Disease related symptoms session 4 :
Coagulation disorder
Board review in oncology pharmacy 2013 “Managing Disease – or – Treatment Related Complication”
Suthan Chanthawong, B. Pharm, RPh.
Identify risk factors for VTE
Develop a patient-specific plan
Provide counseling to the individual receiving anticoagulant treatment
Describe the management of an individual with cancer who experiences bleeding or INR above goal range
Objectives
Coagulation disorder
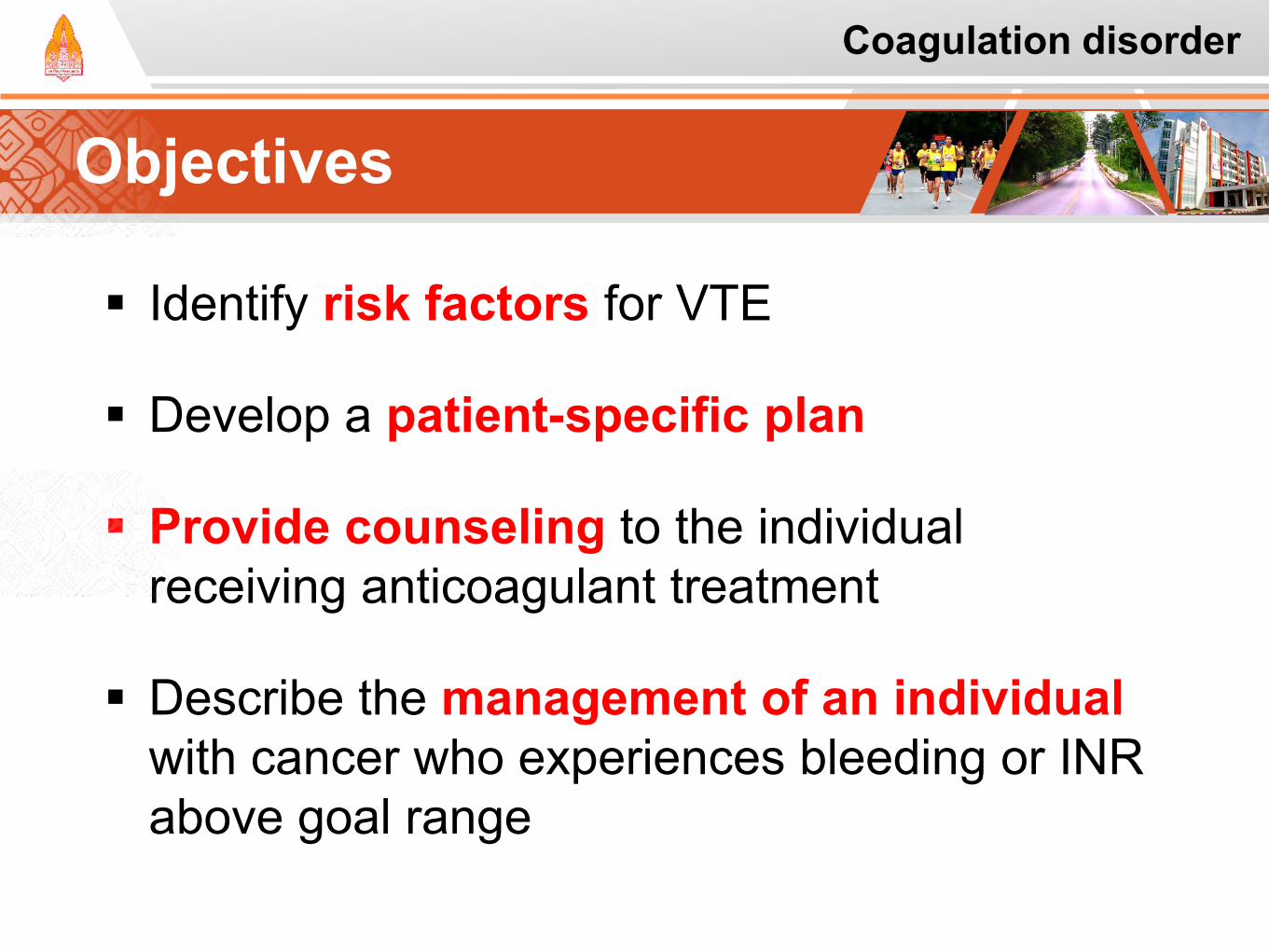
Lectures in Clinical Medicine Association recognized since Trousseau’s
observation more than 130 years ago1
Of all cases of VTE, approximately 4-20% occur in cancer patients.2
VTE has been reported in up to 50% on postmortem examination.3-4
Cancer-associated VTE has important clinical and economic consequences5-7
Armand Trousseau
1. Trousseau, Armand. In Clinique Medicale de l'Hôtel-Dieu de Paris, 2nd ed. Paris: J.B. Bailliere et Fils; 1865 2. Lee AY. Br J. Haematol. 2005;128:291-302. 3. Gao S et al: Expert Rev Anticncer Ther 2004; 4: 303-320.
4. Lyman GH et al: J Clin Oncol 2007; 25: 5490-5505. 5. Sorensen HT, et al. N Engl J Med. 2000;343:1846-1850. 6. Prandoni P, et al. Blood. 2002;100:3484-3488. 7. Khorana AA, et al. J Clin Oncol. 2006;24:484-490.
Patients with cancer: 20%
All deep venous thrombosis and
pulmonary embolism
Coagulation disorder
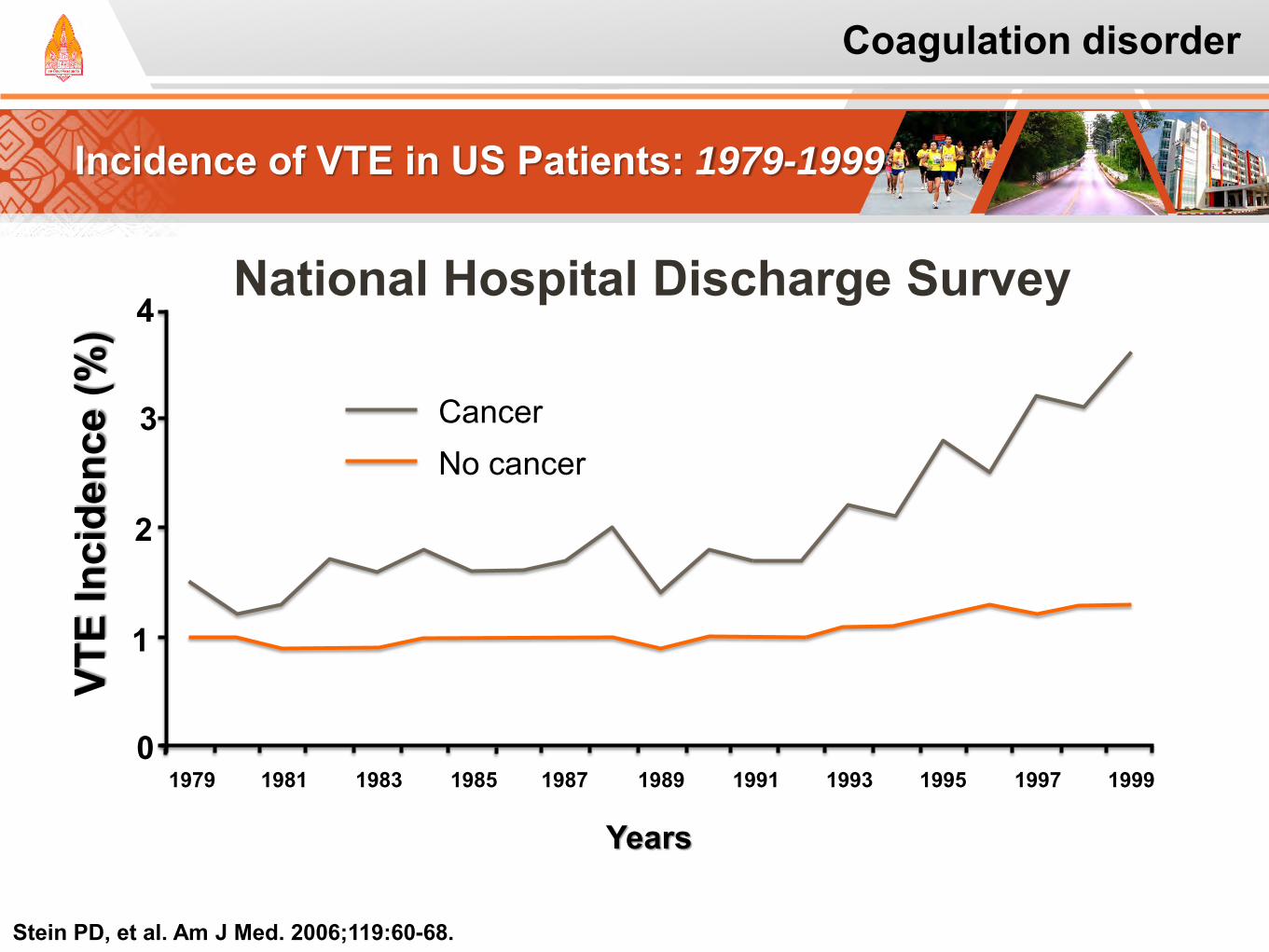
Incidence of VTE in US Patients: 1979-1999
1979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999
1
0
2
3
4 National Hospital Discharge Survey
VTE
Inci
denc
e (%
)
Cancer No cancer
Years
Stein PD, et al. Am J Med. 2006;119:60-68.
Coagulation disorder
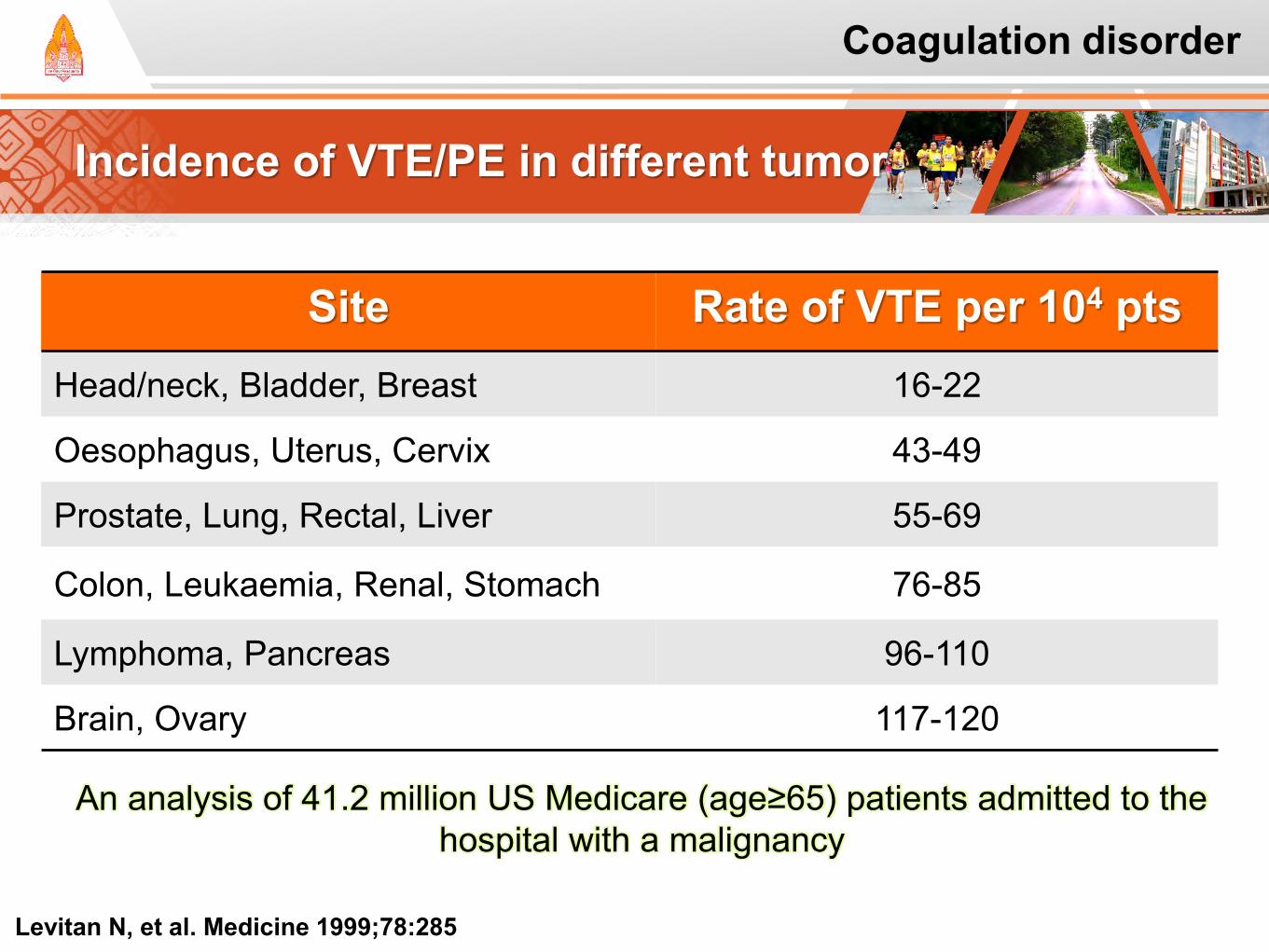
Incidence of VTE/PE in different tumor
Levitan N, et al. Medicine 1999;78:285
An analysis of 41.2 million US Medicare (age≥65) patients admitted to the hospital with a malignancy
Site Rate of VTE per 104 pts Head/neck, Bladder, Breast 16-22
Oesophagus, Uterus, Cervix 43-49
Prostate, Lung, Rectal, Liver 55-69
Colon, Leukaemia, Renal, Stomach 76-85
Lymphoma, Pancreas 96-110
Brain, Ovary 117-120
Coagulation disorder
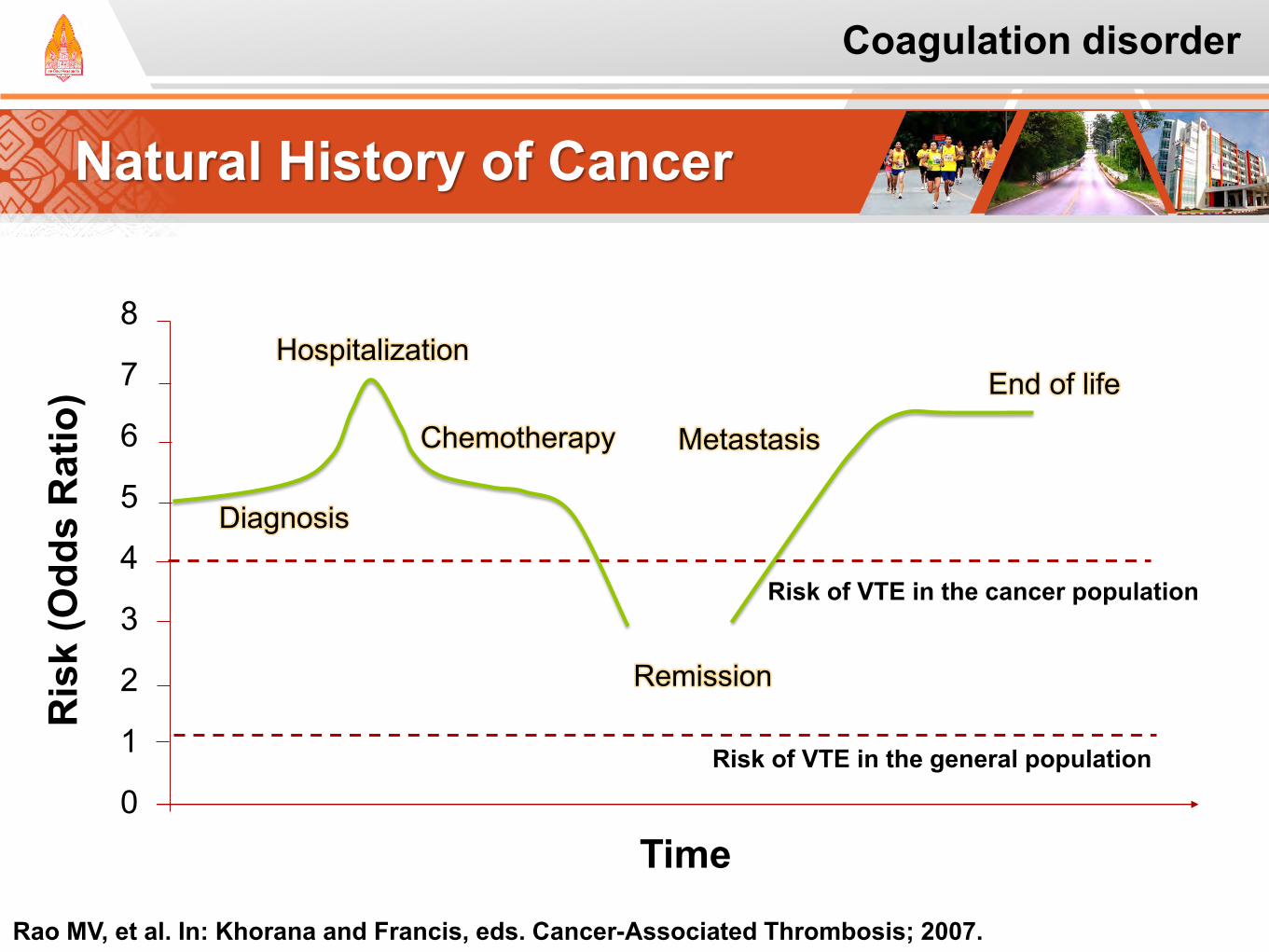
Natural History of Cancer
8
7
6
5
4
3
2
1
0
Chemotherapy
Risk of VTE in the cancer population
Remission
Risk of VTE in the general population
Time
Diagnosis
Metastasis
End of life Hospitalization
Ris
k (O
dds
Rat
io)
Rao MV, et al. In: Khorana and Francis, eds. Cancer-Associated Thrombosis; 2007.
Coagulation disorder
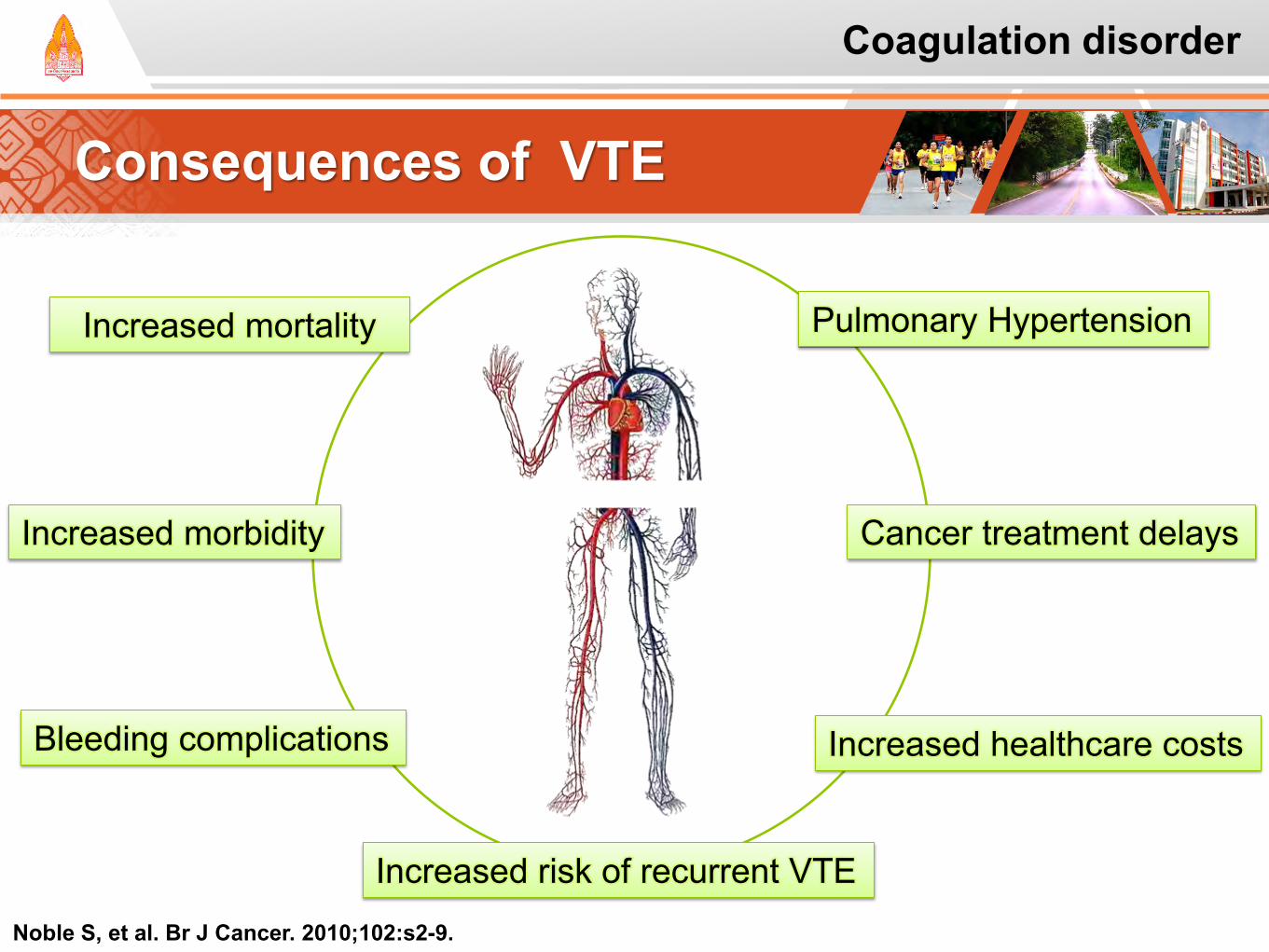
Consequences of VTE
Noble S, et al. Br J Cancer. 2010;102:s2-9.
Increased mortality
Increased morbidity
Increased risk of recurrent VTE
Bleeding complications
Pulmonary Hypertension
Cancer treatment delays
Increased healthcare costs
Coagulation disorder
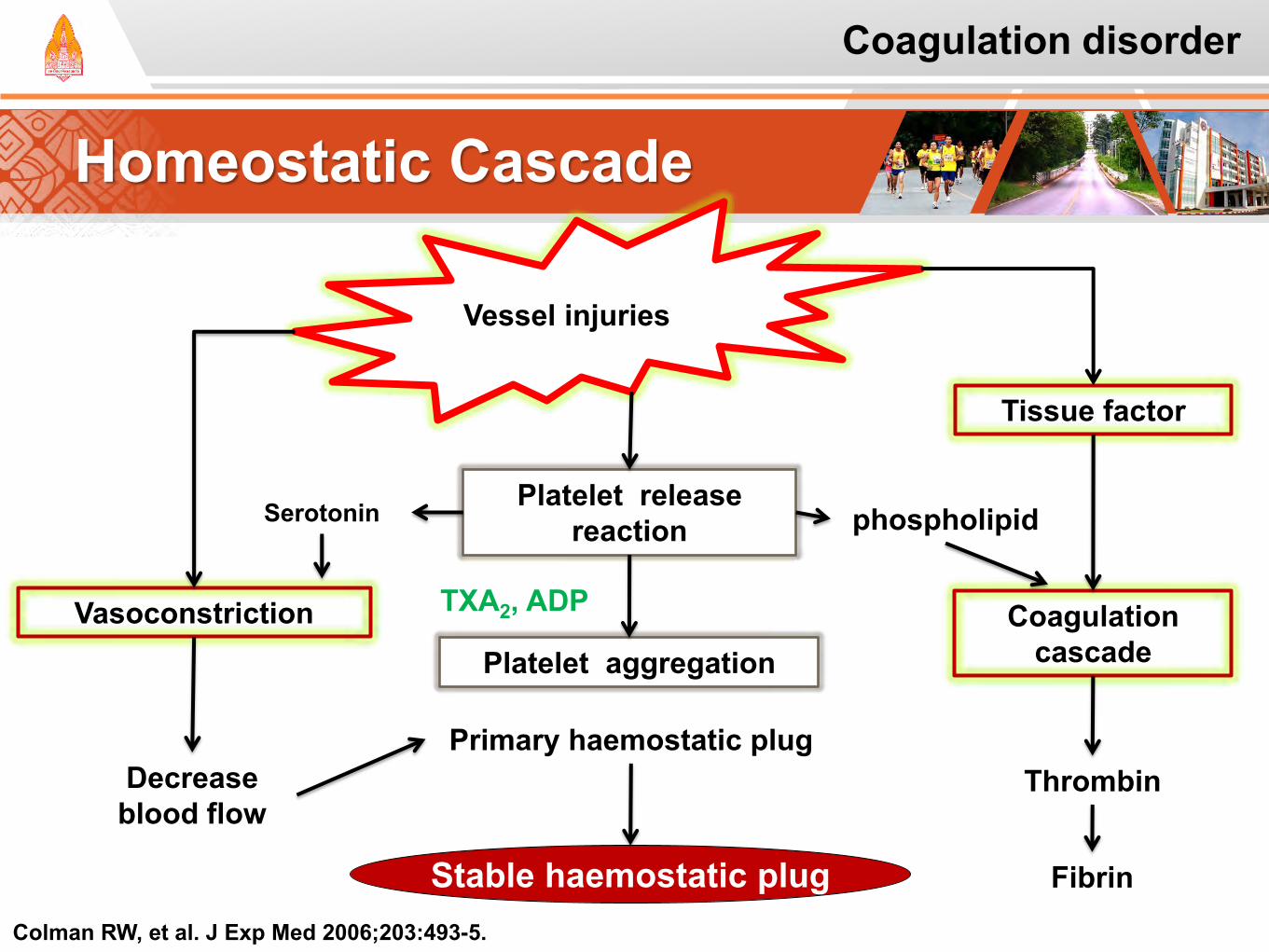
Homeostatic Cascade
Colman RW, et al. J Exp Med 2006;203:493-5.
Vessel injuries
Vasoconstriction
Decrease blood flow
Platelet release reaction Serotonin
Platelet aggregation
TXA2, ADP
Primary haemostatic plug
Stable haemostatic plug
Tissue factor
Coagulation cascade
Thrombin
Fibrin
phospholipid
Coagulation disorder
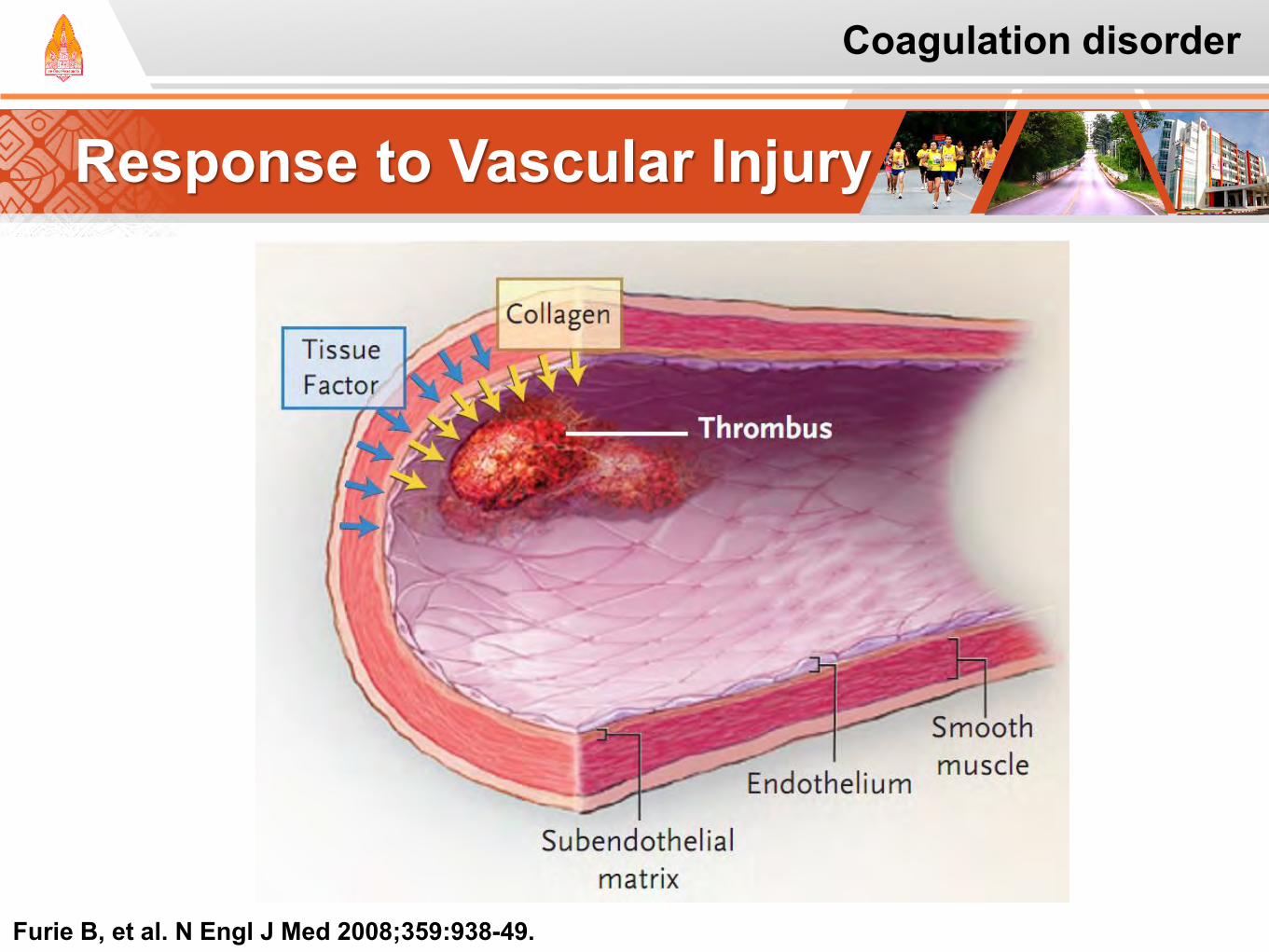
Response to Vascular Injury
Furie B, et al. N Engl J Med 2008;359:938-49.
Coagulation disorder
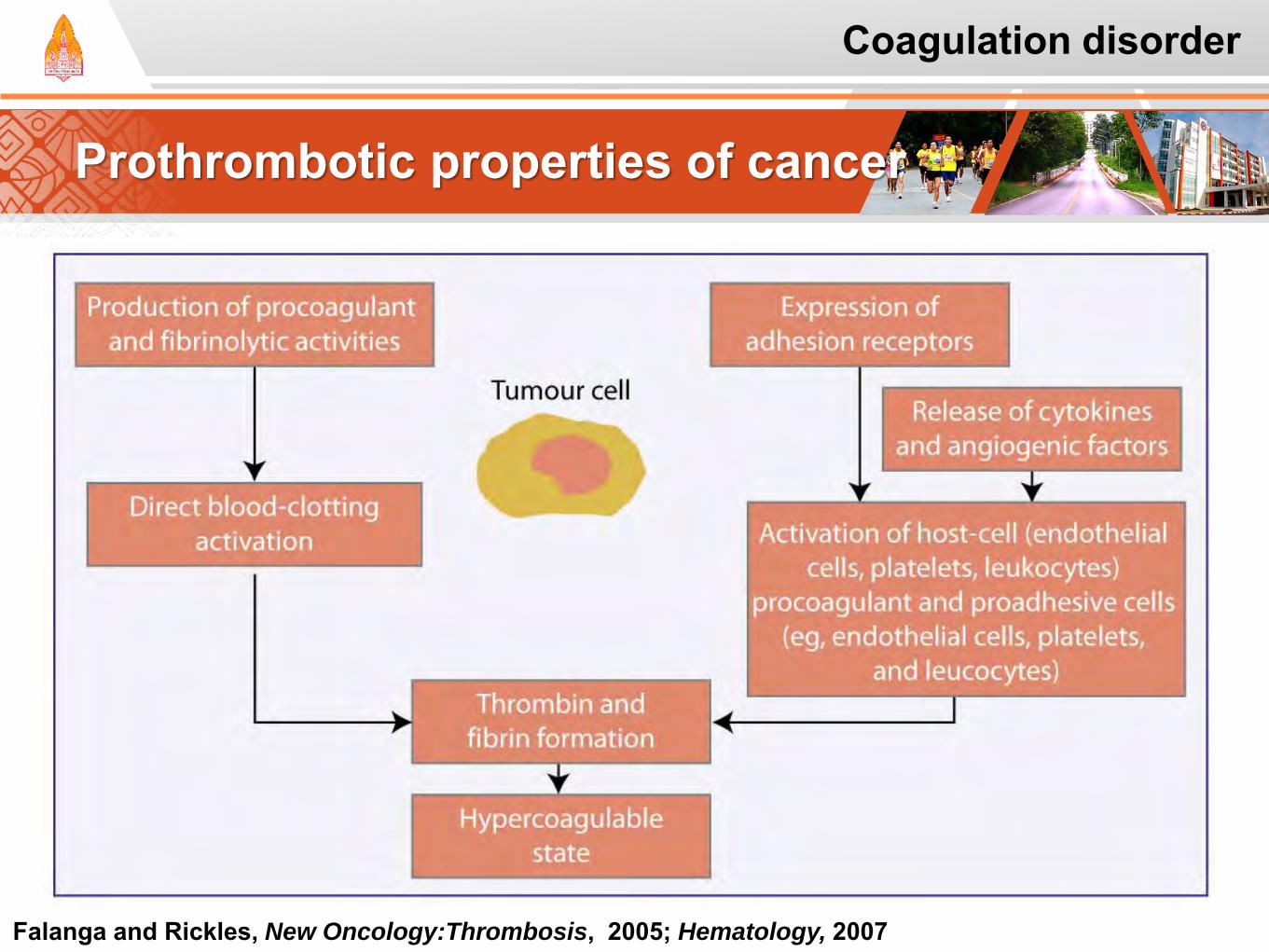
Prothrombotic properties of cancer
Falanga and Rickles, New Oncology:Thrombosis, 2005; Hematology, 2007
Coagulation disorder
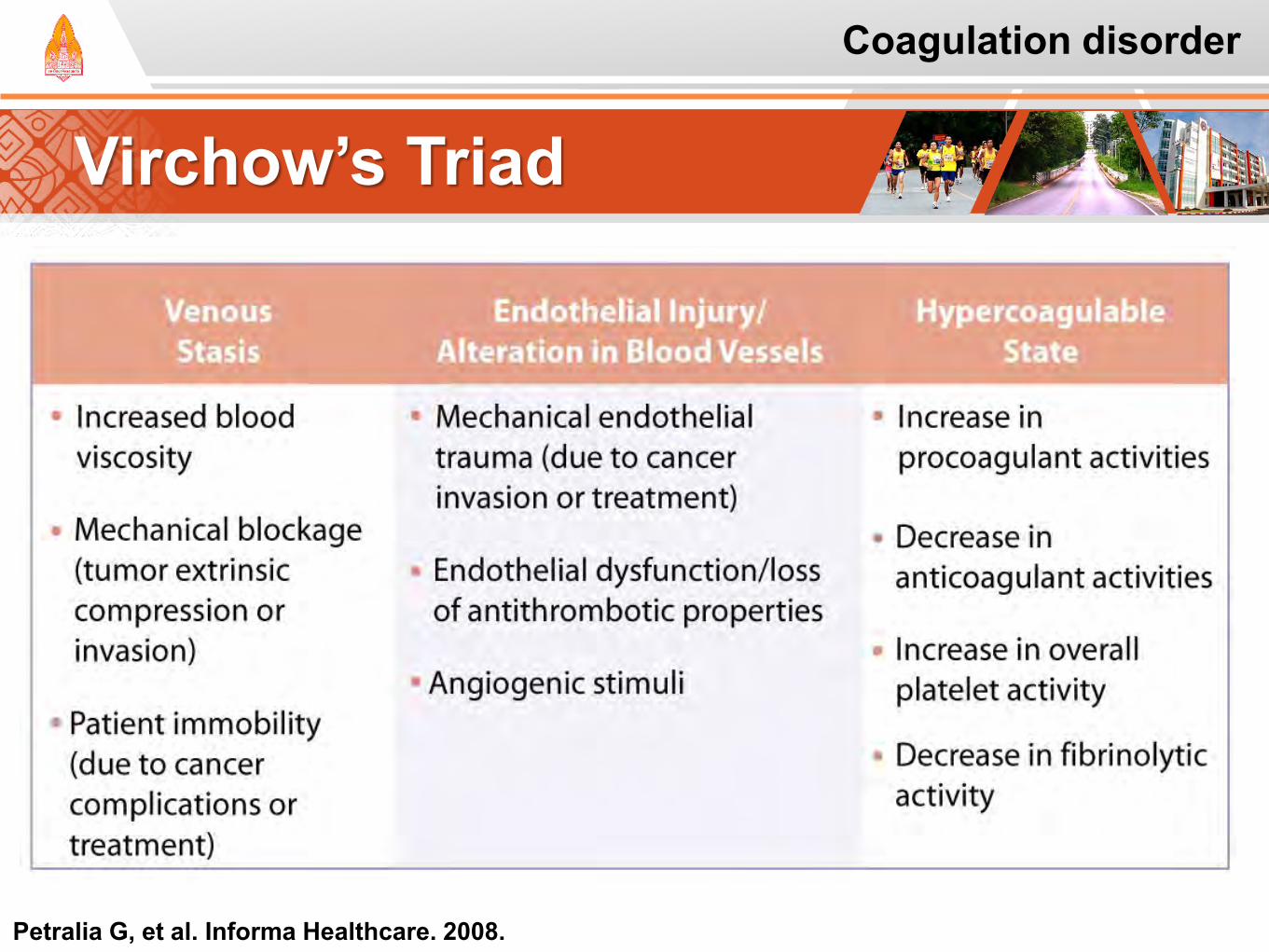
Virchow’s Triad
Petralia G, et al. Informa Healthcare. 2008.
Coagulation disorder
Case study: Uraka
Coagulation disorder
UK is a 56-year-old woman recently diagnosed with colon cancer. She has had resection of the cancer.
She is scheduled to start adjuvant chemotherapy with oxaliplatin, fluorouracil, and leucovorin (FOLFOX).
Last week, a central venous catheter (CVC) was placed to facilitate the administration of the IV fluorouracil.
She now reports some swelling in her arm on the same side as the CVC.
She concern about the risk of a blood clot.
Case study: Uraka
Coagulation disorder
Questions: What is/are risk factor(s) for VTE UK?
What is appropriate counseling for UK?
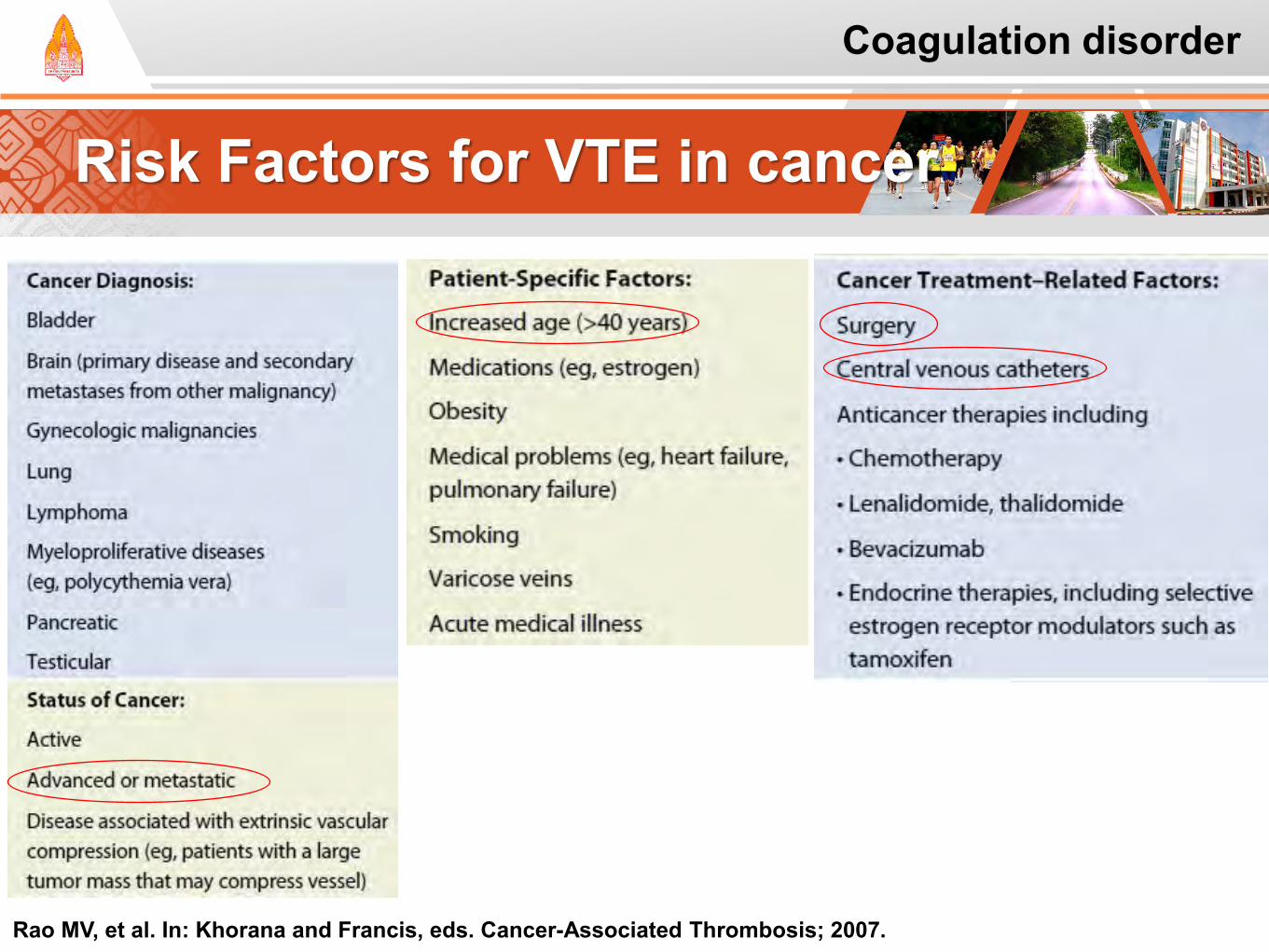
Risk Factors for VTE in cancer
Rao MV, et al. In: Khorana and Francis, eds. Cancer-Associated Thrombosis; 2007.
Coagulation disorder
Case study: Risk Factors
Coagulation disorder
Diagnosis of Colon cancer: It is important to realize that she has received a
curative surgery for the treatment of colon cancer, and does not have active disease at this time.
Surgery also increases risk of thrombosis.
She has a CVC.
While she has not yet started chemotherapy, it will pose a risk once therapy is initiated.
Case study: Counseling
Coagulation disorder
Recommend that UK seek medical advice immediately to have the situation evaluated with appropriate imaging. This is not a diagnosis that should be made based on clinical symptoms alone.
Encourage the patient to contact her oncology team, as most oncology teams have on-call numbers available for this type of issue.
Encourage the patient to seek medical evaluation immediately, and not to wait until her next appointment.

Diagnosis of VTE Overview
Sign and Symptom DVT Leg pain, tenderness, ankle oedema, calf
tenderness, and swelling, dilated veins, and Homan’s sign (a sharp pain on dorsiflexion of the foot)
PE The signs and symptoms are present to varying degrees in patients with DVT
That objective testing must be carried out to confirm the diagnosis of DVT
Haeger K, et al. Angiology 1969;20:219-23.
Coagulation disorder
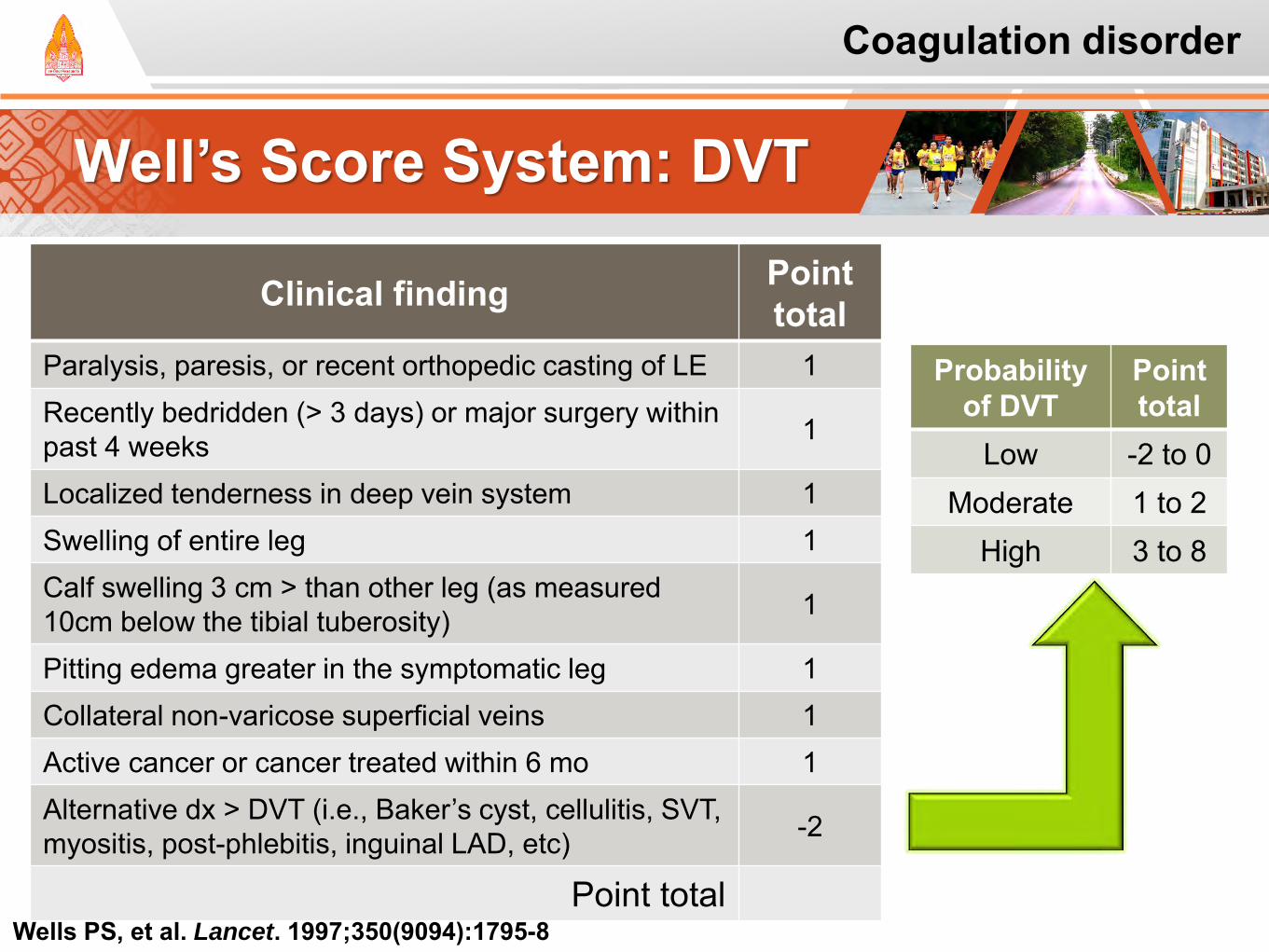
Well’s Score System: DVT
Clinical finding Point total
Paralysis, paresis, or recent orthopedic casting of LE 1 Recently bedridden (> 3 days) or major surgery within past 4 weeks 1
Localized tenderness in deep vein system 1 Swelling of entire leg 1 Calf swelling 3 cm > than other leg (as measured 10cm below the tibial tuberosity) 1
Pitting edema greater in the symptomatic leg 1 Collateral non-varicose superficial veins 1 Active cancer or cancer treated within 6 mo 1 Alternative dx > DVT (i.e., Baker’s cyst, cellulitis, SVT, myositis, post-phlebitis, inguinal LAD, etc) -2
Point total
Probability of DVT
Point total
Low -2 to 0 Moderate 1 to 2
High 3 to 8
Wells PS, et al. Lancet. 1997;350(9094):1795-8
Coagulation disorder
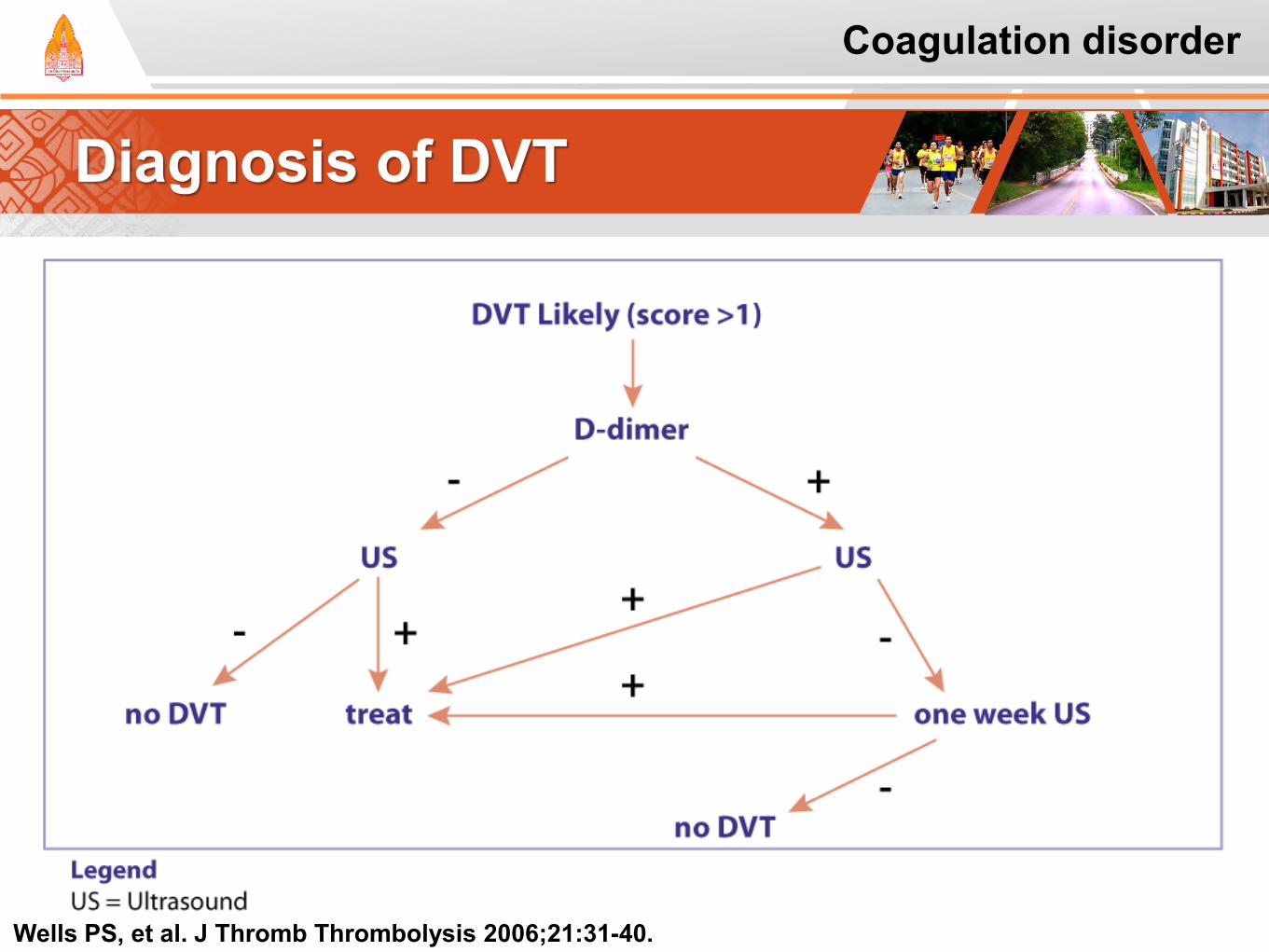
Diagnosis of DVT
Wells PS, et al. J Thromb Thrombolysis 2006;21:31-40.
Coagulation disorder
Laboratory testing: PE
Abnormalities on ECG: Unexplained tachycardia
Chest radiographs
Arterial PO2 and the alveolar-arterial oxygen
Elevation of D-dimer level
Limitation: false positive
Infection, cancer, trauma, and other inflammatory states
Tapson VF, et al. Am J Respir Crit Care Med 1999;160:1043-66. Tapson VF. N Engl J Med 2008;358:1037-52.
Coagulation disorder
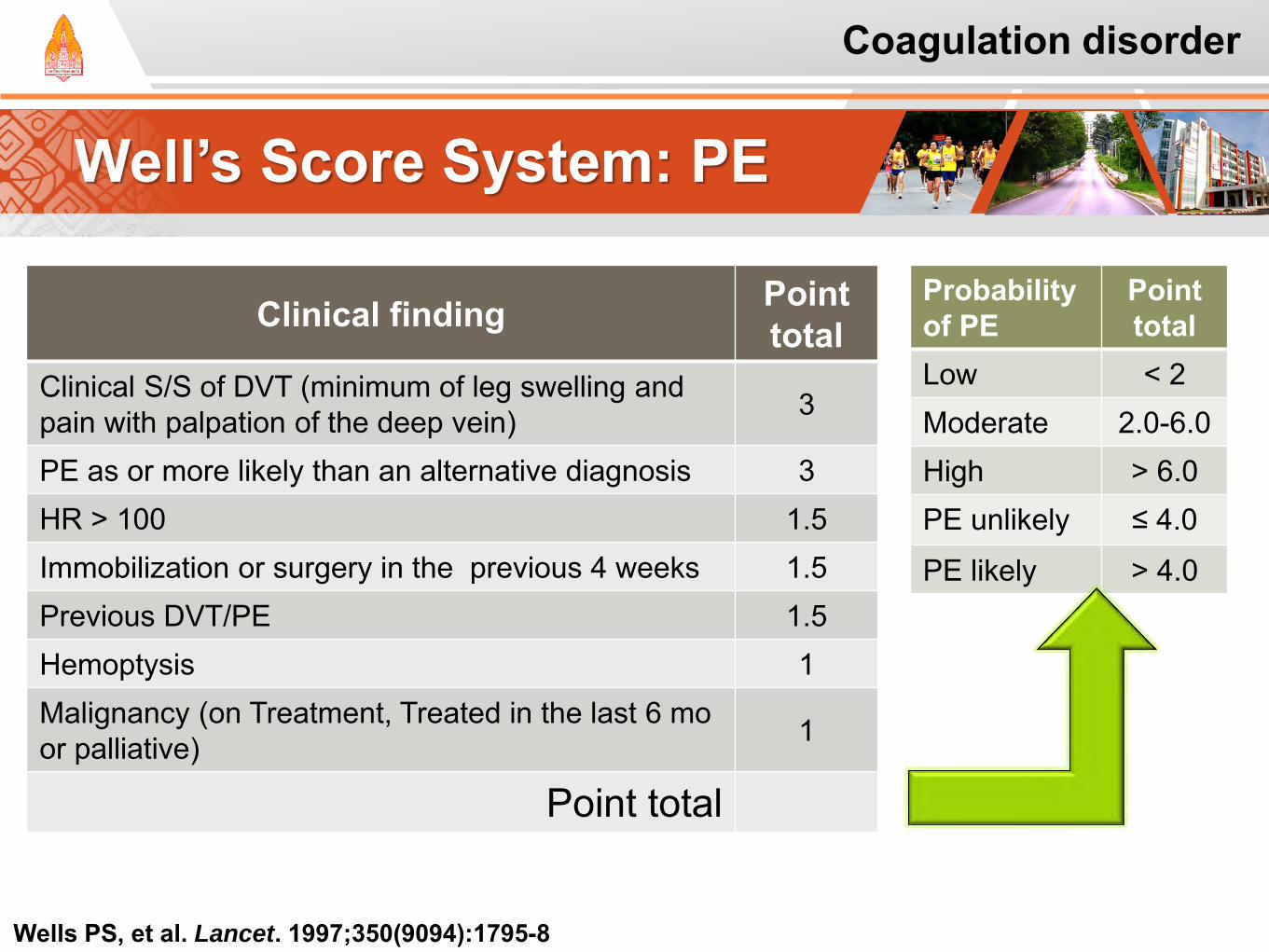
Well’s Score System: PE
Clinical finding Point total
Clinical S/S of DVT (minimum of leg swelling and pain with palpation of the deep vein) 3
PE as or more likely than an alternative diagnosis 3 HR > 100 1.5 Immobilization or surgery in the previous 4 weeks 1.5 Previous DVT/PE 1.5 Hemoptysis 1 Malignancy (on Treatment, Treated in the last 6 mo or palliative) 1
Point total
Probability of PE
Point total
Low < 2 Moderate 2.0-6.0 High > 6.0 PE unlikely ≤ 4.0
PE likely > 4.0
Wells PS, et al. Lancet. 1997;350(9094):1795-8
Coagulation disorder
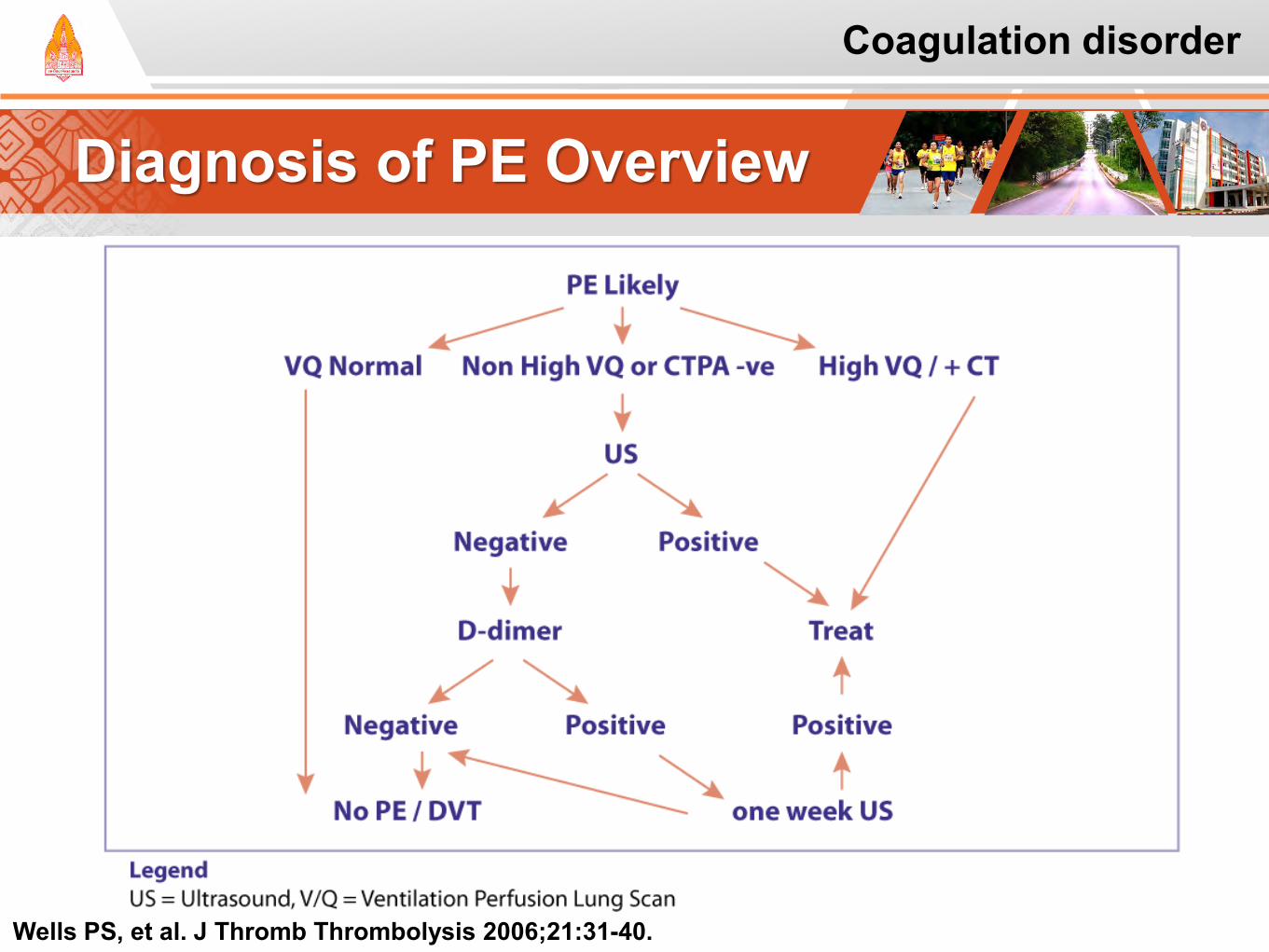
Diagnosis of PE Overview
Wells PS, et al. J Thromb Thrombolysis 2006;21:31-40.
Coagulation disorder
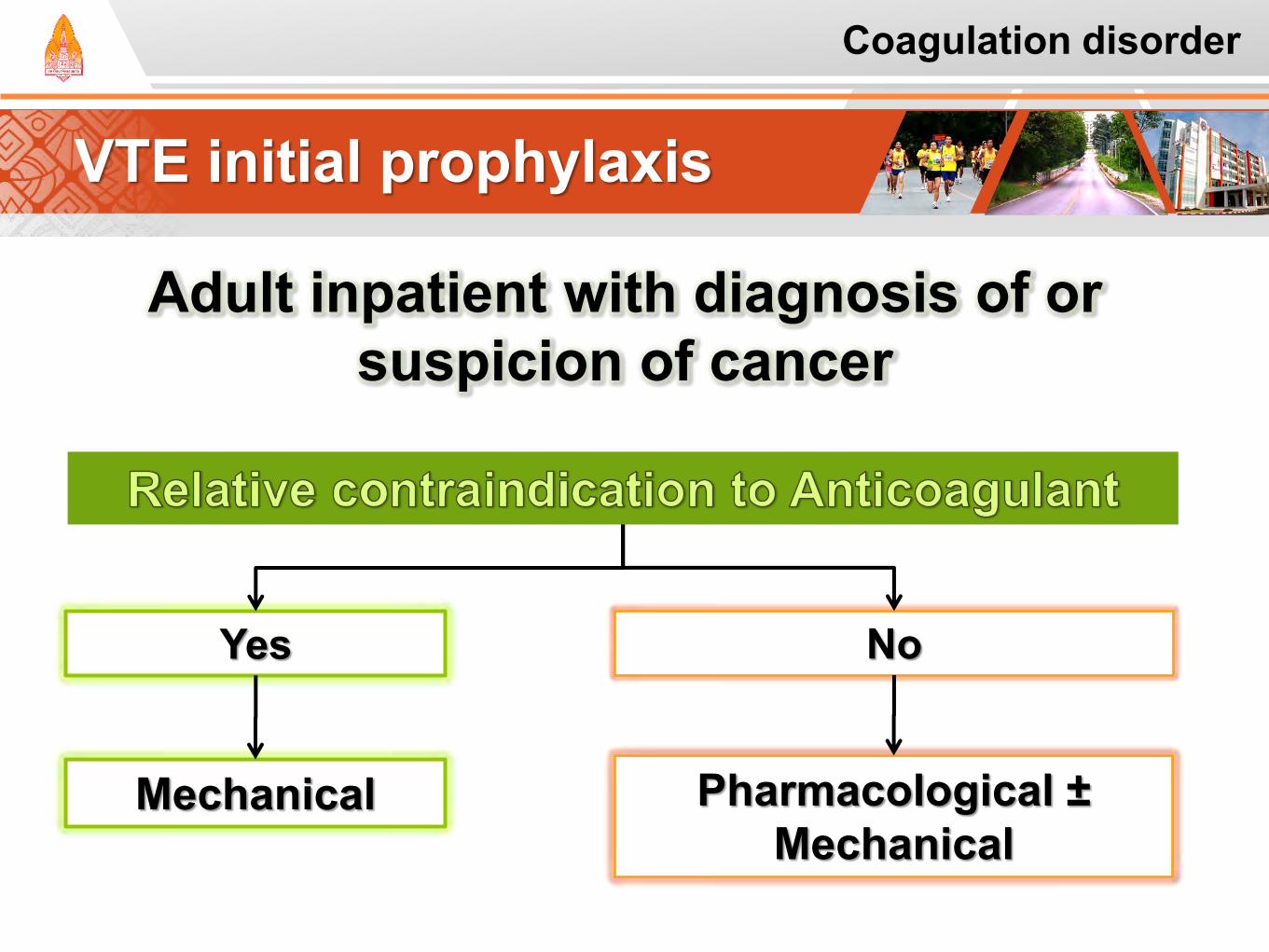
VTE initial prophylaxis
Adult inpatient with diagnosis of or suspicion of cancer
Yes
Mechanical
No
Pharmacological ± Mechanical
Coagulation disorder
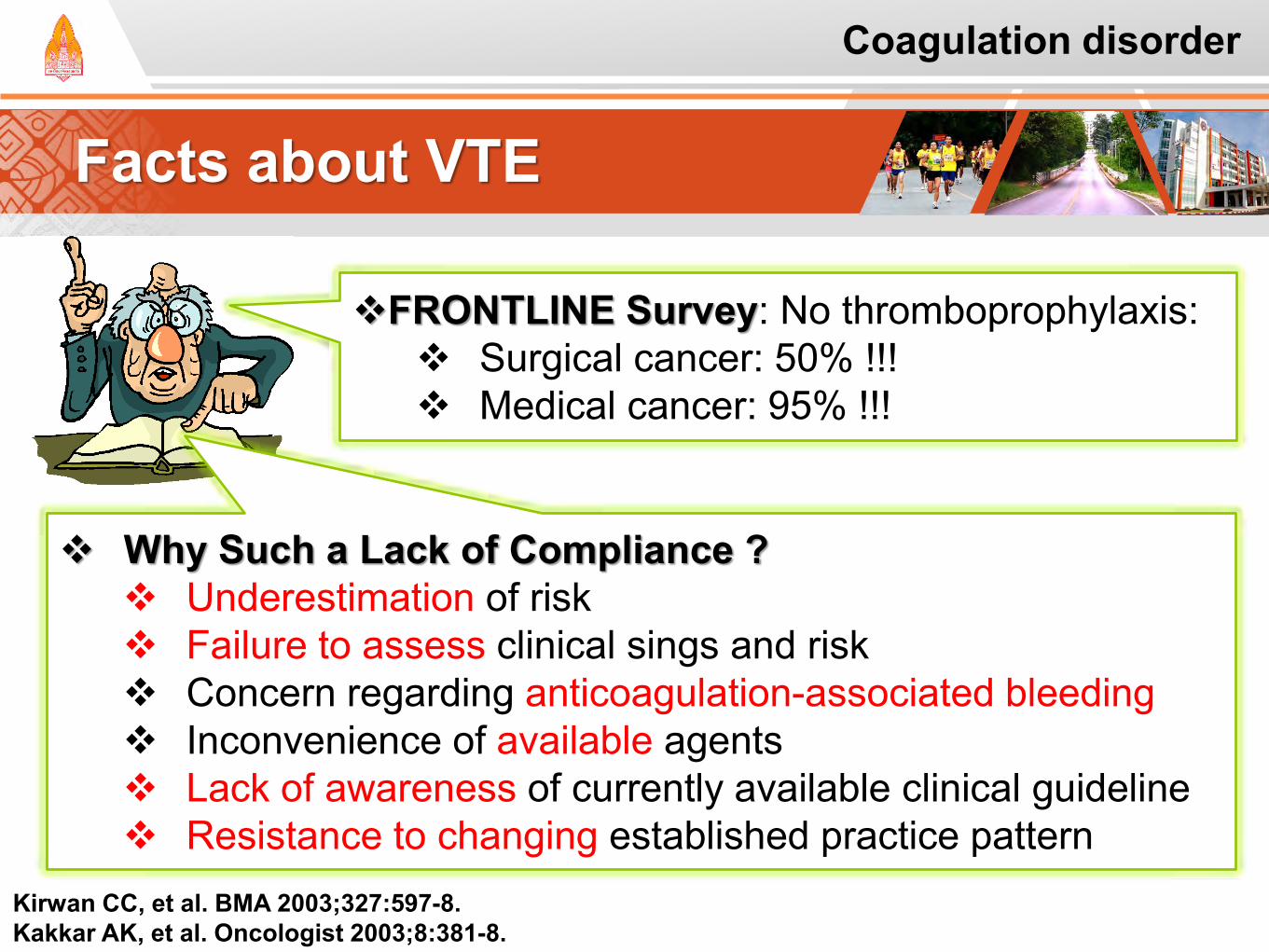
Facts about VTE
Kirwan CC, et al. BMA 2003;327:597-8. Kakkar AK, et al. Oncologist 2003;8:381-8.
FRONTLINE Survey: No thromboprophylaxis: Surgical cancer: 50% !!! Medical cancer: 95% !!!
Why Such a Lack of Compliance ? Underestimation of risk Failure to assess clinical sings and risk Concern regarding anticoagulation-associated bleeding Inconvenience of available agents Lack of awareness of currently available clinical guideline Resistance to changing established practice pattern
Coagulation disorder
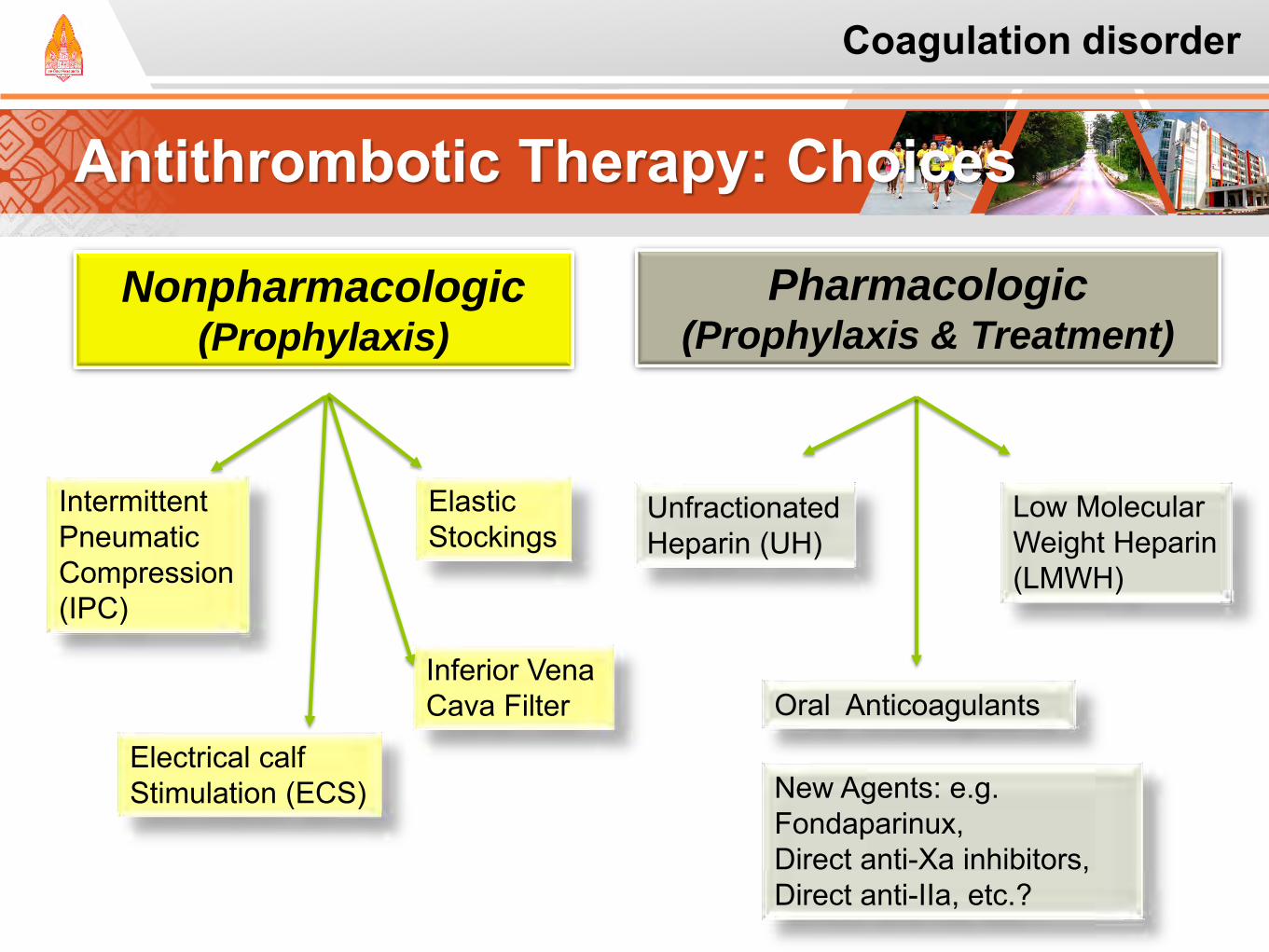
Antithrombotic Therapy: Choices
Pharmacologic (Prophylaxis & Treatment)
Low Molecular Weight Heparin (LMWH)
Nonpharmacologic (Prophylaxis)
Unfractionated Heparin (UH)
Oral Anticoagulants
Elastic Stockings
Inferior Vena Cava Filter
Intermittent Pneumatic Compression (IPC)
New Agents: e.g. Fondaparinux, Direct anti-Xa inhibitors, Direct anti-IIa, etc.?
Electrical calf Stimulation (ECS)
Coagulation disorder
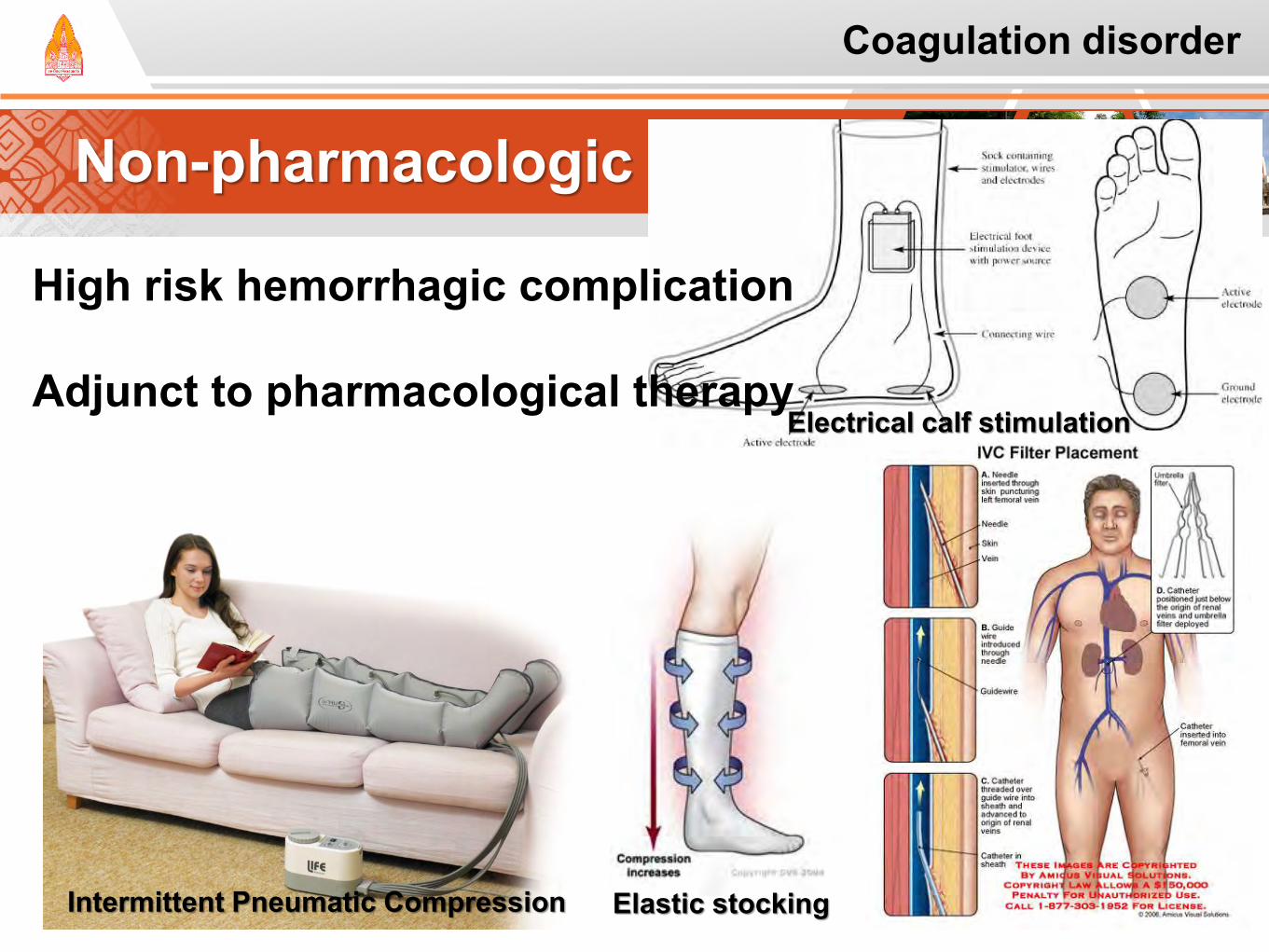
Non-pharmacologic Prophylaxis
High risk hemorrhagic complication
Adjunct to pharmacological therapy
Intermittent Pneumatic Compression Elastic stocking
Electrical calf stimulation
Coagulation disorder
Pharmacologic Prophylaxis
Aspirin
Warfarin
Unfractionated heparin (UFH)
Low molecular weight heparin (LMWH)
Fondaparinux
Coagulation disorder
Aspirin
Limited evidence in cancer In general; Should not be used
as a 1st pharmacological modality
Geerts WH, et al. Chest 2008;133:381s-453s.
Coagulation disorder
Warfarin: Oral Vitamin K antagonist
Rapidly absorption Long t1/2 36-42 hrs Inter-individual variation Narrow therapeutic window Drug-Drug interaction
Zacharski LR, et al. Oncologist 2005;10:72-9. Hutten BA, et al. J Clin Oncol 2000;18:3078-83.
Retrospective study in 2000 Cancer VS non-cancer Intervention: Warfarin 3 mos (keep INR 2-3) Results: Tumor increased incidence of
Recurrence: 27.1/100 vs 9.0/100 pt-yr Bleeding: 13.3/100 vs 2.1/100 pt-yr
Coagulation disorder
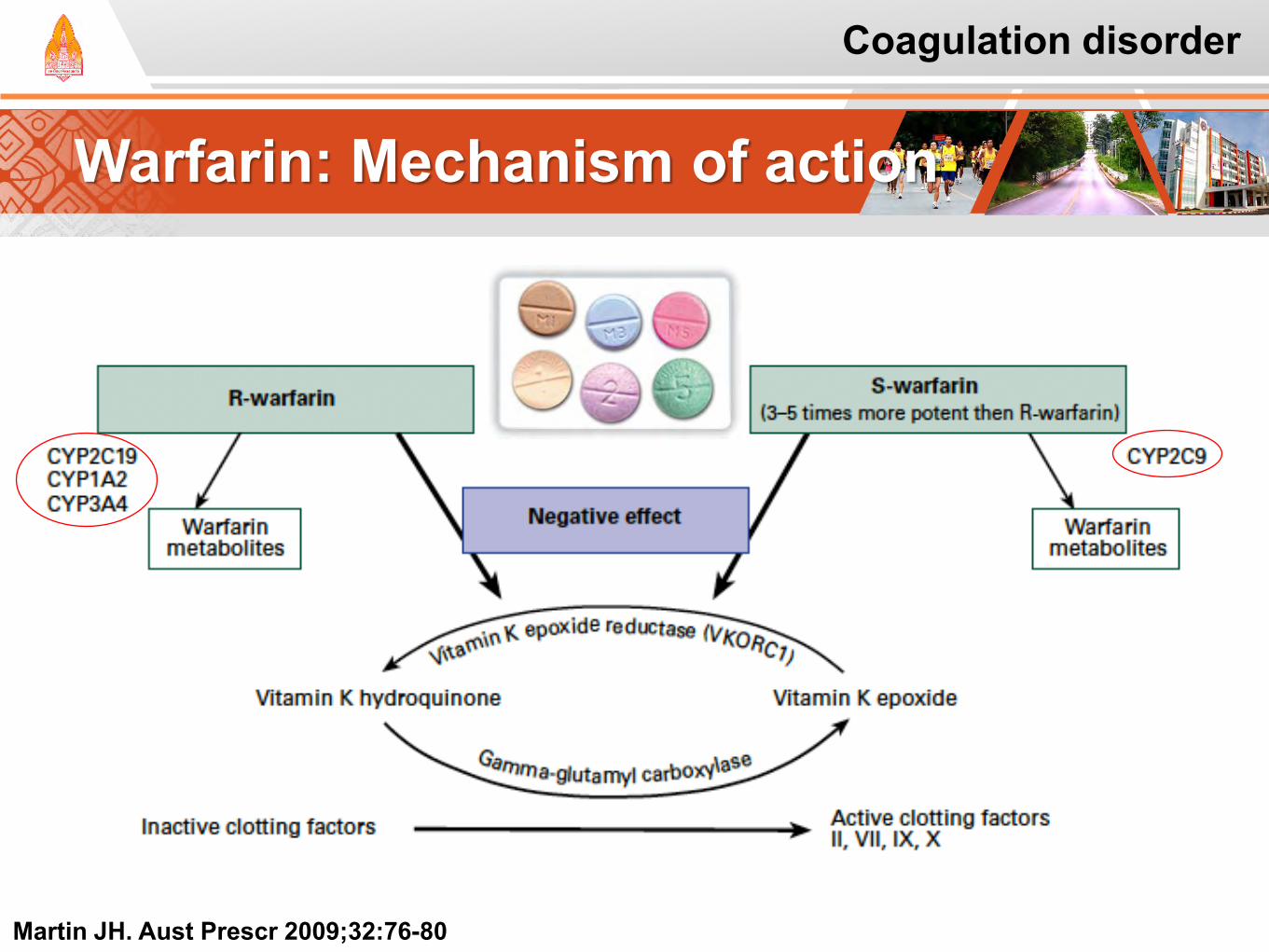
Warfarin: Mechanism of action
Martin JH. Aust Prescr 2009;32:76-80
Coagulation disorder
Warfarin: Interindividual Variability
Redman AR, Pharmacotherapy, 2001; 21:235–242
Coagulation disorder
Unfractionated Heparin
Sulphated-mucopolysaccharides 3000-30,000 Dal (mean 15,000 Dal) Continuous infusion or SQ
Hirsh J, et al. Chest 2008;133:141s-159s.
Important Limitations: High protein binding Non-linear pharmacokinetic Heparin-induced thrombocytopenia (HIT) Osteoporosis Narrow therapeutic window:
aPTT monitoring
Coagulation disorder
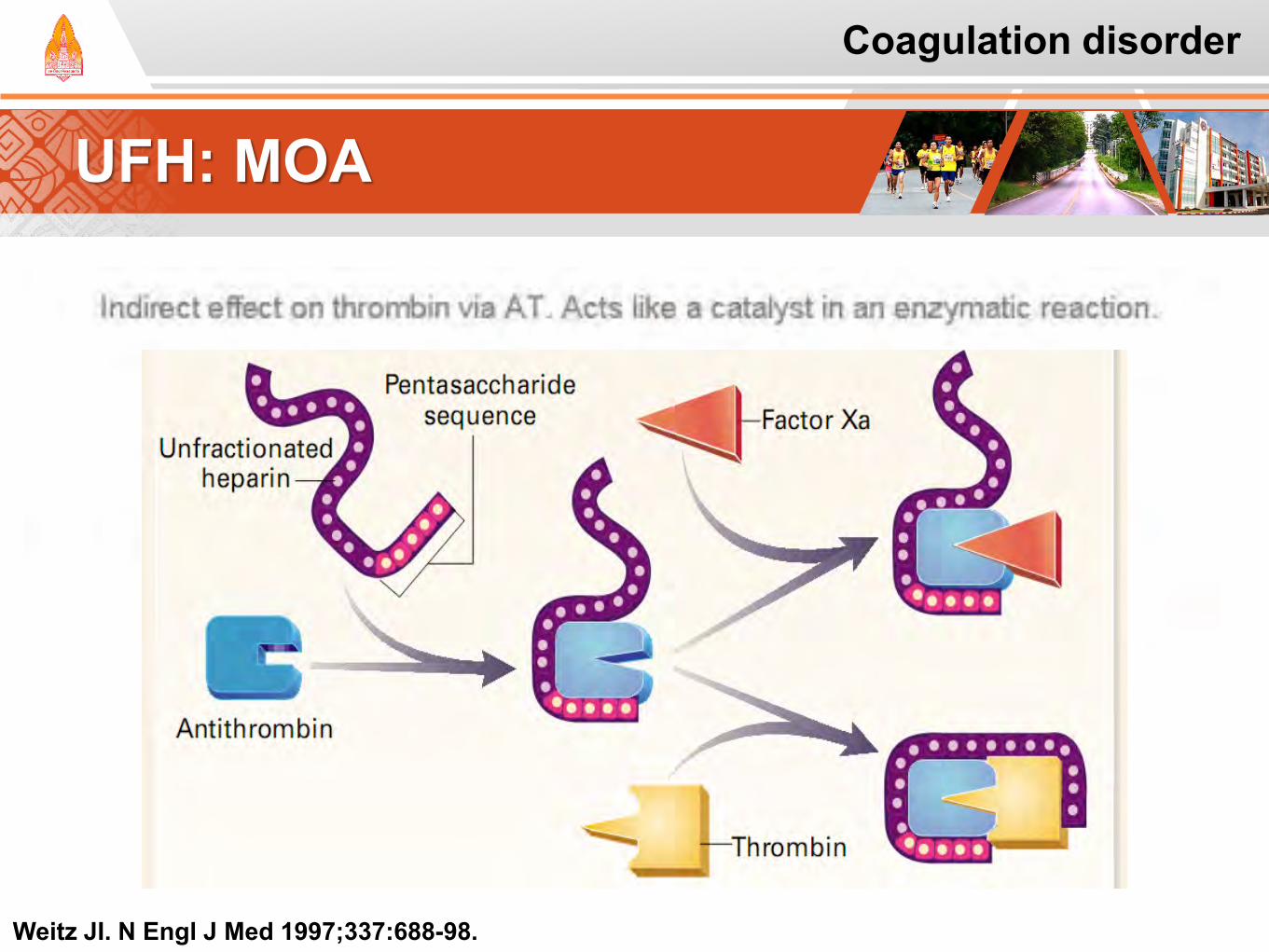
UFH: MOA
Coagulation disorder
Weitz JI. N Engl J Med 1997;337:688-98.
Low Molecular Weight Heparin
Enzymatic depolymerization 4000-5,000 Da Dalteparin, Enoxaparin, Tinzaparin, Nadroparin, Bemiparin Once daily, Fixed or Wt-base Regular monitoring is not indicated
Excepts in obese, renal insufficiency
Hirsh J, et al. Chest 2008;133:141s-159s.
Benefits: Improve anticogulant effect Improve PK profile Reduced propensity:
Osteoporosis HIT
Coagulation disorder
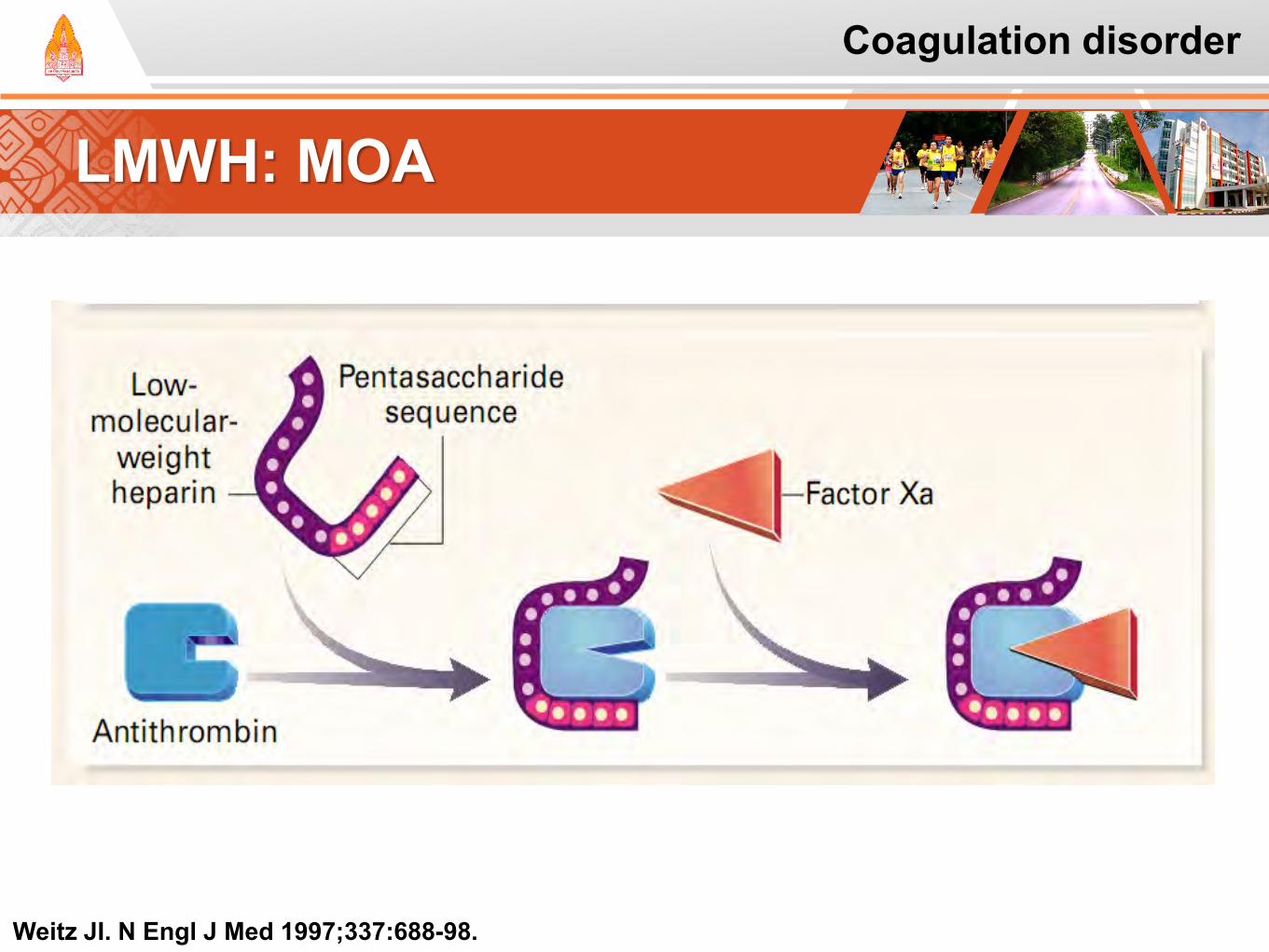
LMWH: MOA
Weitz JI. N Engl J Med 1997;337:688-98.
Coagulation disorder
Fondaparinux
AT-binding polysaccharide Act through AT-mediating selective inhibition of factor Xa Fixed dose 2.5 mg S.Q. Regular monitoring is not indicated
Hirsh J, et al. Chest 2008;133:141s-159s.
Coagulation disorder
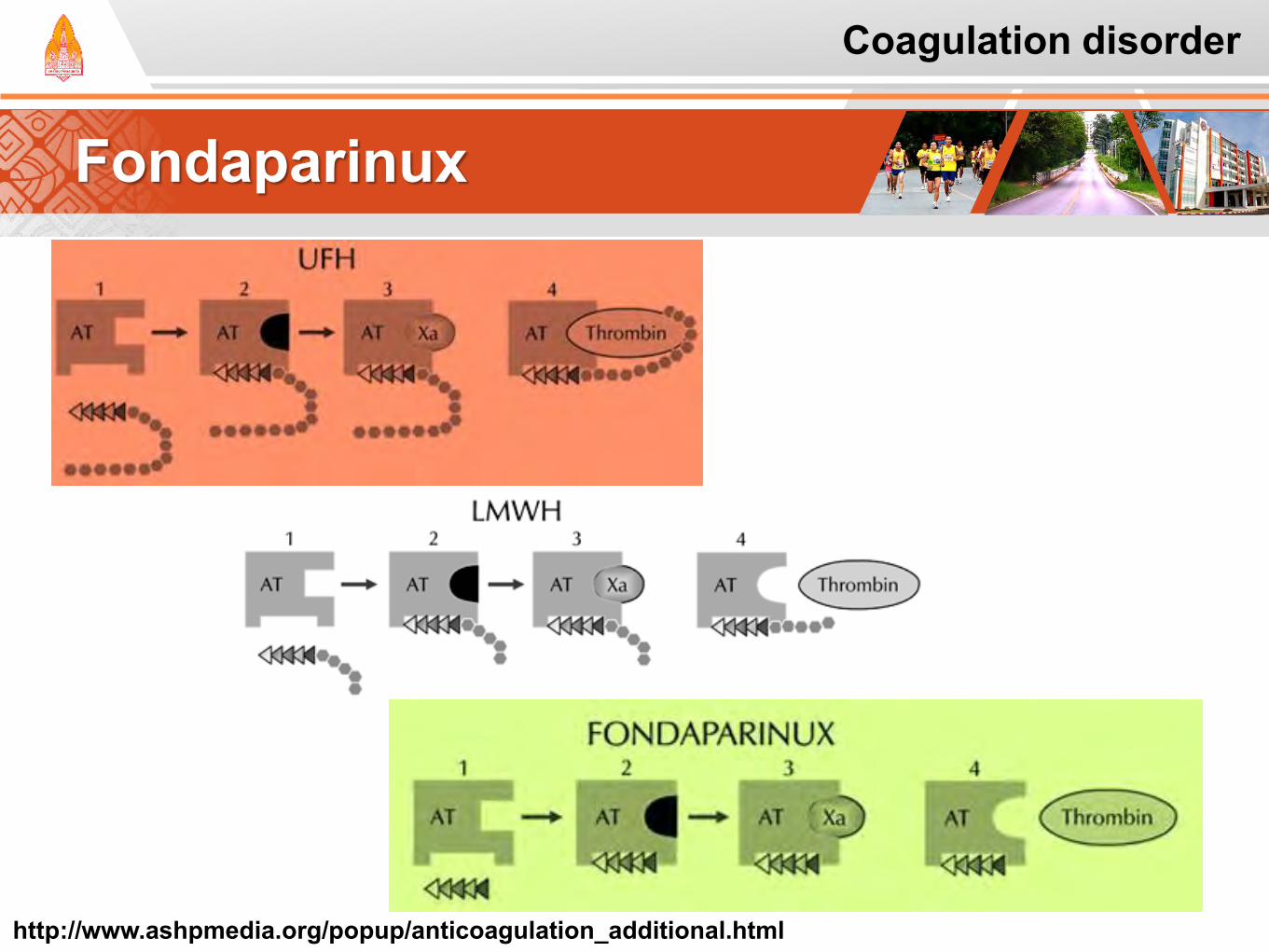
Fondaparinux
http://www.ashpmedia.org/popup/anticoagulation_additional.html
Coagulation disorder
VTE Prophylaxis and Treatment
Prophylaxis in
Hospitalized Patient
Prophylaxis in
ambulatory patients
Prophylaxis in patients undergoing
surgery
Treatment of VTE and
prevention of recurrent
Coagulation disorder
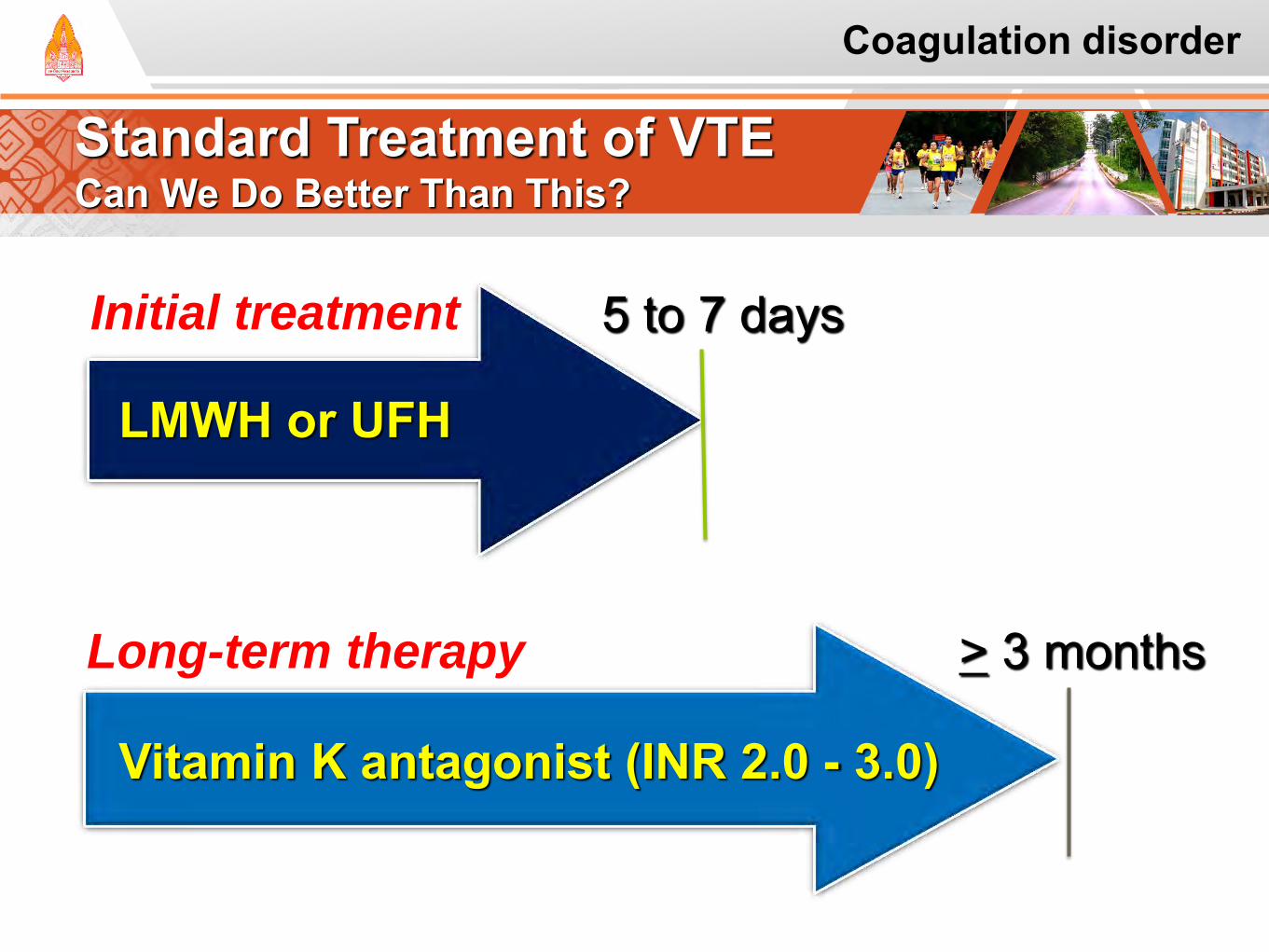
Standard Treatment of VTE Can We Do Better Than This?
Vitamin K antagonist (INR 2.0 - 3.0)
> 3 months
LMWH or UFH
5 to 7 days Initial treatment
Long-term therapy
Coagulation disorder
Gap of Knowledge before 2003
This multicenter, RCT was conducted to compare the efficacy of dalteparin, an LMWH, with short-term dalteparin followed by long-term oral anticoagulation with a coumarin in preventing recurrent VTE in patients with cancer
Short-term LMWH treatment, followed by
long-term oral anticoagulation, was the standard of care for prevention of recurrent VTE in patients with cancer. While providing some efficacy, oral anticoagulation is associated with a number of limitations, some of which are specific to patients with cancer.
Lee AYY, et al. N Engl J Med 2003;349:146-53.
Coagulation disorder
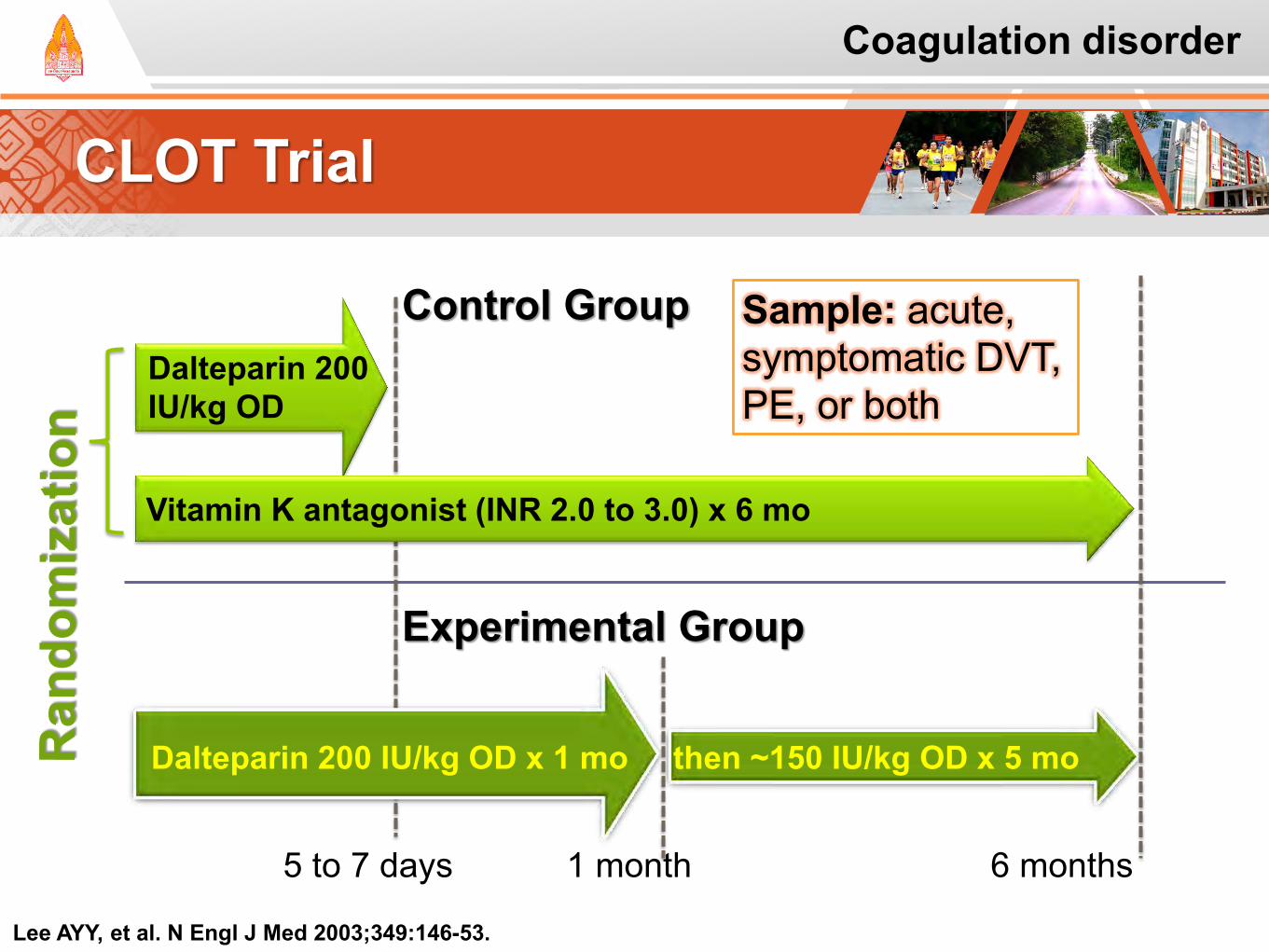
CLOT Trial
Lee AYY, et al. N Engl J Med 2003;349:146-53.
5 to 7 days
Dalteparin 200 IU/kg OD
Vitamin K antagonist (INR 2.0 to 3.0) x 6 mo
Control Group
Dalteparin 200 IU/kg OD x 1 mo then ~150 IU/kg OD x 5 mo
Experimental Group
1 month 6 months
Coagulation disorder
Sample: acute, symptomatic DVT, PE, or both
CLOT Trial
End points:
Primary end point:
The first episode of objectively documented, symptomatic, recurrent DVT, PE, or both during the 6-month study period
Secondary outcomes:
Clinically overt bleeding and death
Lee AYY, et al. N Engl J Med 2003;349:146-53.
Coagulation disorder
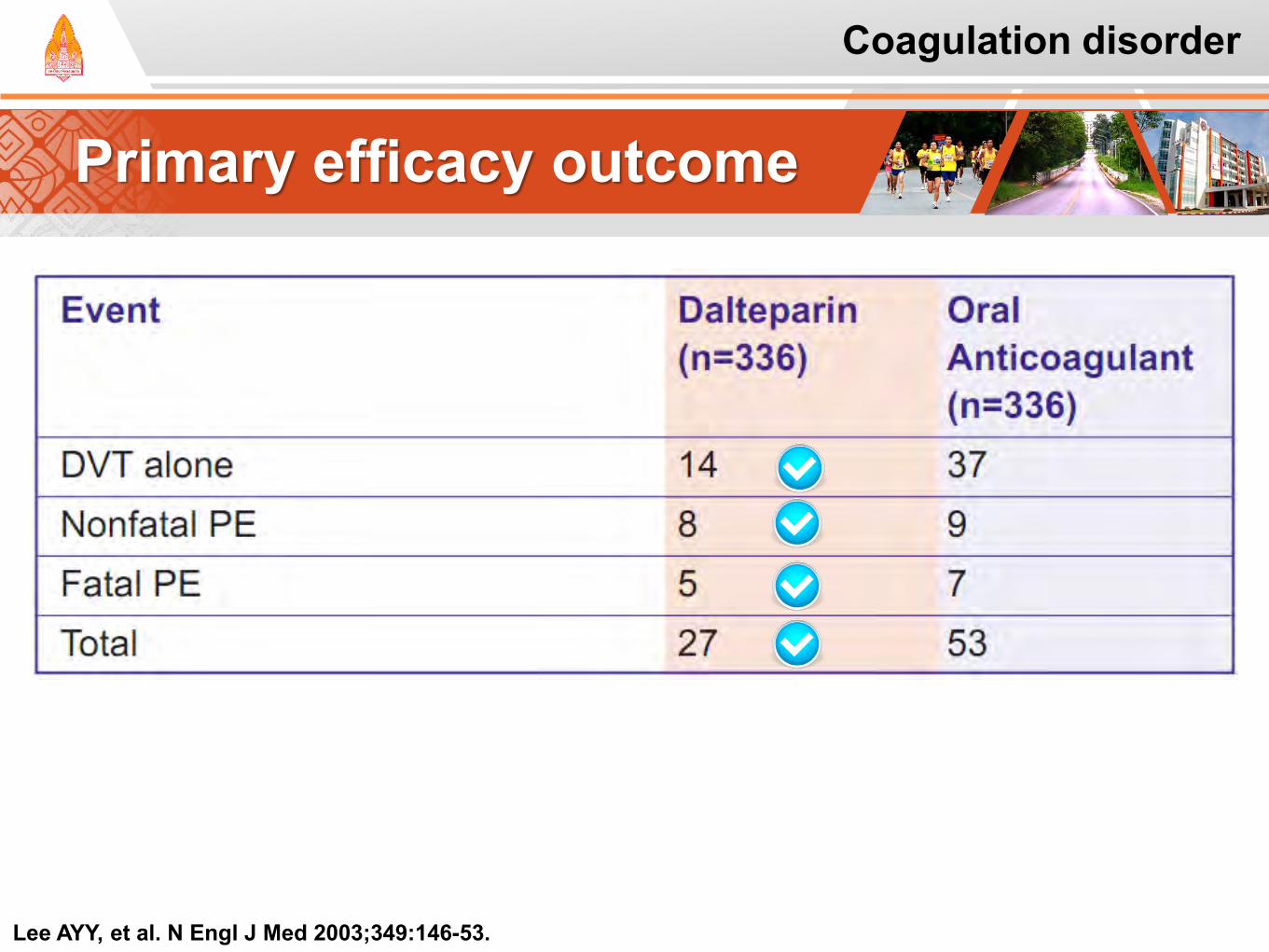
Primary efficacy outcome
Lee AYY, et al. N Engl J Med 2003;349:146-53.
Coagulation disorder
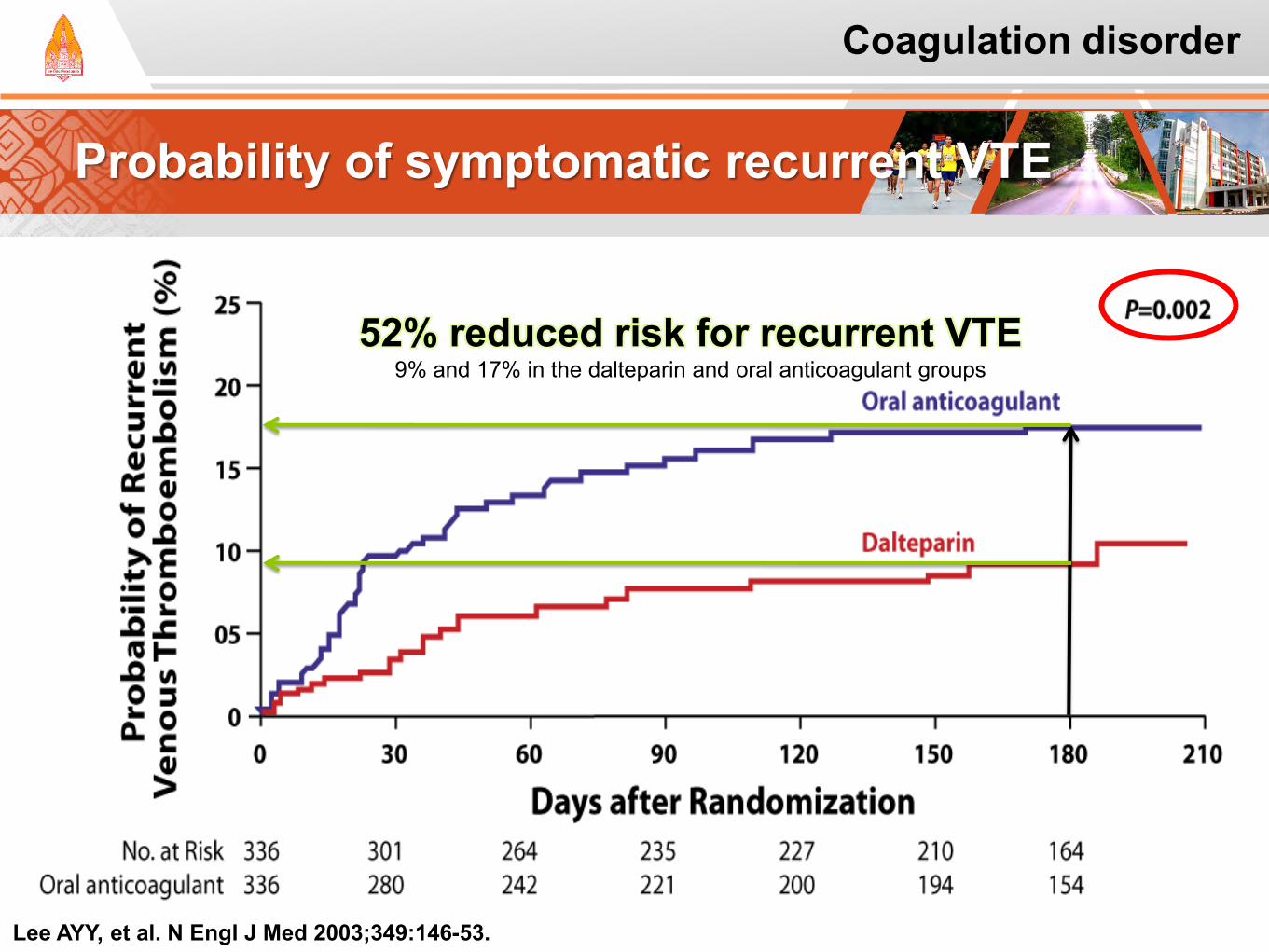
Probability of symptomatic recurrent VTE
Lee AYY, et al. N Engl J Med 2003;349:146-53.
52% reduced risk for recurrent VTE 9% and 17% in the dalteparin and oral anticoagulant groups
Coagulation disorder
Secondary Outcome
Safety
There was no significant difference between the dalteparin and oral anticoagulant groups (p=0.27) in
Rate of major bleeding (6% vs 4%, respectively)
Or any bleeding (14% vs 19%, respectively)
Lee AYY, et al. N Engl J Med 2003;349:146-53. Lee AYY. et al. J Clin Oncol; 23:2123-2129 2005
Coagulation disorder
Secondary Outcome
Mortality
During the 6 month treatment period:
130 and 136 patients died in the dalteparin and oral anticoagulant groups, respectively (p=0.53)
Lee AYY, et al. N Engl J Med 2003;349:146-53. Lee AYY. et al. J Clin Oncol; 23:2123-2129 2005
Coagulation disorder
CLOT Trial: Conclusions
Lee AYY, et al. N Engl J Med 2003;349:146-53.
An only-dalteparin regimen was more effective than a regimen consisting of short-term dalteparin followed by oral anticoagulation in reducing the risk of recurrent VTE The two regimens produced approximately equivalent risks for hemorrhagic complications Long-term self-injection of LMWH was acceptable to patients enrolled in this study
Coagulation disorder
ONCENOX study
Patients were randomized to receive 1 of 3 treatment regimens: Low-dose enoxaparin:
BID enoxaparin (1.0 mg/kg) for 5 d OD enoxaparin (1.0 mg/kg) for 175 d High-dose enoxaparin:
BID enoxaparin (1.0 mg/kg) for 5 d OD enoxaparin (1.5 mg/kg) for 175 d Oral anticoagulation:
BID enoxaparin (1.0 mg/kg) for 5 d until stable INR 2-3 on oral warfarin begun on day 2 of enoxaparin
The efficacy and safety of extended-duration (6 month) low- or high-dose enoxaparin, compared with initial enoxaparin followed by warfarin in the secondary prevention of VTE in patients with cancer was examined in the ONCENOX study
Deitcher SR, et al. Clin Appl Thromb Hemost 2006;12:389-96.
Coagulation disorder
ONCENOX: Clinical Outcomes
The incidence of recurrent VTE (ITT population):
There was no difference between the low- and high-dose enoxaparin groups
Major hemorrhagic events:
1 patient (3%) in the warfarin group
2 (6%) in the low-dose enoxaparin group
4 (11%) in the high-dose enoxaparin group
Deitcher SR, et al. Clin Appl Thromb Hemost 2006;12:389-96.
These data suggest
that enoxaparin,
administered for
6 months in patients
with cancer, is safe
Coagulation disorder
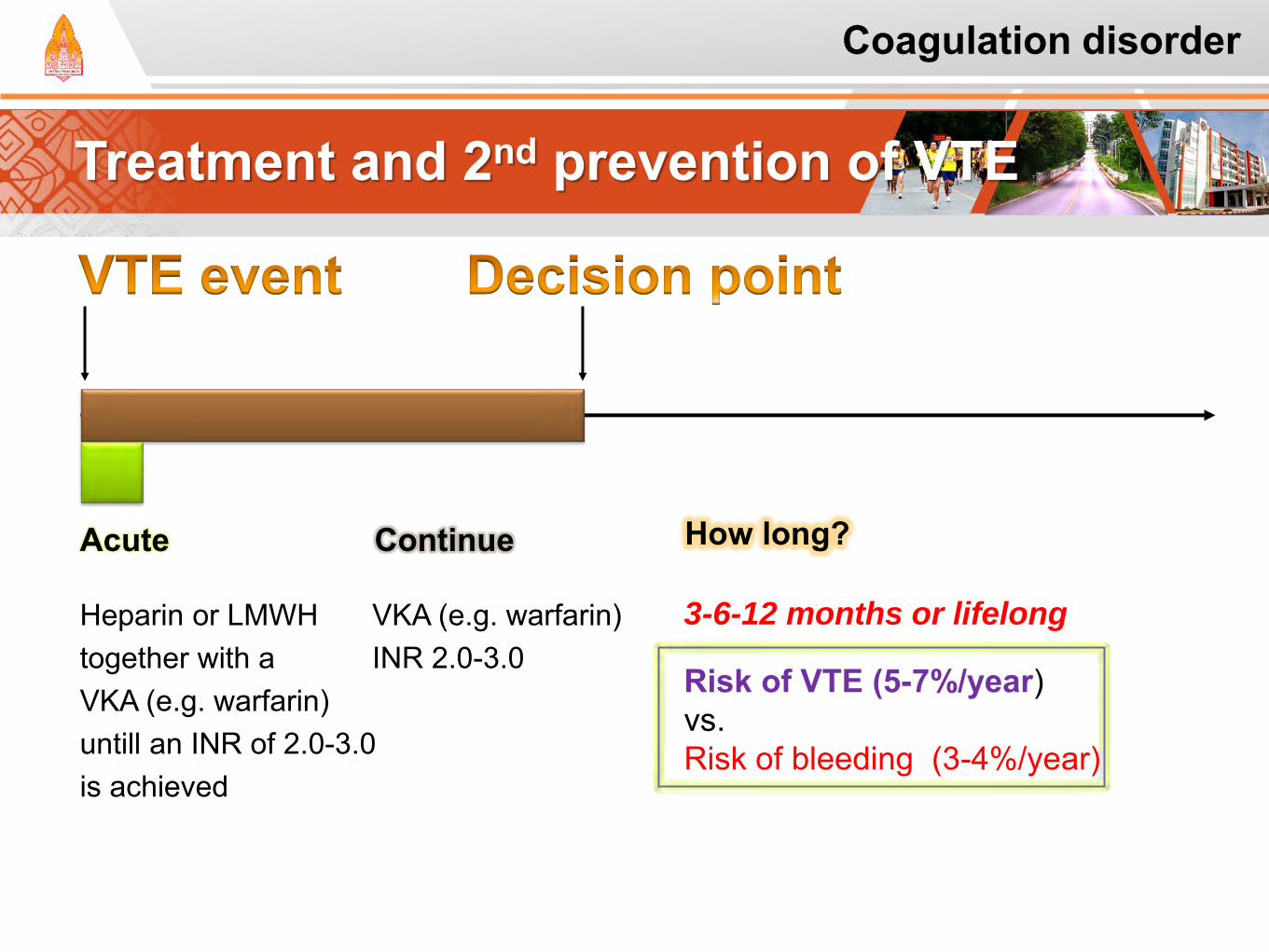
Treatment and 2nd prevention of VTE
Acute Continue
Heparin or LMWH together with a VKA (e.g. warfarin) untill an INR of 2.0-3.0 is achieved
VKA (e.g. warfarin) INR 2.0-3.0
3-6-12 months or lifelong
Risk of VTE (5-7%/year) vs. Risk of bleeding (3-4%/year)
How long?
Coagulation disorder
Case study: Furby
Coagulation disorder
FB is an elderly man with a long history of prostate cancer.
Until recently, his prostate cancer was managed with antiandrogen therapy.
There is evidence of disease progression, and he now has metastatic prostate cancer.
The plan was to start chemotherapy. He was recently D/C from the hospital after it was
discovered he had spinal cord compression, and he has severely limited mobility.
Case study: Furby
Coagulation disorder
Additionally, he was found to have a lower extremity DVT.
His family has a number of questions about his medications, and is very concerned that he will be on a "blood thinner."
They have done some research, and their understanding is that he will continue on anticoagulation therapy for 3 months.
Question: What is the duration of therapy for
anticoagulation in the patient with VTE and cancer?
Case study: Discussion
Coagulation disorder
There is not one correct answer for this question. The duration of anticoagulation therapy is
determined on an individual case basis. Consider base on risk versus benefit issues. At any time, if the risk of anticoagulation therapy
outweighs its perceived benefit, the therapy should be discontinued.
Therefore, in counseling FB and his family, it is
important to discuss that a definitive answer may
not be appropriate.
Case study: Why???
Coagulation disorder
FB require anticoagulation therapy because of his disease state (advanced).
Although FB will be receiving CMT to decrease disease progression (not to cure the cancer). It is likely that FB will remain on anticoagulation
therapy for the rest of his life, unless there is a change in status that makes the risk of anticoagulation outweigh the benefit.
Case study: Discussion
Coagulation disorder
Patients with curable cancers may not require anticoagulation therapy longer than the time recommended for individuals without cancer. Unfortunately, this is not the situation with FB.
Patients with VTE associated with a CVC will
require anticoagulation therapy for the duration of the time they have the device in place. Again, this is considered on an individual basis.

Case study: Nong Neoi
Coagulation disorder
NN a 45-year-old man with history of NHL.
He was initially treated with rituximab and cyclophosphamide, doxorubicin, vincristine, and prednisone chemotherapy with CR.
After 6 cycles, he had no evidence of cancer.
Unfortunately, recent follow-up imaging scans show a recurrence of cancer and an incidental finding of a PE.
Case study: NN
Coagulation disorder
The plan is to begin anticoagulation therapy as well as therapy for recurrent NHL.
The oncologist has told NN he will receive 2 cycles of chemotherapy and then proceed with an autologous SCT.
Question: What are appropriate options for
management of this PE in NN?
Case study: Discussion
Coagulation disorder
Acute Management: An incidental finding of PE requires treatment,
and anticoagulation should be started immediately.
Therapy could include UFH, but as this would require hospitalization, LMWH is probably a better option.
Case study: Discussion
Coagulation disorder
Chronic Management: Chronic therapy with LMWH offers many
benefits, including the ability to easily hold anticoagulation for a short period of time when needed for procedures e.g, placement of CVC, BM biopsy
Another beneficial effect of chronic therapy with LMWH is a lack of drug–drug interactions.
Case study: Rum phoung
Coagulation disorder
RP is a 35-year-old woman with lung cancer.
She was recently diagnosed with a thrombosis associated with her infusion port and was started on LMWH.
She has limited insurance coverage at this time, and the plan is to start warfarin for chronic anticoagulation.
Question:
Case study: Discussion
Coagulation disorder
Concurrent LMWH with warfarin until the INR is within the targeted therapeutic range.
Initiation with warfarin 3-5 mg for 1 to 2 days, and subsequent dosing is based on INR response.
Lower doses are suggested for Older, debilitated, malnourished, have liver disease and/or
dysfunction, or are taking medications known to increase sensitivity to warfarin
Case study: VKAs
Coagulation disorder
Assessment (before start VKAs) Nutritional status Concurrent dietary intake of vitamin K,
Nutritional supplements Vitamins Diet
Concomitant drug therapy Liver function
Case study: Line Pop
Coagulation disorder
LP is a 39-year-old man with head and neck cancer receiving radiation therapy.
He has had extensive surgery, and his oral intake is limited to nutritional supplements.
Other medical problems include history of DVT in his left leg, hypertension, and liver dysfunction secondary to chronic alcohol use.
Case study: LP
Coagulation disorder
He has been managed with LMWH, but he has requested that he be changed to another therapy.
He has continued on LMWH and was started on warfarin 2 mg po daily.
Two days after initiation of warfarin, his INR is 2.9 with a target goal of 2 to 3.
Question:
Case study: Discussion
Coagulation disorder
Concurrent warfarin with LMWH at least 4-5 days.
INR is 2.9 after only 2 days of warfarin, and the full effect of these doses has not been seen.
Dose of warfarin should be decreased even though his INR is in the goal range.
It is important to closely monitor INR.
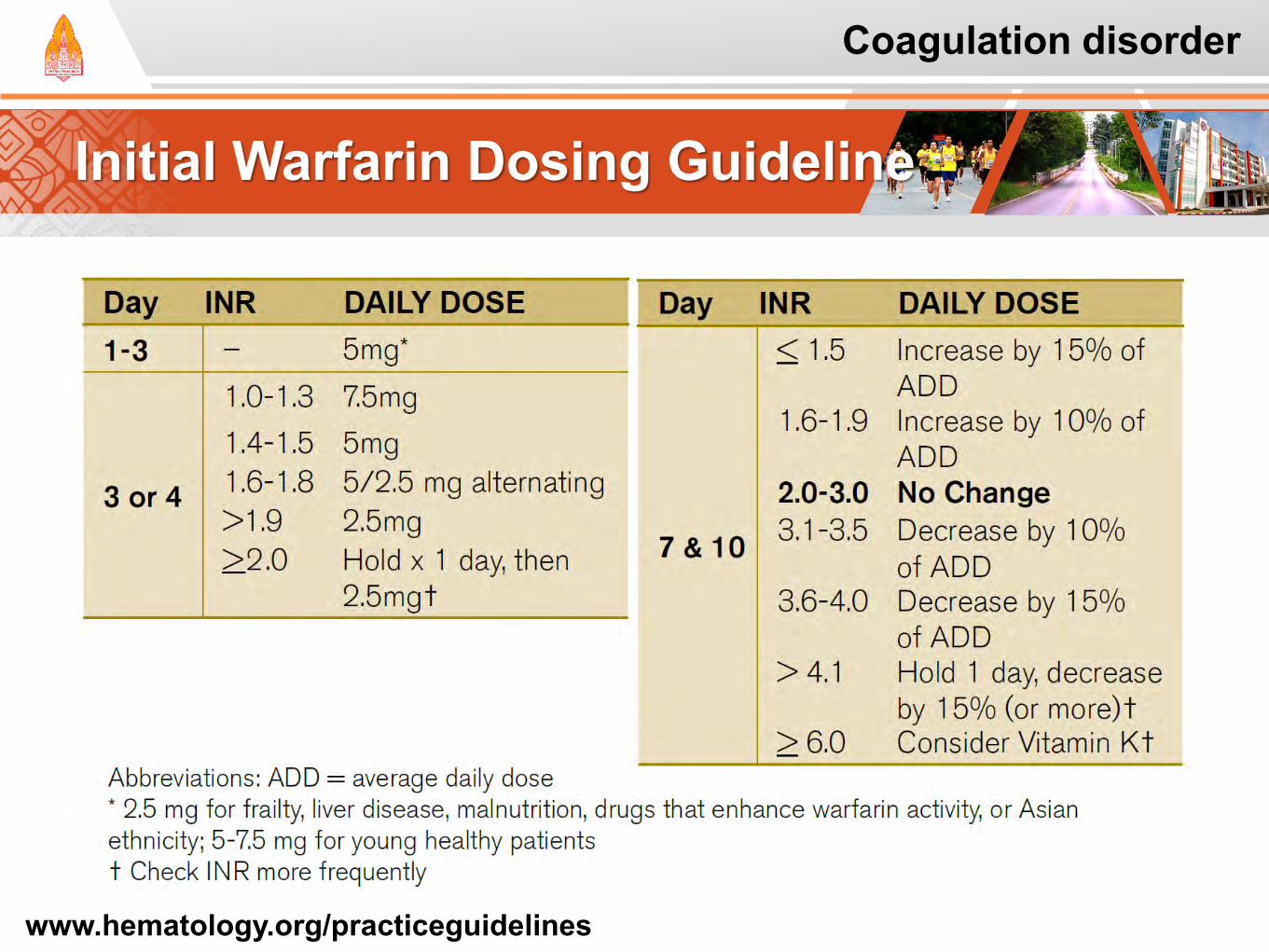
Initial Warfarin Dosing Guideline
Coagulation disorder
www.hematology.org/practiceguidelines
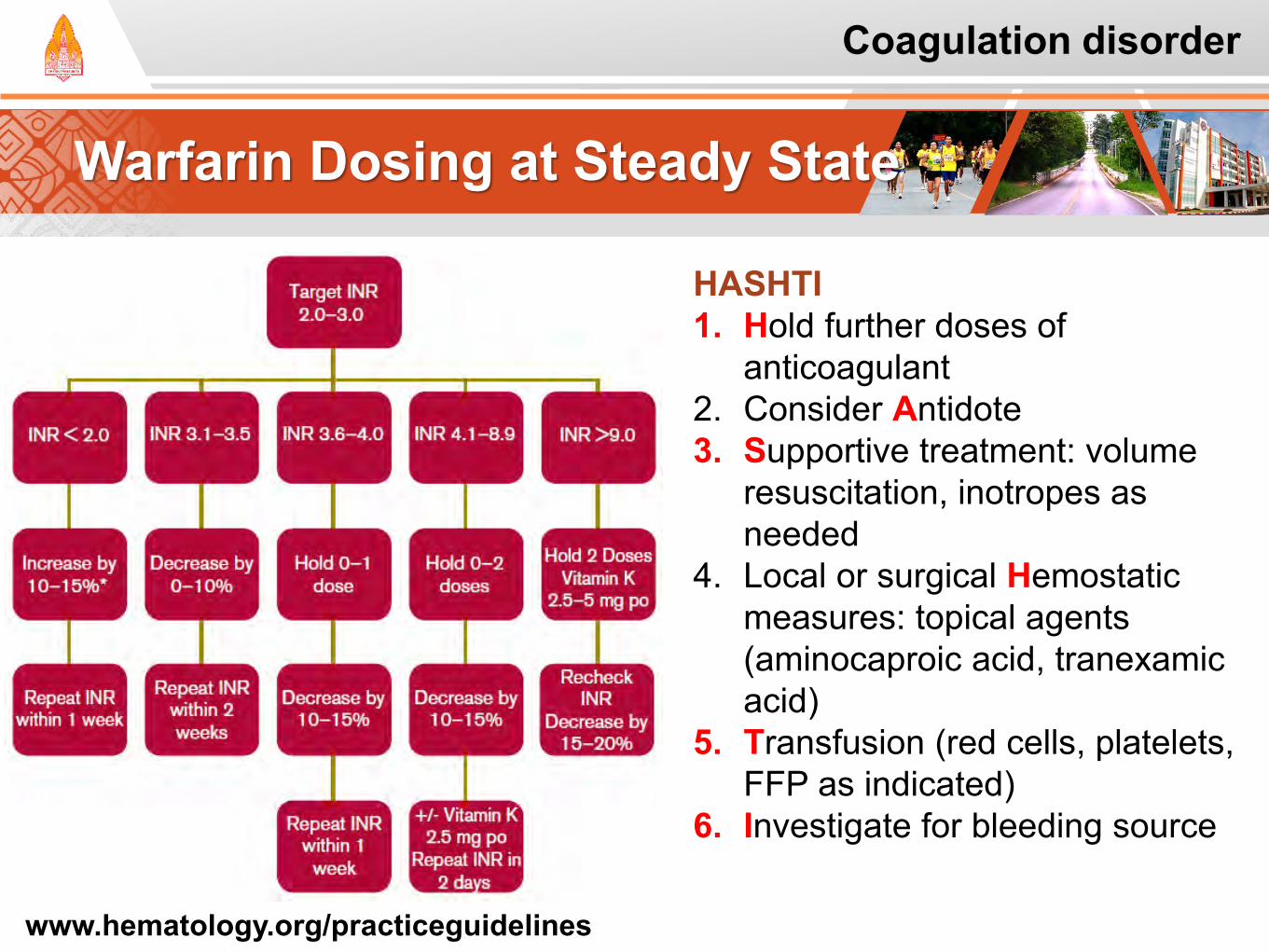
Warfarin Dosing at Steady State
Coagulation disorder
HASHTI 1. Hold further doses of
anticoagulant 2. Consider Antidote 3. Supportive treatment: volume
resuscitation, inotropes as needed
4. Local or surgical Hemostatic measures: topical agents (aminocaproic acid, tranexamic acid)
5. Transfusion (red cells, platelets, FFP as indicated)
6. Investigate for bleeding source
www.hematology.org/practiceguidelines
Case study: Discussion
Coagulation disorder
There is an opportunity to talk with LP to determine what the impact of diet, concomitant drug therapy, and/or other modifiable factors have on the apparent low warfarin dose requirement. Assess amount of nutritional supplementation
(and vitamin K content in supplementation) Obtain a complete medication history Evaluate alcohol use
Case study: Po Po
Coagulation disorder
PP is a 57-year-old man with a history of a neuroendocrine tumor of the pancreas.
He has been receiving monthly injections of
octreotide with relatively good management of diarrhea.
About 1 week ago, he noted new-onset shortness of breath and was found to have a PE.
Case study: PP
Coagulation disorder
He was started on LMWH for initial treatment, but then bridged to warfarin therapy as he refused to subcutaneously self-administer any medication chronically.
His INR has been erratic, and his dose of warfarin has been modified weekly. He is very upset that he is still having his blood work done once weekly.
Question:
Case study: Discussion
Coagulation disorder
Dietary changes, including vitamin K containing vegetables, liver, nutritional supplement, etc.
Changes in bowel function, especially in relation to monthly octreotide injections, as some patients will have an increase in diarrhea for the days to 1 week prior to scheduled dose of octreotide.
Adherence to the dosing regimen prescribed.
Nutescu EA, et al. Expert Opin Drug Saf. 2006;5(3):433-451.
Case study: Discussion
Coagulation disorder
Alcohol use (eg, chronic alcohol use may increase warfarin requirements and episodic alcohol use may increase INR for individuals on warfarin).
Use of OTC medications and complementary medications including acetaminophen and multivitamins.
Nutescu EA, et al. Expert Opin Drug Saf. 2006;5(3):433-451.
Case study: Be Be
Coagulation disorder
BB is a 44-year-old woman with MBC who has a relatively recent history of DVT managed with warfarin 7.5 mg po daily.
Her INRs have ranged from 1.9 to 2.3 over the last few weeks.
She was doing well until recently when she experienced confusion and severe headaches.
Subsequent evaluation demonstrated multiple brain lesions consistent with brain metastases.
Case study: BB
Coagulation disorder
She is scheduled to start RT and was started on dexamethasone 4 mg po every 8 hours.
Her INR today was 5.6 when she had blood work prior to radiation.
The INR results were not reported until BB left the
physician's office, and she is now at home. Question:
Case study: Discussion
Coagulation disorder
Reversal of warfarin is based on S/S, INR, and the patient's risk of bleeding.
It is important to assess whether the INR is stable or is escalating secondary to recent changes in medications (eg, dexamethasone).
Case study: Discussion
Coagulation disorder
PP has not reported bleeding, but this should be evaluated.
She is not currently receiving therapy that will cause thrombocytopenia and has no known risk for bleeding that we are aware of at this time.
One possible consideration is the risk of gastric irritation with dexamethasone.
Case study: Discussion
Coagulation disorder
The recent addition of dexamethasone may have a significant impact on INR for a patient on warfarin.
As this medication is likely to be continued, and eventually tapered, it will be important to closely monitor INR with dexamethasone dose changes.
Consideration of holding the dose of warfarin should be determined by both the clinical situation as well as the INR.
Case study: Discussion
Coagulation disorder
The use of oral phytonadione 1 to 2.5 mg may be used in patients with high risk of bleeding.
Although phytonadione has been given subcutaneously to manage elevated INRs, the absorption is erratic and delayed.
The use of intravenous phytonadione, given slowly to avoid anaphylaxis, should be considered when there is serious bleeding
Case study: Discussion
Coagulation disorder
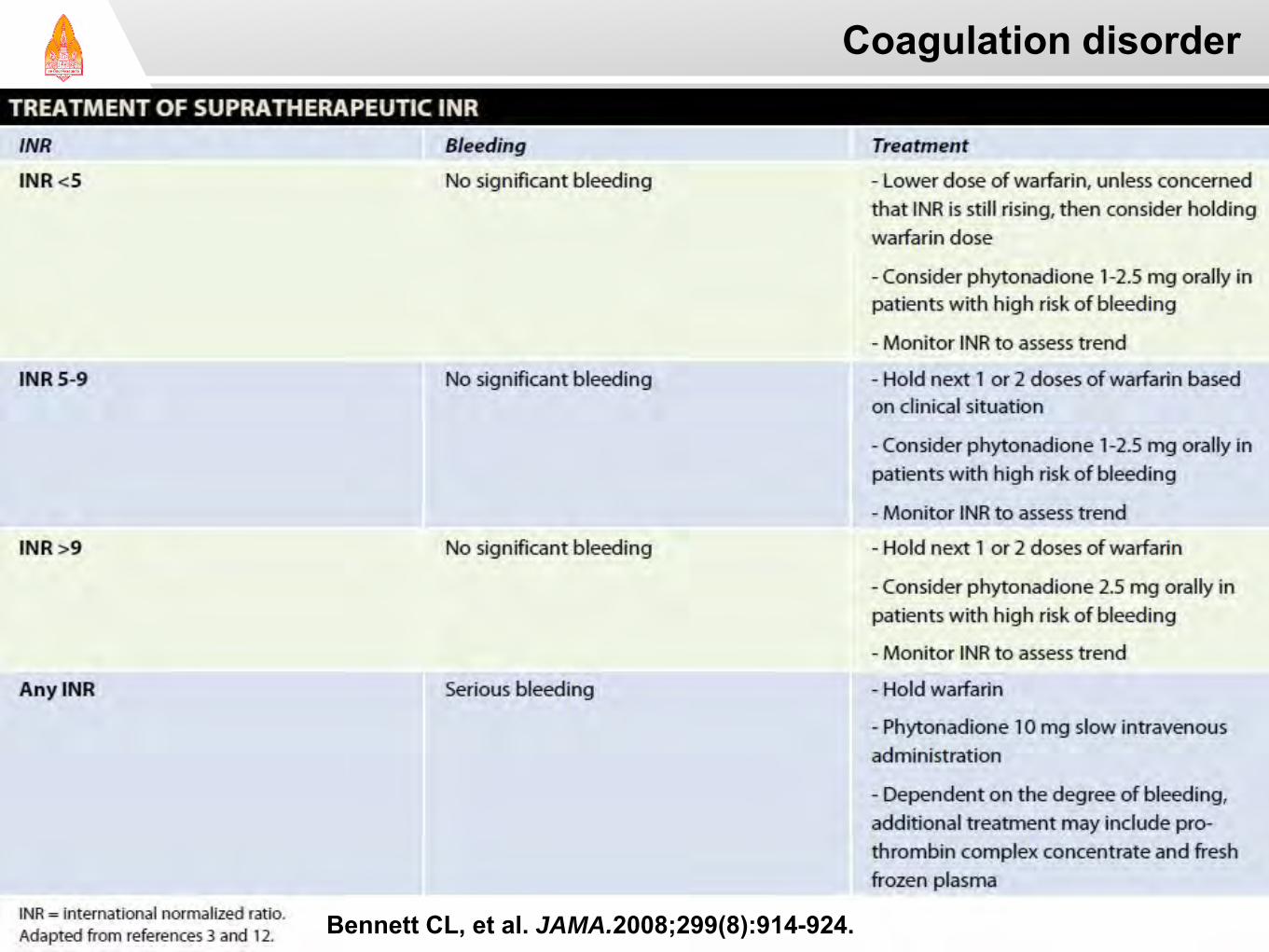
Bennett CL, et al. JAMA.2008;299(8):914-924.
8th, 9th ACCP: Long-term treatment
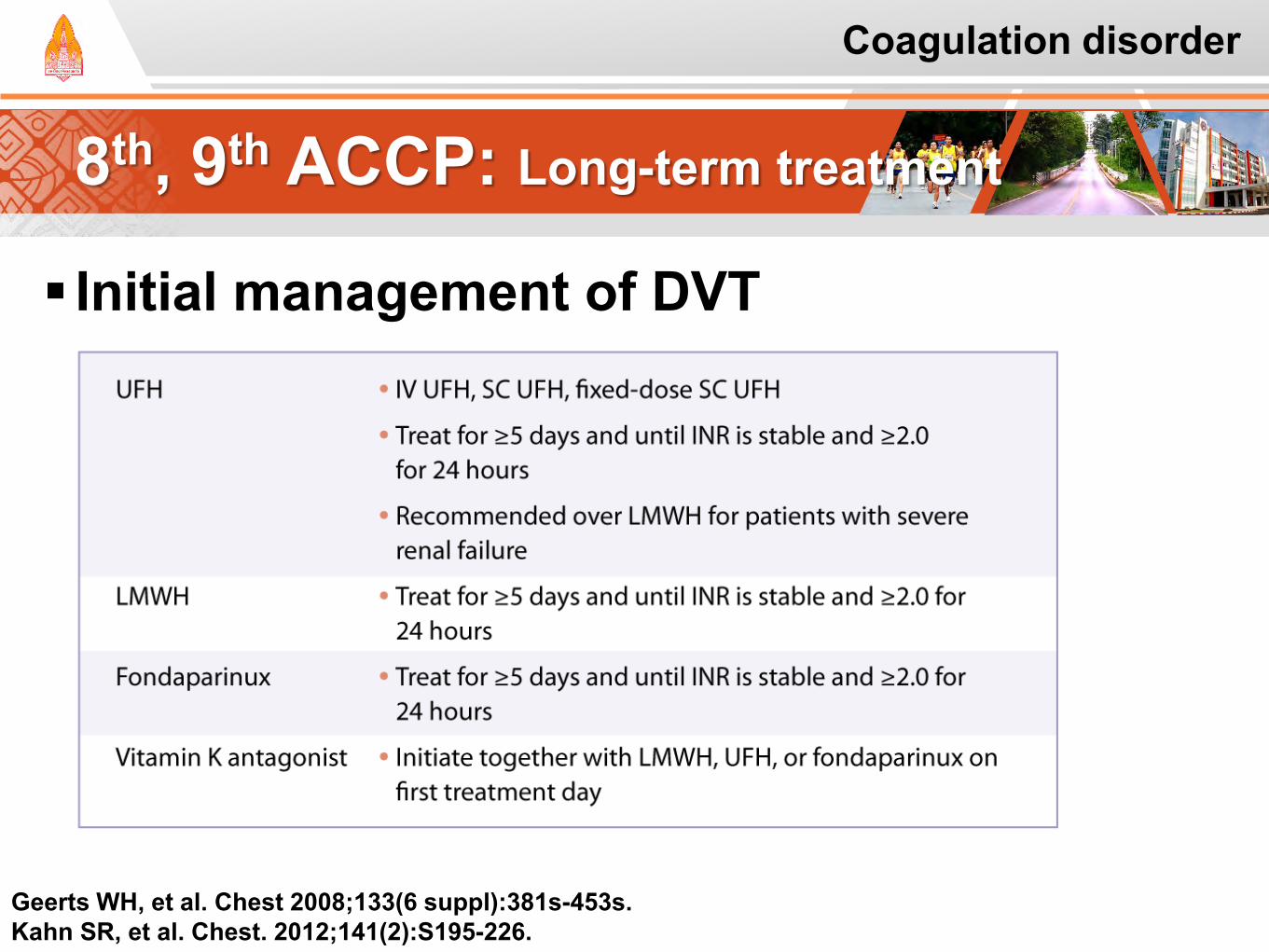
Geerts WH, et al. Chest 2008;133(6 suppl):381s-453s. Kahn SR, et al. Chest. 2012;141(2):S195-226.
Initial management of DVT
Coagulation disorder
8th, 9th ACCP: Long-term treatment
Geerts WH, et al. Chest 2008;133(6 suppl):381s-453s.
2nd prevention in patients with cancer LMWH for the first 3 to 6 months
Duration of therapy Warfarin or LMWH:
Indefinitely or until the cancer is resolved
Coagulation disorder
Geerts WH, et al. Chest 2008;133(6 suppl):381s-453s. Kahn SR, et al. Chest. 2012;141(2):S195-226.
Prevention of VTE in Nonsurgical Patients
Coagulation disorder
Kahn SR, et al. Chest. 2012;141(2):S195-226.
Cancer in Outpatient Setting
Cancer patient w/o additional VTE risk factors, suggest against routine use of prophylactic LMWH/LDUH (2B) or prophylactic VKAs (1B)
Solid tumor outpatients with additional VTE risk factors and low bleeding risk, suggest prophylactic-dose LMWH or LDUH (2B)
LDUH: low-dose unfractionated heparin; LMWH: low-molecular weight heparin
Prevention of VTE in Nonsurgical Patients
Coagulation disorder
Kahn SR, et al. Chest. 2012;141(2):S195-226.
Cancer in Outpatient Setting: Remarks Additional risk factors for VTE in cancer outpatients
Previous venous thrombosis
Immobilization
Hormonal therapy
Angiogenesis inhibitors
Thalidomide
Lenalidomide
Antithrombotic Therapy for VTE
Coagulation disorder
Kahn SR, et al. Chest. 2012;141(2):S195-226.
Long term PE treatment Cancer patients with PE, suggest LMWH over
VKA therapy (2B). If not treated with LMWH, suggest VKA over
dabigatran or rivaroxaban (2C)
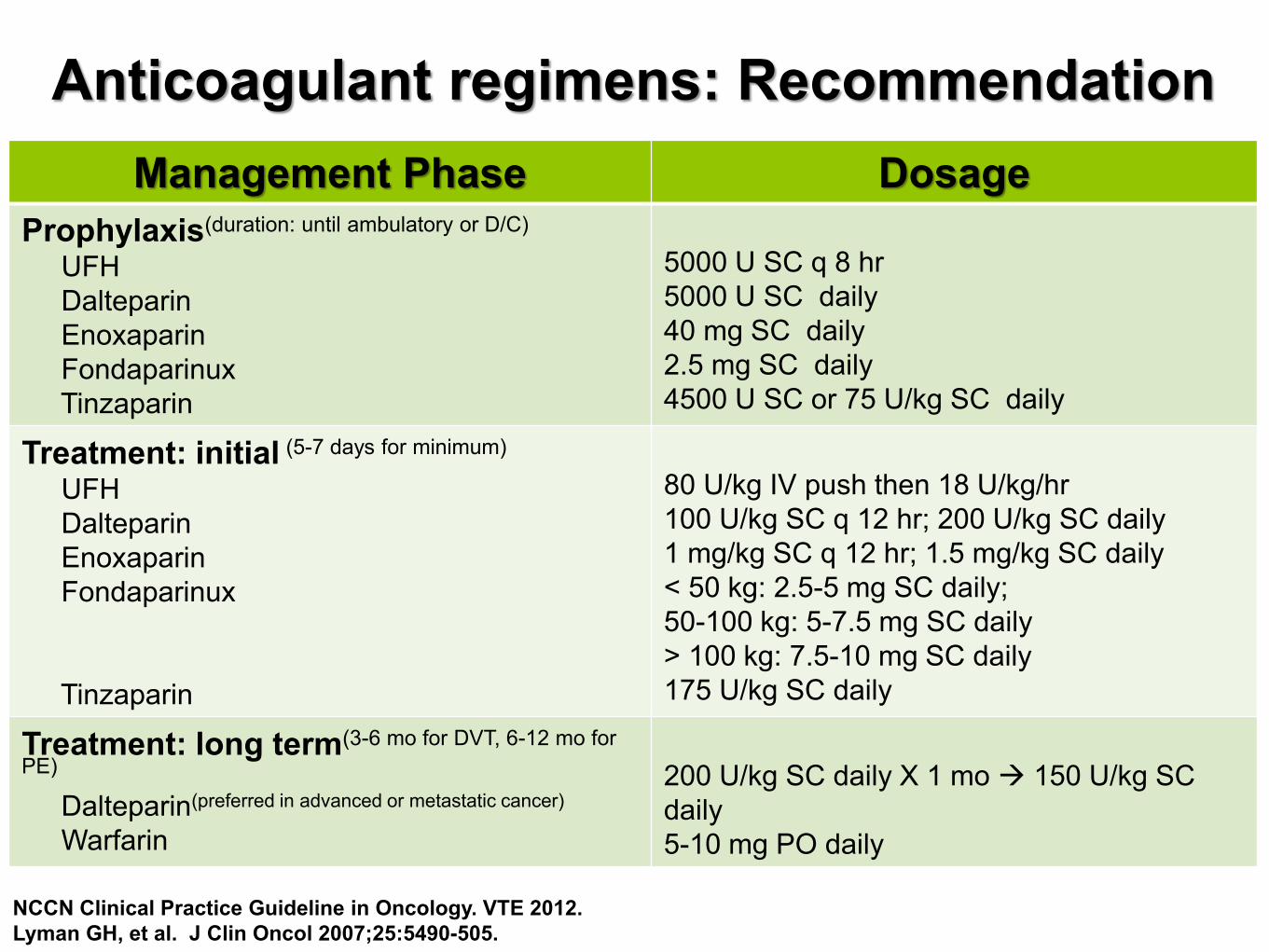
Anticoagulant regimens: Recommendation
NCCN Clinical Practice Guideline in Oncology. VTE 2012. Lyman GH, et al. J Clin Oncol 2007;25:5490-505.
Management Phase Dosage Prophylaxis(duration: until ambulatory or D/C)
UFH Dalteparin Enoxaparin Fondaparinux Tinzaparin
5000 U SC q 8 hr 5000 U SC daily 40 mg SC daily 2.5 mg SC daily 4500 U SC or 75 U/kg SC daily
Treatment: initial (5-7 days for minimum)
UFH Dalteparin Enoxaparin Fondaparinux Tinzaparin
80 U/kg IV push then 18 U/kg/hr 100 U/kg SC q 12 hr; 200 U/kg SC daily 1 mg/kg SC q 12 hr; 1.5 mg/kg SC daily < 50 kg: 2.5-5 mg SC daily; 50-100 kg: 5-7.5 mg SC daily > 100 kg: 7.5-10 mg SC daily 175 U/kg SC daily
Treatment: long term(3-6 mo for DVT, 6-12 mo for PE)
Dalteparin(preferred in advanced or metastatic cancer) Warfarin
200 U/kg SC daily X 1 mo 150 U/kg SC daily 5-10 mg PO daily
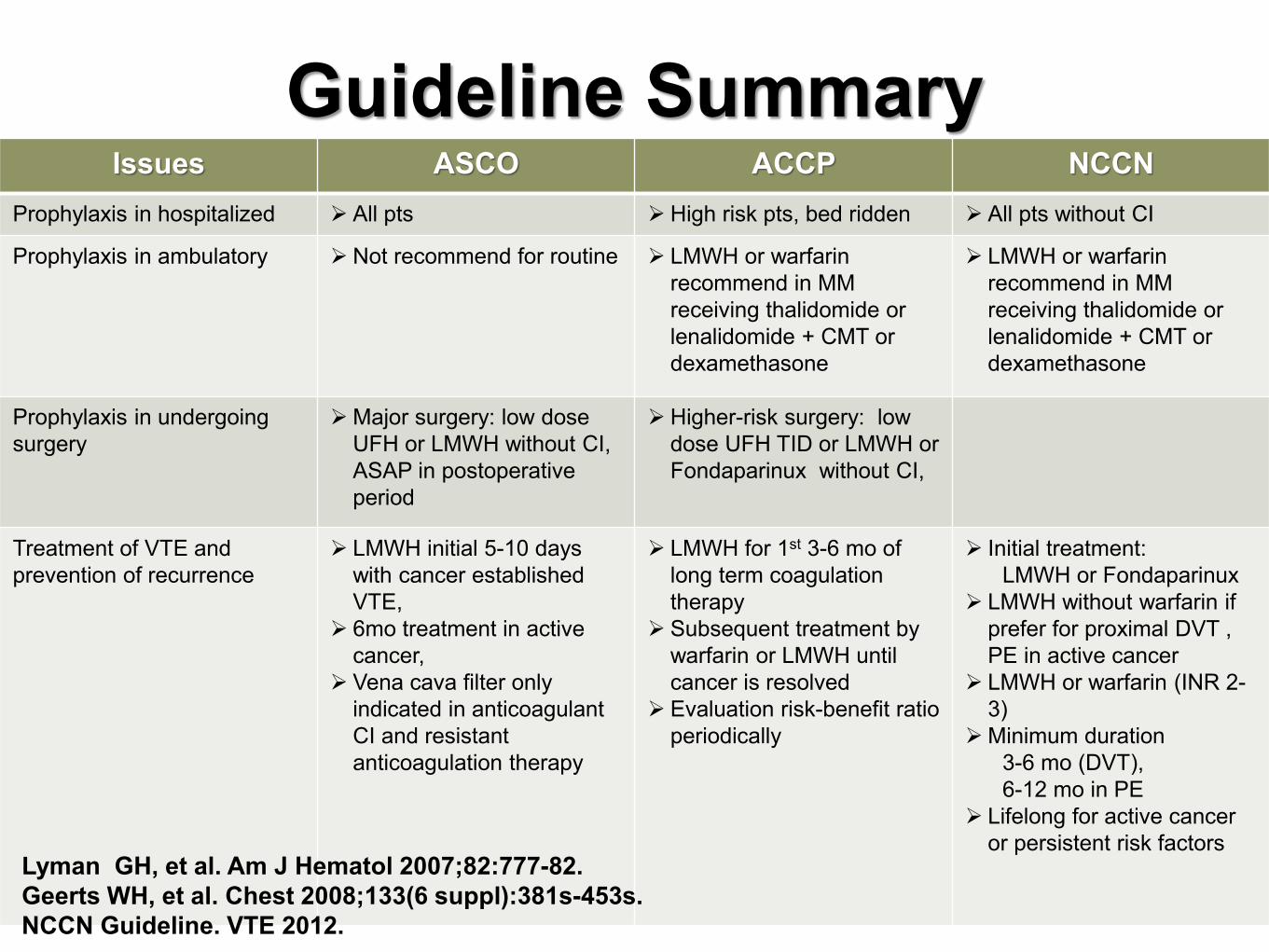
Issues ASCO ACCP NCCN Prophylaxis in hospitalized All pts High risk pts, bed ridden All pts without CI
Prophylaxis in ambulatory Not recommend for routine LMWH or warfarin recommend in MM receiving thalidomide or lenalidomide + CMT or dexamethasone
LMWH or warfarin recommend in MM receiving thalidomide or lenalidomide + CMT or dexamethasone
Prophylaxis in undergoing surgery
Major surgery: low dose UFH or LMWH without CI, ASAP in postoperative period
Higher-risk surgery: low dose UFH TID or LMWH or Fondaparinux without CI,
Treatment of VTE and prevention of recurrence
LMWH initial 5-10 days with cancer established VTE,
6mo treatment in active cancer,
Vena cava filter only indicated in anticoagulant CI and resistant anticoagulation therapy
LMWH for 1st 3-6 mo of long term coagulation therapy
Subsequent treatment by warfarin or LMWH until cancer is resolved
Evaluation risk-benefit ratio periodically
Initial treatment: LMWH or Fondaparinux LMWH without warfarin if
prefer for proximal DVT , PE in active cancer
LMWH or warfarin (INR 2-3)
Minimum duration 3-6 mo (DVT), 6-12 mo in PE Lifelong for active cancer
or persistent risk factors
Guideline Summary
Lyman GH, et al. Am J Hematol 2007;82:777-82. Geerts WH, et al. Chest 2008;133(6 suppl):381s-453s. NCCN Guideline. VTE 2012.
Take Home Messages
Coagulation disorder
Management of VTE remains a challenge LMWH preferred use as the initial treatment and
secondary prevention
Minimum of 6 months and longer duration if the cancer remains active
Both recurrent thrombosis and bleeding remain problems
Need to make research more for the advent of new anticoagulants
Thank you!
Recommended