Journal of the International Society of Head and Neck Trauma (ISHANT)
Poster presentations
Received July 2016. Accepted following peer review August 2016. Published August 2016
JISHANT 2016:4
To view full size, click here
Emergency management for Orbital Compartment Syndrome – How important
is decompression?
P152
Priyanka Patel, Atheer Ujam, Mike Perry
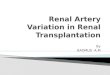
Clinically evident proptosis and periorbital swelling
Orbital compartment syndrome. Axial and sagittal CT imaging confirmed a true proptosis with the left optic nerve on stretch, the so called “balloon on a string” appearance. This was secondary to oedema and a small amount of blood (arrows).
Abstract Current guidelines in the urgent management of orbital compartment syndrome (OCS) includes immediate lateral canthotomy and cantholysis, followed by open surgical
decompression. Medical treatment is also advocated to ‘buy time’ while preparing the patient for theatre. This consists of high dose steroids, mannitol and Acetazolamide diuretics to reduce swelling and orbital pressures.
It is generally recognised that late or delayed intervention is associated with poor outcomes, including blindness. With early presentation, given the potential risk to sight, there is generally a low threshold for treating suspected cases. However, whether or not to treat late cases is more controversial, partly because clinicians could face accusations of medical
negligence if they do nothing. We present a case of a patient who sustained orbital trauma to his only seeing eye, which resulted in acute proptosis and loss of vision. He received no treatment at all for what
appeared to be an orbital compartment syndrome secondary to retrobulbar haemorrhage, but surprisingly made a full recovery of vision within 48 hours. In contrast to the current literature, this case would appear to cast some doubt over the understanding of the role of OCS / RBH in the aetiology of blindness.
Case report
Mr S, a 76 year old gentleman, presented to A+E following a fall at home. He was referred to the maxillofacial team 4 hours later (approximately 5 hours after his injury), when an ED doctor noticed he was blind in his left eye and his CT head showed a bleed into the left orbit with an associated proptosis. Medical history: •Pre existing blindness in the opposite eye •Chronic renal failure requiring twice weekly renal dialysis. •Anuria related to his poor renal function •History of peptic ulcers The following features were noted: 1.Acute tense and painful proptosis of the left eye, with a “stoney hard” feel to the globe. 2.Fixed dilated left pupil 3.Blindness in left eye - no perception to light 4.Ophthalmoplegia 5.Pre-existing blindness to the right eye
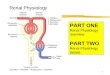
Management
option
Contraindication
Diuretics Renal failure requiring weekly dialysis
High dose steroids GI bleed risk due to peptic ulcer disease
Decompression under GA
Age, comorbidities, total loss of vision and time delay
Lateral canthotomy and cantholysis
Refused by patient in view of comorbidities
Progress following injury
Injury Day -Complete loss of vision -Fixed and dilate pupil -Opthalmoplegia -Proptosis
Post-injury Day 1 -Signs of light perception left eye
Post-injury Day 2 -Return of full vision to left eye assessed by Snellen Chart
Post-injury 1 week: -Opthalmoplegia and proptosis resolving
Post-injury 6 months: - Continued normal vision with no relapse
Discussion
What confounds this topic is the role of other pathological processes in the traumatised orbit. Specifically, do cases of suspected OCS following trauma have an element of traumatic optic neuropathy (TON) which contributes to the visual loss ? High energy impacts to the upper face are well known to result in varying degrees of traumatic optic neuropathy so such an association is possible. This in itself can cause confusion in establishing the precise pathophysiology of impaired vision in the proptosed eye. Surgery in such cases may therefore fail to restore vision and high dose steroids have variable outcomes. The benefits of high dose steroids in TON are controversial . This was a totally unexpected series of events with an outcome that seemed to contradict the perceived current wisdom in management of retrobulbar haemorrhage. It can be argued that there is nothing to lose by performing a lateral canthotomy and cantholysis under local anaesthesia, but this technique is variably described in the literature and requires experience. In some cases formal decompression is necessary but can only be performed by orbital exploration under a general anaesthetic. In patients with complex medical histories, placing them at risk category for general anaesthetic, it is prudent to carefully consent the patients of the risks and benefits of surgery. In particular it seems that the evidence from the literature confirms that intervention after several hours of injury is usually associated with no change to the outcome and that patients will not recover sight in the affected eye. What we can add to this data is that it appears that in some cases spontaneous recovery may be possible.
Recommended