~ _ _ _ _ _ ~
INTERVENTIONAL PROCEDURES IN MUSCULOSKELETAL RADIOLOGY I 0033-8389/98 $8.00 + .OO
DIAGNOSTIC AND THERAPEUTIC FEATURES OF FACET AND
SACROILIAC JOINT INJECTION Anatomy, Pathophysiology, and Technique
Catherine Maldjian, MD, Mamed Mesgarzadeh, MD,? and Jamshid Tehranzadeh, MD
The therapeutic benefit of facet joint injection for low back pain has been debated in the literature. Various studies have pro- duced diverse results and have failed to re- solve this issue. Even investigators who sub- scribe to this technique do not concur regarding specific methods of administering this therapy. For instance, whether or not a purely intra-articular injection is required to achieve pain relief has been addressed, and data exist supporting both methods. This arti- cle addresses the anatomy, pathophysiology, and salient radiographic features of the lum- bar apophyseal joints. Our technique for facet joint injections is also discussed in addition to the pharmacology of various agents uti- lized for facet joint injection. Sacroiliac joint injection is also addressed.
ANATOMY AND PATHOPHYSIOLOGY The lumbar facet joints assume a prominent
role in resisting stress. Various features per-
This article is dedicated to the memory of Dr. Mamed Mesgarzadeh, who passed away during its preparation. We will always cherish his memory as a mentor, col- league, and friend. His many contributions to radiology will never be forgotten.
taining to the anatomy of these structures imparts this ability to withstand axial and shearing forces. The intervertebral disks are more vulnerable to the latter, although they are believed to play a more significant role in counteracting loading forces. In extension, however, the facets participate to a similar extent as the disk in withstanding compres- sive load.' Furthermore, disk space narrowing may also confer relatively increased loading onto the facets.8, ~ 5 , 41 The facets demonstrate a 30- to 60-degree angulation on axial inspec- tion.17 One anatomic study found the L1 slope to be 35 degrees, the L2 slope to be 30 de- grees, the L3 slope to be 34 degrees, the L4 slope to be 41 degrees, the L5 slope to be 53 degrees, and the S1 slope to be the greatest at 58 The progressive coronal orienta- tion of the lower facets (perpendicular to the plane of force), coupled with their increasing surface area, seems well adapted for accom- modating a greater load. Furthermore, trophic changes that occur in this setting imply that this is also the case. The decreasing height and anterior-to-posterior dimension of the lower facets decreases the transmitted force applied to the pedicles, whose increasing mediolateral size (cross-sectional area) also
From the Department of Diagnostic Imaging, Temple University (CM), Philadelphia, Pennsylvania; ?Deceased; formerly from the Department of Diagnostic Imaging, Temple University (MM), Philadelphia, Pennsylvania; and the Depart- ment of Radiological Sciences, University of California, Irvine UT), Orange, California
RADIOLOGIC CLINICS OF NORTH AMERICA
VOLUME 36 * NUMBER 3 MAY 1998 497

498 MALDJIAN et a1
participates in counteracting loading stress on the spine. Alternatively, some investigators suggest that the facets in the upper lumbar spine incur relatively greater loads.', Critics of this indicate that these studies were per- formed in vitro and compression was applied in an artificial manner, not taking into account the normal propensity for additional forward or shearing stress present specifically in this location.37
The superior facets face anterolaterally, whereas the inferior facets face posterome- dially, with the posterior aspects of both structures lying further from the midline than the anterior aspects. The superior facet has a concave orientation at the joint to accommo- date the more convex orientation of the infe- rior facet at the joint interface. Synovium may extend under or into the ligamentum flavum as well as along the articular processes, and there is considerable variability to the con- fines of the joint caps~le. '~ Autonomic nerves have been reported to exist in the joint and may contribute to low back pain.* The role of nocioceptors in this capacity has also been suggested, but remains controversial.ls, 23 A dual neural supply is provided to each facet joint, one from the dorsal rami at the same level as well as one from the level above. This may account for the somewhat diffuse pattern of pain associated with the facet joint syn- drome. Trauma, inflammation, arthritis, syno- vial impingement, meniscoid entrapment, and chondromalacia are suggested etiologies of facet pain7
INDICATIONS
Degenerative changes of facet joints are commonly noticed on radiographs, skeletal scintigraphy, CT scan, and MR imaging in asymptomatic patients.
In selecting patients with low back pain for facet joint therapy, careful clinical and radio- logic examination should be undertaken to exclude other causes, such as disk herniation, spinal stenosis, and nerve entrapment syn- drome due to hypertrophic spondylosis and the like.
Meticulous patient selection is an im- portant factor in achieving a successful rate of response to facet joint injection. Diagnostic features of lumbar facet syndrome include low back pain that is brought about or in- creased by movements, such as stretching, bending sideways, or attainment and mainte-
nance of certain positions, such as sitting erect for a long period of time. An important sign is focal tenderness on palpation directly over the facet joint. Other situations are low back pain, with or without sciatica, but with a nor- mal radiographic work-up; postlaminectomy syndrome with no evidence of arachnoiditis or recurrent disk disease; and persistent low back pain after a stable posterolateral spine fusion.4o
TECHNIQUE
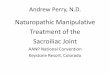
The procedure is performed in an outpa- tient setting with no premedication necessary. After obtaining informed consent, the patient is placed prone on the fluoroscopy table with a cushion under the abdomen (Fig. 1). If the joint space is not visualized, either the patient or the C-arm is rotated slightly until the joint space is detected. If the patient is rotated too far, the anterior portion of the joint space is detected rather than the posterior aspect. This is because the facet joints are curved, with the posterior aspects projecting in tangent in a posteroanterior view or shallow oblique and the anterior aspects coursing anteromedially, projecting best in a steeper oblique orienta- tion. The apex of this convexity divides the joint into anteromedial and posterolateral halves. During fluoroscopy these two parts of the joint lie tangent to the radiograph beam at different obliquities. With steeper obliquity, the anteromedial aspect of the joint is visual- ized and with a shallow obliquity the postero- lateral aspect of the joint (where the needle is to be placed) is seen. In order to determine and mark the entry points on the skin, under fluoroscopy the patient is gradually rotated opposite to the side of facet joint injection. When the joint is visualized at least obliquity, its location is marked on the skin. With fur- ther obliquity the anteromedial aspect of the joint may become tangent to the beam and visualized. This part of the joint cannot be accessed with a needle, however, and the pa- tient should be rotated back to a shallower obliquity to detect the posterolateral aspect of the joint. Obviously, the upper lumbar spine requires the least obliquity (as little as 30 degrees) and the lower lumbar spine may require a steeper obliquity (as great as 60 degrees).
The patient is cleansed in the appropriate area at least five times with a povidone-iodine solution. The drapes are placed in proper po-

DIAGNOSTIC AND THERAPEUTIC FEATURES OF FACET AND SACROILIAC JOINT INJECTION 499
A B 'r Figure 1. A, Patient is positioned prone on fluoroscopy table with a cushion under the abdomen to reduce the lumbar spine curvature. B, The posterior aspect of the facet joint can be brought to tangent for needle placement by slowly raising the affected side, often to a shallow anterior oblique position. (From Tehranzedah J: Percutaneous facet injection for the treatment of lumbar facet syndrome. In Kadir S (ed): Current Practice of lnterventional Radiology. Philadelphia, BC Decker, 1991, pp 750-753; with permission.)
sition. After anesthetizing the skin with a small 25-gauge needle, the needle is retained in the skin to double-check the entrance point and readjust if necessary. As soon as the 25- gauge needle projects vertically over the cen- ter of the joint, it is replaced with a 22-gauge spinal needle. In most instances a 3.5-in nee- dle is sufficient, although in extremely obese patients a 5-in Chiba needle may be neces- sary. The needle is directed straight down- ward and its perpendicular course is checked with every 2 cm of penetration. Insertion of the needle is continued until it contacts bone. It is the posterior portion of the joint that we penetrate for facet joint injections. A 22-gauge spinal needle is then placed into the joint with a vertical or nearly vertical approach. A vertical approach for the upper lumbar facets is adopted because these joints are more sagit- tally aligned. A slightly more oblique ap- proach is recommended in the lower lumbar spine, because these facets assume a progres- sively more oblique orientation (Fig. 2). Nee- dle position can be confirmed with contrast (Figs. 3,4, and 5). If the needle tip is correctly positioned inside the joint, it moves with the joint if the patient is rotated to the left or to the right. In a patient with a high-riding iliac crest, the L5 to S1 joint may be entered with
the needle tip slightly bent. This helps negoti- ate the crest, and when the desired depth is reached the needle can be rotated and aimed at the joint space.4o
If the referring physician requests docu- mentation of intra-articular location with con- trast injection we then perform an arthro- gram; otherwise, we avoid the use of contrast. We feel that if the objective of the procedure is for therapeutic benefit, then contrast should not be administered because it may serve as an irritant to the synovium and may subvert possible benefits of the other agents. To test the proper placement of the needle after the initial aspiration, one drop of contrast agent (preferably nonionic agent [e.g., Omnipaque 1801) is injected. If the needle is not in the joint, the contrast agent stays in the soft tissue at the tip of the needle. If the needle is in the joint, the drop of contrast agent quickly moves away from the needle tip to collect in the dependent portion of the joint capsule.4o The capacity of the joint is reportedly 1 to 2 mL.6f l5 When injection of contrast is re- quested, we inject approximately 0.1 to 0.3 mL of nonionic contrast into the joint. Subse- quently, 2 mL of bupivacaine= mixed with 0.4 mL of betametha~one~~ or equal amount of any other brand of long-acting steroid (such

500 MALDJIAN et a1
Figure 2. These anatomic specimens demonstrate the relatively sagittal orientation of the facet joints in the upper lumbar spine and the relatively coronal orientation in the lower lumbar spine. A, The top left is the L1-2 level; the bottom right is the L5-Sl level. B, The L1-2 level. C, The L5-Sl level.
as 20 to 40 mg or 0.5 to 1 mL of methylpred- nisolone acetate) for intra-articular use is gradually injected into the joint. In order to avoid capsular rupture, the injection is termi- nated when there is resistance. Although we have not conducted a formal study, we have found that extravasation of medication is a more effective technique for producing a ther- apeutic result.
PHARMACOLOGY
Betamethasone
We instill 0.5 mL of a betamethasone sus- pension33 with 2 to 3 mL of bupivacaine hy- drochloride. The betamethasone suspension consists of a combination of betamethasone bound to sodium phosphate and betametha-
sone bound to acetate in equal quantities with various chelates in an aqueous suspension. The actual chemical compounds involved are 9-fluoro-11B,17,21-trihydroxyl-l6B-methyl- pregna-1,4-diene-3,2O-dione21 -(disodium phosphate) and 9-fluoro-llB,17,21-trihy- droxyl-lbB-methylpregna-l,4-diene-3,20 di- one-21-acetate. These synthetic steroid ester compounds possess slightly different proper- ties. Betamethasone acetate is not water solu- ble, conferring a greater long-lasting effect. Betamethasone disodium phosphate is misci- ble in water and demonstrates a more rapid effect. Infection constitutes a major contrain- dication. Recommended dosages for intra-ar- ticular administration do not exceed 2 mL. When this agent is given in conjunction with a local anesthetic, as we do for our facet injections, paraben or phenol-containing for- mulations should not be considered because

DIAGNOSTIC AND THERAPEUTIC FEATURES OF FACET AND SACROILIAC JOINT INJECTION 501
Figure 3. Facet arthritis. A, Technetium-99m phosphate bone scan (posterior view) shows focal increased radionuclide uptake at L3-4 facet joint on the left side (arrow). 6, CT (prone position) confirms narrowing and arthritis of L3-4 facet joint on the left side (arrow). C, Contrast agent injection at L3-4 facet on the left side. Note leakage of contrast agent from the superior recess caused by overdistention of the joint following injection of Bupivacaine and melthylprednisolone acetate. (From Tehranzadeh J: Percutaneous facet injection for the treatment of lumbar facet syndrome. In Kadir S (ed): Current Practice of lnterventional Radiology. Philadelphia, BC Decker, 1991, pp 750-753; with permission.)

502 MALDJIAN et a1
absorption varies by mode of administration and dosage. The rate of systemic absorption can be inhibited to some extent by combining the preparation with epinephrine, a potent vasoconstrictor.
Peak blood levels are attained in 30 to 40 minutes with epidural or peripheral nerve blocks, with a gradual decline over 3 to 6 hours. Because its metabolism is dependent on hepatic function, hepatic derangements may predispose to toxicity of this agent, con- sisting mainly of cardiovascular and central nervous system disturbances. The mechanism of action is by inhibition of the initial neural impulse as well as neural conduction. Pro- posed explanations for this are increased neu- ral threshold, decreased propagation, and slowing of the action potential. The first func- tion to be affected is pain sensation, followed by temperature, touch, proprioception, and finally muscle tone. Bupivacaine has a rapid
Figure 4. Facet arthritis. Posterior-anterior projection of lower lumbosacral spine showing contrast material in the left L4-5 facet joint and confirming proper needle position in the facet joint in another patient with facet arthritis.
they can promote flocculation of the steroid (Table 1). Furthermore, the two compounds should not be mixed into one container, but rather only the requisite dose should be ex- tracted from each vial and then mixed in the syringe gently. Although initial dosages may vary, some systemic absorption does occur; therefore, recommended dosage limits should not be exceeded. Recommended dosages for intra-articular usage are shown in Table 1. These substances have potent anti-inflamma- tory effects and in high enough doses can cause immunosuppression. Suppression of the hypothalamic-pituitary axis has also been shown due to systemic absorption. The mech- anism of action in facet joint syndrome is believed to pertain to its anti-inflammatory properties; however, this has not been sub- stantiated because the mechanism of action on the facet joints has never been elucidated.
Bupivacaine Hydrochloride
Bupivacaine hydrochloride is a local anes- thetic agent related to the aminoacyl group of compounds. The fundamental composition of these agents consists Of a benzene ring linked to a piperidine group by an intervening am- ide group. Preparations that are methylpara- ben-free are available and these are recom- mended for intra-articular use with steroid
2)‘ Contraindications include hypersensitivity to this drug or to related compounds. Systemic
Figure 5. Severe osteoarthritis of the facet joint. CT of lumbar spine (bone windows) in supine position. A, Transaxial CT image at L5-Sl shows severe osteoarthritis with proliferative hypertrophic changes and vacuum phe- nomenon in the facet joints predominantly on the right side. 6, Hypertrophic bone changes on the right at L4-5 level completely obstruct the facet joint access (arrow). Note also sclerosis and erosive subchondral cyst forma- tion.
as discussed previously

DIAGNOSTIC AND THERAPEUTIC FEATURES OF FACET AND SACROILIAC JOINT INJECTION 503
Table 1. LONG-ACTING STEROIDS
Long-Acting Steroid Concentration Dose
Celestone suspension' 6 mg/mL 0.25-0.5 mL (1 5-3 mg)
Aristospan suspension* 20 mg/mL 0.1-0.3 mL (2-6 mg)
Hydeltranol 20 mg/mL 0.2-0.5 mL (4-10 mg)
betamethasone sodium phosphate and betamethasone sodium acetate
triamcinolone hexacetonide
prednisolone tebutate
'When these agents are given in combination with local anesthetics, the anesthetic should be methylparaben-free. propylparaben-free. and phenol-free; othewise flocculation may occur.
and relatively long-lasting effect, more so than any other anesthetic agent in its class. Although its mechanism of action in the facet joints is not known for certain, it is believed to act on the dorsal rami that innervate the joint capsule.
DISCUSSION
Facet joint syndrome is largely a diagnosis of exclusion. Degenerative disc disease and other disorders of the spine must be ex- cluded. When no other identifiable source for the back pain is found, then an investigation for a possible facet syndrome may be contem- plated. To even consider the diagnosis there must be failure of conventional therapy for at least 6 weeks' duration. Early investigators described pain on extension, radiating to the hip and thigh, as signs of possible facet joint syndrome. These have all been disputed. To comprehend fully the concept of a facet joint syndrome, one must trace the evolution of this entity from its incipience as a mere hy- pothesis.
The notion of pain originating from the facet joints was introduced by GoldthwaiP almost 90 years ago. About 20 years later, Ghormley14 provided the now familiar termi- nology of facet joint syndrome. This notion was further developed by Mooney and Robert-
son?* who were able to elicit pain in normal volunteers with hypertonic saline injections that then subsided with local anesthetic injection into the joint. Hirsch et alZ1 had pre- viously shown this but their data lacked ra- diographic confirmation that they were truly in the joint space. Subsequent investigators sought to demonstrate if there was a differ- ence between intra-articular and extra-articu- lar injections, generating mixed results. Des- touet et a15 demonstrated immediate relief and long-term pain relief in 54% and 21% of patients, respectively, with intra-articular injections. Lynch et alZ6 achieved 28% total pain relief and 28% partial relief at 6 months in their population. Their injections were in- tra-articular and only long-acting steroid was utilized. They furthermore demonstrated a greater success rate with multilevel injections and intracapsular as opposed to periarticular injections. A prior investigation by Raymond and Dumas36 produced disappointing results with solely intra-articular injections. Moran et alZ9 produced similar results, achieving a beneficial response in only 13%. Griffiths et all7 achieved long-term pain relief in 50% of their population with immediate relief in 90%. Murtagh30 reported a diagnostic re- sponse to lidocaine injections in 94% of injections, with steroid injection producing a long-term benefit in 54%.
Table 2. LOCAL ANESTHETIC AGENTS
Local Anesthetic Aaents Concentration Dose
Xylocaine-MPF* lidocaine HCI
Carbocaine HCI mepivacaine HCI
Sensorcainet bupivacaine HCI-MPF'
Marcainet bupivacaine HCI
0.5% or 1 Yo concentration
1% conc, 30-mL vial; 10 mg/mL
0.25%, 2.5 mg/mL
0.25% 10 mL or 30-mL vial for
1-5 mL (5-25 mg)
1-5 mL (10-50 mg)
1-5 mL (2.5-12.5 mg)
1-5 mL (2.5-12.5 mg) single dose*
'These agents are methylparaben free. ?These are the longest-acting agents in their class. HCI = hydrochloride; MPF = methylparaben free.

504 MALDJIAN et a1
Few prospective, controlled, and random- ized studies have addressed this subject. One such study by Lilius et alz4 assessed 109 pa- tients with chronic low back pain. Three ran- domized groups were designated as follows: (1) one group received intra-articular injection of a steroid mixed with local anesthetic agent, (2) another group received a pericapsular injection of the same mixture, and (3) the third group received physiologic saline intra- articularly into two joints. Neither the method, the type of injection, nor the dura- tion of symptoms correlated with outcome. Another randomized controlled study was performed by Carette et a13 in which 101 pa- tients were selected based on a 50% or greater reduction in pain with a single lidocaine block. Subsequently, 58% of the patients re- ported a reduction of pain by at least one half. One month later, 42% of patients receiv- ing steroid and 33% receiving saline injection had sustained pain reduction. Six months after injection these rates were 46% and 15%, respectively. Although these investigators saw greater improvement with a greater re- duction in pain and disability in their study group with steroid injection, they deemed this technique to be of marginal benefit to patients with low back pain. Critics of this study have pointed out that the investigators did not fol- low patients during the peak effect of methyl- prednisone (2 weeks) based on its biopharma- cokinetic properties7 Furthermore, critics have also suggested that a positive response to saline does not preclude facets as the source of pain because saline may potentially lyse adhesions within the joint capsule. Saline injections have shown beneficial results greater than those of placebo in myofascial syndromes. The prospective study by Lilius et a P has been criticized for using large vol- umes for intra-articular injections consisting of 8 mL, whereas several studies have demon- strated the capacity of the facet joint to be only 2 mL.
Possible positive predictors to facet joint injections have also been analyzed. Jackson et a P assessed 127 possible predictors for posi- tive response. They were unable to demon- strate any correlation after intra-articular injections of triamcinolone and bupivacaine hydrochloride. Prior studies claimed to iden- tify positive predictive factors. Fairbank et allo found acute back pain, pain augmented by sitting and bending, and back pain occurring with straight leg raising to be associated fre- quently with responders. Helbig and Leez0
similarly identified variables that correlated with a positive response. These consisted of paravertebral tenderness, symptoms elicited by extension-rotation movements, back pain in conjunction with groin or thigh pain, asso- ciated radiographic findings, and pain ex- tending below the knee. The criteria of these latter two investigators were challenged by a subsequent study by Schwarzer et a1,3* who found these criteria inadequate for differenti- ating facet joint pain from pain attributed to other sources. Schwarzer et aP9 also demon- strated that provocative joint injections in 90 patients were not predictive for symptomatic joints.
An alternative application for facet joint injection is in the setting of spondylolysis. The pars interarticularis communicates with the facet joint, being situated in the joint cap- sule.13 Furthermore, a diagnostic study for pars defect-related pain is particularly useful when there is concomitant disc disease for which spinal fusion surgery is being consid- e ~ e d . ~
In pathologic studies, 68% of patients over age 60 were found to have facet joint arthri- ti^.^^ Radiographic and CT classification schemes have been devised for this. Moder- ate-to-severe arthritis was demonstrated on CT in over 60% of the patients over age 40.3z In groups with low back pain, 28% had mod- erate to severe degenerative arthritis by ra- diograph or CT.32 Trophic changes are slightly more common at L5 to S1 than at L4 to L5.33 These changes appear unrelated to low back pain and degenerative disc disease!, 31 Such changes may impede access for facet joint injections (see Fig. 3).
SACROILIAC JOINT INJECTION
Injection of the sacroiliac joint can be per- formed either under CT guidance or fluoro- scopic control. Because the depth of the nee- dle is easier to assess by CT, we suggest the novice perhaps would be more accurate and comfortable to perform this procedure under CT. Later, when more experience is gained, it is actually easier and faster to perform this procedure under fluoroscopic control. The same agents are used as for facet injection.
The patient is prone on the fluoroscopy table and positioned slightly oblique to view the joint in tangent. The entrance point is marked on the skin with an indelible marker. The needle is directed toward the inferior

DIAGNOSTIC AND THERAPEUTIC FEATURES OF FACET AND SACROILIAC JOINT INJECTION 505
aspect of the joint because this is the di- arthrodial or synovial component of the sa- croiliac joint (Fig. 6). The upper portion is amphiarthrodial or fibrous and does not con- stitute a true joint. If two joint planes are visualized, the more medial one is selected because this represents the posterior joint plane. The more lateral joint silhouette is the anterior joint plane. The inferior-most portion of the sacroiliac joint demonstrates overlap of the anterior and posterior components and may impede posterior penetration because the anterior component is larger; 5 to 20 de- grees of contralateral rotation may assist in separating these two aspects of the joint. If too steep an obliquity is required to achieve this effect, then the most lucent portion of the inferior aspect of the joint should be accessed. After proper sterile conditions are obtained, the joint should be approached at the skin surface from a slight medial and superior po- sition with the needle tip angled laterally so that the needle can be directed in the same angle as the joint space. A 3.5-in 22-gauge spinal needle is advanced into the lower one third of the joint in this manner. To assess the depth of the needle in the joint, it is helpful to aim the needle toward the medial aspect of the iliac cortex. When the needle gently touches the iliac cortex, the needle is moved slightly medially to be placed in the joint space. Once the posterior ligaments are tra- versed, there should be abrupt decreased re- sistance, often described as a "pop." Al- though bone usually prevents passage through the anterior ligaments and into the presacral region, this is not always the case and lateral imaging should be performed to confirm proper placement; 0.5 to 1 mL of nonionic contrast may be instilled. Once joint penetration has been documented, the ste- roid-anesthetic combination is administered intra-articularly. Forty milligrams (1 mL) of methylprednisolone acetate and 3 mL of bup- ivacaine hydrochloride are adequate for each joint (see Fig. 6).
CT-GUIDED SACROILIAC JOINT INJECTION
The patient is placed prone on the CT table. Transaxial 5-mm sections are obtained at the mid and lower sacroiliac joint. One of the sections at the lower third of the joint is de- picted and the level is marked on the skin with indelible ink. The distance of the desired
sacroiliac joint is then measured and marked by a metallic paper clip and imaged and marked with indelible ink. Following proper preparation and draping and local anesthesia, a 22-gauge 3.5-in spinal needle is inserted in the joint. Occasionally, the patient and the needle need to be angled to overcome the obliquity of the joint (Fig. 7).
Pain referral maps have been successful as a screening tool for sacroiliac joint-related pa- thology." Sixteen of 54 patients were selected by pain-mapping criteria derived from a prior study of 10 volunteers who underwent sacro- iliac joint injection of contrast agent followed by lidocaine.12 All 16 patients demonstrated a positive provocative test for sacroiliac joint- related pain. Subsequently, discography and facet injections were performed on this group, neither of which produced a positive provoc- ative response. Corticosteroid sacroiliac joint injection in seronegative spondyloarthropa- thy has been shown to be of benefit.27 Al- though there are limited data on sacroiliac joint syndromes, it appears that sacroiliac joint pain is a more clear-cut entity to recog- nize clinically than facet joint syndrome.
CONCLUSION
Many studies investigating diagnostic crite- ria and therapeutic methods for facet joint syndrome have generated mixed results. It has emerged primarily as a wastebasket term and is invoked when no other etiology for low back pain fits the clinical data. Critics of the facet joint syndrome indicate that well- defined criteria for this entity have never been consistently established. Proponents of the facet joint syndrome designate a positive response to treatment as a diagnostic gold standard and criticize studies with unfavor- able results for having poor patient selection criteria. The reason that facet joint syndrome is an ill-defined, nebulous entity may be due in part to the diffuse, poorly localized pattern of pain generated by the dual nerve supply. Although there is no consensus on the exact definition of facet joint syndrome, clearly in some studies facet joint injections have pre- cipitated pain remission. We believe that per- cutaneous facet joint block is a useful diag- nostic and therapeutic procedure in the management of lumbar facet syndrome if used in a meticulously selected patient popu- lation. Careful clinical evaluation, use of CT, and proper fluoroscopic-guided injection of a

506 MALDJIAN et a1
Figure 6. Sacroiliac joint injection under fluoroscopy. A, Needle tip touching the iliac cortex of sacroiliac (SI) joint. This provides the information regarding the depth of the joint. Note indistinct cortices of ilium and sacrum in SI joint caused by arthritis. B, The needle is moved slightly (2 mm) more medial to be placed in the joint. C, The contrast agent flowing through the joint space confirms the correct needle placement.

DIAGNOSTIC AND THERAPEUTIC FEATURES OF FACET AND SACROILIAC JOINT INJECTION 507
Figure 7. Sacroiliac (SI) joint injection under CT guidance. A, 5-mm sections in the middle- and lower-third of the SI joint are obtained. 6, The needle is placed in the lower third of the SI joint.
local anesthetic and steroid provide a more favorable success rate. Sacroiliac joint syn- drome appears to be a more tangible entity from a diagnostic point of view and perhaps for that reason may be more amenable to this mode of therapy.
References
1. Adams MA, Hutton WC: The mechanical function of the lumbar apophyseal joints. Spine 8:327-330, 1983
2. Ashton IK, Ashton BA, et a1 Morphological basis for back pain. The demonstration of nerve fibers and neuropeptides in the lumbar facet joint capsule but not in the ligamentum flavum. J Orthop Res 1072- 78, 1992
3. Carette S, Marcoux S, et al: A controlled trial of corticosteroid injections into facet joints for chronic low back pain. N Engl J Med 325:1002, 1991
4. Cassidy JD, Loback D, et al: Lumbar facet joint asym-
5.
6.
7.
8.
9.
10.
11.
12.
metry. Interventional disc herniation. Spine 17570, 1992 Destouet JM, Gilula LA, et al: Lumbar facet joint injection: Indication, technique, clinical correlation, and preliminary results. Radiology 145:321-325,1982 Dory MA: Arthrography of the lumbar facet joints. Radiology 140:23-27, 1981 Dreyfuss PH, Dreyer SJ, et al: Lumbar zygapophyseal (facet) joint injections. Spine 20:2040-2047, 1995 Dunlop RB, Adams MA, et a1 Disc space narrowing and the lumbar facet joints. J Bone Joint Surg Br 66706710, 1984 El-Khoury GY, et al: Interventional musculoskeletal radiology. Curr Probl Diagn Radio1 23:162-203, 1994 Fairbank JCT, Park WM, et a1 Apophyseal injection of local anesthetic as a diagnostic aid in primary low back pain syndromes. Spine 6:598-605,1981 Fortin JD, April1 CN, et al: Sacroiliac joint: Pain refer- ral maps upon applying a new injection/arthrogra- phy technique. Part 11: Clinical evaluation. Spine 19:148%1489, 1994 Fortin JD, Dwyer AD, et al: Sacroiliac joint: Pain referral maps upon applying a new injection/

508 MALDJIAN et a1
arthrography technique. Part I: Asymptomatic volun- teers. Spine 19:1475-1482,1994
13. Ghelman B, Doherty J H Demonstration of spondylo- lysis by arthrography of the zygoapophyseal joint. AJR Am J Roentgen01 130986987,1978
14. Ghormley lW Low back pain with special reference to the articular facets, with presentation of an opera- tive procedure. JAMA 101:773, 1933
15. Glover JR Arthrography of the joints of the lumbar vertebral arches. Orthop Clin North Am 8:37-42,1977
16. Goldthwait JE: The lumbosacral articulation: An ex- planation of many cases of lumbago, sciatica and paraplegia. Boston Med Surg J 164:365-372, 1911
17. Griffiths H, Parantainen H, et al: Disease of the lum- bosacral facet joints. Neuroimaging Clin North Am
18. Gronblad M, Korkala, et al: Silver impregnation and immunohistochemical study of nerves in lumbar facet joint plical tissue. Spine 1634-38, 1991
19. Guang LX, Haughton Vh4, et a1 Lumbar facet joint capsule: Appearance at MR imaging and CT. Radiol- ogy 177:415-420, 1990
20. Helbig T, Lee CK The lumbar facet syndrome. Spine 13:61-64, 1988
21. Hirsch C, Iglemark 8, et al: The anatomical basis for low back pain. Acta Orthop Scand 33:l-17,1963
22. Jackson RP, Jacobs RR, et al: Facet joint injection in low back pain: A prospective statistical study. Spine 13:96&971, 1988
23. Konttinen YT, Gronblad M, et a1 Immunohistochemi- cal demonstration of subclasses of inflammatory cells and active collagen-producing fibroblasts in the syno- vial plicae of lumbar facet joints. Spine 15387-390, 1990
24. Lilius G, Laasonen EM, et al: Lumbar facet joint syndrome: A randomized clinical trial. J Bone Joint Surg Br 71:681-684, 1989
25. Lorenz M, Patwardham A, et al: Load-bearing char- acteristics of lumbar facets in normal and surgically altered spinal segments. Spine 8:122, 1983
3:567-575,1993
26. Lynch MC, Taylor JF, et a1 Facet joint injection for low back pain. A clinical study. J Bone Joint Surg Br 68:138-141, 1986
27. Maugars Y, Mathis C, et a1 Corticosteroid injection of the sacroiliac joint in patients with seronegative spondyloarthropathy. Arthritis Rheum 35:564-568, 1992
28. Mooney V, Robertson J: Facet joint syndrome. C l i
29. Moran R, OConnell D, et a1 The diagnostic value of facet joint injections. Spine 121407-1410, 1986
30. Murtagh FR: Computed tomography and fluoros- copy guided anesthesia and steroid injection in facet syndrome. Spine 13:686-689, 1988
31. Murtagh FR, Paulsen RD, et al: The role and inci- dence of facet tropism in lumbar spine degenerative disc disease. J Spinal Disord 486, 1991
32. Parthria M, Sartoris D, Resnick D: Osteoarthritis of the facet joints: Accuracy of oblique radiographic assessment. Radiology 164:227-230, 1987
33. Physicians' Desk Reference (PDR). Montvale, NJ, Medical Economics, 1996
36. Raymond J, Dumas JM: Intraarticular facet block: Diagnostic tests or therapeutic procedure? Radiology 151:333-336, 1984
37. Schneck C D The anatomy of lumbar spondylosis. Clin Orthop 18320-37,1985
38. Schwarzer AC, Aprill CN, et al: Clinical features of patients with pain stemming from the lumbar zygoapophyseal joints: Is the lumbar facet syndrome a clinical entity? Spine 191132-1137, 1994
39. Schwarzer AC, Derby R, et al: The value of the prov- ocation response in zygapophyseal joint injections. Clin J Pain 10309-313, 1994
40. Tehranzadeh J: Percutaneous facet injection for the treatment of lumbar facet syndrome. In Leadir S (ed): Current Practice of Interventional Radioloo. Phila- delphia, BC Decker, 1991, pp 750-753
41. Yang KH, King A1 Mechanism of facet load trans- mission as a hypothesis for low back pain. Spine
0rth0p 115149-156, 1976
9~557-565, 1984
Address reprint requests to Jamshid Tehranzadeh, MD
Department of Radiological Sciences University of California, Irvine
Medical Center 101 The City Drive
Orange, CA 92868-3298
Recommended