Differential Diagnosis of Disc Edema
Moderated by: Dr. Parul Ichhpujani
Presented by: Dr. Sahil Thakur
Historical Context
1860: Albrecht von Graefe first reported his observations in 4patients with brain tumor and a swelling of the ONH; hecalled it Stauungspapille.
1908:Parsons coined the English term papilledema
1911: Paton and Holmes differentiated between papilledemawith increased intracranial pressure (ICP) and optic neuritis.
Basic differentiation was based on visual function.
Edema of the nerve head with decreased vision was considered opticneuritis and edema of the ONH without decreased vision waspapilledema secondary to increased ICP.
As experience has taught us, decreased vision also occurs as a resultof chronic papilledema secondary to increased ICP and subsequentoptic nerve atrophy.
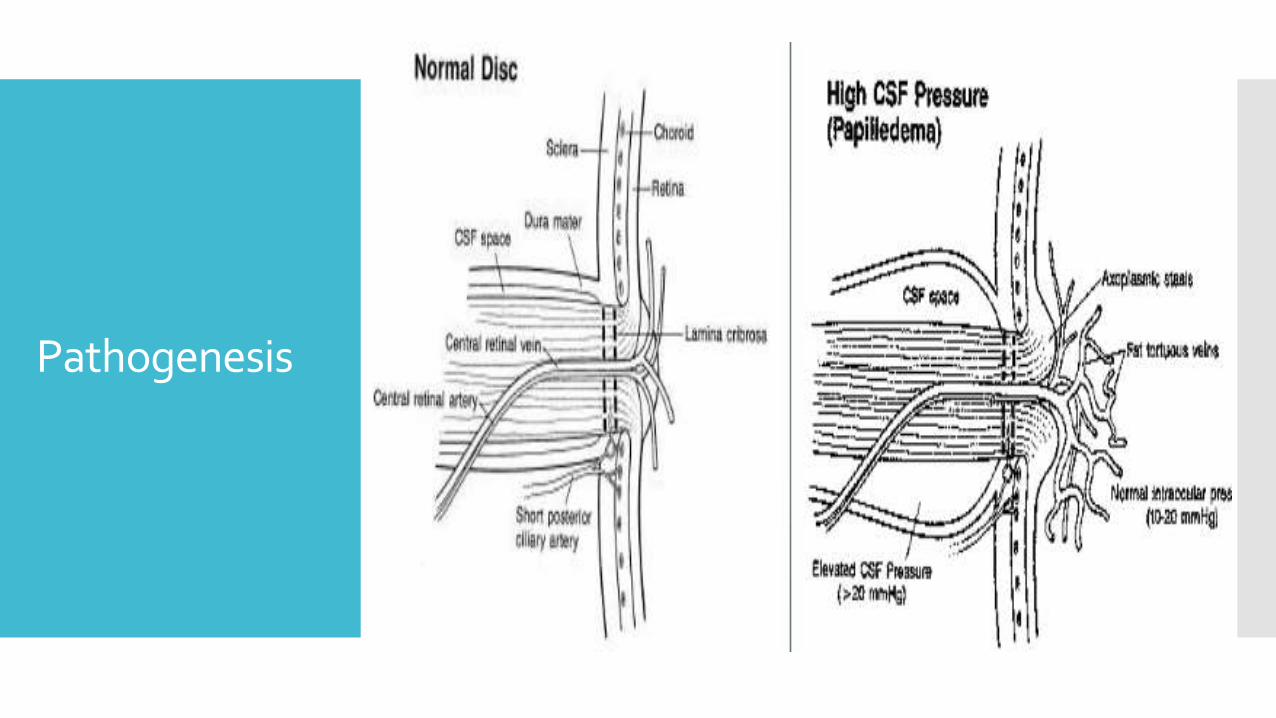
Pathogenesis
Weiss and Hiscoe’s concept:
Axoplasmic flow: Flow of subcellular and molecular particles along the axonsof the nerves
3 types of axoplasmic flow exist; these occur simultaneously and somewhatindependently and are affected by different pathologic processes.
Orthograde rapid flow, which moves along the axon at a rate of 200 to 1000mm/day and subserves synaptic transmission.
Orthograde slow flow, which moves at 0.5 to 3 mm/day. Maintains the growthand metabolic stability of the axon.
Retrograde flow that moves at 50 to 75 mm/day. Allows the axon to sample itsenvironment and send information back to the cell body.
Different mechanisms of insult differentially affect the axoplasmic flowcomponents.
Ischemia predominantly blocks rapid axoplasmic flow, whereas compression ofan axon blocks slow axoplasmic flow.
The former situation occurs in anterior ischemic optic neuropathy, and thelatter in increased intracranial pressure.
Causes of Disc Edema
Most common causes of optic nerve swelling are: Non-arteritic anterior ischaemic optic neuropathy (35%) Optic neuritis (31%) Intracranial pathology (14%)
Causes of Unilateral optic disc swelling: Demyelinating optic neuritis NA-AION Retinal vein occlusion Diabetic papillopathy
Causes of Bilateral optic disc swelling: Papilledema, Toxic optic neuropathy Malignant hypertension PIH
Jung JJ, Baek S-H, Kim US. Korean Journal of Ophthalmology : KJO. 2011;25(1):33-36.
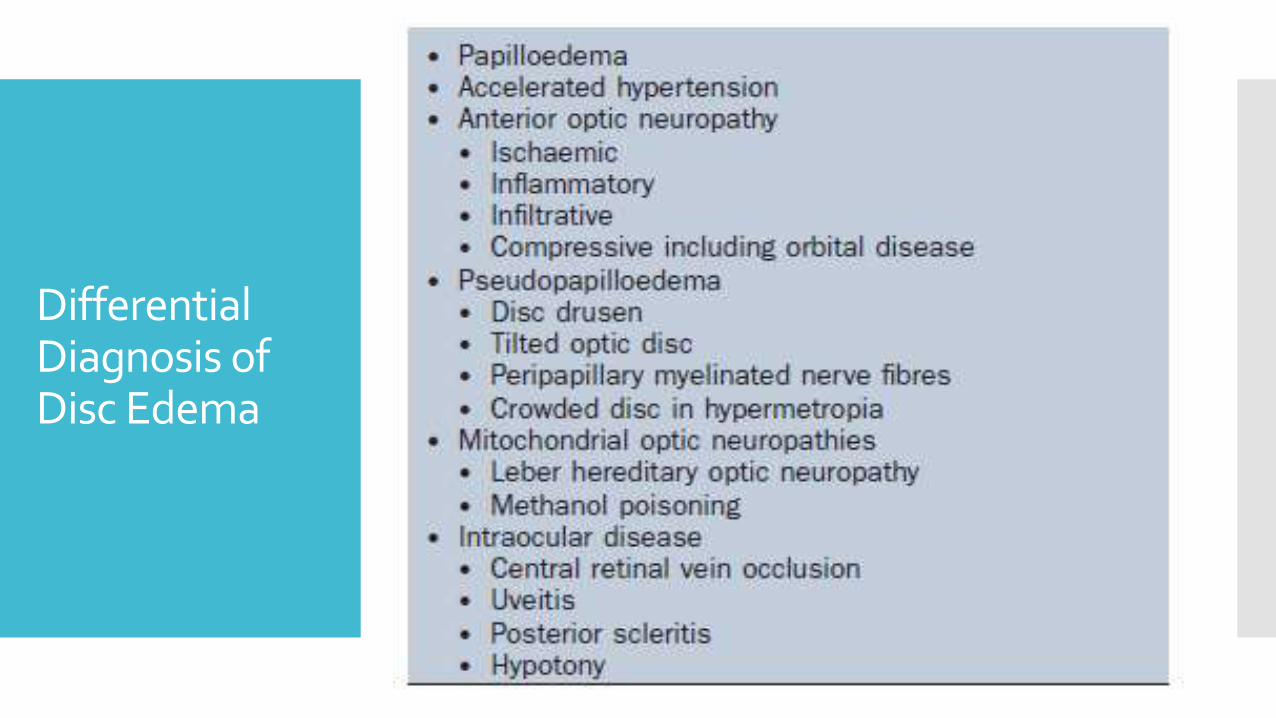
Differential Diagnosis ofDisc Edema
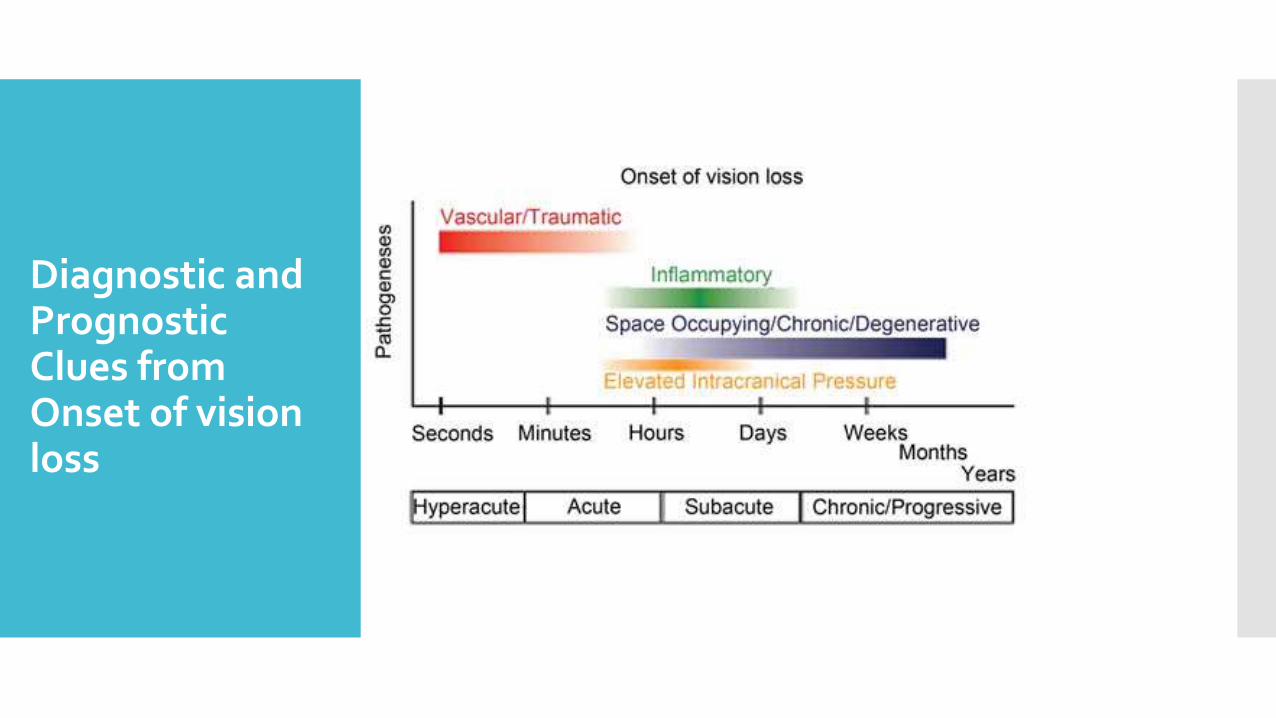
Diagnostic and Prognostic Clues from Onset of vision loss
Symptoms(Ocular) Transient visual obscuration (TVO)
Central vision affected late
Horizontal diplopia
Decreased Visual Acuity
Blind spot enlargement
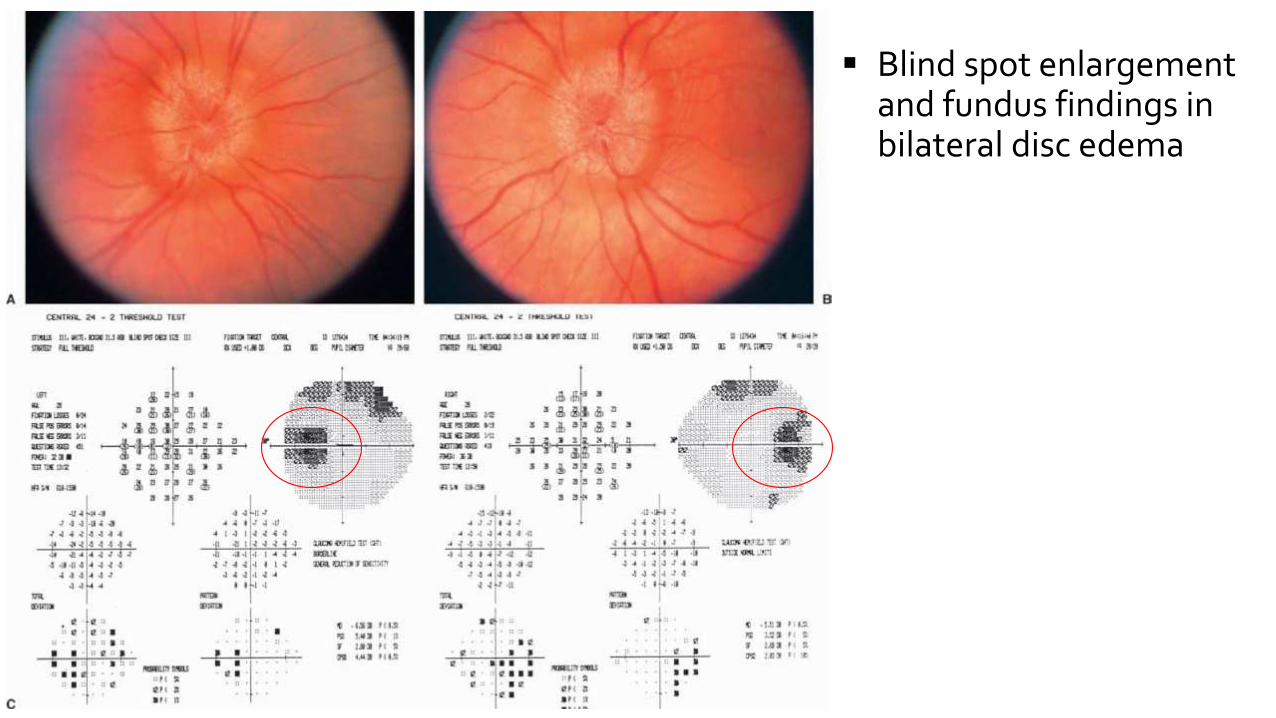
Blind spot enlargement and fundus findings in bilateral disc edema
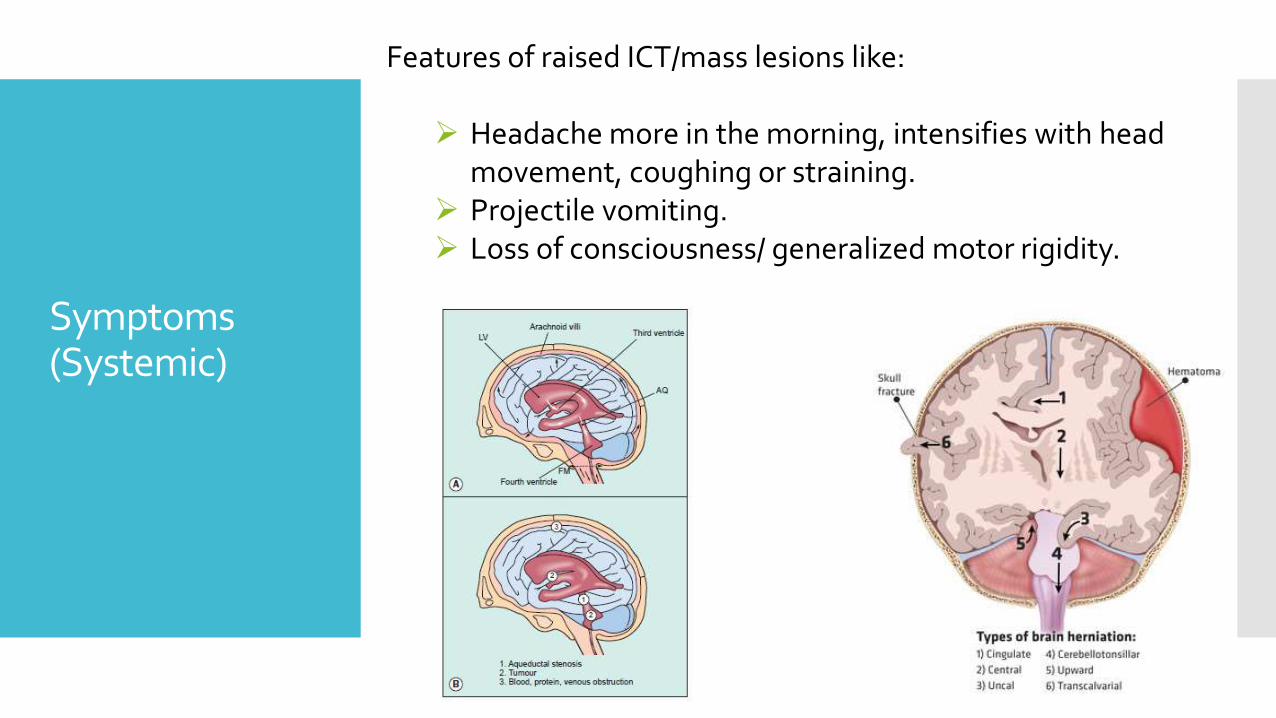
Features of raised ICT/mass lesions like:
Headache more in the morning, intensifies with head movement, coughing or straining.
Projectile vomiting. Loss of consciousness/ generalized motor rigidity.
Symptoms(Systemic)
Signs of Disc Edema
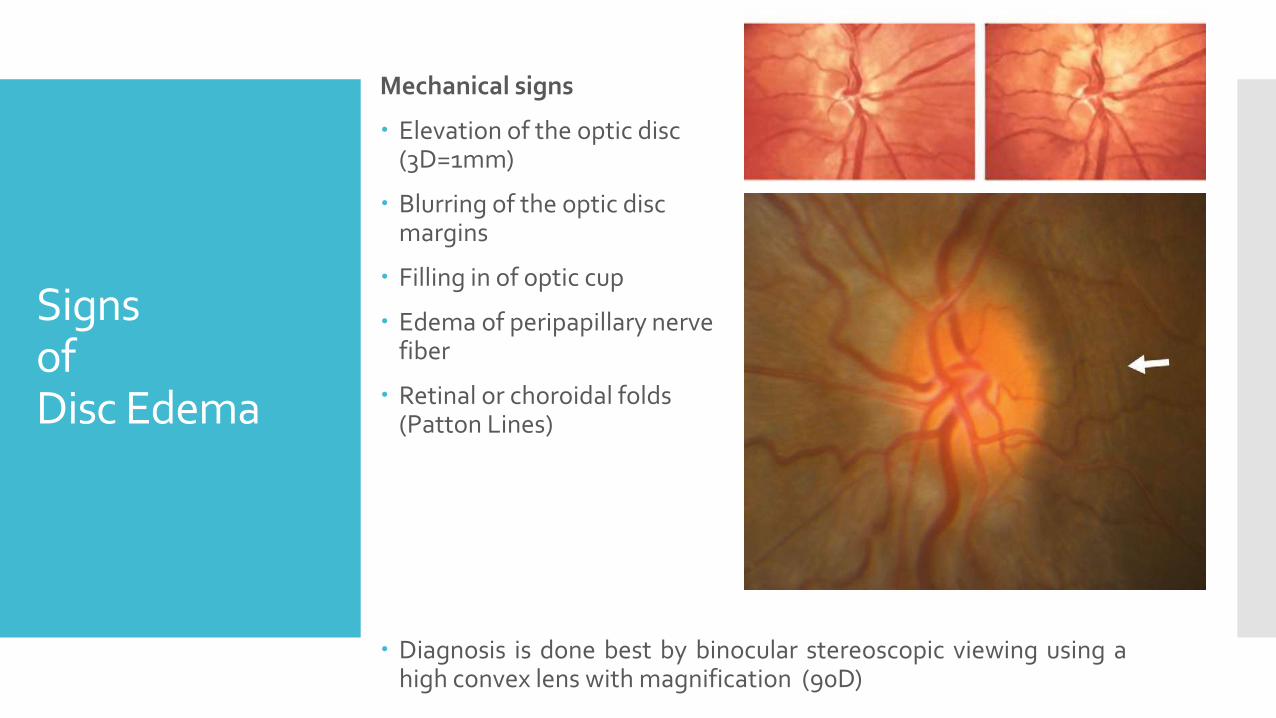
Mechanical signs
Elevation of the optic disc (3D=1mm)
Blurring of the optic disc margins
Filling in of optic cup
Edema of peripapillary nerve fiber
Retinal or choroidal folds (Patton Lines)
Diagnosis is done best by binocular stereoscopic viewing using ahigh convex lens with magnification (90D)
Signs of Disc Edema
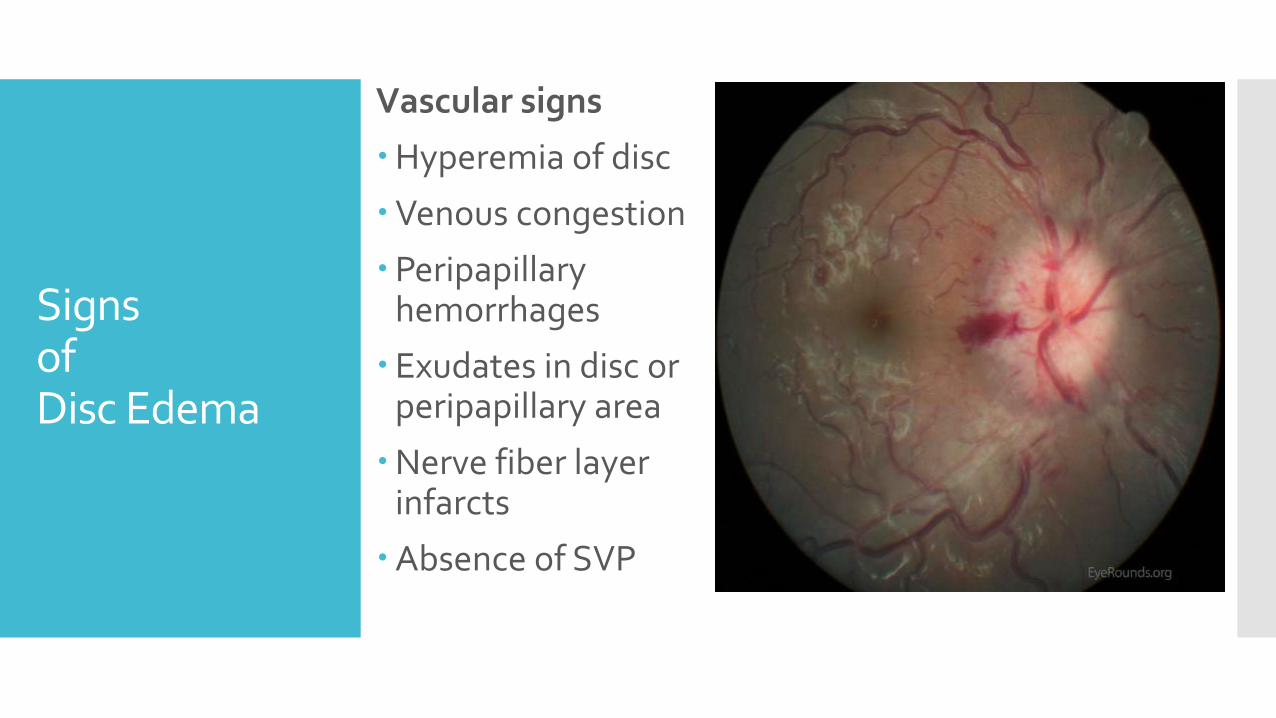
Vascular signs
Hyperemia of disc
Venous congestion
Peripapillary hemorrhages
Exudates in disc or peripapillary area
Nerve fiber layer infarcts
Absence of SVP
Mechanism of Vision Loss
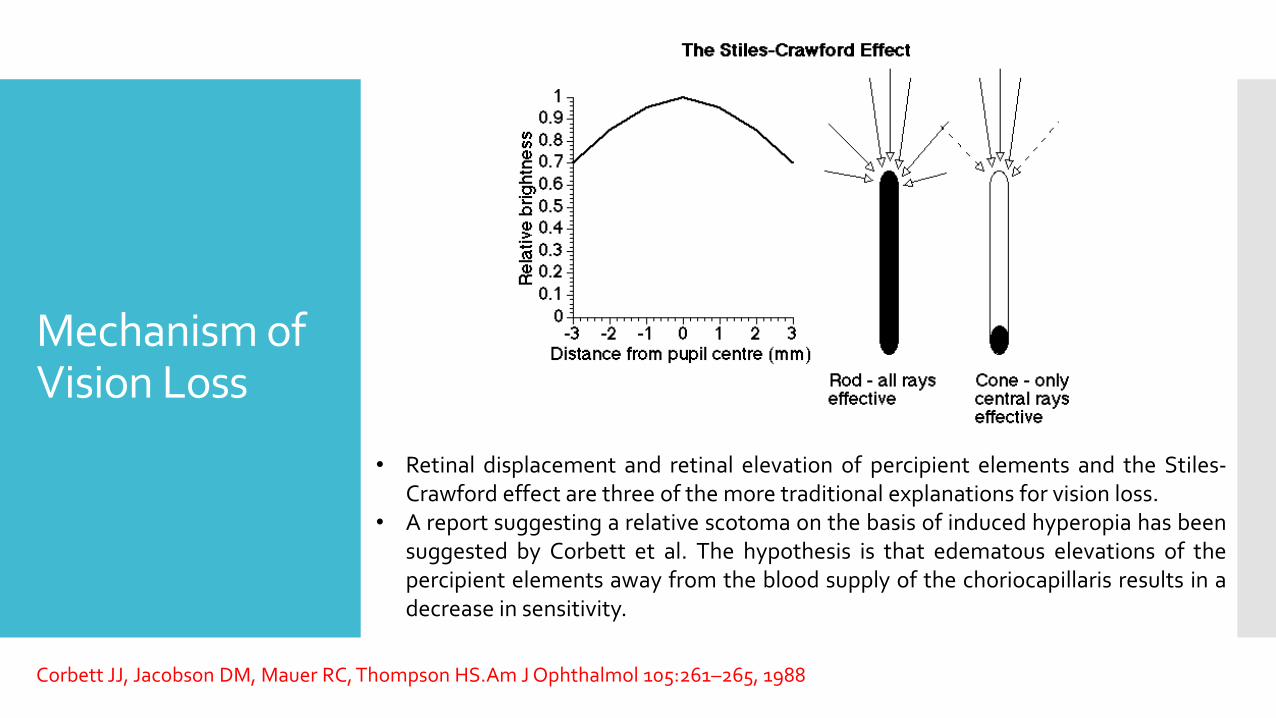
• Retinal displacement and retinal elevation of percipient elements and the Stiles-Crawford effect are three of the more traditional explanations for vision loss.
• A report suggesting a relative scotoma on the basis of induced hyperopia has beensuggested by Corbett et al. The hypothesis is that edematous elevations of thepercipient elements away from the blood supply of the choriocapillaris results in adecrease in sensitivity.
Corbett JJ, Jacobson DM, Mauer RC, Thompson HS.Am J Ophthalmol 105:261–265, 1988
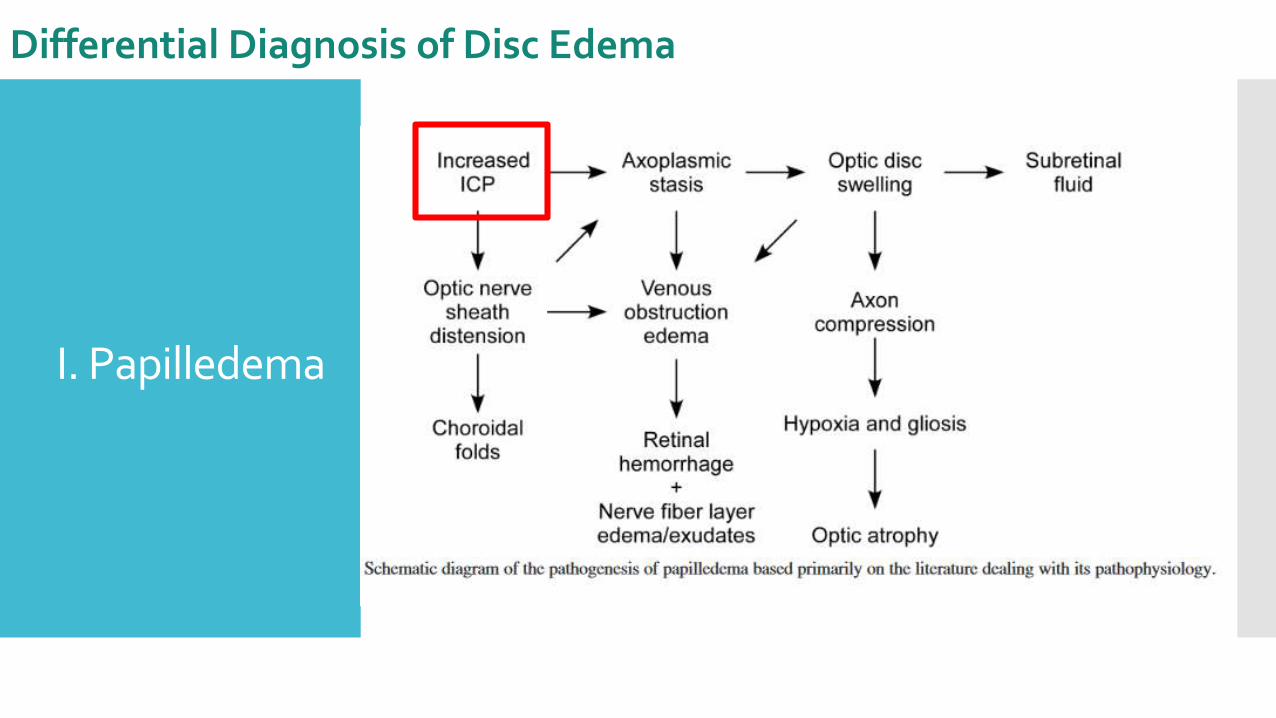
I. Papilledema
Differential Diagnosis of Disc Edema
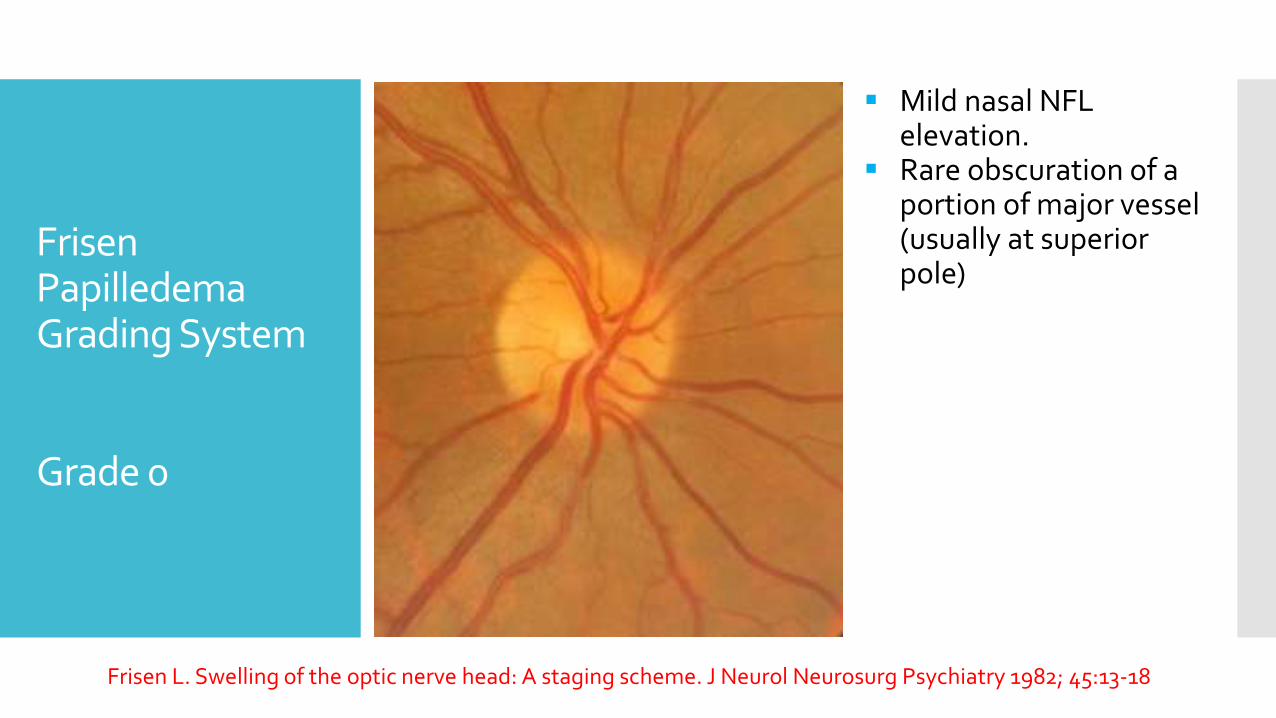
Frisen Papilledema Grading System
Grade 0
Mild nasal NFL elevation.
Rare obscuration of a portion of major vessel (usually at superior pole)
Frisen L. Swelling of the optic nerve head: A staging scheme. J Neurol Neurosurg Psychiatry 1982; 45:13-18
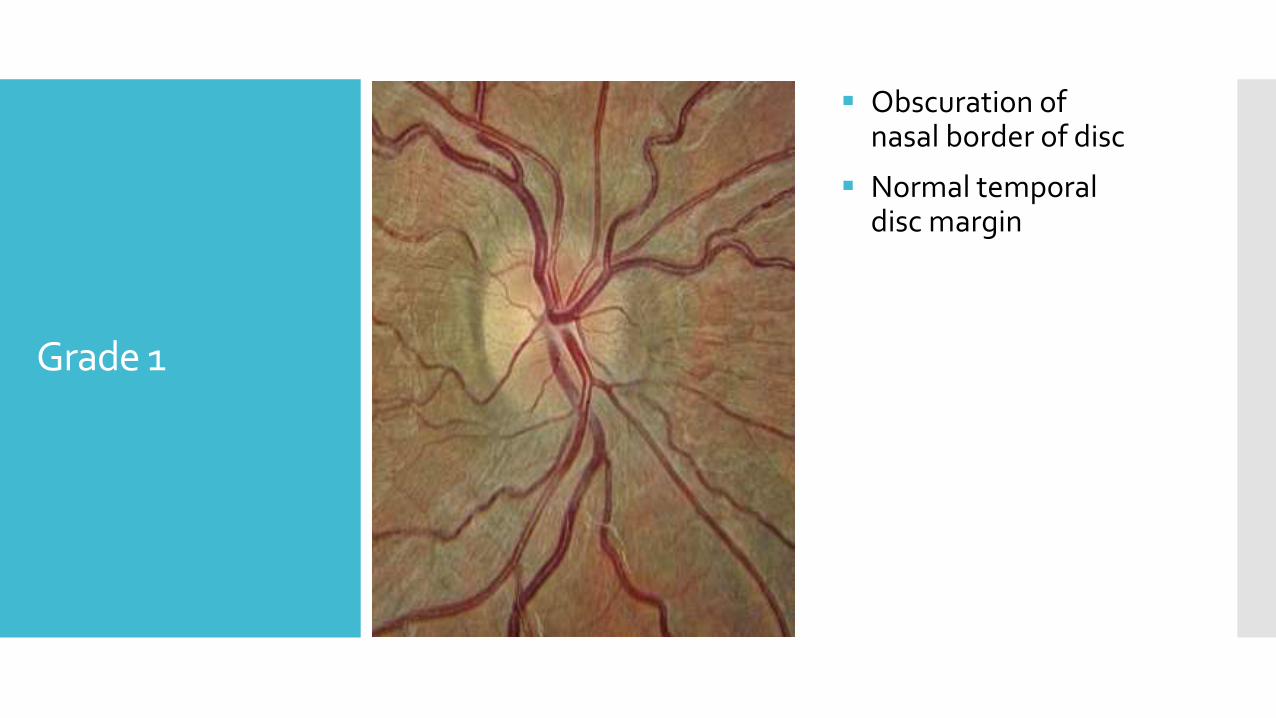
Grade 1
Obscuration of nasal border of disc
Normal temporal disc margin
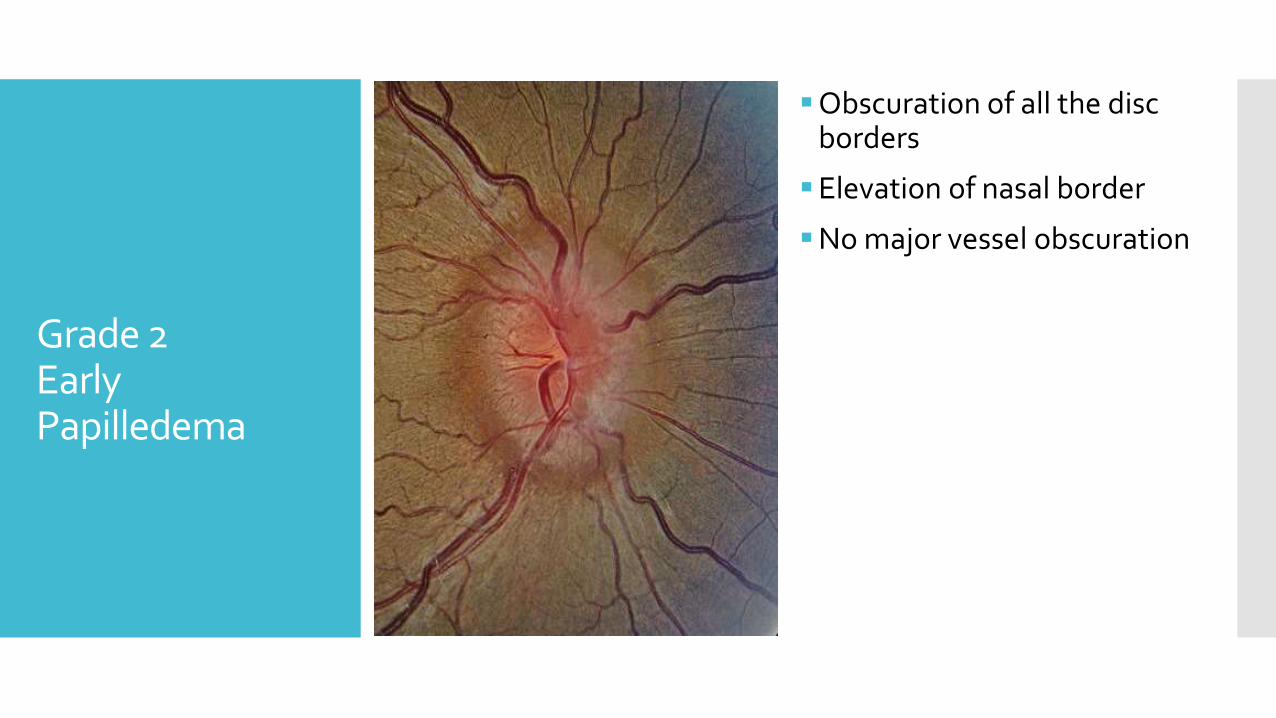
Grade 2Early Papilledema
Obscuration of all the disc borders
Elevation of nasal border
No major vessel obscuration
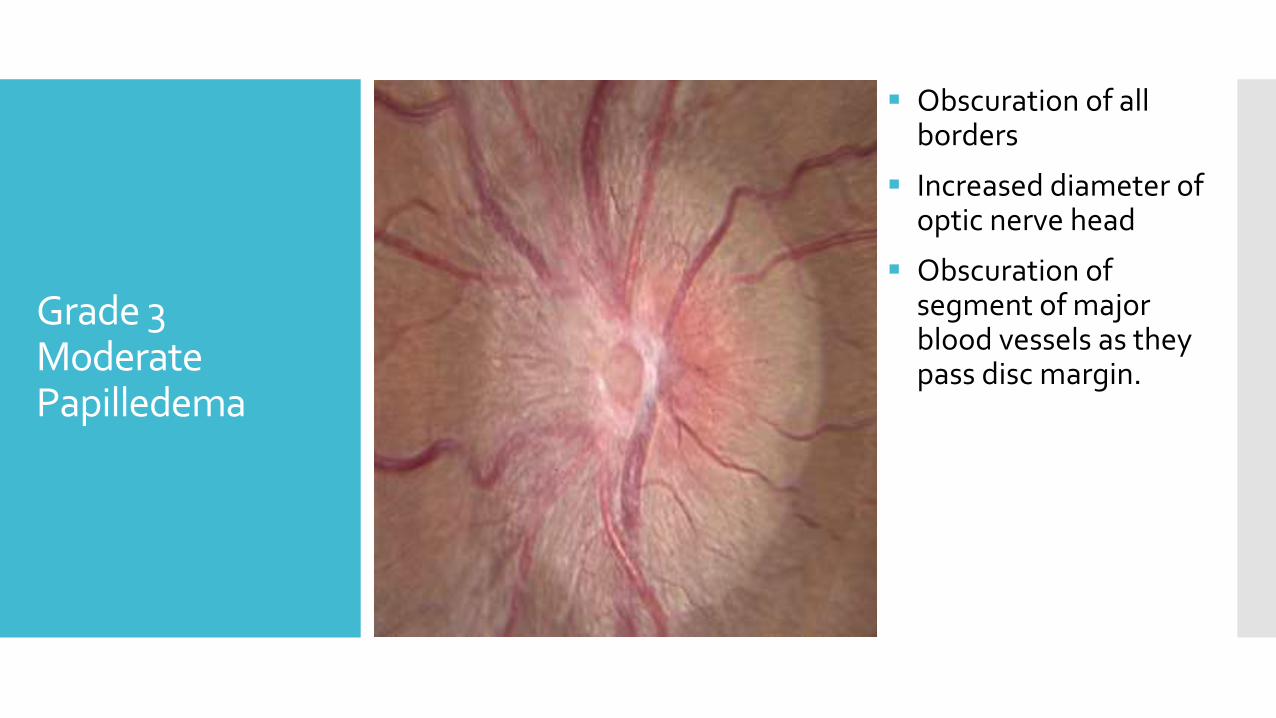
Grade 3ModeratePapilledema
Obscuration of all borders
Increased diameter of optic nerve head
Obscuration of segment of major blood vessels as they pass disc margin.
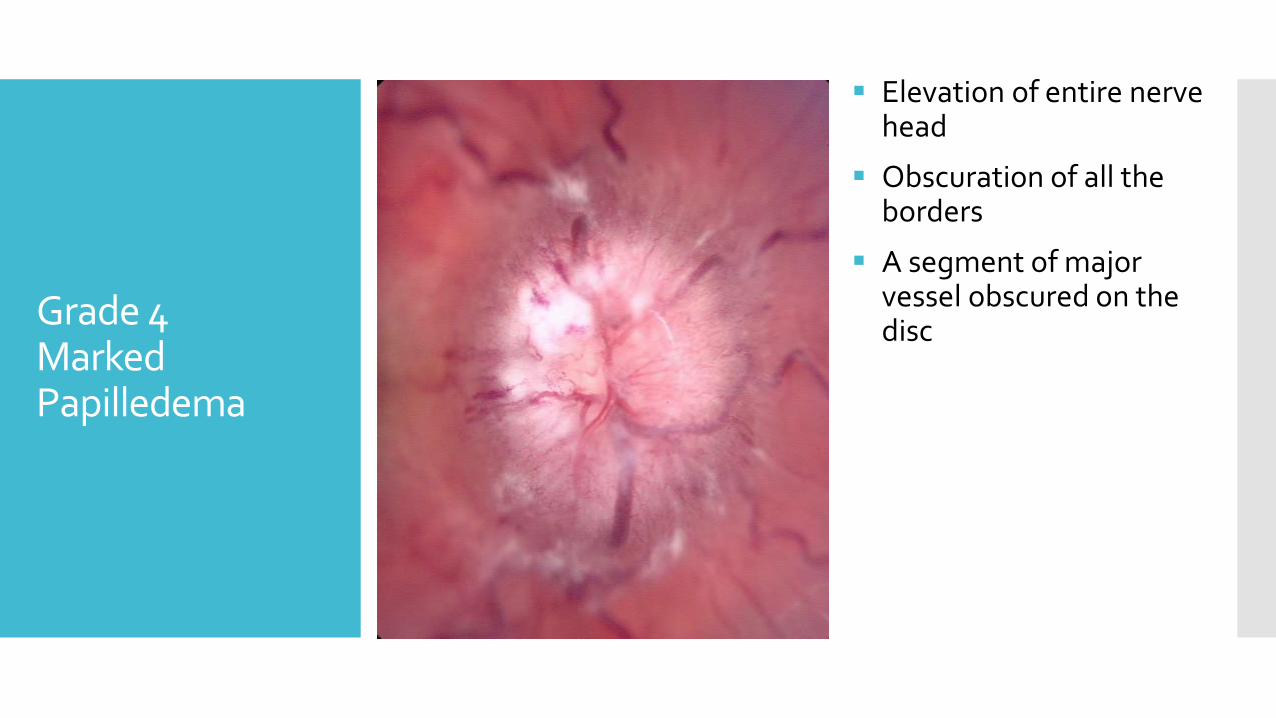
Grade 4MarkedPapilledema
Elevation of entire nerve head
Obscuration of all the borders
A segment of major vessel obscured on the disc
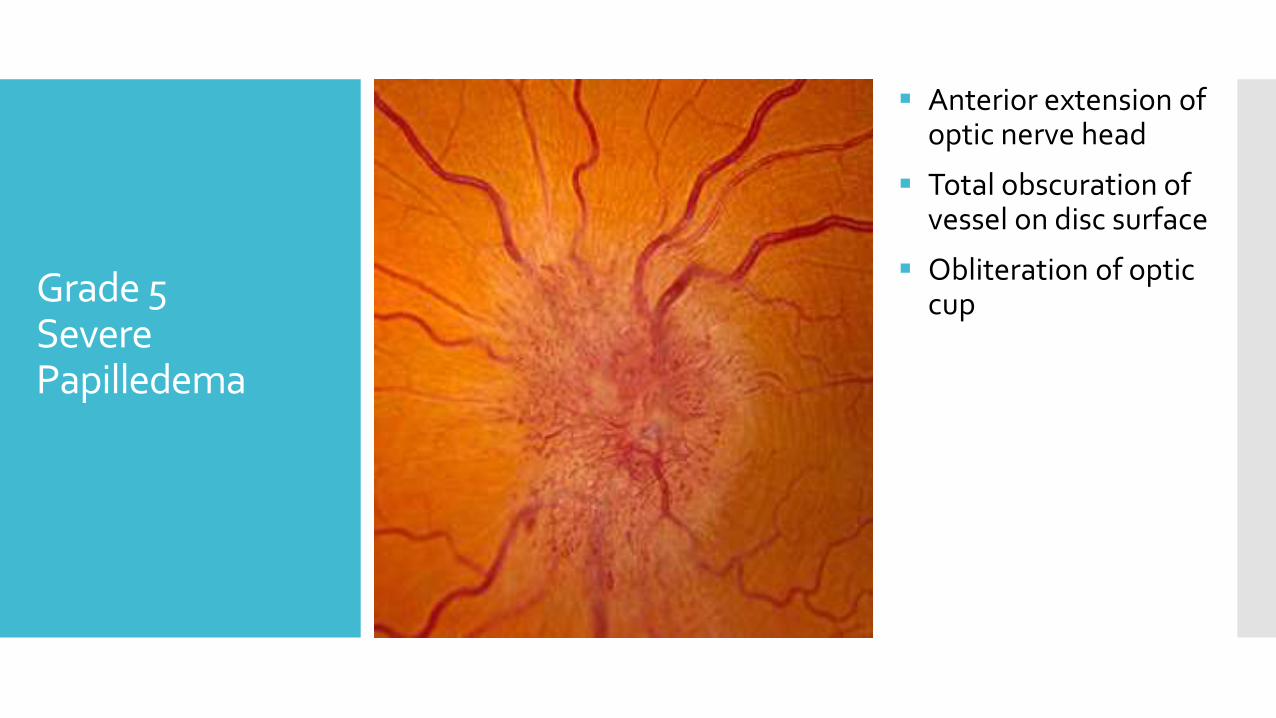
Grade 5Severe Papilledema
Anterior extension of optic nerve head
Total obscuration of vessel on disc surface
Obliteration of optic cup
Papilledemaor Papillitis?
Once true disc edema is established, papilledema(due to raised ICT) has to be distinguished fromother optic neuropathies which can be of variedetiology
Main difference: Visual acuity and optic nerve function Papilledema: Normal
Papillitis: Disturbed
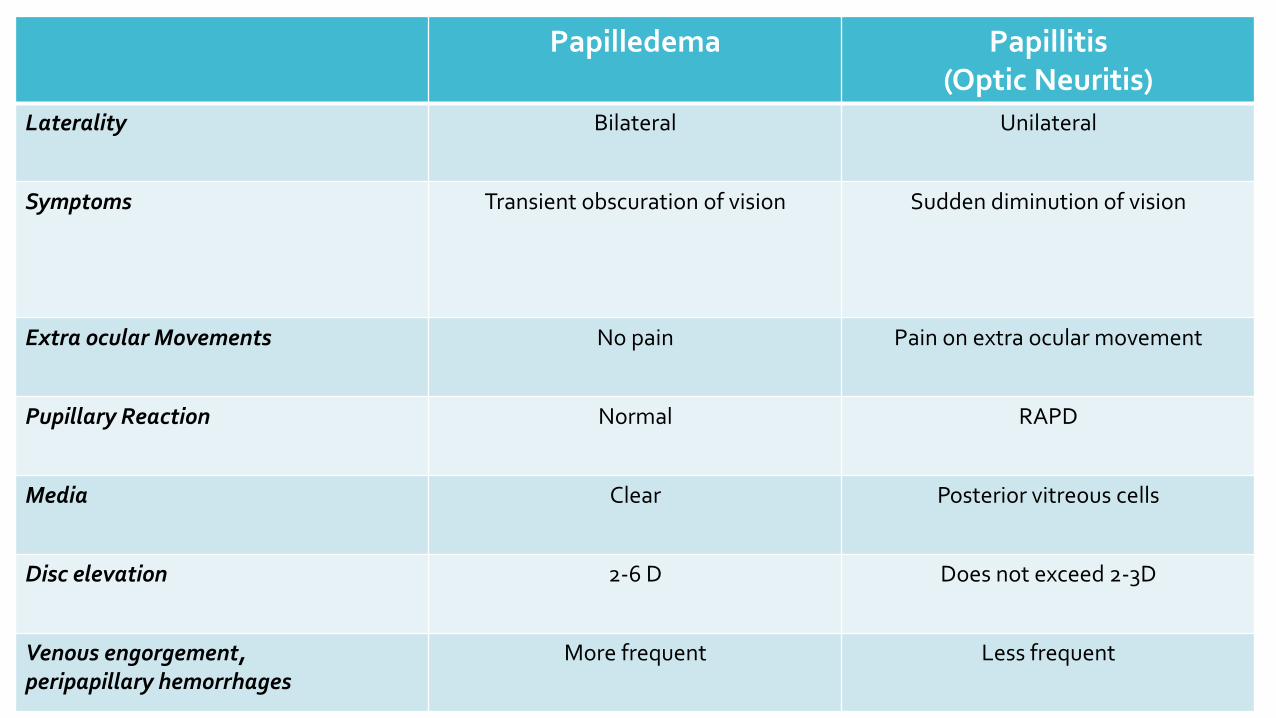
Papilledema Papillitis(Optic Neuritis)
Laterality Bilateral Unilateral
Symptoms Transient obscuration of vision Sudden diminution of vision
Extra ocular Movements No pain Pain on extra ocular movement
Pupillary Reaction Normal RAPD
Media Clear Posterior vitreous cells
Disc elevation 2-6 D Does not exceed 2-3D
Venous engorgement, peripapillary hemorrhages
More frequent Less frequent
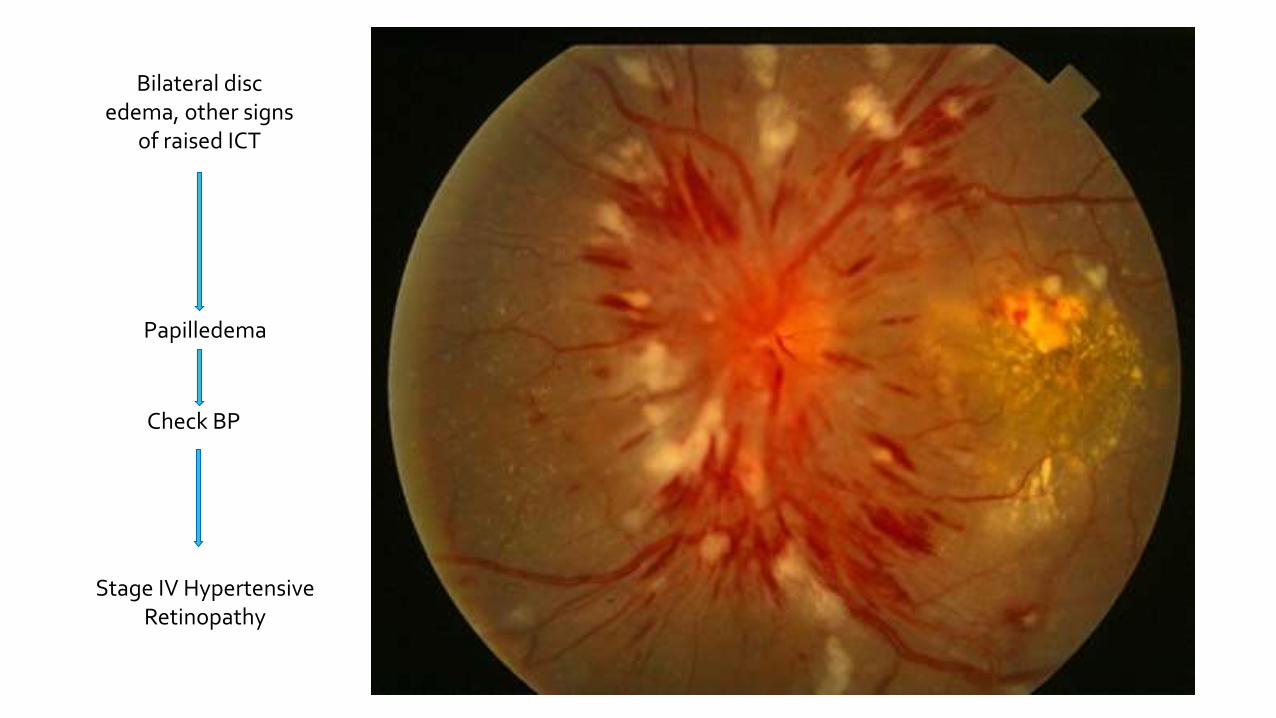
Papilledema
Check BP
Stage IV Hypertensive Retinopathy
Bilateral disc edema, other signs
of raised ICT
II. Grade IV Hypertensive Retinopathy
Malignant hypertension
Young individuals, smokers and uncontrolled blood pressure
Severe attenuation of arterioles
Neuroretinopathy, presence of disc edema, multiple cotton wool patches, hard exudates, macular star
Poor prognosis associated with renal insufficiency, stroke, myocardial infarction and death
Henderson AD, et al. Western Journal of Emergency Medicine. 2012;13(6):529-534.
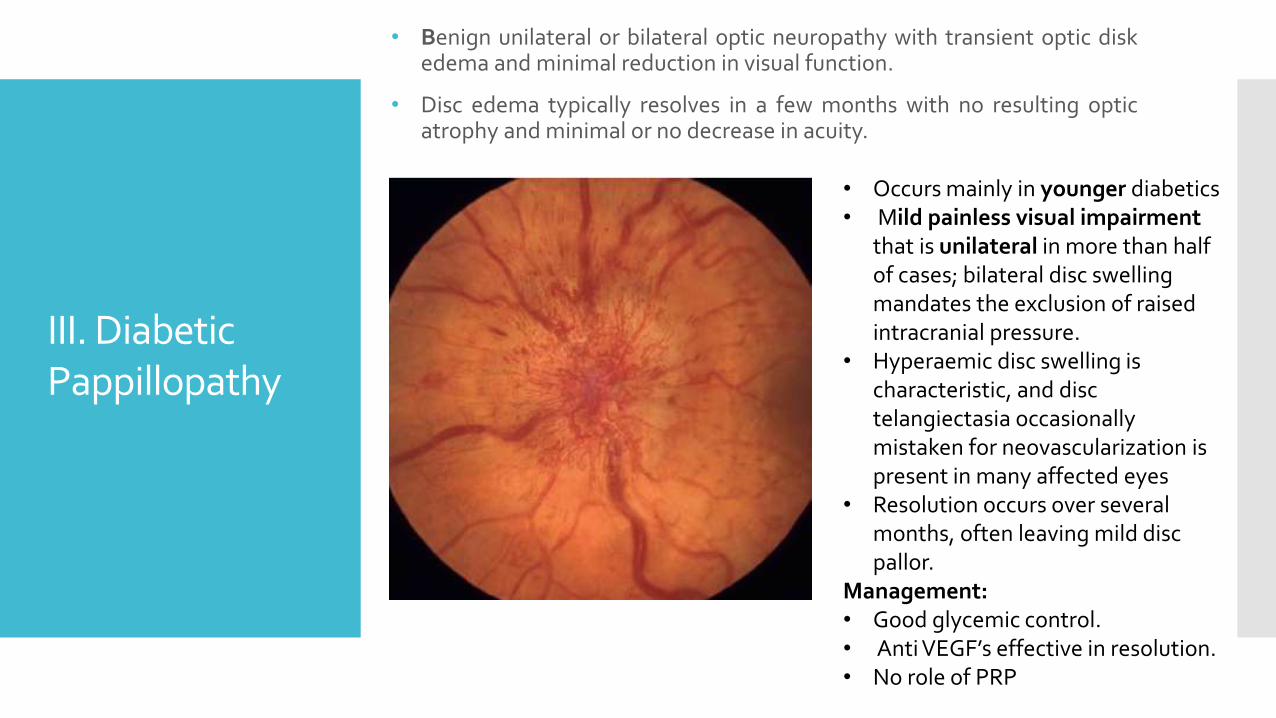
• Benign unilateral or bilateral optic neuropathy with transient optic diskedema and minimal reduction in visual function.
• Disc edema typically resolves in a few months with no resulting opticatrophy and minimal or no decrease in acuity.
III. Diabetic Pappillopathy
• Occurs mainly in younger diabetics• Mild painless visual impairment
that is unilateral in more than half of cases; bilateral disc swelling mandates the exclusion of raised intracranial pressure.
• Hyperaemic disc swelling is characteristic, and disc telangiectasia occasionally mistaken for neovascularization is present in many affected eyes
• Resolution occurs over several months, often leaving mild disc pallor.
Management:• Good glycemic control.• Anti VEGF’s effective in resolution.• No role of PRP
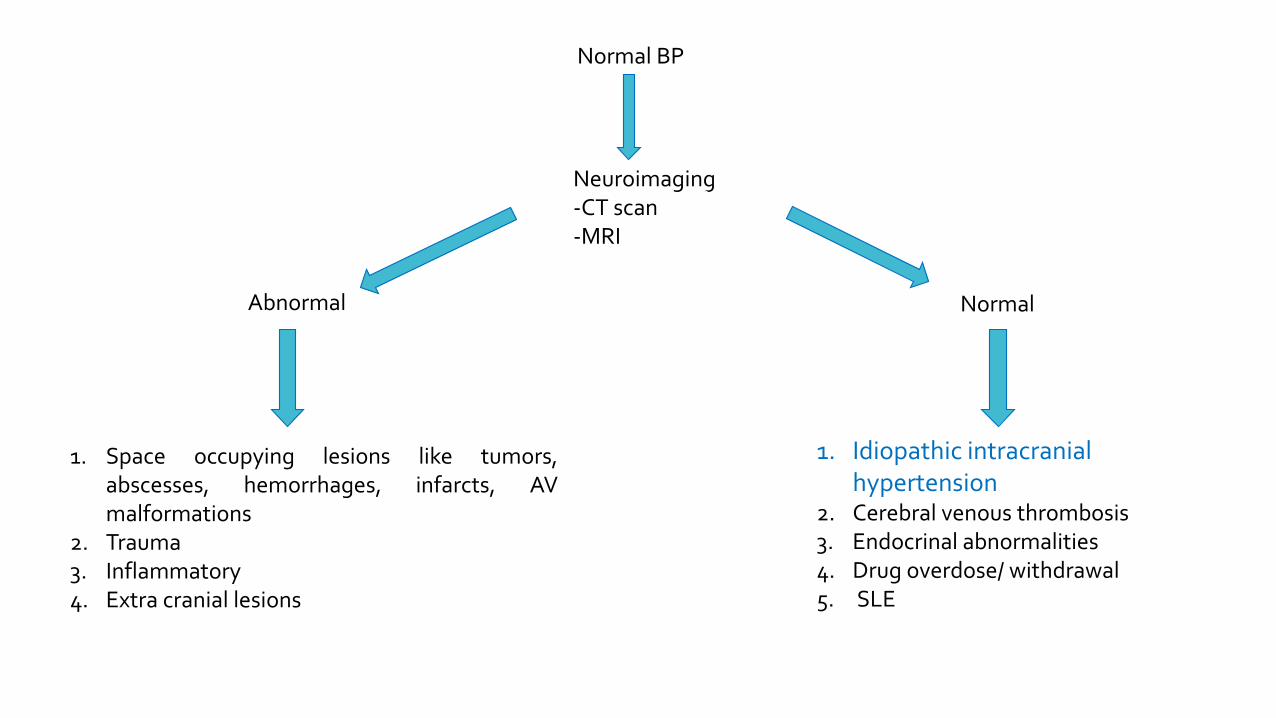
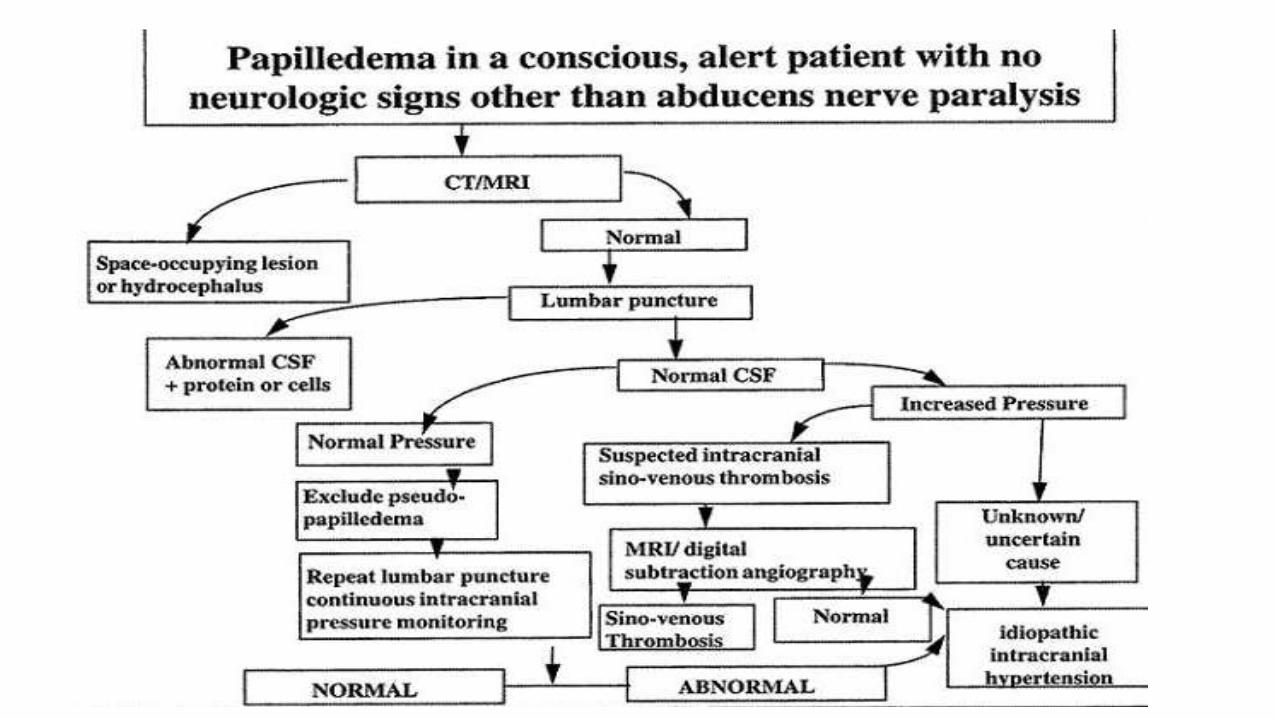
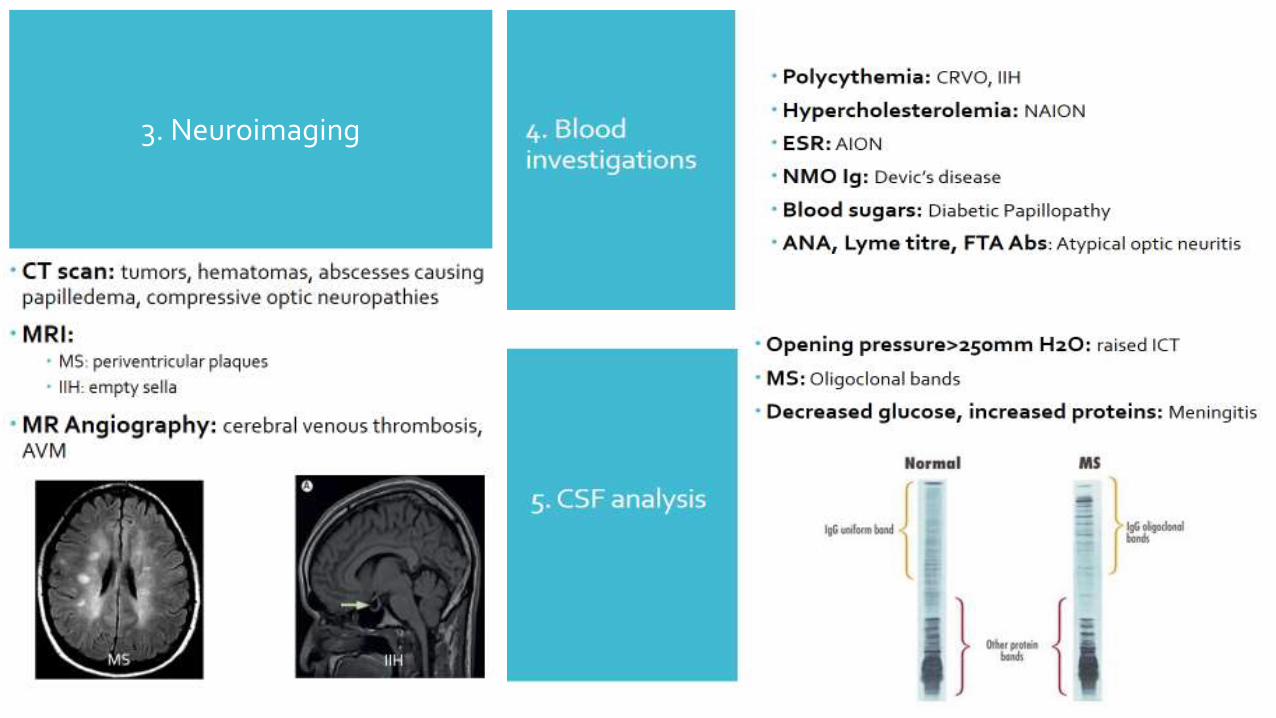
Neuroimaging -CT scan-MRI
Abnormal
1. Space occupying lesions like tumors,abscesses, hemorrhages, infarcts, AVmalformations
2. Trauma3. Inflammatory4. Extra cranial lesions
1. Idiopathic intracranial hypertension
2. Cerebral venous thrombosis3. Endocrinal abnormalities4. Drug overdose/ withdrawal5. SLE
Normal
Normal BP
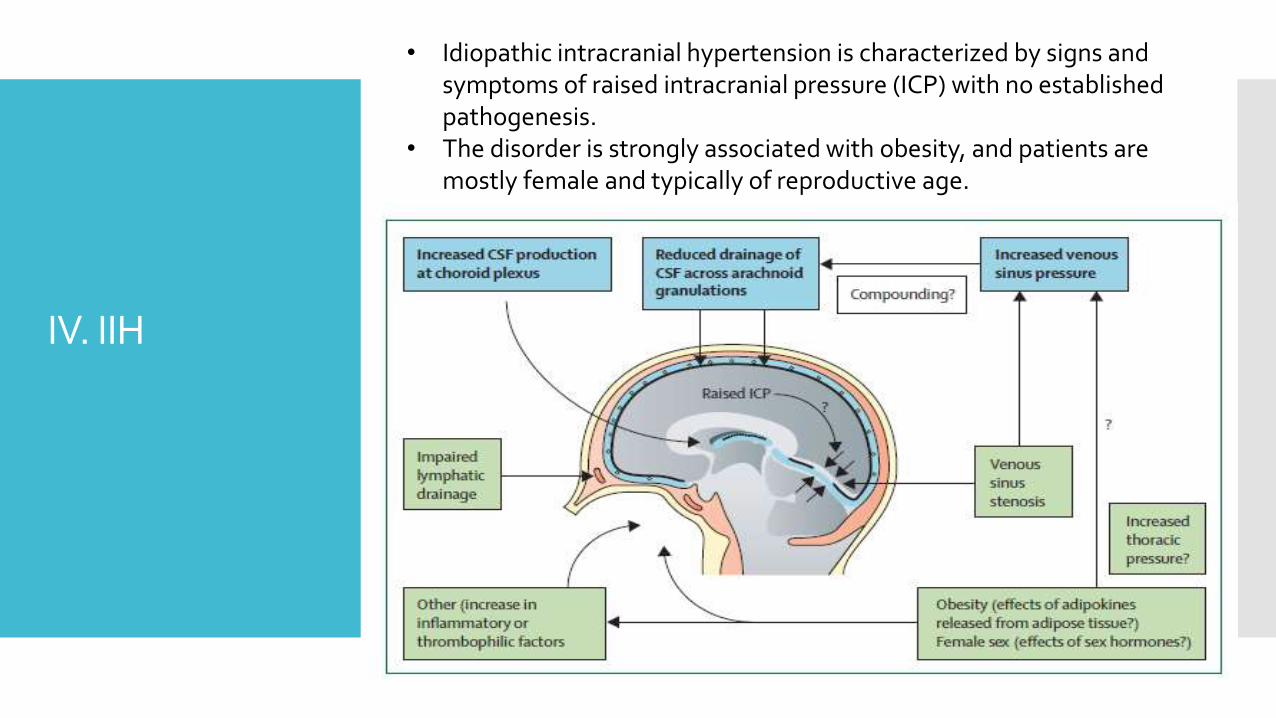
IV. IIH
• Idiopathic intracranial hypertension is characterized by signs and symptoms of raised intracranial pressure (ICP) with no established pathogenesis.
• The disorder is strongly associated with obesity, and patients are mostly female and typically of reproductive age.
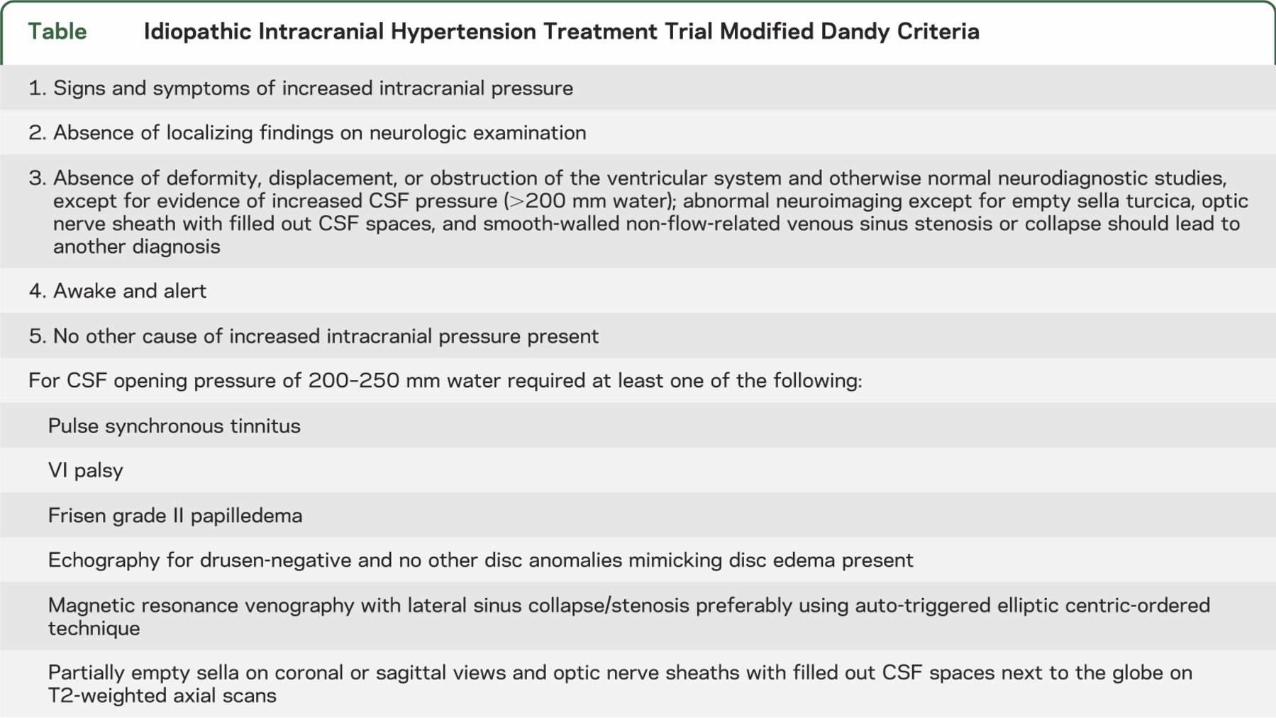
Modified Dandy criteriafor IIH
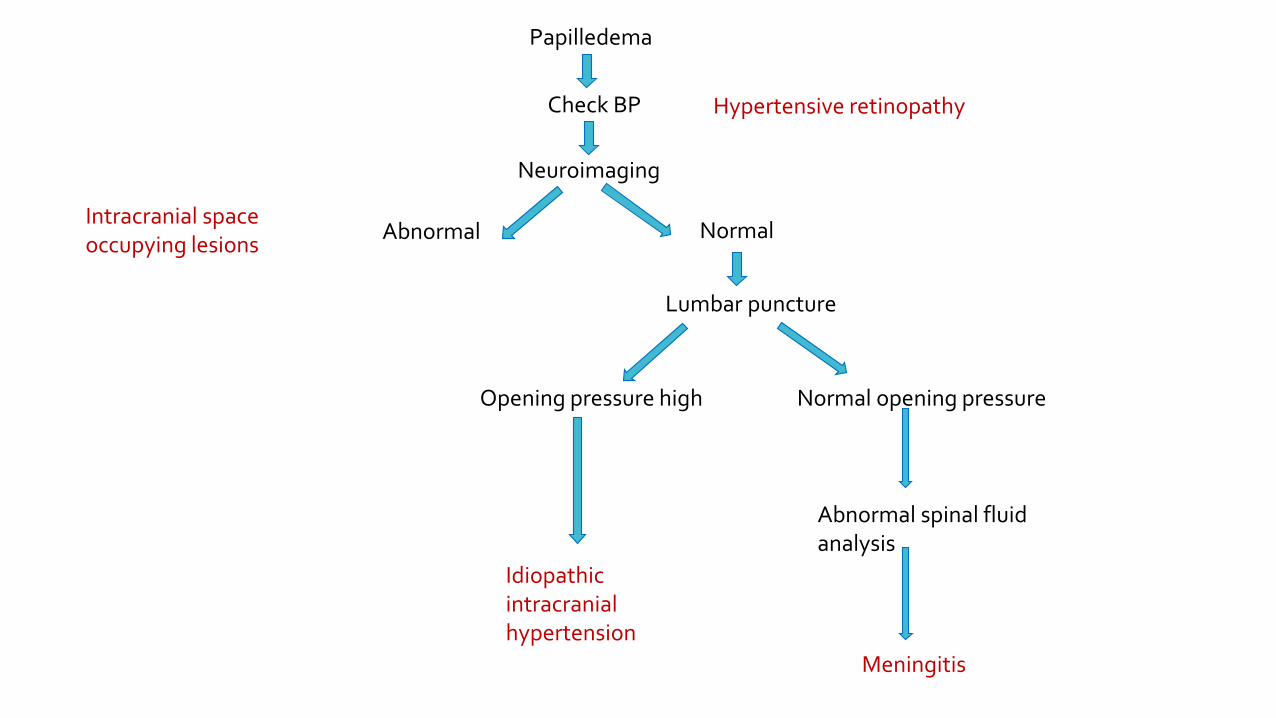
Papilledema
Check BP Hypertensive retinopathy
Neuroimaging
Abnormal Normal Intracranial space occupying lesions
Lumbar puncture
Opening pressure high
Idiopathic intracranial hypertension
Normal opening pressure
Abnormal spinal fluid analysis
Meningitis
Characteristics of optic neuropathies
Optic neuropathies should be considered under two circumstances
Visual loss associated with anomalous, swollen or pale disc
Fundus is normal, but acuity, color vision, field abnormalities are accompanied by RAPD
Other optic neuropathies causing Disc Edema
Anterior optic neuropathyInflammatory optic neuropathy
Ischemic optic neuropathy
Compressive optic neuropathy
Toxic and hereditary optic neuropathy
Infiltrative optic neuropathy
Intraocular causes CRVO, posterior uveitis, posterior scleritis, hypotony
Neuroretinitis
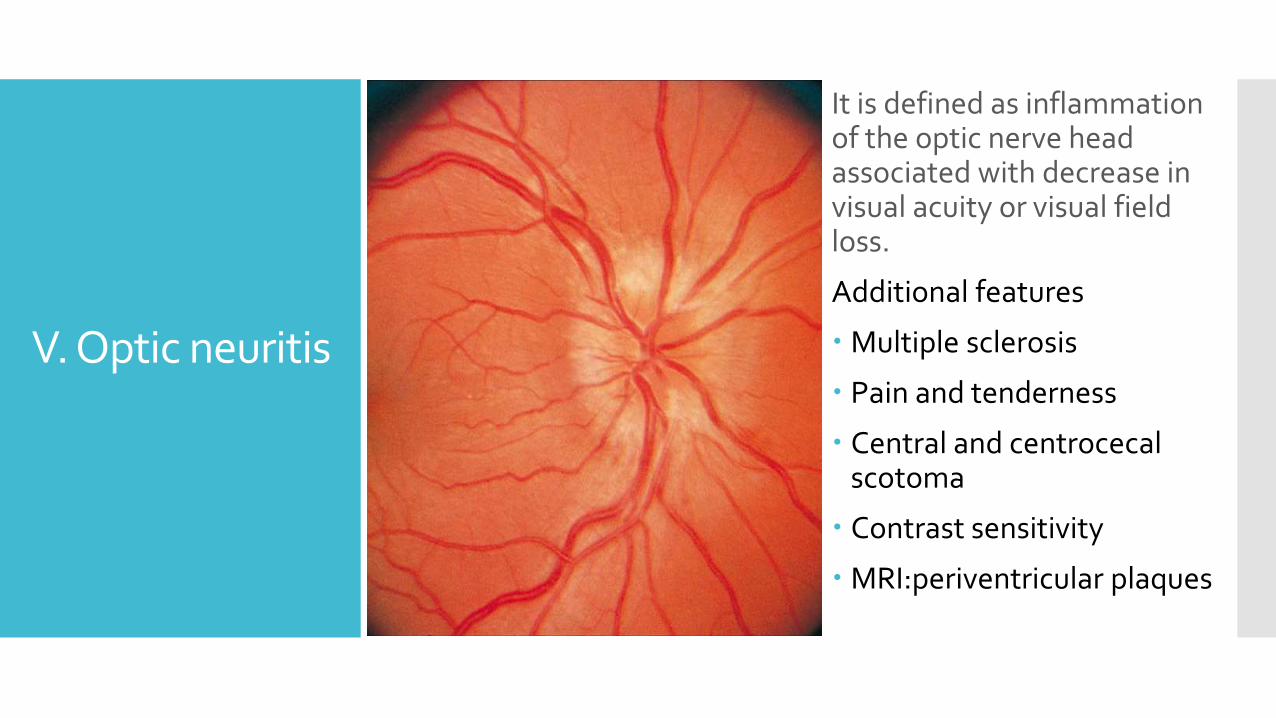
V. Optic neuritis
It is defined as inflammation of the optic nerve head associated with decrease in visual acuity or visual field loss.
Additional features
Multiple sclerosis
Pain and tenderness
Central and centrocecalscotoma
Contrast sensitivity
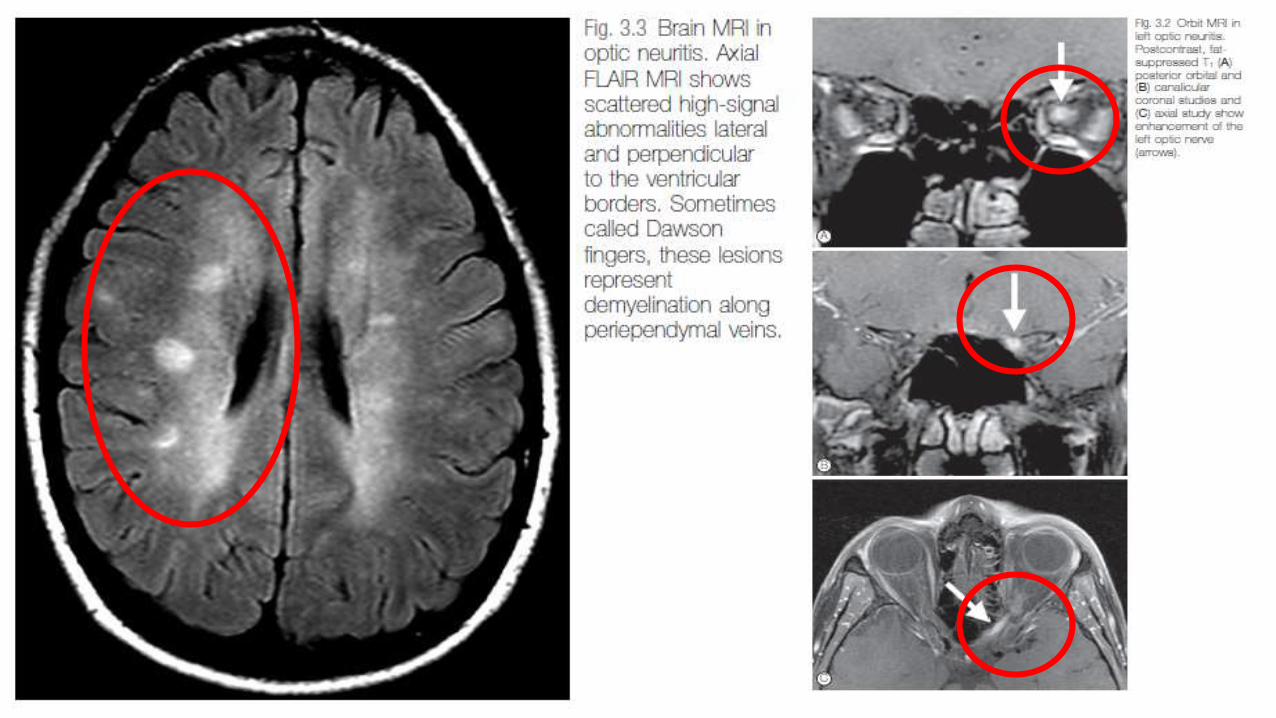
MRI:periventricular plaques
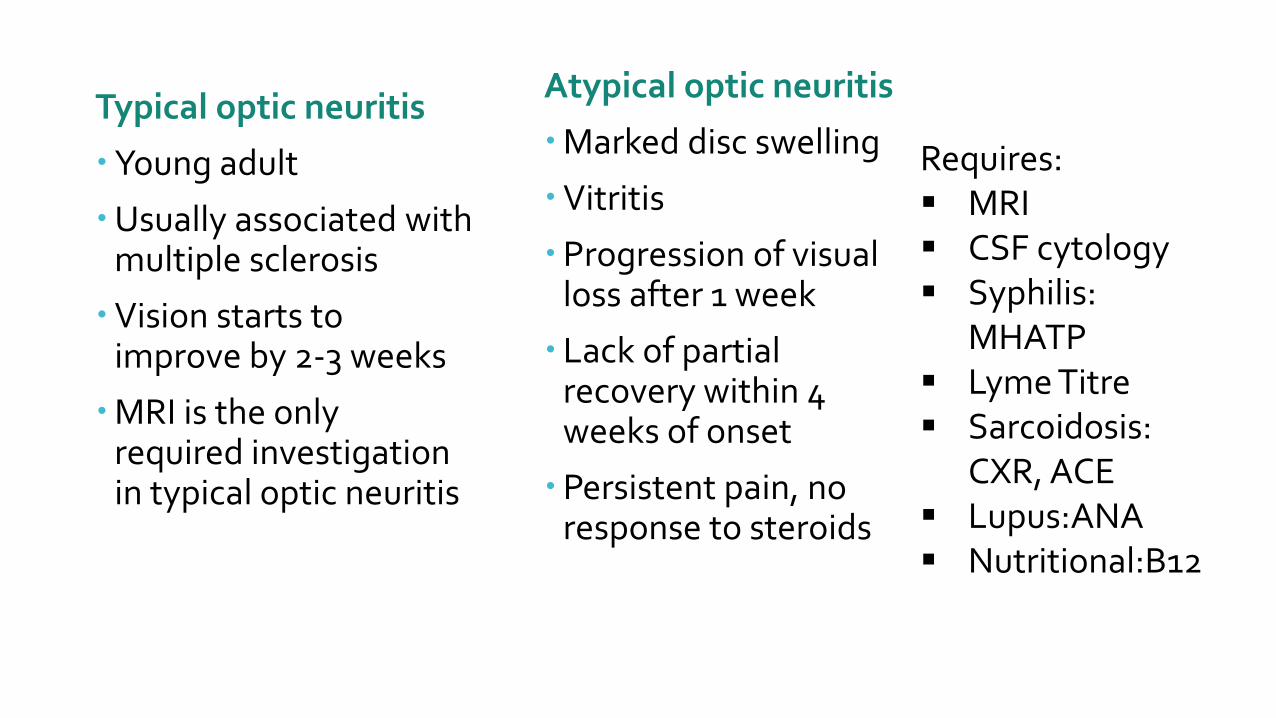
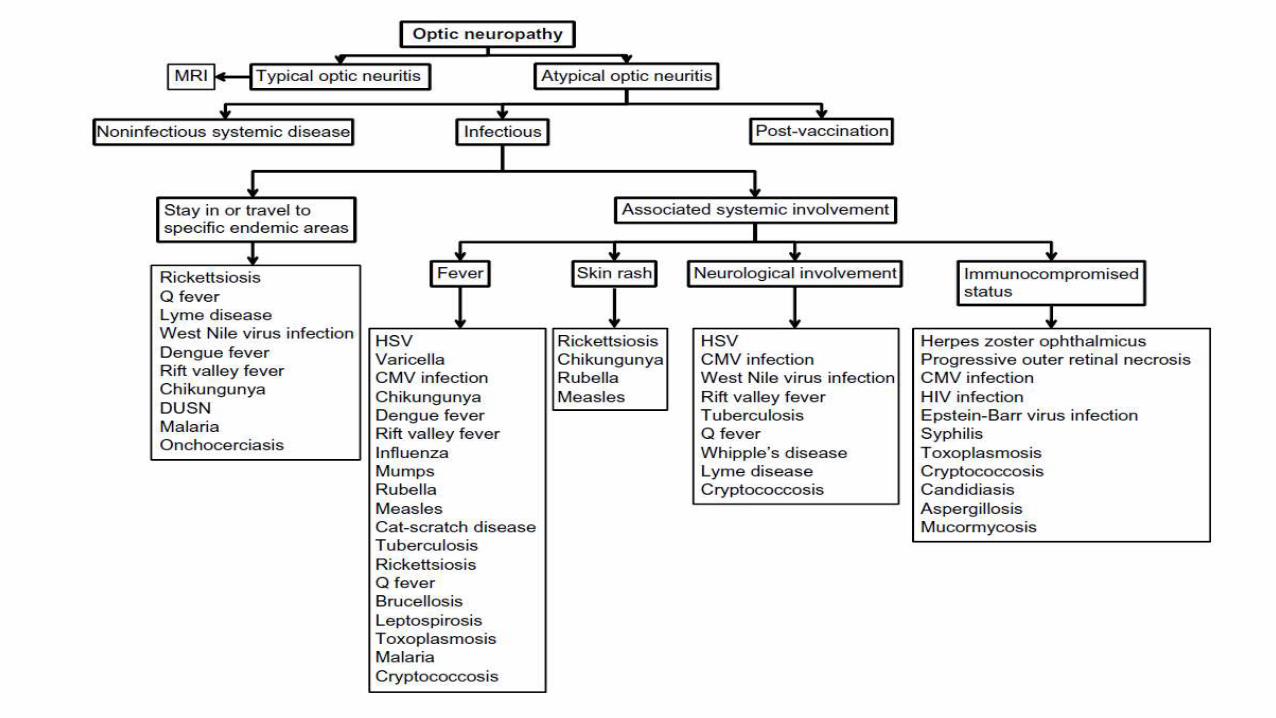
Typical optic neuritis
Young adult
Usually associated with multiple sclerosis
Vision starts to improve by 2-3 weeks
MRI is the only required investigation in typical optic neuritis
Atypical optic neuritis
Marked disc swelling
Vitritis
Progression of visual loss after 1 week
Lack of partial recovery within 4 weeks of onset
Persistent pain, no response to steroids
Requires: MRI CSF cytology Syphilis:
MHATP Lyme Titre Sarcoidosis:
CXR, ACE Lupus:ANA Nutritional:B12
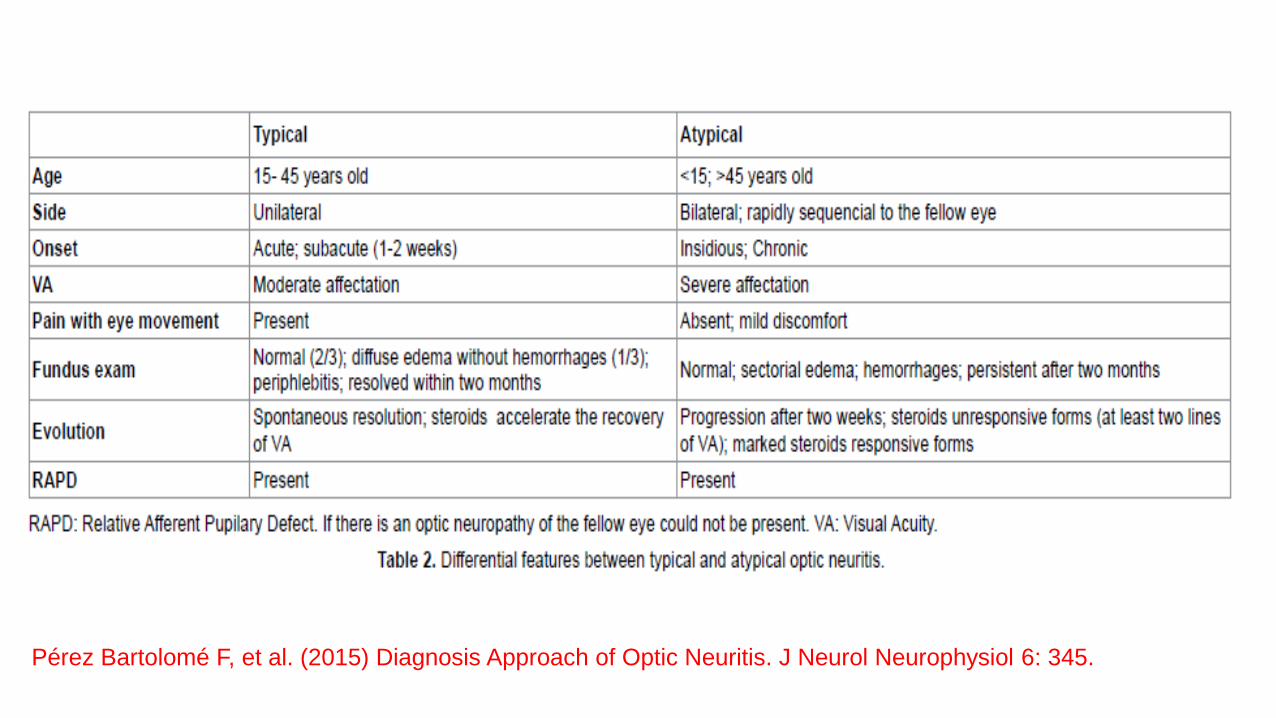
Pérez Bartolomé F, et al. (2015) Diagnosis Approach of Optic Neuritis. J Neurol Neurophysiol 6: 345.
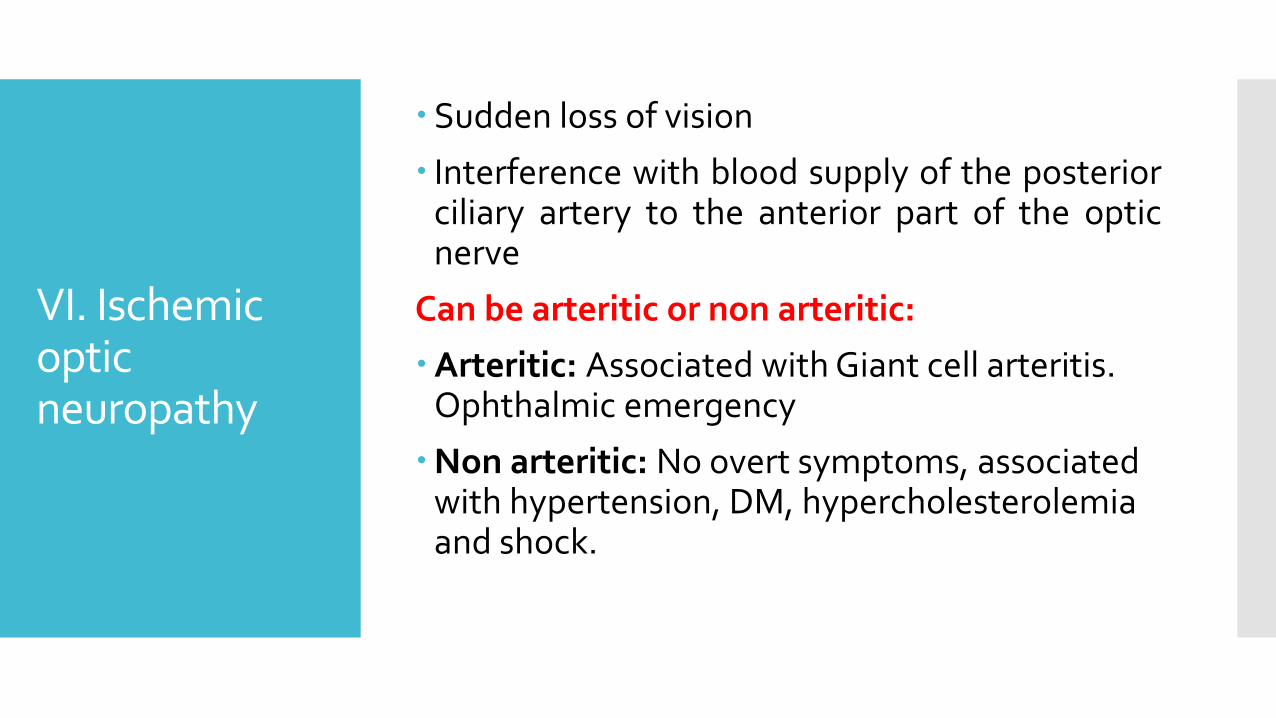
VI. Ischemic optic neuropathy
Sudden loss of vision
Interference with blood supply of the posteriorciliary artery to the anterior part of the opticnerve
Can be arteritic or non arteritic:
Arteritic: Associated with Giant cell arteritis. Ophthalmic emergency
Non arteritic: No overt symptoms, associated with hypertension, DM, hypercholesterolemia and shock.
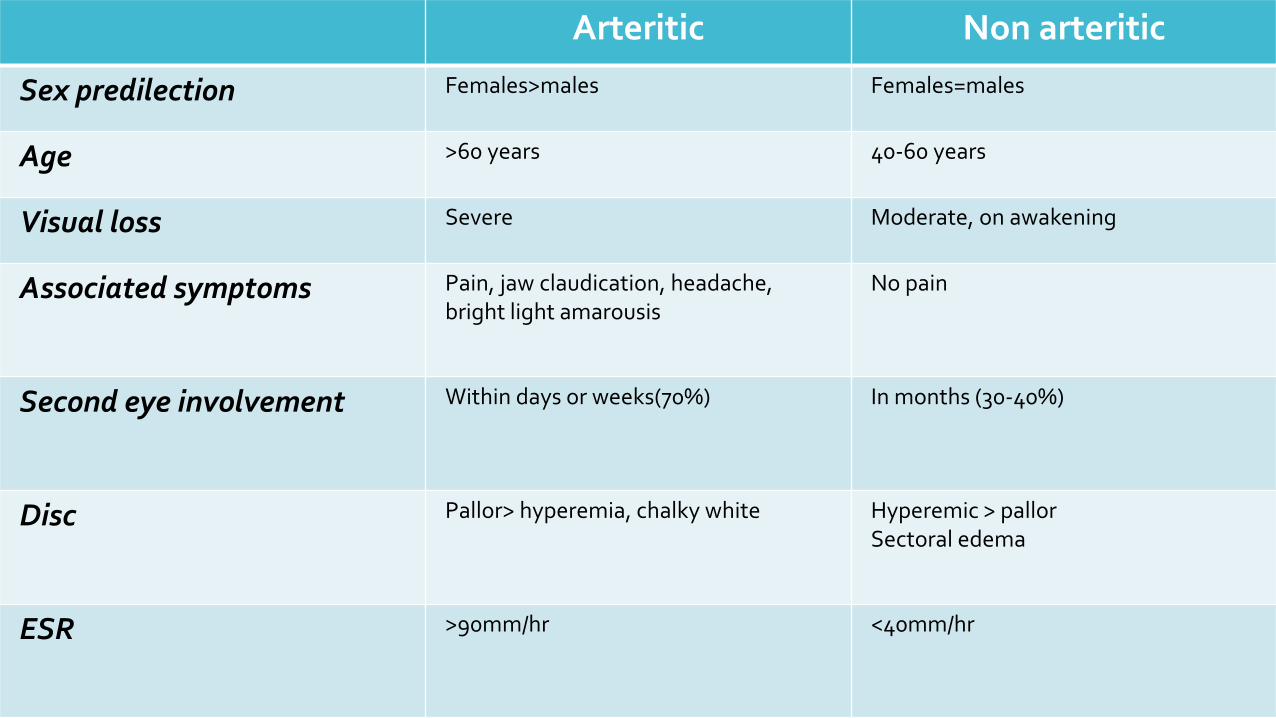
Arteritic Non arteritic
Sex predilection Females>males Females=males
Age >60 years 40-60 years
Visual loss Severe Moderate, on awakening
Associated symptoms Pain, jaw claudication, headache, bright light amarousis
No pain
Second eye involvement Within days or weeks(70%) In months (30-40%)
Disc Pallor> hyperemia, chalky white Hyperemic > pallorSectoral edema
ESR >90mm/hr <40mm/hr
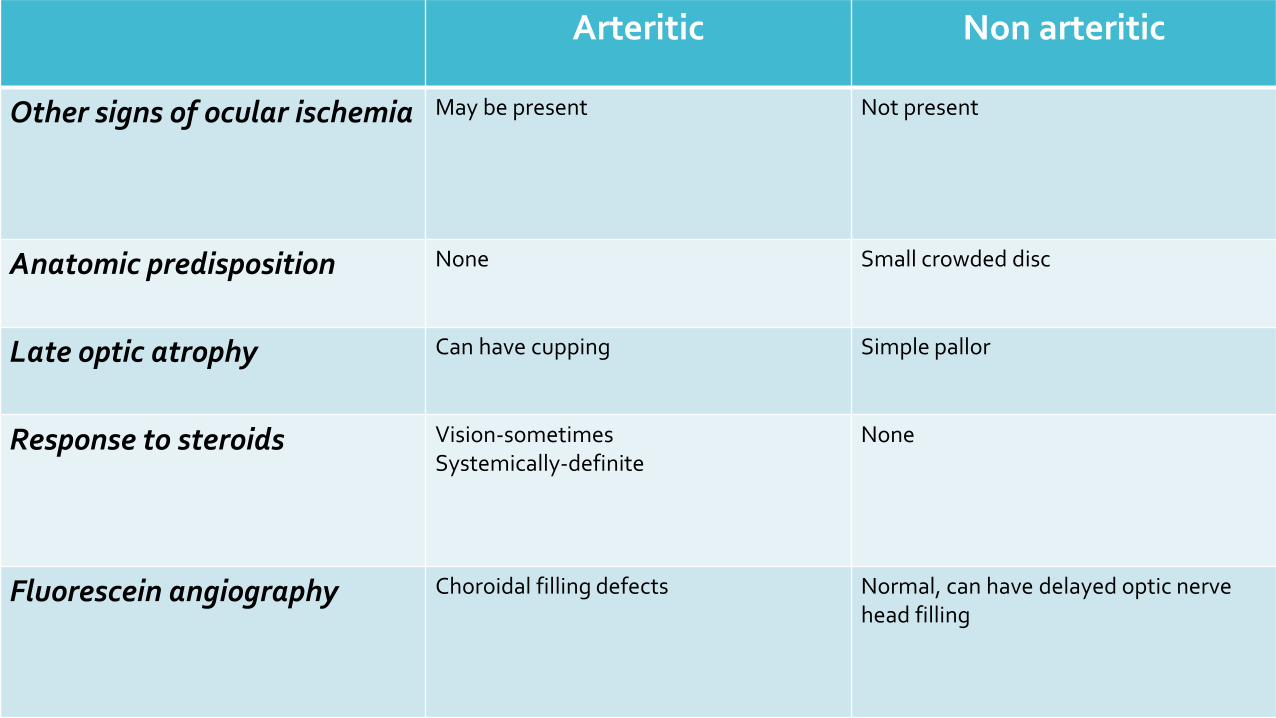
Arteritic Non arteritic
Other signs of ocular ischemia May be present Not present
Anatomic predisposition None Small crowded disc
Late optic atrophy Can have cupping Simple pallor
Response to steroids Vision-sometimesSystemically-definite
None
Fluorescein angiography Choroidal filling defects Normal, can have delayed optic nerve head filling
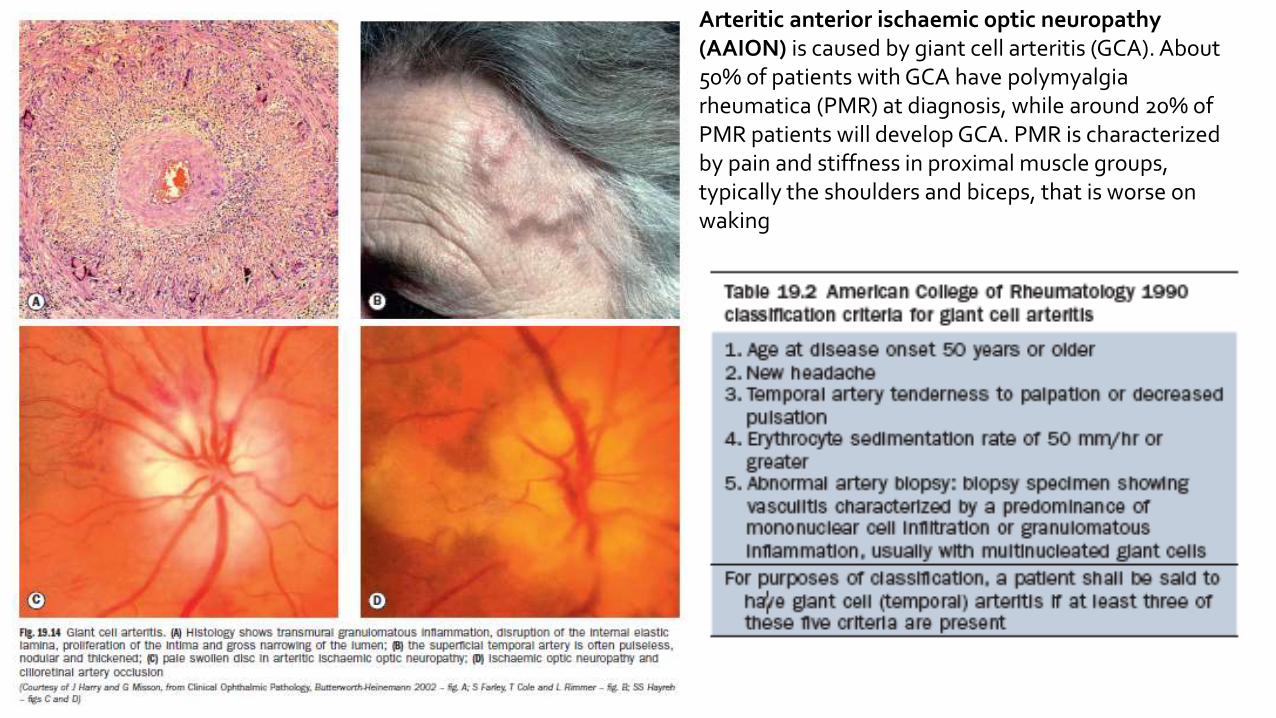
Arteritic anterior ischaemic optic neuropathy (AAION) is caused by giant cell arteritis (GCA). About 50% of patients with GCA have polymyalgia rheumatica (PMR) at diagnosis, while around 20% of PMR patients will develop GCA. PMR is characterized by pain and stiffness in proximal muscle groups, typically the shoulders and biceps, that is worse on waking
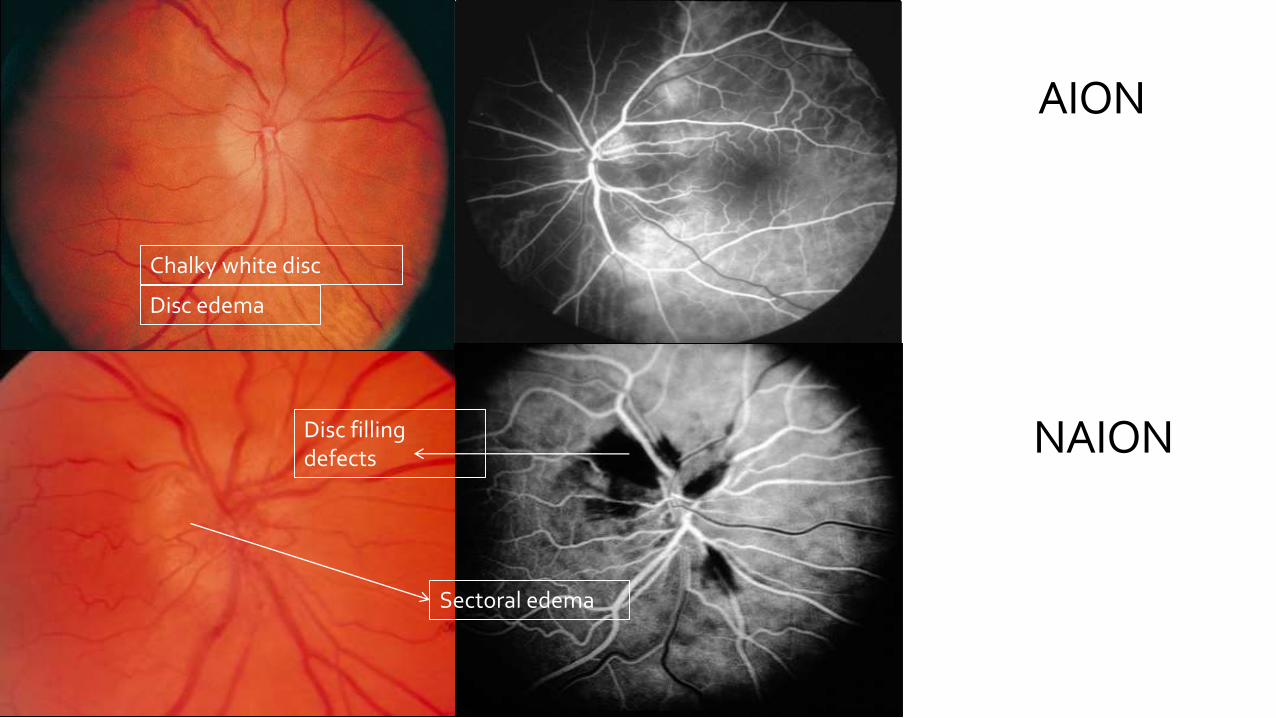
AION
NAIONDisc filling defects
Sectoral edema
Chalky white disc
Disc edema
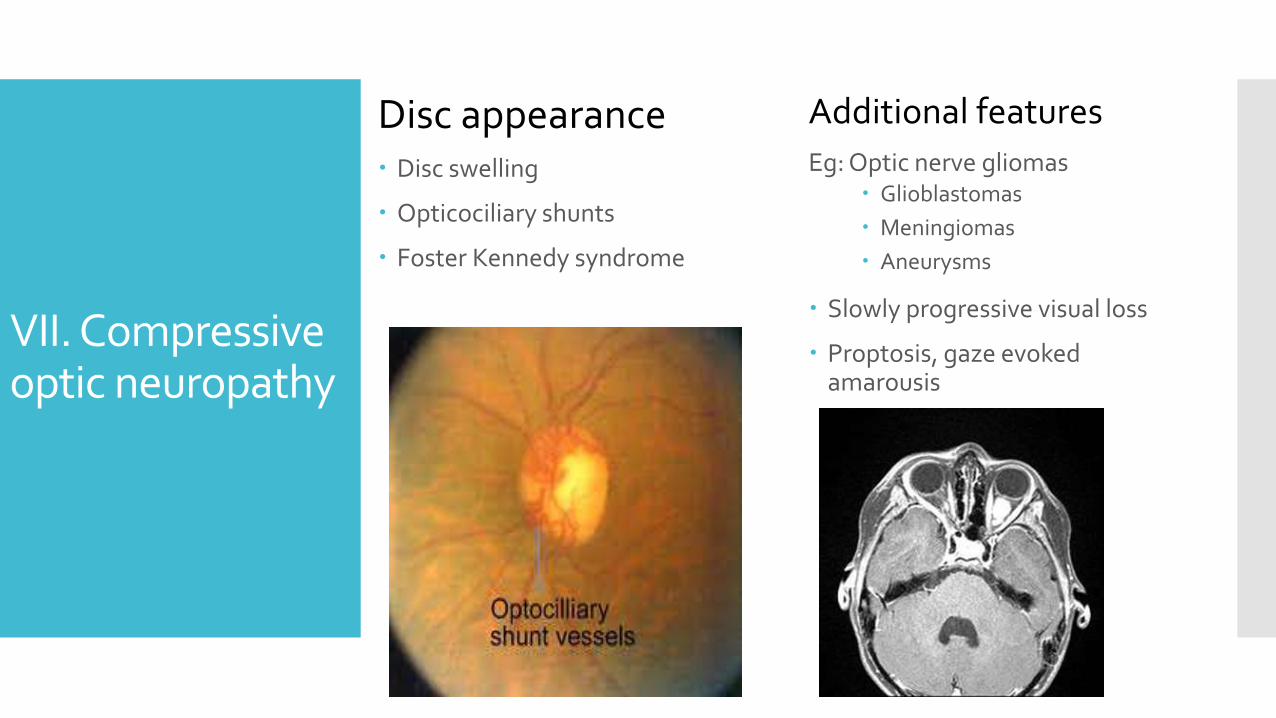
VII. Compressive optic neuropathy
Disc appearance Disc swelling
Opticociliary shunts
Foster Kennedy syndrome
Additional features
Eg: Optic nerve gliomas Glioblastomas
Meningiomas
Aneurysms
Slowly progressive visual loss
Proptosis, gaze evoked amarousis
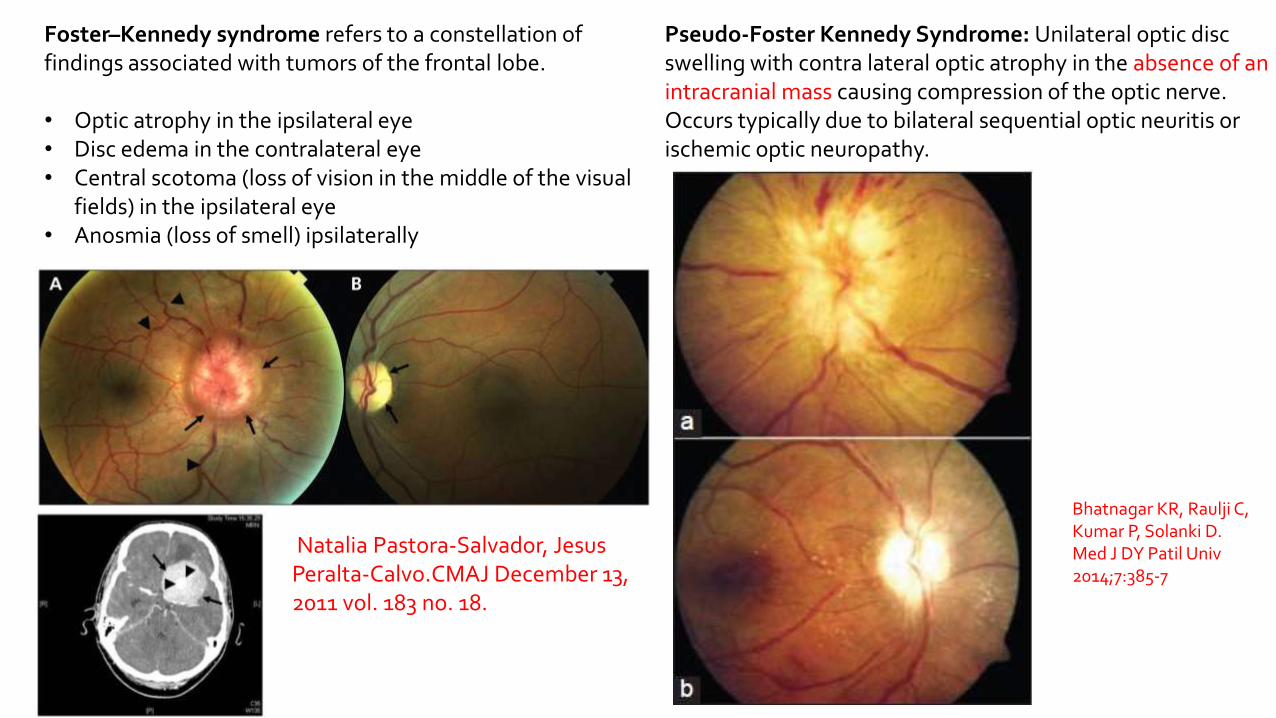
Pseudo-Foster Kennedy Syndrome: Unilateral optic disc swelling with contra lateral optic atrophy in the absence of an intracranial mass causing compression of the optic nerve. Occurs typically due to bilateral sequential optic neuritis or ischemic optic neuropathy.
Foster–Kennedy syndrome refers to a constellation of findings associated with tumors of the frontal lobe.
• Optic atrophy in the ipsilateral eye• Disc edema in the contralateral eye• Central scotoma (loss of vision in the middle of the visual
fields) in the ipsilateral eye• Anosmia (loss of smell) ipsilaterally
Bhatnagar KR, Raulji C, Kumar P, Solanki D. Med J DY Patil Univ2014;7:385-7
Natalia Pastora-Salvador, Jesus Peralta-Calvo.CMAJ December 13, 2011 vol. 183 no. 18.
VIII. Hereditary optic neuropathy
Disc appearance
Disc hyperemia
Obscuration of disc margins
Dilated capillaries on disc surface that may extend into surrounding retina (telangiectatic microaneurysms),
Additional features
Swelling of NFL layer and dilatation
Tortuosity of posterior pole vasculature
Maternally inherited mt DNA mutations
Males, 15-35 years
Subacute painless severe loss of vision in one eye, followed by the other
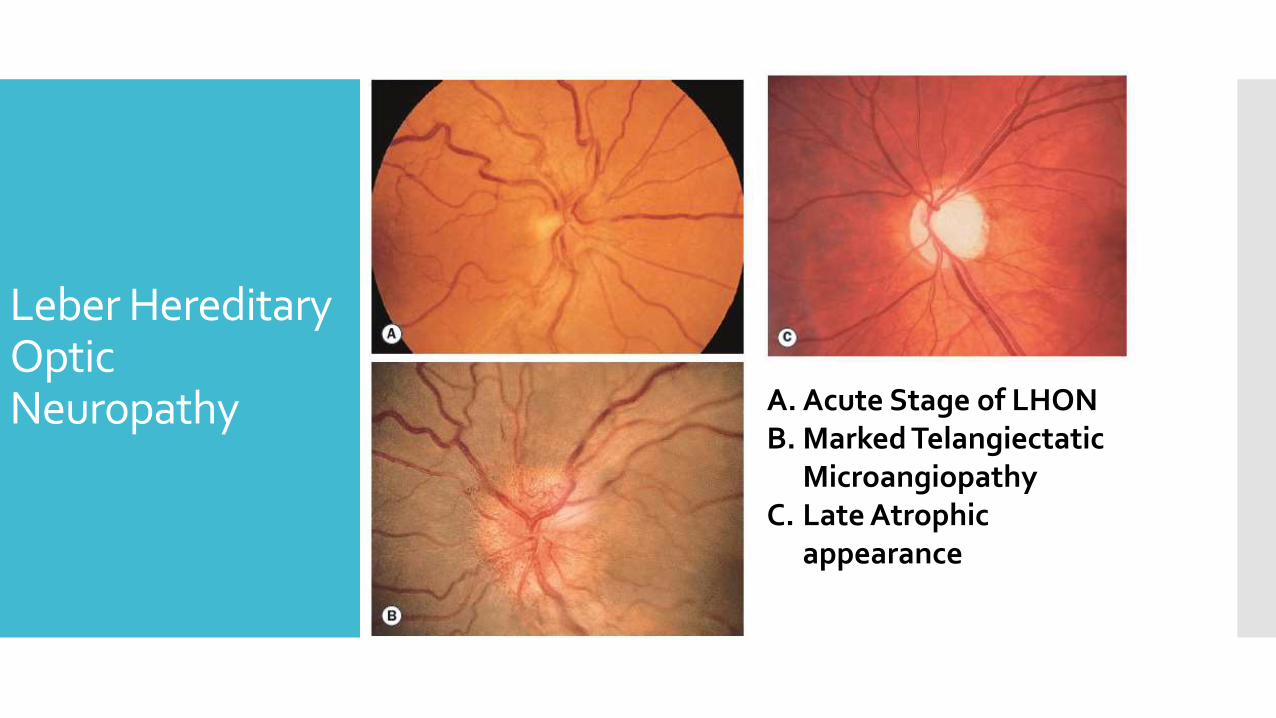
Leber HereditaryOptic Neuropathy A. Acute Stage of LHON
B. Marked Telangiectatic Microangiopathy
C. Late Atrophic appearance
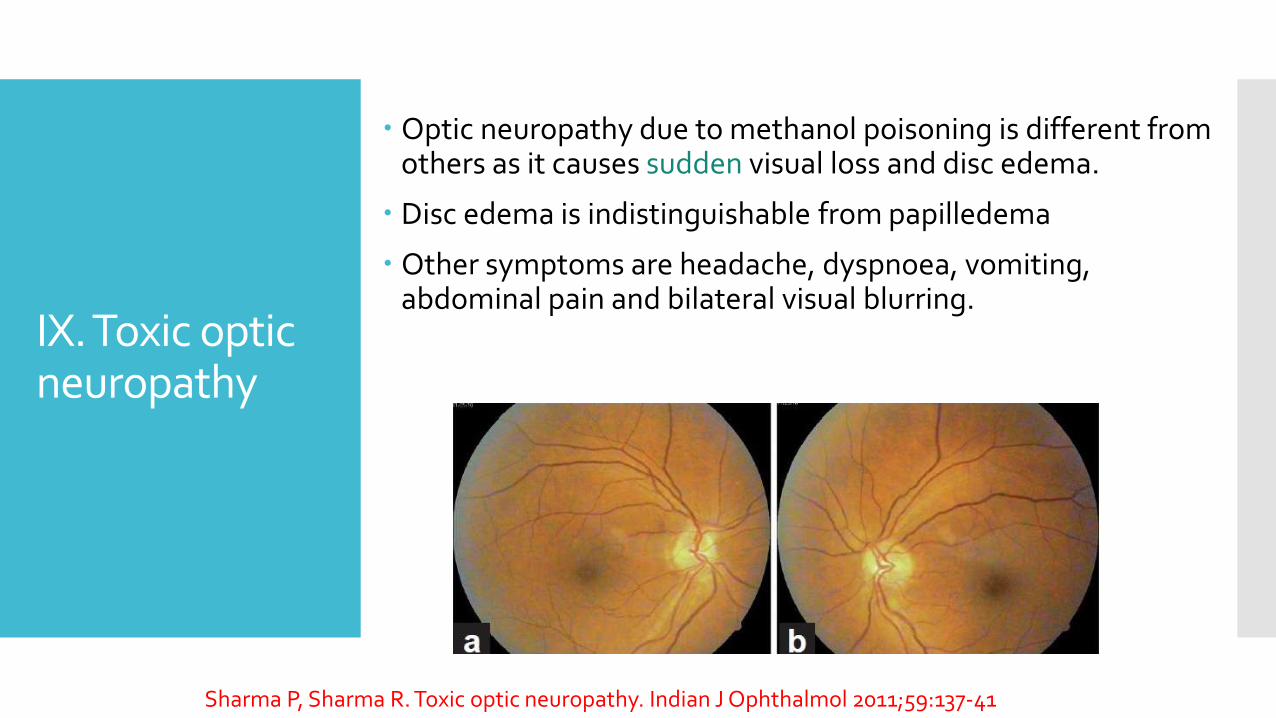
IX. Toxic optic neuropathy
Optic neuropathy due to methanol poisoning is different from others as it causes sudden visual loss and disc edema.
Disc edema is indistinguishable from papilledema
Other symptoms are headache, dyspnoea, vomiting, abdominal pain and bilateral visual blurring.
Sharma P, Sharma R. Toxic optic neuropathy. Indian J Ophthalmol 2011;59:137-41

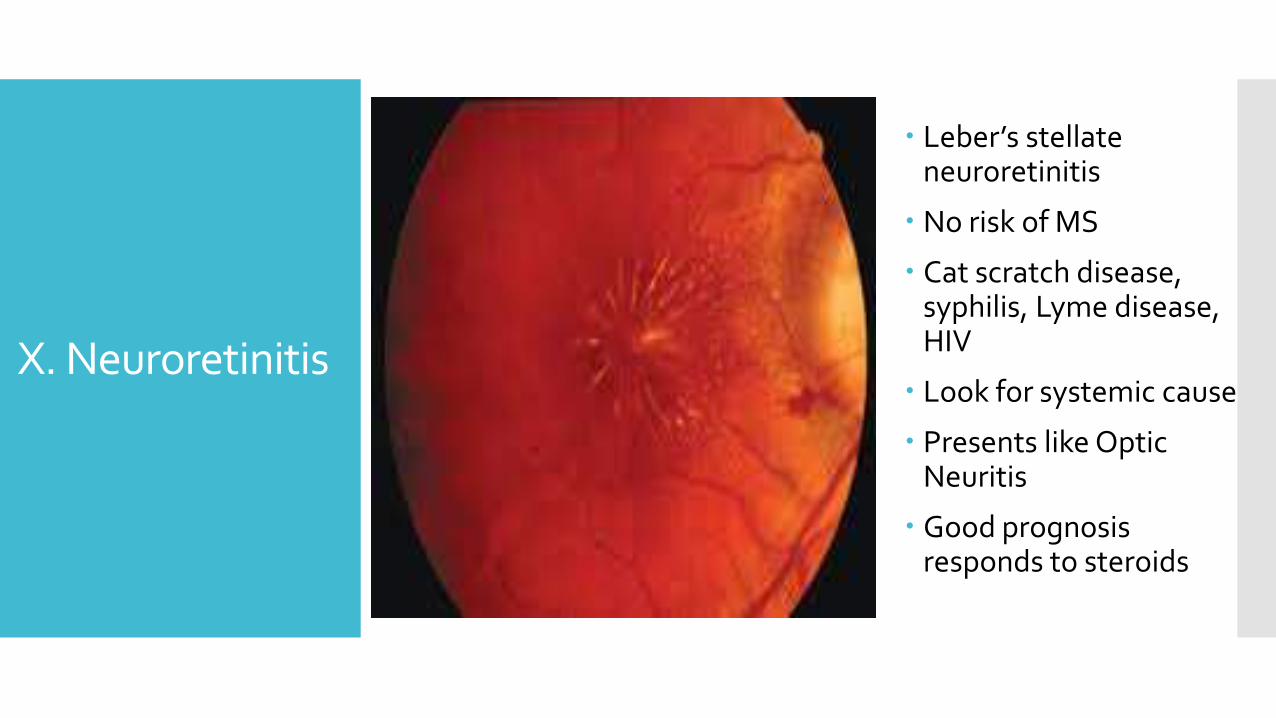
X. Neuroretinitis
Leber’s stellate neuroretinitis
No risk of MS
Cat scratch disease, syphilis, Lyme disease, HIV
Look for systemic cause
Presents like Optic Neuritis
Good prognosis responds to steroids
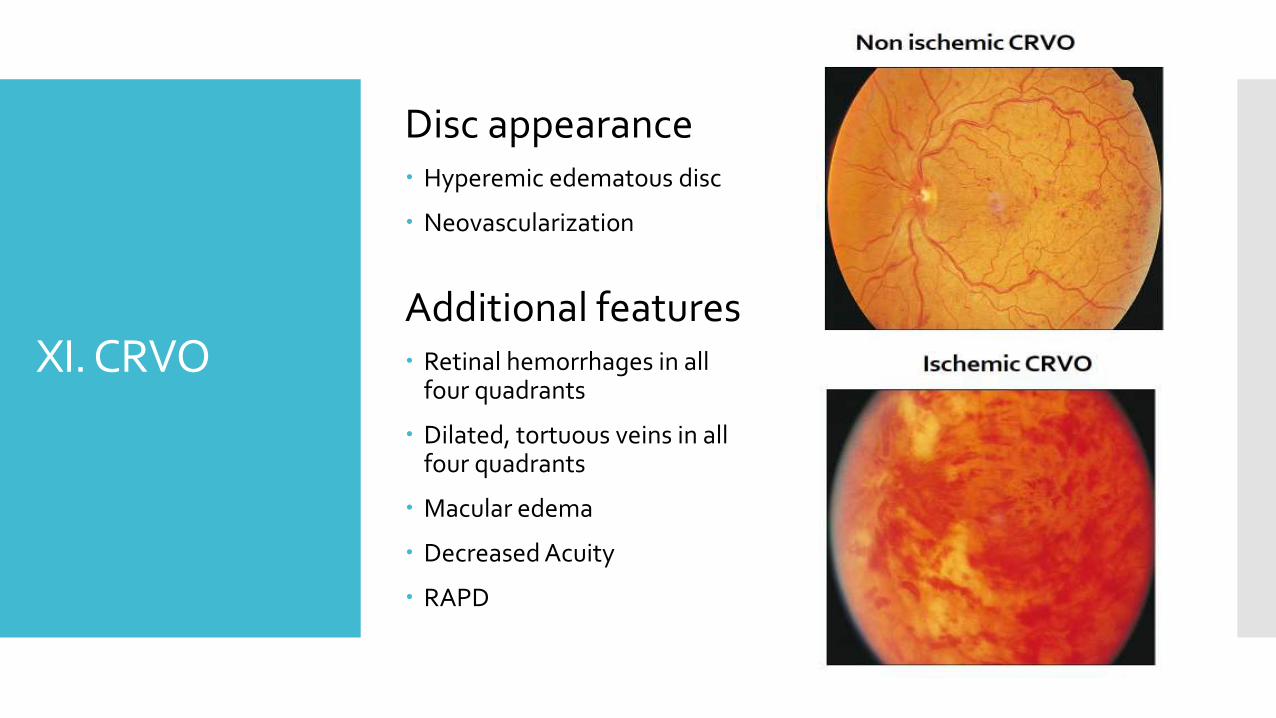
XI. CRVO
Disc appearance Hyperemic edematous disc
Neovascularization
Additional features Retinal hemorrhages in all
four quadrants
Dilated, tortuous veins in all four quadrants
Macular edema
Decreased Acuity
RAPD
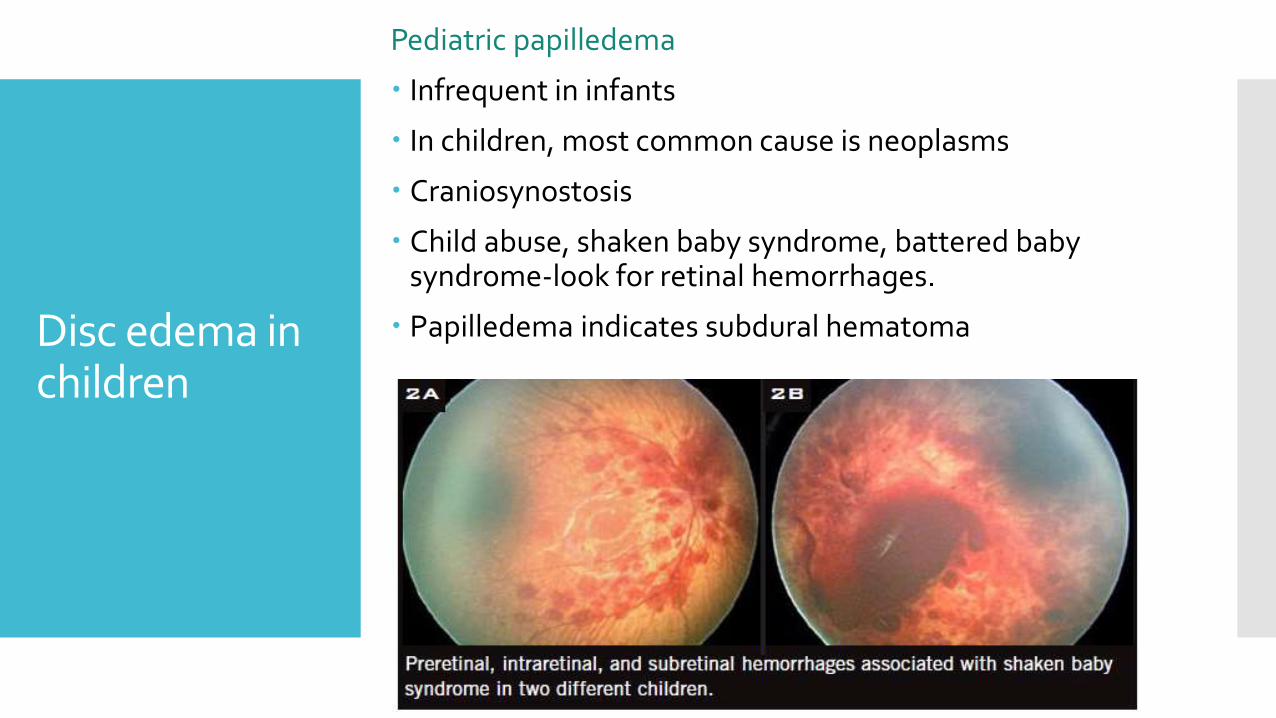
Disc edema in children
Pediatric papilledema
Infrequent in infants
In children, most common cause is neoplasms
Craniosynostosis
Child abuse, shaken baby syndrome, battered baby syndrome-look for retinal hemorrhages.
Papilledema indicates subdural hematoma
Pediatric optic neuritis
Usually bilateral, disc swelling more common
More aggressive treatment
Immune mediated Usually bilateral, post infectious
Acute demyelinating encephalopathy
Good prognosis
Idiopathic Demyelination
10-50% eventually develop MS
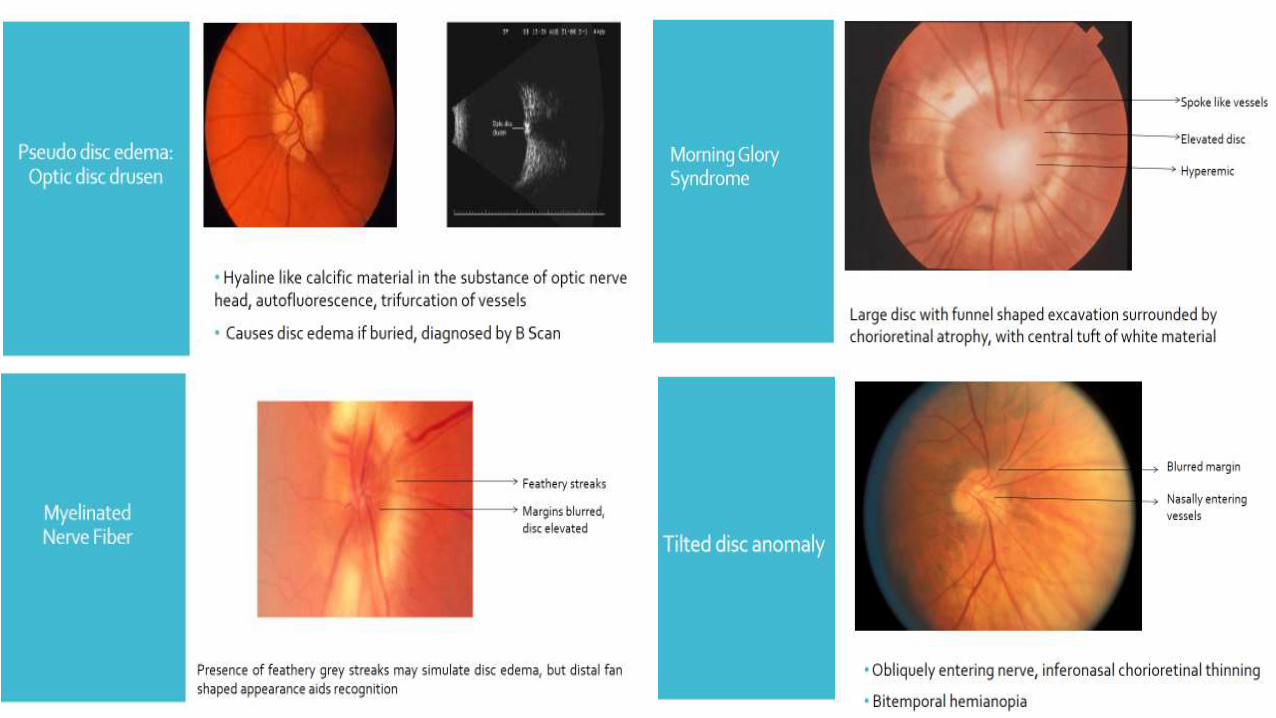
Is there true disc edema…?
Causes of pseudo disc edemaOptic nerve head drusen : disc elevation
Medullated nerve fibres : blurred margins
Morning glory syndrome: elevated disc
Tilted disc: blurred margins
Small hyperopic disc: hyperemic disc
Optic disc dysplasia
Bergmeister’s papilla
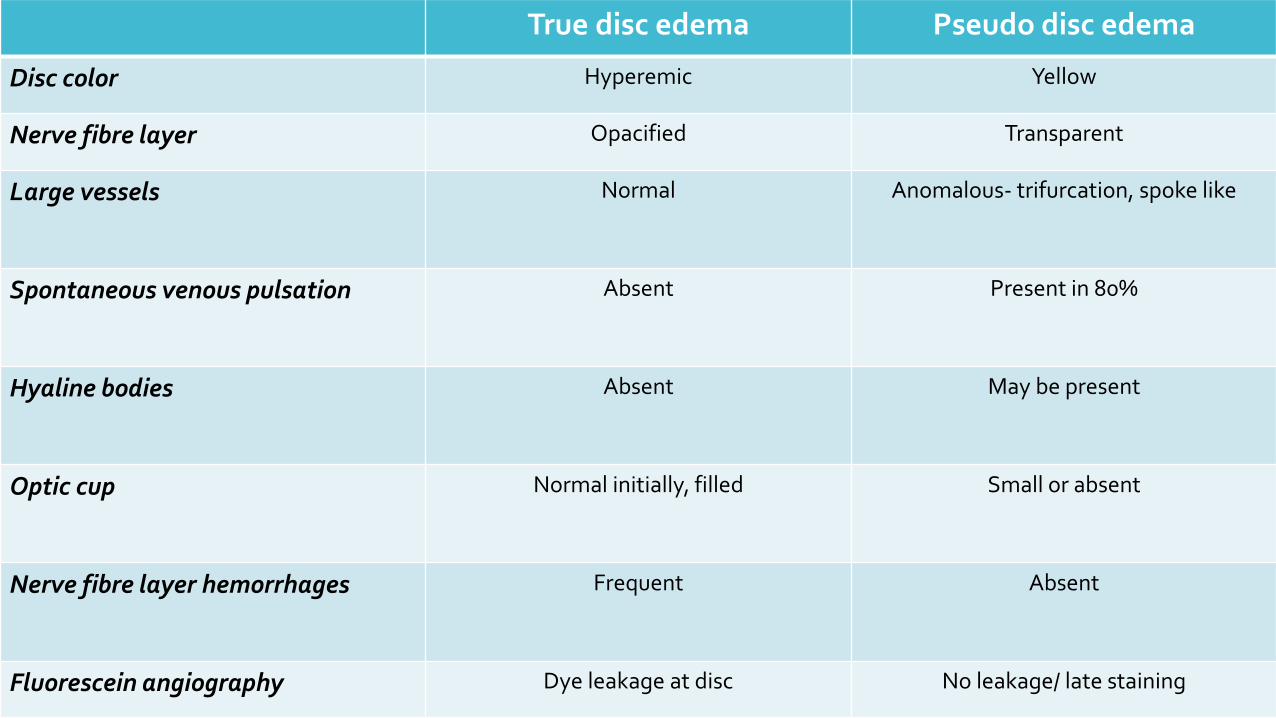
True disc edema Pseudo disc edema
Disc color Hyperemic Yellow
Nerve fibre layer Opacified Transparent
Large vessels Normal Anomalous- trifurcation, spoke like
Spontaneous venous pulsation Absent Present in 80%
Hyaline bodies Absent May be present
Optic cup Normal initially, filled Small or absent
Nerve fibre layer hemorrhages Frequent Absent
Fluorescein angiography Dye leakage at disc No leakage/ late staining
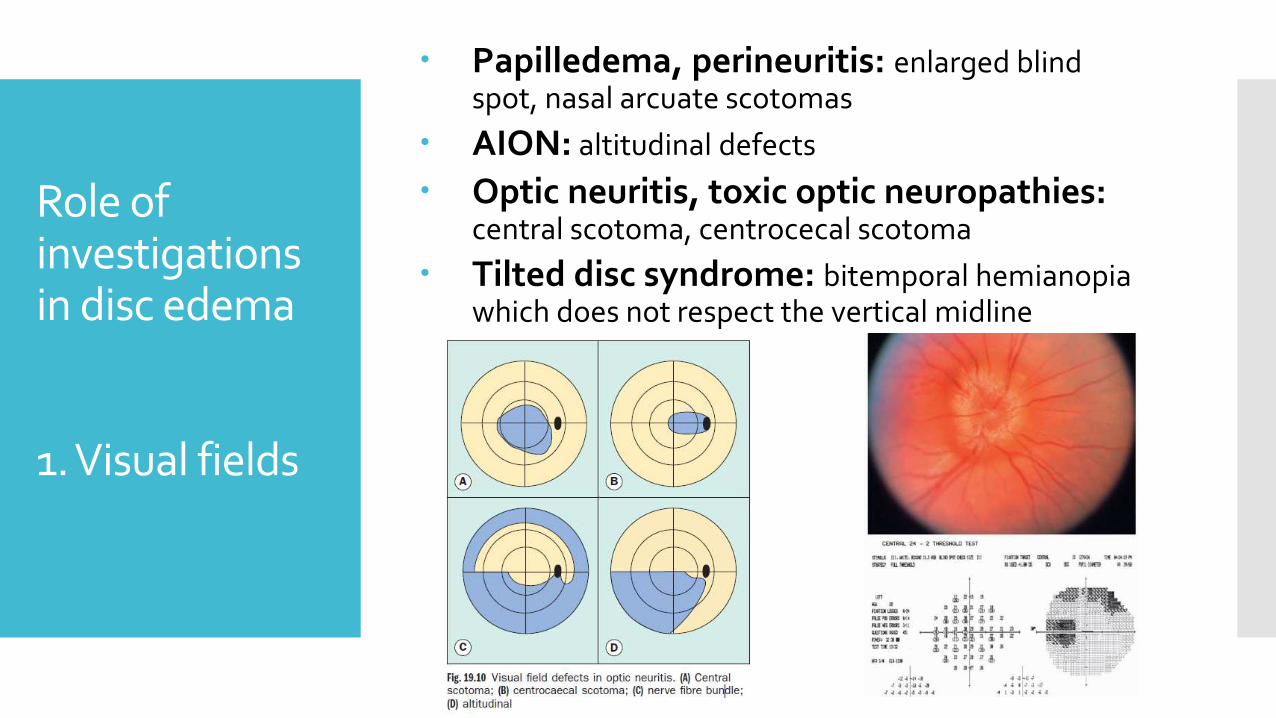
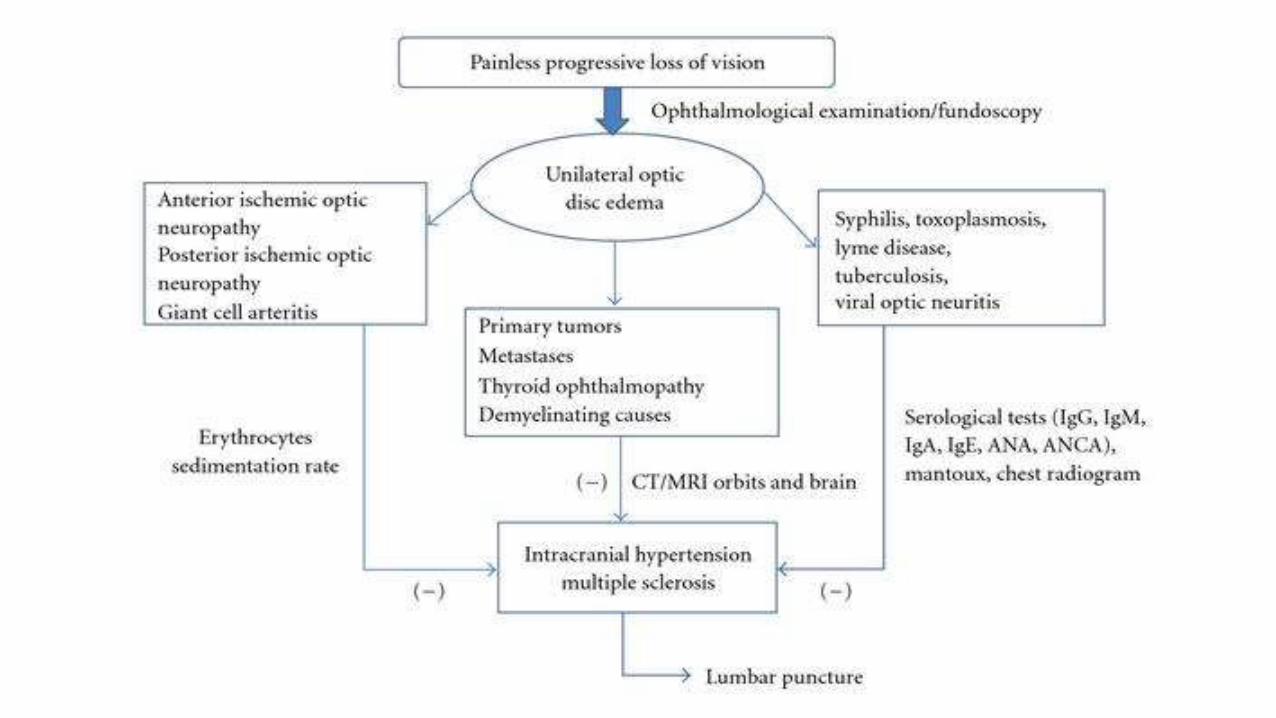
Role of investigations in disc edema
1. Visual fields
Papilledema, perineuritis: enlarged blind spot, nasal arcuate scotomas
AION: altitudinal defects
Optic neuritis, toxic optic neuropathies: central scotoma, centrocecal scotoma
Tilted disc syndrome: bitemporal hemianopia which does not respect the vertical midline
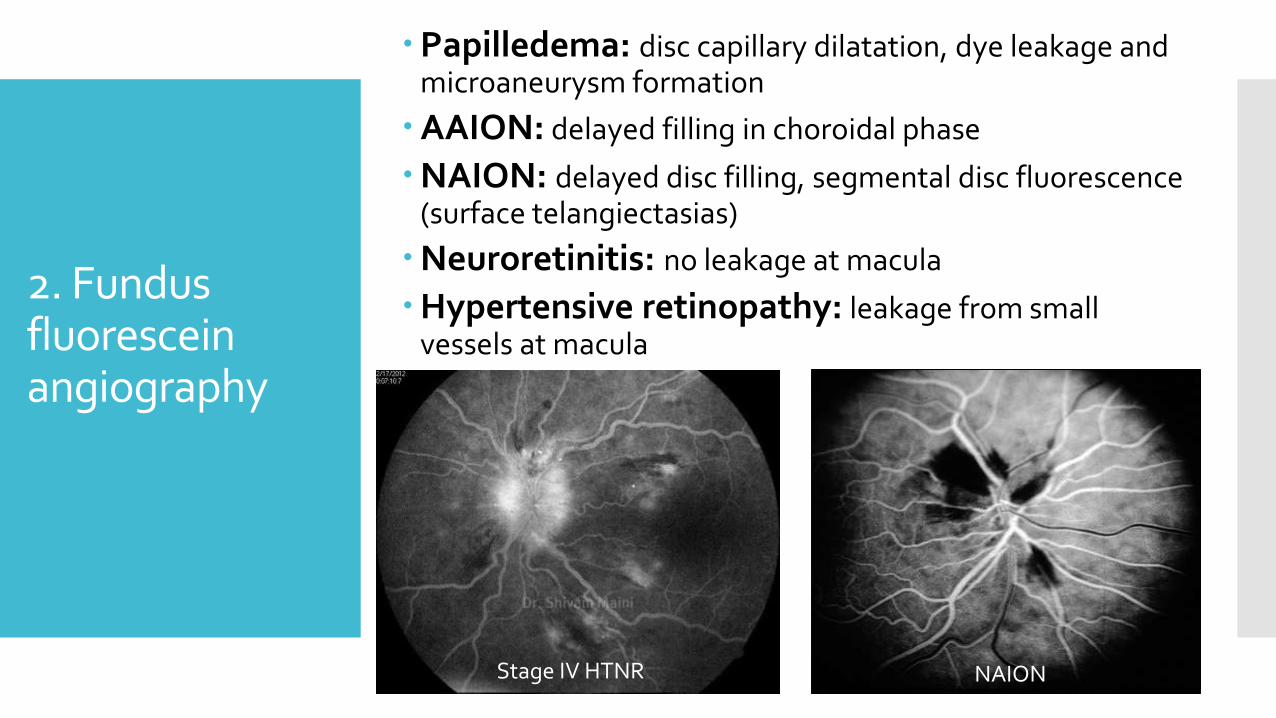
2. Fundus fluorescein angiography
Papilledema: disc capillary dilatation, dye leakage and microaneurysm formation
AAION: delayed filling in choroidal phase
NAION: delayed disc filling, segmental disc fluorescence (surface telangiectasias)
Neuroretinitis: no leakage at macula
Hypertensive retinopathy: leakage from small vessels at macula
NAIONStage IV HTNR
3. Neuroimaging
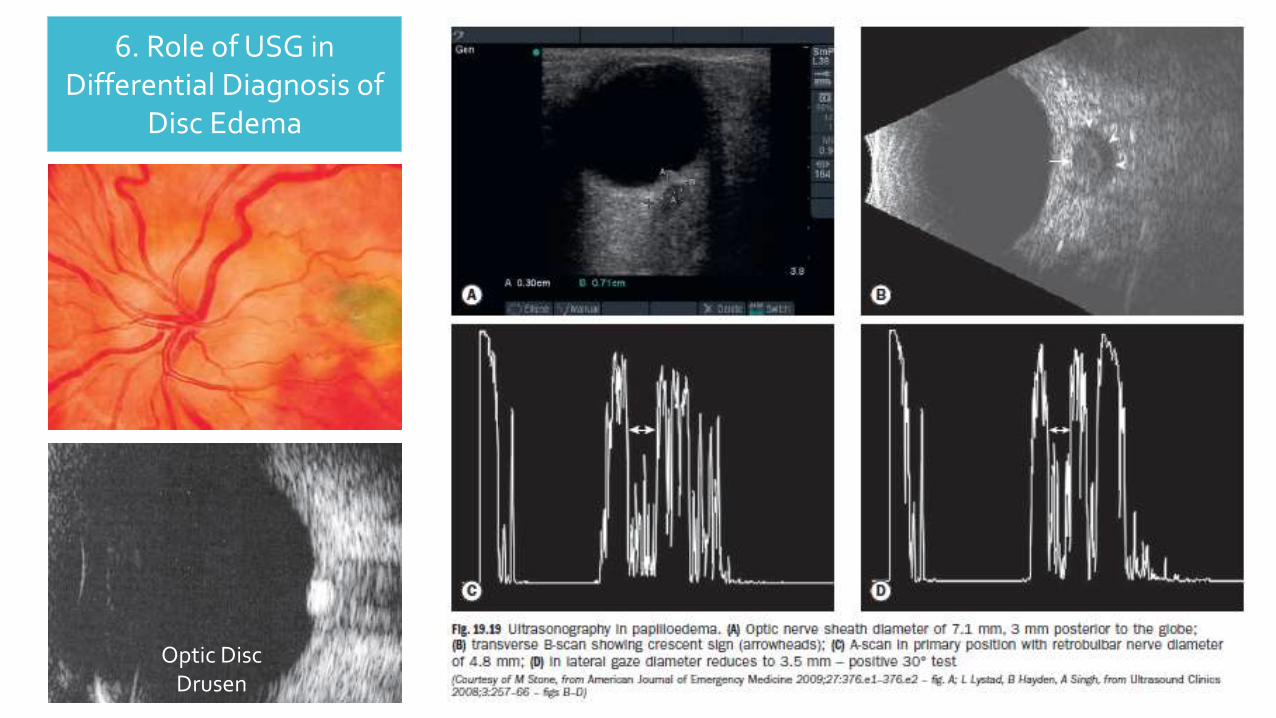
6. Role of USG in Differential Diagnosis of
Disc Edema
Optic Disc Drusen
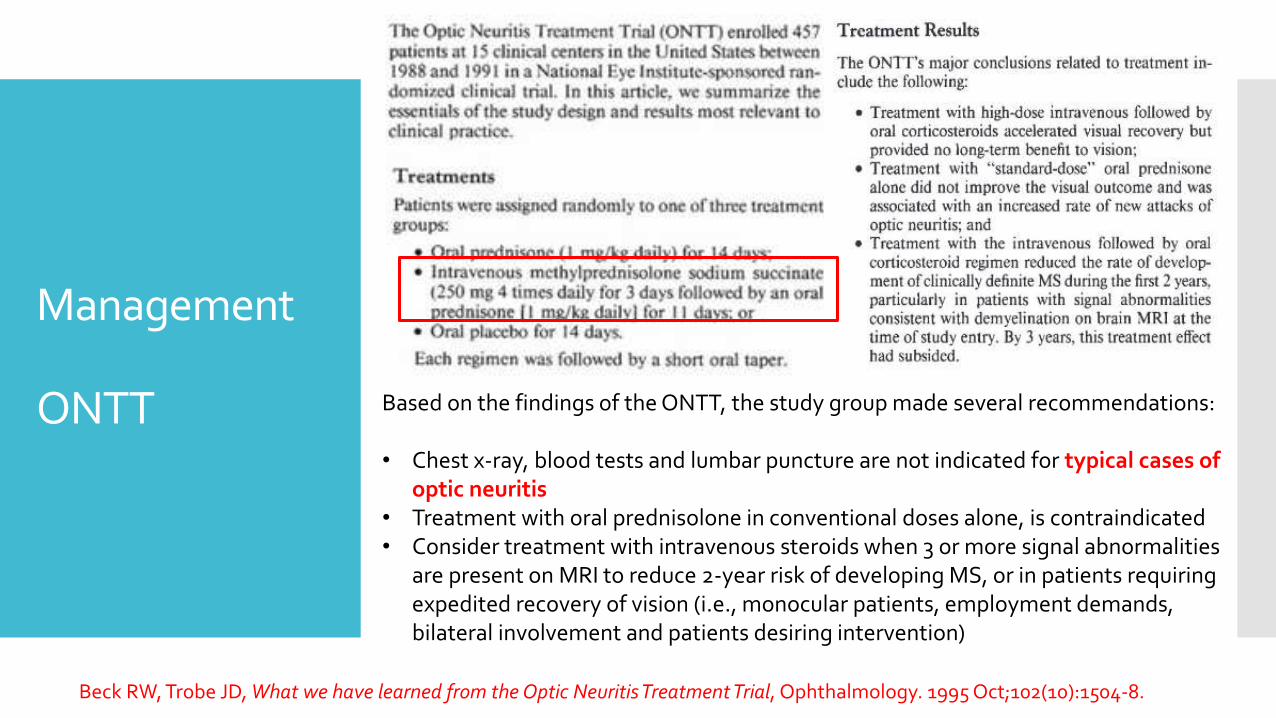
Management
ONTT Based on the findings of the ONTT, the study group made several recommendations:
• Chest x-ray, blood tests and lumbar puncture are not indicated for typical cases of optic neuritis
• Treatment with oral prednisolone in conventional doses alone, is contraindicated• Consider treatment with intravenous steroids when 3 or more signal abnormalities
are present on MRI to reduce 2-year risk of developing MS, or in patients requiring expedited recovery of vision (i.e., monocular patients, employment demands, bilateral involvement and patients desiring intervention)
Beck RW, Trobe JD, What we have learned from the Optic Neuritis Treatment Trial, Ophthalmology. 1995 Oct;102(10):1504-8.
Management1.AAION2.NAION
NAION Treatment:• There is no definitive treatment.• Optic nerve fenestration has not been shown to be ofbenefit.• Some authorities advocate short-term systemic steroidtreatment.• Any underlying systemic predispositions should be treated.• Although aspirin is effective in reducing systemic vascularevents and is frequently prescribed in patients with NAION,it does not appear to reduce the risk of involvement of thefellow eye.
AAION Treatment:• Absence of visual symptoms: oral prednisolone
1 mg/kg/day • CRP may play an important role in monitoring
disease activity• Treatment is aimed at preventing blindness of
the fellow eye• The second eye may still become involved in
25% despite early steroid administration. • Intravenous methylprednisolone, 500 mg to 1
g/day for 3 days followed by oral prednisolone 1–2 mg/kg/day. After 3 more days the oral dose is reduced to 50–60 mg (not less than 0.75 mg/kg) for 4 weeks or until symptom resolution and ESR/CRP normalization
• Antiplatelet therapy, e.g. aspirin 600 mg stat then 100 mg/day should be commenced as this has been .shown to reduce the risk of visual loss and stroke.
• Immunosuppressives such as methotrexate may be used as adjuncts or as steroid-sparing agents.
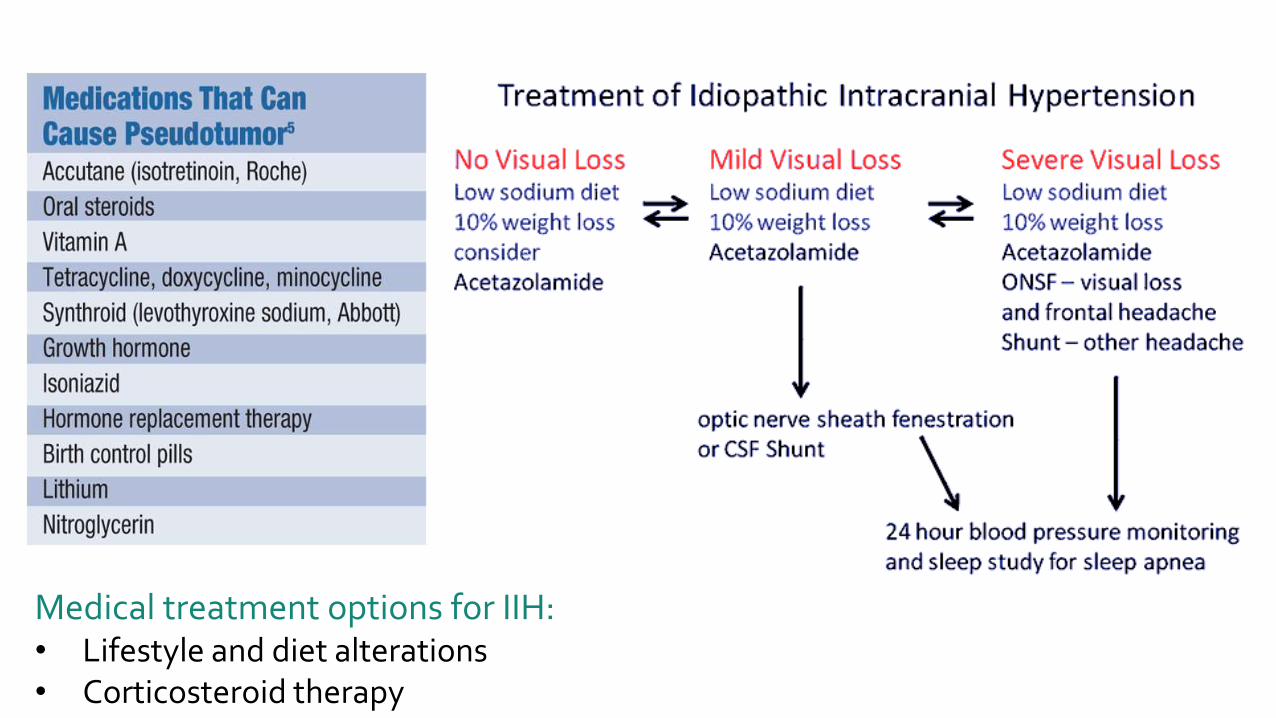
Medical treatment options for IIH:• Lifestyle and diet alterations• Corticosteroid therapy
Papilledema in PIH
General : Bed rest.
Control of BP.
Control of Edema : Diuretic, Hypertonic glucose.
Non responders : Termination of pregnancy.
Schiffman JS, Scherokman B, Tang RA, Dorotheo EU, Prieto P, Varon J, Evaluation and treatment of papilledema in pregnancy.,Compr Ophthalmol Update. 2006 Jul-Aug;7(4):187-202.
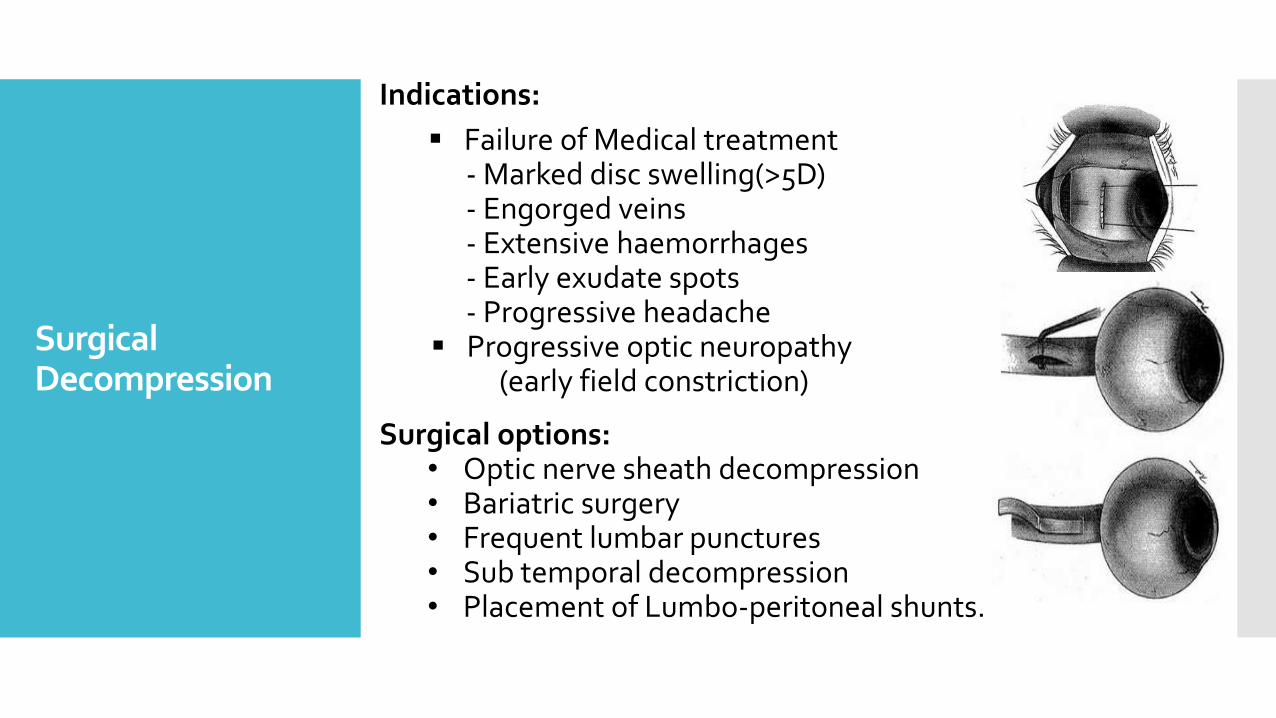
Surgical Decompression
Indications:
Failure of Medical treatment- Marked disc swelling(>5D)- Engorged veins- Extensive haemorrhages- Early exudate spots- Progressive headache
Progressive optic neuropathy (early field constriction)
Surgical options:• Optic nerve sheath decompression• Bariatric surgery• Frequent lumbar punctures • Sub temporal decompression• Placement of Lumbo-peritoneal shunts.
Recommended
![Uveitic macular edema: a stepladder treatment paradigm€¦ · of macular edema [1,3–4], this review will focus on uveitic macular edema specifically. Uveitic macular edema Macular](https://img.pdfslide.us/doc/110x75/5ed770e44d676a3f4a7efe51/uveitic-macular-edema-a-stepladder-treatment-paradigm-of-macular-edema-13a4.jpg)
















