REVIEW
Disease management
Drug therapy in cardiac arrest: a reviewof the literatureAndreas Lundin1*, Therese Djarv2, Johan Engdahl3, Jacob Hollenberg4,Per Nordberg4, Annika Ravn-Fischer5, Mattias Ringh4, Susanne Rysz6,Leif Svensson4, Johan Herlitz7,8, and Peter Lundgren5
1Department of Anaesthesia and Intensive Care, Sahlgrenska Universitetssjukhuset, Per Dubbsgatan 15, Gothenburg 41345, Sweden; 2Department of Medicine, Karolinska Institutet,Solna, Sweden; 3Department of Medicine, Halland Hospital, Halmstad, Sweden; 4Department of Cardiology, Center for Resuscitation Science, Karolinska Institutet, Solna, Sweden;5Department of Cardiology, Sahlgrenska University Hospital, Gothenburg, Sweden; 6Department of Anesthesiology, Surgical Services and Intensive Care Medicine, KarolinskaInstitutet, Solna, Sweden; 7The Prehospital Research Centre for Western Sweden, PreHospen, University of Boras, Boras, Sweden; and 8Deparment of Clinical and Molecular Medicine/Cardiology, Sahlgrenska University Hospital, Goteborg, Sweden
Received 15 September 2015; revised 27 October 2015; accepted 28 October 2015; online publish-ahead-of-print 26 November 2015
The aim of this study was to review the literature on human studies of drug therapy in cardiac arrest during the last 25 years. In May 2015, asystematic literature search was performed in PubMed, Embase, the Cochrane Library, and CRD databases. Prospective interventional andobservational studies evaluating a specified drug therapy in human cardiac arrest reporting a clinical endpoint [i.e. return of spontaneous cir-culation (ROSC) or survival] and published in English 1990 or later were included, whereas animal studies, case series and reports, studies ofdrug administration, drug pharmacology, non-specified drug therapies, preventive drug therapy, drug administration after ROSC, studies withprimarily physiological endpoints, and studies of traumatic cardiac arrest were excluded. The literature search identified a total of 8936 articles.Eighty-eight articles met our inclusion criteria and were included in the review. We identified no human study in which drug therapy, comparedwith placebo, improved long-term survival. Regarding adrenaline and amiodarone, the drugs currently recommended in cardiac arrest, twoprospective randomized placebo-controlled trials, were identified for adrenaline, and one for amiodarone, but they were all underpoweredto detect differences in survival to hospital discharge. Of all reviewed studies, only one recent prospective study demonstrated improvedneurological outcome with one therapy over another using a combination of vasopressin, steroids, and adrenaline as the intervention comparedwith standard adrenaline administration. The evidence base for drug therapy in cardiac arrest is scarce. However, many human studies on drugtherapy in cardiac arrest have not been powered to identify differences in important clinical outcomes such as survival to hospital discharge andfavourable neurological outcome. Efforts are needed to initiate large multicentre prospective randomized clinical trials to evaluate both cur-rently recommended and future drug therapies.- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Drug therapy † Cardiac arrest
IntroductionIn clinical terms, cardiac arrest is defined as a sudden and sustainedloss of consciousness with pulselessness and apnoea or agonalbreathing.1 It is a heterogeneous condition in terms of underlyingpathology, initial rhythm, time in no flow, and concurrent health is-sues. The pathophysiology of cardiac arrest is mainly attributed toeither cardiac, metabolic, or mechanical causes.1 Rhythm at initialpresentation is the most important prognostic factor,2 dictates theimmediate treatment,3 and is affected by underlying pathology, timefrom collapse to rhythm recording, and bystander cardiopulmonary
resuscitation (CPR).4 In the majority of patients with out-of-hospital cardiac arrest (OHCA), primary cardiac pathology is theunderlying cause of the arrest and one-third present with a shock-able rhythm,5 increasing to two-thirds when time from collapse toresuscitation is within a few minutes.6 In patients with in-hospitalcardiac arrest (IHCA), the proportion of primary cardiac path-ology is lower and patients more frequently present with pulselesselectrical activity (PEA) as the initial rhythm,7 indicating differencesin patient characteristics and underlying pathology. In both groups,asystole is common when the time from collapse to resuscitation isprolonged.5,7
* Corresponding author. Tel: +46 73 5064648, Fax: +46 73 5064648, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2015. For permissions please email: [email protected]
European Heart Journal – Cardiovascular Pharmacotherapy (2016) 2, 54–75doi:10.1093/ehjcvp/pvv047
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

The pathophysiology of cardiac arrest of primary cardiac causehas been described by Weisfeldt and Becker8 as a time-sensitivethree-phase model. The first 4–5 min constitute the electrical phaseand with immediate defibrillation, survival is .50%.9 – 11 However,recurrent or shock-resistant ventricular fibrillation occurs in 10–25% of all OHCA12 and anti-arrhythmic drugs are often adminis-tered when defibrillation fails. Anti-arrhythmics possibly reducethe likelihood of arrhythmia being maintained or recurring afterthe return of spontaneous circulation (ROSC).13– 15 The effects ofanti-arrhythmic drugs on the defibrillation threshold are, however,inconsistent and most anti-arrhythmics also have pro-arrhythmiceffects.16,17
The circulatory phase follows after 4–5 min, when tissue hypoxiaand the accumulation of metabolites reduce the likelihood of suc-cessful defibrillation. Restoration of coronary perfusion pressure(CPP) is imperative. Animal studies have demonstrated an associ-ation with a CPP of .20–40 mmHg during resuscitation andROSC, and also an increased likelihood of conversion to PEA orasystole with defibrillation if adequate CPP is not established.18– 22
One human study demonstrated a positive correlation with initialand maximum CPP and ROSC during resuscitation, and initial CPPwas a stronger predictor of subsequent ROSC than no-flow time.23
Haemodynamic improvement during the circulatory phase providesthe rationale for vasopressor treatment during resuscitation.
In the metabolic phase (i.e. .10–15 min), survival is dismal due toglobal ischaemia and reperfusion injury, and the beneficial effects ofcirculatory supportive measures are diminished.24,25 In a survivalmodel of OHCA patients, Valenzuela et al.26 found that delayingCPR for .10 min rendered defibrillation ineffectual in terms of sur-vival. Moreover, the benefit of immediate CPR declined if defibrilla-tion was delayed for .10 min. If a large proportion of patients withprolonged circulatory arrest are included in trials of cardiac arrest,proving benefit will be difficult, as survival is dismal regardless oftreatment.
The early initiation of CPR and defibrillation has been shown toincrease survival in cardiac arrest and is well established in treatmentalgorithms.27,28 From a theoretical point of view, several drug ther-apies are appealing, but supporting clinical data in human studies areless robust.29– 31 To summarize the evidence base for drug therapyin cardiac arrest, we decided to review the literature on humanstudies of drug therapy in cardiac arrest during the last 25 years.
MethodsIn May 2015, a literature search was performed in PubMed, Embase, theCochrane Library, and CRD databases. The search terms used, in differ-ent combinations, were ‘Cardiac arrest’, ‘Heart arrest’, ‘Circulatory ar-rest’, ‘Cardiopulmonary arrest’, ‘Drug’, ‘Drugs’, ‘Drug therapy’,‘Medication’, ‘Medications’, ‘Pharmacology’, ‘Pharmaceutical’, ‘Pharma-ceutical preparations’, and ‘Cardiovascular agents’. We included articleswritten in English from 1990 and onwards. Eligible articles were pro-spective interventional studies and observational studies evaluating aspecified drug therapy during the resuscitation phase of human cardiacarrest, reporting a clinical endpoint (i.e. ROSC or survival). We ex-cluded animal studies, case series and case reports, studies of drug ad-ministration, studies of drug pharmacology, studies of non-specifieddrug therapies, studies with primarily physiological endpoints, studies
of preventive drug therapy, studies of traumatic cardiac arrest, andstudies of drug administration after ROSC.
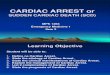
ResultsThe literature search identified a total of 8936 articles (after the re-moval of duplicates). After screening of titles and abstracts by two ofthe authors (A.L. and P.L.), 769 were considered to be potentiallyrelevant for research on drug therapy in cardiac arrest. Of these,681 were excluded, whereas 88 articles met our inclusion criteriaand were included in the review (Figure 1). Reasons for exclusionwere case series (n ¼ 45), review article (n ¼ 326), study of drug ad-ministration or pharmacology (n ¼ 11), study with physiologicaloutcome (n ¼ 18), animal studies (n ¼ 263), and preventive orpost-resuscitative intervention (n ¼ 18). Of 88 included studies,40 were classified as observational studies and 48 as interventionalstudies. Sixty-three studies enrolled patients with OHCA, 16 studiesenrolled patients with IHCA, and 9 studies enrolled both. The in-cluded studies comprised 17 different drugs such as adrenaline(n ¼ 33), vasopressin (n ¼ 14), methoxamine (n ¼ 1), iso-proterenol (n ¼ 1), amiodarone (n ¼ 7, two studies presented in ni-fekalant section), lidocaine (n ¼ 6, three studies presented inlidocaine and nifekalant section), sotalol (n ¼ 1, presented in lido-caine section), procainamide (n ¼ 2), atropine (n ¼ 1), aminophyl-line (n ¼ 3), nifekalant (n ¼ 4), beta-blockers (n ¼ 1), magnesium(n ¼ 5), thrombolytics (n ¼ 6), corticosteroids (n ¼ 1), sodium bi-carbonate (n ¼ 3), erythropoietin (n ¼ 1), and crystalloid and col-loids (n ¼ 2). Of the interventional studies, the median and meanstudy size were 199 and 442 patients (range 30–3327 patients), re-spectively. Of the interventional studies, 38 reported time from col-lapse to study drug administration (or a proximate surrogate), withan average time interval of 16 min (range 1–43 min). Most interven-tional studies allowed only intravenous drug administration, al-though a few allowed intraosseous or endotracheal administrationif intravenous access could not be established. Details of studiesare summarized in Tables 1 and 2.
Vasopressor drugs
AdrenalineAdrenaline is an a- and b-adrenergic agonist and its cardiovasculareffects include venous and arterial vasoconstriction, increased ino-tropy, and chronotropy.32 Studies of adrenaline in animal models ofcardiac arrest have demonstrated increased diastolic blood pressureand CPP,20,33,34 but also pulmonary vasoconstriction,35 increasedmyocardial oxygen demand, and myocardial oxygen imbalance36
as well as cerebral vasoconstriction and diminished cerebral bloodflow.37 Clinical effects from adrenaline in animal studies include anincreased rate of ROSC and short-term survival,22,38 but also post-resuscitative myocardial dysfunction,39 cerebral ischaemia,40 andpoor neurological outcome as well as decreased short-term sur-vival.41 Less myocardial dysfunction has been demonstrated withpure a-agonists38 and with adrenaline plus b-adrenergic antago-nists.42,43 Both beneficial and harmful effects of adrenaline wereaugmented with higher doses.44–46 The electrophysiological effectsof adrenaline are complex, and animal studies have demonstrated
Drug therapy in cardiac arrest 55
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

increased myocardial instability47,48 as well as beneficial electro-physiological effects.49 In humans, adrenaline has been associatedwith more rhythm transitions to ventricular arrhythmias afterROSC.50
We found 33 studies51– 83 evaluating adrenaline administration inhuman cardiac arrest. Fifteen were interventional and 18 were ob-servational studies. Thirteen interventional studies compared high-dose adrenaline (i.e. .0.02 mg/kg) with a standard dose (i.e. 0.01–0.02 mg/kg).51 – 63 Although four of these reported higher rates ofROSC,53 – 56 only one small study of paediatric patients found in-creased survival to hospital discharge with a higher dose of adren-aline.53 In the largest study, Gueugniaud et al. randomized 3327adult patients with OHCA to 5 or 1 mg of adrenaline. The higherdose increased the rate of ROSC (40.4 vs. 36.4%, P ¼ 0.02), but sur-vival to hospital discharge was not statistically different.56 Further-more, two other large multicentre trials did not demonstrate anysignificant benefit from higher dosages.51,55
We found two studies that compared adrenaline with pla-cebo.64,65 Woodhouse et al. randomized 194 patients to high-dose
adrenaline (10 mg) or placebo. There were more rhythm transitionsin the adrenaline group but no difference in survival. The results aredifficult to interpret, as there were major imbalances in baselinecharacteristics between groups.64 Jacobs et al. randomized 500OHCA patients to standard treatment with adrenaline (1 mg) vs. sa-line placebo. The adrenaline group had a higher rate of ROSC (23.5vs. 8.4%, P , 0.001), but there was no significant difference in sur-vival to hospital discharge. The trial was underpowered, as the en-rolment of 5000 patients was planned to detect a 2% absolutedifference in survival to hospital discharge, from a baseline survivalrate of 5%.65
Of 18 observational studies,66 – 83 8 retrospectively comparedoutcome in patients with cardiac arrest depending on whether ornot adrenaline was administered.71,73,74,77,78,80,82 Three studiesfound no difference in survival,69,74,78 while three reported reducedsurvival associated with adrenaline administration71,73,82 and two re-ported increased survival.75,77 Three of the studies used data fromthe same national registry in Japan, with inconsistent findings.73,77,80
Hagihara et al.73 found that adrenaline was associated with increased
Figure 1 PRISMA 2009 flow diagram.
A. Lundin et al.56
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

ROSC, but reduced overall and neurologically intact survival at1 month. In contrast, Nakahara et al.,80 using the same registry, re-ported increased 1-month survival in patients receiving adrenalinebut no difference in neurologically intact survival. Both studiesused propensity scoring to adjust for confounders, but Nakaharaet al. used time-dependent statistics which, according to the authors,could explain the different findings. Recently, Dumas et al.,82 usingvarious statistical methodologies, reported a significantly poorerneurological outcome in resuscitated OHCA patients who receivedadrenaline. This association was observed, regardless of length of re-suscitation, and there was an inverse linear relationship between to-tal dose (i.e. dose effect), as well as the timing of first dose, andneurological outcome.
Five studies looked at the association between the timing ofadrenaline administration and survival.75,76,79,81,83 Three reportedan association between the earlier administration of adrenalineand ROSC or survival,75,76,81 whereas one small study was unableto find any association.79 One recent retrospective study of 20000 patients with IHCA found a correlation between increasing dos-age intervals of adrenaline and survival to hospital discharge.83 Com-pared with a dosage period of 4–5 min, the adjusted odds ratio forsurvival to hospital discharge was 2.17 (95% CI: 1.62–2.92) for dos-age intervals of 9–10 min.
Two studies evaluated the association between total adrenalinedose and outcome, and both reported that the cumulative doseof adrenaline is independently associated with poor outcome.70,72
Finally, three small studies reported on survival in adult and paediat-ric patients receiving high-dose or standard-dose adrenaline, withno significant difference in ROSC or survival.66– 68
VasopressinVasopressin is a neurohypophysical hormone84 and its cardiovascu-lar effects include increased inotropy, systemic and coronaryvasoconstriction,85 and the potentiation of catecholaminergic ef-fects.86,87 In animal models of cardiac arrest, vasopressin increaseddiastolic blood pressure and CPP.88– 90 Compared with adrenaline,vasopressin has been associated with less impairment of cerebralblood flow,91 less attenuation from acidosis,92 less tachyphylaxiaand pulmonary vasoconstriction,93 as well as longer effect dur-ation.94 Vasopressin mediates ACTH release and, in animal studiesof cardiac arrest, the levels of ACTH and cortisol were higher afterthe administration of vasopressin compared with adrenaline.86,95
High endogenous vasopressin levels, as well as increased cortisol le-vels, have been associated with improved survival after cardiacarrest.96,97
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Included studies
Study drug Design OHCA/IHCAa
No. ofstudies
Interventional Observational
Randomizedprospective
Non-randomizedprospective
Prospective withhistorical controls
Adrenalineb 13 1 1 18 27/6 33
Vasopressinc 8 2 4 8/6 14
Methoxamine 1 0/1 1
Isoproterenol 1 1/0 1
Amiodaroned 2 3 2/3 5
Lidocainee,f 2 1 3/0 3
Aminophylline 3 3/0 3
Sodium bicarbonate 1 2 2/1 3
Magnesium 4 1 3/2 5
Beta-blocker 1 1/0 1
Thrombolytics 3 1 4 7/1 8
Erythropoietin 1 0 1/0 1
Corticosteroids 1 0 1/0 1
Crystalloids 1 1 2/0 2
Procainamide 2 1/1 2
Atropine 1 0/1 1
Nifekalant 4 3/1 4
48 40 64/23 88
aStudies enrolling both IHCA and OHCA patients are classified as OHCA if the primary setting was emergency department, and if the primary setting was in-hospital (includingemergency department), studies are classified as IHCA.bIn total, 41 studies evaluated adrenaline as an intervention, and 8 are classified in other sections (vasopressin).cIn two studies, intervention included corticosteroids.dIn total, seven studies evaluated amiodarone, and two studies are classified in other sections (nifekalant).eIn total, six studies evaluated lidocaine, and three studies are classified in other sections (nifekalant and amiodarone).fOne study included comparison with sotalol.
Drug therapy in cardiac arrest 57
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Prospective interventional studies of drug therapy in human cardiac arrest
Author (year) Study design Study size Setting Inclusion ofparticipants
Intervention1 Control1 Time to studydrugadministration(min)
Admin. route Primaryoutcome(s)
Results
Adrenaline Goetting et al.(1991)
Prospectiveinterventionvs. historicalcontrolgroup
40 patients Prehospital Paediatric patientsw/ witnessedcardiac arrest,refractory totwo standarddoses ofadrenaline
HDE (0.2 mg/kg) afterfailure of two dosesSDE
SDE (0.01 mg/kg) 4 iv ROSC ROSC: 70 vs. 0%(P , 0.001) andsurvival to discharge40 vs. 0% in theintervention groupand control group,respectively
Lindner et al.(1991)
Prospective,randomizedtrial
68 patients Emergencydepartment
Adult patients w/IHCA orOHCA andasystole orPEA
HDE (5 mg), followed bystandard ACLStreatment
SDE (1 mg) Not stated iv ROSC, survival tohospitaldischarge.
ROSC: 57 vs. 15%(P , 0.01) andsurvival to discharge11 vs. 4% (P ¼ NS) inthe intervention andcontrol groups,respectively
Brown et al.(1992)
Prospective,randomizedtrial
1280 patients Prehospital Adult patients w/OHCA
HDE (0.2 mg/kg), onedose, followed bystandard ACLStreatment
SDE (0.02 mg/kg) 17 iv ROSC ROSC: 22 vs. 23% andsurvival to discharge5 vs. 7% in theintervention andcontrol groups,respectively(P ¼ NS)
Callaham et al.(1992)
Prospective,randomizedtrial
546 patients Prehospital Adult patients w/OHCA
HDE (15 mg), maximumthree doses, followedby standard ACLStreatment
SDE (1 mg) 16 iv ROSC ROSC: 13 vs. 8%(P ¼ 0.01) andsurvival to hospitaldischarge 1.7 vs. 1.2%(P ¼ NS) in theintervention andcontrol groups,respectively
Stiell et al. (1992) Prospective,randomizedtrial
650 patients In hospital Adult patients w/IHCA orOHCA inhospital ortreated in theED
HDE, 7 mg every 5 min upto five doses. followedby standard ACLStreatment
SDE (1 mg), repeateddoses
15 min (OHCApatients), 7 min(IHCApatients)
iv or endotracheal ROSC ROSC: 18 vs. 23% andsurvival to hospitaldischarge 3 vs. 5% inthe intervention andcontrol groups,respectively(P ¼ NS)
Lipman et al.(1993)
Prospective,randomizedtrial
40 patients In hospital Adult ICUpatients w/IHCA andasystole
HDE (10 mg) every 5 min.Maximum threedoses, followed bystandard ACLStreatment
SDE (1 mg), every5 min
Not reported iv Not reported ROSC: 68 vs. 68% and24 h survival 21 vs.31% in theintervention andcontrol groups,respectively(P ¼ NS). Onepatient in the controlgroup survived todischarge
A.Lundin
etal.58
by guest on August 22, 2016 http://ehjcvp.oxfordjournals.org/ Downloaded from

Polglase et al(1994)
Prospective,randomizedtrial
105 patients Prehospital Adult patients w/OHCA
5 mg (30 patients) or10 mg (34 patients)adrenaline, repeateddoses
SDE (1 mg) 41patients, repeateddoses
Not reported iv Not reported ROSC: 14 vs. 20 vs. 20%in 1, 5, and 10 mggroups, respectively(P ¼ NS). No patientsurvived to hospitaldischarge
Choux et al.(1995)
Prospective,randomizedtrial
536 patients Prehospital Adult patients w/OHCA
HDE (5 mg), repeateddoses
SDE (1 mg), repeateddoses
22 iv ROSC, survival tohospitaladmission andsurvival tohospitaldischarge
ROSC: 35.5 vs. 32% andsurvival to hospitaladmission: 24 vs. 20%in the interventionand control groups,respectively(P ¼ NS)
Woodhouse et al.(1995)
Prospective,randomized,placebo-controlledtrial
194 patients Emergencydepartment
Adults patients w/OHCA ofcardiacaetiology
Adrenaline 10 mg Saline placebo Not reported iv Immediate survival(i.e. stablecardiac rhythmw/a palpablepulse)
Immediate survival: 9.7vs. 7% and survival tohospital discharge: 2vs. 0% in theintervention andcontrol groups,respectively(P ¼ NS)
Carvolth et al.(1996)
Prospectiveinterventionvs. historicalcontrolgroup
1174 patients (594patients in thehistoricalcontrol group)
Prehospital Adult patients w/OHCA
HDE: 5, 10, and 15 mgdosing to a total doseof 30 mg
SDE (1 mg) repeateddoses to amaximum of 4 mg
Not reported iv or endotracheal Survival to hospitaladmission,survival todischarge
Survival to hospitaladmission: 15.3 and14.5% and survival tohospital discharge 4.8and 4.9% in theintervention andcontrol groups,respectively(P ¼ NS)
Sherman et al.(1997)
Prospective,randomizedtrial
140 patients Emergencydepartment
Adult patients w/OHCArefractory toSDE
HDE (0.1 mg/kg),repeated every 5 min
SDE (0.01 mg/kg),repeated every5 min
23 (time torandomization)
iv Improvement incardiac rhythmor ROSC
ROSC: 19 vs. 11% in theintervention andcontrol groups,respectively(P ¼ NS), no patientsurvived to hospitaldischarge
Gueugniaud et al.(1998)
Prospective,randomizedtrial
3327 patients Prehospital Adult patients w/OHCA andshock-resistant VF,asystole orPEA
HDE; 5 mg, repeateddosing (maximum 15doses)
SDE; 1 mg, repeateddoses
20 iv or endotracheal ROSC, survival tohospitaladmission anddischarge
ROSC: 40.4 vs. 36.4%(P , 0.05) andsurvival to hospitaldischarge: 2.3 vs.2.8% (P ¼ NS) in theintervention andcontrol groups,respectively
Perondi et al.(2004)
Prospective,randomizedtrial
68 patients In hospital Paediatric patientsw/ IHCArefractory toinitial SDE
HDE (0.1 mg/kg),repeated doses
SDE (0.01 mg/kg) 2 iv 24 h survival ROSC: 44 vs. 24%(P ¼ NS) and 24 hsurvival 3 vs. 21%(P ¼ 0.05) in theintervention andcontrol groups,respectively
Continued
Drug
therapyin
cardiacarrest
59
by guest on August 22, 2016 http://ehjcvp.oxfordjournals.org/ Downloaded from

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Continued
Author (year) Study design Study size Setting Inclusion ofparticipants
Intervention1 Control1 Time to studydrugadministration(min)
Admin. route Primaryoutcome(s)
Results
Patterson et al.(2005)
Prospective,randomizedtrial
230 patients Emergencydepartment
Paediatric patients(,22 years) inED w/ OHCArefractory toprehospitalresuscitation
HDE, 0.1 mg/kg for theinitial dose and 0.2 mg/kg for subsequentdoses
SDE (0.01 mg/kg) Not reported iv or endotracheal Survival todischarge andneurologicaloutcome
Survival to hospitaldischarge: 7 vs. 2% inthe intervention andcontrol groups,respectively(P ¼ NS)
Jacobs et al.(2011)
Prospective,randomized,placebo-controlledtrial
534 patients Prehospital Adult patents w/OHCA
SDE (1 mg), repeateddosing every 3 min
Placebo (0.9% saline) 10 (time to EMSarrival)
iv Survival to hospitaldischarge
ROSC: 23.5 vs. 8.4%(P , 0.05) andsurvival to hospitaldischarge 4.0 and1.9% (P ¼ NS) in theintervention andcontrol groups,respectively
Vasopressin Lindner et al.(1997)
Prospective,randomizedtrial
40 patients Prehospital Adult patients w/OHCA andshock-resistant VF
Vasopressin (40 IU), onedose, followed bystandard ACLStreatment
Standard ACLStreatment.
14 iv Survival to hospitaladmission
Survival to hospitaladmission: 70 vs. 35%(P ¼ 0.06) andsurvival to hospitaldischarge: 40 vs. 15%in the interventionand control groups,respectively(P ¼ NS)
Stiell et al. (2001) Prospective,randomizedtrial
200 patients In hospital Adult patients w/IHCA
Vasopressin (40 mg) onedose, followed bystandard ACLStreatment
Standard ACLStreatment
6 iv Survival to hospitaldischarge
Survival to hospitaldischarge: 12 vs. 14%in the interventionand control groups,respectively(P ¼ NS)
Wenzel et al.(2004)
Prospective,randomizedtrial
1219 patients Prehospital Adult patents w/out-of-hospitalcardiac arrest
Two injections of 40 IU ofvasopressin, followedby additionaltreatment w/adrenaline if needed
Standard ACLStreatment
10 iv Survival to hospitaladmission
ROSC: 25 vs. 28%(P ¼ 0.19) andsurvival to hospitaladmission: 36 vs. 31%(P ¼ 0.06) in theintervention andcontrol groups,respectively
Callaway et al.(2008)
Prospective,randomizedtrial
325 patients Prehospital Adult patients w/OHCA,requiring atleast one doseof adrenaline
Vasopressin (40 IU), onedose, followed bystandard ACLStreatment
One dose salineplacebo in additionto standard ACLStreatment
14 iv ROSC, presence ofpulses athospital arrival
ROSC: 31 vs. 30% andsurvival to hospitaladmission: 19 vs. 23%in the interventionand control groups,respectively(P ¼ NS)
A.Lundin
etal.60
by guest on August 22, 2016 http://ehjcvp.oxfordjournals.org/ Downloaded from

Gueugniaud et al.(2008)
Prospective,randomizedtrial
2894 patients Prehospital Adult patients w/OHCA
Adrenaline (1 mg) andvasopressin (40 IU),maximum two doses,followed by standardACLS treatment
1 mg adrenaline andsaline placebo,maximum twodoses, followed bystandard ACLStreatment
21 iv Survival to hospitaladmission
ROSC: 28.6 vs. 29.5%and survival tohospital admission20.7 vs. 21.3%; in theintervention groupand control groups,respectively(P ¼ NS)
Mentzelopouloset al. (2009)
Prospective,randomizedtrial
100 patients In hospital Adult patients w/IHCA
Vasopressin (20 IU) plusadrenaline (1 mg) inrepeated doses(maximum 5 cycles)w/ methyl-prednisolone (40 mg)on the first cycle.Additional adrenalineif needed. Post-resuscitation shocktreated w/hydrocortisone2
Adrenaline (1 mg) plussaline placebo formaximum fivecycles. Salineplacebo forpatients w/ post-resuscitation shock
1 (time to ACLS) iv ROSC and survivalto hospitaldischarge
ROSC: 81 vs. 52%(P ¼ 0.003) andsurvival to hospitaldischarge 19 vs. 4%(P ¼ 0.02) in theintervention andcontrol groups,respectively
Mukoyama et al.(2009)
Prospective,randomizedtrial
336 patients Emergencydepartment
Adult patients inED w/ OHCArefractory toprehospitalresuscitation
Vasopressin (40 IU)repeated every5–10 min untilcumulative dose of160 IU
Adrenaline (1 mg),repeated every5–10 min untilcumulative dose of4 mg
33 iv Survival to hospitaldischarge
ROSC: 28.7 vs. 26.6%and survival tohospital discharge 5.6vs. 3.8% in theintervention andcontrol groups,respectively(P ¼ NS)
Carroll et al.(2012)
Prospectiveinterventionvs. historicalcontrolgroup
30 patients (20patients inhistoricalcontrol group)
In hospital Paediatric patientsin ICU w/cardiac arrestrefractory toat least onedoseadrenaline
Vasopressin (0.8 mg/kg),one dose, followed bystandard ACLStreatment
Historical controlgroup (paediatricpatients in the ICUthat received atleast two doses ofvasopressormedication, but notvasopressin)
1 iv or io Assess feasibility ofa futurerandomizedcontrolled trial
24-h survival: 80 vs. 30%,(P , 0.05) andsurvival to discharge:60 vs. 25% (P ¼ 0.07)in the interventionand control groups,respectively
Ong et al. (2012) Prospective,randomizedtrial
727 patients Emergencydepartment
Adult patients w/OHCA(includingarrest in theED)
Vasopressin (40 IU), onedose, followed bystandard ACLStreatment
Standard ACLStreatment
35 (time to EDarrival)
iv Survival to hospitaldischarge
ROSC: 30 vs. 31% andsurvival to discharge:2.3 vs. 2.9% in theintervention andcontrol groups,respectively(P ¼ NS)
Mentzelopouloset al. (2013)
Prospective,randomizedtrial
268 patients In hospital Adult patients w/IHCA
See Mentzelopoulos(2009)
See Mentzelopoulos(2009)
2 (time to ACLS) iv Survival to hospitaldischarge w/favourableneurologicalrecovery
ROSC: 83.9 vs. 65.9%(P ¼ 0.005) andneurologicallyfavourable survival13.9 vs. 5.1%(P ¼ 0.02) in theintervention andcontrol groups,respectively
Continued
Drug
therapyin
cardiacarrest
61
by guest on August 22, 2016 http://ehjcvp.oxfordjournals.org/ Downloaded from

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Continued
Author (year) Study design Study size Setting Inclusion ofparticipants
Intervention1 Control1 Time to studydrugadministration(min)
Admin. route Primaryoutcome(s)
Results
Methoxamine Patrick et al.(1995)
Prospective,randomizedtrial
199 patients In hospital Adult patients w/witnessedIHCA andOHCApresenting tothe ED
Methoxamine (40 mg),repeated doses
Adrenaline (2 mg),repeated doses
3 iv ROSC ROSC: 42 vs. 53% in theintervention andcontrol groups,respectively(P ¼ NS)
Isoproterenol Jaffe et al. (2004) Prospective,randomizedtrial
79 patients Prehospital Adult patients w/OHCA andasystole
Isoprenaline (200 mg)every 3–5 min,maximum 600 mg
Standard ACLStreatment[including atropine1 mg (total 3 mg)every 3–5 min]
7 iv ROSC ROSC: 46 vs. 45% andsurvival to hospitaldischarge 3 vs. 7%, inthe intervention andcontrol groups,respectively(P ¼ NS)
Amiodarone Kudenchuk et al.(1999)
Prospective,randomizedtrial
504 patients Prehospital Adult patients w/OHCA andshock-resistant VF
One dose of 300 mg ofintravenousamiodarone
Saline placebo 21 iv Survival to hospitaladmission
Survival to hospitaladmission 44 vs. 34%(P ¼ 0.03) andsurvival to hospitaldischarge: 13.4 and13.2% in theintervention andcontrol groups,respectively
Dorian et al.(2002)
Prospective,randomizedtrial
347 patients Prehospital Adult patients w/shock-resistant VF/VT
Amiodarone (5 mg/kg)plus saline placebo. IfVF persisted a seconddose of amiodarone(2.5 mg/kg) plusplacebo was given
Lidocaine (1.5 mg/kg)plus amiodaroneplacebo. If VFpersisted, a seconddose of lidocaine(1.5 mg/kg) wasgiven
24 iv Survival to hospitaladmission
Survival to hospitaladmission: 22.8 vs.12.0% (P ¼ 0.009)and survival tohospital discharge: 5vs. 3% (P ¼ NS) inthe intervention andcontrol groups,respectively
Lidocaine Weaver et al.(1990)
Prospective,randomizedtrial
199 patients Prehospital Adult patients w/OHCA andshock-resistant VF
100-mg bolus of lidocaine.A second doselidocaine (100 mg)was given before thenext shock if VFpersisted
Adrenaline (0.5 mg).Additionaladrenaline (0.5 mg)was given if VFpersisted
9 (time todefibrillation)
iv Not reported ROSC: 48 vs. 54% andsurvival to discharge:19 vs. 20% in theintervention andcontrol groups,respectively(P ¼ NS)
Aminophylline Mader et al.(1999)
Prospective,randomized,placebo-controlledtrial
82 patients Prehospital Adult patients w/OHCA andasystole
Aminophylline (250 mg),one dose
Saline placebo 12 iv ROSC ROSC: 27 vs. 20% in theintervention andcontrol groups,respectively(P ¼ NS)
Mader et al.(2003)
Prospective,randomized,placebo-controlledtrial
112 patients Prehospital Adult patients w/OHCA andasystole aftertreatment w/adrenaline andatropine
One dose ofaminophylline(250 mg)
Saline placebo 12 iv ROSC ROSC: 22.7 vs. 15.6% inthe intervention andcontrol groups,respectively(P ¼ NS). No patientsurvived to hospitaldischarge
A.Lundin
etal.62
by guest on August 22, 2016 http://ehjcvp.oxfordjournals.org/ Downloaded from

Abu-Laban et al.(2006)
Prospective,randomizedtrial
971 patients Prehospital Adult patients w/OHCA andasystole orPEA,refractory toinitialtreatment w/adrenaline andatropine
Aminophylline (250 mg),up to two doses
Saline placebo 27 iv ROSC ROSC: 24.5 vs. 23.7%and survival tohospital admission:6.6 and 7.6% in theintervention andcontrol groups,respectively(P ¼ NS)
Sodiumbicarbonate
Dybvik et al.(1995)
Prospective,randomized,placebo-controlledtrial
502 patients Prehospital Adult patients w/OHCA andasystole orshock-resistant VF
250 mL of Tribonat(sodium bicarbonate-trometamol-phosphate), bufferingcapacity 500 mmol/L
250 mL of salineplacebo
6 (time to EMSarrival)
iv Survival to hospitaladmission andto hospitaldischarge
Survival to hospitaladmission: 36 vs. 36%and survival todischarge: 10 vs. 14%in the interventionand control groups,respectively(P ¼ NS)
Magnesium Miller et al.(1995)
Prospectiveinterventionvs. historicalcontrolgroup
62 patients (33patients in thehistoricalcontrol group)
Emergencydepartment
Adult patients w/cardiac arrestand shock-resistant VF
One dose intravenousmagnesium-sulphate(2.5–5 g)
Standard ACLStreatment
13 iv ROSC . 30 min ROSC: 35 vs. 21%(P ¼ 0.21) andsurvival to discharge:5.2 vs. 4.5% in theintervention andcontrol groups,respectively
Fatovich et al.(1997)
Prospectiverandomized,placebo-controlledtrial
67 patients Emergencydepartment
Adult patients w/in the ED w/OHCArefractory toprehospitalresuscitation
Magnesium (5 g), onedose
Saline placebo 33 iv ECG rhythm 2 minafter drugadministration
ROSC: 23 vs. 22% andsurvival to discharge3 and 0% in theintervention andplacebo groups,respectively(P ¼ NS)
Thel et al. (1997) Prospective,randomizedplacebo-controlledtrial
156 patients In hospital Adult patients w/IHCA
Magnesium (2 g bolus),followed by 8 g over24 h
Saline placebo 11 iv ROSC ROSC: 54 vs. 60%(P ¼ 0.44) andsurvival to hospitaldischarge 21 vs. 21%(P ¼ NS) in theintervention andcontrol groups,respectively
Allegra et al.(2001)
Prospective,randomized,placebo-controlledtrial
116 patients Prehospital Adult patients w/OHCA and VF
Magnesium (2 g) one dose Saline placebo andadrenalineaccording toguidelines
28 iv ROSC in the fieldand a perfusingpulse on arrivalat the ED
ROSC 25.5 vs. 18.5%and survival todischarge: 3.6 and3.7% in theintervention andcontrol groups,respectively.(P ¼ NS)
Hassan et al.(2002)
Prospective,randomized,placebo-controlledtrial
105 patients Prehospital(includingemergencydepartment)
Adult patients w/OHCA andshock-resistant orrecurrent VF
Magnesium-sulphate (2–4 g)
Saline placebo 8 (time to EMSarrival)
iv ROSC ROSC: 17 vs. 13% andsurvival to hospitaldischarge 4 vs. 2% inthe intervention andcontrol groups,respectively(P ¼ NS)
Continued
Drug
therapyin
cardiacarrest
63
by guest on August 22, 2016 http://ehjcvp.oxfordjournals.org/ Downloaded from

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Continued
Author (year) Study design Study size Setting Inclusion ofparticipants
Intervention1 Control1 Time to studydrugadministration(min)
Admin. route Primaryoutcome(s)
Results
Thrombolytics Bottiger et al.(2001)
Prospectiveinterventionvs. historicalcontrolgroup
90 patients (50patients in thehistoricalcontrol group)
Prehospital Adult patients w/OHCA ofcardiacaetiologywithout ROSCafter 15 min
5000 U of heparin bolusand tPA (50 mg),intervention wasrepeated if no ROSCafter 30 min
ACLS treatment 8 (time to EMSarrival)
iv Safety of theprotocol (i.e.,bleedingcomplications),ROSC andsurvival tohospitaladmission
ROSC: 68 vs. 44%(P ¼ 0.026) andsurvival to discharge15 vs. 8% (P ¼ NS) inthe intervention andcontrol groups,respectively
Abu-Laban et al.(2002)
Prospectiverandomized,placebo-controlledtrial
233 patients Prehospital Adult patients w/OHCA andPEA refractoryto initialtherapy
Tenecteplase (100 mg),one dose. Afterenrolment standardresuscitation wascontinued for at least15 min
Saline placebo 35 iv. Survival to hospitaldischarge
ROSC: 21.4 vs. 23.3%and survival todischarge 0.8 and 0%in the interventionand control groups,respectively(P ¼ NS)
Fatovich et al.(2004)
Prospective,randomized,placebo-controlledtrial
35 patients Emergencydepartment
Adult patients inED w/ OHCArefractory toprehospitalresuscitation
Tenecteplase (50 mg) asfirst drug, one dose
Saline placebo,followed by ACLStreatment
43 iv ROSC ROSC: 42 vs. 6%(P , 0.05) andsurvival to discharge5 vs. 6% (P ¼ NS) inthe intervention andcontrol groups,respectively
Bottiger et al.(2008)
Prospectiverandomizedplacebo-controlledtrial
1050 patients Prehospital Adult patients w/witnessedOHCA andinitiation ofACLS within10 min
Tenecteplase (50 mg),one dose
Saline placebo. 18 iv 30-day survival ROSC: 55.0 vs. 54.6%and survival todischarge: 15.1 vs.17.5% in theintervention andcontrol groups,respectively(P ¼ NS)
A.Lundin
etal.64
by guest on August 22, 2016 http://ehjcvp.oxfordjournals.org/ Downloaded from

Erythropoietin Grmec et al.(2009)
Prospective,non-randomizedtrial w/prospectiveandhistoricalcontrolgroup
54 prospectivelyincludedpatients (24erythropoietinand 30 saline),48 patients inthe historicalcontrol group
Prehospital Adult patients w/OHCA
Erythropoietin (90 000 IUof beta-epoetin), onedose0
Saline placebo(prospectivecontrols), standardACLS treatment(historicalcontrols)
6 (time to CPR) iv Survival to ICUadmission
ROSC: 92 vs. 53%(P ¼ 0.03) in theintervention andconcurrent controlgroups. ICUadmission: 92 vs. 50%and 65% (adjustedP ¼ NS) in theintervention group,concurrent controlsand matchedcontrols, respectively
Corticosteroids Tsai et al. (2007) Prospective,non-randomized,trial
97 patients Emergencydepartment
Adult patient inthe ED w/OHCArefractory toprehospitalresuscitation
100 mg Hydrocortisone,one dose
Saline placebo Not reported iv Not reported ROSC: 61 vs. 39%(P ¼ 0.038) andsurvival to hospitaldischarge 8 vs. 10%(P ¼ NS) in theintervention andcontrol groups,respectively
Crystalloids/colloids
Breil et al. (2012) Prospectiverandomizedtrial
203 patients Prehospital Adult patents w/OHCA
2 mL/kg of 7.2% NaCl w/6% HES (200 000/0.5),infused over 10 min
2 mL/kg of 6% HES(200 000/0.5),infused over 10 min
14 iv Survival to hospitaladmission andhospitaldischarge
Survival to hospitaladmission: 50 vs. 47%and survival tohospital discharge 23vs. 21% in theintervention andcontrol groups,respectively(P ¼ NS)
ACLS: advanced cardiac life support; OHCA: out-of hospital cardiac arrest; IHCA: in-hospital cardiac arrest; ED: emergency department; PEA: pulseless electrical activity; EMS: emergency medical services; ROSC: return of spontaneouscirculation; iv: intravenous; HES: hydroxyethyl starch; NS: non-significant; ICU: intensive care unit; VF: ventricular fibrillation; HDE: high-dose adrenaline; SDE: standard-dose adrenaline 1: standard ACLS treatment (adrenaline 1 mg repeatedevery 3–5 min) was provided in the intervention and control groups if not stated otherwise; 2: 300 mg hydrocortisone daily for 7 days maximum, w/ gradual taper.
Drug
therapyin
cardiacarrest
65
by guest on August 22, 2016 http://ehjcvp.oxfordjournals.org/ Downloaded from

Our search yielded 1498 –111 studies involving vasopressin duringhuman resuscitation, including 10 prospective interventionaltrials.90 – 99,98 – 107 Two small, randomized, controlled trials (total240 patients) compared adrenaline (1 mg) with vasopressin(40 IU), and neither ROSC nor survival to discharge differed be-tween groups.98,99 Callaway et al. randomized 325 patients to thecombination of adrenaline and vasopressin (40 IU) or adrenalinealone. The rates of ROSC and survival to discharge were similar.100
Mukoyama et al.101 randomized 336 OHCA patients after pro-longed cardiac arrest to repeated doses of vasopressin (40 IU) oradrenaline (1 mg). There were no differences in ROSC or survivalto hospital discharge.
Three large, multicentre studies evaluated vasopressin and adren-aline.102– 104 Wenzel et al.102 randomized 1219 OHCA patients totwo doses of either 40 IU of vasopressin or 1 mg of adrenaline andadditional treatment with adrenaline was added if needed. Overall,there was no difference in survival to discharge. In a prespecifiedsubgroup of patients with asystole, vasopressin resulted in a signifi-cantly higher rate of ROSC and survival to hospital discharge (29 vs.20%, P ¼ 0.02, and 4.7 vs. 1.5%, P ¼ 0.04, respectively). Gueugniaudet al. randomized 1442 OHCA patients to either adrenaline (1 mg)and vasopressin (40 IU) or adrenaline and placebo. There was nodifference in the primary outcome, i.e. survival to hospital admis-sion103 This study differed from the former, as rates of asystolewere higher (83 vs. 44%) and time to drug administration was longer(21 vs. 10 min). Ong et al.104 randomized 727 OHCA patients to asingle dose of adrenaline (1 mg) or vasopressin (40 IU) at presenta-tion in the emergency department (ED). There was no difference inthe primary outcome, survival to hospital discharge, although therewas a trend towards improved survival with vasopressin in a sub-group with shockable rhythm. More than 90% of patients in bothgroups received additional open-label adrenaline. In two placebo-controlled studies, a group from Greece randomized patients to re-peated doses of adrenaline (1 mg) or a combination of vasopressin(20 IU) and adrenaline every 3–5 min.105,106 Concurrent with thefirst injection, one dose methyl-prednisolone (40 mg), was adminis-tered to the intervention group. If haemodynamic instability devel-oped after resuscitation, hydrocortisone (300 mg) daily, withgradual tapering, was administered to the intervention group. Thefirst study enrolled 99 patients and there was a significant benefitin the treatment group for the primary endpoints of ROSC (81 vs.52%, P ¼ 0.003) and survival to hospital discharge (19 vs. 4%, P ¼0.02). The second study, powered to detect a difference in neuro-logically favourable survival, enrolled 268 adult IHCA patients.Haemodynamic parameters, during and after resuscitation, ROSC(83.9 vs. 65.9%, P ¼ 0.005), and neurologically favourable survivalto hospital discharge (13.9 vs. 5.1%, P ¼ 0.02) improved significantlyin the intervention group. The cause of arrest was deemed to behypotension or respiratory failure in .70% of patients, 16% hadan initial shockable rhythm, and the median time to resuscitationfrom collapse was 2 min.
Four observational studies evaluated vasopressin in cardiac ar-rest.108 – 111 Two studies reported an association between onedose of vasopressin (40 IU), alone or in combination with adren-aline, and increased ROSC, but none demonstrated a significant dif-ference in survival.108,109 Duncan et al.110 found an associationbetween vasopressin use and a reduced likelihood of ROSC in
paediatric ICU patients. The second study comprised only 10 pa-tients.104 Finally, one study reported an increased rate of ROSC(63 vs. 37%, P ¼ 0.01) in a subgroup of cardiac arrest patientswith acidosis, when vasopressin and adrenaline were administeredcompared with adrenaline alone.111
MethoxamineMethoxamine is an a1-adrenergic receptor agonist, similar in struc-ture to phenylephrine. It increases peripheral resistance and after-load through vasoconstriction, and can cause reduced cardiacoutput and reflexive bradycardia.112 In animal studies, methoxamineresulted in increased coronary blood flow and ROSC,33,113 and inone study, there was less myocardial oxygen imbalance and impair-ment of cerebral blood flow compared with adrenaline.114 Wefound only one human trial of methoxamine. Patrick et al.115 rando-mized 199 adult patients (of whom 145 were analysed) with IHCAto either 2 mg of adrenaline or 40 mg of methoxamine every 4 min.Return of spontaneous circulation, survival to discharge, and neuro-logical outcome did not differ significantly between groups.
IsoproterenolIsoproterenol is a pure b-adrenergic agonist with inotropic andchronotropic effects. It increases cardiac output and myocardialoxygen consumption, and can exacerbate ischaemia and arrhyth-mias in patients with ischaemic heart disease or impaired ventricularfunction.116 It is primarily used for the temporary treatment of bra-dyarrhythmias.3 Animal studies have reported a reduction in bloodpressure and CPP with isoproterenol during resuscitation.33,117 Wefound one study by Jaffe et al.,118 evaluating isoproterenol in humancardiac arrest. Seventy-nine patients with asystole as the initialrhythm were included in an open-label randomized trial. Patients re-ceived standard advanced cardiac life support (ACLS) treatment in-cluding atropine and were randomized to 200 mg of open-labelisoproterenol every 3–5 min or no isoproterenol. There was no dif-ference in the rate of ROSC or survival to hospital admission and thestudy was terminated prematurely due to futility.
Anti-arrhythmic drugs
AmiodaroneAmiodarone is classified as a class III anti-arrhythmic, although itspharmacodynamic effects are pleiotropic and include blockage ofsodium channels, calcium channels, and a- and b-antagonisticeffects.114 –116,119 – 121 Acute intravenous amiodarone has been re-ported to increase, cause no change in, and reduce the defibrillationthreshold in animal studies of ventricular fibrillation.14,16
We found seven studies of amiodarone in human cardiac ar-rest.14,16,117 – 128 Two compared amiodarone with nifekalant andwill be discussed in another section.127,128 Two randomized, con-trolled trials compared amiodarone with placebo and lidocaine,respectively.122,123 Both studies evaluated a dose of 300 mg of amio-darone in shock-resistant ventricular arrhythmia and the primaryoutcome was survival to hospital admission. Kudenchuk et al.122
enrolled 504 patients in cardiac arrest who were randomly assignedto 300 mg of intravenous amiodarone or placebo. Survival tohospital admission was higher with amiodarone (44 vs. 34%,
A. Lundin et al.66
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

P ¼ 0.03). In the ALIVE trial, Dorian et al.123 randomized 347patients with shock-resistant ventricular fibrillation or relapse ofventricular fibrillation to lidocaine (1.5 mg/kg) or amiodarone(5 mg/kg). If ventricular fibrillation persisted, another dose of amio-darone (2.5 mg/kg) could be administered. The survival to hospitaladmission was higher with amiodarone than with lidocaine (22.8 vs.12%, P , 0.05). Neither study was powered to detect differencesin survival to discharge.
We found three observational studies of amiodarone.124 – 126
One small retrospective study evaluated the use of amiodaroneand reported no statistically significant difference in survival, regard-less of whether or not amiodarone was given, and only 36 patientsreceived amiodarone.124 In a retrospective study, Rea et al.125 com-pared survival in 194 patients who received lidocaine, amiodarone,or a combination of the two. Twenty-four-hour survival did not dif-fer statistically between the three groups. Finally, one study re-viewed paediatric patients with IHCA and survival in relation towhether amiodarone, lidocaine, both or none were adminis-tered.126 Only lidocaine was associated with improved ROSC andshort-term survival.
LidocaineLidocaine is a class Ib anti-arrhythmic; it prolongs conduction vel-ocity and shortens action potential duration and the effective refrac-tory period.13 Prior to the ALIVE trial in 2002, lidocaine wasrecommended for shock-resistant arrhythmias.123
We found seven studies of lidocaine in cardiac arrest. Four com-pared lidocaine with amiodarone or nifekalant and are discussed inother sections.123,125,126,129 Weaver et al.130 randomized 192 pa-tients with shock-resistant ventricular fibrillation to either adren-aline or lidocaine. There was no significant difference in the rate ofROSC or survival between the groups. Patients who receivedlidocaine had a three times higher rate of asystole following defib-rillation. A small randomized trial compared sotalol (100 mg) andlidocaine (100 mg) in shock-resistant ventricular fibrillation andfound no significant difference in survival to hospital admissionor discharge.131 Finally, a retrospective study of 1212 patients,33% of whom received lidocaine, reported an association be-tween lidocaine and survival to hospital admission (38 vs. 18%,P , 0.01), although there was no difference in survival to hospitaldischarge.132
ProcainamideProcainamide is a class Ia anti-arrhythmic and, unlike lidocaine, it alsoblocks potassium channels, prolonging action potential duration andQT time.13 It has been used since the 1950s to treat various arrhyth-mias, including ventricular fibrillation. Whereas early animal studiesof cardiac arrest found it inferior to vasopressors,33 others have de-monstrated beneficial electrophysiological effects and, in a humanstudy, procainamide was superior to lidocaine in converting sus-tained monomorphic ventricular tachycardia in humans.15,133
We found two observational studies of procainamide in humancardiac arrest.134,135 In a small comparison study of 20 patients, pro-cainamide was associated with increased survival in undifferentiatedcardiac arrest.134 The second study retrospectively compared out-come in 665 patients with shock-resistant ventricular fibrillation, ofwhom 176 had received procainamide and, after adjustment for
baseline imbalances, there was no association between treatmentwith procainamide and survival.135
AtropineAtropine is an anticholinergic drug used to treat bradyarrhythmiasand its cardiac effects are mainly on the sinus and the atrioventricu-lar nodes.136 It was introduced in the treatment for bradyasystolicarrests after a case series in the 1970s.137 In 2010, atropine was re-moved from European Resuscitation Council Guidelines for Resus-citation due to the lack of evidence. Animal studies of atropine inPEA report contradictory results in terms of ROSC.138,139 Wefound one, retrospective study of atropine in human cardiac ar-rest,140 in which 7448 adult patients, 6419 with asystole and 1029with PEA, were included. Patients with asystole had a significantlyhigher rate of ROSC if atropine and adrenaline were given, whencompared with adrenaline alone (adjusted OR 1.6; P , 0.05). Thetwo groups had similar 30-day favourable neurological outcomes.In the PEA group, atropine and adrenaline were associated withsignificantly lower 30-day survival compared with only adrenaline(adjusted OR 0.4, P ¼ 0.016).
AminophyllineAminophylline has complex cardiovascular effects dependent onthe effect of theophylline, as both a phosphodiesterase inhibitorand an adenosine receptor antagonist.141 Cardiac effects include in-creased inotropy, chronotropy, and coronary vasoconstriction.During myocardial ischaemia, the accumulation of endogenous ad-enosine can result in bradycardia, vasodilation, and negative inotro-py, and could perpetuate asystole.142 Aminophylline couldtheoretically prevent bradyasystolic arrest and post-defibrillatoryasystole and PEA. This latter theory was tested in two animal modelswith prolonged ventricular fibrillation.143,144 Aminophylline admin-istration, in addition to adrenaline, neither increased the rate ofROSC nor reversed PEA after defibrillation.
We identified three studies of aminophylline in human cardiac ar-rest.145– 147 Two small studies randomized a total of 184 patients incardiac arrest to aminophylline or placebo in addition to standardACLS treatment.145,146 Both were negative for the primary out-come, rate of ROSC. Abu-Laban et al.147 studied the effect of ami-nophylline in patients with bradyasystolic arrest or PEA and 971patients, refractory to treatment with adrenaline and atropine,were randomized to aminophylline or placebo. There was no differ-ence in the rates of ROSC or survival to hospital discharge.
NifekalantNifekalant is a potassium channel antagonist used in Japan to treatventricular arrhythmias. In animal studies, nifekalant prolongs the re-fractory period and has been reported to reduce the number andthe energy level of defibrillations, the adrenaline dose, and thetime to ROSC compared with placebo.148 We found four studiesof nifekalant in human cardiac arrest.127 –129,149 All were from Japan,all had a retrospective design and all compared nifekalant with eitheramiodarone or lidocaine. The studies comparing nifekalant withlidocaine found that nifekalant was associated with a higher rate ofROSC and 24-h survival.129,149 The studies comparing amiodaronewith nifekalant in patients with shock-resistant ventricular fibrilla-tion found no difference in terms of ROSC or survival,127,128
Drug therapy in cardiac arrest 67
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

although one study reported a significantly shorter time to ROSCwith nifekalant, 6 vs. 20 min.128
Beta-blockersBeta-blockers reduce the risk of ventricular arrhythmias and suddencardiac death in many myocardial pathologies150 –152 In animal mod-els, beta-blockade during resuscitation is associated with improvedrates of ROSC, less tachycardia, an improved myocardial oxygenbalance, less post-resuscitation myocardial dysfunction, and a highercardiac index after resuscitation.43,153 –155 Beta-blockade could po-tentially be beneficial in refractory ventricular fibrillation, as en-dogenous and exogenous catecholamines facilitate myocardialinstability,48,156 increases defibrillatory threshold, and relapse toventricular arrhythmias after ROSC.157 Furthermore, animal studiessuggest that beta-blockers reduce cardiac dysfunction afterresuscitation.43
We identified one study of beta-blockers during resuscitation inhumans. Driver et al.157 retrospectively studied 25 patients with re-fractory ventricular fibrillation; six patients received a short-actingb-1 antagonist (esmolol) during CPR and 19 did not. All patientshad multiple defibrillations and received adrenaline, amiodarone,and sodium bicarbonate. A higher rate of ROSC (66 and 32%)and survival with good neurological outcome (50 and 11%) wereachieved in the group treated with esmolol, although the differenceswere not statistically significant.
MagnesiumMagnesium is the second most common intracellular cation. Itcauses systemic and coronary vasodilatation and diminishes the con-tractility of vasopressors.158,159 The electrophysiological effects in-clude reduced ventricular conduction and suppression of early andlate after-depolarizations.160 In an animal study, magnesium admin-istration increased the threshold to induce ventricular arrhyth-mias.161,162 It is used for treating polymorphic ventriculartachycardia associated with a prolonged QT interval.163
We identified five studies of magnesium in human cardiac ar-rest.158 – 162,164 – 168 All were small randomized trials, comprising atotal of 506 patients. Three studies included only patients with ven-tricular fibrillation.164 – 166 All patients received standard ACLStreatment and magnesium was administered when defibrillationhad failed, with doses ranging from 2 to 5 g. In no study was magne-sium administration associated with a higher rate of either ROSC orsurvival to hospital discharge, although small sample sizes make itdifficult to exclude a type II error. However, a meta-analysis of mag-nesium administration in cardiac arrest did not find any significantincrease in ROSC or survival to hospital discharge with magnesiumadministration.169 This study reportedly had an 80% power to de-tect a 10% difference in survival to hospital discharge.
Miscellaneous drugs
Thrombolytic drugsThrombolytics convert plasminogen to plasmin,170 which degradesfibrin and has been shown to reduce mortality in ST-segment-elevation myocardial infarction171 and haemodynamically unstablepulmonary embolism.172 The rationale for the use of thrombolytics
in cardiac arrest is to dissolve possible blood clots in the coronary orpulmonary circulation. Furthermore, Fischer et al.173 demonstratedimproved microcirculatory cerebral perfusion in a cat model of car-diac arrest with the administration of thrombolytics duringresuscitation.
Six studies evaluated thrombolytics in human cardiac arrest.174 –
179 Four were randomized trials enrolling a total of .2700 pa-tients.174 – 176 All studies used Tenecteplase as the intervention.Two small studies reported increased rates of ROSC and one re-ported increased survival to hospital admission with Tenecte-plase.174,175 Two large randomized trials, however, found nobenefit in terms of survival to discharge in the group that receivedtissue plasminogen activator (tPA). In the first, Abu-laban et al.176
randomized 1500 patients with PEA to receive 100 mg of t-PA orplacebo. Only one patient in the intervention group and none inthe control group survived to hospital discharge. Bottiger et al.177
randomized 1050 patients with undifferentiated cardiac arrest toTenecteplase or placebo. The study was stopped early as a resultof futility. The rates of ROSC and 30-day survival did not differ be-tween groups (55.0 vs. 54.6%, P ¼ 0.96, and 14.7 vs. 17.0%, P ¼ 0.39,respectively). In a post hoc analysis of a large clinical trial, Stadlbaueret al.178 found that hospital admission rates were significantly higherin patients who received thrombolysis than in those who did not(45.5 vs. 32.7%, P ¼ 0.01). However, patients in the thrombolysisgroup were significantly younger and were more likely to have ashockable rhythm and to receive bystander CPR. Finally, a small ob-servational trial compared 50 patients with treatment-refractorycardiac arrest who received Tenecteplase with 113 concurrent con-trols.179 The rates of ROSC and survival to hospital admission weresignificantly higher in the thrombolysis group (26 vs. 12.4%, P ¼0.04, and 12 vs. 0%, P , 0.05, respectively).
CorticosteroidsCortisol affects a wide range of physiological processes, includingthe regulation of catecholamine synthesis, and their effects on thecardiovascular system.96 The potential role in resuscitation includesthe potentiation of catecholaminergic vasoconstriction and protec-tion from ischaemia–reperfusion injury.180 The vasoconstrictive ef-fects of noradrenaline are augmented within minutes aftertreatment with topical cortisone, supporting a relatively immediateeffect.181,182 In a rat model of cardiac arrest, hydrocortisone admin-istration increased ROSC.183 In observational studies, higher serumcortisol, during resuscitation and after ROSC, is associated with agreater likelihood of survival and less likelihood of circulatory shockas cause of death, in both animal models and humans.97,184 –188 Cor-tisol levels after resuscitation are inversely correlated with no-flowtime and insufficient cortisol levels are possibly a consequence of is-chaemic injury to the hypothalamic–pituitary–adrenal axis.97,189
We found three human studies evaluating corticosteroids in car-diac arrest. In a non-randomized prospective trial, Tsai et al.190 in-cluded 97 OHCA patients upon arrival at the ED, whereas 36patients received 100 mg of hydrocortisone and 61 received saline.Eighty per cent had asystole as the initial rhythm. The rate of ROSCwas higher in the hydrocortisone group (61 vs. 39%, P ¼ 0.038), butthere was no difference in survival. Two studies, mentioned previ-ously, demonstrated an improved outcome for IHCA patients ran-domized to the combination of adrenaline, vasopressin, and
A. Lundin et al.68
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

methyl-prednisolone followed by daily hydrocortisone for patientswith post-cardiac arrest syndrome.105,106 The role of corticoster-oids is difficult to delineate because of the combinatorial interven-tion. There was, however, a significantly higher rate of neurologicallyfavourable survival in the subgroup with post-cardiac arrest syn-drome who received hydrocortisone after resuscitation comparedwith placebo.
ErythropoietinErythropoietin has anti-apoptotic properties and promotes prolifer-ation and maturation of erythrocytes in the bone marrow.191 Animalmodels have demonstrated neuroprotective effects from erythro-poietin after regional CNS ischaemia,192 although not after cardiacarrest.193 Interestingly, erythropoietin improves haemodynamicvariables, increases ROSC and short-term survival, and reducespost-resuscitative myocardial dysfunction in animal models of car-diac arrest.194 – 197 The immediate effects of erythropoietin onhaemodynamic parameters during resuscitation are not wellunderstood.198
We found one study evaluating erythropoietin during resuscita-tion in humans. Grmec et al.199 prospectively compared 24 patientswith OHCA who received erythropoietin (90 000 IU of beta-epoetin) with 30 OHCA patients who received 0.9% saline. Out-come was also compared retrospectively with that of 48 matchedcontrols. In the prospective comparison, the rate of ROSC andICU admission, but not 24-h survival, was higher in the erythropoi-etin group after adjustment for baseline characteristics. Comparedwith historical controls, erythropoietin administration was asso-ciated with significantly higher rates of ROSC and ICU admission, al-though 24-h survival and survival to hospital discharge were notstatistically different.
Sodium bicarbonateThe physiological effects of acidosis include increased sympatheticoutput, myocardial depression, and arteriolar vasodilation, with adecreased response to catecholamines.200,201 Sodium bicarbonatehas an alkalizing effect in plasma by increasing strong ion differenceand shifting the bicarbonate to carbondioxide ratio.202,203 The effecton intracellular pH, however, is uncertain, as generated carbon di-oxide diffuses readily across the cellular membrane.202,204 In animalstudies, sodium bicarbonate administration is associated with eitherunchanged or reduced aortic pressure and CPP.205 –208 It has a spe-cific role in the treatment of cardiac arrest secondary to intoxicationwith sodium channel blockers or hyperkalaemia.209
We found three studies evaluating the effect of sodium bicarbon-ate in human cardiac arrest.210 –212 Dybvik et al.210 performed a ran-domized trial of 502 patients with OHCA. The patients wererandomized to 250 mL of Tribonat (i.e. sodium bicarbonate, trome-tamol, and disodium phosphate) or saline. There was no differencein survival to hospital admission or discharge. One small retrospect-ive study found no association between ROSC and sodium bicar-bonate treatment in patients with prolonged (.15 min) cardiacarrest.211 Finally, in a retrospective study of paediatric cardiac arrest,the use of sodium bicarbonate was associated with a reduction inshort-term survival and survival to discharge, although sodium bi-carbonate administration was also associated with arrest in theICU and longer resuscitation efforts.212
Crystalloids and colloidsHypertonic solutions have been found to increase myocardial bloodflow, cerebral perfusion, and ROSC during resuscitation in an animalmodel of cardiac arrest.213,214 We identified one study examiningthe effects of hypertonic solution in human resuscitation.215 Breilet al. randomized 203 patients with OHCA to an infusion of 2 mL/kg of hypertonic saline (7.2% NaCl with 6% hydroxyethyl starch 200000/0.5) or only hydroxyethyl starch. There was no difference insurvival to hospital admission or survival. One observational studycompared ROSC and survival in relation to whether or not LactatedRinger’s was administered.216 More than 500 000 patients from alarge registry in Japan were included. The administration of LactatedRinger’s was associated with a reduced likelihood of survival withgood functional outcome after 1-month survival (adjusted oddsratio 0.764, P ¼ 0.04).
DiscussionThis review of the literature of human studies of the last 25 yearssuggests that there is still equipoise for the use of drug therapy incardiac arrest. Out of 88 studies, we identified no study in whichdrug therapy, compared with placebo, improved long-term survival.Regarding adrenaline and amiodarone, the drugs currently recom-mended in cardiac arrest,3 two prospective randomized placebo-controlled trials, were identified for adrenaline,64,65 and one foramiodarone,122 all were underpowered to detect differences in sur-vival to hospital discharge.
Our results are in line with other systematic reviews of drug ther-apy in cardiac arrest.217 – 225 They are also in line with the results oftwo studies evaluating drug therapy in cardiac arrest that were notincluded in our review, since they did not evaluate a specified drug.Olasveengen et al.29 randomized 1183 OHCA patients to intraven-ous access or no intravenous access and Stiell et al.31 enrolled 5638OHCA patients in a ‘before–after’ study evaluating the effects ofACLS implementation. Both were neutral for their primary out-come of survival to hospital discharge.
Conducting prospective trials of interventions in cardiac arrestpose several difficulties. Time constraints, prehospital environment,lack of informed consent, and preconceptions regarding treatmentpose methodological, ethical, and pedagogical obstacles to trialistsand may explain why trials in cardiac arrest, including other interven-tions than drug therapy,226 – 232 often result in neutral outcomes.Nonetheless, there is a need for placebo-controlled trials of drugtherapy in cardiac arrest. Evaluation of adrenaline is particularly war-ranted, both because of its ubiquitous use as well as animal36,37,39–41
and observational data,82,233,234 suggesting the lack of long-termbenefit and possibly direct harm with treatment. In 2010, The Inter-national Liaison Committee for Resuscitation stated that placebo-controlled trials to evaluate the use of vasopressors in adult andpaediatric cardiac arrest are needed.235
Our review identifies multiple issues with interventional studiesof human cardiac arrest. First, there were overall small sample sizesand limited statistical power to detect differences in patient import-ant outcomes (e.g. survival to hospital discharge), especially as sur-vival rates were generally low. Observational studies, while larger,often revealed inconsistent results which probably reflects
Drug therapy in cardiac arrest 69
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

differences in registries, variations in statistical methodology, andgeographical and temporal differences in the care of cardiac arrestpatients.73,77,80 The ongoing PARAMEDIC2 trial (ISRCTN:73485024) is planning to randomize 8000 patients to adrenalineor placebo and the ROC-ALPS trial will randomize 3000 patientswith shock-resistant OHCA to amiodarone, lidocaine, or pla-cebo.236 The studies are in OHCA patients and are planned to becompleted in 2018 and late 2015, respectively. They will hopefullyprovide valuable data on the use of drug therapy in cardiac arrest.
A second issue is time to drug administration in studies of OHCA.If circulatory arrest is prolonged .10–15 min, survival is dismal re-gardless of treatment26 and time to intervention is crucial. Thismight be one possible explanation for the discrepancy betweenfindings in animal and human studies. In a systematic review ofdrug therapy in animal studies, the average time to drug administra-tion was 9.5 min,237 but in our review of human studies it was 16 minand only one study of vasopressor therapy in OHCA patients had amedian time to drug administration ,10 min.
Third, most studies enrolled patient with undifferentiated cardiacarrest irrespective of time in no-flow, aetiology, initial rhythm, orpredicted survival. However, as outlined earlier, the pathophysi-ology of cardiac arrest is different depending on patient characteris-tics and comorbidities, aetiology of arrest, time in no-flow and initialrhythm, and likelihood of survival can range from a few per cent toover 50%.5,8 A single drug or intervention could have unequal effectsdepending on such differences, which would augment the difficultiesof demonstrating beneficial effects of a certain intervention andeffect sizes risk depletion. Meanwhile, intervention or drug recom-mendations cannot be too complicated to allow for implementationinto clinical practice. Even in the context of a clinical trial interven-tions are likely to fail if too complex.
Fourth, many of the trials were performed before the use of cur-rent post-resuscitative interventions (e.g. target temperature man-agement and percutaneous cardiac intervention) and thereforemight have had less chance of translating an improvement inROSC or survival to hospital admission into improved long-termsurvival. In fact, registries from Europe and the USA have reportedimproved survival in patients with cardiac arrest, regardless ofrhythm, during the last 10–15 years, even though no significantchange in resuscitation guidelines has taken place during thisperiod.5,7,238 – 240
Finally, in addition to, or instead of, currently recommendeddrugs in cardiac arrest our review suggests that ‘new’ drugs, suchas corticosteroids, beta-blockers, and erythropoietin, with supportfrom animal studies, but as of yet insufficient data from human trials,could be promising for future clinical trials. Of all reviewed studies,only one prospective study on IHCA demonstrated improvedneurological outcome with one therapy over another106 using acombination of vasopressin, steroids, and adrenalin as the interven-tion compared with standard adrenaline administration. However,survival in the control group was low, survival in the interventiongroup was not higher than in registries from Sweden and theUSA,5,7 and the results should probably not be generalized toOHCA patients as only IHCA patients were enrolled. The role ofeach individual drug is also unclear.
Regardless of the intervention, future trials should be well de-signed and controlled regarding timing of drug administration and
preferably conducted in large research networks to be able to enrollarge enough sample sizes in order to demonstrate differences inrelevant outcomes.
ConclusionThe evidence base for drug therapy in cardiac arrest is scarce. Manydrugs have been considered and several have shown promising re-sults in animal studies. Regarding adrenaline and amiodarone, thedrugs currently recommended in cardiac arrest, there is no evidenceof improved long-term survival with a favourable neurological out-come in humans. However, many human studies of drug therapy incardiac arrest have not been powered to identify differences in im-portant clinical outcomes such as survival to hospital discharge andfavourable neurological outcome. Efforts are needed to initiate largemulticentre, prospective, randomized, clinical trials to evaluate bothcurrently recommended and future drug therapies.
AcknowledgementsMany thanks to librarian Eva-Lotta Daxberg, Medical Library, Sahl-grenska University Hospital, Goteborg.
Conflict of interest: none declared.
References1. Myerburg RJ, Castellanos A. Cardiac arrest and sudden cardiac death. In
Bonow RO, ed. Braunwalds Heart Disease: A Textbook of Cardiovascular Medicine.9th ed. Philadelphia: Elsevier Saunders; 2012. p. 863.
2. Engdahl J, Bang A, Lindqvist J, Herlitz J. Factors affecting short- and long-term prog-nosis among 1069 patients with out-of-hospital cardiac arrest and pulseless elec-trical activity. Resuscitation 2001;51:17–25.
3. Soar J, Nolan JP, Bottiger BW, Perkins GD, Lott C, Carli P, Pellis T, Sandroni C,Skrifvars MB, Smith GB, Sunde K, Deakin CD. European Resuscitation CouncilGuidelines for Resuscitation 2015: Section 3. Adult advanced life support. Resus-citation 2015;95:100–147.
4. Swor RA, Boji B, Cynar M. Bystander vs EMS first-responder CPR: initial rhythmand outcome in witnessed nonmonitored out-of-hospital cardiac arrest. AcadEmerg Med 1995;2:494–498.
5. Herlitz J, Aune S, Claesson A, Svensson L. Epidemiology of cardiac arrest outsideand inside hospital. Experiences from registries in Sweden. SIGNA VITAE 2010;5 (Suppl 1):44–45.
6. Valenzuela TD, Roe DJ, Nichol G, Clark LL, Spaite DW, Hardman RG. Outcomesof rapid defibrillation by security officers after cardiac arrest in casinos. N Engl JMed 2000;343:1206–1209.
7. Girotra S, Nallamothu BK, Spertus JA, Li Y, Krumholz HM, Chan PS. Trends in sur-vival after in-hospital cardiac arrest. N Engl J Med 2012;367:1912–1920.
8. Weisfeldt ML, Becker LB. Resuscitation after cardiac arrest: a 3-phase time-sensitive model. JAMA 2002;288:3035–3038.
9. MacDonald RD, Mottley JL, Weinstein C. Impact of prompt defibrillation on car-diac arrest at a major international airport. Prehosp Emerg Care 2002;6:1–5.
10. Swerdlow C, Russo A, Degroot P. The dilemma of ICD implant testing. Pacing ClinElectrophysiol 2007;30:675.
11. De Maio VJ, Stiell IG, Wells GA, Spaite DW. Optimal defibrillation response inter-vals for maximum out-of-hospital cardiac arrest survival rates. Ann Emerg Med2003;42:242–250.
12. Sarkozy A, Dorian P. Strategies for reversing shock-resistant ventricular fibrilla-tion. Curr Opin Crit Care 2003;9:189–193.
13. Kowey PR. Pharmacological effects of antiarrhythmic drugs. Review and update.Arch Intern Med 1998;158:325–332.
14. Zhou L, Chen BP, Kluger J, Fan C, Chow MS. Effects of amiodarone and its activemetabolite desethylamiodarone on the ventricular defibrillation threshold. J AmColl Cardiol 1998;31:1672–1678.
15. Kwan YY, Fan W, Hough D, Lee JJ, Fishbein MC, Karagueuzian HS, Chen PS. Effectsof procainamide on wave-front dynamics during ventricular fibrillation in open-chest dogs. Circulation 1998;97:1828–1836.
A. Lundin et al.70
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

16. Huang J, Skinner JL, Rogers JM, Smith WM, Holman WL, Ideker RE. The effects ofacute and chronic amiodarone on activation patterns and defibrillation thresholdduring ventricular fibrillation in dogs. J Am Coll Cardiol 2002;40:375–383.
17. Dhein S, Muller A, Gerwin R, Klaus W. Comparative study on the proarrhythmiceffects of some antiarrhythmic agents. Circulation 1993;87:617–630.
18. Yakaitis RW, Ewy GA, Otto CW, Taren DL, Moon TE. Influence of time and ther-apy on ventricular defibrillation in dogs. Crit Care Med 1980;8:157–163.
19. Niemann JT, Haynes KS, Garner E, Rennie CJ, Jagels G, Stormo O. Postcounter-shock pulseless rhythms: response to CPR, artificial cardiac pacing, and adrenergicagonists. Ann Emerg Med 1986;15:112–120.
20. Sanders AB, Ewy GA, Taft TV. Prognostic and therapeutic importance of the aor-tic diastolic pressure in resuscitation from cardiac arrest. Crit Care Med 1984;12:871–873.
21. Reynolds JC, Salcido DD, Menegazzi JJ. Coronary perfusion pressure and return ofspontaneous circulation after prolonged cardiac arrest. Prehosp Emerg Care 2010;14:78–84.
22. Kern KB, Ewy GA, Voorhees WD, Babbs CF, Tacker WA. Myocardial perfusionpressure: a predictor of 24-hour survival during prolonged cardiac arrest indogs. Resuscitation 1988;16:241–250.
23. Paradis NA, Martin GB, Rivers EP, Goetting MG, Appleton TJ, Feingold M,Nowak RM. Coronary perfusion pressure and the return of spontaneous circula-tion in human cardiopulmonary resuscitation. JAMA 1990;263:1106–1113.
24. Vanden Hoek TL, Shao ZH, Li CQ. Do we reperfuse or cool down first to resus-citate ischemic tissue? Circulation 2000;102:A2765.
25. Gordon E. Special report cardiocerebral resuscitation. The new cardiopulmonaryresuscitation. Circulation 2005;111:2134–2142.
26. Valenzuela TD, Roe DJ, Cretin S, Spaite DW, Larsen MP. Estimating effectivenessof cardiac arrest interventions: a logistic regression survival model. Circulation1997;96:3308–3313.
27. Hasselqvist-Ax I1, Riva G, Herlitz J, Rosenqvist M, Hollenberg J, Nordberg P,Ringh M, Jonsson M, Axelsson C, Lindqvist J, Karlsson T, Svensson L. Early cardio-pulmonary resuscitation in out-of-hospital cardiac arrest. N Engl J Med 2015;372:2307–2315.
28. Cummins RO, Eisenberg MS, Hallstrom AP, Litwin PE. Survival of out-of-hospitalcardiac arrest with early initiation of cardiopulmonary resuscitation. Am J EmergMed 1985;3:114–119.
29. Olasveengen TM, Sunde K, Brunborg C, Thowsen J, Steen PA, Wik L. Intravenousdrug administration during out-of-hospital cardiac arrest: a randomized trial. JAMA2009;302:2222–2229.
30. Ong ME, Tan EH, Ng FS, Panchalingham A, Lim SH, Manning PG, Ong VY, Lim SH,Yap S, Tham LP, Ng KS, Venkataraman A; Cardiac Arrest and ResuscitationEpidemiology Study Group. Survival outcomes with the introduction of intraven-ous epinephrine in the management of out-of-hospital cardiac arrest. Ann EmergMed 2007;50:635–642.
31. Stiell IG, Wells GA, Field B, Spaite DW, Nesbitt LP, De Maio VJ, Nichol G,Cousineau D, Blackburn J, Munkley D, Luinstra-Toohey L, Campeau T,Dagnone E, Lyver M. Advanced cardiac life support in out-of-hospital cardiacarrest. N Engl J Med 2004;351:647–656.
32. Ahlquist RP. A study of the adrenotropic receptors. Am J Physiol 1948;153:586–600.
33. Redding JS, Pearson JW. Evaluation of drugs for cardiac resuscitation. Anesthesi-ology 1963;24:203–207.
34. Pearson JW, Redding JS. Peripheral vascular tone on cardiac resuscitation. AnesthAnalg 1965;44:746–752.
35. Tang W, Weil MH, Gazmuri RJ, Sun S, Duggal C, Bisera J. Pulmonary ventilation/perfusion defects induced by epinephrine during cardiopulmonary resuscitation.Circulation 1991;84:2101–2107.
36. Ditchey RV, Lindenfeld J. Failure of epinephrine to improve the balance betweenmyocardial oxygen supply and demand during closed-chest resuscitation in dogs.Circulation 1988;78:382–389.
37. Ristagno G, Tang W, Huang L, Fymat A, Chang YT, Sun S, Castillo C, Weil MH.Epinephrine reduces cerebral perfusion during cardiopulmonary resuscitation.Crit Care Med 2009;37:1408–1415.
38. Yakaitis RW, Otto CW, Blitt CD. Relative importance of alpha and beta adrener-gic receptors during resuscitation. Crit Care Med 1979;7:293–296.
39. Tang W, Weil MH, Sun S, Noc M, Yang L, Gazmuri RJ. Epinephrine increases theseverity of postresuscitation myocardial dysfunction. Circulation 1995;92:3089–3093.
40. Ristagno G, Sun S, Tang W, Castillo C, Weil MH. Effects of epinephrine and vaso-pressin on cerebral microcirculatory flows during and after cardiopulmonary re-suscitation. Crit Care Med 2007;35:2145–2149.
41. McCaul CL, McNamara PJ, Engelberts D, Wilson GJ, Romaschin A, Redington AN,Kavanagh BP. Epinephrine increases mortality after brief asphyxial cardiac arrest inan in vivo rat model. Anesth Analg 2006;102:542–548.
42. Ditchey RV, Rubio-Perez A, Slinker BK. Beta-adrenergic blockade reduces myo-cardial injury during experimental cardiopulmonary resuscitation. J Am Coll Cardiol1994;24:804–812.
43. Zhang Q, Li C. Combination of epinephrine with esmolol attenuates post-resuscitation myocardial dysfunction in a porcine model of cardiac arrest. PLoSONE 2013;8:e82677.
44. Chase PB, Kern KB, Sanders AB, Otto CW, Ewy GA. Effects of graded doses ofepinephrine on both noninvasive and invasive measures of myocardial perfusionand blood flow during cardiopulmonary resuscitation. Crit Care Med 1993;21:413–419.
45. Berg RA, Otto CW, Kern KB, Hilwig RW, Sanders AB, Henry CP, Ewy GA.A randomized, blinded trial of high-dose epinephrine vs. standard-dose epineph-rine in a swine model of pediatric asphyxial cardiac arrest. Crit Care Med 1996;24:1695–1700.
46. Hoekstra JW, Griffith R, Kelley R, Cody RJ, Lewis D, Scheatzle M, Brown CG.Effect of standard-dose vs. high-dose epinephrine on myocardial high-energyphosphates during ventricular fibrillation and closed-chest CPR. Ann Emerg Med1993;22:1385–1391.
47. Han J, de Jalon G, Moe GK. Adrenergic effects on ventricular vulnerability. Circ Res1964;14:516–524.
48. Taggart P, Sutton P, Chalabi Z, Boyett MR, Simon R, Elliott D, Gill JS. Effect ofadrenergic stimulation on action potential duration restitution in humans. Circula-tion 2003;107:285–289.
49. Suddath WO, Deychak Y, Varghese PJ. Electrophysiologic basis by which epineph-rine facilitates defibrillation after prolonged episodes of ventricular fibrillation.Ann Emerg Med 2001;38:201–206.
50. Neset A, Nordseth T, Kramer-Johansen J, Wik L, Olasveengen TM. Effects ofadrenaline on rhythm transitions in out-of-hospital cardiac arrest. Acta Anaesthe-siol Scand 2013;57:1260–1267.
51. Stiell IG, Hebert PC, Weitzman BN, Wells GA, Raman S, Stark RM, Higginson LA,Ahuja J, Dickinson GE. High-dose epinephrine in adult cardiac arrest. N Engl J Med1992;327:1045–1050.
52. Lipman J, Wilson W, Kobilski S, Scribante J, Lee C, Kraus P, Cooper J, Barr J,Moyes D. High-dose adrenaline in adult in-hospital asystolic cardiopulmonary re-suscitation: a double-blind randomised trial. Anaesth Intensive Care 1993;21:192–196.
53. Goetting MG, Paradis NA. High-dose epinephrine improves outcome from pedi-atric cardiac arrest. Ann Emerg Med 1991;20:22–26.
54. Lindner KH, Ahnefeld FW, Prengel AW. Comparison of standard and high-doseadrenaline in the resuscitation of asystole and electromechanical dissociation. ActaAnaesthesiol Scand 1991;35:253–256.
55. Callaham M, Madsen CD, Barton CW, Saunders CE, Pointer J. A randomized clin-ical trial of high-dose epinephrine and norepinephrine vs standard-dose epineph-rine in prehospital cardiac arrest. JAMA 1992;268:2667–2672.
56. Gueugniaud PY, Mols P, Goldstein P, Pham E, Dubien PY, Deweerdt C,Vergnion M, Petit P, Carli P. A comparison of repeated high doses and repeatedstandard doses of epinephrine for cardiac arrest outside the hospital. EuropeanEpinephrine Study Group. N Engl J Med 1998;339:1595–1601.
57. Brown CG, Martin DR, Pepe PE, Stueven H, Cummins RO, Gonzalez E,Vergnion M, Petit P, Carli P. A comparison of standard-dose and high-doseepinephrine in cardiac arrest outside the hospital. The Multicenter High-DoseEpinephrine Study Group. N Engl J Med 1992;327:1051–1055.
58. Carvolth RD, Hamilton AJ. Comparison of high-dose epinephrine versusstandard-dose epinephrine in adult cardiac arrest in the prehospital setting. Pre-hosp Disaster Med 1996;11:219–222.
59. Choux C, Gueugniaud PY, Barbieux A, Pham E, Lae C, Dubien PY, Petit P. Stand-ard doses versus repeated high doses of epinephrine in cardiac arrest outside thehospital. Resuscitation 1995;29:3–9.
60. Patterson MD, Boenning DA, Klein BL, Fuchs S, Smith KM, Hegenbarth MA,Carlson DW, Krug SE, Harris EM. The use of high-dose epinephrine for patientswith out-of-hospital cardiopulmonary arrest refractory to prehospital interven-tions. Pediatr Emerg Care 2005;21:227–237.
61. Sherman BW, Munger MA, Foulke GE, Rutherford WF, Panacek EA. High-doseversus standard-dose epinephrine treatment of cardiac arrest after failure ofstandard therapy. Pharmacotherapy 1997;17:242–247.
62. Perondi MB, Reis AG, Paiva EF, Nadkarni VM, Berg RA. A comparison of high-doseand standard-dose epinephrine in children with cardiac arrest. N Engl J Med 2004;350:1722–1730.
63. Polglase RF, Parish DC, Camp B. Prehospital administration of high-dose epineph-rine. Am J Emerg Med 1994;12:688–689.
64. Woodhouse SP, Cox S, Boyd P, Case C, Weber M. High dose and standard doseadrenaline do not alter survival, compared with placebo, in cardiac arrest. Resus-citation 1995;30:243–249.
Drug therapy in cardiac arrest 71
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

65. Jacobs IG, Finn JC, Jelinek GA, Oxer HF, Thompson PL. Effect of adrenaline onsurvival in out-of-hospital cardiac arrest: a randomised double-blind placebo-controlled trial. Resuscitation 2011;82:1138–1143.
66. Callaham M, Barton CW, Kayser S. Potential complications of high-dose epineph-rine therapy in patients resuscitated from cardiac arrest. JAMA 1991;265:1117–1122.
67. Martens PR, Mullie A. The availability of 10 mg epinephrine vials for cardiac arrest:a retrospective analysis. The Belgian Cerebral Resuscitation Study Group. Resus-citation 1991;22:219–228.
68. Dieckmann RA, Vardis R. High-dose epinephrine in pediatric out-of-hospital car-diopulmonary arrest. Pediatrics 1995;95:901–913.
69. Herlitz J, Ekstrom L, Wennerblom B, Axelsson A, Bang A, Holmberg S. Adrenalinein out-of-hospital ventricular fibrillation. Does it make any difference? Resuscitation1995;29:195–201.
70. Behringer W, Kittler H, Sterz F, Domanovits H, Schoerkhuber W, Holzer M,Mullner M, Laggner AN. Cumulative epinephrine dose during cardiopulmonaryresuscitation and neurologic outcome. Ann Intern Med 1998;129:450–456.
71. Holmberg M, Holmberg S, Herlitz J. Low chance of survival among patients requir-ing adrenaline (epinephrine) or intubation after out-of-hospital cardiac arrest inSweden. Resuscitation 2002;54:37–45.
72. Arrich J, Sterz F, Herkner H, Testori C, Behringer W. Total epinephrine dose dur-ing asystole and pulseless electrical activity cardiac arrests is associated with un-favourable functional outcome and increased in-hospital mortality. Resuscitation2012;83:333–337.
73. Hagihara A, Hasegawa M, Abe T, Nagata T, Wakata Y, Miyazaki S. Prehospital epi-nephrine use and survival among patients with out-of-hospital cardiac arrest.JAMA 2012;307:1161–1168.
74. Machida M, Miura S, Matsuo K, Ishikura H, Saku K. Effect of intravenous adrenalinebefore arrival at the hospital in out-of-hospital cardiac arrest. J Cardiol 2012;60:503–507.
75. Nakahara S, Tomio J, Nishida M, Morimura N, Ichikawa M, Sakamoto T. Associ-ation between timing of epinephrine administration and intact neurologic survivalfollowing out-of-hospital cardiac arrest in Japan: a population-based prospectiveobservational study. Acad Emerg Med 2012;19:782–792.
76. Cantrell CL Jr, Hubble MW, Richards ME. Impact of delayed and infrequent ad-ministration of vasopressors on return of spontaneous circulation duringout-of-hospital cardiac arrest. Prehosp Emerg Care 2013;17:15–22.
77. Goto Y, Maeda T, Goto Y. Effects of prehospital epinephrine duringout-of-hospital cardiac arrest with initial non-shockable rhythm: an observationalcohort study. Crit Care 2013;17:R188.
78. Hayakawa M, Gando S, Mizuno H, Asai Y, Shichinohe Y, Takahashi I, Makise H.Effects of epinephrine administration in out-of-hospital cardiac arrest based ona propensity analysis. J Intensive Care 2013;1:12.
79. Koscik C, Pinawin A, McGovern H, Allen D, Media DE, Ferguson T, Hopkins W,Sawyer KN, Boura J, Swor R. Rapid epinephrine administration improves earlyoutcomes in out-of-hospital cardiac arrest. Resuscitation 2013;84:915–920.
80. Nakahara S, Tomio J, Takahashi H, Ichikawa M, Nishida M, Morimura N,Sakamoto T. Evaluation of pre-hospital administration of adrenaline (epinephrine)by emergency medical services for patients with out of hospital cardiac arrest inJapan: controlled propensity matched retrospective cohort study. BMJ 2013;347:f6829.
81. Donnino MW, Salciccioli JD, Howell MD, Cocchi MN, Giberson B, Berg K,Gautam S, Callaway C. Time to administration of epinephrine and outcome afterin-hospital cardiac arrest with non-shockable rhythms: retrospective analysis oflarge in-hospital data registry. BMJ 2014;348:g3028.
82. Dumas F, Bougouin W, Geri G, Lamhaut L, Bougle A, Daviaud F, Morichau-Beauchant T, Rosencher J, Marijon E, Carli P, Jouven X, Rea TD, Cariou A. Is epi-nephrine during cardiac arrest associated with worse outcomes in resuscitatedpatients? J Am Coll Cardiol 2014;64:2360–2367.
83. Warren SA, Huszti E, Bradley SM, Chan PS, Bryson CL, Fitzpatrick AL, Nichol G.Adrenaline (epinephrine) dosing period and survival after in-hospital cardiac ar-rest: a retrospective review of prospectively collected data. Resuscitation 2014;85:350–358.
84. Goldsmith SR. Baroreceptor-mediated suppression of osmotically stimulatedvasopressin in normal humans. J Appl Physiol 1988;65:1226–1230.
85. Maturi MF, Martin SE, Markle D, Maxwell M, Burruss CR, Speir E, Greene R,Young MR, Vitale D, Green M, Goldstein S, Bacharach S, Patterson P. Coronaryvasoconstriction induced by vasopressin. Production of myocardial ischemia indogs by constriction of nondiseased small vessels. Circulation 1991;83:2111–2121.
86. den Ouden DT, Meinders AE. Vasopressin: physiology and clinical use in patientswith vasodilatory shock: a review. Neth J Med 2005;63:4–13.
87. Mulligan KA, McKnite SH, Lindner KH, Lindstrom PJ, Detloff B, Lurie KG. Syner-gistic effects of vasopressin plus epinephrine during cardiopulmonary resuscita-tion. Resuscitation 1997;35:265–271.
88. Lindner KH, Brinkmann A, Pfenninger EG, Lurie KG, Goertz A, Lindner IM. Effectof vasopressin on hemodynamic variables, organ blood flow, and acid-base statusin a pig model of cardiopulmonary resuscitation. Anesth Analg 1993;77:427–435.
89. Wenzel V, Lindner KH, Prengel AW, Maier C, Voelckel W, Lurie KG,Strohmenger HU. Vasopressin improves vital organ blood flow after prolongedcardiac arrest with postcountershock pulseless electrical activity in pigs. CritCare Med 1999;27:486–492.
90. Babar SI, Berg RA, Hilwig RW, Kern KB, Ewy GA. Vasopressin vs. epinephrine dur-ing cardiopulmonary resuscitation: a randomized swine outcome study. Resuscita-tion 1999;41:185–192.
91. Prengel AW, Lindner KH, Keller A. Cerebral oxygenation during cardiopulmonaryresuscitation with epinephrine and vasopressin in pigs. Stroke 1996;27:1241–1248.
92. Fox AW, May RE, Mitch WE. Comparison of peptide and nonpeptide receptor-mediated responses in rat tail artery. J Cardiovasc Pharmacol 1992;20:282–289.
93. Currigan DA, Hughes RJ, Wright CE, Angus JA, Soeding PF. Vasoconstrictor re-sponses to vasopressor agents in human pulmonary and radial arteries: an in vitrostudy. Anesthesiology 2014;121:930–936.
94. Wenzel V, Lindner KH, Krismer AC. Repeated administration of vasopressin butnot epinephrine maintains coronary perfusion pressure after early and late admin-istration during prolonged cardiopulmonary resuscitation in pigs. Circulation 1999;99:1379–1384.
95. Kornberger E, Prengel AW, Krismer A, Schwarz B, Wenzel V, Lindner KH, Mair P.Vasopressin-mediated adrenocorticotropin release increases plasma cortisolconcentrations during cardiopulmonary resuscitation. Crit Care Med 2000;28:3517–3521.
96. Ullian ME. The role of corticosteriods in the regulation of vascular tone. CardiovascRes 1999;41:55–64.
97. Lindner KH, Strohmenger HU, Ensinger H, Hetzel WD, Ahnefeld FW,Georgieff M. Stress hormone response during and after cardiopulmonary resus-citation. Anesthesiology 1992;77:662–668.
98. Lindner KH, Dirks B, Strohmenger HU, Prengel AW, Lindner IM, Lurie KG. Ran-domised comparison of epinephrine and vasopressin in patients without-of-hospital ventricular fibrillation. Lancet 1997;349:535–537.
99. Stiell IG, Hebert PC, Wells GA, Vandemheen KL, Tang AS, Higginson LA,Dreyer JF, Clement C, Battram E, Watpool I, Mason S, Klassen T,Weitzman BN. Vasopressin vs. epinephrine for inhospital cardiac arrest: a rando-mised controlled trial. Lancet 2001;358:105–109.
100. Callaway CW, Hostler D, Doshi AA, Pinchalk M, Roth RN, Lubin J, Newman DH,Kelly LJ. Usefulness of vasopressin administered with epinephrine duringout-of-hospital cardiac arrest. Am J Cardiol 2006;98:1316–1321.
101. Mukoyama T, Kinoshita K, Nagao K, Tanjoh K. Reduced effectiveness of vasopres-sin in repeated doses for patients undergoing prolonged cardiopulmonary resus-citation. Resuscitation 2009;80:755–761.
102. Wenzel V, Krismer AC, Arntz HR, Sitter H, Stadlbauer KH, Lindner KH. A com-parison of vasopressin and epinephrine for out-of-hospital cardiopulmonaryresuscitation. N Engl J Med 2004;350:105–113.
103. Gueugniaud PY, David JS, Chanzy E, Hubert H, Dubien PY, Mauriaucourt P,Braganca C, Billeres X, Clotteau-Lambert MP, Fuster P, Thiercelin D,Debaty G, Ricard-Hibon A, Roux P, Espesson C, Querellou E, Ducros L,Ecollan P, Halbout L, Savary D, Guillaumee F, Maupoint R, Capelle P, Bracq C,Dreyfus P, Nouguier P, Gache A, Meurisse C, Boulanger B, Lae C, Metzger J,Raphael V, Beruben A, Wenzel V, Guinhouya C, Vilhelm C, Marret E. Vasopressinand epinephrine vs. epinephrine alone in cardiopulmonary resuscitation. N Engl JMed 2008;359:21–30.
104. Ong ME, Tiah L, Leong BS, Tan EC, Ong VY, Tan EA, Poh BY, Pek PP, Chen Y.A randomised, double-blind, multi-centre trial comparing vasopressin and adren-aline in patients with cardiac arrest presenting to or in the emergency department.Resuscitation 2012;83:953–960.
105. Mentzelopoulos SD, Zakynthinos SG, Tzoufi M. Vasopressin, epinephrine, andcorticosteroids for in-hospital cardiac arrest. Arch Intern Med 2009;169:15–24.
106. Mentzelopoulos SD, Malachias S, Chamos C. Vasopressin, steroids, and epineph-rine and neurologically favorable survival after in-hospital cardiac arrest: a rando-mized clinical trial. JAMA 2013;310:270–279.
107. Carroll TG, Dimas VV, Raymond TT. Vasopressin rescue for in-pediatric intensivecare unit cardiopulmonary arrest refractory to initial epinephrine dosing: a pro-spective feasibility pilot trial. Pediatr Crit Care Med 2012;13:265–272.
108. Grmec S, Mally S. Vasopressin improves outcome in out-of-hospital cardiopul-monary resuscitation of ventricular fibrillation and pulseless ventricular tachycar-dia: a observational cohort study. Crit Care 2006;10:R13.
109. Guyette FX, Guimond GE, Hostler D. Vasopressin administered with epinephrineis associated with a return of a pulse in out-of-hospital cardiac arrest. Resuscitation2004;63:277–282.
A. Lundin et al.72
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

110. Duncan JM, Meaney P, Simpson P. Vasopressin for in-hospital pediatric cardiac ar-rest: results from the American Heart Association National Registry of Cardiopul-monary Resuscitation. Pediatr Crit Care Med 2009;10:191–195.
111. Turner DW, Attridge RL, Hughes DW. Vasopressin associated with an increase inreturn of spontaneous circulation in acidotic cardiopulmonary arrest patients. AnnPharmacother 2014;48:986–991.
112. Mills JC, Moyer JH. Methoxamine; effect on blood pressure and renal hemo-dynamics. Am J Med Sci 1957;233:409–417.
113. Livesay JJ, Follette DM, Fey KH, Nelson RL, DeLand EC, Barnard RJ, Buckberg GD.Optimizing myocardial supply/demand balance with alpha-adrenergic drugs dur-ing cardiopulmonary resuscitation. J Thorac Cardiovasc Surg 1978;76:244–251.
114. Roberts D, Landolfo K, Dobson K, Light RB. The effects of methoxamine and epi-nephrine on survival and regional distribution of cardiac output in dogs with pro-longed ventricular fibrillation. Chest 1990;98:999–1005.
115. Patrick WD, Freedman J, McEwen T, Light RB, Ludwig L, Roberts D. A rando-mized, double-blind comparison of methoxamine and epinephrine in human car-diopulmonary arrest. Am J Respir Crit Care Med 1995;152:519–523.
116. Guzman SV, Deleon AC Jr, West JW, Bellet S. Cardiac effects of isoproterenol,norepinephrine and epinephrine in complete A-V heart block during experimen-tal acidosis and hyperkalemia. Circ Res 1959;7:666–672.
117. von Planta I, Wagner O, von Planta M, Scheidegger D. Coronary perfusion pres-sure, end-tidal CO2 and adrenergic agents in haemodynamic stable rats. Resuscita-tion 1993;25:203–217.
118. Jaffe R, Rubinshtein R, Feigenberg Z, Talor E, Michaelson M, Karkabi B, Halon DA,Flugelman MY, Lewis BS. Evaluation of isoproterenol in patients undergoing resus-citation for out-of-hospital asystolic cardiac arrest (the Israel Resuscitation withIsoproterenol Study Prospective Randomized Clinical Trial). Am J Cardiol 2004;93:1407–1409.
119. Roden DM. Antiarrhythmic drugs: from mechanisms to clinical practice. Heart2000;84:339–346.
120. Myerburg RJ, Castellanos A. Therapy for cardiac arrhythmias. In Bonow RO, ed.Braunwalds Heart Disease: A Textbook of Cardiovascular Medicine. 9th ed. Philadel-phia: Elsevier Saunders; 2012. p. 710.
121. Van Herendael H, Dorian P. Amiodarone for the treatment and prevention ofventricular fibrillation and ventricular tachycardia. Vasc Health Risk Manag 2010;6:465–472.
122. Kudenchuk PJ, Cobb LA, Copass MK, Cummins RO, Doherty AM,Fahrenbruch CE et al. Amiodarone for resuscitation after out-of-hospital cardiacarrest due to ventricular fibrillation. N Engl J Med 1999;341:871–878.
123. Dorian P, Cass D, Schwartz B, Cooper R, Gelaznikas R, Barr A. Amiodarone ascompared with lidocaine for shock-resistant ventricular fibrillation. N Engl JMed 2002;346:884–890.
124. Pollak PT, Wee V, Al-Hazmi A, Martin J, Zarnke KB. The use of amiodarone forin-hospital cardiac arrest at two tertiary care centres. Can J Cardiol 2006;22:199–202.
125. Rea RS, Kane-Gill SL, Rudis MI, Seybert AL, Oyen LJ, Ou NN, Stauss JL, Kirisci L,Idrees U, Henderson SO. Comparing intravenous amiodarone or lidocaine, orboth, outcomes for inpatients with pulseless ventricular arrhythmias. Crit CareMed 2006;34:1617–1623.
126. Valdes SO, Donoghue AJ, Hoyme DB, Hammond R, Berg MD, Berg RA,Samson RA. Outcomes associated with amiodarone and lidocaine in the treat-ment of in-hospital pediatric cardiac arrest with pulseless ventricular tachycardiaor ventricular fibrillation. Resuscitation 2014;85:381–386.
127. Amino M, Yoshioka K, Opthof T, Morita S, Uemura S, Tamura K, Fukushima T,Higami S, Otsuka H, Akieda K, Shima M, Fujibayashi D, Hashida T, Inokuchi S,Kodama I, Tanabe T. Comparative study of nifekalant vs. amiodarone for shock-resistant ventricular fibrillation in out-of-hospital cardiopulmonary arrest pa-tients. J Cardiovasc Pharmacol 2010;55:391–398.
128. Harayama N, Nihei S, Nagata K, Isa Y, Goto K, Aibara K, Kamochi M, Sata T.Comparison of nifekalant and amiodarone for resuscitation of out-of-hospitalcardiopulmonary arrest resulting from shock-resistant ventricular fibrillation.J Anesth 2014;28:587–592.
129. Tahara Y, Kimura K, Kosuge M, Ebina T, Sumita S, Hibi K, Toyama H, Kosuge T,Moriwaki Y, Suzuki N, Sugiyama M, Umemura S. Comparison of nifekalant andlidocaine for the treatment of shock-refractory ventricular fibrillation. Circ J2006;70:442–446.
130. Weaver WD, Fahrenbruch CE, Johnson DD, Hallstrom AP, Cobb LA, Copass MK.Effect of epinephrine and lidocaine therapy on outcome after cardiac arrest due toventricular fibrillation. Circulation 1990;82:2027–2034.
131. Kovoor P, Love A, Hall J, Kruit R, Sadick N, Ho D, Adelstein BA, Ross DL. Rando-mized double-blind trial of sotalol vs. lignocaine in out-of-hospital refractory car-diac arrest due to ventricular tachyarrhythmia. Intern Med J 2005;35:518–525.
132. Herlitz J1, Ekstrom L, Wennerblom B, Axelsson A, Bang A, Lindkvist J,Persson NG, Holmberg S. Lidocaine in out-of-hospital ventricular fibrillation.Does it improve survival? Resuscitation 1997;33:199–205.
133. Gorgels AP, van den Dool A, Hofs A, Mulleneers R, Smeets JL, Vos MA,Wellens HJ. Comparison of procainamide and lidocaine in terminating sustainedmonomorphic ventricular tachycardia. Am J Cardiol 1996;78:43–46.
134. Stiell IG, Wells GA, Hebert PC, Laupacis A, Weitzman BN. Association of drugtherapy with survival in cardiac arrest: limited role of advanced cardiac life supportdrugs. Acad Emerg Med 1995;2:264–273.
135. Markel DT, Gold LS, Allen J, Fahrenbruch CE, Rea TD, Eisenberg MS,Kudenchuk PJ. Procainamide and survival in ventricular fibrillation out-of-hospitalcardiac arrest. Acad Emerg Med 2010;17:617–623.
136. Morton HJ, Thomas ET. Effect of atropine on the heart-rate. Lancet 1958;2:1313–1315.
137. Brown DC, Lewis AJ, Criley JM. Asystole and its treatment: the possible role of theparasympathetic nervous system in cardiac arrest. JACEP 1979;8:448–452.
138. Blecic S, Chaskis C, Vincent JL. Atropine administration in experimental electro-mechanical dissociation. Am J Emerg Med 1992;10:515–518.
139. DeBehnke DJ, Swart GL, Spreng D, Aufderheide TP. Standard and higher doses ofatropine in a canine model of pulseless electrical activity. Acad Emerg Med 1995;2:1034–1041.
140. Nagao K, Yagi T, Sakamoto T, Koseki K, Igarashi M, Ishimatsu S, Sato A, Hori S,Kanesaka S, Hamabe Y, Saito D, Kitamura S, Nonaka A, Katsumi A, Sakurai A,Suzuki H, Imai H, Miyauchi H, Suga H, Tomioka J, Imai K, Kiyota K, Arima K,Takuhiro K, Matsuda K, Takahashi K, Naito M, Yagi M, Honma M, Sasaki M,Suzuki M, Nakano M, Fugiyoshi N, Kozima N, Harada N, Ohashi N, Suzuki N,Moriwaki R, Takahashi R, Kikuchi S, Noda S, Oda S, Imaki S, Fugikawa T,Kikuno T, Kamohara T, Suda T, Ishii T, Irabu T, Sadahiro T, Ikeda T, Tanaka T,Obayashi T, Ogawa T, Miyahara Y, Nakagawa Y, Tokuyasu Y, Tawara Y, Haga Y,Minowa Y, Tanaka Y, Sasaki Z, Fudouzi Z. Atropine sulfate for patients without-of-hospital cardiac arrest due to asystole and pulseless electrical activity.Circ J 2011;75:580–588.
141. Rutherford JD, Vatner SF, Braunwald E. Effects and mechanism of action of ami-nophylline on cardiac function and regional blood flow distribution in consciousdogs. Circulation 1981;63:378–387.
142. Stark U, Brodmann M, Lueger A, Stark G. Antiarrhythmic effects of adenosine onischemia-induced ventricular fibrillation. J Crit Care 2001;16:8–16.
143. Littmann L, Ashline PT, Hayes WJ, Kempler P, Raymond RM, Norton HJ,Svenson RH, Tuntelder JR, Tatsis GP. Aminophylline fails to improve theoutcome of cardiopulmonary resuscitation from prolonged ventricular fibrilla-tion: a placebo-controlled, randomized, blinded experimental study. J Am CollCardiol 1994;23:1708–1714.
144. Burton JH, Mass M, Menegazzi JJ, Yealy DM. Aminophylline as an adjunct to stand-ard advanced cardiac life support in prolonged cardiac arrest. Ann Emerg Med1997;30:154–158.
145. Mader TJ, Smithline HA, Gibson P. Aminophylline in undifferentiatedout-of-hospital asystolic cardiac arrest. Resuscitation 1999;41:39–45.
146. Mader TJ, Smithline HA, Durkin L, Scriver G. A randomized controlled trial ofintravenous aminophylline for atropine-resistant out-of-hospital asystolic cardiacarrest. Acad Emerg Med 2003;10:192–197.
147. Abu-Laban RB, McIntyre CM, Christenson JM, van Beek CA, Innes GD,O’Brien RK, Wanger KP, McKnight RD, Gin KG, Zed PJ, Watts J, Puskaric J,MacPhail IA, Berringer RG, Milner RA. Aminophylline in bradyasystolic cardiacarrest: a randomised placebo-controlled trial. Lancet 2006;367:1577–1584.
148. Ji XF, Li CS, Wang S, Yang L, Cong LH. Comparison of the efficacy of nifekalant andamiodarone in a porcine model of cardiac arrest. Resuscitation 2010;81:1031–1036.
149. Yoshioka K, Amino M, Morita S, Nakagawa Y, Usui K, Sugimoto A, Matsuzaki A,Deguchi Y, Yamamoto I, Inokuchi S, Ikari Y, Kodama I, Tanabe T. Can nifekalanthydrochloride be used as a first-line drug for cardiopulmonary arrest (CPA)?Comparative study of out-of-hospital CPA with acidosis and in-hospital CPA with-out acidosis. Circ J 2006;70:21–27.
150. Brophy JM, Joseph L, Rouleau JL. Beta-blockers in congestive heart failure. ABayesian meta-analysis. Ann Intern Med 2001;134:550.
151. Ryden L, Ariniego R, Arnman K, Herlitz J, Hjalmarson A, Holmberg S, Reyes C,Smedgard P, Svedberg K, Vedin A, Waagstein F, Waldenstrom A,Wilhelmsson C, Wedel H, Yamamoto M. A double-blind trial of metoprolol inacute myocardial infarction. Effects on ventricular tachyarrhythmias. N Engl JMed 1983;308:614–618.
152. Hayashi M, Denjoy I, Extramiana F, Maltret A, Buisson NR, Lupoglazoff JM, Klug D,Hayashi M, Takatsuki S, Villain E, Kamblock J, Messali A, Guicheney P, Lunardi J,Leenhardt A. Incidence and risk factors of arrhythmic events in catecholaminergicpolymorphic ventricular tachycardia. Circulation 2009;119:2426–2434.
153. Theochari E, Xanthos T, Papadimitriou D, Demestiha T, Condilis N,Tsirikos-Karapanos N, Kamochi M, Sata T. Selective beta blockade improvesthe outcome of cardiopulmonary resuscitation in a swine model of cardiac arrest.Ann Ital Chir 2008;79:409–414.
Drug therapy in cardiac arrest 73
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

154. Huang L, Weil MH, Cammarata G, Sun S, Tang W. Nonselective beta-blockingagent improves the outcome of cardiopulmonary resuscitation in a rat model.Crit Care Med 2004;32(9 Suppl):S378–S380.
155. Wang J, Weil MH, Tang W, Sun S, Huang L. Levosimendan improves postresusci-tation myocardial dysfunction after beta-adrenergic blockade. J Lab Clin Med 2005;146:179–183.
156. Nademanee K, Taylor R, Bailey WE. Treating electrical storm: sympathetic block-ade vs. advanced cardiac life support-guided therapy. Circulation 2000;102:742–747.
157. Driver BE, Debaty G, Plummer DW, Smith SW. Use of esmolol after failure ofstandard cardiopulmonary resuscitation to treat patients with refractory ventricu-lar fibrillation. Resuscitation 2014;85:1337–1341.
158. Fawcett WJ, Haxby EJ, Male DA. Magnesium: physiology and pharmacology. Br JAnaesth 1999;83:302–320.
159. Brown CG, Griffith RF, Neely D, Hobson J, Miller B. The effect of intravenousmagnesium administration on aortic, right atrial and coronary perfusion pressuresduring CPR in swine. Resuscitation 1993;26:3–12.
160. DiCarlo LA Jr, Morady F, de Buitleir M, Krol RB, Schurig L, Annesley TM. Effects ofmagnesium sulfate on cardiac conduction and refractoriness in humans. J Am CollCardiol 1986;7:1356–1362.
161. Ghani MF, Rabah M. Effect of magnesium chloride on electrical stability of theheart. Am Heart J 1977;94:600–602.
162. Keller PK, Aronson RS. The role of magnesium in cardiac arrhythmias. Prog Cardi-ovasc Dis 1990;32:433–448.
163. Thomas SH, Behr ER. Pharmacological treatment of acquired QT prolongationand torsades de pointes. Br J Clin Pharmacol 2015; doi:10.1111/bcp.12726.
164. Miller B, Craddock L, Hoffenberg S, Heinz S, Lefkowitz D, Callender ML,Battaglia C, Maines C, Masick D. Pilot study of intravenous magnesium sulfatein refractory cardiac arrest: safety data and recommendations for future studies.Resuscitation 1995;30:3–14.
165. Allegra J, Lavery R, Cody R, Birnbaum G, Brennan J, Hartman A, Horowitz M,Nashed A, Yablonski M. Magnesium sulfate in the treatment of refractory ven-tricular fibrillation in the prehospital setting. Resuscitation 2001;49:245–249.
166. Hassan TB, Jagger C, Barnett DB. A randomised trial to investigate the efficacy ofmagnesium sulphate for refractory ventricular fibrillation. Emerg Med J 2002;19:57–62.
167. Thel MC, Armstrong AL, McNulty SE, Califf RM, O’Connor CM. Randomised trialof magnesium in in-hospital cardiac arrest. Duke Internal Medicine Housestaff.Lancet 1997;350:1272–1276.
168. Fatovich DM, Prentice DA, Dobb GJ. Magnesium in cardiac arrest (the magic trial).Resuscitation 1997;35:237–241.
169. Chen F, Lin Q, Chen G. Does intravenous magnesium benefit patients of cardiacarrest? A meta- analysis. Hong Kong J Emerg Med 2012;19:103–109.
170. Marshall RS. Progress in intravenous thrombolytic therapy for acute stroke. JAMANeurol 2015;72:928–934.
171. Solhpour A, Yusuf SW. Fibrinolytic therapy in patients with ST-elevation myocar-dial infarction. Expert Rev Cardiovasc Ther 2014;12:201–215.
172. Marti C, John G. Systemic thrombolytic therapy for acute pulmonary embolism: asystematic review and meta-analysis. Eur Heart J 2015;36:605–614.
173. Fischer M, Bottiger BW, Popov-Cenic S, Hossmann KA. Thrombolysis using plas-minogen activator and heparin reduces cerebral no-reflow after resuscitationfrom cardiac arrest: an experimental study in the cat. Intensive Care Med 1996;22:1214–1223.
174. Bottiger BW, Bode C, Kern S, Gries A, Gust R, Glatzer R, Bauer H, Motsch J,Martin E. Efficacy and safety of thrombolytic therapy after initially unsuccessfulcardiopulmonary resuscitation: a prospective clinical trial. Lancet 2001;357:1583–1585.
175. Fatovich DM, Dobb GJ, Clugston RA. A pilot randomised trial of thrombolysis incardiac arrest (The TICA trial). Resuscitation 2004;61:309–313.
176. Abu-Laban RB, Christenson JM, Innes GD, van Beek CA, Wanger KP,McKnight RD, MacPhail IA, Puskaric J, Sadowski RP, Singer J, Schechter MT,Wood VM. Tissue plasminogen activator in cardiac arrest with pulseless electricalactivity. N Engl J Med 2002;346:1522–1528.
177. Bottiger BW, Arntz HR, Chamberlain DA, Bluhmki E, Belmans A, Danays T,Carli PA, Adgey JA, Bode C, Wenzel V, Chamberlain DA. Thrombolysis duringresuscitation for out-of-hospital cardiac arrest. N Engl J Med 2008;359:2651–2662.
178. Stadlbauer KH, Krismer AC, Arntz HR, Mayr VD, Lienhart HG, Bottiger BW,Jahn B, Lindner KH, Wenzel V. Effects of thrombolysis during out-of-hospital car-diopulmonary resuscitation. Am J Cardiol 2006;97:305–308.
179. Bozeman WP, Kleiner DM, Ferguson KL. Empiric Tenecteplase is associated withincreased return of spontaneous circulation and short term survival in cardiac ar-rest patients unresponsive to standard interventions. Resuscitation 2006;69:399–406.
180. Varvarousi G, Stefaniotou A, Varvaroussis D, Xanthos T. Glucocorticoids as anemerging pharmacologic agent for cardiopulmonary resuscitation. CardiovascDrugs Ther 2014;28:477–488.
181. Reis DJ. Potentiation of the vasoconstrictor action of topical norepinephrine onthe human bulbar conjuctival vessels after topical application of certain adreno-cortical hormones. J Clin Endocrinol Metab 1960;20:446–456.
182. Kadowitz PJ, Yard AC. Influence of hydrocortisone on cardiovascular responsesto epinephrine. Eur J Pharmacol 1971;13:281–286.
183. Smithline H, Rivers E, Appleton T, Nowak R. Corticosteroid supplementationduring cardiac arrest in rats. Resuscitation 1993;25:257–264.
184. Yard AC, Kadowitz PJ. Studies on the mechanism of hydrocortisone potentiationof vasoconstrictor responses to epinephrine in the anesthetized animal. Eur J Phar-macol 1972;20:19.
185. Tavakoli N, Bidari A, Shams Vahdati S. Serum cortisol levels as a predictor ofneurologic survival in successfully resuscitated victims of cardiopulmonary arrest.J Cardiovasc Thorac Res 2012;4:107–111.
186. Hekimian G, Baugnon T, Thuong M, Monchi M, Dabbane H, Jaby D, Rhaoui A,Laurent I, Moret G, Fraisse F, Adrie C. Cortisol levels and adrenal reserve aftersuccessful cardiac arrest resuscitation. Shock 2004;22:116–119.
187. Schultz CH, Rivers EP, Feldkamp CS, Goad EG, Smithline HA, Martin GB, Fath JJ,Wortsman J, Nowak RM. A characterization of hypothalamic-pituitary-adrenalaxis function during and after human cardiac arrest. Crit Care Med 1993;21:1339–1347.
188. Miller JB, Donnino MW, Rogan M, Goyal N. Relative adrenal insufficiency in post-cardiac arrest shock is under-recognized. Resuscitation 2008;76:221–225.
189. Kim JJ, Hyun SY, Hwang SY, Jung YB, Shin JH, Lim YS, Cho JS, Yang HJ, Lee G.Hormonal responses upon return of spontaneous circulation after cardiac arrest:a retrospective cohort study. Crit Care 2011;15:R53.
190. Tsai MS, Huang CH, Chang WT. The effect of hydrocortisone on the outcome ofout-of-hospital cardiac arrest patients: a pilot study. Am J Emerg Med 2007;25:318–325.
191. Nguyen AQ, Cherry BH, Scott GF, Ryou MG, Mallet RT. Erythropoietin: powerfulprotection of ischemic and post-ischemic brain. Exp Biol Med (Maywood) 2014;239:1461–1475.
192. Fisher JW. Erythropoietin: physiology and pharmacology update. Exp Biol Med2003;228:1–14.
193. Popp E, Vogel P, Teschendorf P, Bottiger BW. Effects of the application of erythro-poietin on cerebral recovery after cardiac arrest in rats. Resuscitation 2007;74:344–351.
194. Huang CH, Hsu CY, Chen HW, Tsai MS, Cheng HJ, Chang CH, Lee YT, Chen WJ.Erythropoietin improves the postresuscitation myocardial dysfunction and sur-vival in the asphyxia-induced cardiac arrest model. Shock 2007;28:53–58.
195. Borovnik-Lesjak V, Whitehouse K, Baetiong A, Artin B, Radhakrishnan J,Gazmuri RJ. High-dose erythropoietin during cardiac resuscitation lessens post-resuscitation myocardial stunning in swine. Transl Res 2013;162:110–121.
196. Vasileiou PV, Xanthos T, Barouxis D, Pantazopoulos C, Papalois AE, Lelovas P,Kotsilianou O, Pliatsika P, Kouskouni E, Iacovidou N. Erythropoietin administra-tion facilitates return of spontaneous circulation and improves survival in a pigmodel of cardiac arrest. Am J Emerg Med 2014;32:871–877.
197. Singh D, Kolarova JD, Wang S, Ayoub IM, Gazmuri RJ. Myocardial protection byerythropoietin during resuscitation from ventricular fibrillation. Am J Ther 2007;14:361–368.
198. Gazmuri RJ, Radhakrishnan J. Protecting mitochondrial bioenergetic function dur-ing resuscitation from cardiac arrest. Crit Care Clin 2012;28:245–270.
199. Grmec S, Strnad M, Kupnik D, Sinkovic A, Gazmuri RJ. Erythropoietin facilitatesthe return of spontaneous circulation and survival in victims of out-of-hospitalcardiac arrest. Resuscitation 2009;80:631–637.
200. Kraut JA, Madias NE. Metabolic acidosis: pathophysiology, diagnosis and manage-ment. Nat Rev Nephrol 2010;6:274–285.
201. Davies AO. Rapid desensitization and uncoupling of human beta-adrenergic re-ceptors in an in vitro model of lactic acidosis. J Clin Endocrinol Metab 1984;59:398–405.
202. Forsythe SM, Schmidt GA. Sodium bicarbonate for the treatment of lactic acid-osis. Chest 2000;117:260–267.
203. Langer T, Ferrari M, Zazzeron L. Effects of intravenous solutions on acid-baseequilibrium: from crystalloids to colloids and blood components. Anaesthesiol In-tensive Ther 2014;46:350–360.
204. Kette F, Weil MH, von Planta M, Gazmuri RJ, Rackow EC. Buffer agents do notreverse intramyocardial acidosis during cardiac resuscitation. Circulation 1990;81:1660–1666.
205. Federiuk CS, Sanders AB, Kern KB, Nelson J, Ewy GA. The effect of bicarbonateon resuscitation from cardiac arrest. Ann Emerg Med 1991;20:1173–1177.
206. Kette F, Weil MH, Gazmuri RJ. Buffer solutions may compromise cardiac resusci-tation by reducing coronary perfusion pressure. JAMA 1991;266:2121–2126.
A. Lundin et al.74
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from

207. Bleske BE, Rice TL, Warren EW. An alternative sodium bicarbonate regimen dur-ing cardiac arrest and cardiopulmonary resuscitation in a canine model. Pharmaco-therapy 1994;14:95–99.
208. Leong EC, Bendall JC, Boyd AC, Einstein R. Sodium bicarbonate improves thechance of resuscitation after 10 minutes of cardiac arrest in dogs. Resuscitation2001;51:309–315.
209. Vanden Hoek TL, Morrison LJ, Shuster M. Part 12: cardiac arrest in special situa-tions: 2010 American Heart Association Guidelines for Cardiopulmonary Resus-citation and Emergency Cardiovascular Care. Circulation 2010;122(18 Suppl 3):S829–S861.
210. Dybvik T, Strand T, Steen PA. Buffer therapy during out-of-hospital cardiopul-monary resuscitation. Resuscitation 1995;29:89–95.
211. Weng YM, Wu SH, Li WC, Kuo CW, Chen SY, Chen JC. The effects of sodiumbicarbonate during prolonged cardiopulmonary resuscitation. Am J Emerg Med2013;31:562–565.
212. Raymond TT, Zaritsky AL, Nadkarni V, Bembea M, Fink E, Gaies MG,Guerguerian AM, Parshuram C, Knight L, Kleinman M, Laussen PC, Schex-nayder SM, Sutton R, Topjian AA. Sodium bicarbonate use during in-hospital pedi-atric pulseless cardiac arrest—a report from the American Heart Association GetWith The Guidelines((R))-Resuscitation. Resuscitation 2015;89:106–113.
213. Breil M, Krep H, Sinn D, Hagendorff A, Dahmen A, Eichelkraut W, Hoeft A,Fischer M. Hypertonic saline improves myocardial blood flow during CPR, butis not enhanced further by the addition of hydroxy ethyl starch. Resuscitation2003;56:307–317.
214. Krep H, Breil M, Sinn D. Effects of hypertonic vs. isotonic infusion therapy onregional cerebral blood flow after experimental cardiac arrest cardiopulmonaryresuscitation in pigs. Resuscitation 2004;63:73–83.
215. Breil M, Krep H, Heister U, Bartsch A, Bender R, Schaefers B, Hoeft A, Fischer M.Randomised study of hypertonic saline infusion during resuscitation fromout-of-hospital cardiac arrest. Resuscitation 2012;83:347–352.
216. Hagihara A, Hasegawa M, Abe T, Wakata Y, Nagata T, Nabeshima Y. Prehospitallactated Ringer’s solution treatment and survival in out-of-hospital cardiac arrest:a prospective cohort analysis. PLoS Med 2013;10:e1001394.
217. Bakalos G, Mamali M, Komninos C, Koukou E, Tsantilas A, Tzima S, Rosenberg T.Advanced life support versus basic life support in the pre-hospital setting: ameta-analysis. Resuscitation 2011;82:1130–1137.
218. Larabee TM, Liu KY, Campbell JA. Vasopressors in cardiac arrest: a systematic re-view. Resuscitation 2012;83:932–939.
219. Ong ME, Pellis T, Link MS. The use of antiarrhythmic drugs for adult cardiac arrest:a systematic review. Resuscitation 2011;82:665–670.
220. de Oliveira FC, Feitosa-Filho GS, Ritt LE. Use of beta-blockers for the treatmentof cardiac arrest due to ventricular fibrillation/pulseless ventricular tachycardia: asystematic review. Resuscitation 2012;83:674–683.
221. Huang Y, He Q, Yang M, Zhan L. Antiarrhythmia drugs for cardiac arrest: a system-ic review and meta-analysis. Crit Care 2013;17:R173.
222. Hurley KF, Magee K, Green R. Aminophylline for bradyasystolic cardiac arrest inadults. Cochrane Database Syst Rev 2013;8:CD006781.
223. Lin S, Callaway CW, Shah PS, Wagner JD, Beyene J, Ziegler CP. Adrenaline forout-of-hospital cardiac arrest resuscitation: a systematic review and meta-analysisof randomized controlled trials. Resuscitation 2014;85:732–740.
224. Layek A, Maitra S, Pal S, Bhattacharjee S, Baidya DK. Efficacy of vasopressin duringcardio-pulmonary resuscitation in adult patients: a meta-analysis. Resuscitation2014;85:855–863.
225. Hurley KF, Magee K, Green R. Aminophylline for bradyasystolic cardiac arrest inadults. Cochrane Database Syst Rev 2013;8:CD006781.
226. Aufderheide TP, Nichol G, Rea TD, Brown SP, Leroux BG, Pepe PE, Kudenchuk PJ,Christenson J, Daya MR, Dorian P, Callaway CW, Idris AH, Andrusiek D,Stephens SW, Hostler D, Davis DP, Dunford JV, Pirrallo RG, Stiell IG,Clement CM, Craig A, Van Ottingham L, Schmidt TA, Wang HE, Weisfeldt ML,Ornato JP, Sopko G. A trial of an impedance threshold device in out-of-hospitalcardiac arrest. N Engl J Med 2011;365:798–806.
227. Wik L, Olsen JA, Persse D, Sterz F, Lozano M Jr, Brouwer MA, Westfall M,Souders CM, Malzer R, van Grunsven PM, Travis DT, Whitehead A,Herken UR, Lerner EB. Manual vs. integrated automatic load-distributing bandCPR with equal survival after out of hospital cardiac arrest. The randomizedCIRC trial. Resuscitation 2014;85:741–748.
228. Perkins GD, Lall R, Quinn T, Deakin CD, Cooke MW, Horton J, Lamb SE,Slowther AM, Woollard M, Carson A, Smyth M, Whitfield R, Williams A,Pocock H, Black JJ, Wright J1, Han K, Gates S. Mechanical versus manual chestcompression for out-of-hospital cardiac arrest (PARAMEDIC): a pragmatic, clus-ter randomised controlled trial. Lancet 2015;385:947–955.
229. Rubertsson S, Lindgren E, Smekal D, Ostlund O, Silfverstolpe J, Lichtveld RA,Boomars R, Ahlstedt B, Skoog G, Kastberg R, Halliwell D, Box M, Herlitz J,Karlsten R. Mechanical chest compressions and simultaneous defibrillation vsconventional cardiopulmonary resuscitation in out-of-hospital cardiac arrest:the LINC randomized trial. JAMA 2014;311:53–61.
230. Stiell IG, Nichol G, Leroux BG, Rea TD, Ornato JP, Powell J, Christenson J,Callaway CW, Kudenchuk PJ, Aufderheide TP, Idris AH, Daya MR, Wang HE,Morrison LJ, Davis D, Andrusiek D, Stephens S, Cheskes S, Schmicker RH,Fowler R, Vaillancourt C, Hostler D, Zive D, Pirrallo RG, Vilke GM, Sopko G,Weisfeldt M. Early versus later rhythm analysis in patients with out-of-hospitalcardiac arrest. N Engl J Med 2011;365:787–797.
231. Wik L, Hansen TB, Fylling F, Steen T, Vaagenes P, Auestad BH, Steen PA. Delayingdefibrillation to give basic cardiopulmonary resuscitation to patients without-of-hospital ventricular fibrillation: a randomized trial. JAMA 2003;289:1389–1395.
232. Brooks SC, Hassan N, Bigham BL, Morrison LJ. Mechanical versus manual chestcompressions for cardiac arrest. Cochrane Database Syst Rev 2014;2:CD007260.
233. Sanghavi P, Jena AB, Newhouse JP, Zaslavsky AM. Outcomes after out-of-hospitalcardiac arrest treated by basic vs advanced life support. JAMA Intern Med 2015;175:196–204.
234. Olasveengen TM, Wik L, Sunde K, Steen PA. Outcome when adrenaline (epineph-rine) was actually given vs. not given—post hoc analysis of a randomized clinicaltrial. Resuscitation 2012;83:327–332.
235. Deakin CD, Morrison LJ, Morley PT, Callaway CW, Kerber RE, Kronick SL,Lavonas EJ, Link MS, Neumar RW, Otto CW, Parr M, Shuster M, Sunde K,Peberdy MA, Tang W, Hoek TL, Bottiger BW, Drajer S, Lim SH, Nolan JP.Part 8: advanced life support: 2010 International Consensus on CardiopulmonaryResuscitation and Emergency Cardiovascular Care Science with TreatmentRecommendations. Resuscitation 2010;81 (Suppl 1):e93–e174.
236. Kudenchuk PJ, Brown SP, Daya M, Morrison LJ, Grunau BE, Rea T, Aufderheide T,Powell J, Leroux B, Vaillancourt C, Larsen J, Wittwer L, Colella MR, Stephens SW,Gamber M, Egan D, Dorian P. Resuscitation Outcomes Consortium-Amiodarone,Lidocaine or Placebo Study (ROC-ALPS): rationale and methodology behind anout-of-hospital cardiac arrest antiarrhythmic drug trial. Am Heart J 2014;167:653–659.
237. Reynolds JC, Rittenberger JC, Menegazzi JJ. Drug administration in animal studiesof cardiac arrest does not reflect human clinical experience. Resuscitation 2007;74:13–26.
238. Margey R, Browne L, Murphy E, O’Reilly M, Mahon N, Blake G, McCann H,Sugrue D, Galvin J. The Dublin cardiac arrest registry: temporal improvementin survival from out-of-hospital cardiac arrest reflects improved pre-hospitalemergency care. Europace 2011;13:1157–1165.
239. Daya MR, Schmicker RH, Zive DM, Rea TD, Nichol G, Buick JE, Brooks S,Christenson J, MacPhee R, Craig A, Rittenberger JC, Davis DP, May S,Wigginton J, Wang H. Out-of-hospital cardiac arrest survival improving overtime: results from the Resuscitation Outcomes Consortium (ROC). Resuscitation2015;91:108–115.
240. Wong MK, Morrison LJ, Qiu F, Austin PC, Cheskes S, Dorian P, Scales DC, Tu JV,Verbeek PR, Wijeysundera HC, Ko DT. Trends in short- and long-term survivalamong out-of-hospital cardiac arrest patients alive at hospital arrival. Circulation2014;130:1883–1890.
Drug therapy in cardiac arrest 75
by guest on August 22, 2016
http://ehjcvp.oxfordjournals.org/D
ownloaded from
Recommended