-
7/30/2019 Dialysis in ESRD
1/59
Dialysis in ESRD
Velma Herwanto
-
7/30/2019 Dialysis in ESRD
2/59
ESRD Treatment Options
Hemodialysis
Peritoneal dialysis:
less efficient in soluteclearance
Transplantation
Outcomes aresimilar
preference andquality-of-lifeconsideration
-
7/30/2019 Dialysis in ESRD
3/59
Epidemiology
Mortality rate on dialysis in US: 1820%/year, 5-year survival
rate 3035%
Deaths are due mainly to cardiovascular
diseases (50%) and infections (15%)
Important predictors of death: age >, male,nonblack race, DM,
malnutrition, underlyingheart disease
-
7/30/2019 Dialysis in ESRD
4/59
Initiation on Maintenance Dialysis
Uremic symptoms: encephalopathy, neuropathy,pericarditis,
pleuritis
Persistent ECV expansion despite diuretic therapy
Bleeding diathesis
Hypertension poorly responsive to
antihypertensivemedications
Persistent metabolic disturbances that are refractory tomedical
therapy
Persistent nausea and vomiting
Evidence of malnutrition
CrCl or eGFR < 10 mL/min/ 1.73 m2
Do not delay the initiation of dialysisuntil one of this is
present!
-
7/30/2019 Dialysis in ESRD
5/59
Relative Indications to InitiateDialysis
Decreased attentivenessand cognitive tasking
Depression Persistent pruritus
Restless leg syndrome
-
7/30/2019 Dialysis in ESRD
6/59
hemodialysis
-
7/30/2019 Dialysis in ESRD
7/59
Hemodialysis
-
7/30/2019 Dialysis in ESRD
8/59
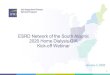
Scheme for Hemodialysis
Extracorporeal circuit indialysis machine
Dialysis access
Blood pump: 250-500 mL/min,negative hydrostatis pressure
ultrafiltration
Dialysis solution delivery system
Safety monitor
DIALYZER
Bundles of capillarytube: 1,5-2 m2
Cellulose vs.synthetic
Reprocessed and
reused
DIALYSATEK+ 0-4 mmol/LCa2+ 1.25 mmol/L: modification in
hypocalcemiaNa+ 140 mmol/L lower hypotension,cramping, nausea,
vomiting, fatigue, dizziness
Water 120 L: reverse osmosis
BLOOD DELIVERY
-
7/30/2019 Dialysis in ESRD
9/59
-
7/30/2019 Dialysis in ESRD
10/59
Hemodialysis Membrane
-
7/30/2019 Dialysis in ESRD
11/59
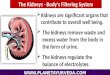
Chronic Dialysis Access
Fistula, graft, or tunneled catheter
AV fistula:
Brescia-Cimino fistula: radiocephalic/
brachiocephalic/brachiobasiclic arterialization of the vein
The highest long-term patency rate and lower complication
Synthetic graft: PTFE straight/ looped forearm,straight/ looped
upper arm
Smaller-caliber veins/ veins have been damaged
Complication: thrombosis, infection, steal, aneurysms,venous
hypertension, seromas, heart failure, and localbleeding
-
7/30/2019 Dialysis in ESRD
12/59
Chronic Dialysis Access
Dual-lumen tunneled catheter
Indication:
To allow maturation of fistulas/ grafts
CVC(require HD
-
7/30/2019 Dialysis in ESRD
13/59
Chronic Dialysis Access
-
7/30/2019 Dialysis in ESRD
14/59
Dialysis in Series
CVC: Entire systemic compartment is available forurea extraction
urea removal would be maximized
-
7/30/2019 Dialysis in ESRD
15/59
Dialysis in Parallel
AV access: reduce extraction of urea < theoreticalclearance
urea removal is limited (the capillaries where
this blood refills with urea)
- 60-70%
- 5-15%
-
7/30/2019 Dialysis in ESRD
16/59
Goals of Dialysis
Removing both low- and high-molecular-weight solutes
Heparinized blood300-500mL/min
Dialysate500-800mL/min
Efficiency of dialysis
blood and dialysate flowand dialyzer characteristics
Adequacy of dialysis:fractional removal of urea
nitrogen and derivationsthereof
-
7/30/2019 Dialysis in ESRD
17/59
-
7/30/2019 Dialysis in ESRD
18/59
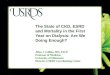
The effect of increasing dialyzer blood flow (Qb) ontotal body
urea clearance (Ktb) during HD
-
7/30/2019 Dialysis in ESRD
19/59
Movement of Waste Product
-
7/30/2019 Dialysis in ESRD
20/59
Dialytic Clearance of Solute
Diffusion Ultrafiltration
-
7/30/2019 Dialysis in ESRD
21/59
Convective Clearance
-
7/30/2019 Dialysis in ESRD
22/59
Membrane:Flux, Permeability, and Efficiency
Komass transfer coefficient; Asurface area
-
7/30/2019 Dialysis in ESRD
23/59
Dialysis Prescription (KDOQI 2006)
Urea removal normalized for a measure ofbody size
Kt/V
K = dialyzer urea clearance data dialysismembrane size, Qb,
Qd
t = duration of dialysis in minutes modifiable!
V = patient's urea space
-
7/30/2019 Dialysis in ESRD
24/59
Adequacy of HD (KDOQI 2006)
-
7/30/2019 Dialysis in ESRD
25/59
Delivering Adequate Dose ofDialysis
-
7/30/2019 Dialysis in ESRD
26/59
Urea Equilibration in HD
Degree of urea removal rateof urea equilibration between
IC and the ECSlow equilibrators lower BUN but a slower rate of
total
urea removal
-
7/30/2019 Dialysis in ESRD
27/59
Organ Reservoirs of Urea
Low ratio of blood flow to urea content sequester upto 80% of
the total body urea rebound and
dialysis efficiency
15-20% CO
-
7/30/2019 Dialysis in ESRD
28/59
HD Increase in... (KDOQI 2006)
Minimally adequate dose
, any body size
Smaller patients
BW 20% less or fluid is removed at the beginning)
-
7/30/2019 Dialysis in ESRD
35/59
Complication During HD
Muscle cramp:
Excessively aggressive volume removal (>dry weight)
Use of low-sodiumcontaining dialysate
Management:
volume removal
UF profiling
Higher concentrations of sodium in thedialysate or sodium
modeling
-
7/30/2019 Dialysis in ESRD
36/59
Sodium Modelling
Intracellularmovement of water
+UF of water hypotension
-
7/30/2019 Dialysis in ESRD
37/59
Complication During HD
Anaphylactoid reaction to dialyzer
Type A: IgE-mediated hypersensitivityreaction to ethylene oxide
within the
first few minutes steroids orepinephrine
Type B: nonspecific chest and back pain,
from complement activation andcytokine release several
minutes,resolve over time
-
7/30/2019 Dialysis in ESRD
38/59
Dialysis Disequilibrium Syndrome
Central nervous system disorder in dialysis patients
Pathophysiology: cerebral edema
Reverse osmotic shift
Fall in cerebral intracellular pH
At risk: new HD patients (with >> BUN), severe
metabolicacidosis, older age, pediatric, presence of CNS
disease
Headache, nausea, disorientation, restlessness, blurred
vision,asterixis, muscle cramps, anorexia, dizziness
More severe: confusion, seizures, coma, death
-
7/30/2019 Dialysis in ESRD
39/59
DDS: Treatment and Prevention
Qb, consider stop the dialysis session
Hypertonic mannitol or 23% saline
Prevention: slow urea removal
Initial HD: 2 hours, Qb 150-250 mL/min, small surfacearea
dialyzer, concurrent blood and dialysate flow 3-4days 50 mL/min (up
to 300-400 mL/min),duration 30 minute
Marked fluid overload: UF followed by a short period ofHD
PD
Prophylactic phenytoin and/ or mannitol
-
7/30/2019 Dialysis in ESRD
40/59
Peritoneal Dialysis
-
7/30/2019 Dialysis in ESRD
41/59
Normal Anatomy
Peritoneal contains 100 ml fluid
Adult can tolerate > 2 L fluid withoutpain or alteration to
the respiratory
function : peritoneal cavity is closed
: peritoneal cavity is continuous
with the Fallopian tubes
PD fluidbecome blood-stained during amenstrual period
-
7/30/2019 Dialysis in ESRD
42/59
Principles of Peritoneal Dialysis
Jeremy Levy et al, Oxford Handbook of Dialysis, 2003
-
7/30/2019 Dialysis in ESRD
43/59
Solute and Water Transport Mechanism in PD
Diffusion Solute(e.g. Ur,Cr, K)
Via mid-size pores Most important
High concentration (blood) low concentration(dialysate)
to the concentration gradient
Best for clearance of small molecules
Convection Solute(e.g.protein,Na)
In response to a positive transmembrane pressure
Less dependent on molecular size
Ultrafiltratio
n
Water Low osmotic concentration (blood) high osmotic
concentration (dialysate), via aquaporin-1 Highest at the
beginning, ceases when osmolarity hasdecreased to equal serum
osmolarity
Reabsorbtion of water if dialysate is allowed to dwellbeyond the
time past when osmotic equilibrium isreached
-
7/30/2019 Dialysis in ESRD
44/59
Access to Peritoneal Cavity
Peritoneal catheter: silicon rubberwith numerous side holes at
thedistal end
Dacron cuffs: promote fibroblastproliferation, granulation,
andinvasion of the cuff
Seal from bacteria from the skin surface
Prevents external leakage of fluid
-
7/30/2019 Dialysis in ESRD
45/59
Types of PD Catheter
-
7/30/2019 Dialysis in ESRD
46/59
-
7/30/2019 Dialysis in ESRD
47/59
PD Solutions
Ideal osmotic agents:
Metabolized easily with non-toxic degradation products
Poorly absorbed
Inert and non-toxic to the peritoneal membrane Inexpensive
Effective osmotic agent at low concentration
No metabolic consequences of absorption
Must be of nutritional value
Not difficult to manufacture
Should not inhibit peritoneal defenses
-
7/30/2019 Dialysis in ESRD
48/59
PD Solutions
High molecular weight Glucose polymer (icodextran 7.5%):
Polypeptides (5%): Glucose-containing (dextrose monohydrate 1.5,
2.5, 4.25%): Amino acid (1.1%): Glycerol:Low molecular weight
Glucose polymer (icodextran 7.5%): Polypeptides (5%):
Glucose-containing (dextrose monohydrate 1.5, 2.5, 4.25%): Amino
acid (1.1%): Glycerol:
-
7/30/2019 Dialysis in ESRD
49/59
PD Solutions
Solutions: 1.5 to 6.0 L
Lactate is the preferred buffer, other:acetate, bicarbonate
Electrolyte: Na, Ca, Mg, K
Additives: heparin, antibiotics, insulin
-
7/30/2019 Dialysis in ESRD
50/59
CAPD3-5x/ day
CCPD
DAPD
NIPD
-
7/30/2019 Dialysis in ESRD
51/59
Adequacy of PD: K/ DOQI 2006
T Peritoneal
-
7/30/2019 Dialysis in ESRD
52/59
Calculation of Solute Clearance
, 70 kg on CAPD has a drain volumeof 10.5 L/day, and D/P urea of
0.95
Kt = 10.5 x 0.95 = 10 L
The urea volume of distribution (V) =42 L (60% of lean body
weight inmen, 55% in women)
Daily Kt/Vurea = 10 42 = 0.24
Weekly Kt/Vurea = 0.24 x 7 = 1.68
-
7/30/2019 Dialysis in ESRD
53/59
Adequacy of PD
Efficiency of solute clearance volume of dialysate (> volumes
> solute clearance), physical activity
Peritoneal equilibrium test: measures the transfer rates
ofcreatinine and glucose across the peritoneal membrane
Low transporter: fewer exchanges
Lowaverage transporter
Highaverage transporter
High transporters: absorb > glucose, lose efficiency of UF
with longdaytime dwells, lose > albumin require more frequent,
shorter dwell
time exchanges
PET: 3-4 weeks after catheter insertion and on complication
U i T t T t
-
7/30/2019 Dialysis in ESRD
54/59
Using Transport Type toSelect PD Regimen
High
-
7/30/2019 Dialysis in ESRD
55/59
Indication to Repeat PeritonealMembrane Transport Testing
KDOQI 2006
Unexplained volume overload
Decreasing drain volume on: overnight dwell (CAPD)
or daytime dwell (APD)Increasing clinical need for hypertonic
dialysatedwells to maintain DV
Worsening of HTN
Change in measured peritoneal solute removal(Kt/Vurea)
Unexplained signs/ symptoms of uremia
PD P i ti T t d
-
7/30/2019 Dialysis in ESRD
56/59
PD Prescription Target andMeasurement (KDOQI 2006)
If a patient is not thriving + no otheridentifiable cause,
consider to
increase dialysis dose.
Patient with minimal RKF
continuous 24 h/day of PD dwell tomaximize middle molecule
clearance
-
7/30/2019 Dialysis in ESRD
57/59
Fluid Balance
The 2006 NKF-KDOQI guidelines: oneshould achieve euvolemia
andoptimal BP control
Maintenance of euvolemia: PD drainvolume, RKF, blood
pressure
The 2005 European Best PracticesGuidelines: in anuric
patients,minimum UF target is 1.0 L/day
-
7/30/2019 Dialysis in ESRD
58/59
Complications During PD
Peritonitis: peritoneal fluid leukocytes 100/mm3 (at least50%
are PMN) pain, cloudy dialysate, fever
Gram-positive cocci, gram-negative rod, fungal,
mycobacterial
Intraperitoneal/ oral antibiotics
Due to hydrophilic gram negative rods (e.g.,Pseudomonas
sp.) oryeast: require catheter removal
Catheter-associated nonperitonitis infections
Weight gain
Hypoproteinemia: dietary protein intake
Hyperglycemia
Hypertriglyceridemia
Residual uremia (esp. in patients with no residual
kidneyfunction)
-
7/30/2019 Dialysis in ESRD
59/59
Terima Kasih