1338
Since 1995, more than 45,000 people inthe United States have died waitingfor a suitable donor organ. Although
an oft-cited poll (1) showed that 85% ofAmericans approve of organ donation, lessthan half had made a decision about donat-ing, and fewer still (28%) had granted per-mission by signing a donor card, a patternalso observed in Germany, Spain, andSweden (2–4). Given the shortage ofdonors, the gap between approval and ac-tion is a matter of life and death.
What drives the decision to become apotential donor? Within the EuropeanUnion, donation rates vary by nearly an or-der of magnitude across countries and thesedifferences are stable from year to year.Even when controlling for variables such astransplant infrastructure, economic and ed-ucational status, and religion (5), large dif-ferences in donation rates persist. Why?
Most public policy choices have a no-action default, that is, a condition is im-posed when an individual fails to make adecision (6, 7). In the case of organ dona-tion, European countries have one of twodefault policies. In presumed-consentstates, people are organ donors unless theyregister not to be, and in explicit-consentcountries, nobody is an organ donor with-out registering to be one.
According to a classical economics view,preferences exist and are available to the de-cision-maker—people simply find too littlevalue in organ donation. This view has ledto calls for the establishment of a regulatedmarket for the organs of the deceased (8, 9),for the payment of donors or donors’ fami-lies (10, 11), and even for suggestions thatorgans should become public property upondeath (12). Calls for campaigns to changepublic attitudes (13) are widespread. In clas-sical economics, defaults should have a lim-ited effect: when defaults are not consistentwith preferences, people would choose anappropriate alternative.
A different hypothesis arises from re-search depicting preferences as constructed,that is, not yet articulated in the minds ofthose who have not been asked (14–16). If
preferences for being an organ donor areconstructed, defaults can influence choicesin three ways: First, decision-makers mightbelieve that defaults are suggestions by thepolicy-maker, which imply a recommendedaction. Second, making a decision often in-volves effort, whereas accepting the defaultis effortless. Many people would ratheravoid making an active decision about dona-tion, because it can be unpleasant and stress-ful (17). Physical effort such as filling out aform may also increase acceptance of the de-fault (18). Finally, defaults often representthe existing state or status quo, and changeusually involves a trade-off. Psychologistshave shown that losses loom larger than theequivalent gains, a phenomenon known asloss aversion (19). Thus, changes in the de-fault may result in a change of choice.
Governments, companies, and publicagencies inadvertently run “natural experi-ments” testing the power of defaults.Studies of insurance choice (20), selectionof Internet privacy policies (21, 22), andthe level of pension savings (23) all showlarge effects, often with substantial finan-cial consequences.
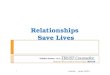
Defaults and Organ DonationsWe investigated the effect of defaults ondonation agreement rates in three studies.The first used an online experiment (24):161 respondents were asked whether theywould be donors on the basis of one ofthree questions with varying defaults. Inthe opt-in condition, participants were toldto assume that they had just moved to anew state where the default was not to bean organ donor, and they were given achoice to confirm or change that status.The opt-out condition was identical, exceptthe default was to be a donor. The third,neutral condition simply required them tochoose with no prior default. Respondentscould at a mouse click change their choice,largely eliminating effort explanations.
The form of the question had a dramat-ic impact (see figure, left): Revealed dona-tion rates were about twice as high whenopting-out as when opting-in. The opt-outcondition did not differ significantly fromthe neutral condition (without a default op-tion). Only the opt-in condition, the currentpractice in the United States, was signifi-cantly lower.
In the last two decades, a number ofEuropean countries have had opt-in or opt-out default options for individuals’ deci-sions to become organ donors. Actual deci-sions about organ donation may be affectedby governmental educational programs, the
M E D I C I N E
Do Defaults Save Lives?Eric J. Johnson* and Daniel Goldstein
POLICY FORUM
The authors are at the Center for Decision Sciences,Columbia University, New York, NY 10027, USA.
*To whom all correspondence should be addressed:[email protected]
42
82 79
Opt-In Opt-Out Neutral
Per
cen
t co
nse
nti
ng
to b
ein
g d
on
ors
0
10
20
30
40
50
60
70
80
90
100
Effective consent rates, online experiment,
as a function of default.
4.25
27.5
17.1712
99.98 98 99.91 99.97 99.5 99.64
85.9
0
10
2030
40
50
60
70
80
90
100
Den
mar
k
Net
herla
nds
Eff
ecti
ve c
on
sen
t p
erce
nta
ge
Uni
ted
Kin
gdom
Ger
man
y
Aus
tria
Bel
gium
Fra
nce
Hun
gary
Pol
and
Por
tuga
l
Sw
eden
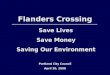
Effective consent rates, by country. Explicit consent (opt-in, gold) and presumed consent (opt-
out, blue).
21 NOVEMBER 2003 VOL 302 SCIENCE www.sciencemag.org

1339
efforts of public health organizations, andcultural and infrastructural factors. We ex-amined the rate of agreement to become adonor across European countries with ex-plicit and presumed consent laws. We sup-plemented the data reported in Gäbel (25)by contacting the central registries for sever-al countries, which allowed us to estimatethe effective consent rate, that is, the numberof people who had opted in (in explicit-con-sent countries) or the number who had notopted out (in presumed-consent countries).If preferences concerning organ donationare strong, we would expect defaults to havelittle or no effect. However, as can be seen inthe figure (page 1338, bottom), defaults ap-pear to make a large difference: the four opt-in countries (gold) had lower rates than thesix opt-out countries (blue). The two distri-butions have no overlap, and nearly 60 per-centage points separate the two groups. Onereason these results appear to be greater thanthose in our laboratory study is that the costof changing from the default is higher; it in-volves filling out forms, making phonecalls, and sending mail. These low rates ofagreement to become a donor come, insome cases, despitemarked efforts to in-crease donation rates. Inthe Netherlands, for ex-ample, the 1998 cre-ation of a national donorregistry was accompa-nied by an extensive ed-ucational campaign anda mass mailing (of morethan 12 million letters ina country of 15.8 mil-lion) asking citizens toregister, which failed tochange the effectiveconsent rate (26).
Do increases inagreement rates resultin increased rates of do-nation? There are many reasons preventingregistered potential donors from actuallydonating. These include: families’ objec-tions to a loved one’s consent, doctors’ hes-itancy to use a default option, and a mis-match with potential recipients, as well asdifferences in religion, culture, and infra-structure.
To examine this, we analyzed the actualnumber of cadaveric donations made permillion on a slightly larger list of countries,with data from 1991 to 2001 (27). We ana-lyzed these data using a multiple regressionanalysis with the actual donation rates as de-pendent measures and the default as a pre-dictor variable. To control for other differ-ences in countries’ propensity to donate,transplant infrastructure, educational level,and religion, we included variables known to
serve as proxies for these constructs (5) andan indicator variable representing each year.
This analysis presents a strong conclu-sion. Although there are no differencesacross years, there is a strong effect of the de-fault: When donation is the default, there is a16.3% (P < 0.02) increase in donation, in-creasing the donor rate from 14.1 to 16.4million (see figure, this page, blue line).Using similar techniques, but looking only at1999 for a broader set of European countries,including many more from Eastern Europe,Gimbel et al. (5) report an increase in therate from 10.8 to 16.9, a 56.5% increase (seefigure, this page, red line). Differences in theestimates of size may be due to differences inthe countries included in the analysis: Manyof the countries examined by Gimbel et al.had much lower rates of donation.
ConclusionsHow should policy-makers choose defaults?First, consider that every policy must have ano-action default, and defaults impose physi-cal, cognitive, and, in the case of donation,emotional costs on those who must changetheir status. As noted earlier, both national
surveys and the no-de-fault condition in our ex-periment suggest thatmost Americans favororgan donation. This im-plies that explicit con-sent policies impose thecosts of switching on theapparent majority (28).
Second, note that de-faults can lead to twokinds of misclassifica-tion: willing donorswho are not identifiedor people who becomedonors against theirwishes. Balancing theseerrors with the gooddone by the lives saved
through organ transplantation leads to deli-cate ethical and psychological questions.These decisions should be informed by fur-ther research examining the role of the threecauses of default effects. For example, onemight draw different conclusions if the ef-fect of defaults on donation rates is due pri-marily to the physical costs of responding,than if they were due to loss aversion.
The tradeoff between errors of classifi-cation and physical, cognitive, and emo-tional costs must be made with the knowl-edge that defaults make a large differencein lives saved through transplantation.
Our data and those of Gimbel et al. sug-gest changes in defaults could increase do-nations in the United States of additionalthousands of donors a year. Because eachdonor can be used for about three trans-
plants, the consequences are substantial inlives saved. Our results stand in contrastwith the suggestion that defaults do notmatter (29). Policy-makers performinganalysis in this and other domains shouldconsider that defaults make a difference.
References and Notes1. The Gallup Organization, “The American Public’s
Attitude Toward Organ Donation and Trans-plantation” (Gallup Organization, Princeton, NJ,1993).
2. S. M. Gold, K. Shulz, U. Koch, The Organ DonationProcess: Causes of the Organ Shortage andApproaches to a Solution (Federal Center for HealthEducation, Cologne, 2001),
3. H. Gäbel, H. N. Rehnqvist, Transplant. Proc. 29, 3093(1997).
4. C. Conesa et al., , Transplant. Proc. 35,1276 (2003).5. R. W. Gimbel, M. A. Strosberg, S. E. Lehrman, E.
Gefenas, F. Taft, Progr. Transplant. 13, 17 (2003).6. R. H. Thaler, C. Sunstein, Univ. Chicago Law Rev., in
press.7. C. Camerer, S. Issacharoff, G. Loewenstein, T.
O’Donoghue, M. Rabin, Univ. Penn. Law Rev. 151,2111 (2003).
8. M. Clay, W. Block, J. Soc. Polit. Econ. Stud. 27, 227(2002).
9. J. Harris, C. Erin, BMJ 325, 114 (2002).10. C. E. Harris, S. P. Alcorn, Issues Law Med. 3, 213 (2001).11. D. Josefson, BMJ 324, 1541 (2002).12. J. Harris, J. Med. Ethics 29, 303 (2003).13. J. S.Wolf, E. M. Servino, H. N. Nathan, Transplant. Proc.
29, 1477 (1997).14. J. W. Payne, J. R. Bettman, E. J. Johnson, Annu. Rev.
Psychol. 43, 87 (1992).15. P. Slovic, Am. Psychol. 50, 364 (1995).16. D. Kahneman, A. Tversky, Eds., Choices, Values, and
Frames (Cambridge Univ. Press, Cambridge, 2000).17. J. Baron, I. Ritov, Org. Behav. Hum. Decision Processes
59, 475 (1994).18. W. Samuelson, R. Zeckhauser, J. Risk Uncertainty 1, 7
(1988).19. A. Tversky, D. Kahneman, Q. J. Econ. 106(4), 1039
(1991).20. E. J. Johnson, J. Hershey, J. Meszaros, H. Kunreuther, J.
Risk Uncertainty 7, 35 (1993).21. S. Bellman, E. J. Johnson, G. L. Lohse, Commun. ACM
(Assoc. Comput. Machin.) 44, 25 (February 2001).22. E. J. Johnson, S. Bellman, G. L. Lohse, Marketing Lett.
13, 5 (February 2002).23. B. C. Madrian, D. Shea, Q. J. Econ. 116(1), 1149 (2001).24. Methods and details of analysis are available as sup-
porting material on Science online.25. H. Gäbel, “Donor and Non-Donor Registries in Europe”
(on behalf of the committee of experts on theOrganizational Aspects of Co-operation in OrganTransplantation of the Council of Europe, Brussels,2002).
26. M. C. Oz et al., J. Heart Lung Transplant. 22, 389(2003).
27. We used a times series analysis to account for possi-ble changes in transplant technology and infrastruc-ture, as well as the effects of continuing public edu-cation campaigns.
28. An alternative advocated by the American MedicalAssociation (30) is mandated choice, which imposesthe cost of making an active decision on all. This prac-tice is currently employed in the state of Virginia, but,consistent with the constructive preferences perspec-tive, about 24% of the first million Virginians askedsaid they were undecided (31).
29. A. L. Caplan, JAMA 272, 1708 (1994).30. American Medical Association, “Strategies for cadav-
eric organ procurement: Mandated choice and pre-sumed consent” (American Medical Association,Chicago, 1993).
31. A. C. Klassen, D. K. Klassen, Ann. Intern. Med. 125, 70(1996).
32. This research has been supported by the ColumbiaUniversity Center for Decision Science and theColumbia Business School Center for Excellence in E-Business. We thank L. Roels for providing the data onactual donation rates.
Supporting Online Materialwww.sciencemag.org/cgi/content/full/302/5649/1338/
DC1
Opt-in Opt-outDefault
Do
nat
ion
rat
e p
er m
illio
n
9
11
13
15
17
19
Estimated donation rate, opt-in versus
opt-out, as a function of default,
1991–2001. Means ± SEM; this paper,
blue; Gimbel et al. (5), red.
P O L I C Y F O R U M
www.sciencemag.org SCIENCE VOL 302 21 NOVEMBER 2003
Recommended