Emergency Department Utilization: Emergency Department Utilization: Facts and MythsFacts and Myths
Lynne D. Richardson, M.D., F.A.C.E.P.Lynne D. Richardson, M.D., F.A.C.E.P.Vice Chair and Associate Professor
Department of Emergency Medicine
Mount Sinai School of Medicine
August 26, 2009

THE FACTSTHE FACTS
Emergency Department Utilization – Who?– Why?
Emergency Department Crowding– What?– Why?

MYTH #1:MYTH #1:
“Increasing penetration of managed care will decrease the use of emergency departments.”

Annual U.S. ED Visits & EDsAnnual U.S. ED Visits & EDs 1995 – 2006 1995 – 2006 (NHAMCS)(NHAMCS)
2006

The Emergency Department:The Emergency Department:A Unique Care ProviderA Unique Care Provider
Immediate care available
24 hours/day; 7 days/week Complex life-saving interventions – simple
first aid access, regardless of ability to pay,
mandated by federal law (EMTALA) only available access to care for many
vulnerable and disenfranchised individuals

The Emergency DepartmentThe Emergency DepartmentThe Ultimate “Safety Net” ProviderThe Ultimate “Safety Net” Provider
ED disproportionately used by: patients without insurance patients with Medicaid patients without primary care physicians members of racial and ethnic minorities other “vulnerable populations”

MYTH #2MYTH #2
“Emergency departments are used mainly by patients who have nowhere else to go: uninsured, illegal immigrants, homeless, etc, etc.”

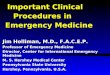
ED Visit Rates by Payment SourceED Visit Rates by Payment Source (NHAMCS 2006)(NHAMCS 2006)

ED Visits by Payment SourceED Visits by Payment Source (NHAMCS 2006)(NHAMCS 2006)
2367230351
47284
20777
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
50,000
Medicare Medicaid Private Uninsured

U.S. Hospital Admissions by RouteU.S. Hospital Admissions by Route (NHAMCS 1996, 2006)(NHAMCS 1996, 2006)

U.S. ED Visit Rates by patient age, U.S. ED Visit Rates by patient age, race & ethnicity: 2005 race & ethnicity: 2005 (NHAMCS)(NHAMCS)

MYTH #3MYTH #3
“There is frequent misuse or inappropriate use of the ED for non-urgent problems”

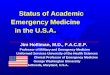
ED Patient Acuity ED Patient Acuity ((NHAMCS 2006)
5%
13%
12%
22%37%
11%
< 1 minute
1-15 minutes
15-60 minutes
1 - 2 hours
>2 hours
Unknown

EMPATH: EMPATH: Emergency Medicine Emergency Medicine Patients’ Access to HealthcarePatients’ Access to Healthcare
Principal Reasons for Coming to the ED Medical Necessity ED Preference Convenience Affordability Limitations of Insurance
Ragin et al, Acad Emerg Med 2005

EMPATH Study: ConclusionsEMPATH Study: Conclusions
Use of the ED is driven by: comprehensive scope of services Immediate availability of services quality of care provided lack of affordable alternatives

Emergency Department CROWDING
Definitions & Measures Causes of Crowding Impact on patient
outcomes Short term strategies Long term solutions

ED Crowding: Asplin’s ModelED Crowding: Asplin’s Model

ED Crowding: “Upstream” ED Crowding: “Upstream” (INPUT)(INPUT) Issues Issues
Inadequate primary care capacity Insufficient “walk in” & off hours
availability of PCPs Increasing number of uninsured Declining Medicaid enrollment Declining coverage for immigrants Less funding for uncompensated care

ED Crowding: ED Crowding: THROUGHPUTTHROUGHPUT issues issues
Increasing acuity Increasing volume Staff shortages: particularly nurses Operational inefficiencies:
– Registration– Laboratory– Radiology– Consults

ED Crowding: OUTPUT IssuesED Crowding: OUTPUT Issues
Boarding of admitted patients Decreasing hospital bed capacity Institutional / organizational culture Declining reimbursement Shrinking hospital profit marginsDecreased primary care capacityInsufficient access to specialty care

ED Boarding of Admitted PatientsED Boarding of Admitted Patients
Often cited as #1 cause of ED Crowding* 62.5% hospitals board admitted patients**
– 14.9% “board” on inpatient units– 35.6% observation/clinical decision unit– 35.2% electronic dashboard– 21.1% full capacity protocol
19.5 % expanded ED within past 2 years 31.5% have ED expansion plans
*GAO Report; ACEP Task Force; **NHAMCS 2007 E-Stat

Adverse Impact on OutcomesAdverse Impact on Outcomes
Increased waiting times Increases in leaving without treatment
or AMA Increased risk of in-hospital mortality Increased time to antibiotics for
pneumonia Reduced promptness & quality of pain
management

“ “ Knowing is not enough, we must apply.Knowing is not enough, we must apply.Willing is not enough, we must do.”Willing is not enough, we must do.”
Goethe


RWJF Urgent Matters ProgramRWJF Urgent Matters Program
National program to develop solutions to ED Crowding
Elmhurst Hospital one of ten sites Results released May/June 2004
summary available at http://www.urgentmatters.org

Institute of Medicine Report on Institute of Medicine Report on Future of Emergency Care in the United States
Key Findings & Recommendations– released June 2006
Hospital-Based ED Care Emergency Care for Children Pre-hospital Emergency Care

IOM Future of Emergency Care IOM Future of Emergency Care RecommendationsRecommendations
Improve hospital efficiency & patient flow A coordinated, regionalized, accountable
EMS system Increased reimbursement Increased resources for research &
disaster preparedness Focused attention to care of children

Williams, R. NEJM, 1996.– ED: High fixed costs; low marginal costs
– True costs of non-urgent care in the ED are relatively low
Tyrance, P. AJPH, 1996– Only 12% of “ED spending” by uninsured
– ED expenditures only 1.9% of US health costs
– Decreasing ED use will not generate much overall US health cost savings
Cost of Care in the EDCost of Care in the ED
Recommended