DR. S.K CHATURVEDIUNICEF
HIV/AIDS PREVENTION PROGRAMME
PROGRAMME PLAN OF COOPERATION
2003-2007
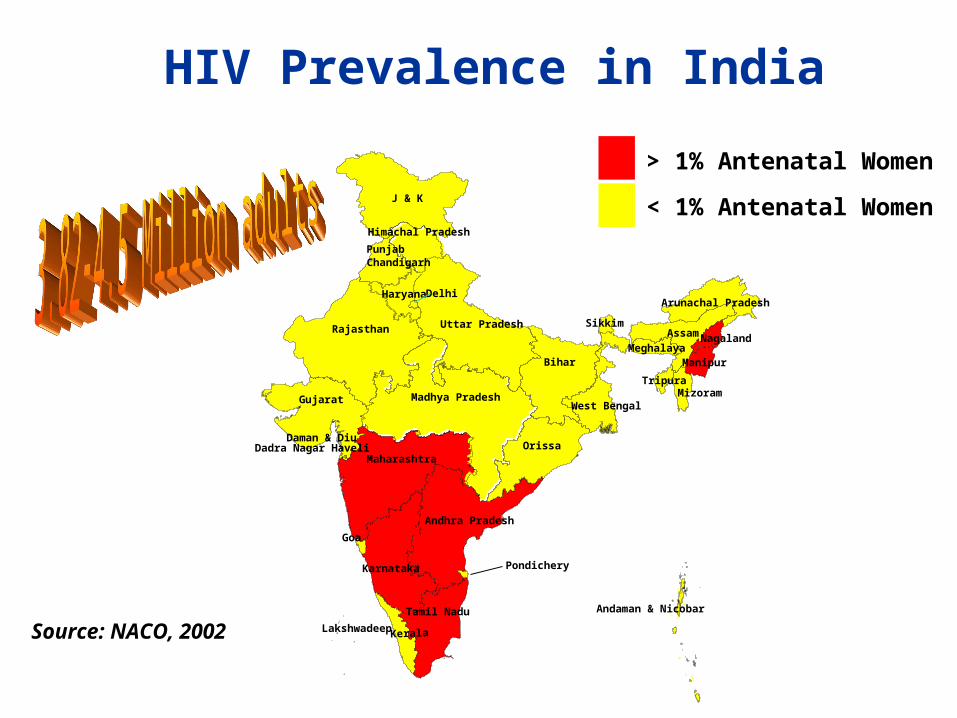
HIV Prevalence in India
Pondichery
Gujarat
Karnataka
Goa
Lakshwadeep
Dadra Nagar HaveliMaharashtra
Madhya Pradesh
Kerala
Tamil Nadu
Andhra Pradesh
Punjab
Rajasthan
Daman & Diu
J & K
Haryana
Uttar Pradesh
Himachal Pradesh
Delhi
Chandigarh
Bihar
West Bengal
Orissa
Andaman & Nicobar
Mizoram
Meghalaya
AssamSikkim
Manipur
Tripura
Arunachal Pradesh
Nagaland
Source: NACO, 2002
> 1% Antenatal Women
< 1% Antenatal Women

Child Mortality as an Indicator of Vulnerability
Pondichery
Gujarat
KarnatakaGoa
Lakshwadeep
Dadra Nagar HaveliMaharashtra
Madhya Pradesh
Kerala
Tamil Nadu
Andhra Pradesh
Punjab
Rajasthan
Daman & Diu
Jammu & Kashmir
Haryana
Uttar Pradesh
Himachal Pradesh
Delhi
Chandigarh
Bihar
West Bengal
Orissa
Andaman & Nicobar
Mizoram
Meghalaya
Assam
Sikkim
Manipur
Tripura
Arunachal Pradesh
Nagaland
HIV + U5MR
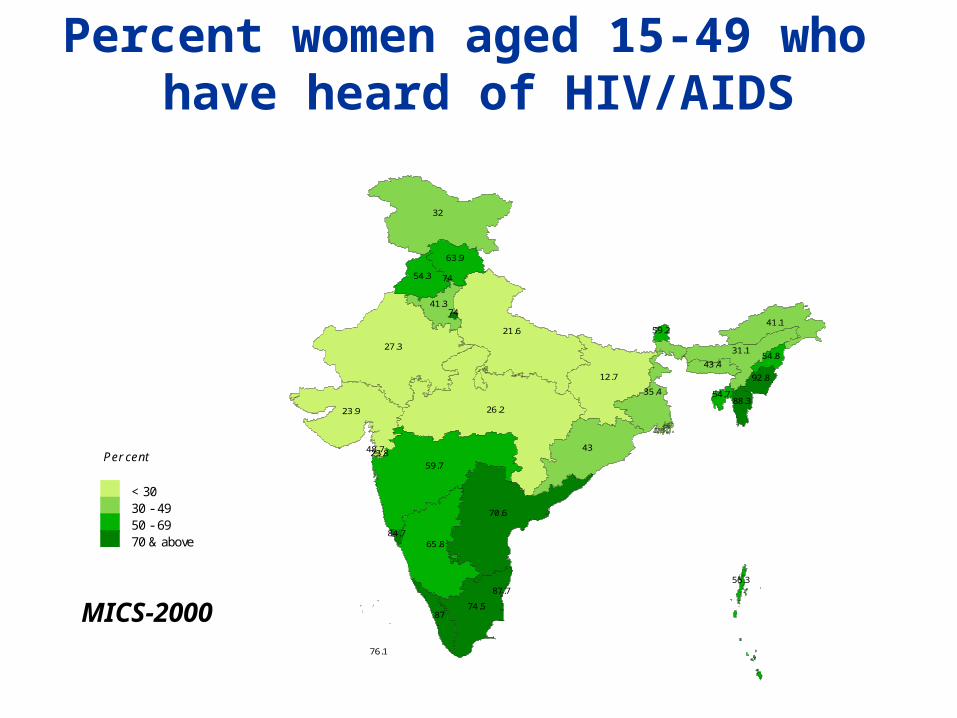
Percent women aged 15-49 who have heard of HIV/AIDS
21.6
26.2
65.8
76.1
59.7
84.7
8774.5
87.7
70.6
23.8
27.3
23.9
48.7
32
7441.3
54.3 74
12.7
35.4
43
56.3
88.3
43.4
31.1
59.2
92.8
54.7
41.1
54.8
63.9
Per cent
< 3030 - 4950 - 6970 & above
MICS-2000

Percent women aged 15-49 who know all threemodes of vertical transmission of HIV/AIDS
13.3
13
40.6
34.4
31.4
40.8
36.642.2
46.9
46.8
14
12.8
11.5
30.8
19
37.821.1
39.6 36.1
6.8
17.7
23.4
36.9
58.1
21
15
21.1
50.2
29.9
17.2
26.2
31.1
Per cent
< 2020 - 2930 - 3940 & above
MICS-2000
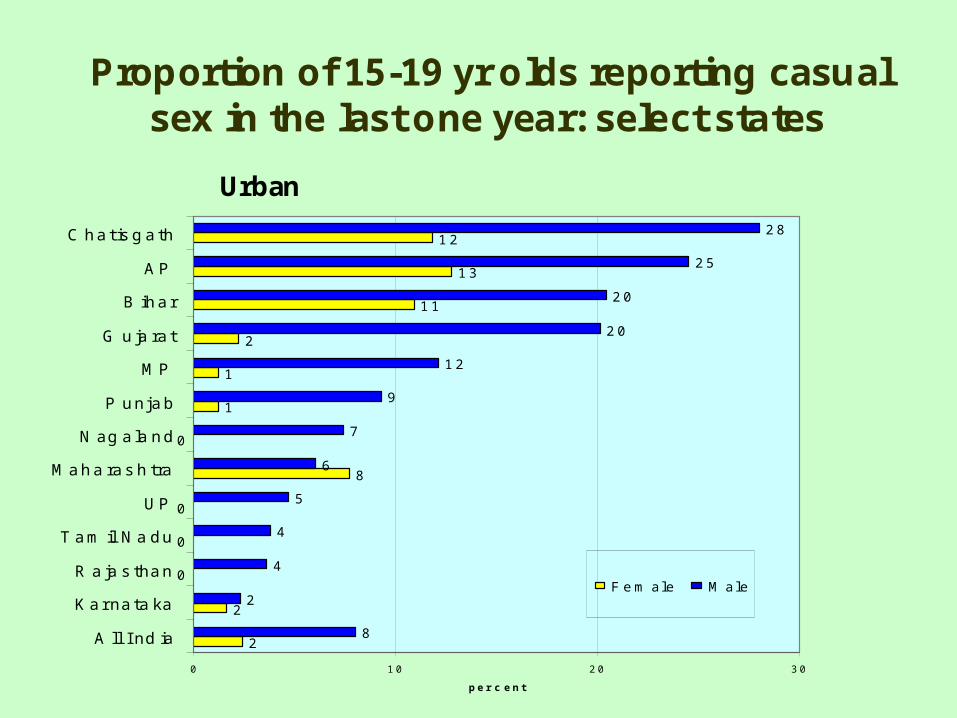
Proportion of 15-19 yr olds reporting casualsex in the last one year: select states
2
2
0
0
0
8
0
1
1
2
1 1
1 3
1 2
8
2
4
4
5
6
7
9
1 2
2 0
2 0
2 5
2 8
0 1 0 2 0 3 0
A ll I nd ia
K a r na ta ka
R a ja s tha n
T a m il N a d u
U P
M a h a ra s h tra
N ag a la n d
P u n j a b
M P
G u ja ra t
B ih a r
A P
C h a t is g a th
p e r c e n t
F e m a l e M a l e
Urban

HIV/AIDS Awareness among Adolescents< 20 years - FHAC 2000
0
10
20
30
40
50
60
RuralUrban Slums
Correct knowledge about benefitsof condom use to prevent STI/HIV
Used condomduring last intercourse
Source: FHAC Coverage EvaluationAIIMS/INCLEN/USAID 2000
32
53
3.46.3
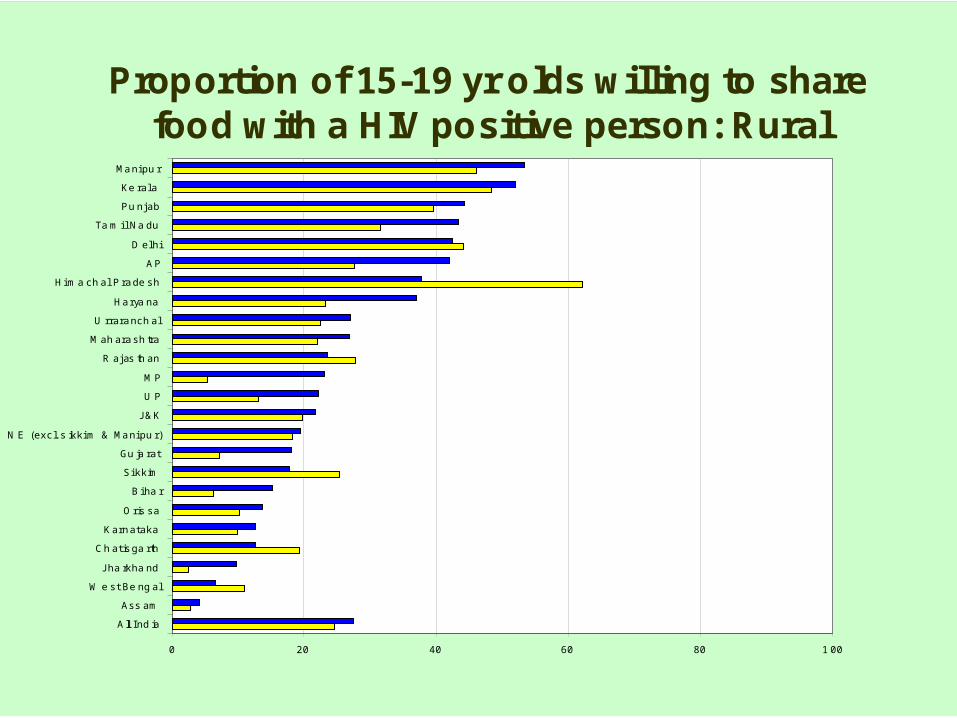
Proportion of 15-19 yr olds willing to sharefood with a HIV positive person: Rural
0 20 40 60 80 1 00
A ll I nd ia
Ass am
W e st Be ng al
Jha rkha nd
Ch at is ga rth
K arn at aka
O ris sa
B i ha r
Si kk im
Gu ja rat
N E (exc l. s ikk i m & Ma ni pu r)
J& K
U P
M P
R aj as th an
M ah ara sh tra
U rrara nch al
Ha rya na
Hi m a ch al P ra de sh
A P
D el hi
Ta m i l Na du
Pu nj ab
Ke ral a
Ma ni pu r
Reported Data in 2001
• Over 50% of all new infections occurring among young people aged below 25.
• 25% of all HIV infection fall in women, with an accompany increase in vertical transmission and pediatric HIV.
• Reported median of HIV prevalence among pregnant women exceed 2% in most high prevalence states.
• Already about 660,000 young women and 345,000 young men aged between 15-24 years are living with HIV/AIDS
• 120,000 AIDS orphan children and 160,000 AIDS children living in the country.
Who Are Now Infected & Affected by HIV/AIDS?

ICO HIV/AIDS Programme Strategy
• Phased approach: Initial focus on four high prevalence states
- 2002-3: High Prevalence 2004-5: Concentrated
2006-7: Low
- AP, Mah, TN & Nagaland + Karnataka and Manipur (PPTCT)
• Modeling scaled-up actions in support of the National Programme
• Strong emphasis on building evidence-based approaches

Projects
PPTCT
Adolescents & YoungPeople
IntegratedCommunication
Thrusts
Scaling up to nationallevel of prevention of MTCT
Prevention of HIVamong young below theage of 25
Building an enablingenvironment for anexpanded responseagainst HIV
Results
Scaled up interventionson HIV prevention
Replicable models of Life Skills Education
Replicable district models
Young People
Coalition of civil societygroups & NGOs
VCCT services forpregnant women
Evidence based national
Operational network ofhealth facilities
policy
PPTCT
Programme Goal: To reduce the prevalence of HIV/AIDS among children and to alleviate the impact of AIDS on children, adolescents
and families affected by HIV/AIDS

PMTCT
1) Scaling up
Expected outputs
• An operational network of health facilities providing quality PPTCT services established
• PPTCT used as an opportunity to strengthen MCH services.
2) District Models
Expected outputs
• A comprehensive, integrated and sustainable distrit- based PPTCT programme
• Pre and in-service training modules for care providers to integrate youth friendly services
Key results:
• Operational network of health facilities for PPTCT established• A National Policy for PPTCT • Replicable district PPTCT models• Partnerships and resources mobilized for scaled up
3) Learning for Policy Development
Expected outputs
• A Feasibility Study of “PPTCT Plus”
• Studies on HIV and infant feeding
• Evidence-based National PPTCT Policy

Scaling up PPTCT to cover the whole countryTiming: Cumulative total of medical
centres participating:
11 Centers of ExcellencePilot project:2000-2002 11
81 Medical Colleges inHigh Prevalence States
December 2002 92
159 District Hospitals/Maternity Hospitals inHigh Prevalence States
June 2003 242
59 Medical Colleges inLow Prevalence States
Dec. 2003 301
450+ District Hospitals/Maternity Hospitals inLow Prevalence States
In 2004 780+
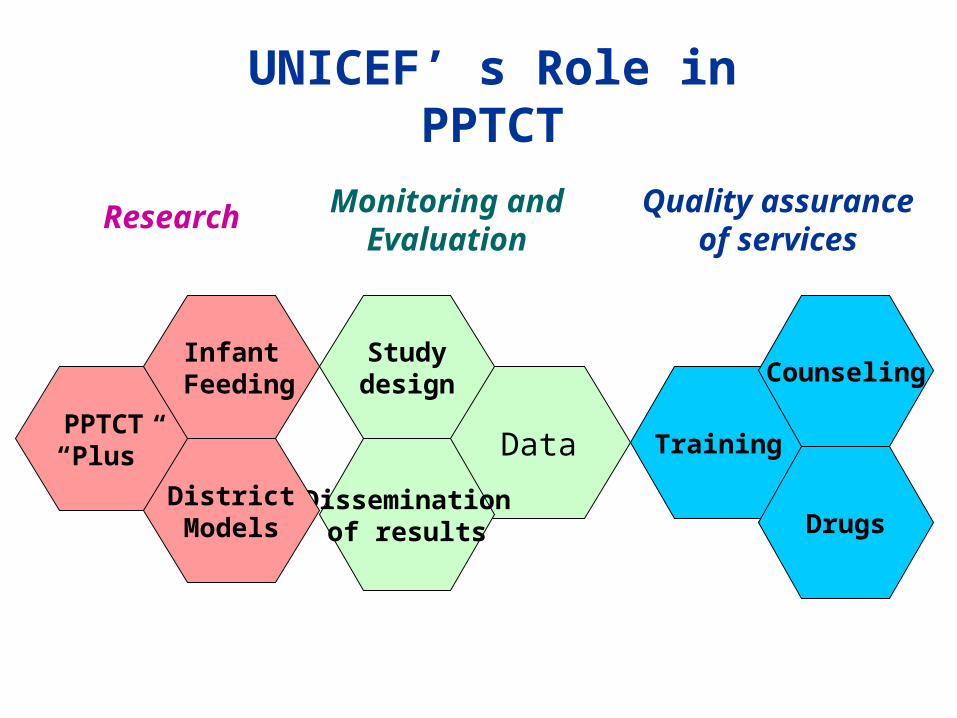
Monitoring and Evaluation
Quality assurance of
services
UNICEF’ s Role in PPTCT
Research
Training
Drugs
Counseling
Data
Disseminationof results
Studydesign
PPTCT“Plus”
DistrictModels
Infant Feeding
Adolescents & Young People
1) Preventive & Peer Education in School
Expected outputs
• Effective intervention models for scaling up in schools
• State-led sustainable response plan
• Linkages of life skills education to other key strategies
2) Young People as Agents of Change
Expected outputs
• Increased participation of young people in HIV/AIDS prevention
• Peer Education Package for out-of-school adolescents and young people
• A Youth forum for public debate and dialogue about HIV/AIDS and related issues
Key results:
• Scaled up interventions on HIV prevention in school• Replicable models of skills-based prevention education for young people
out of school• Coalition of civil society groups and NGOs on YP and HIV/AIDS
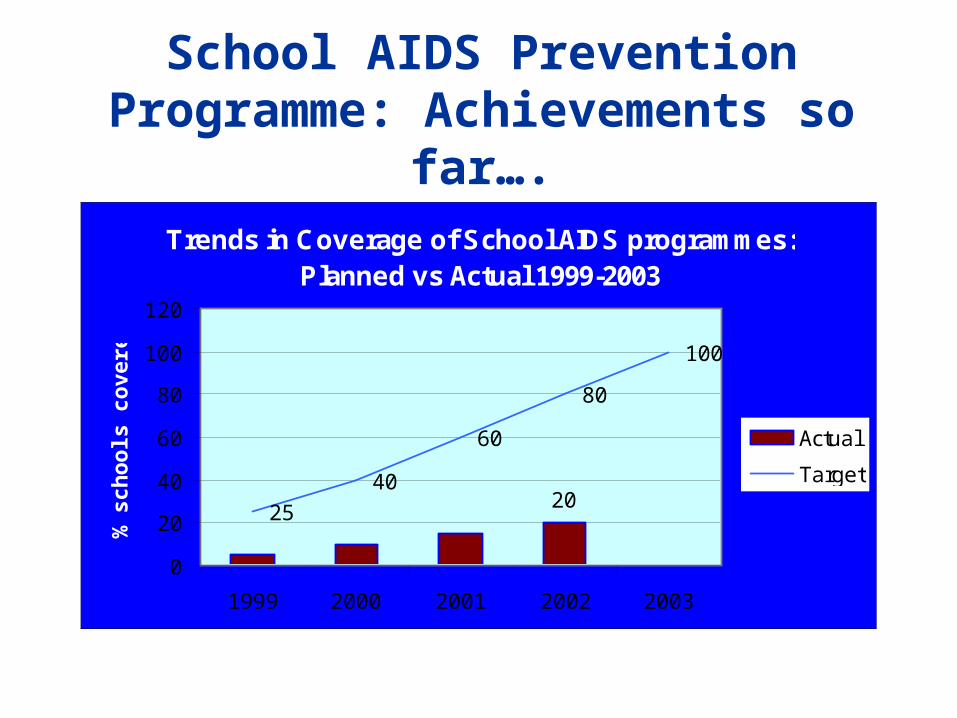
School AIDS Prevention Programme: Achievements so far….
Trends in Coverage of School AIDS programmes: Planned vs Actual 1999-2003
2025
40
60
80
100
0
20
40
60
80
100
120
1999 2000 2001 2002 2003
% s
ch
oo
ls c
ov
ere
d
Actual
Target

Impact of school HIV education
Delayed Sexual Debut Primary students (13-16yrs) following IEC
0
10
20
30
40
50
60
70
Boys Girls
% S
exu
al in
nitia
tion
1994
1996
2001
Source: AMREF 2001

Integrated Communication
1) Advocacy and Mobilization for Social Change
Expected outputs
• Documentation on the impact of HIV/AIDS and data analysis to sensitize key stakeholders for policy formulation and increased resource allocation
• Communication Strategies to reduce risks, increase demand for health services, and address stigma and discrimination among health care providers and the general population
• Expanded partnerships and alliances with civil society & private sector
2) Behavior Development and Change
Expected outputs
• Increased participation of communities, families, individuals, and service providers in responding to HIV/AIDS prevention.
• Effective communication packages for behavior change, focusing in safe behaviors and health care services
• Communication strategy to support PPTCT and Young People interventions
Key Results:
• Partnerships and resources mobilized for scaled up interventions• Packages of communication initiatives including innovative approaches
Recommended

















