Brook J Hill, HMS/HST IVGillian Lieberman, MD
Diagnostic Imaging of Intracranial Tumors in Adults
Brook J Hill, Harvard Medical School, Year IVGillian Lieberman, MD, Beth Israel Deaconess
Hospital and Harvard Medical School
July 2003

2
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Patient P.W.
• P.W. is a 63 year-old female who complains of 1 month of progressive headache and confusion. She also reports constantly misplacing objects, increasing forgetfulness, feeling very tired, and “leaning to the left” while walking.
• Physical exam: Slight left facial droop; LEU finger-to-nose and rapid alternating movements abnormal; unsteady tandem gait with lean to left. Otherwise normal.
• Head CT at an OSH revealed a right frontal mass.
3
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Indications for Imaging
• Signs and/or symptoms suggestive of intracranial neoplasm:– PROGRESSIVE neurologic dysfunction– New onset seizures (or change in character)– Signs/symptoms of elevated intracranial
pressure (ICP)– Known systemic tumor with possible
intracranial metastasis

4
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Focal vs. General Signs/Sx
• Focal:– Focal seizures (25-50%)– Weakness– Sensory abnormalities– Gait changes– Speech disturbances– Visual defects
• General:– Papilledema (59%) – Generalized convulsions
(25-50%) – Headache (50%) – Mental changes– Nausea and vomiting– Signs/Sx of herniation
Focal signs/sx are caused by localized brain damage, while general signs/sx are caused by elevated ICP.

5
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Mental Changes Associated with Intracranial Tumors
• Psychomotor retardation– Impersistence in routine tasks– Inertia– Reduction in the range of mental
activity – Reduced initiative and spontaneity– Blunted affect
• Sleep disturbances– Insomnia– Early rising– Excessive daytime sleepiness
• Cognitive disturbances– Forgetfulness– Lack of concentration
– Language disorders– Concreteness– Faulty insight– Frank dementia
• Social disturbances– Disheveled appearance– Inappropriate behavior– Loss of inhibitions– Indifference to social practices
• "Psychological" symptoms– Depression– Hypomania– Euphoria– Emotional lability

6
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Menu of Tests Available
• MRI• CT• SPECT• PET• X-Ray

7
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI
• First-line diagnostic test for imaging of suspected intracranial tumors
• Multiplanar, high resolution, high contrast
• Standard protocols: T1, T2, proton density (PD)
• Advanced protocols: FLAIR, DSC, others
Sagittal
Axial
Coronal
Images from PACS,

8
Brook J Hill, HMS/HST IVGillian Lieberman, MD
CT• Generally not recommended
to diagnose or follow intracranial tumors
• Single plane (axial)• Lower resolution than MRI• Less soft-tissue contrast• However, CT is the first-line
test for suspected intracranial hemorrhage
BIDMC, PACS

9
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI vs. CT
• Greater soft tissue contrast (e.g. white vs. grey matter)
• More sensitive to soft tissue abnormalities (i.e. can detect small differences in water content)
• Smaller amount of contrast needed• Better tumor characterization (e.g. subacute vs.
chronic hematomas, vascular lesions, cystic contents)
• Multiplanar imaging• Lack of beam hardening artifact near bony
structures • No ionizing radiation• Compatible with orthopedic implants, vascular
clips excluding aneurysm clips, dental fillings, and ventricular shunts
• Superior visualization of bony/calcific structures
• More rapid image acquisition• Easier monitoring of acutely ill
patients• Compatible with pacemakers,
ferromagnetic aneurysm clips, intraocular foreign bodies, and virtually all prostheses
• Better tolerated by claustrophobic patients
Benefits of MRI: Benefits of CT:

10
Brook J Hill, HMS/HST IVGillian Lieberman, MD
SPECT• Single Photon Emission Computed Tomography• A multislice nuclear medicine study - “Brain scan”• 99mTc-hexamethyl-propylenamine-oxime (99mTc-HMPAO) • Provides functional information about regional cerebral blood
flow (rCBF), which helps: – determine tumor burden both before and after surgery– distinguish between viable tumor, necrosis, and edema after
surgical resection• Also used in dementia, cerebrovascular disease, epilepsy, encephalitis,
and trauma• Readily available, relatively inexpensive, and well-tolerated• Limitations:
– Inherently poorer resolution than PET, CT, and MRI – Absolute quantification of blood flow is not possible– Involves ionizing radiation
www.bae.ncsu.edu

11
Brook J Hill, HMS/HST IVGillian Lieberman, MD
PET• Positron Emission Tomography• Also a multislice nuclear medicine study• Blood flow, oxygen uptake, and glucose consumption• Provides functional information about the metabolic profile of
tumors, enabling the radiologist to:– estimate aggressiveness of tumors (correlates with metabolic
activity) – distinguish viable recurrent tumor from radiation necrosis
after surgical resection• Better spatial resolution than SPECT• Limitations:
– Poor spatial resolution compared to CT and MRI – Expensive and therefore not universally available– Involves ionizing radiation
www.epub.org.br

12
Brook J Hill, HMS/HST IVGillian Lieberman, MD
X-Ray
• “Historical” test for intracranial tumors, but common findings still important:– Erosion of dorsum sellae (elevated ICP)– “J-shaped” sella (chronic hydrocephalus)– Tumor calcification– Cranial vault erosion– Enlargement of middle meningeal groove (e.g.
meningioma)
13
Brook J Hill, HMS/HST IVGillian Lieberman, MD
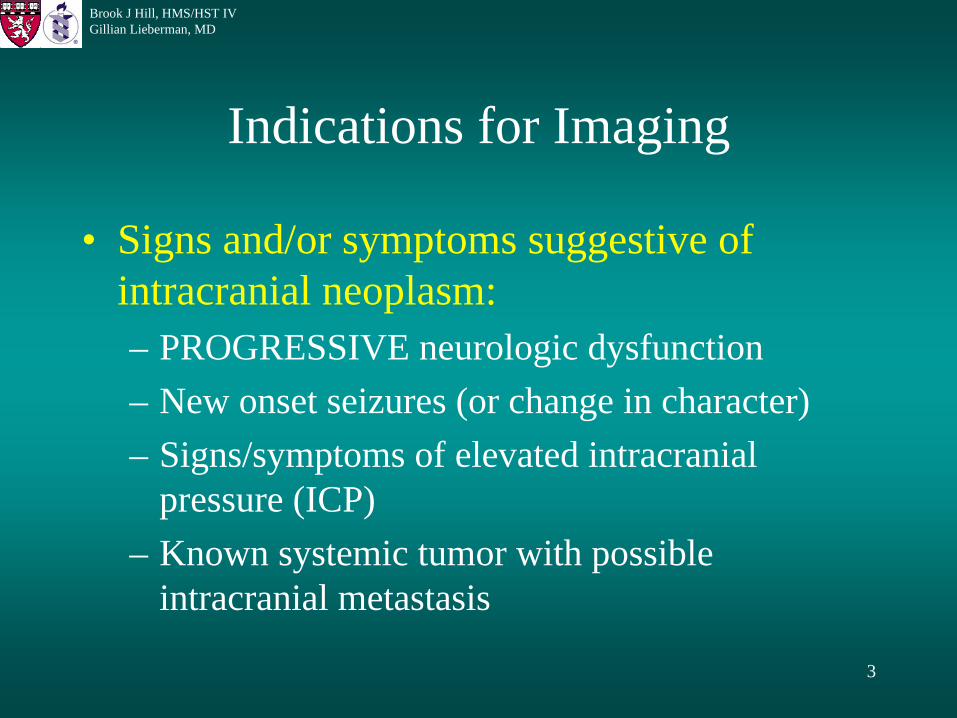
X-Ray: Erosion of Dorsum SellaeNormal Sella: Elevated ICP:
• Erosion into cancellous bone (white arrow) underlying sella
• Erosion of lamina dura (ld) of dorsum sellae (ds), often the earliest bony change with elevated ICP
Images adapted from Grainger & Allison's Diagnostic Radiology: A Textbook of Medical Imaging, 4th Ed., Copyright © 2001 Churchill Livingstone, Inc.
• Sella can reossify and remodel upon relief of elevated ICP

14
Brook J Hill, HMS/HST IVGillian Lieberman, MD
X-Ray: “J-Shaped” SellaNormal Sella: Chronic Hydrocephalus:
Images adapted from Grainger & Allison's Diagnostic Radiology: A Textbook of Medical Imaging, 4th Ed., Copyright © 2001 Churchill Livingstone, Inc.
• Truncated dorsum sellae (ds)
• Large anterior clinoid process (acp)
• Deep sulcus chiasmaticus (sc)
• J-shape caused by direct pressure form dilated third ventricle

15
Brook J Hill, HMS/HST IVGillian Lieberman, MD
X-Ray: Tumor Calcification
http://www.pathology.vcu.edu
• Tumors that often calcify:• Craniopharyngioma (40-80%)• Meningioma (15%)• Glioma (10-15%) • Lipoma
• Physiologic calcification:• Pineal (50%)• Choroid (50%)• Dura • Arachnoid granulations• Basal ganglia• Corotid arteries

16
Brook J Hill, HMS/HST IVGillian Lieberman, MD
X-Ray: Tumor Calcification• Expansile radiolucent mass in sella tursica (open arrows)
• Dystrophic soft-tissue calcification
• Tissue diagnosis = Craniopharyngioma
• Erosion of dorsum sellae
http://www.pathology.vcu.edu
17
Brook J Hill, HMS/HST IVGillian Lieberman, MD
X-Ray: Cranial Vault Erosion
• PATHOLOGIC TUMORS:– Epidermoid cyst, hamangioma, eosinic granuloma, multiple myeloma– Metastases (virtually always LYTIC in the skull, even if sclerotic
elsewhere in the body)• BENIGN CHANGES:
– Venous lakes, enlarged parietal foramina, parietal thinning • OTHERS:
– Pagets, osteomyelitis, leptomeningeal cyst
Meningioma, however, typically causes increased bone density due to trophic effects on the inner table.

18
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

19
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

20
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

21
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

22
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

23
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

24
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC
25
Brook J Hill, HMS/HST IVGillian Lieberman, MD
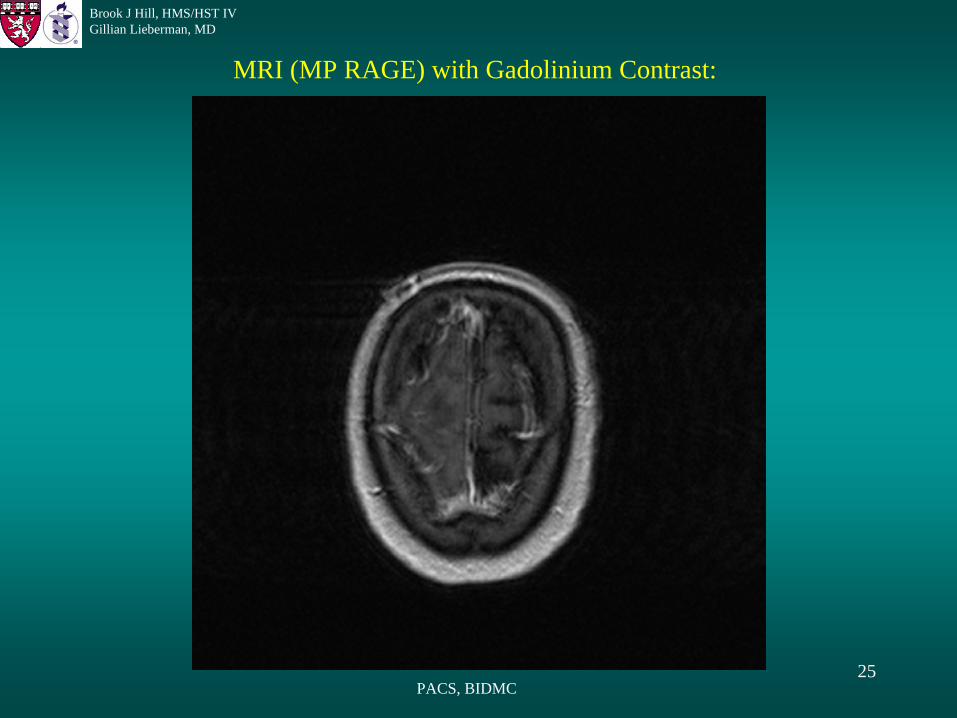
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

26
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

27
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

28
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

29
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

30
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

31
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

32
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

33
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

34
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

35
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

36
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC
37
Brook J Hill, HMS/HST IVGillian Lieberman, MD
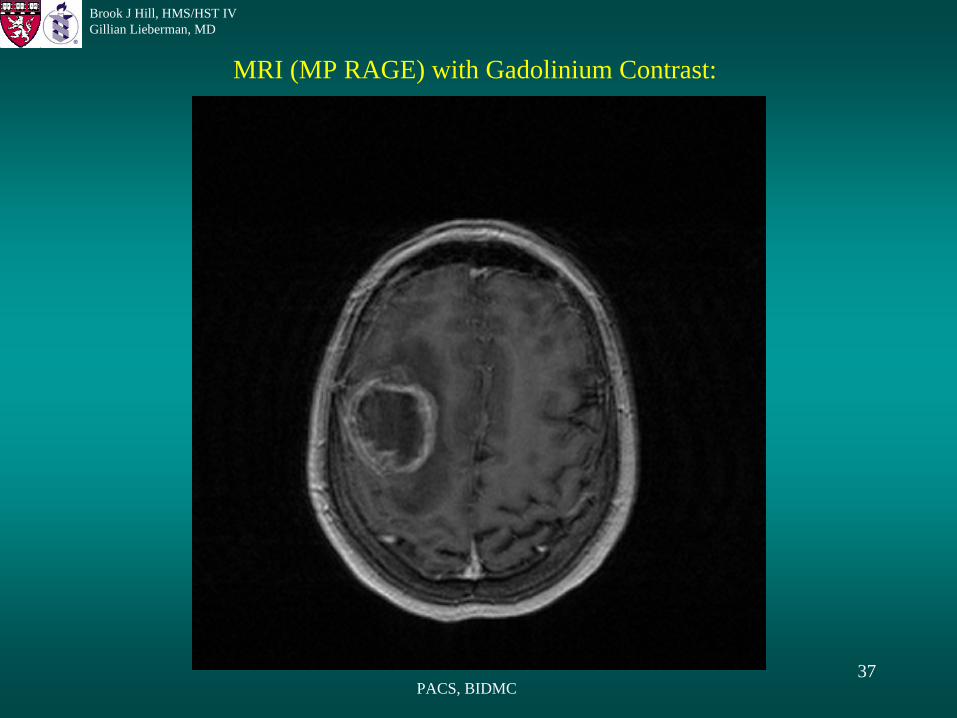
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

38
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

39
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

40
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

41
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

42
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

43
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

44
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

45
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

46
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

47
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

48
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

49
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI (MP RAGE) with Gadolinium Contrast:
PACS, BIDMC

50
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Describing the Lesion
• Size and Shape• Location• Number• Density• Enhancement• Edema• Mass Effect

51
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Describing the Lesion: Location
• Intra-axial vs. Extra-axial:– Intra-axial = within the brain parenchyma– Extra-axial = outside the brain parenchyma– Step #1 in differentiating intracranial tumors– Not always possible to differentiate
• Supratentorial vs. Infratentorial:– Supratentorial = above the tentorium cerebelli– Infratentorial = below the tentorium cerebelli

52
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Describing the Lesion: Density
• CT: – Compare attenuation of lesion with
that of surrounding normal parenchyma (25-40 HU)
– Higher attenuation = cells (30-60 HU), hemorrhage (85 HU if acute), calcification
– Lower attenuation = fluid (0 HU if CSF), fat (-100 HU)
• MRI:– Compare signal intensity on
T1, T2 etc. with normal parenchyma
– T1:• High signal = adipose,
proteinacous fluid, contrast, low flow
• Low signal = bone, calcifications, fluid, air, high flow
– T2:• High signal = fluid,
hemorrhage, low flow• Low signal = bone,
calcifications, air, high flow
Because tumor often is the same attenuation as normal parenchyma, many tumors are missed on CT.

53
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Describing the Lesion: Enhancement
• Compare images taken before contrast administration with those taken after contrast administration
• “Nonenhancing, Homogenous, Ring, Heterogenous, Serpentine”• Normal blood-brain barrier (BBB) does NOT allow passage of iodine
or gadolinium contrast• BBB breakdown can be seen in infarction, infection, abscess,
neoplasia, and trauma• Neovascularity can be seen in tumor, infarction, infection
In general, malignant tumors enhance; benign tumors do not.

54
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Describing the Lesion: Edema and Mass Effect
• Edema Pattern:– “Vasogenic, ischemic, cytotoxic,
periventricular interstitial”• Mass Effect:
– Midline shift– Herniation (uncal, transtentorial, etc.)

55
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Patient P.W. – MRI Findings • 4 x 4.5 cm solitary mass
• Irregular border
• Right frontal lobe (intra-axial)
• Low signal core (necrosis)
• Heterogenous, ring
enhancement
• Vasogenic edema pattern
• Mild midline shiftPACS, BIDMC

56
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Patient P.W. – MRI Findings
PACS, BIDMC
• DDx (imaging alone):– Glioblastoma multiforme– Anaplastic astrocytoma– Metastatic tumor– Lymphoma– Tuberculoma– Abscess
• DDx (imaging + history):– Glioblastoma multiforme– Anaplastic astrocytoma– Metastatic tumor– Lymphoma
• Treatment = surgical excision

57
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
Pre-Op:
POD #194
POD #83:Post-Op Day (POD) #1:
• T1, no gadolinium
• POD #1: tumor bed with high signal (acute hematoma + Surgicel)
• POD #83: tumor bed with low signal (resolving hematoma)
• POD #194: tumor bed enlarged with mixed signal (fluid + Gliadel wafers s/p second excision)

58
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
Pre-Op:
POD #194POD #139
POD #83:POD #1:
• T1 + gadolinium
• POD #83: linear enhancement surrounding region of XRT (radiation necrosis); 2 x 2 cm heterogenously enhancing mass anteromedial to original tumor bed (recurrent tumor)

59
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
Pre-Op:
POD #194POD #139
POD #83:POD #1:
• POD #139 (1 Day s/p resection of recurrent tumor): tumor bed with areas of no signal (air) and heterogenous signal (Gliadel wafers + Surgicel + blood)
• POD #194: Gliadel wafers; enhancing tumor bed margins with no signs of recurrence

60
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
Pre-Op:
POD #194POD #139
POD #83:POD #1:
• T2
• POD #1: extensive vasogenic edema surrounding tumor bed
• POD #83: vasogenic edema of anterior right frontal lobe surrounding site of recurrent tumor
• POD #194: fluid-filled resection site with no surrounding edema

61
Brook J Hill, HMS/HST IVGillian Lieberman, MD
FLAIR MRI• Fluid Attenuated Inversion Recovery
• Heavily T2 weighted
• CSF signal is nulled by sampling the MR image at an appropriate time after magnetization inversion, when longitudinal magnetization of CSF is zero
• Similar to STIR, except used for CSF instead of fat
• Allows better characterization of lesions adjacent to CSF-filled structures
• Clinically useful in several situations:– Intraxial brain tumors: differentiation between tumor and edema
– Tumor follow-up: identification of residual tumor at the resection margin
– Acute subarachnoid hemorrhage, Herpes encephalitis, Tuberous sclerosis, Mesial temporal sclerosis
• Limited by inability to fully suppress CSF signal when contaminated by blood/protein
62
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
Pre-Op:
POD #194POD #139
POD #83:
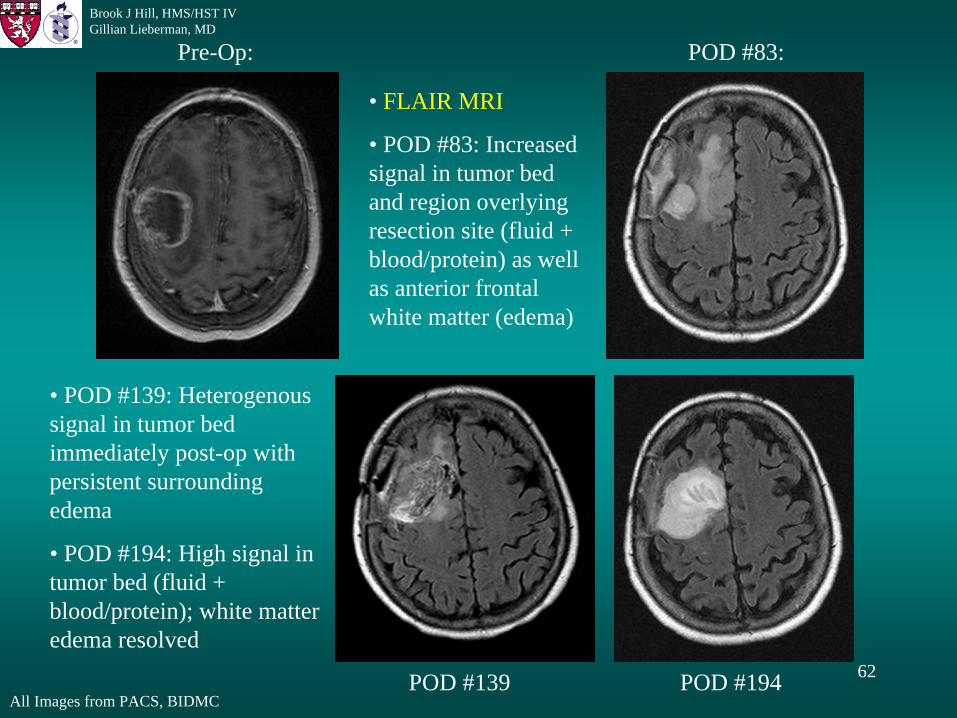
• FLAIR MRI
• POD #83: Increased signal in tumor bed and region overlying resection site (fluid + blood/protein) as well as anterior frontal white matter (edema)
• POD #139: Heterogenous signal in tumor bed immediately post-op with persistent surrounding edema
• POD #194: High signal in tumor bed (fluid + blood/protein); white matter edema resolved

63
Brook J Hill, HMS/HST IVGillian Lieberman, MD
DSC MRI• Dynamic Susceptibility Contrast-Enhanced MRI• A.K.A. “Susceptibility” MRI• Uses gradient echo or echo planar imaging techniques to enable measurement
of regional cerebral blood volume and regional cerebral blood flow• Provides functional information in addition to structural information• Multiple clinical uses in brain tumors:
– Provides additional information about the microvascular structure of gliomas (flow and permeability properties)
– Noninvasively grade gliomas
– Determine optimal biopsy sites
– Distinguish radiation necrosis from tumor regrowth
– Plan and follow irradiation, chemotherapy, and antiangiogenic therapy

64
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
Pre-Op:
POD #194POD #139
POD #83:POD #1:
• DSC MRI
• POD #1: High signal in resection site (blood) with peripheral areas of very low signal (Surgicel)
• POD #83: Persistent high signal in resection site
• POD #139: Heterogenous, but mainly very low signal in resection site (mostly Surgicel + Gliadel with some blood)

65
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
POD #194:POD #83:
T1:
2x2 cm low signal lesion in the left insular cortex.
No visible lesions.

66
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
POD #194:POD #83:
T1 + gadolinium:POD #139:
No visible lesions. 2x2 cm heterogenously enhancing lesion in left insular cortex (recurrent tumor).
No visible lesions.

67
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
POD #194:POD #83:
T2:POD #139:
2x2 cm region of increased signal in left insular cortex.
8x8 mm region of increased signal in left insular cortex.
10x10 mm region of increased signal in left insular cortex.

68
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
POD #194:POD #83:
FLAIR:POD #139:
8x8 mm region of increased signal in left insular cortex.
2x2 cm region of increased signal in left insular cortex.
10x10 mm region of increased signal in left insular cortex.

69
Brook J Hill, HMS/HST IVGillian Lieberman, MD
All Images from PACS, BIDMC
POD #194:POD #83:
DSC:POD #139:
2x2 cm region of increased signal in left insular cortex.
Subtle 10x10 mm region of increased signal in left insular cortex.
Barely visible 8x8 mm region of increased signal in left insular cortex.

70
Brook J Hill, HMS/HST IVGillian Lieberman, MD
MRI vs. CTFLAIR MRI (POD #139): CT (POD #150):
Images from PACS, BIDMC
10x10 mm region of increased signal in left insular cortex.
No visible lesions.

71
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Summary• Indications for intracranial imaging:
– Progressive neurologic dysfunction, Seizures, Elevated ICP, Known cancer with possibility of metastases
• Tests available: – MRI, CT, SPECT, PET, X-ray
• MRI is first-line test• SPECT and PET are functional studies and are good for follow-up• Describing the lesion:
– Size, Shape, Location, Number, Density, Enhancement, Edema, Mass Effect• FLAIR MRI: Nulls CSF signal, allowing better characterization of lesions
adjacent to or within CSF– Excellent for early detection of recurrent tumor
• DSC MRI: Provides functional information about regional blood volume and regional blood flow
– Allows noninvasive grading of gliomas

72
Brook J Hill, HMS/HST IVGillian Lieberman, MD
Acknowledgements
• Dr. Gillian Lieberman• Dr. Steve Reddy• Pamela Lepkowski• Larry Barbaras• Atara, Becca, Brian, Dave, Heather, Raj, Sarah, Suzie,
Taylor, Tim, and Wynn

73
Brook J Hill, HMS/HST IVGillian Lieberman, MD
ReferencesAbeloff MD, et al. Clinical Oncology, 2nd ed. Edinburgh: Churchill Livingstone, 2000.Aronen HJ, Perkio J. Dynamic susceptibility contrast MRI of gliomas. Neuroimaging Clin N Am. 2002 Nov;12(4):501-23.
Cha S, Johnson G, Wadghiri YZ, Jin O, Babb J, Zagzag D, Turnbull DH. Dynamic, contrast-enhanced perfusion MRI in mouse gliomas: Correlation with histopathology. Magn Reson Med 2003 May;49(5):848-55.
Essig M. Fast fluid-attenuated inversion recovery (FLAIR) MR imaging in the assessment of intraxial brain tumors. J Magn Reson Imag 1998;8:789-798.
Essig M. Contrast optimization of fluid-attenuated inversion-recovery (FLAIR) MR imaging in patients with high CSF blood or protein content. Magn Reson Med - 01-May-2000; 43(5): 764-7.
Essig M, Wenz F, Scholdei R, Bruning R, Berchtenbreiter C, Meurer M, Knopp MV. Dynamic susceptibility contrast-enhanced echo-planar imaging of cerebral gliomas: effect of contrast medium extravasation. Acta Radiol 2002;43:354-359.
Goetz CG, Pappert EJ. Textbook of Clinical Neurology. Philadelphia: Saunders, 1999.Hammoud DA, Belden CJ, Ho AC, Dal Pan GJ, Herskovits EH, Hilt DC, Brem H, Pomper MG. The surgical bed after BCNU polymer
wafer placement for recurrent glioma: serial assessment on CT and MR imaging. AJR Am J Roentgenol 2003 May;180(5):1469-75.Jackson A, Jayson GC, Li KL, Zhu XP, Checkley DR, Tessier JJ, Waterton JC. Reproducibility of quantitative dynamic contrast-
enhanced MRI in newly presenting glioma. Br J Radiol 2003 Mar;76(903):153-62.Jacobs AH, Winkler A, Dittmar C, Gossman A, Deckert M, Kracht L, Thiel A, Garlip G, Hilker R, Sobesky J, Vollmar S,
Kummer C, Graf R, Voges J, Wienhard K, Herholz K, Heiss WD. Molecular and functional imaging technology for the development of efficient treatment strategies for gliomas. Technol Cancer Res Treat 2002 Jun;1(3):187-204.
Latchaw RE, ed. MR and CT imaging of the Head, Neck, and Spine, 2nd ed. St Louis: Mosby, 1991. Li KL, Zhu XP, Checkley DR, Tessier JJ, Hillier VF, Waterton JC, Jackson A. Simultaneous mapping of blood volume and endothelial
permeability surface area product in gliomas using iterative analysis of first-pass dynamic contrast enhanced MRI data. Br J Radiol 2003 Jan;76(901):39-50.
Rempp KA, Brix G, Wenz F, Becker CR, Guckel F, Lorenz WJ. Quantification of regional cerebral blood flow and volume with dynamic susceptibility contrast-enhanced MR imaging. Radiology 1994;193:637.
Rydberg JN, et al. Initial clinical experience in MR imaging of the brain with a fast fluid-attenuated inversion-recovery pulse sequence. Radiology 1994;193:173-180.
Woodruff WW. Fundamentals of Neuroimaging. Philadelphia: Saunders, 1993.
Recommended