine, Chicago, IL.
Int J Radiol Oncol Biol Phys,. Volume 84, Number 2 (2012) 415-419.
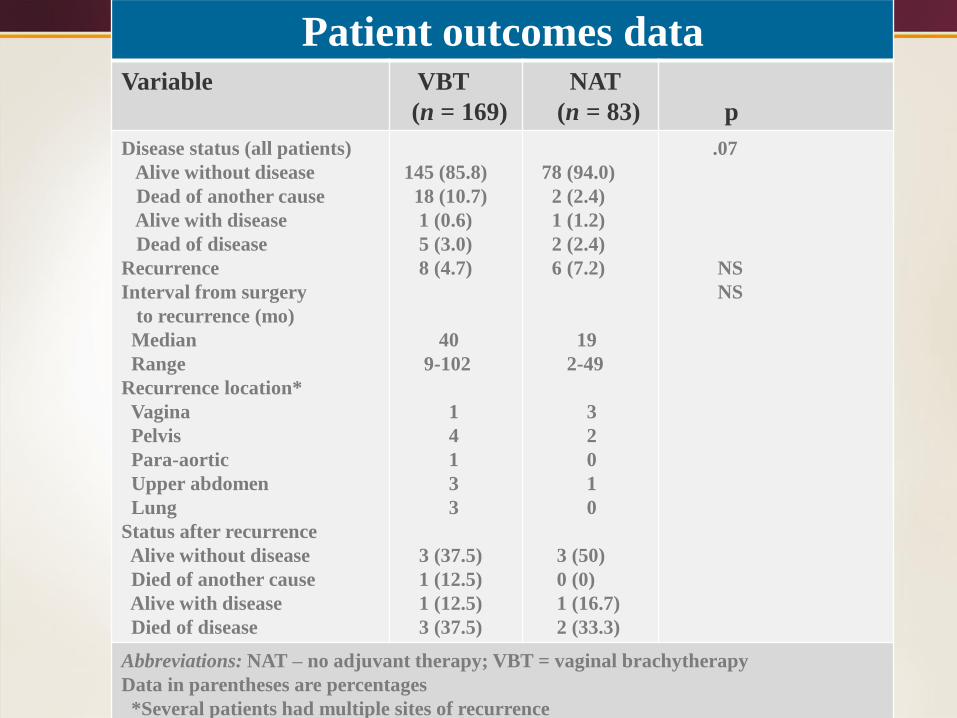
Patient outcomes dataVariable VBT
(n = 169)
NAT
(n = 83) p
Disease status (all patients)
Alive without disease
Dead of another cause
Alive with disease
Dead of disease
Recurrence
Interval from surgery
to recurrence (mo)
Median
Range
Recurrence location*
Vagina
Pelvis
Para-aortic
Upper abdomen
Lung
Status after recurrence
Alive without disease
Died of another cause
Alive with disease
Died of disease
145 (85.8)
18 (10.7)
1 (0.6)
5 (3.0)
8 (4.7)
40
9-102
1
4
1
3
3
3 (37.5)
1 (12.5)
1 (12.5)
3 (37.5)
78 (94.0)
2 (2.4)
1 (1.2)
2 (2.4)
6 (7.2)
19
2-49
3
2
0
1
0
3 (50)
0 (0)
1 (16.7)
2 (33.3)
.07
NS
NS
Abbreviations: NAT – no adjuvant therapy; VBT = vaginal brachytherapy
Data in parentheses are percentages
*Several patients had multiple sites of recurrence
Vaginal Brachytherapy Techniques
Aims
• To update the current practice patterns for the treatment of postoperative endometrial cancer from the ABS survey sent in 2003 and published in 2005 (Small et al, IJROBP 2005).
• To present the practice patterns of vaginal brachytherapy (VBT) regarding patient selection, treatment planning, treatment delivery, and quality assurance.
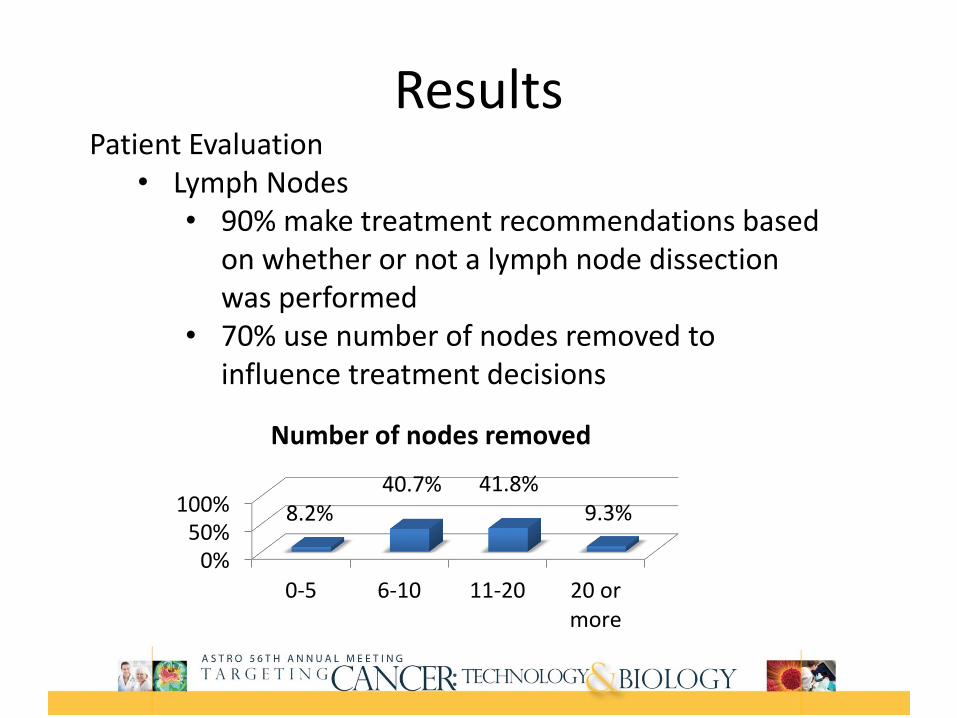
ResultsPatient Evaluation
• Lymph Nodes• 90% make treatment recommendations based
on whether or not a lymph node dissection was performed
• 70% use number of nodes removed to influence treatment decisions
0%50%
100%
0-5 6-10 11-20 20 ormore
8.2%40.7% 41.8%
9.3%
Number of nodes removed
Results
Treatment Planning•26% place radio-opaque (i.e. gold) markers at the vaginal apex•53% report doses at both the surface and 0.5cm•80% document dose to normal tissues•Most common dose rate
•96% HDR•3% LDR•1% Both•0% PDR
Results
HDR Brachytherapy•83% use single channel and 14% use a multi-channel cylinder•83% perform CT planning
•26% for each fraction•74% for first fraction only
•Most common dose prescription location•Vaginal surface – 23%•0.5cm depth – 60%•Other – 17%
Results
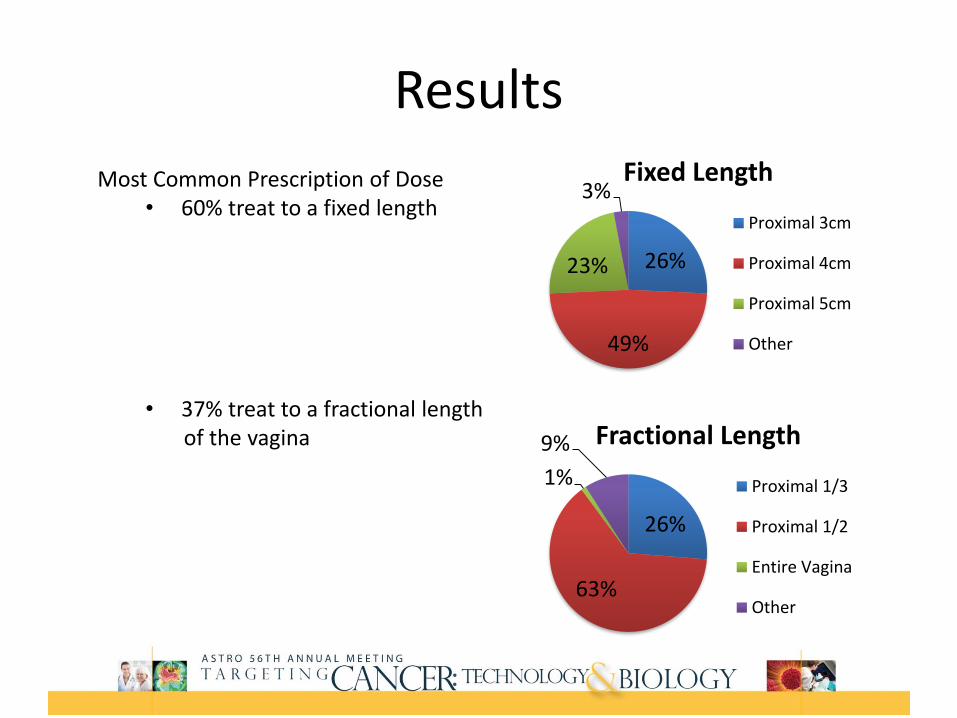
Most Common Prescription of Dose• 60% treat to a fixed length
• 37% treat to a fractional length of the vagina
26%
49%
23%
3%Fixed Length
Proximal 3cm
Proximal 4cm
Proximal 5cm
Other
26%
63%
1%
9% Fractional Length
Proximal 1/3
Proximal 1/2
Entire Vagina
Other
Results
Treating the entire length of the vagina• 26% treat for CCC/UPSC histology• 11% for grade 3• 13% for LVSI• 65% never
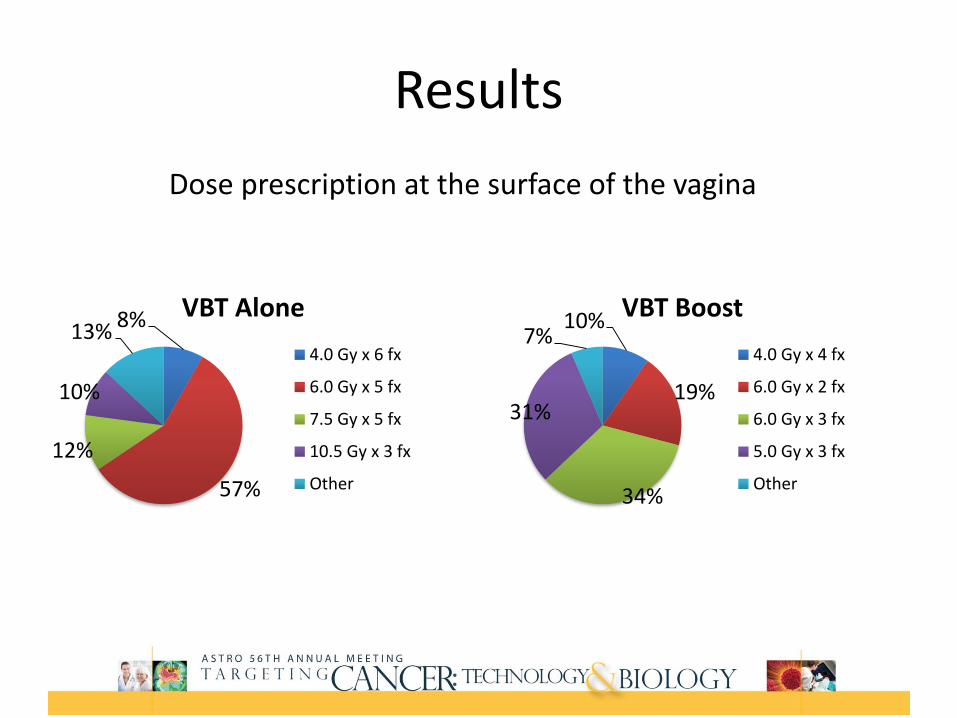
Results
Dose prescription at the surface of the vagina
8%
57%
12%
10%
13%VBT Alone
4.0 Gy x 6 fx
6.0 Gy x 5 fx
7.5 Gy x 5 fx
10.5 Gy x 3 fx
Other
10%
19%
34%
31%
7%VBT Boost
4.0 Gy x 4 fx
6.0 Gy x 2 fx
6.0 Gy x 3 fx
5.0 Gy x 3 fx
Other
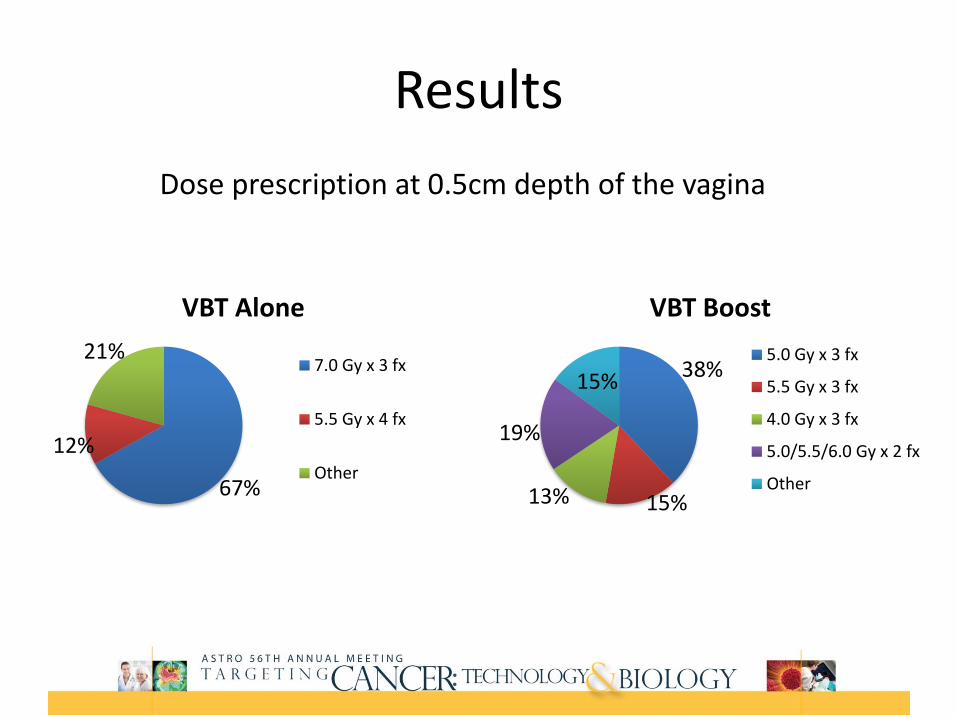
Results
Dose prescription at 0.5cm depth of the vagina
67%
12%
21%
VBT Alone
7.0 Gy x 3 fx
5.5 Gy x 4 fx
Other
38%
15%13%
19%
15%
VBT Boost
5.0 Gy x 3 fx
5.5 Gy x 3 fx
4.0 Gy x 3 fx
5.0/5.5/6.0 Gy x 2 fx
Other
Results
Treatment Planning & Delivery•Fractions per week
•1 – 34%•2 – 52%•3 – 13%•4 or 5 – 2%
•73% place optimization points at the vaginal apex AND lateral to the cylinder•99% perform secondary QA checks
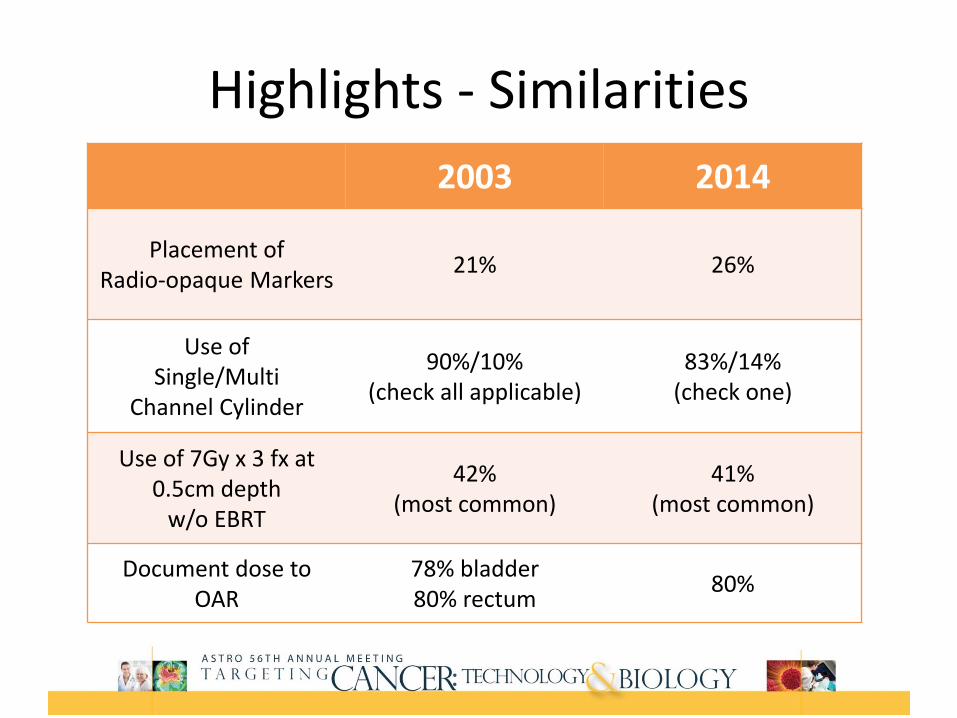
Highlights - Similarities
2003 2014
Placement of Radio-opaque Markers
21% 26%
Use of Single/Multi
Channel Cylinder
90%/10%(check all applicable)
83%/14%(check one)
Use of 7Gy x 3 fx at 0.5cm depth
w/o EBRT
42%(most common)
41%(most common)
Document dose to OAR
78% bladder80% rectum
80%
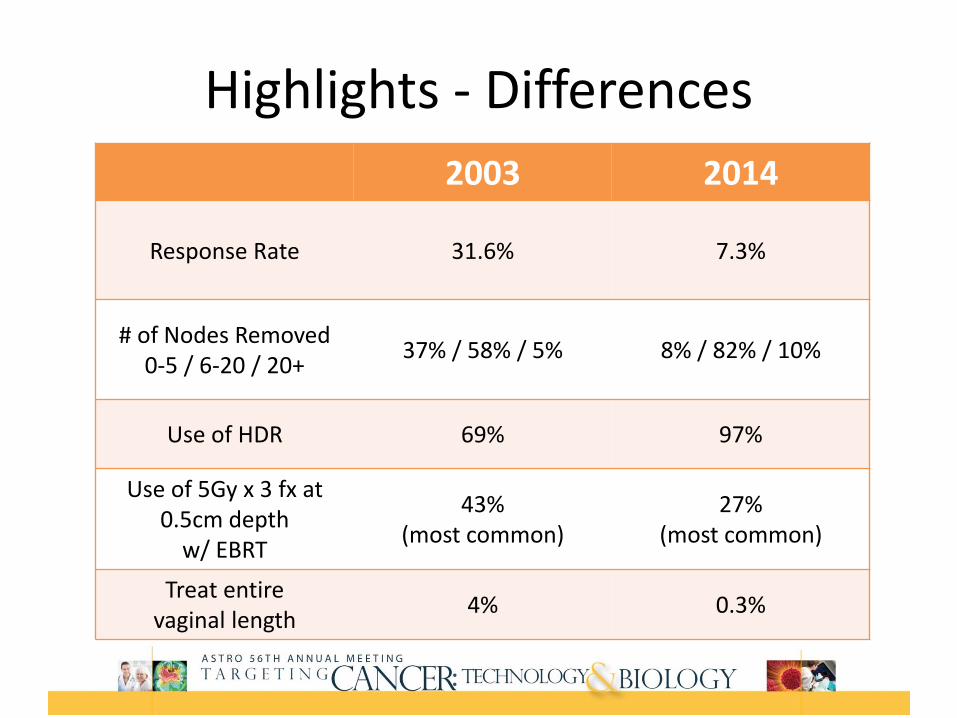
Highlights - Differences
2003 2014
Response Rate 31.6% 7.3%
# of Nodes Removed0-5 / 6-20 / 20+
37% / 58% / 5% 8% / 82% / 10%
Use of HDR 69% 97%
Use of 5Gy x 3 fx at 0.5cm depth
w/ EBRT
43%(most common)
27%(most common)
Treat entire vaginal length
4% 0.3%
Conclusions
•Electronic surveys are possible though response rate is lower than the original study
•In a population of ABS/ASTRO members•HDR Brachytherapy is the most common delivery modality•Responders are seeing increased nodal dissections•Fractionation schedules continue to be highly variable•Almost all are doing secondary QA checks•Treatment devices and planning techniques are variable but they generally align with the ABS recommendations
American Brachytherapy Society consensus guidelines for adjuvant vaginal cuff brachytherapy after hysterectomy.
William Small, Jr., M.D.,1*, Sushil Beriwal, M.D., 2 D. Jeffrey Demanes, M.D.,3 Kathryn E. Dusenbery, M.D., 4 Patricia Eifel, M.D.,5 Beth Erickson, M.D., 6 Ellen Jones, M.D., 7 Jason J. Rownd, M.D.,8 Jennifer F. De Los Santos, M.D., 9Akila N. Viswanathan, M.D.,10 and David Gaffney, M.D.11
Brachytherapy 11(2012) 58-47.
Pretherapy Evaluation
Pay particular attention to healing – especially
on the current proliferation of robotic surgery.
Choose the applicator that is correct for the
clinical situation.
Cylinders most common which range in size
from 2 – 4 cm.
Brachytherapy Technique
Placement of a radio-opaque seed or clip(s) at
the vaginal apex should be considered.
Place the largest cylinder that fits comfortably.
Minimize movement from placement, planning
and treatment.
Dose Fractionation
7 Gy X 3 to 0.5 cm is the most commonly
prescribed fractionation scheme.
Many sites use different fractionation schemes.
I use 5.5 Gy X 4 to 0.5 cm.
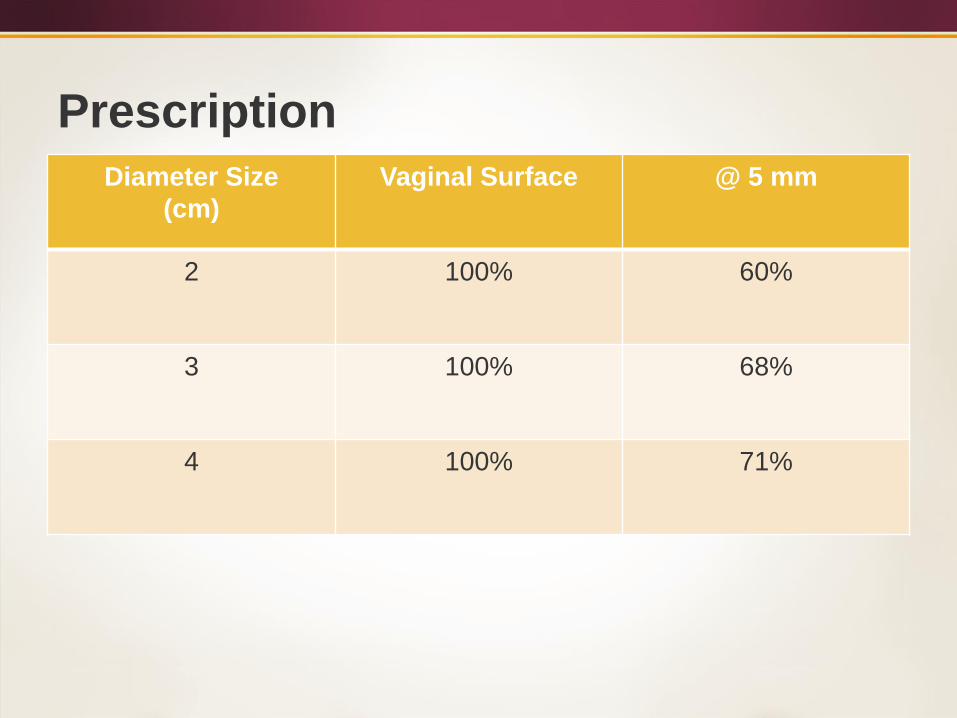
Prescription
Diameter Size
(cm)
Vaginal Surface @ 5 mm
2 100% 60%
3 100% 68%
4 100% 71%
External Beam Techniques
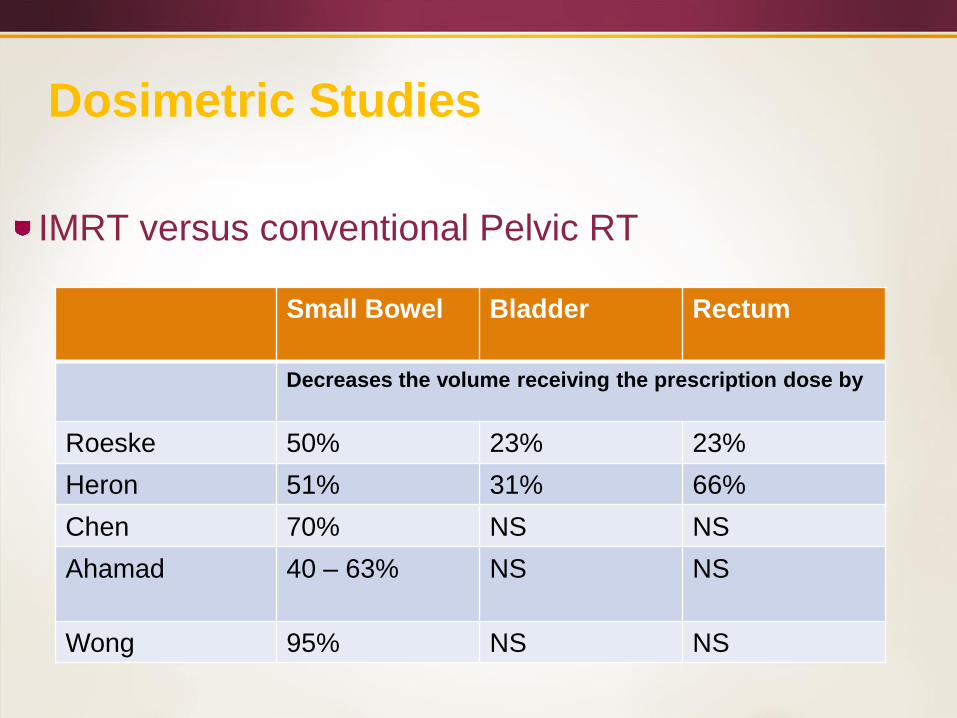
Dosimetric Studies
IMRT versus conventional Pelvic RT
Small Bowel Bladder Rectum
Decreases the volume receiving the prescription dose by
Roeske 50% 23% 23%
Heron 51% 31% 66%
Chen 70% NS NS
Ahamad 40 – 63% NS NS
Wong 95% NS NS
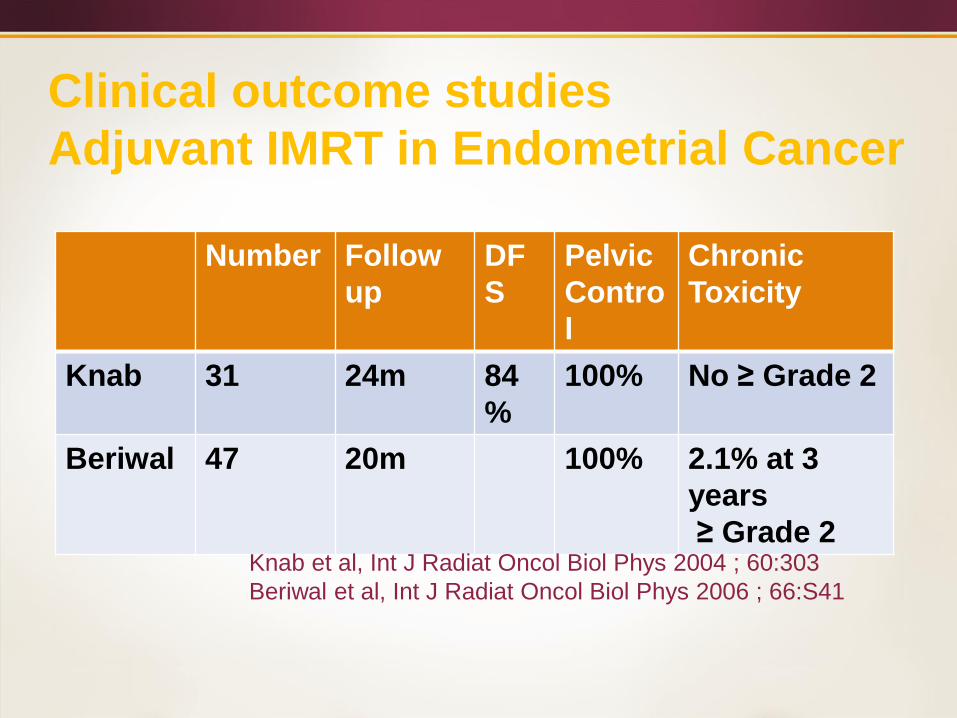
Clinical outcome studies
Adjuvant IMRT in Endometrial Cancer
Number Follow
up
DF
S
Pelvic
Contro
l
Chronic
Toxicity
Knab 31 24m 84
%
100% No ≥ Grade 2
Beriwal 47 20m 100% 2.1% at 3
years
≥ Grade 2Knab et al, Int J Radiat Oncol Biol Phys 2004 ; 60:303
Beriwal et al, Int J Radiat Oncol Biol Phys 2006 ; 66:S41
A RANDOMIZED PHASE III STUDY (NRG Oncology’s RTOG 1203) OF STANDARD VS. IMRT PELVIC RADIATION FOR POST-OPERATIVE TREATMENT OF ENDOMETRIAL AND CERVICAL
CANCER (TIME-C)
Ann H. Klopp MD, PhD
MD Anderson Cancer Center
Ann Klopp, Anamaria Yeung, Snehal Deshmukh, Karen M Gil, Lari Wenzel, Shannon Westin, Kent Gifford, David Gaffney, William Small, Jr., Spencer Thompson, Desiree Doncals,
Guilherme Cantuaria, Brian Yaremko, Amy Chang, Vijayananda Kundapur, Dasarahally Mohan, Michael Haas, Yong Bae Kim, Catherine Ferguson,
Deborah W.Bruner
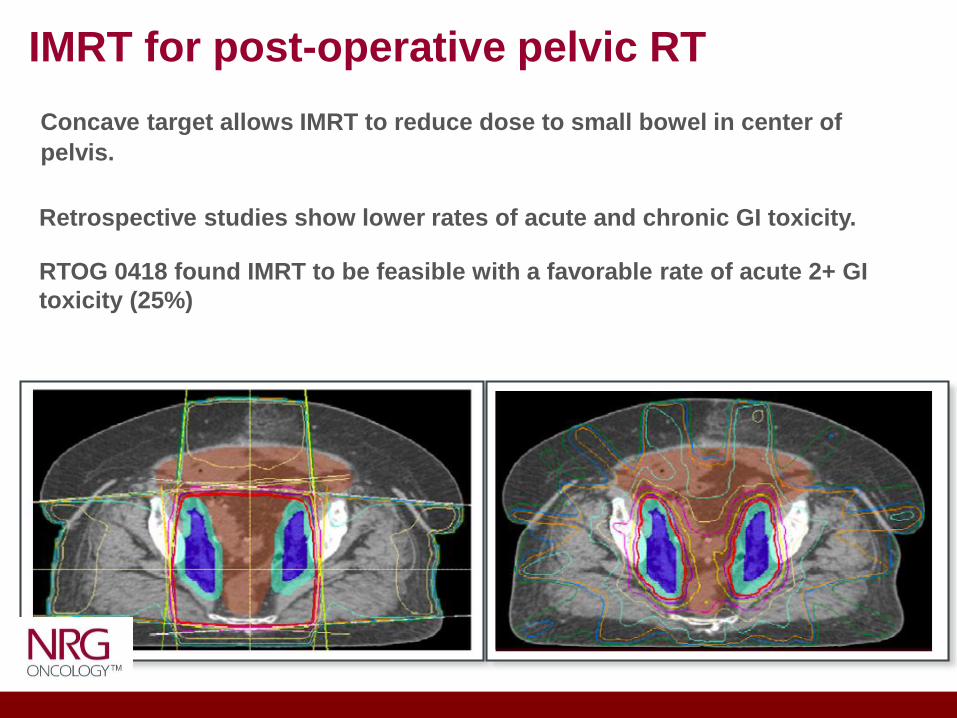
Retrospective studies show lower rates of acute and chronic GI toxicity.
RTOG 0418 found IMRT to be feasible with a favorable rate of acute 2+ GI
toxicity (25%)
IMRT for post-operative pelvic RT
Concave target allows IMRT to reduce dose to small bowel in center of
pelvis.
Objectives
Determine if acute GI toxicity is reduced with IMRT in week 5 of RT
using patient reported measure of toxicity
Secondary endpoints
• Acute urinary toxicity with EPIC tool
• Acute GI toxicity with PRO-CTCAE
• Quality of life (FACT)
• LRC, DFS, OS
• Health utilities analysis
Primary endpoint: Determine if acute GI toxicity is reduced with IMRT in week 5 on RT using patient reported measure of toxicity.
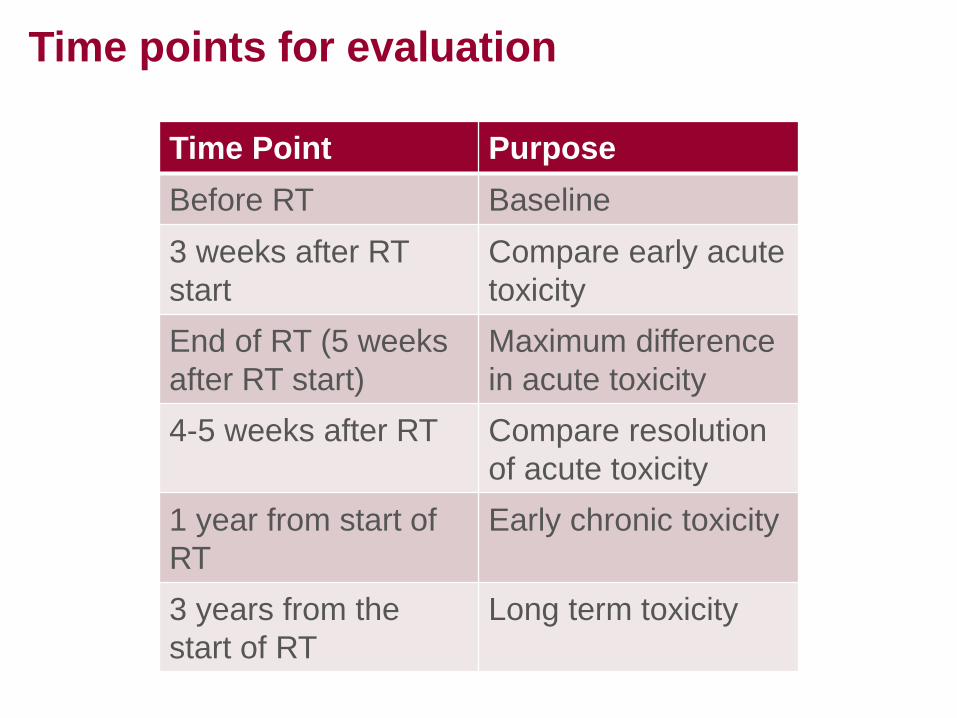
Time points for evaluation
Time Point Purpose
Before RT Baseline
3 weeks after RT
start
Compare early acute
toxicity
End of RT (5 weeks
after RT start)
Maximum difference
in acute toxicity
4-5 weeks after RT Compare resolution
of acute toxicity
1 year from start of
RT
Early chronic toxicity
3 years from the
start of RT
Long term toxicity
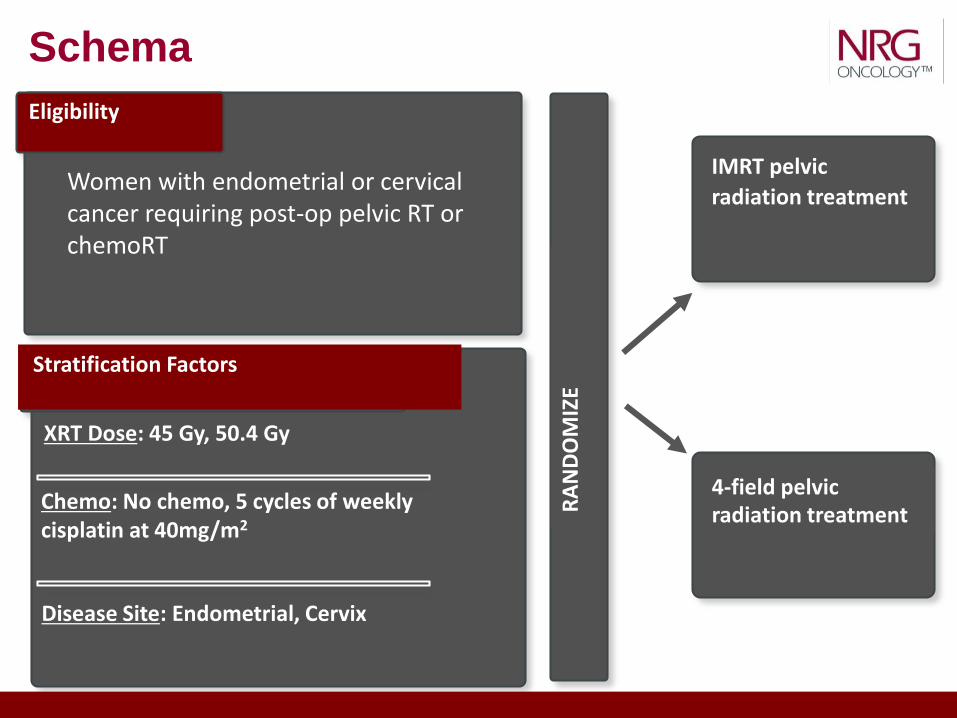
Eligibility
Women with endometrial or cervical cancer requiring post-op pelvic RT or chemoRT
Stratification Factors
Disease Site: Endometrial, Cervix
XRT Dose: 45 Gy, 50.4 Gy
Chemo: No chemo, 5 cycles of weekly cisplatin at 40mg/m2
RA
ND
OM
IZE
IMRT pelvic
radiation treatment
4-field pelvic radiation treatment
Schema
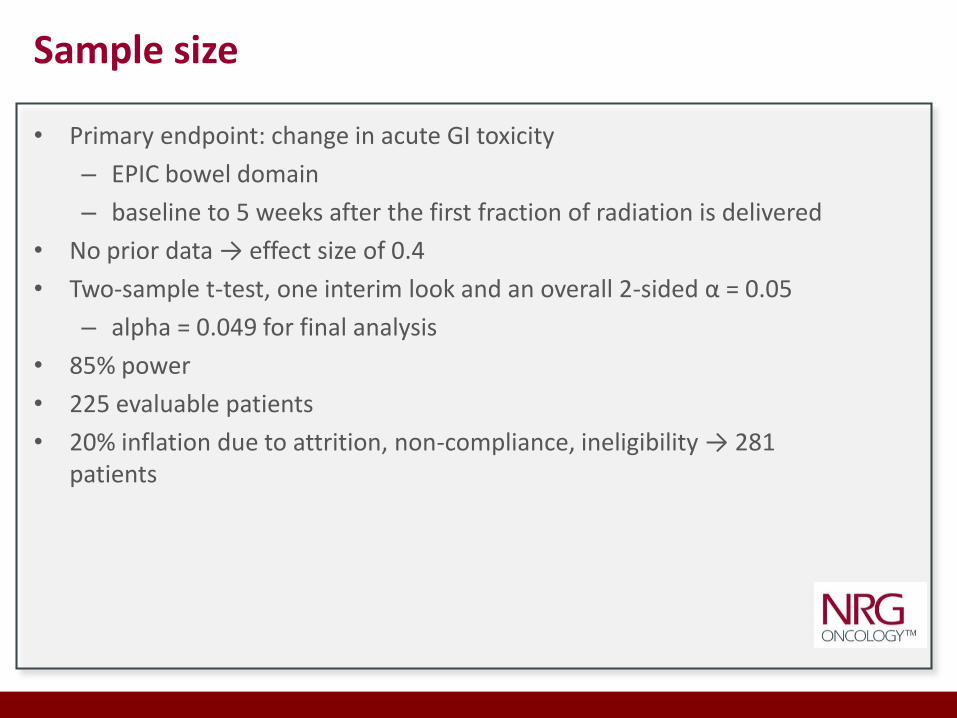
• Primary endpoint: change in acute GI toxicity
– EPIC bowel domain
– baseline to 5 weeks after the first fraction of radiation is delivered
• No prior data → effect size of 0.4
• Two-sample t-test, one interim look and an overall 2-sided α = 0.05
– alpha = 0.049 for final analysis
• 85% power
• 225 evaluable patients
• 20% inflation due to attrition, non-compliance, ineligibility → 281 patients
Sample size
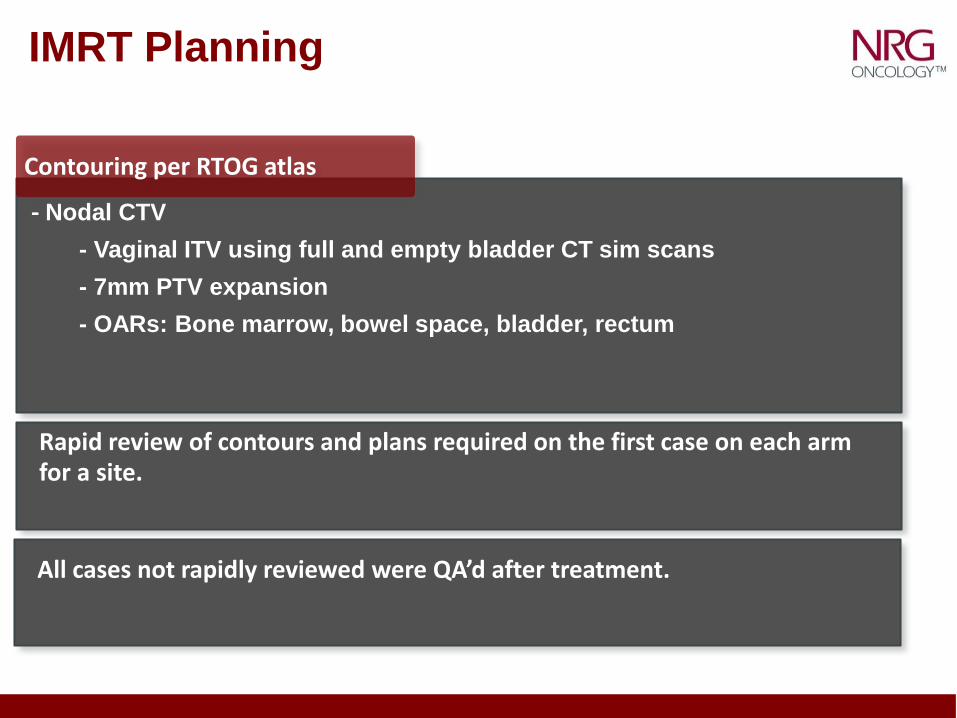
IMRT Planning
- Nodal CTV
- Vaginal ITV using full and empty bladder CT sim scans
- 7mm PTV expansion
- OARs: Bone marrow, bowel space, bladder, rectum
Rapid review of contours and plans required on the first case on each arm for a site.
All cases not rapidly reviewed were QA’d after treatment.
Contouring per RTOG atlas
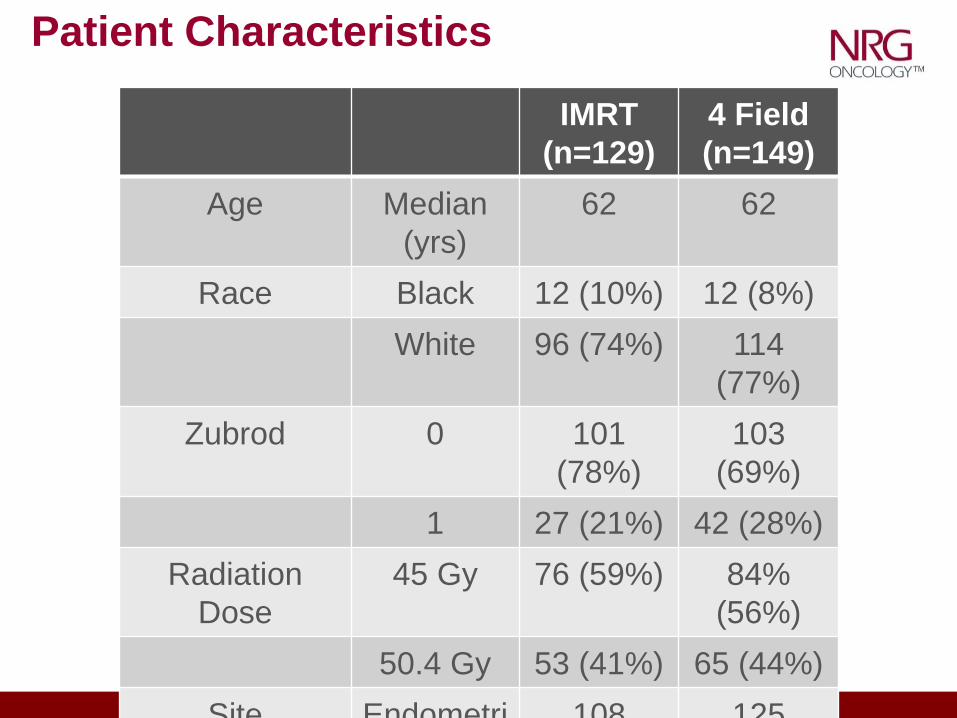
Patient Characteristics
IMRT
(n=129)
4 Field
(n=149)
Age Median
(yrs)
62 62
Race Black 12 (10%) 12 (8%)
White 96 (74%) 114
(77%)
Zubrod 0 101
(78%)
103
(69%)
1 27 (21%) 42 (28%)
Radiation
Dose
45 Gy 76 (59%) 84%
(56%)
50.4 Gy 53 (41%) 65 (44%)
Site Endometri 108 125
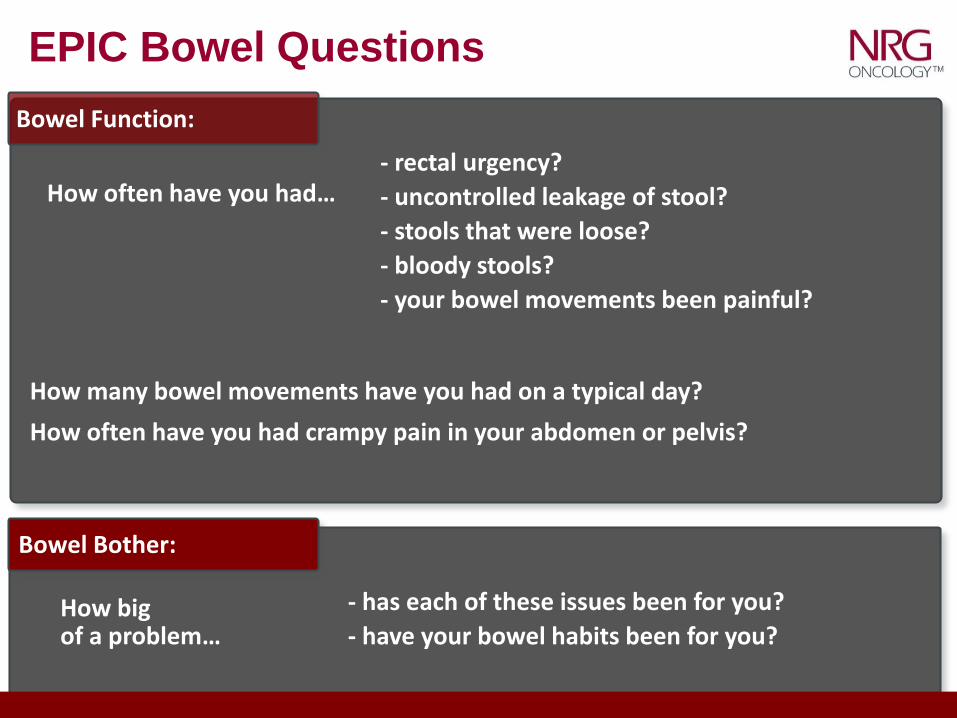
EPIC Bowel Questions
Bowel Function:
- rectal urgency?
- uncontrolled leakage of stool?
- stools that were loose?
- bloody stools?
- your bowel movements been painful?
How often have you had…
How many bowel movements have you had on a typical day?
How often have you had crampy pain in your abdomen or pelvis?
Bowel Bother:
- has each of these issues been for you?
- have your bowel habits been for you?How big of a problem…
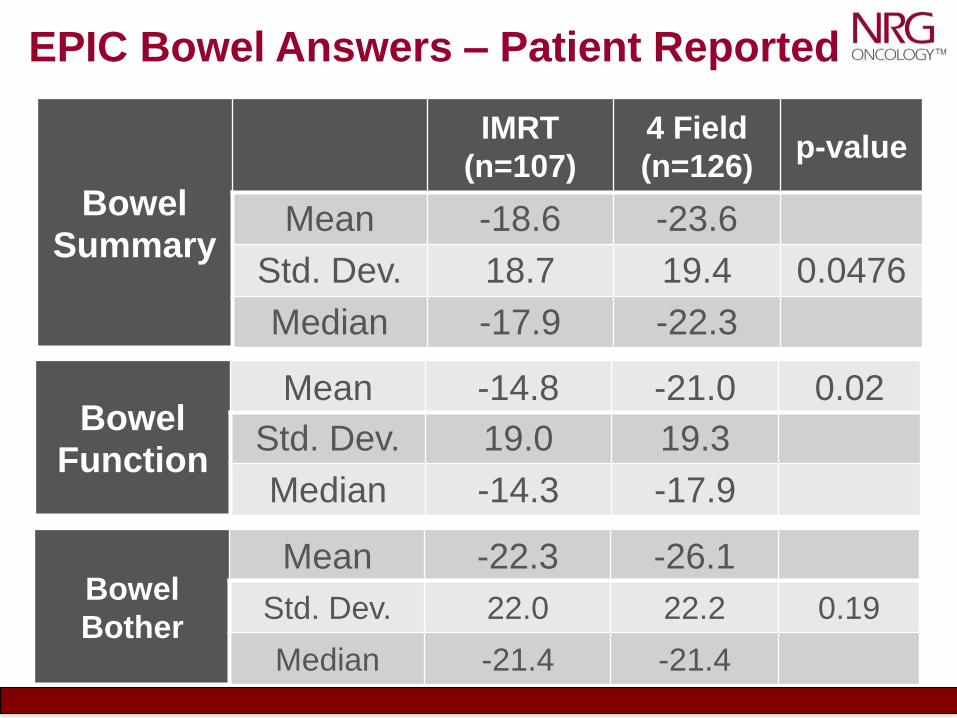
EPIC Bowel Answers – Patient Reported
Bowel Summary
IMRT
(n=107)
4 Field
(n=126)p-value
Mean -18.6 -23.6
Std. Dev. 18.7 19.4 0.0476
Median -17.9 -22.3
Bowel
Bother
Mean -22.3 -26.1
Std. Dev. 22.0 22.2 0.19
Median -21.4 -21.4
Bowel Function
Mean -14.8 -21.0 0.02
Std. Dev. 19.0 19.3
Median -14.3 -17.9
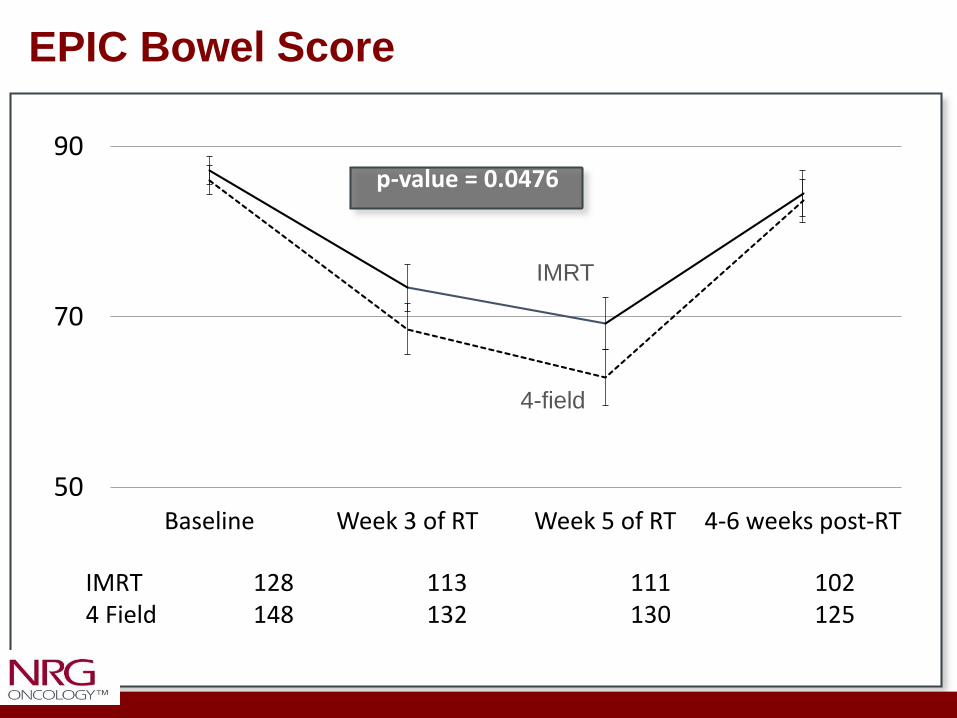
50
70
90
Baseline Week 3 of RT Week 5 of RT 4-6 weeks post-RT
IMRT 128 113 111 1024 Field 148 132 130 125
EPIC Bowel Score
p-value = 0.0476
IMRT
4-field
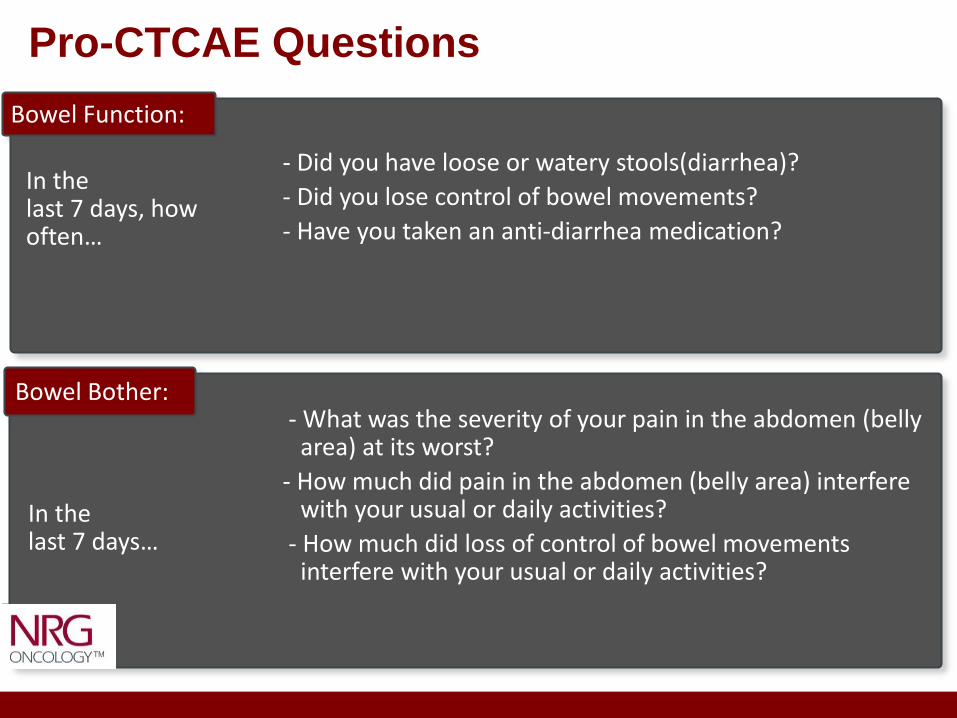
Pro-CTCAE Questions
Bowel Function:
- Did you have loose or watery stools(diarrhea)?
- Did you lose control of bowel movements?
- Have you taken an anti-diarrhea medication?
In the last 7 days, how often…
Bowel Bother:
In the last 7 days…
- What was the severity of your pain in the abdomen (belly area) at its worst?
- How much did pain in the abdomen (belly area) interfere with your usual or daily activities?
- How much did loss of control of bowel movements interfere with your usual or daily activities?
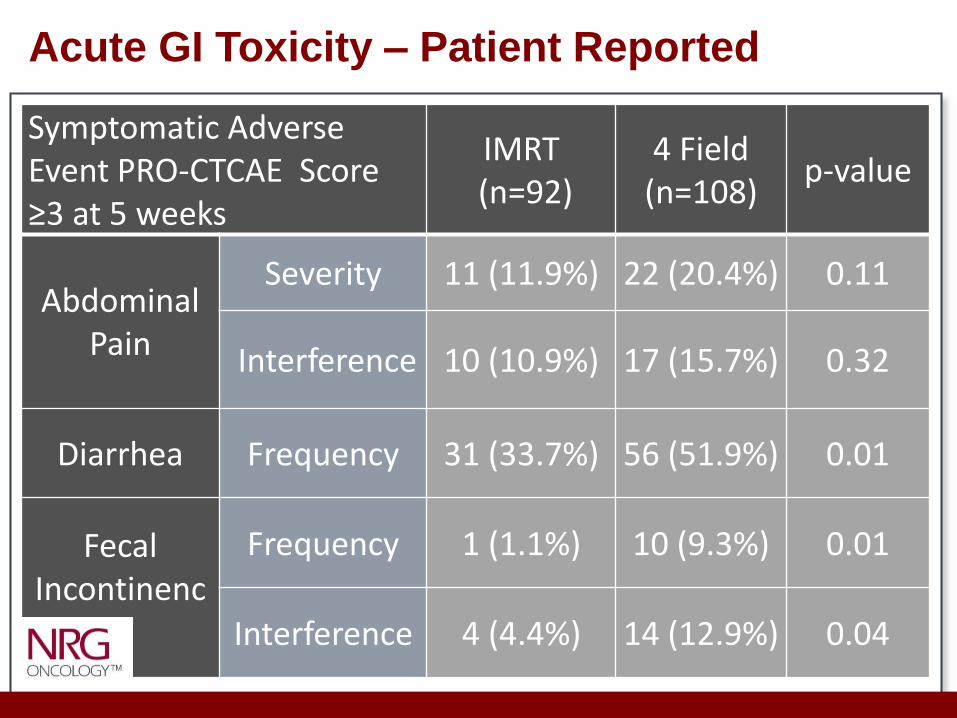
Acute GI Toxicity – Patient Reported
Symptomatic Adverse Event PRO-CTCAE Score ≥3 at 5 weeks
IMRT (n=92)
4 Field (n=108)
p-value
Abdominal Pain
Severity 11 (11.9%) 22 (20.4%) 0.11
Interference 10 (10.9%) 17 (15.7%) 0.32
Diarrhea Frequency 31 (33.7%) 56 (51.9%) 0.01
Fecal Incontinenc
e
Frequency 1 (1.1%) 10 (9.3%) 0.01
Interference 4 (4.4%) 14 (12.9%) 0.04
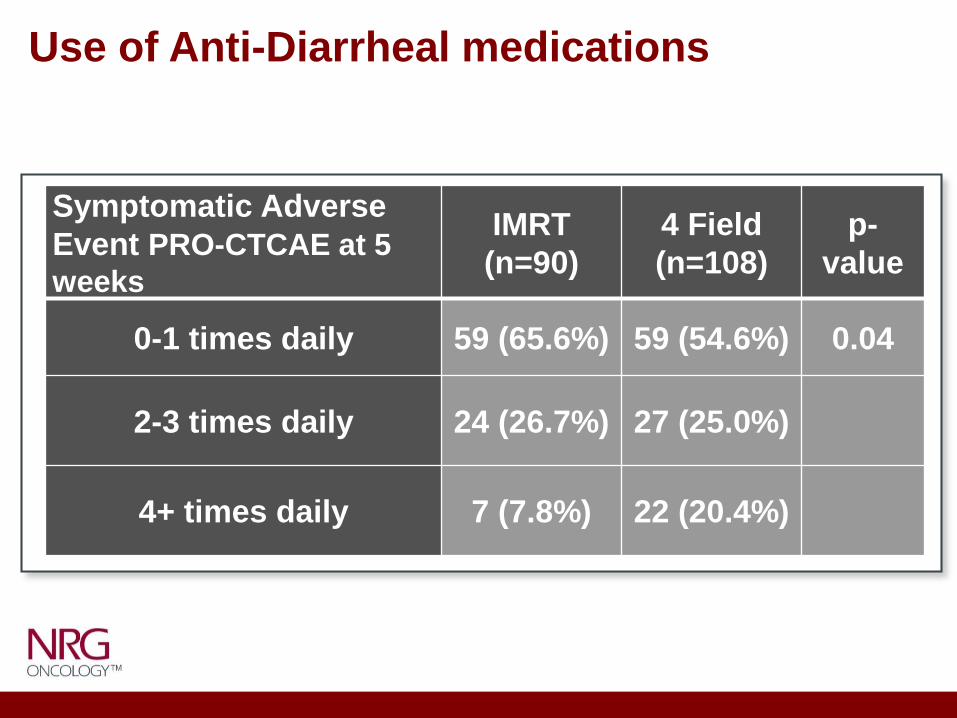
Use of Anti-Diarrheal medications
Symptomatic Adverse
Event PRO-CTCAE at 5
weeks
IMRT
(n=90)
4 Field
(n=108)
p-
value
0-1 times daily 59 (65.6%) 59 (54.6%) 0.04
2-3 times daily 24 (26.7%) 27 (25.0%)
4+ times daily 7 (7.8%) 22 (20.4%)
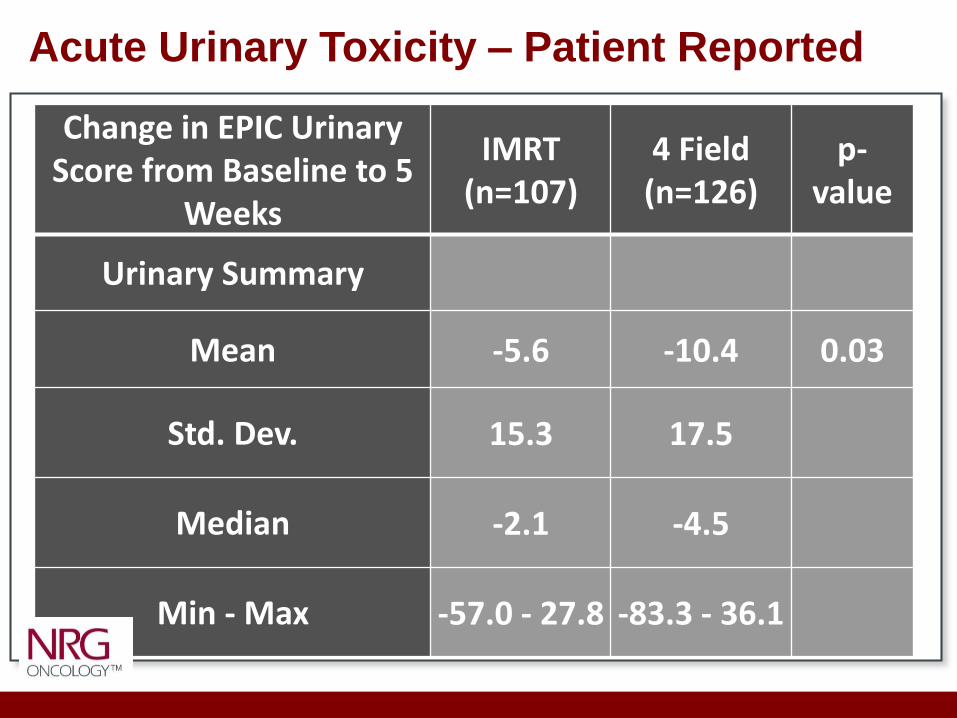
Acute Urinary Toxicity – Patient Reported
Change in EPIC Urinary Score from Baseline to 5
Weeks
IMRT (n=107)
4 Field (n=126)
p-value
Urinary Summary
Mean -5.6 -10.4 0.03
Std. Dev. 15.3 17.5
Median -2.1 -4.5
Min - Max -57.0 - 27.8 -83.3 - 36.1
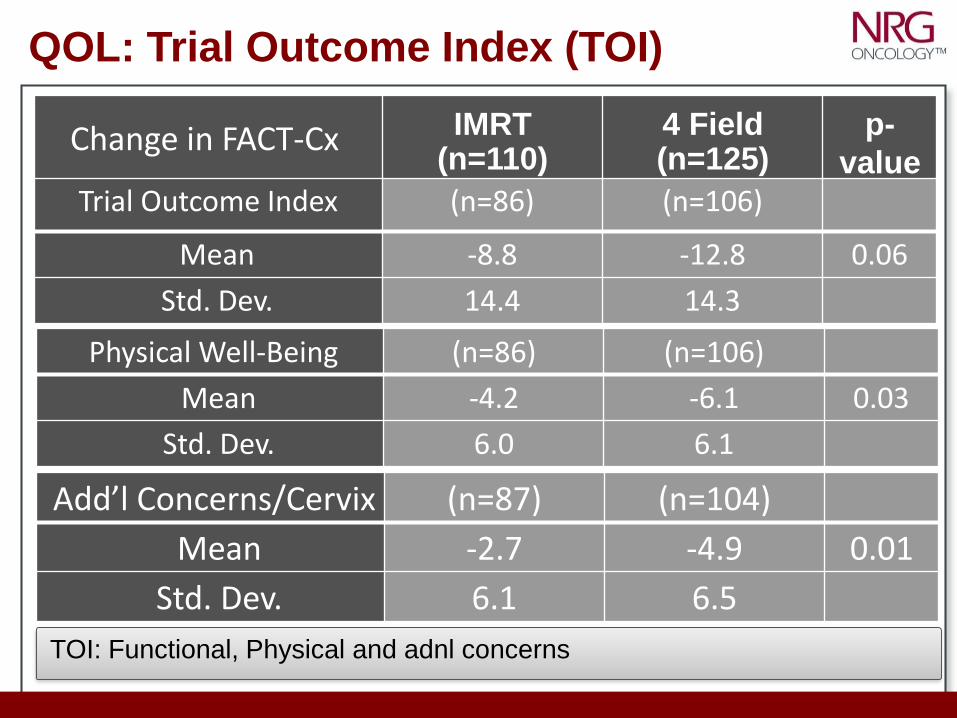
QOL: Trial Outcome Index (TOI)
Change in FACT-Cx IMRT (n=110)
4 Field (n=125)
p-
value
Physical Well-Being (n=86) (n=106)
Mean -4.2 -6.1 0.03
Std. Dev. 6.0 6.1
Add’l Concerns/Cervix (n=87) (n=104)
Mean -2.7 -4.9 0.01
Std. Dev. 6.1 6.5
Trial Outcome Index (n=86) (n=106)
Mean -8.8 -12.8 0.06
Std. Dev. 14.4 14.3
TOI: Functional, Physical and adnl concerns
Pelvic IMRT reduces acute patient reported GI and GU toxicity compared to standard pelvic RT.
Pelvic IMRT improves quality of life metrics during treatment as
compared to standard pelvic RT.
Longer term follow up will determine if these differences in acute
toxicity result in lower rates of late toxicity.
Pelvic IMRT reduces need for anti-diarrheal medications as
compared to standard pelvic RT.
Conclusions
Atlas Update In Progress
• Utilize patterns of recurrence data from RTOG
0418.
• Better define obturator nodal region.
• Eliminate all reference to boney landmarks.
• Give recommendations regarding rectal
distention.
• Included recommendations for common iliacs
and para-aortic CTV.
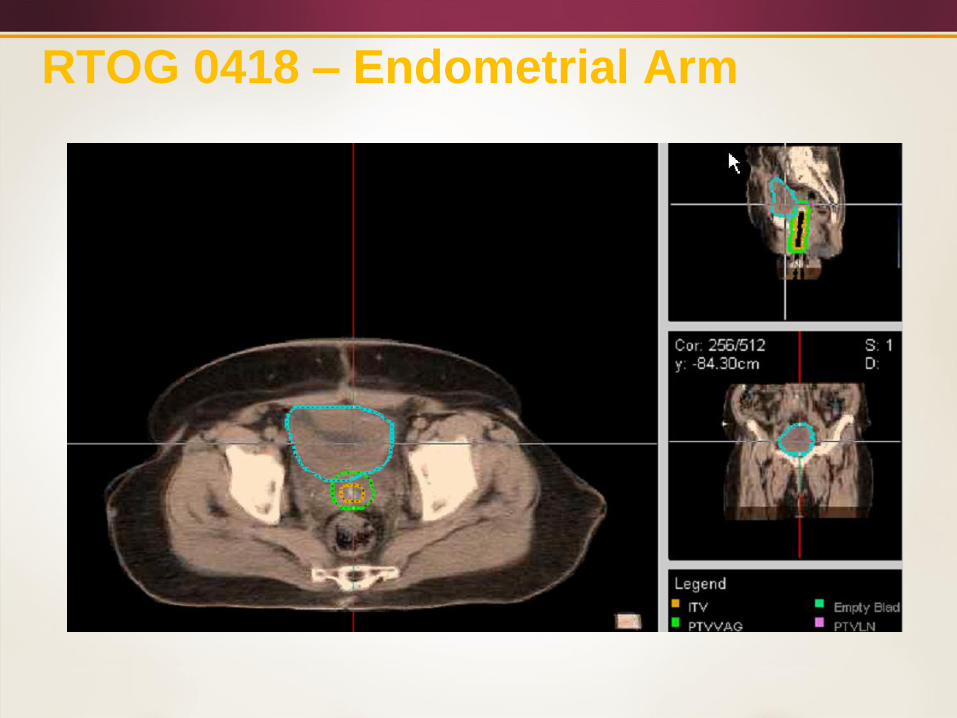
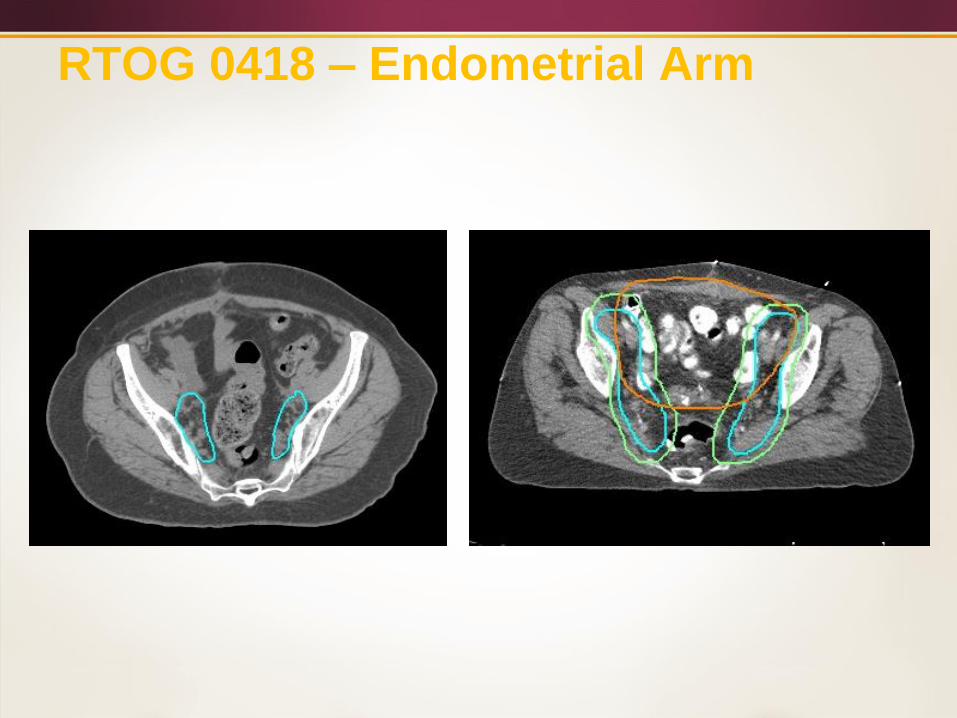
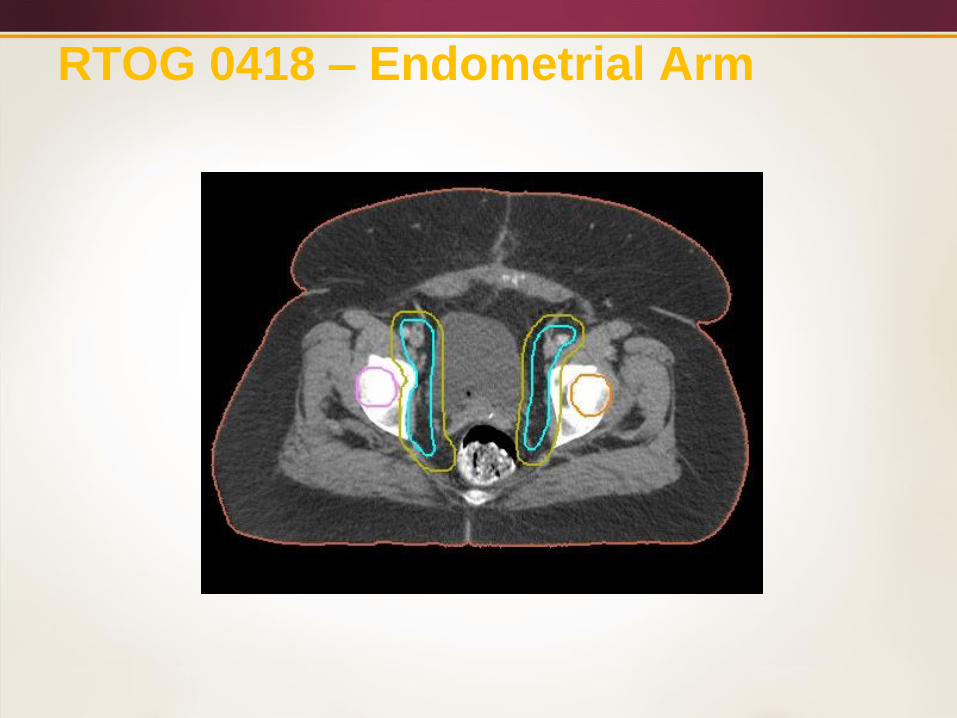
RTOG 0418 – Endometrial Arm
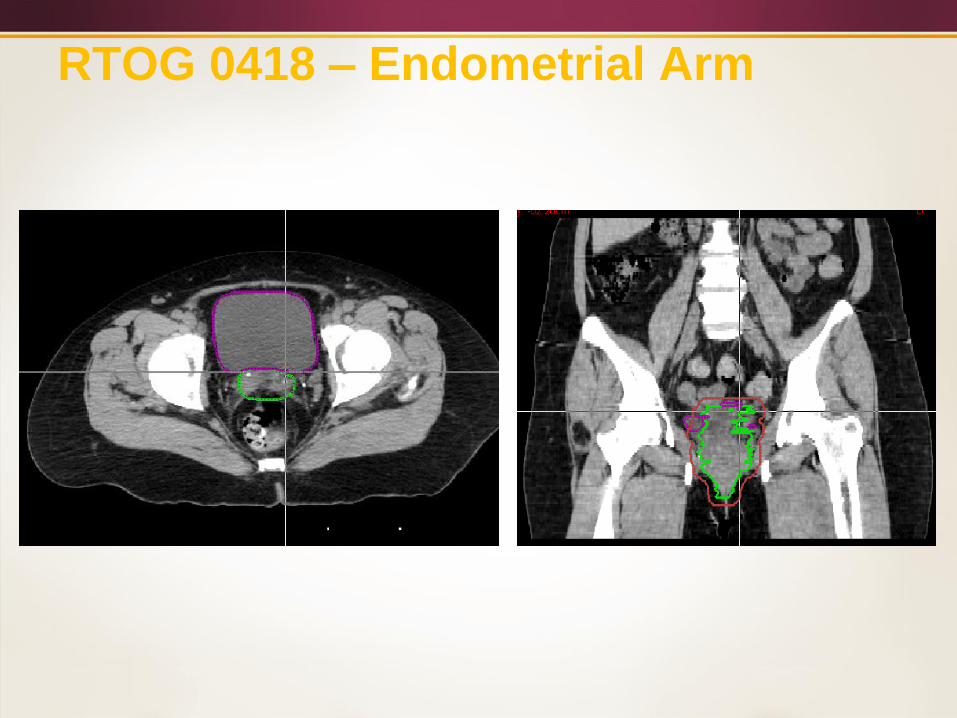
RTOG 0418 – Endometrial Arm
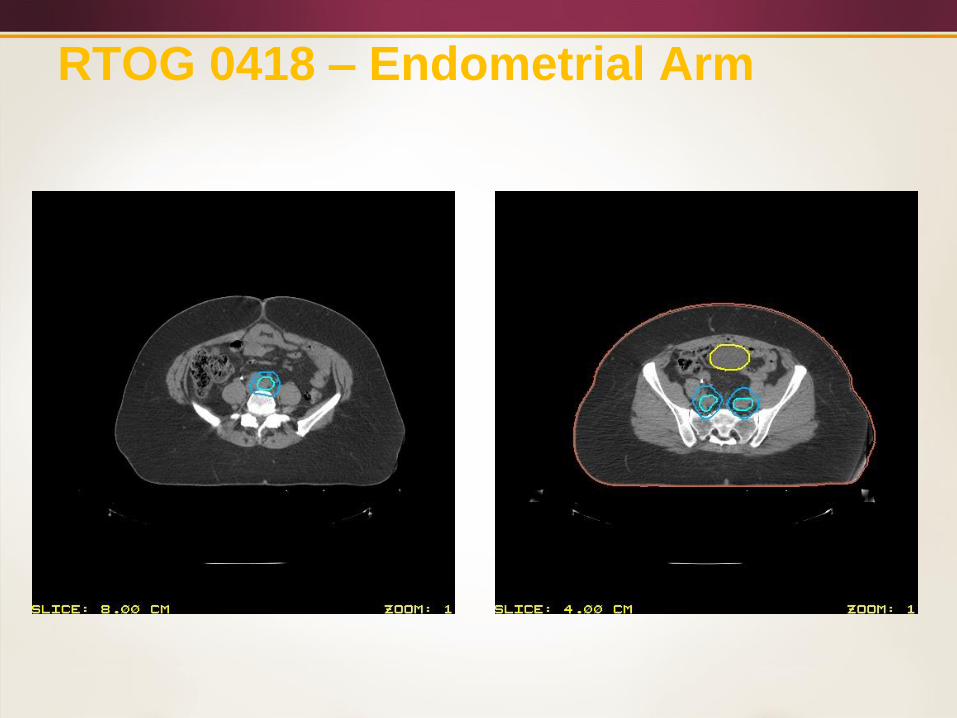
RTOG 0418 – Endometrial Arm
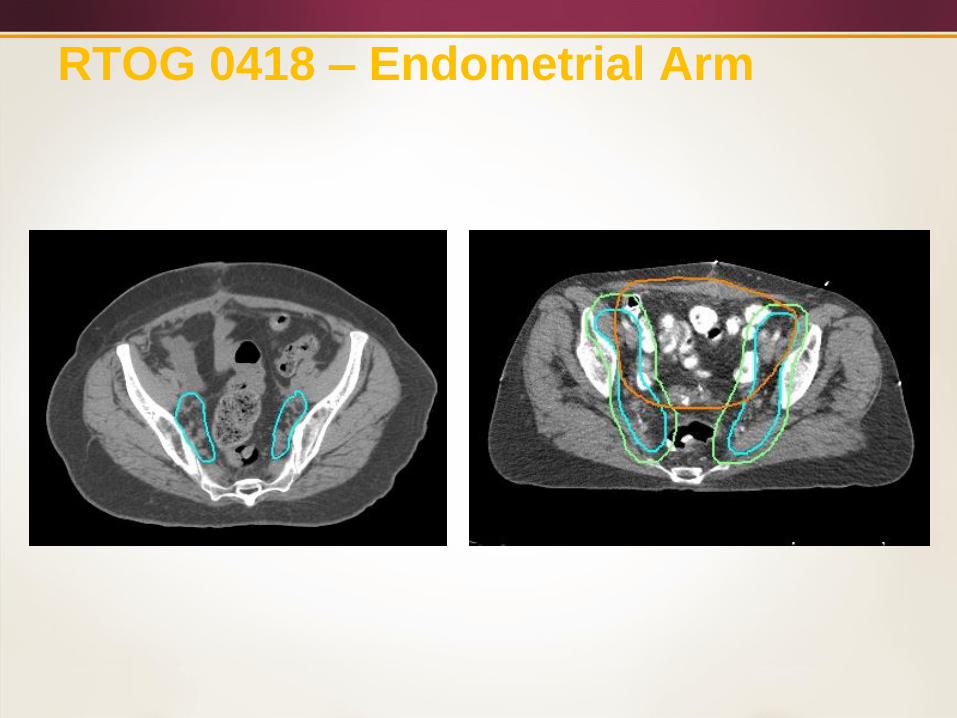
RTOG 0418 – Endometrial Arm
RTOG 0418 – Endometrial Arm
RTOG 0418 – Endometrial Arm
CASE STUDY
The patient was treated with pelvic IMRT on
RTOG 0418 with concurrent weekly cisplatin.
An ITV was accomplished to determine the CTV.
The consensus contouring guidelines were
utilized to draw the CTV.
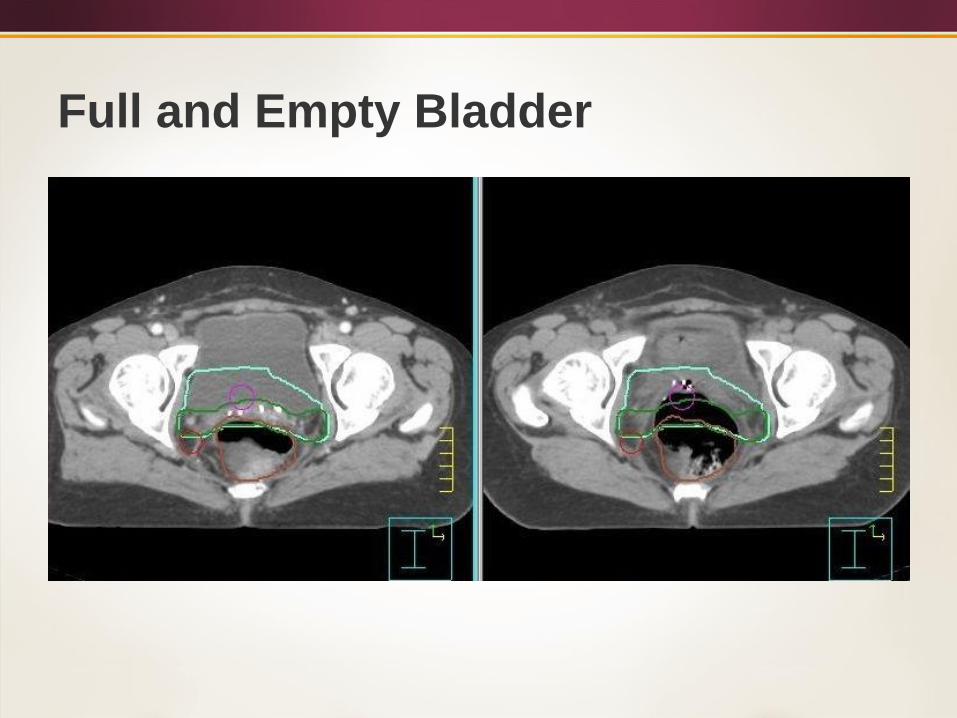
Full and Empty Bladder
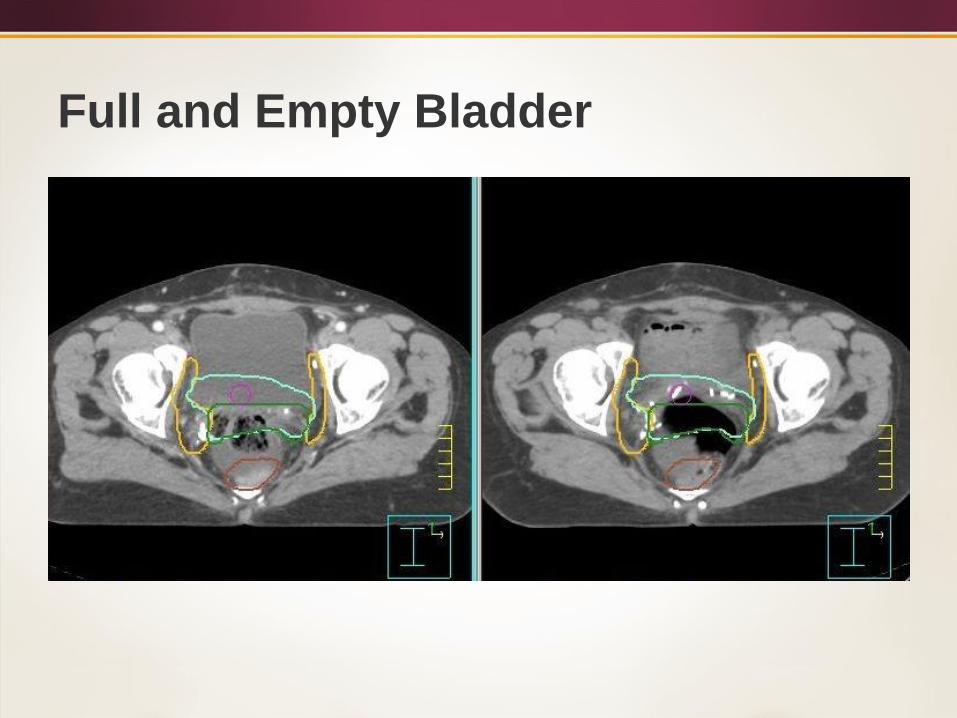
Full and Empty Bladder
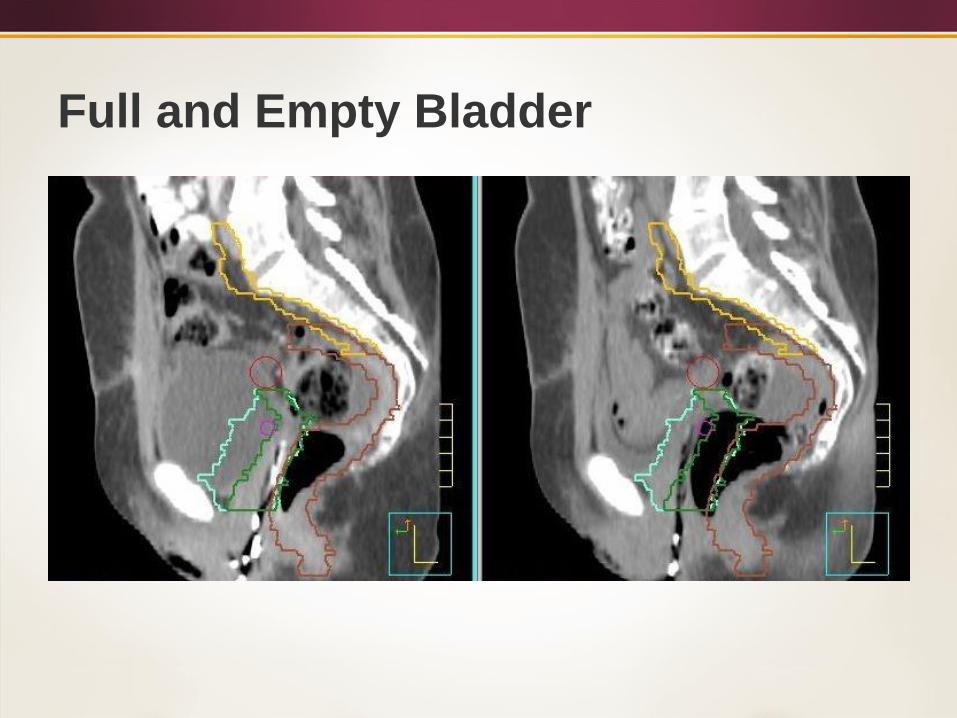
Full and Empty Bladder

Post-Treatment Complications
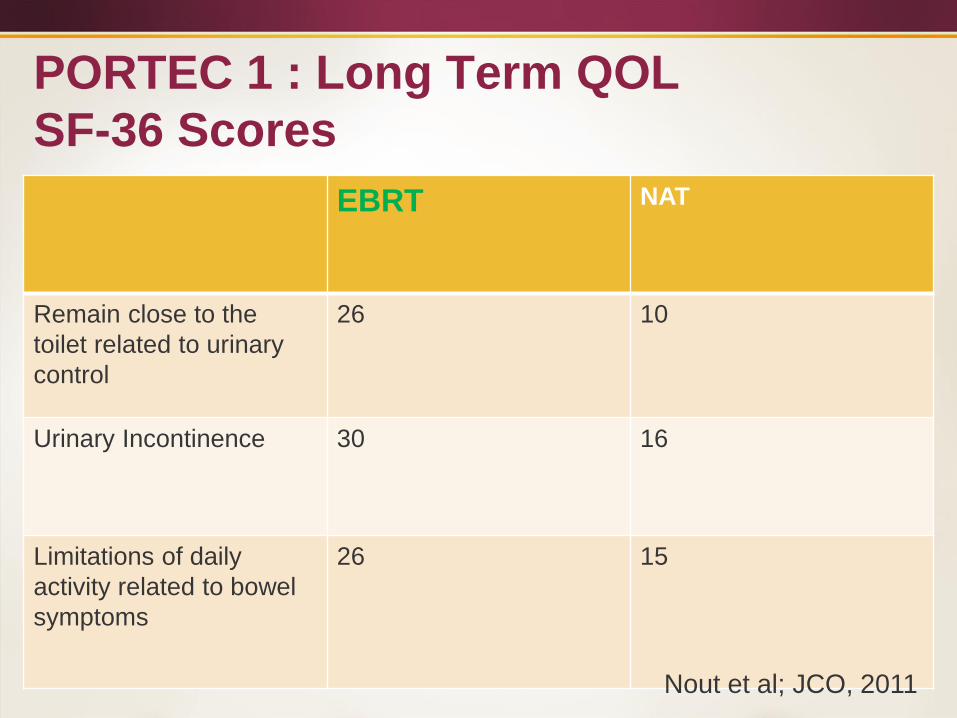
PORTEC 1 : Long Term QOL
SF-36 Scores
EBRT NAT
Remain close to the
toilet related to urinary
control
26 10
Urinary Incontinence 30 16
Limitations of daily
activity related to bowel
symptoms
26 15
Nout et al; JCO, 2011
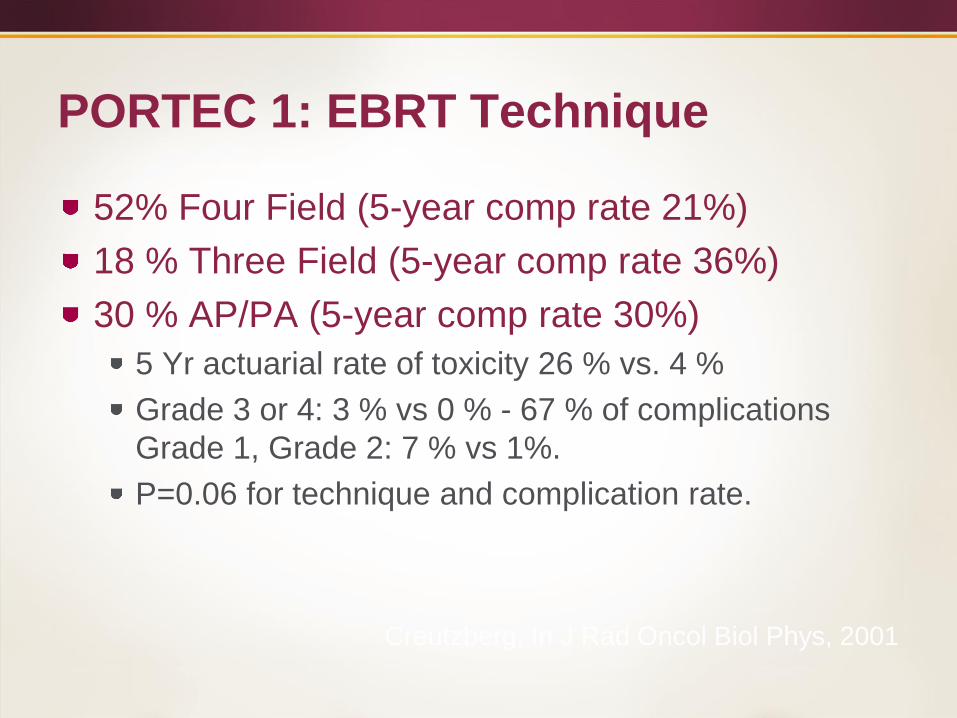
PORTEC 1: EBRT Technique
52% Four Field (5-year comp rate 21%)
18 % Three Field (5-year comp rate 36%)
30 % AP/PA (5-year comp rate 30%)
5 Yr actuarial rate of toxicity 26 % vs. 4 %
Grade 3 or 4: 3 % vs 0 % - 67 % of complications
Grade 1, Grade 2: 7 % vs 1%.
P=0.06 for technique and complication rate.
Creutzberg, In J Rad Oncol Biol Phys, 2001
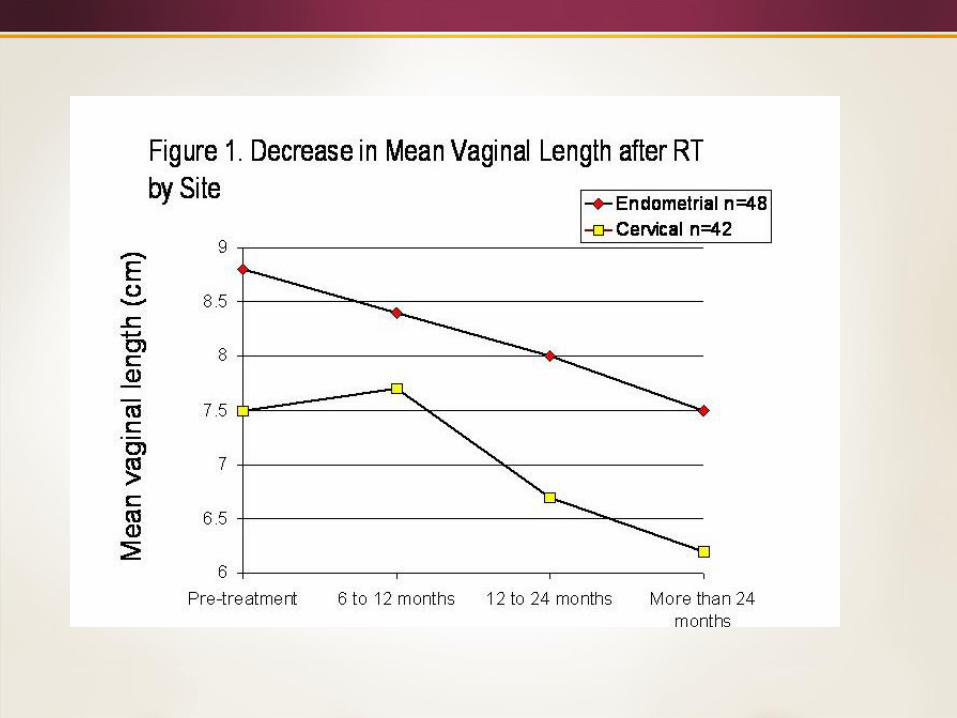
Vaginal Length after Intracavitary
Radiotherapy
Looked at 90 patients with intracavitary RT
after treatment for cervical or endometrial
CA (48).
Measurements were taken at 6 and 12
months and then yearly.
The vaginal dilator compliance rate was 68
% of using 1 o more times per week.
Bruner et al,
Int J Radiol
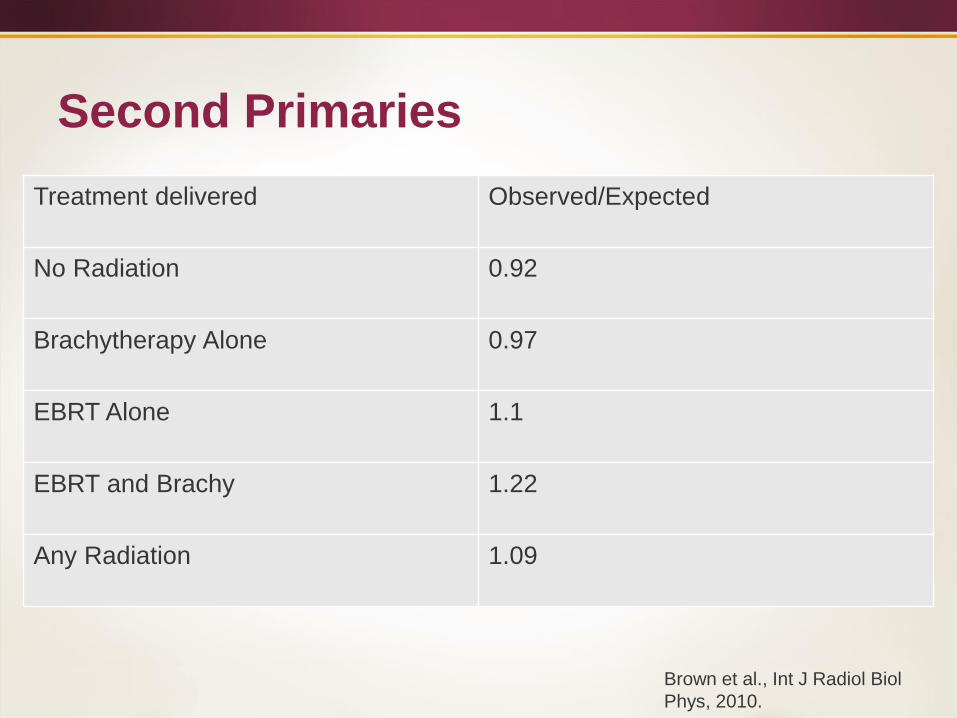
Second Primaries
Treatment delivered Observed/Expected
No Radiation 0.92
Brachytherapy Alone 0.97
EBRT Alone 1.1
EBRT and Brachy 1.22
Any Radiation 1.09
Brown et al., Int J Radiol Biol
Phys, 2010.
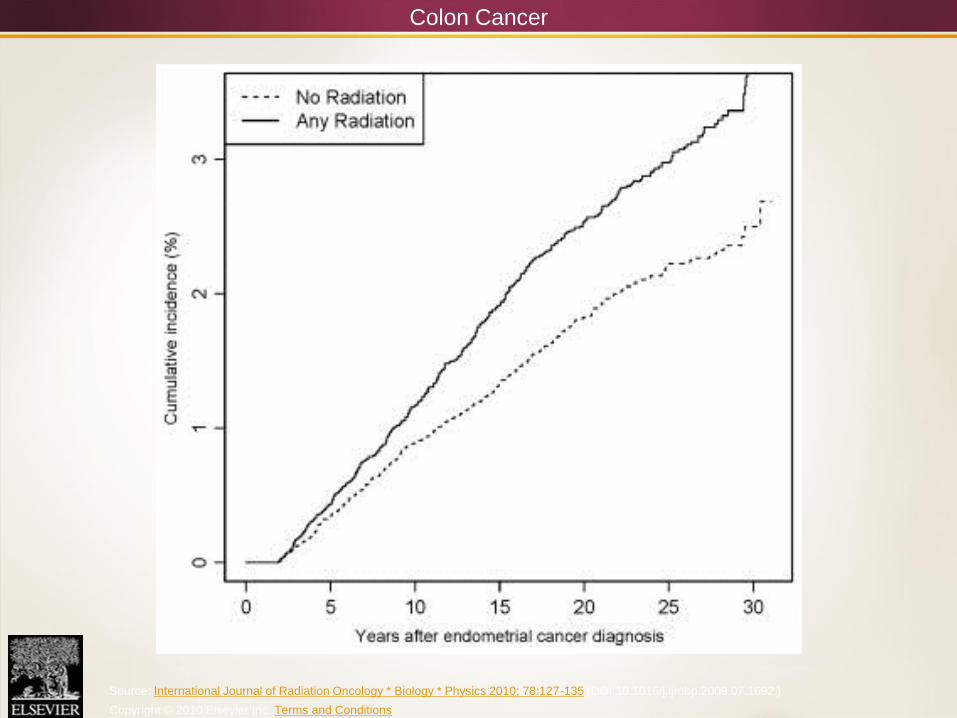
Colon Cancer
Source: International Journal of Radiation Oncology * Biology * Physics 2010; 78:127-135 (DOI:10.1016/j.ijrobp.2009.07.1692 )
Copyright © 2010 Elsevier Inc. Terms and Conditions
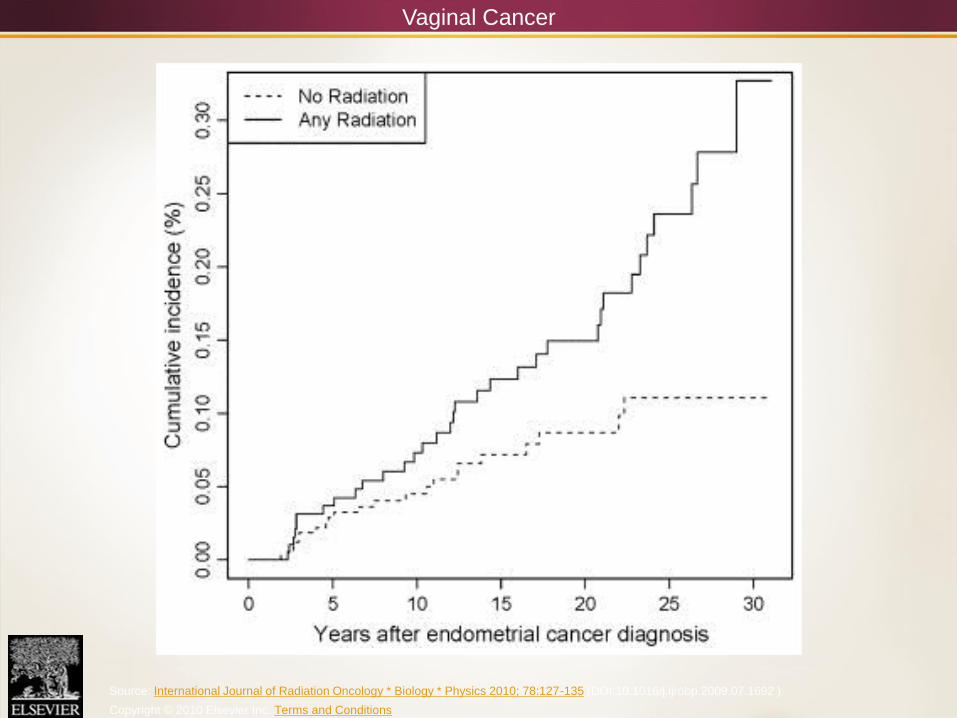
Vaginal Cancer
Source: International Journal of Radiation Oncology * Biology * Physics 2010; 78:127-135 (DOI:10.1016/j.ijrobp.2009.07.1692 )
Copyright © 2010 Elsevier Inc. Terms and Conditions
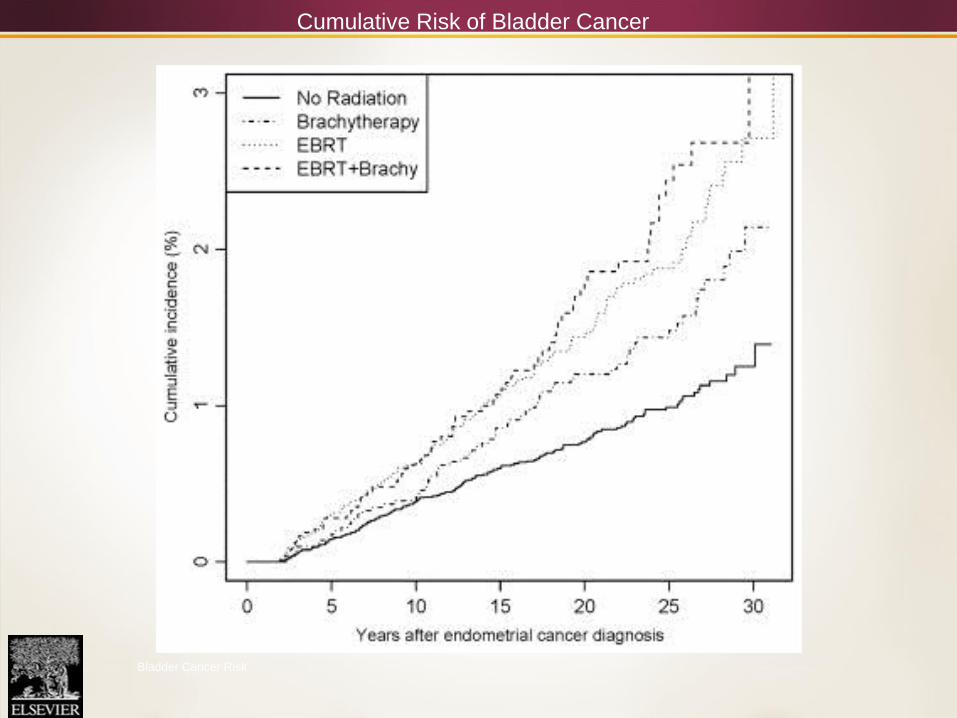
Cumulative Risk of Bladder Cancer
Bladder Cancer Risk
PORTEC 1
At a median follow-up of 13.3 years 19% of the
patients had a second primary.
22% in the EBRT group,
16% in the no additional treatment group
P=0.10
Can Chemotherapy Replace
Pelvic Radiotherapy?
A randomized phase III trial of pelvic radiation therapy
(PXRT) versus vaginal cuff brachytherapy followed by
paclitaxel/carboplatin chemotherapy (VCB/C) in
patients with high risk (HR), early stage endometrial
cancer (EC): a Gynecologic Oncology Group trial.
McMeekin DS, Filiaci VL, Aghajanian C, et al. Proceedings of the 45th
Annual Meeting on Women's Cancer, Society of Gynecologic
Oncology; 2014, March 22; Tampa, FL.
GOG 249
Primary objective: To determine if treatment with VCB/C
reduces the rate of recurrence or death (RFS) when
compared to PXRT
Secondary objectives: Compare OS, patterns of failure,
toxicity/functioning between arms
– All patients underwent hysterectomy +/- staging
CT/MRI required if no LND
– Endometrioid histology- risk criteria
> 70 + 1, age >50 +2, age > 18 + 3
Factors: LVSI, Gr 2-3, outer ½ invasion
– Serous/Clear cell- stage I-II
– Stage II any histology
GOG 249
Therapy initiated within 12 weeks after surgery
Arm I- Pelvic Radiation (PXRT)
– 180cGy/day X 25-28 fractions 4500-5040 in 5-6 weeks
– Standard or IMRT permitted
– VCB allowed for stage II or Stage I S/CC
Arm II- Vaginal Cuff Brachytherapy + Chemotherapy
(VCB/C)
– LDR or HDR
– HDR 6-7 Gy X 3 or 10-10.5 X 3 or 6 Gy X 5
– Chemotherapy to start within three weeks of VCB
– Carboplatin AUC 6 + Paclitaxel 175mg/m2 every 21 days X 3
Statistical Design
1:1 Randomization
Stratification:
– Lymphadenectomy
– Intent to use VCB in Arm I
Assumptions:
– 85% of patients treated with PXRT alive, recurrence –
free at three years
– Relative decrease in recurrence/death hazard of 49%
increases three year RFS to 92% important
– Required 77 failures (90% power, type 1 error= 0.05
(one tailed) sample size 562 patients
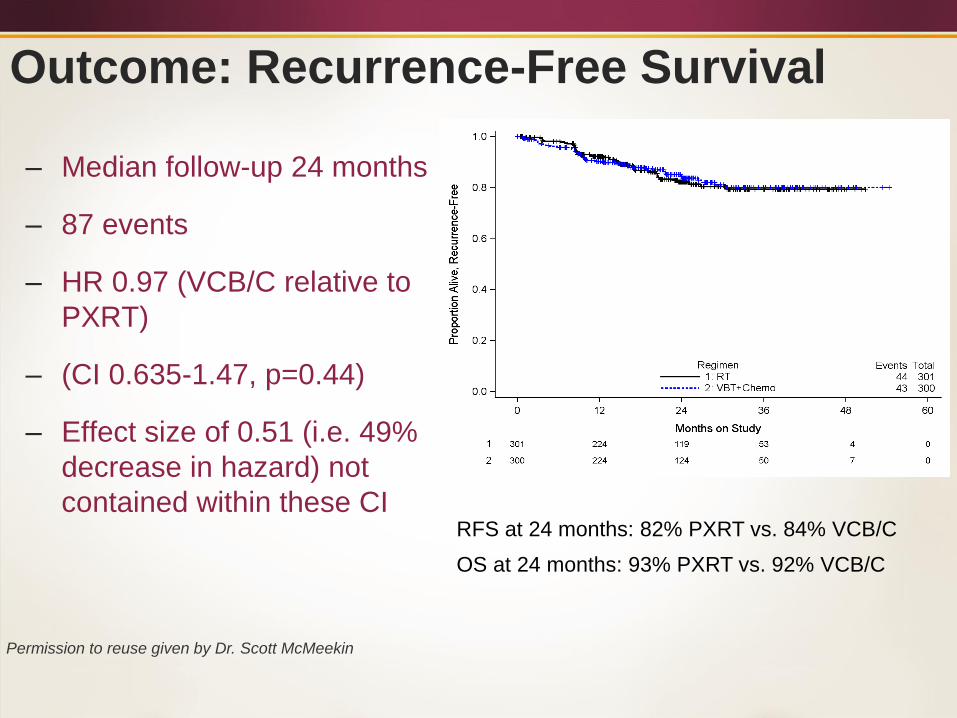
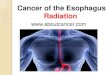
Outcome: Recurrence-Free Survival
– Median follow-up 24 months
– 87 events
– HR 0.97 (VCB/C relative to
PXRT)
– (CI 0.635-1.47, p=0.44)
– Effect size of 0.51 (i.e. 49%
decrease in hazard) not
contained within these CIRFS at 24 months: 82% PXRT vs. 84% VCB/C
OS at 24 months: 93% PXRT vs. 92% VCB/C
Permission to reuse given by Dr. Scott McMeekin
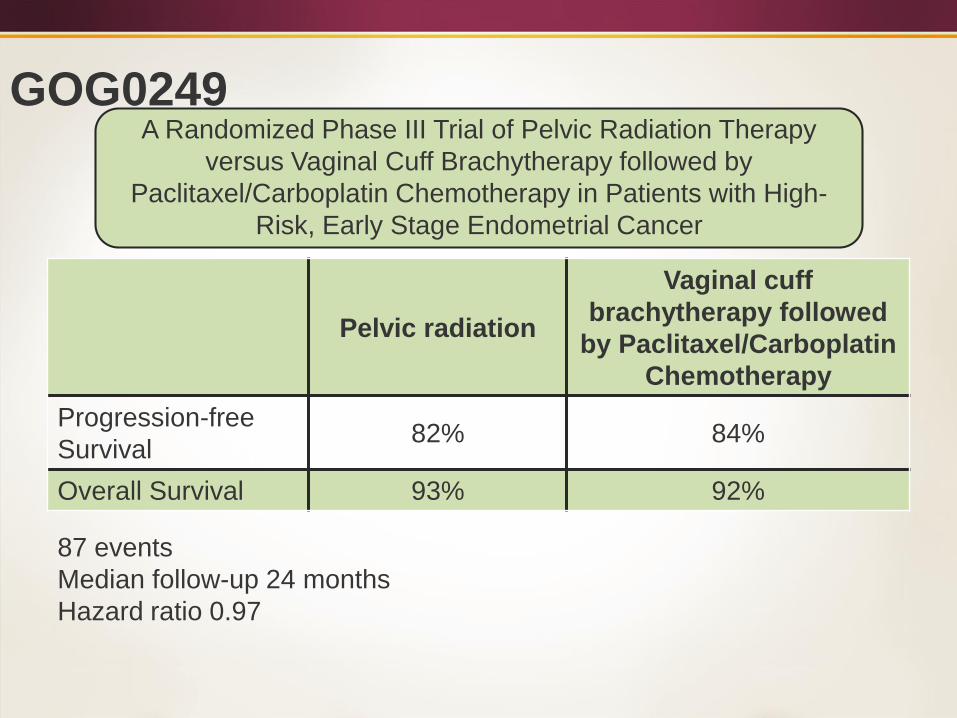
GOG0249
Pelvic radiation
Vaginal cuff
brachytherapy followed
by Paclitaxel/Carboplatin
Chemotherapy
Progression-free
Survival82% 84%
Overall Survival 93% 92%
87 events
Median follow-up 24 months
Hazard ratio 0.97
A Randomized Phase III Trial of Pelvic Radiation Therapy
versus Vaginal Cuff Brachytherapy followed by
Paclitaxel/Carboplatin Chemotherapy in Patients with High-
Risk, Early Stage Endometrial Cancer
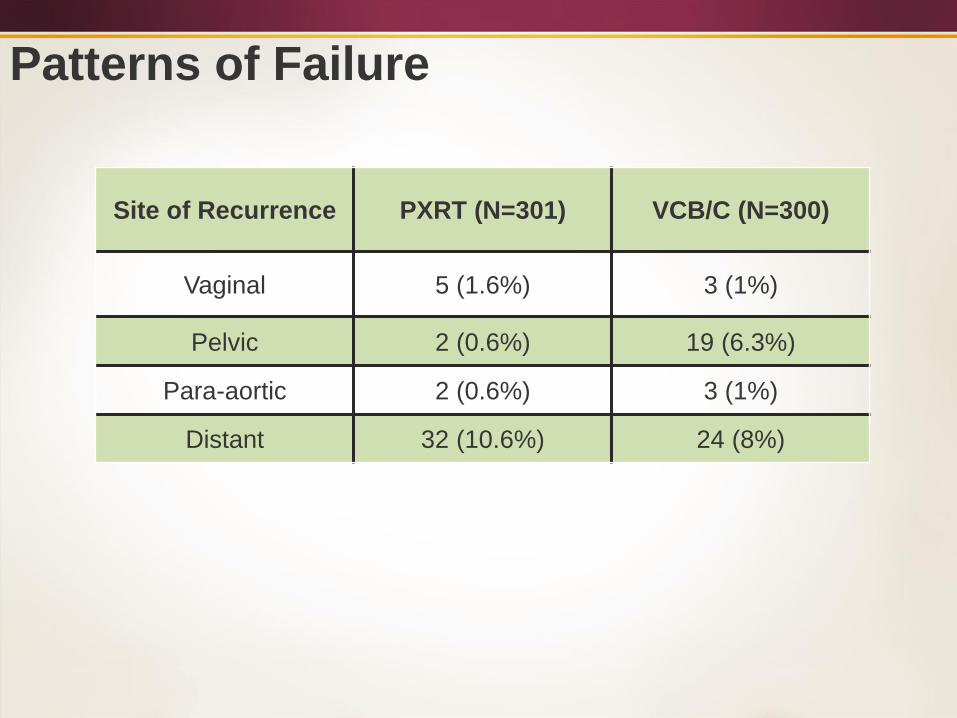
Patterns of Failure
Site of Recurrence PXRT (N=301) VCB/C (N=300)
Vaginal 5 (1.6%) 3 (1%)
Pelvic 2 (0.6%) 19 (6.3%)
Para-aortic 2 (0.6%) 3 (1%)
Distant 32 (10.6%) 24 (8%)
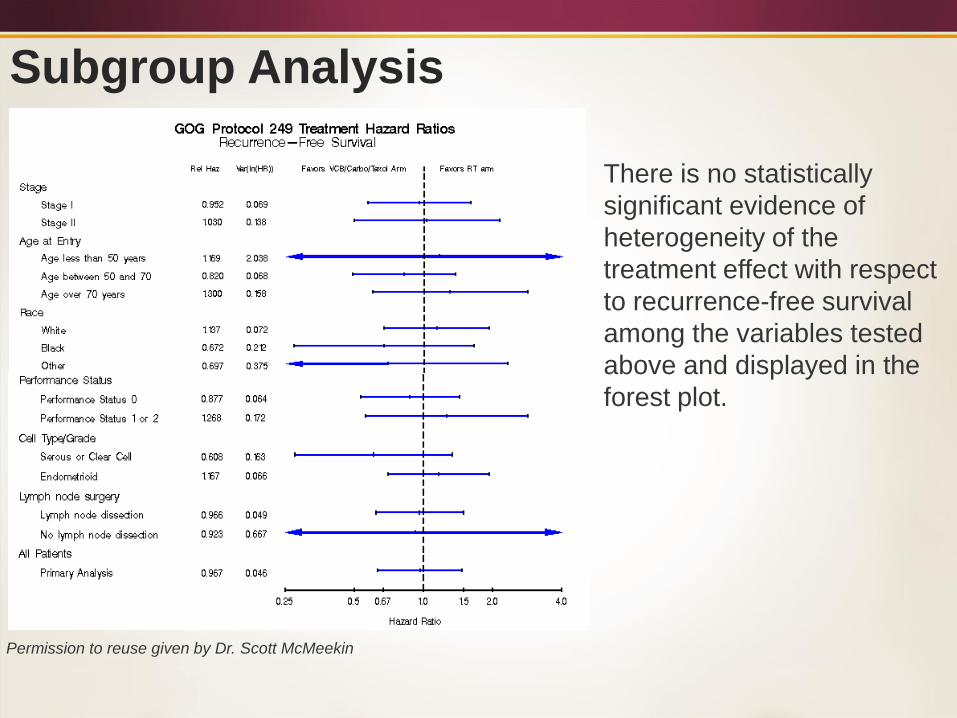
Subgroup Analysis
There is no statistically
significant evidence of
heterogeneity of the
treatment effect with respect
to recurrence-free survival
among the variables tested
above and displayed in the
forest plot.
Permission to reuse given by Dr. Scott McMeekin
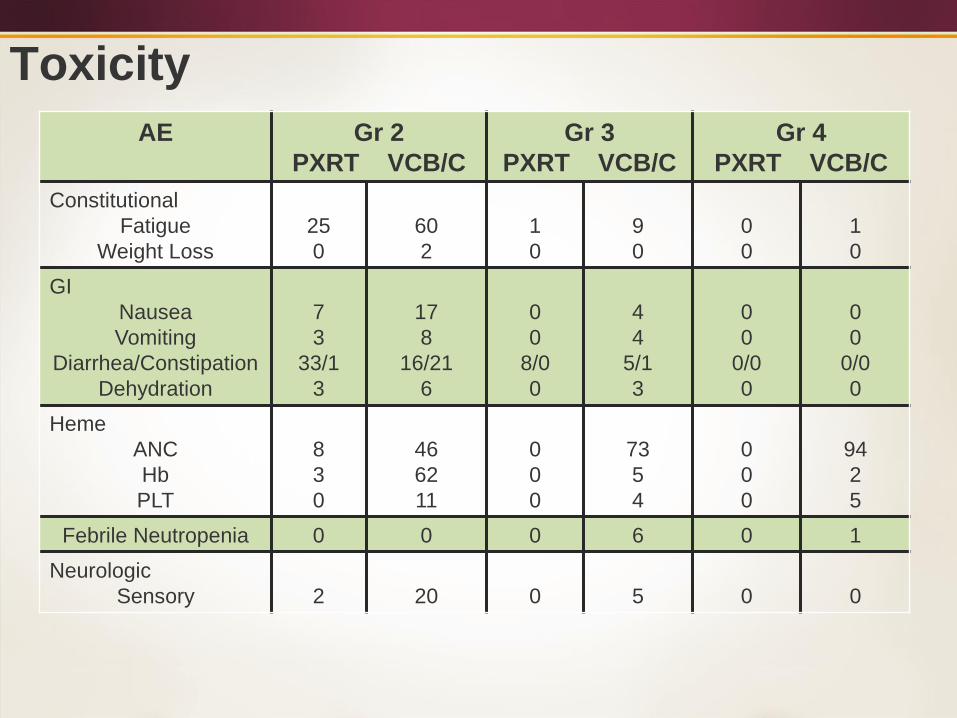
Toxicity
AE Gr 2
PXRT VCB/C
Gr 3
PXRT VCB/C
Gr 4
PXRT VCB/C
Constitutional
Fatigue
Weight Loss
25
0
60
2
1
0
9
0
0
0
1
0
GI
Nausea
Vomiting
Diarrhea/Constipation
Dehydration
7
3
33/1
3
17
8
16/21
6
0
0
8/0
0
4
4
5/1
3
0
0
0/0
0
0
0
0/0
0
Heme
ANC
Hb
PLT
8
3
0
46
62
11
0
0
0
73
5
4
0
0
0
94
2
5
Febrile Neutropenia 0 0 0 6 0 1
Neurologic
Sensory 2 20 0 5 0 0
Locally Advanced Disease
In general, most reports have used “involved field”
radiotherapy for patients with Stage III disease.
Whole Abdominal Radiotherapy
GOG 122 noted a significant worse outcome in
advanced patients with WAR (38% 5-year survival)
as compared to chemotherapy.
GOG 122 delivered 30 Gy to the whole abdomen
and 15 Gy to the pelvis – 25 % of patients with
stage IV.
Our series of WAR patients noted a 86 % 5-year
survival, Smith et al noted a 77 % 3-year survival.
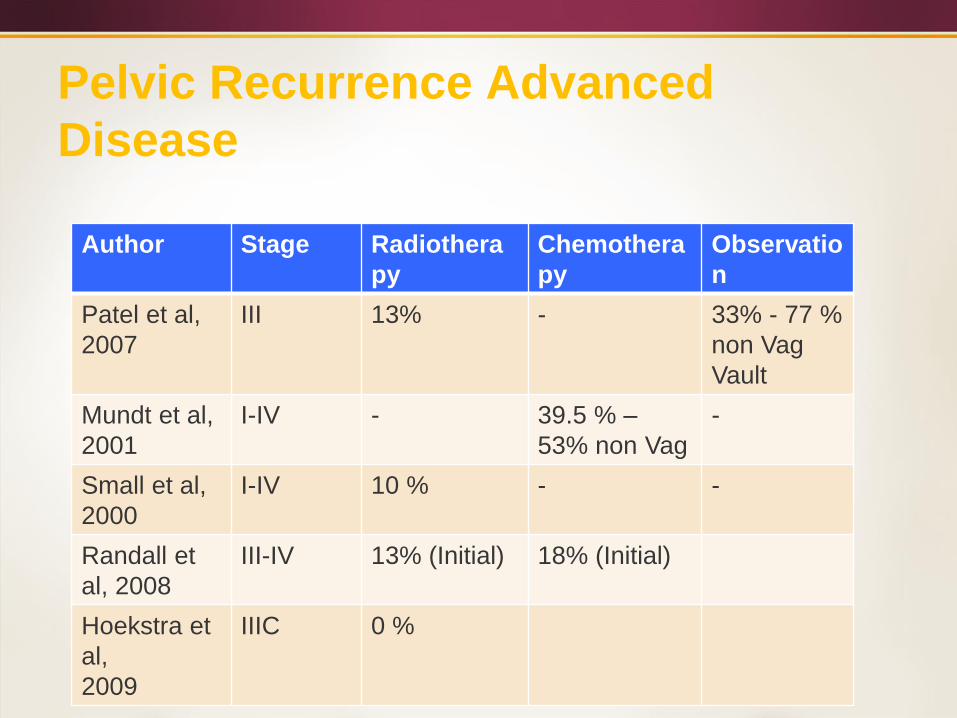
Pelvic Recurrence Advanced
Disease
Author Stage Radiothera
py
Chemothera
py
Observatio
n
Patel et al,
2007
III 13% - 33% - 77 %
non Vag
Vault
Mundt et al,
2001
I-IV - 39.5 % –
53% non Vag
-
Small et al,
2000
I-IV 10 % - -
Randall et
al, 2008
III-IV 13% (Initial) 18% (Initial)
Hoekstra et
al,
2009
IIIC 0 %
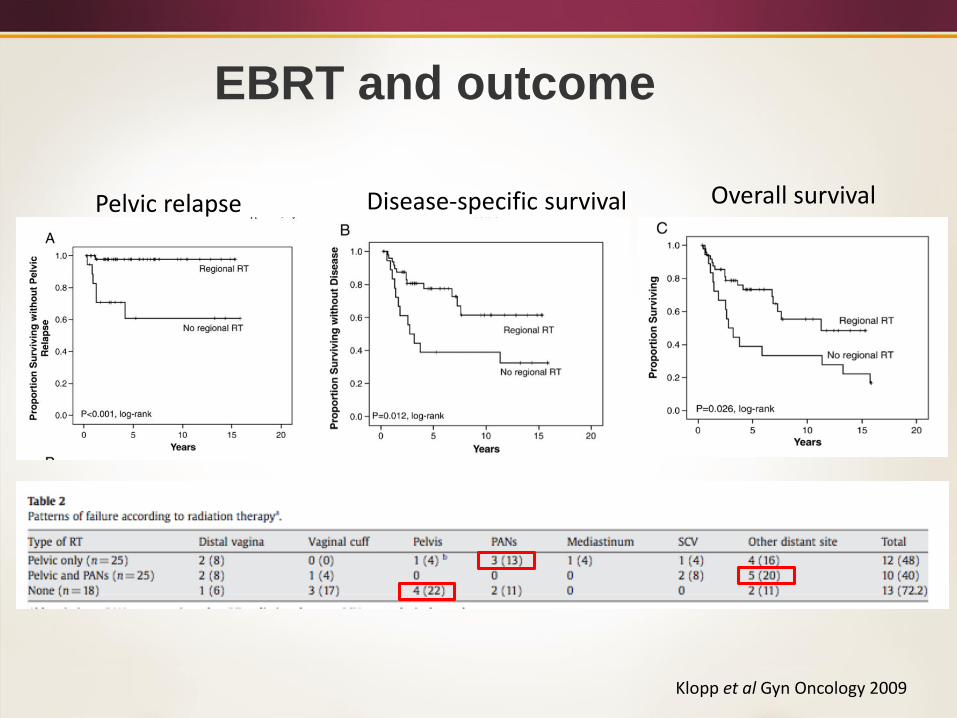
EBRT and outcome
Pelvic relapse Disease-specific survival Overall survival
Klopp et al Gyn Oncology 2009
SEER DATA
Schmid et al (Gyn Onc, 2009) reviewed the
SEER data base from 1988 – 2001
5-year disease specific survival (DSS) with RT
67.9% vs 53.4% without RT (p<0.001).
Single lymph node DSS 74.3 vs. 54.4 %
(p<0.001), 2-5 lymph nodes DSS 59.7 vs. 52.7
% (p=0.089).
SEER DATA
Endometroid 73.7 vs 61.9% (p=0.007)
Clear Cell 77.1 vs. 39.2% (p=0.046)
Papillary Serous 44 vs. 45.5 % (p=0.48)
Sarcoma 44.9 vs 46.3 % (p=0.51)
The data remained significant on multivariate analysis
Pelvic Lymphadenopathy
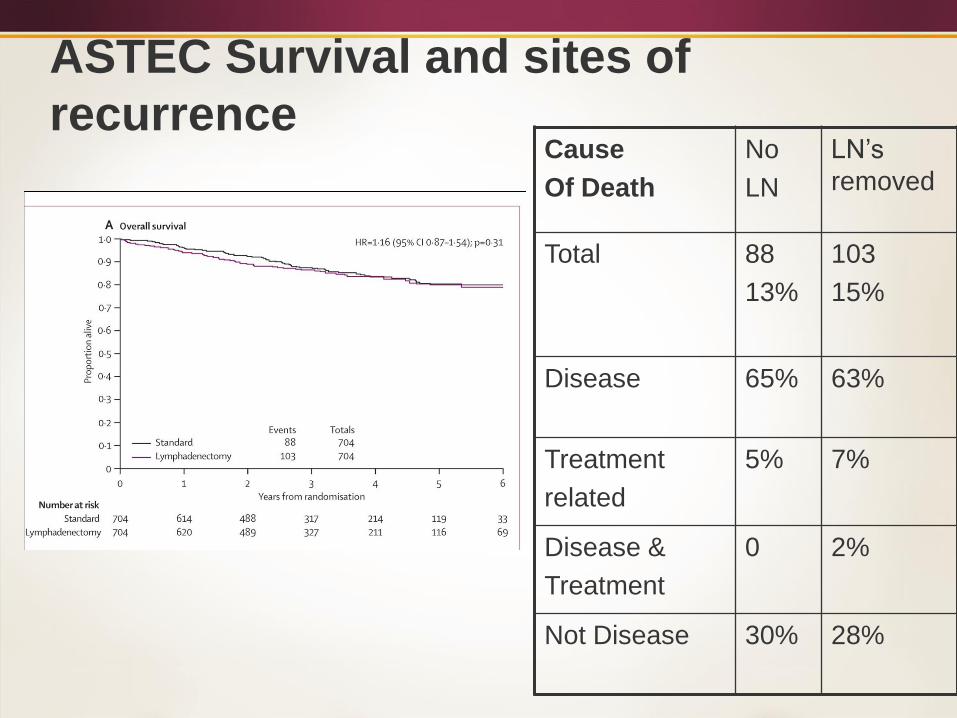
ASTEC Survival and sites of
recurrenceCause
Of Death
No
LN
LN’s
removed
Total 88
13%
103
15%
Disease 65% 63%
Treatment
related
5% 7%
Disease &
Treatment
0 2%
Not Disease 30% 28%
What About Chemotherapy?
Is it the next step to improving
overall survival?
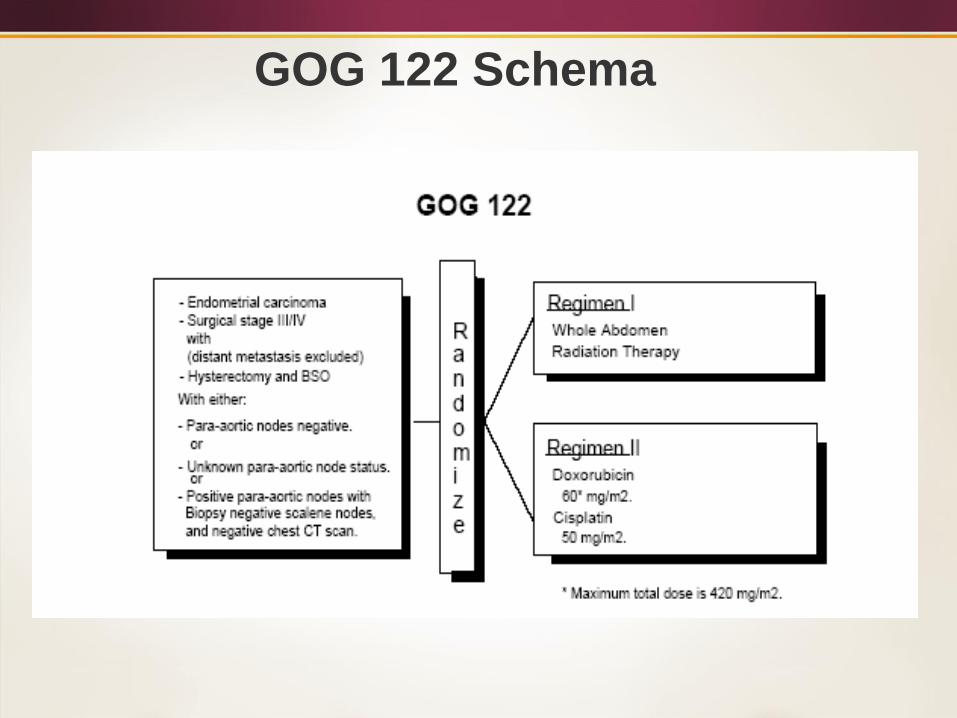
GOG 122 Schema
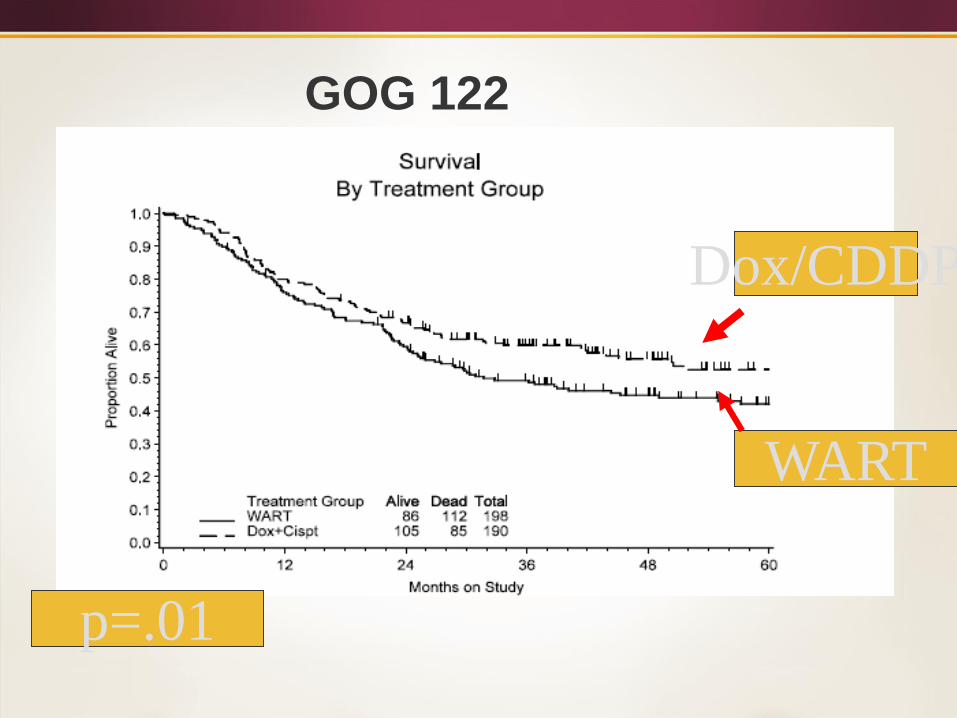
GOG 122
Dox/CDDP
WART
p=.01
Adjuvant chemotherapy versus radiotherapy
in high-risk endometrial carcinoma: result of
a randomised trial
R Maggi et al, BJC,2006;95:266
Stage IC G3
STAGE II G3
>50% MI
Stage III
Regimen 1:
Pelvic RT (45-50 gy)
Regimen 2:
CDDP, Adriamycin, Cytoxan
5 cycles
Adjuvant chemotherapy versus radiotherapy
in high-risk endometrial carcinoma: result of
a randomised trial
Median follow up 95.5 monthsNo difference in 5 Year DFS or OSRT
locoregional initial recurrence: 7 %, Distant: 21 %, Both:5
Chemotherapylocoregional initial recurrence: 11%,
Distant: 16 %, Both:5 %
RT reduced local recurrence, chemotherapy reduced distant failure
R Maggi et al, BJC,2006;95:266
Chemotherapy
Such results suggest that a more
prudent approach would be to combine
chemotherapy and RT
Published trials, however, have reported
mixed results
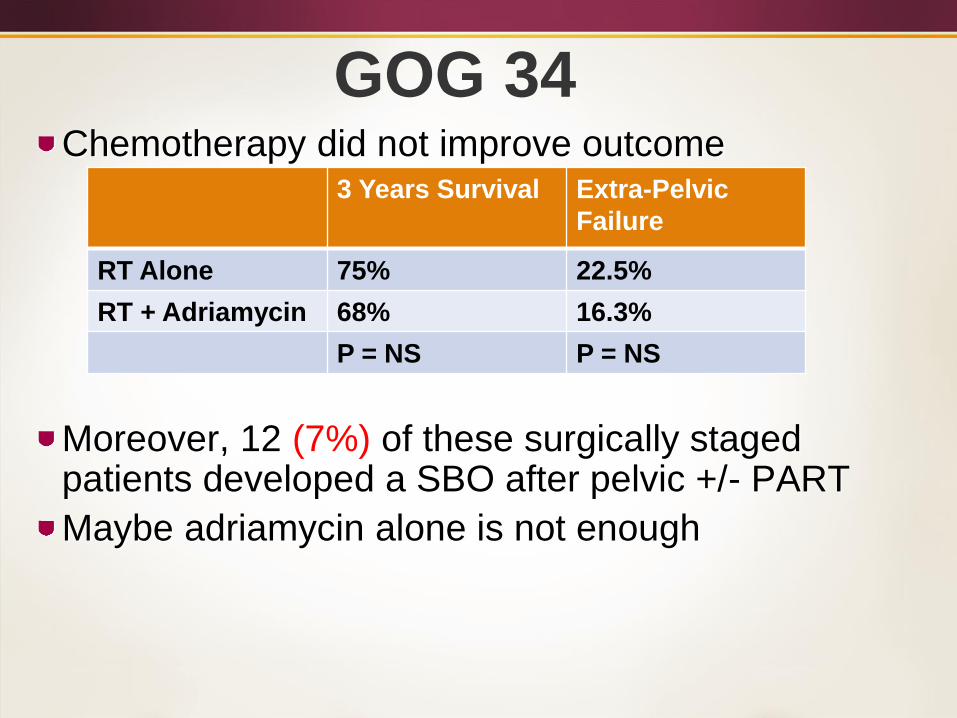
GOG 34Chemotherapy did not improve outcome
Moreover, 12 (7%) of these surgically staged patients developed a SBO after pelvic +/- PART
Maybe adriamycin alone is not enough
3 Years Survival Extra-Pelvic
Failure
RT Alone 75% 22.5%
RT + Adriamycin 68% 16.3%
P = NS P = NS
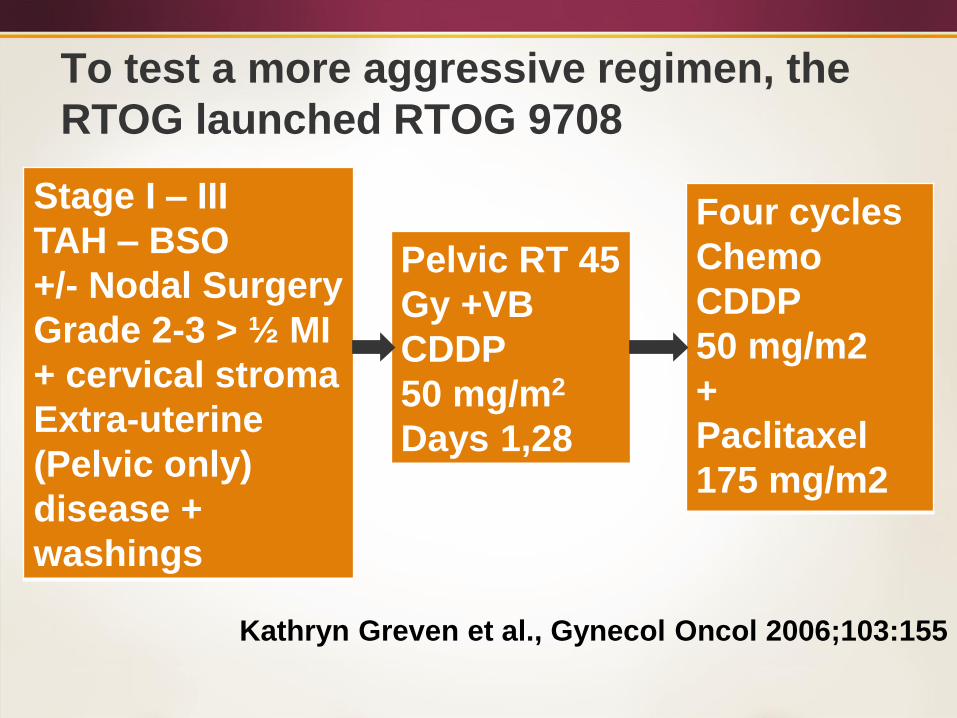
To test a more aggressive regimen, the
RTOG launched RTOG 9708
Kathryn Greven et al., Gynecol Oncol 2006;103:155
Stage I – III
TAH – BSO
+/- Nodal Surgery
Grade 2-3 > ½ MI
+ cervical stroma
Extra-uterine
(Pelvic only)
disease +
washings
Pelvic RT 45
Gy +VB
CDDP
50 mg/m2
Days 1,28
Four cycles
Chemo
CDDP
50 mg/m2
+
Paclitaxel
175 mg/m2
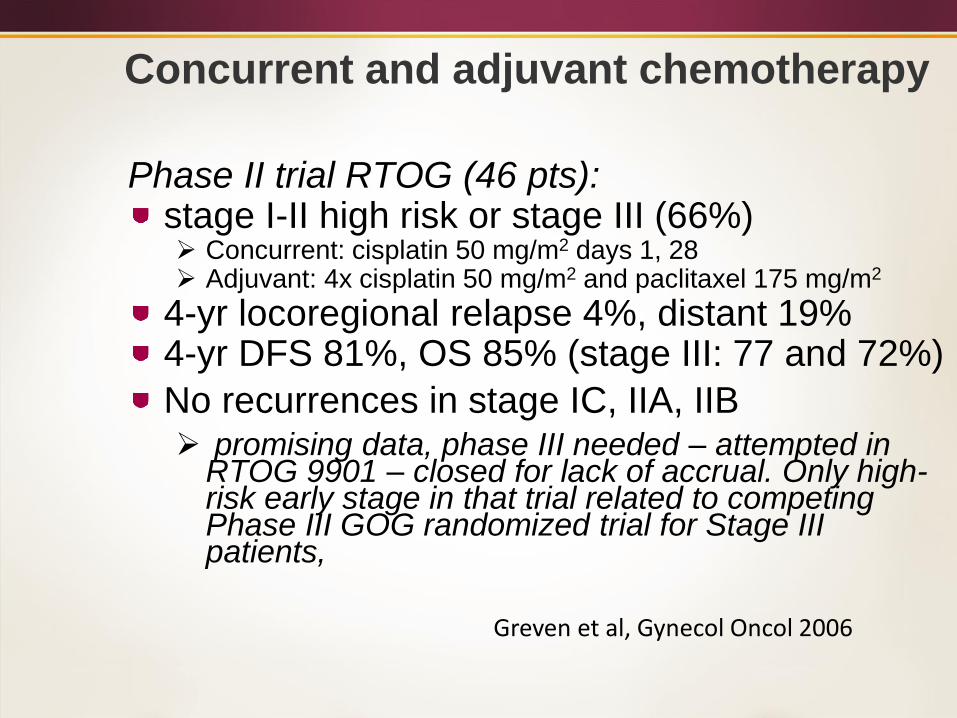
Phase II trial RTOG (46 pts): stage I-II high risk or stage III (66%) Concurrent: cisplatin 50 mg/m2 days 1, 28 Adjuvant: 4x cisplatin 50 mg/m2 and paclitaxel 175 mg/m2
4-yr locoregional relapse 4%, distant 19%4-yr DFS 81%, OS 85% (stage III: 77 and 72%)
No recurrences in stage IC, IIA, IIB promising data, phase III needed – attempted in
RTOG 9901 – closed for lack of accrual. Only high-risk early stage in that trial related to competing Phase III GOG randomized trial for Stage III patients,
Concurrent and adjuvant chemotherapy
Greven et al, Gynecol Oncol 2006
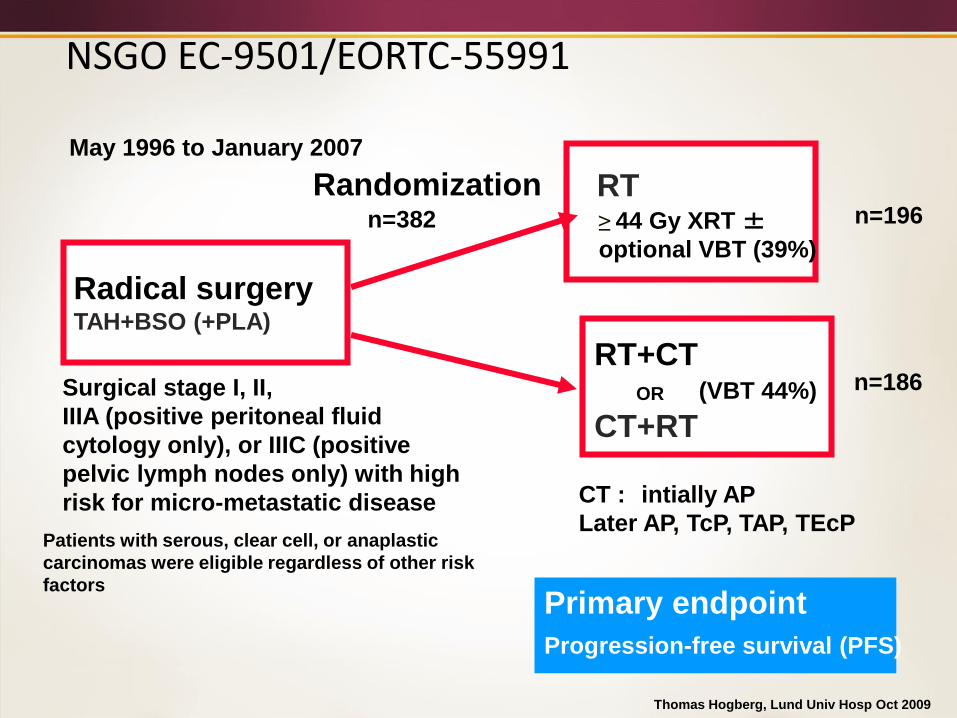
Radical surgeryTAH+BSO (+PLA)
RT+CT
RT
CT+RTOR
Randomization
Primary endpoint
Progression-free survival (PFS)
Surgical stage I, II,
IIIA (positive peritoneal fluid
cytology only), or IIIC (positive
pelvic lymph nodes only) with high
risk for micro-metastatic disease
Patients with serous, clear cell, or anaplastic
carcinomas were eligible regardless of other risk
factors
≥ 44 Gy XRT ±optional VBT (39%)
CT : intially AP
Later AP, TcP, TAP, TEcP
n=196
n=186
n=382
May 1996 to January 2007
(VBT 44%)
NSGO EC-9501/EORTC-55991
Thomas Hogberg, Lund Univ Hosp Oct 2009
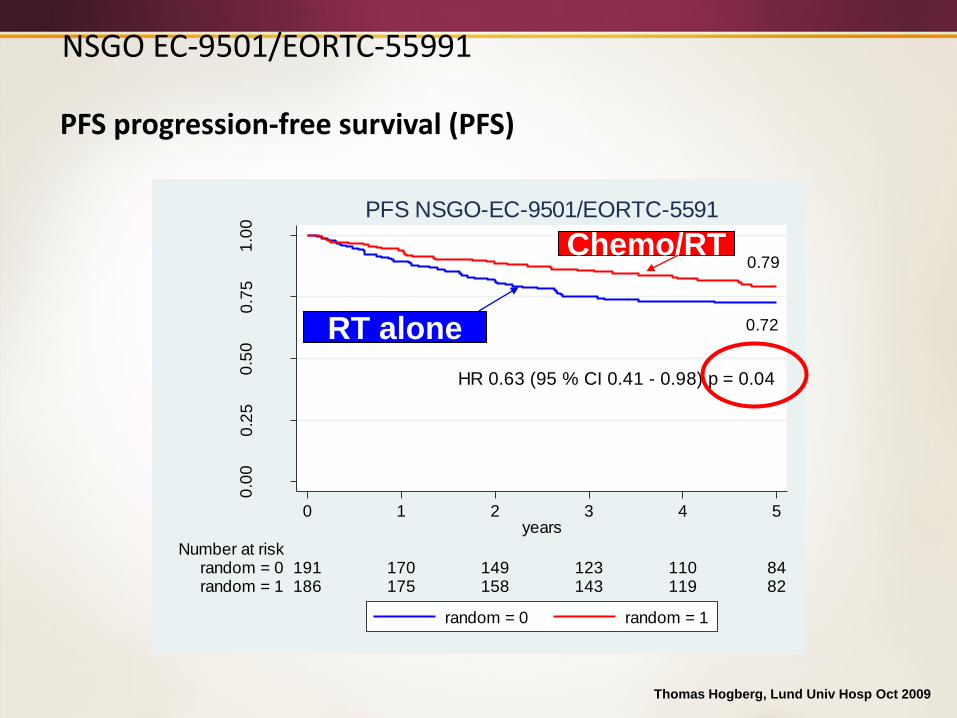
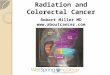
NSGO EC-9501/EORTC-55991
PFS progression-free survival (PFS)
Thomas Hogberg, Lund Univ Hosp Oct 2009
HR 0.63 (95 % CI 0.41 - 0.98) p = 0.04
0.72
0.790
.00
0.2
50
.50
0.7
51
.00
pro
ba
bili
ty o
f su
rviv
al
186 175 158 143 119 82random = 1191 170 149 123 110 84random = 0
Number at risk
0 1 2 3 4 5years
random = 0 random = 1
PFS NSGO-EC-9501/EORTC-5591
RT alone
Chemo/RT
NSGO EC-9501/EORTC-55991
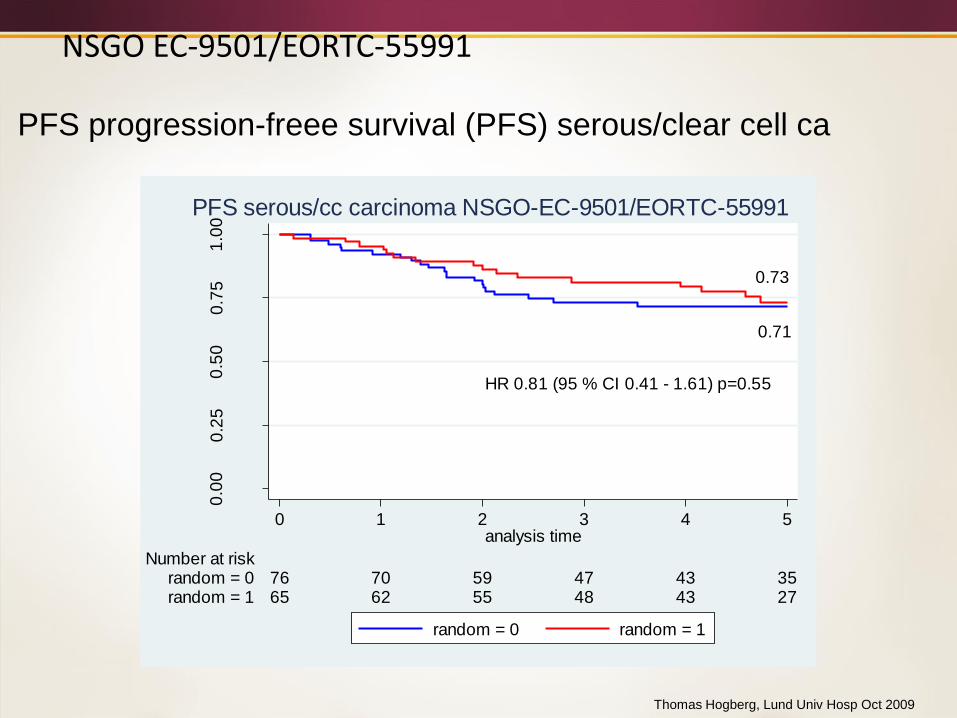
PFS progression-freee survival (PFS) serous/clear cell ca
Thomas Hogberg, Lund Univ Hosp Oct 2009
HR 0.81 (95 % CI 0.41 - 1.61) p=0.55
0.73
0.71
0.0
00
.25
0.5
00
.75
1.0
0
65 62 55 48 43 27random = 176 70 59 47 43 35random = 0
Number at risk
0 1 2 3 4 5analysis time
random = 0 random = 1
PFS serous/cc carcinoma NSGO-EC-9501/EORTC-55991
Combined Modality TrialsSeveral new combined modality trials are underway or in theplanning stages
PORTEC-3 comparing pelvic RT versus pelvic RT +chemotherapy in high risk pts
GOG 258 compares chemotherapy alone versuschemotherapy plus volume directed RT in advanced stagepatients.
GOG 258:Phase III Randomized Study of Adjuvant
Chemoradiotherapy Comprising Cisplatin and Tumor
Volume-Directed Radiotherapy Followed by
Carboplatin and Paclitaxel Versus Carboplatin and
Paclitaxel Alone in Patients With Stage III or IVA
Endometrial Carcinoma
Objective:Compare the recurrence-free survival of
patients with stage III or IVA endometrial carcinoma
treated with adjuvant chemoradiotherapy
comprising cisplatin and tumor volume-directed
radiotherapy followed by carboplatin and paclitaxel
vs carboplatin and paclitaxel alone.
GOG 258 Submitted to ASCO 2017 as
a late breaking abstract!
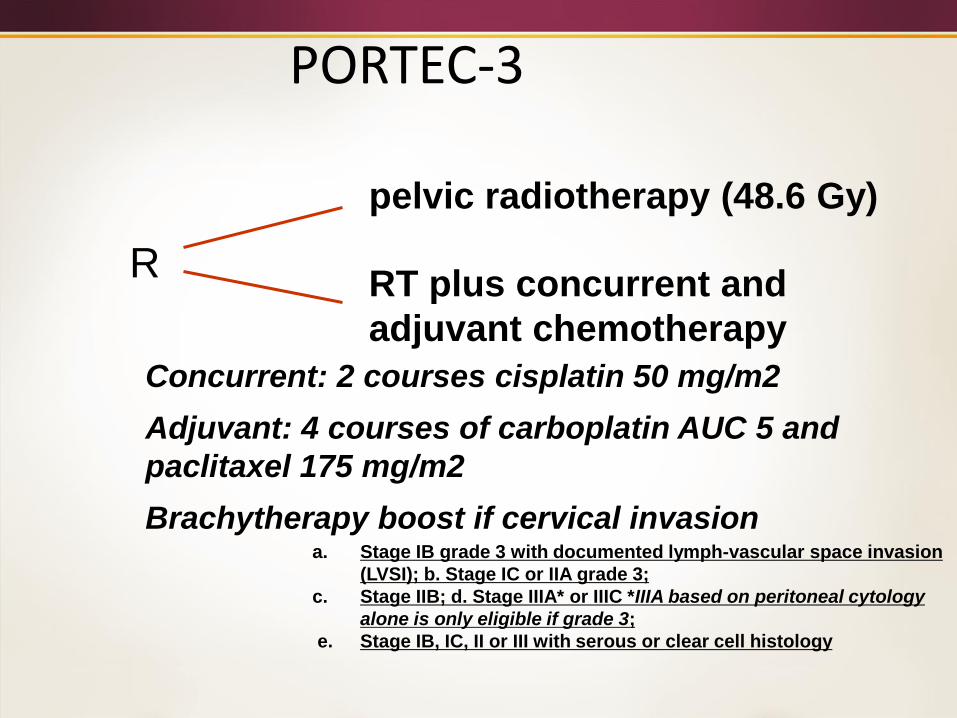
R
pelvic radiotherapy (48.6 Gy)
RT plus concurrent and
adjuvant chemotherapy
PORTEC-3
Concurrent: 2 courses cisplatin 50 mg/m2
Adjuvant: 4 courses of carboplatin AUC 5 and
paclitaxel 175 mg/m2
Brachytherapy boost if cervical invasiona. Stage IB grade 3 with documented lymph-vascular space invasion
(LVSI); b. Stage IC or IIA grade 3;
c. Stage IIB; d. Stage IIIA* or IIIC *IIIA based on peritoneal cytology
alone is only eligible if grade 3;
e. Stage IB, IC, II or III with serous or clear cell histology
Medically Inoperable Endometrial
Cancer
Schwartz, J., Beriwal, S., Esthappan, J, Erickson, B., Feltmate, C.,
Fyles, A., Gaffney, D., Jones, E., Klopp, A., Small, Jr., W.,
Thomadsen, B., Yashar, C., Viswanathan, A., Consensus
statement for brachytherapy for the treatment of medically
inoperable entometrial cancer, Brachytherapy, Sept-Oct 2015;
14(5): 587-599.
Conclusions
RT continues to play an important role in endometrial
cancer
Its optimal role is still evolving
Attention turning to combined modality approaches in
high risk patients following surgery
Recommended