Do Trauma Centers Save Lives?
A Statistical Solution
Daniel O. Scharfstein

Collaborators
• Brian Egleston
• Ciprian Crainiceanu
• Zhiqiang Tan
• Tom Louis

Issues
• Outcome Dependent Sampling• Missing Data• Confounding
– Direct Adjustment– Propensity Score Weighting
• Propensity Model Selection• Weight Trimming• Clustering

Population: (Y,X,T)
Counterfactual Population: Y(0),XCounterfactual Population: Y(1),X
Counterfactual Sample Counterfactual Sample
Sub-Sample
Sample
Big Picture

Population: (Y,X,T)
Sub-Sample
Sample


TC NTC
N 10970 4039
% Dying 8.0% 5.9%


TC NTC
N 3044 1999
% Dying 27.8% 11.9%


Sample Weights
• Reciprocal of the conditional probability of being included in the sub-sample given– ISS– AIS– Age– Dead/Alive at Sample Ascertainment– Dead/Alive at 3 Months post injury
• Weights depend on outcome - they can’t be ignored.


Missing DataSocio-demographic Pre-Hospital Injury Severity Hospital Injury Severity
Age (0%) SBP/Shock (38.1%) AIS (0%)
Gender (0%) GCS Motor (30.0%) NISS (0%)
Race (0%) Paralytics (8.6%) Lowest SRR (0%)
Insurance (1.2%) Intubation (6.0%) APS (0%)
EMS Level/
Mode of Transport (19.0%)
SBP/Shock (1.0%)
Outcome MOI (2.0%) Pupils (5.7%)
Death (0%) GCS Motor (2.4%)
Midline Shift (1.8%)
Co-morbidities Open Skull Fracture (0%)
Obesity (4.6%) Flail Chest (0%)
Coagulopathy (4.6%) Heart Rate (0.9%)
Charlson (4.6%) Paralysis (1.1%)
Long Bone Fracture/Amputation (0%)

Multiple Imputation
• For proper MI, we fill in the missing data by randomly drawing from the posterior predictive distribution of the missing data given the observed data.
• To reflect the uncertainty in these imputed values, we create multiple imputed datasets.
• An estimate (and variance) of the effect of trauma center is computed for each completed data.
• The results are combined to obtain an overall estimate. • The overall variance is the sum of the within imputation
variance and the between imputation variance.

Multiple Imputation
• To draw from the posterior predictive distribution, a model for the joint distribution of the variables and a prior distribution on the model parameters must be specified.
• Joe Schafer’s software• UM’s ISR software - IVEWARE
– Specifies a sequence of full conditionals, which is not, generally, compatible with a joint distribution.
• WINBUGS - Crainiceanu and Egleston– Specifies a sequence of conditional models, which
is compatible with a joint distribution

Selection Bias
TC NTC
Age < 55 79% 53%
Male 73% 57%
Race
White, Non-Hispanic 56% 72%
Hispanic 18% 13%
Non-white, Non-Hispanic 26% 16%
Charlson
0 77% 58%
1 14% 17%
2 5% 10%
3 or more 5% 16%

TC NTC
Mechanism of Injury
Blunt - Motor Vehicle 53% 32%
Blunt - Fall 20% 53%
Blunt - Other 10% 10%
Penetrating - Firearm 12% 4%
Penetrating - Other 5% 2%
Pupils - Abnormal 9% 5%
GCS Motor Score
6 74% 90%
4-5 8% 4%
2-3 1% 1%
1 - Not Chemically Paralyzed 5% 3%
Chemically Paralyzed 12% 2%
Selection Bias

TC NTC
NISS
<16 24% 52%
16-24 16% 56%
25-34 29% 15%
>34 18% 9%
Max AIS
<=3 8% 73%
4 27% 20%
5-6 15% 7%
EMS Level/Intubation
ALS - Intubated 12% 3%
ALS - Not Intubated 69% 41%
BLS 11% 35%
Not Transported by EMS 8% 22%
Selection Bias

Notation
• T denotes treatment received (0/1)• X denotes measured covariates• Y(1) denotes the outcome a subject would
have under trauma care.• Y(0) denotes the outcome a subject would
have under non-trauma care.• Only one of these is observed, namely Y=Y(T),
the outcome of the subject under the care actually received.
• Observed Data: (Y,T,X)

Causal Estimand

Selection Bias
• We worked with scientific experts to define all possible “pre-treatment” variables which are associated with treatment and mortality.
• We had extensive discussions about unmeasured confounders.
• Within levels of the measured variables, we assumed that treatment was randomized.
• T is independent of {Y(0),Y(1)} given X

Example (Hernan et al., 2000)

Direct Adjustment

Direct Adjustment

Direct Adjustment

Direct Adjustment

Direct Adjustment

Direct Adjustment

Population: (Y,X,T)
Counterfactual Population: Y(0),XCounterfactual Population: Y(1),X
Counterfactual Sample Counterfactual Sample
Sub-Sample
Sample

Propensity Score Weighting


Y(1) Counterfactual Population

Y(0) Counterfactual Population

Why does this work?

Propensity Model Selection
• Select a propensity score model such that the distribution of X is comparable in the two counterfactual populations (Tan, 2004).

Weight Trimming
• The propensity score weighted estimator can be sensitive to individuals with large PS weights.
• When the weights are highly skewed, the variance of the estimator can be large.
• We trim the weights to minimize MSE.


Clustering
• Assumed a working independence correlation structure.
• Fixed up standard errors using the sandwich variance technique.

Results
TC NTC TC NTC
Age < 55 79% 53% 72% 73%
Male 73% 57% 69% 67%
Race
White, Non-Hispanic 56% 72% 60% 58%
Hispanic 18% 13% 16% 17%
Non-white, Non-Hispanic 26% 16% 24% 25%
Charlson
0 77% 58% 72% 73%
1 14% 17% 14% 13%
2 5% 10% 6% 6%
3 or more 5% 16% 8% 8%
CounterfactualPopulationsSample

TC NTC TC NTC
Mechanism of Injury
Blunt - Motor Vehicle 53% 32% 48% 50%
Blunt - Fall 20% 53% 28% 27%
Blunt - Other 10% 10% 10% 9%
Penetrating - Firearm 12% 4% 10% 10%
Penetrating - Other 5% 2% 4% 4%
Pupils - Abnormal 9% 5% 8% 9%
GCS Motor Score
6 74% 90% 78% 77%
4-5 8% 4% 7% 6%
2-3 1% 1% 1% 1%
1 - Not Chemically Paralyzed 5% 3% 4% 4%
Chemically Paralyzed 12% 2% 10% 11%
ResultsCounterfactualPopulationsSample

TC NTC TC NTC
NISS
<16 24% 52% 30% 30%
16-24 16% 56% 7% 7%
25-34 29% 15% 26% 24%
>34 18% 9% 16% 19%
Max AIS
<=3 8% 73% 61% 60%
4 27% 20% 26% 26%
5-6 15% 7% 13% 14%
EMS Level/Intubation
ALS - Intubated 12% 3% 10% 10%
ALS - Not Intubated 69% 41% 61% 61%
BLS 11% 35% 17% 17%
Not Transported by EMS 8% 22% 12% 12%
ResultsCounterfactualPopulationsSample

30 Days 90 Days 365 Days
Total NSCOT Population
% Dying in TC 7.6% 8.7% 10.4%
% Dying in NTC 10.0% 11.4% 13.8%
RR 0.76 (0.58,1.00) 0.77 (0.60,0.98) 0.75 (0.60,0.95)
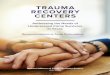
Results

Case Fatality Ratios Adjusted for Differences in Casemix
0
5
10
15
InHospital
30 days 90 days 365 daysTCs
NTCs
Adjusted
Relative Risk:
.60.75
.95

30 Days 90 Days 365 Days
AGE<55
% Dying in TC 7.6% 8.7% 10.4%
% Dying in NTC 10.0% 11.4% 13.8%
RR 0.76 (0.58,1.00) 0.77 (0.60,0.98) 0.75 (0.60,0.95)
AGE>=55
% Dying in TC 1.5% 1.5% 1.8%
% Dying in NTC 1.1% 1.2% 2.9%
RR 1.39 (0.68,2.84) 1.33 (0.68,2.60) 0.63 (0.32,1.22)
Results
MAXAIS <=3

30 Days 90 Days 365 Days
AGE<55
% Dying in TC 6.0% 6.7% 7.4%
% Dying in NTC 9.4% 11.1% 13.2%
RR 0.64 (0.44,0.93) 0.60 (0.41,0.89) 0.56 (0.38,0.82)
AGE>=55
% Dying in TC 14.0% 17.2% 23.9%
% Dying in NTC 15.1% 23.0% 27.4%
RR 0.92 (0.54,1.57) 0.75 (0.51,1.11) 0.87 (0.58,1.32)
Results
MAXAIS = 4

30 Days 90 Days 365 Days
AGE<55
% Dying in TC 25.1% 26.1% 26.3%
% Dying in NTC 38.5% 38.5% 38.5%
RR 0.65 (0.45,0.94) 0.68 (0.47,0.98) 0.68 (0.47,0.99)
AGE>=55
% Dying in TC 44.6% 50.2% 51.5%
% Dying in NTC 61.6% 63.7% 63.7%
RR 0.72 (0.45,1.17) 0.79 (0.51,1.21) 0.81 (0.53,1.23)
Results
MAXAIS = 5,6

Relative Risks by Age and Severity
Age of Patient
Severity < 55 >=55
Moderate (AIS 3) 0.32
0.631.22 0.74
1.081.57
Serious (AIS 4) 0.38
0.560.82 0.58
0.871.32
Severe (AIS 5-6) 0.47
0.680.99 0.53
0.811.23

Potential Lives Saved Nationwide H-CUP Hospital Discharge Data
360,293 adults who meet NSCOT inclusion criteria
45% Treated in NTCs162,132
16,862 DeathsIf Treated in TCs
22,374 Deaths If Treated in NTCs
5,512 Each Year

Conservative Estimate
• Study non-trauma centers were limited to those treating at least 25 major trauma patients each year; most non-trauma centers are smaller
• 17 of the study non-trauma centers had a designated trauma team and 8 had a trauma director

Conclusions . . . to date
• The results demonstrate the benefits of trauma center care and argue strongly for continued efforts at regionalization
• At the same time, they highlight the difficulty in improving outcomes for the geriatric trauma patient

Biostatistician’s Dream
• More efficient estimation (Tan,Wang)• Functional outcomes in the presence of death
(Egleston)• Sensitivity Analysis (Egleston)• Instrumental variable analysis (Cohen, Louis,
Crainiceanu)• Imputation (Crainiceanu, Egleston)
Recommended