
Dr Mayur Bodani
Consultant Neuropsychiatrist
Raphael Medical Centre 26.11.14

Epidemiology traumatic brain injury (tbi)
Definitions
Sleep disorders in tbi
Disorders of fatigue in tbi
Possible pathophysiology

Neil Munroe
• Brain Maps
‘damage to brain tissue caused by an external mechanical force, as evidenced by loss of consciousness, post-traumatic amnesia, skull fracture, or objective neurological findings that can be reasonably attributed to tbi on physical examination or mental status examination’
TBI Model Systems Task Force, 1998

Focal
Diffuse
Haemorrhagic
Non-haemorrhagic
Coup and contrecoup
Contusional
Compressive (epidural and subdural)

Natural traumatic forces never injure the brain in exactly the same way
Neural circuits will be differentially impaired
Different degrees of dysfunction from individual to individual
Further permutation of each brain’s own unique set of premorbid strengths and weaknesses
1.6 million to 3 million tbi’s in the US and worldwide
51,0000 deaths pa
15,000-20,000 victims in France pa
5-10% severe tbi
Men> Women 2:1
Falls/RTA’s main cause
Young age group: 12-25
290,000 hospitalizations
Mild
13-15
Moderate
9-12
Severe
<= 8
Other Factors:
Mechanism
Open/closed
Neuroimaging
Duration of LOC
PTA
Civilian
Falls 28%
RTA 20%
Object Impact 19%
Assault 11%
Military 11-23% mtbi
59% blast-exposed tbi

12
24
6 Wakefulness
Stage 1-2 sleep
REM sleep
18.00 20.00 22.00 24.00 02.00 04.00 06.00 08.00 10.00 12.00 14.00 16.00
MT
W
REM
1
2
3/4
Time
Sle
ep
sta
ge
REM sleep
18
Adapted from Rogers et al. Sleep. 1994;17:590.
Stage 3-4 sleep
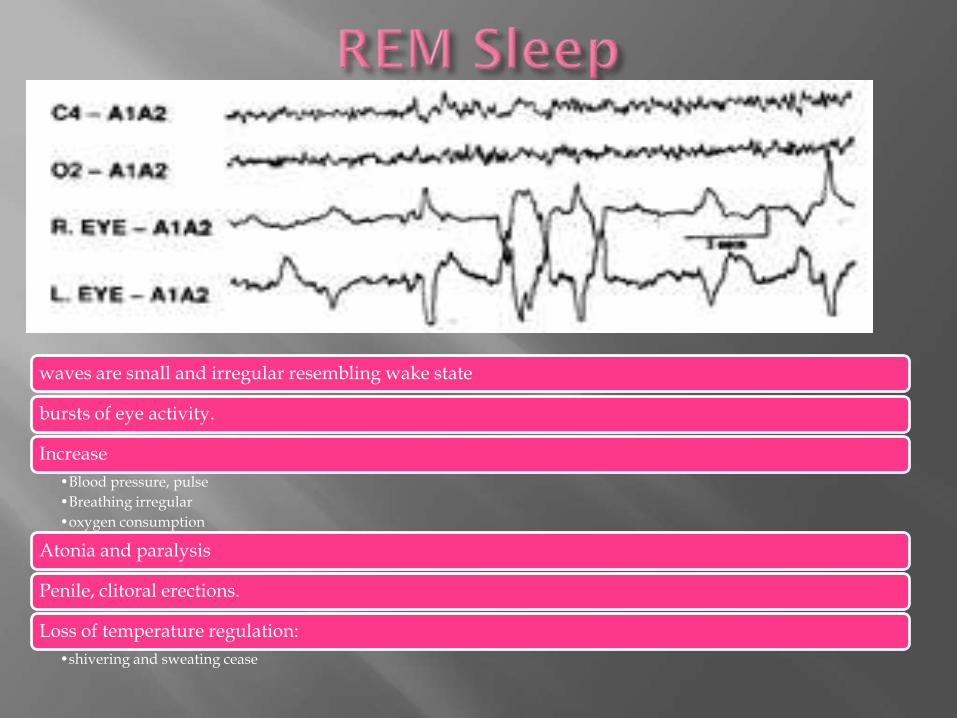
waves are small and irregular resembling wake state
bursts of eye activity.
Increase
•Blood pressure, pulse
•Breathing irregular
•oxygen consumption
Atonia and paralysis
Penile, clitoral erections.
Loss of temperature regulation:
•shivering and sweating cease

N1
•Transition from alpha waves (8Hz to 13 Hz) to theta waves (4Hz to 7 Hz)
•Drowsy sleep.
•Hypnogogic) myoclonus or hallucinations.
N2
•Conscious awareness of the external environment disappears.
•Muscle activity decreases.
•Blood pressure, heart rate, secretions and metabolism decrease.
N3
•Deep sleep
•Parasomnias
Broad range reported including:
Insomnia
Hypersomnia
Sleep Apnoea
Periodic limb movements
Narcolepsy
Specific:
Snoring, nightmares, poor sleep efficiency
Delayed sleep onset, poor sleep quality
Early awakenings
EDS

68% acute recovery and rehabilitation
Association with being in PTA
50% chronic sleep disturbance
Insomnia
Hypersomnia
OSA
EDS
Tiredness or daytime drowsiness after insufficient sleep or sleep disruption
Hard to disentangle EDS and fatigue MAKLEY, 2008
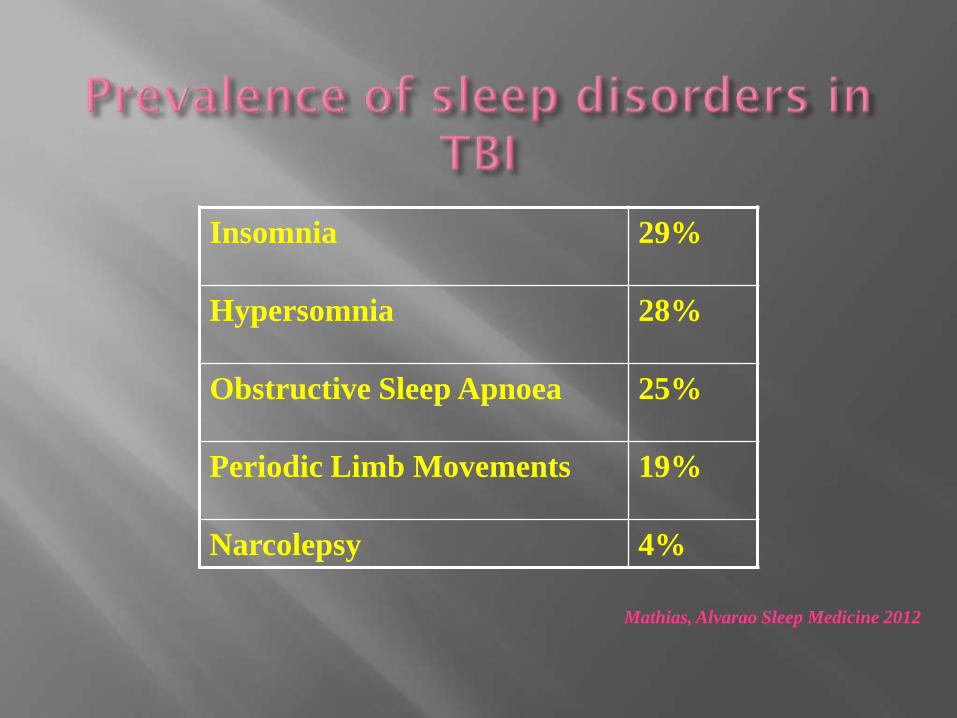
Insomnia 29%
Hypersomnia 28%
Obstructive Sleep Apnoea 25%
Periodic Limb Movements 19%
Narcolepsy 4%
Mathias, Alvarao Sleep Medicine 2012
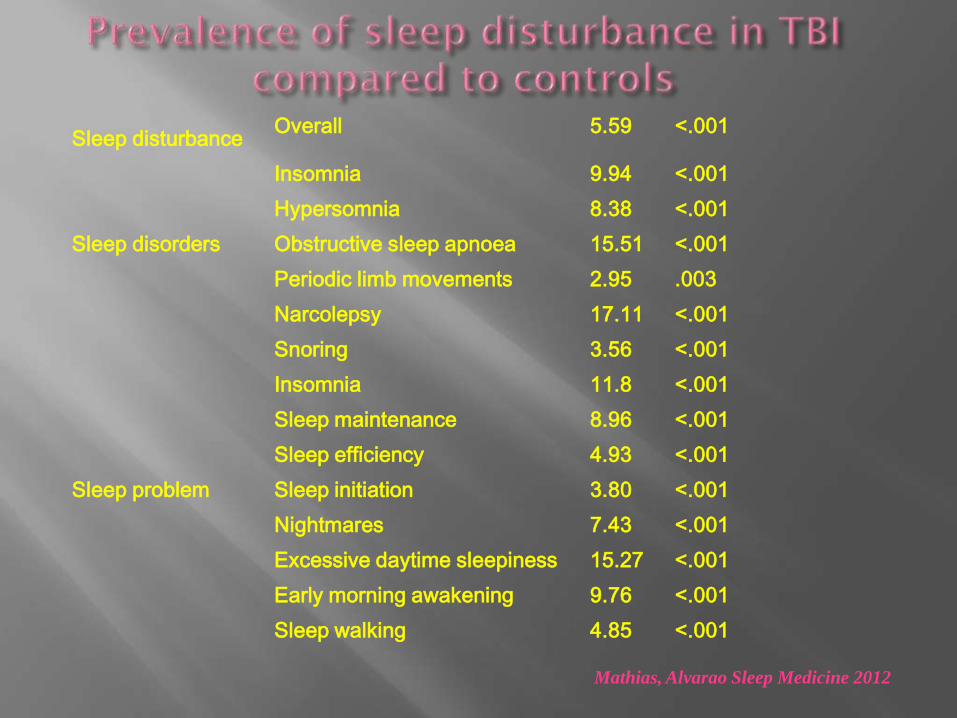
Sleep disturbance Overall 5.59 <.001
Sleep disorders
Insomnia 9.94 <.001
Hypersomnia 8.38 <.001
Obstructive sleep apnoea 15.51 <.001
Periodic limb movements 2.95 .003
Narcolepsy 17.11 <.001
Sleep problem
Snoring 3.56 <.001
Insomnia 11.8 <.001
Sleep maintenance 8.96 <.001
Sleep efficiency 4.93 <.001
Sleep initiation 3.80 <.001
Nightmares 7.43 <.001
Excessive daytime sleepiness 15.27 <.001
Early morning awakening 9.76 <.001
Sleep walking 4.85 <.001
Mathias, Alvarao Sleep Medicine 2012

Primary sleep parasomnias REM
REM sleep behaviour disorder most common parasomnia in TBI ~ 10-15%
NREM Disorders of arousal
Sleep walking ~ 9% Sleep eating ~3%
Either Rhythmic Movement disorder
RLS and PLMS
PLMS in TBI ~ 19% Mathias et al 2012
Enuresis Bruxism
Verma et al 2007

Self-reported problems at variance with objective measures
Polysomnography:
Longer sleep-onset latencies
Increased night-time awakenings
Increased SWS
Changes in REM sleep
Results vary
No differences between tbi and healthy controls
(sleep architecture and sleep continuity) OUELLET & MORIN, 2006
Lower cost alternative to PSG
Wrist watch like device
Continuous record of motor activity
Caution – spasticity, paresis, impulsivity, agitation
Poor sleep efficiency in patients in PTA
Increased time spent asleep>6 months post-injury
Circadian rhythm disturbance in mild tbi BAUMANN, 2007

Clinical Interview
PSG
Actigraphy
Sleep Diary
Maintenance of Wakefulness Test (MWT)
Objective assessment of capacity to remain awake
No sig difference tbi v controls (Beaulieu-Bonneau,2012)
Pittsburg Sleep Quality Index (PSQI)
Epworth Sleepiness Scale

PSQI
Self-report
>8
Insomnia
ESS
Self-rate likelihood of dozing or falling asleep in specified sedentary situations
>=10 [0-24] indicator of EDS

PSQI – poor sleep quality in mild to severe tbi
(Cantor, 2012)
High EDS scores in some studies with moderate to severe tbi
(Ponsford, 2013)
Findings not universal and depend on sample size

65 patients with tbi assessed at 6 months post-injury
72% sleep-wake disturbance
Subjective EDS (28%)
Objective EDS (25%)
Fatigue without EDS (17%)
Hypersomnia (22%)
Insomnia (5%)

Earlier bedtimes
Longer sleep-onset latency
Reduced sleep efficiency
Greater total sleep duration and time in bed
Longer and more frequent daytime naps
Mild to severe tbi
3 months to 11 years post-injury
(Ponsford’s group, Australia)

various
Reduced REM
Increased late REM
Decreased REM latency
12
24
6
Wakefulness
Stage 1-2 sleep
REM sleep
18 Stage 3-4 sleep

Multifactorial
Brain areas associated with sleep regulation
SCN
Hypothalamus
Midbrain
ARAS
NT systems
All vulnerable to tbi
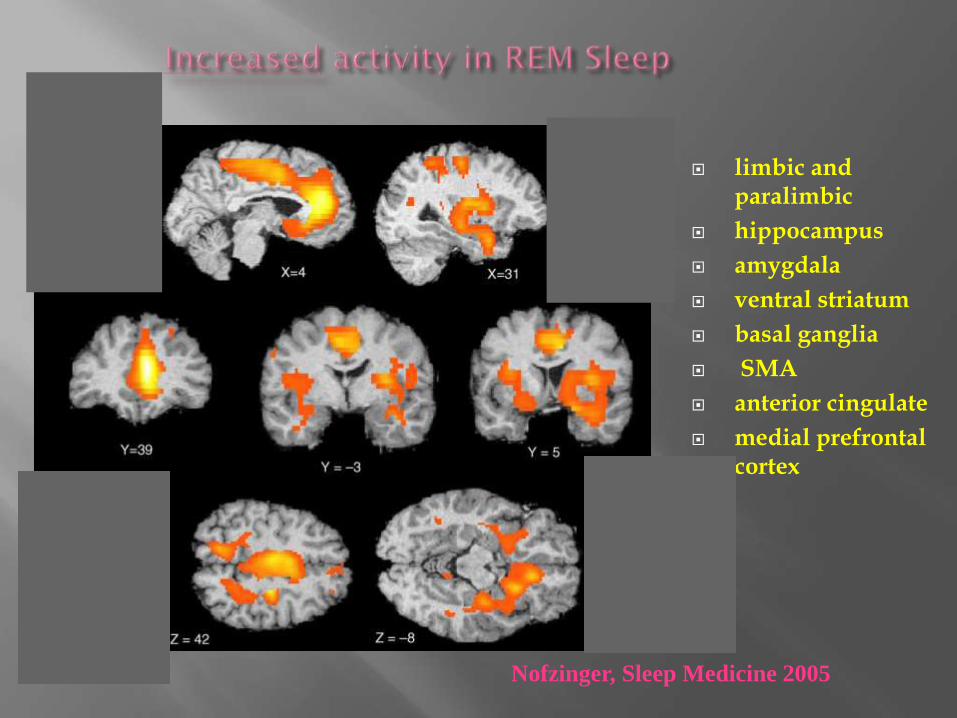
Nofzinger, Sleep Medicine 2005
limbic and paralimbic
hippocampus
amygdala
ventral striatum
basal ganglia
SMA
anterior cingulate
medial prefrontal cortex
,,,,……
…,,.,,,,,,,
,,,,,,,,,,,,,,
,,,,,,,,,,,,,,
,

Locus coeruleus
Raphe nuclei
dorsal, median
LDT, PPT
Peri-aq Grey
Subst. Nigra, VTA
Thalamus

Tubero-mamillary N: TMN
VLPO
SCN
accumbens
Basal forebrain

Lower levels of evening melatonin production (pineal gland) [Shekelton, 2010]
Possible disruption of circadian regulation
(Ayalon, 2007)
Reduced cortical excitability using tms, similar to narcolepsy associated with objectively measured EDS 3 months after mild /moderate tbi [Nardone, 2011]
Possible deficiency in hypocretin/orexin NT system
Pain
Depression
Anxiety
Fatigue
Increased daytime napping night-time sleep quality

Commonly reported
Symptom not diagnosis
Definition and measurement hard to operationalize
Multidimensional construct
Aaronson (1999):
‘the awareness of a decreased capacity for physical and/or mental activity due to an imbalance in the availability, utilization, and/or restoration of resources needed to perform activity’

Physiologic fatigue v. Psychological
Central v. Peripheral
Primary v. Secondary
Psychological fatigue:
‘A state of weariness related to reduced motivation, prolonged mental activity, or boredom that occurs in situations such as stress, anxiety or depression’
The subjective experience of fatigue is likeley a combination of these factors

Various aspects measured
Severity
Impact on daily activities
Associated feelings
No scale specifically for these aspects after tbi
Several scales sensitive to fatigue in tbi population
Visual Analogue Scale for Fatigue (VAS-F)
Subjective, Single point, 18-item
Can measure fatigue at different times of the day, or in response to activity/intervention
Fatigue Severity Scale (FSS)
Behavioral consequences of fatigue
Impact of fatigue on daily living
9 items on a 7-point scale
Barrow Neurologic Institute Fatigue Scale
10 items, 7-point scale

Global Fatigue Index
Multidimensional Assessment of Fatigue
Causes of fatigue questionnaire
Self-report
Few/none validated objective measures in tbi
Search for an objective marker continues

Wide range [21-73%]
Fatigue may decline in the first 6-12 months post injury in moderate – severe tbi but then remain static [Ponsford, 2012]
Even after 10 years significant symptom reporting [Zumstein , 2011]
Considerable individual variation over time
Daytime variation
Progressive increase in fatigue after awakening: reverse of health normals [Beaulieu-Bonneau, 2012]

Group Fatigue (%)
Control 30.6
mtbi 35.1
Mod tbi 32.4
Sev tbi 57.7
[Masson, 1996]
N=231 at 5 years

Cardiac – e.g. Heart failure
Metabolic- e.g. vit D def
Endocrine – e.g. hypopituitarism
Neurologic – e.g. MS
Psychiatric – e.g. Depression, anxiety, PTSD
Infection – e.g. EBV
GI – e.g. Coeliac
Neoplastic
Other

AED
Antihistamines
Antipsychotics
AD
Steroids
Antiarrhythmics
Antiemetics

Primary fatigue – diffuse neuronal injury
Damage to systems that control arousal, attention, response speed
ARAS
Limbic system
Anterior cingulate
Medial frontal
Basal ganglia
[Chaudhuri & Behan, 2000]
Fatigue – result of increased effort required to manage daily activities in the presence of cognitive difficulties
Expending more effort at greater cost
Tonic v phasic arousal
Baseline arousal/alertness
Arousal in response to stimuli
ARAS involved in phasically turning on cortical tissue in an efficient manner
So PTF: inability to activate but also efficiently sustain and recruit cortical tissue
GH deficiency reported in a higher than average proporotion of tbi cases [Englander, 2010]
Lower levels of CSF hypocretin-1 [Baumann, 2009]
Hypocretin levels tend to normalise beyond the acute post-injury stage [Baumann, 2005]
Insulin growth factor -1
Adrenal deficiency
Testosterone deficiency
Sleep disorders
Some tired patients do not have any sleep disorder
All patients with sleep disorder do not have fatigue
Depression
Prevalence after tbi variable [6-77%]
Mental effort seems to correlate with fatigue
Correlation between anxiety and fatigue

Impact on rehabilitation
Constraint on day to day living
Employment
Energy for social activities
Confinement at home
Depression
Effective treatments are limited
Pharmacologic and non-pharmacologic treatments
Recommended

















