Page 1 of 26
Devon Mental Health Crisis Pathway
‘To Be’ VSM Scenario Testing Report
Report Prepared for: Gavin Thistlethwaite, Joint Commissioning Manager – Mental Health, NEW Devon CCG
and Devon County Council
Prepared by: Steve McLauchlan, Managing Consultant, Alexander
Contact Tel: 07554 012119
Email: [email protected]

Page 2 of 26
VERSION CONTROL
Author Version Issue Date Details & Reason for Issue
Steve McLauchlan 0.1 24.11.15 First draft for review and feedback
Steve McLauchlan 0.2 07.12.15
Second draft following feedback from Emily Faircloth and alignment with SG presentation to Devon MH SG on 4.12.15
Keith Pople 1.0 8.12.15 Quality review for release to Gavin Thistlethwaite

Page 3 of 26
Table of Contents
1. Executive Summary ................................................................................. 4
2. Background ............................................................................................. 5
Previous phases of work on the MH Crisis Care Pathway ............................................. 5
3. MH Crisis ‘To Be’ VSM Scenario Testing .................................................. 8
Purpose of the phase ..................................................................................................... 8
What we did – preparation for scenario testing ........................................................... 8
What we did – testing the scenarios ............................................................................. 9
4. MH Crisis ‘To Be’ VSM Scenario Testing - outputs ................................. 10
Participation ................................................................................................................ 10
Rigour in scenario testing ............................................................................................ 10
What we found ............................................................................................................ 10
Implications for MH Crisis ‘To Be’ VSM ....................................................................... 17
Recommendations ....................................................................................................... 18
5. Piloting the MH Crisis ‘To Be’ VSM ........................................................ 19
Critical Success Factors ................................................................................................ 19
Planning & Preparation ............................................................................................... 19
Assumptions & Interdependencies ............................................................................. 20
6. Appendices............................................................................................ 21
Appendix 1 – ‘As Is’ VSM ............................................................................................. 21
Appendix 2 – ‘To Be’ VSM pre scenario testing .......................................................... 23
Appendix 3 – updated ‘To Be’ VSM post scenario testing .......................................... 25

Page 4 of 26
1. Executive Summary
Starting in March 2015, Alexander supported the Devon-wide MH multi-agency working group in preparing a plan to meet the requirements of the MH Crisis Care Concordat and to identify opportunities for improving the Devon and Plymouth MH Crisis Care Pathway.
Outputs from this work included: o An ‘As Is’ Value Stream Map (VSM) (see Appendix 1) delineating current system
arrangements for dealing with MH Crisis. o A set of priorities for improving response to and experience of individuals with
urgent MH needs. o A plan for improvement that was accepted as meeting requirements of the MH
Crisis Care Concordat. o Definitions of what ‘good’ looks like – from the perspectives of people with lived
experience of MH crisis and of provider organisations in the MH system.
In June 2015, Alexander were asked to support the working group in developing an MH Crisis ‘To Be’ VSM, building on outputs from the previous phase.
An MH Crisis ‘To Be’ VSM (see Appendix 2) was presented to the MH ACP Steering Group in July 2015 and it was agreed that this should be subject to ‘scenario testing’ prior to taking decisions around piloting / rolling out a new model for responding to MH Crisis Care needs.
Alexander were asked to provide support to the Scenario Testing phase in September 2015.
This report sets out the approach, methodology and outputs of scenario testing including implications for new key components of a redesigned MH Crisis VSM (see Appendix 3):
o A ‘single, unique, point of contact’ (SUPOC) to address issues around access to MH Crisis response services and with capacity to operate 24/7 and respond to all callers.
o ‘Intoxication Support’ to address issues around the impact that intoxication (in all forms) has on the way that the system responds to MH Crisis.
o A redesigned ‘Crisis Service’ to address issues around responsiveness of current Crisis teams.
It is recommended that these implications are addressed in moving to detailed design as part of preparing and planning a pilot of the ‘To Be’ MH Crisis VSM.
Based on outputs from scenario testing and to inform a decision on moving to detailed design and planning and preparation for a pilot, a set of initial Critical Success Factors, workstreams, assumptions and interdependencies are described.

Page 5 of 26
2. Background
Previous phases of work on the MH Crisis Care Pathway
In March 2015, Alexander were asked to support a Devon-wide multi-agency working group in preparing a plan to meet requirements of the MH Crisis Care Concordat and identifying opportunities for improving the Devon and Plymouth MH Crisis Care Pathway.
The Alexander approach adopted is shown in Figure 1 below and work in the initial phase focused on Feasibility and Analysis stages:
Figure 1: Alexander approach - FARIC
The scope of that phase – MH Crisis in the ACP – is illustrated in Figure 2:
Figure 2: MH Crisis in the ACP

Page 6 of 26
The objectives of the phase were to:
Keep personal experience – and its improvement – at the centre of planning.
Agree what ‘good’ looks like.
Make an express commitment to acting on a system view of meeting urgent MH needs in Devon that is informed by personal experience.
Describe the critical parts of the Value Stream Map (VSM) leading up to when an individual, with urgent MH needs, makes contact with professional MH services so that a course of therapy / treatment may start.
Agree appropriate actions for improving arrangements for: o First contact with services / first response. o Health Based Places of Safety (HBPoS). o S136 detention, including conveyance. o Street Triage.
The outputs of that phase included:
An ‘As Is’ VSM (see Appendix 1) delineating current system arrangements for dealing with MH Crisis.
A set of priorities for improving response to and experience of individuals with MH Crisis needs.
A plan for improvement that was accepted as meeting requirements of the MH Crisis Care Concordat.
Definitions of what ‘good’ looks like – from the perspective of people with lived experience of MH crisis.

Page 7 of 26
And from the perspective of provider organisations in the MH ACP system.
Alexander were then asked, in June 2015, to further support the working group in developing an MH Crisis ‘To Be’ VSM, building on outputs from the previous phase.
This work focused on the Redesign stage in Figure 1 and was completed with input from people with lived experience and clinical professionals, paramedics and police officers.
The principal output of this phase was a ‘To Be’ VSM incorporating several new and / or fundamentally redesigned components:
A ‘single, unique, point of contact’ (SUPOC) to address issues around access to MH Crisis response services and with capacity to operate 24/7, respond to all callers and, in particular:
o Respond to GP, Paramedic and Police calls for information, advice and guidance. o Mobilise MH specialist resources to attend where necessary.
With regards to definition of ‘all callers’, it should be noted that this includes demand involving people of all ages and with needs from seeking information / signposting, through needing someone to ‘talk to’, to needing urgent MH Crisis response.
An ‘Intoxication Support Unit’ to address issues around the impact that intoxication (in all forms) has on the way that the system responds to MH Crisis.
A redesigned ‘Crisis Service’ to address issues around responsiveness of current Crisis Teams.
The MH Crisis ‘To Be’ VSM
An MH Crisis ‘To Be’ VSM (see Appendix 2) was presented to the MH ACP Steering Group in July 2015 and it was agreed that the VSM should be subject to ‘Scenario Testing’ prior to taking decisions around piloting / rolling out a new model for responding to MH Crisis Care needs.
Alexander were asked to provide support to the Scenario testing phase in September 2015.

Page 8 of 26
3. MH Crisis ‘To Be’ VSM Scenario Testing
Purpose of the phase
The purpose of the VSM Scenario testing phase was to:
Develop the ‘To Be’ VSM through a series of scenario testing and review workshops and enable stakeholders to ‘visualise’ benefits of the redesigned model for people with lived experience, families, carers, communities, provider organisations, emergency services and staff
Evaluate readiness of the VSM for piloting including stakeholder commitment, scope, plan, resources, pathway, area, crucial data / data points and measurable CSFs / outcomes
What we did – preparation for scenario testing
In preparing for scenario testing sessions, we:
Gathered a set of scenarios to be tested based on case studies and examples of ‘typical’ demand experienced across the system. These were provided by a range of stakeholders including people with lived experience, support organisations, provider organisations and emergency services.
Designed a ‘scenario template’ to ensure consistency in presentation.
Tested and refined the ‘scenario template’ to facilitate ‘flexing’ of scenarios and ensure rigour in testing of the ‘To Be’ VSM.
Defined components of the ‘To Be’ system and invited organisations representing all components to provide people with experience of responding to MH Crisis to attend the scenario testing and review sessions.
Designed an approach and methodology for conducting scenario testing and review sessions and capturing outputs.
Tested and refined the approach and methodology through workshops with people with lived experience, carers, support organisations and the MH ACP working group.
The approach and methodology for scenario testing included a recognised methodology known as Failure Modes & Effects Analysis (FMEA).
FMEA is a structured approach to identifying ways in which a service or process can fail, assessing the impact of failure and identifying actions to prevent and / or reduce the risk of failure.
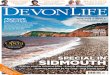
Figure 3 (next page) illustrates how the approach was embodied in scenario testing and review workshops.
The ‘expert panel’ comprised representatives of provider organisations, emergency services and stakeholder organisations.
‘Devil’s Advocates’ included individuals with lived experience of MH Crisis, carers and support organisations.
‘Observers’ included Alexander consultants and NEW Devon CCG officers.

Page 9 of 26
Figure 3: Failure Modes & Effects Analysis approach to scenario testing
What we did – testing the scenarios
A series of scenario testing and review sessions were scheduled over 2 weeks i.e. 3rd – 5th and 10th, 11th November at Exeter Community Centre, St David’s Hill, Exeter.
Separate sessions were scheduled for mornings and afternoons to enable the widest possible range of attendees.
Each scenario testing session started with an ‘orientation’ presentation – ensuring all attendees were familiar with background to the work being undertaken and briefed on the FMEA approach and their roles during scenario testing.
Brief background / contextual details around an example of MH Crisis demand were then introduced by a facilitator (Alexander consultant) and members of the expert panel asked to work through a ‘To Be’ response – starting with an initial point of contact.
As responses were developed, all attendees were able to challenge, identify potential ‘failure modes’ and their effects and vary elements of the scenario to explore a wide range of options at each stage of the VSM.
Outputs were captured by observers and these comprised:
Descriptions of component ‘failure modes’.
The impact of component ‘failure modes’ on other elements of the VSM.
The impact of component ‘failure modes’ on the experience or ‘journey’ of people through the VSM – people, in this context, included everyone involved i.e.
o People experiencing MH Crisis, family members, carers. o Members of the public, employers etc. o GPs, Paramedics, Police Officers, clinical and MH professionals.
Each scenario testing session ended with a review of ‘Organisation’ and ‘People’ learning points to be reflected in adjusting the ‘To Be’ VSM and / or addressed in planning and preparing for piloting.

Page 10 of 26
4. MH Crisis ‘To Be’ VSM Scenario Testing - outputs
Participation
The scenario testing sessions were attended by representatives of all components of the VSM, people with lived experience, carers, support organisations and other stakeholder organisations.
In particular, all sessions were attended by representatives from DPT (including AMHPs), Police, Psychiatric Liaison, people with lived experience and support organisations.
Rigour in scenario testing
Throughout scenario testing sessions, participants ensured that all components of the ‘To Be’ VSM were examined by ‘flexing’ the scenarios to adjust key factors, including:
Person or organisation receiving initial contact.
Person or organisation making initial contact.
Gender, age (including children and older adults), nationality of person experiencing MH crisis.
Time of day.
Physical health issues, MH issues / symptoms.
Attitude of person experiencing MH crisis (co-operative, resistant, violent etc.).
Capacity of person experiencing MH crisis (including a range of forms of intoxication).
Location of person experiencing MH crisis.
What we found
Potential failure modes as they relate to components of the ‘To Be’ MH ACP VSM are set out below with assessments of potential failure effects on organisations and people and required actions:
System component - SUPOC
Potential failure modes Potential failure effects Action required
Insufficient capacity to accommodate demand
Organisation / System:
Unable to provide timely response to demand
Demand escalates to other services e.g. Police, Ambulance, EDs
People:
Inability to access timely response causes confusion, frustration and sub-optimal decision making
Delay in response exacerbates crisis
Inappropriate response exacerbates crisis
Reputation and confidence in MH system is undermined
Collect and analyse data to understand current demand volumes across whole MH Crisis pathway: - Sources of demand - Profile of demand - Range of responses
Model capacity requirements.
Feed in to SUPOC design.
Plan to over resource SUPOC at start of pilot.
Review early intervention / prevention models.
Insufficient breadth / depth of skills, knowledge and experience to respond effectively to full range of demand
Organisation / System:
Unable to provide effective response to demand
Collect and analyse data to understand nature and range of current demand:

Page 11 of 26
System component - SUPOC
Potential failure modes Potential failure effects Action required
Note: Scenario testing sessions identified that design of initial contact / conversations is crucial to effectiveness of response and engagement of people experiencing MH Crisis.
Specifically, behaviours / attitudes / tone of voice can have substantial impact on whether response is effective
Delays in decision making
Sub-optimal decision making
Demand escalates to other services e.g. Police, Ambulance, EDs
Reputation and confidence in MH system is undermined
People:
Inability to access effective response causes confusion, frustration and sub-optimal decision making
Delay in response exacerbates crisis
Inappropriate response exacerbates crisis
- Sources, Types of demand - Age ranges - Language / cultural range - Complexity re related issues e.g.
physical health; family/social context
Model ‘core’ and ‘extended’ ranges of demand and feed into SUPOC design and job design.
Plan to over resource SUPOC at start of pilot.
Review training provision.
SUPOC staff unable to effect seamless hand offs / transfers of calls to other organisations.
SUPOC not able to access full range of information.
SUPOC not able to share information with other organisations.
Organisation / System:
Delays in decision making
Sub-optimal decision making
Delays in connecting people to appropriate services
Reputation and confidence in MH system is undermined
People:
Requirement to make multiple calls to access appropriate sources of support and / or response causes confusion, frustration and sub-optimal decision making
Delay in receiving support / appropriate response exacerbates crisis
Define policy to 'pass through' calls to a range of agencies.
Define information system and technology requirements.
Review policy regarding information sharing.
Develop policy for positive, proactive approach and 'can do' attitude whilst observing legal / regulatory requirements.
Staff training, education and coaching.
Access to a comprehensive directory of services for MH crisis.
Overlap / duplication regarding role / responsibilities of SUPOC and: 1. Other initiatives around ‘single
points of contact’ e.g. DPT, CAMHS.
2. Other components of MH Crisis ‘As Is’ VSM e.g. 111 services, EDT
3. Components of other pathways e.g. MASH
4. Other organisations in wider MH system e.g. My Devon, Bay 6, Samaritans.
Organisation / System:
Proliferation of ‘single points of contact’ causes confusion
Lack of clarity regarding roles and responsibilities
Demand ‘bounces’ around the system
Delays in decision making
Sub-optimal decision making
Reputation and confidence in MH system is undermined
People:
Confusion regarding appropriate sources of support and / or
1. Engage with DPT, CAMHS to
explore detail of proposals and align / rationalise to achieve vision of a SUPOC for the whole MH Crisis pathway.
2. Engage with 111 service re-commissioning project and DPT to align design of SUPOC.
3. Engage with components of other pathways and identify requirements around information sharing, cross-referral etc
4. Gather information regarding full range of organisations and their various offers and consider in commissioning arrangements.

Page 12 of 26
System component - SUPOC
Potential failure modes Potential failure effects Action required response causes confusion, frustration and sub-optimal decision making
Delay in receiving support / appropriate response exacerbates crisis
System component – Intoxication Support Unit
Potential failure modes Potential failure effects Action required
Inconsistency in system response to MH crisis where person is intoxicated i.e. people are ‘pushed away’.
Lack of clarity around purpose, role and functionality of an ‘Intoxication Support Unit’.
Wide range of potential need with regards to severity and cause of intoxication – giving rise to a need for a wide range of responses and capacity / capability.
In cases beyond ‘mild / simple’ intoxication appropriate response is to convey to ED.
Inappropriate attitude to intoxication undermines parity of esteem
Organisation / System:
Does not provide timely and or effective response
Provides inappropriate / sub-optimal response
Demand escalates to other services e.g. Police, Ambulance, EDs
Legal Highs – significant impact on ED and / or hospital wards
Reputation and confidence in MH system is undermined
People:
Inability to access support and / or response whilst intoxicated causes confusion, frustration and sub-optimal decision making
Delay in response exacerbates crisis
Inappropriate response exacerbates crisis
Amend MH Crisis ‘To Be’ MH ACP VSM to remove ‘Intoxication Support Unit’.
Collect and analyse data relating to intoxication and MH Crisis.
Research best practice models e.g. Birmingham & Solihull Compass service.
Review policy and define options for providing ‘Intoxication Support’ at appropriate points in the MH Crisis ‘To Be’ VSM including who is responsible for making decision re fitness for MH assessment.
System component – Crisis Service
Potential failure modes Potential failure effects Action required
Lack of current Crisis Team capacity to provide a ‘Crisis Response’.
Current Crisis Teams do not provide 24/7 cover.
Current Crisis Teams are not open to all ages.
Lack of current EDT capacity to provide a consistent 'Crisis Response' across Devon.
Lack of Street Triage capacity to provide consistent support 'on the street'.
Lack of Psychiatric Liaison capacity / capability to deal with all ages.
Organisation / System:
Does not provide comprehensive, consistent, timely and effective response to urgent need for professional MH services
Demand escalates to other services e.g. Police, Ambulance, EDs
Reputation and confidence in MH system is undermined
People:
Inability to access urgent response causes delay, confusion, frustration and sub-optimal decision making
Delay in response exacerbates crisis
Amend MH Crisis ‘To Be’ VSM to remove ‘Crisis Service’.
Collect and analyse data relating to demand requiring ‘Crisis Response’: - Sources of demand - Profile of demand - Points at which demand arises - Range of responses required
Feed in to design of policy and capacity planning around ‘Crisis Response’ at appropriate points in the MH Crisis ‘To Be’ VSM.

Page 13 of 26
System component – Crisis Service
Potential failure modes Potential failure effects Action required Inappropriate response
exacerbates crisis
System component – Ambulance Service
Potential failure modes Potential failure effects Action required
Paramedic do not have access to patient records.
Information systems do not enable electronic transfer of information from control room to paramedics.
Organisation / System:
Paramedics need to repeat process of gathering information
Delay in assessment of MH needs
Sub-optimal decision making based on insufficient / incorrect information
People:
Repeating process of information gathering causes delay, confusion and frustration and can exacerbate crisis
Paramedics lose confidence in 'the system' and their own competence
Collect and analyse data around demand on Ambulance Service that involves MH needs.
Review information system requirements and functionality.
Review process to identify work-rounds.
Consider options for fulfilling demand for ‘real time’ information / guidance.
Variation in Paramedic confidence and competence for handling conversations around MH needs effectively and sensitively including: - Family members / carers having
different view of 'need' from individual.
- Interpretation of 'capacity' under MHA / MCA.
- Finding reasons for not being able to help e.g. confidentiality.
- Lack of clarity regarding powers re restraint, prescribing etc.
Organisation / System:
Delay in assessment of MH needs
Sub-optimal decision making based on insufficient / incorrect knowledge
Inappropriate response
People:
Delay, indecision, dispute can exacerbate crisis
Paramedics lose confidence in 'the system' and their own competence
Develop policies for positive, proactive approach and 'can do' attitude whilst observing legal and regulatory requirements.
Design and deliver training, education and coaching.
Ambulance is not necessary and / or most appropriate mode of conveyance.
Organisation / System:
Sub-optimal use of vehicles
Delay in response
Inappropriate response
People:
Stigma can exacerbate crisis
Resistance to being conveyed in an Ambulance
Heightened tension and stress for individuals, family members, carers, Paramedics
Ambulance service to review policy regarding timing / mode of conveyance.
Delivery in accordance with what is 'promised'.
Assess capacity required and align with service specification.

Page 14 of 26
System component – Police
Potential failure modes Potential failure effects Action required
Control Room - delay in assessing need and providing appropriate response to callers.
Variation in Police officer confidence and competence for identifying MH needs effectively and sensitively.
Lack of clarity around ownership of responsibility for individuals and limits of respective duties / powers e.g. vis-à-vis Paramedics.
HB PoS lack capacity to accommodate individuals in crisis.
Organisation / System:
Delays in providing appropriate support / treatment
Lower order needs escalate to MH crisis
Inappropriate use of s136 powers and / or powers of arrest
Use of inappropriate modes of conveyance.
Use of inappropriate accommodation e.g. police suite, ED open space / cubicle
People:
Delay in receiving appropriate support / treatment for MH needs causes confusion, frustration and sub-optimal decision making
Inappropriate use of S136 powers and / or modes of conveyance escalates crisis and impacts Police officers time
Avoidable exacerbation of MH crisis
Increased risk to person in MH crisis and others
Police officers lose confidence in 'the system' and their own competence
Collect and analyse data around demand on Police that involves MH needs.
Identify root causes of inappropriate use of S136 powers and / or powers of arrest.
System component – GPs
Potential failure modes Potential failure effects Action required
Variation in GP competence and confidence for recognising and dealing with MH issues.
GPs not having timely access to help regarding MH Crisis.
Inconsistency in GPs’ response to MH Crisis.
Organisation / System:
Does not recognise lower order MH needs and provide timely and / or effective response
Sub-optimal decision making
Delays in providing appropriate support / treatment
Lower order needs escalate to MH crisis
People:
Delay in receiving appropriate support / treatment for lower order MH needs causes confusion, frustration and sub-optimal decision making
Lower order needs escalate to MH crisis
GPs lose confidence in 'the system' and their own competence
Consider feasibility of enabling GP access to patients' MH records and plans.
Collect and analyse data relating to MH demand in Primary Care services.
Identify and evaluate options for driving and supporting improvement in GP confidence / competence.
Incorporate provision of ‘real time’ support to GPs in SUPOC capacity planning.

Page 15 of 26
System component – CAMHS
Potential failure modes Potential failure effects Action required
Weakness around Out of Hours coverage.
Variations in services across Devon - age; geography; situation.
Variations in services re Safe Places for Adults and Children e.g. Safe Places work underway does not cover Plymouth.
CAMHS redesign does not align / integrate with wider MH Crisis pathway redesign
Organisation / System:
Does not provide comprehensive, consistent, timely and effective response to urgent need for professional MH services
Demand escalates to other services e.g. Police, Ambulance, EDs
People:
Inability to access urgent response to MH crisis causes delay, confusion, frustration and sub-optimal decision making
Delay in response exacerbates crisis
Inappropriate response exacerbates crisis
CAMHS are working on issues relating to Out of Hours coverage and consistency in services across Devon.
Align / integrate CAMHS work with wider MH Crisis pathway redesign.
Ensure current work around Safe Places takes account of needs for Adults and Children.
Review scope to understand why Plymouth not included.
Single HB PoS for children covering Devon / Torbay / Plymouth is situated in Plymouth.
Organisation / System:
Lack of capacity to provide, consistent, timely and effective response to urgent need for professional MH services
Demand escalates to other services e.g. Police, Ambulance, EDs
People:
Inability to access urgent response to MH crisis causes delay, confusion, frustration and sub-optimal decision making
Delay in response exacerbates crisis
Inappropriate response exacerbates crisis
Collect and analyse data re demand.
Consider need for increased capacity across Devon.
Current service design based on chronological age - clinical debate as to whether this is most effective.
Organisation / System:
Sub-optimal design?
Consider scope for clinical professionals to inform judgements on most effective model.

Page 16 of 26
System component – Emergency Departments
Potential failure modes Potential failure effects Action required
Inappropriate environment for a person in MH crisis.
Requirement to provide information several times.
Delays in physical health assessment.
Delays in MH assessment.
Variation in ED staff competence and confidence for recognising and dealing with MH issues.
Inappropriate attitude / response to MH crisis – particularly when discussing person’s symptoms / background.
Variation in coverage of Alcohol Liaison services.
Information relating to physical health and MH is held on separate systems.
Where S136 is used, person in MH crisis is responsible for information.
Organisation / System:
Does not provide comprehensive, consistent, timely and effective response to urgent need for professional MH services
ED environment exacerbates crisis
Inappropriate attitude / response to MH crisis escalates crisis
Requirement for other services e.g. Police, Ambulance to maintain presence to keep person in MH crisis and others safe.
People:
Inability to access urgent response to MH crisis causes delay, confusion, frustration and sub-optimal decision making
Delay in response exacerbates crisis
Inappropriate response exacerbates crisis
Escalating crisis affects everyone in ED environment
Crisis Care Concordat action plan addressing need for appropriate environment in EDs and ‘Safe Places’.
HB PoS – collect and analyse demand.
Consider need for increased capacity.
Evaluate opportunity for SUPOC, GPs, CMHTs and emergency services to provide early warning where person in MH crisis is being referred or conveyed to ED.
System component – Psychiatric Liaison
Potential failure modes Potential failure effects Action required
Service not available 24/7.
Inability to access information 'out of hours' where person in MH crisis is known and / or open to MH services.
MH assessment is carried out in inappropriate location and can include several professionals.
MH assessment methodology is sub-optimal.
Failure to consider 'whole situation' of an individual.
Failure to explain what is happening / will happen to the individual.
Inappropriate attitude / behaviours of clinical staff.
Organisation / System:
Does not provide comprehensive, consistent, timely and effective response to urgent need for professional MH services
ED environment exacerbates crisis
Inappropriate attitude / response to MH crisis escalates crisis
People:
Inability to access urgent response to MH crisis causes delay, confusion, frustration and sub-optimal decision making
Delay in response exacerbates crisis
Inappropriate response exacerbates crisis
Escalating crisis affects everyone in ED / Hospital environment
Collect and analyse data relating to demand requiring ‘Crisis Response’: - Sources of demand - Profile of demand - Points at which demand arises - Range of responses required
Feed in to design of policy and capacity planning around ‘Crisis Response’ at appropriate points in the MH Crisis ‘To Be’ VSM.

Page 17 of 26
Implications for MH Crisis ‘To Be’ VSM
SUPOC
The SUPOC concept seeks to address issues of access to the MH Crisis pathway; and to provide a wide range of advice, guidance and support, which facilitates both navigation and prevention.
Potentially responding quickly and effectively to all demand from everybody on a 24/7 basis requires:
A wide range of skills, knowledge and experience.
Access to a full range of information sources and systems
Critical functionality for ‘warm’ transfer of calls with full data / information
Requirement to develop protocols for sharing information between services is a key factor in SUPOC design.
DPT and CAMHS ‘SPOC’ / ‘referral hubs’ need to be coordinated and aligned a MH Crisis SUPOC acting for the whole system.
Intoxication Support / Crisis Service
It is not easy to present either ‘Intoxication Support’ or ‘Crisis Service’ in the MH Crisis VSM by a ‘place’, ‘unit’ or ‘team’.
Critical ‘failure modes’: o Lack of responsiveness and judgemental attitudes towards ‘intoxication’ o Lack of capacity to provide consistent, timely and effective response to MH crisis.
Further redesign of the MH Crisis VSM should focus on developing policy and approaches for dealing with intoxication and crisis response – applied consistently throughout the VSM.
Links between components of MH Crisis pathway
Links between components of the VSM are critical to system performance – scenarios involving MH crisis invariably include several organisations and agencies.
Critical failure modes: o Inability to effect seamless transfer of a person in MH crisis from one component to
another. o Inability / failure to share information and reduce / remove need for repeated
‘interrogation’. o Lack of clarity / understanding around respective roles and responsibilities: failure of
one component to respond effectively drives ‘failure demand’ into the system and exacerbates crisis and impact on family members, carers and professionals. Inability to effect seamless transfer of a person in MH crisis from one component to another.
Data
Demand covering MH needs and / or MH crisis provision is not well understood: lack of reliable, up to date, quantitative data is a major issue.
Lack of evidence-informed understanding clearly undermines effective decision-making – particularly around alignment of appropriate resources to need.
This critical weakness must be addressed effectively as part of preparation and planning for a pilot of the ‘To Be’ MH Crisis VSM.

Page 18 of 26
Recommendations
It is recommended that these implications are addressed in moving to detailed design as part of preparing and planning a pilot of an updated MH Crisis ‘To Be’ VSM (see Appendix 3).
It is also recommended that:
The SG is the higher governance body for a pilot and: o Champions the project, collectively and individually, as a joint initiative of the Devon
public service system. o Agrees the mandate; the CSFs; and the required benefits of implementation. o Agrees the immediate process for selecting the pilot geography and then selects the
geography (for the pilot and for implementation). o Agrees (or not) that the whole MH Crisis pathway is within scope. o Raises the profile of MH Crisis-related data / information and commissions work now
to gather and assimilate relevant data / information from across the Devon public service system.
o Invites the CCG to consult with people and to return to the SG with a plan, making recommendations on all these points; those in the P&P slides; and funding / commercial arrangements.

Page 19 of 26
5. Piloting the MH Crisis ‘To Be’ VSM
Critical Success Factors
Criteria for assessing success in the pilot should include:
Proof of concept for a SUPOC reflected in increased confidence of all stakeholders in the MH Crisis pathway and active commitment of MH Crisis pathway stakeholder organisations to leading change.
GPs have increased confidence and competence for dealing with MH issues reflecting their pivotal role in identifying lower order MH issues and preventing escalation.
Improved patient experience reflecting tangible change in the extent to which MH issues are understood across the MH Crisis pathway (non-stigmatising / parity of esteem) and demonstrated through appropriate attitudes and response to MH crisis and associated issues.
Improvement in MH Crisis pathway capacity and competence for coping with intoxication.
Development of consistent, co-ordinated and effective ‘Crisis Response’ reflecting deep understanding of the nature and flow of demand across the MH Crisis pathway and alignment of appropriate resources in appropriate places.
Incorporating initiatives underway and delivered as part of the Crisis Care Concordat plan reflected in understanding what has been done, learning from effects of change and building on progress to improve the MH Crisis pathway.
Sustained reduction in use of S136 powers by Police officers based on appropriate use of powers and more effective support in responding to MH crisis.
Sustained reduction in demand on EDs based on appropriate migration of demand to other part of the MH Crisis pathway.
Development of a comprehensive performance management framework and approach underpinned by shared commitment to a set of performance measures that enable effective, continuous, improvement (Plan, Do, Check, Act). To include feedback from ‘Box 3’.
Planning & Preparation
It is a key assumption that a pilot would need to be ‘commissioned’ and that, in turn, would be informed by detailed planning and preparation including the following workstreams:
Pilot governance arrangements: o Steering Group. o Working Group. o Programme office purpose, role and capacity.
Pilot communications programme: o Stakeholder analysis. o Communications strategy – including public and patient involvement. o Communications plan – channels, media.
Scoping the pilot: o Geography. o Categories of demand. o Component functionality – to include information and communication systems.
Critical Success Factors and key performance measures
Performance management framework and processes: o Approach and methodology. o Performance reporting and analysis. o Benefits capture. o Continuous Improvement. o System Control.

Page 20 of 26
Defining data requirements and sources:
o Baseline current performance. o Defining a ‘control’ area – rest of Devon.
Defining resource requirements based on data analysis to inform: o Component capacity requirements. o Component capability requirements. o Job design.
Agreeing funding arrangements for pilot.
Capturing and recording learning.
Assumptions & Interdependencies
Key assumptions for planning and preparation include:
The timeline for planning and preparation is governed by the need to agree funding arrangements as part of budget setting processes for financial year 2016/17 that are currently underway. The aim is to be ready to start a pilot in April 2016.
Stakeholder organisations will be able to complete internal decision making processes and commit to supporting a pilot by the end of December 2015.
Stakeholder organisations will commit dedicated resource to planning and preparing for the pilot including data specialists.
Interdependencies for planning and preparation include:
Outputs of work completed and ongoing in delivering the Crisis Care Concordat plan.
Initiatives such as the ‘Integrated Care for Exeter’ (ICE) partnership.
Initiatives referred to in this report i.e. DPT and CAMHS ‘single points of contact’ and ‘referral hubs’.

Page 21 of 26
6. Appendices
Appendix 1 – ‘As Is’ VSM
Street triage
(advice,
intervention,
deployment)
Consult Police
data
Attend
No. of calls where
purpose is MH
crisis
Assess physical
and mental health
needs
Encounter in
public place
Check clinical
history
Physical health
emergency?
Yes
Assess physical
and mental health
needs Yes
Mental health
crisis?
No
Yes
Physical health
emergency?
Yes
Mental health
crisis?
Referral
Yes
Physical risk to
self or others?
Yes
Physical health
emergency?
Mental health
crisis?Consult CRHT
Yes
No
On caseload?
Yes
Gather and
evaluate
information
No
Need for
ambulance?
Affected by
alcohol /
drugs?
Yes
No
Yes
Call Ambulance
Need for
ambulance?Transfer to
Ambulance
Physical risk to
self or others?
Yes
Call Ambulance /
Police
No
Call Police
Yes
Physical health
emergency?
Mental health
crisis?
Yes
No
Transfer to
Hospital ED
Transport to
appropriate place
Telephone risk
assessment
111 service
MH professional
calls back
(Devon pilot)
Community Mental Health Team
No
Crisis Resolution & Home Treatment Team
No
Primary Health - GP
NoPrescribe / refer
for treatment
Police
Provide advice
Call Ambulance
Attend
Ambulance
No
Provide advice /
signpost
Transfer to
Hospital ED
No
Acute relapse plan
(Plymouth)
Emergency Duty TeamOut of Hours?
Se
rvic
e U
se
r; F
am
ily
me
mb
er;
Me
mb
er
of
Pu
blic;
Em
plo
ye
r e
tc
MHA
assessment?
MHA
assessment?Yes Yes
Gather and
evaluate
information
MHA
assessment? No
Yes
3rd sector
Crisis House
Samaritans
MIND
WAND
Rethink
Community Support
Organisation
Gather and
evaluate
information
Affected by
alcohol /
drugs?Co-ordinate S12
doctor / AMHP for
assessment
Complete MHA
assessment
Complete MHA
assessment
Detain?
MHA / MCA /
DOLs?
Primary Health – S12 doctor
Approved Mental Health Professional
Yes
No
Yes
No
Recovery plan
No
Follow up / referral
to ACP for
recovery plan
Transport to bed
Find available bed
Yes
Ambulance
Follow up / referral
to ACP for
recovery plan
No
Yes
Detain S136 in
police cell
Take to PoS /
HBPoS
Call Ambulance
Criminal
offence?
No
No further action
No
Detain S136
Take to PoS /
HBPoS
Refer to CRHT
No
The person
moves into
the ACP in a
controlled way
with a plan
supervised by
a competent
professional
The person moves
into a hospital
emergency
department to
address physical
and / or mental
health needs
No of referrals
where person
is known to MH
services
No of calls
requiring MH
professional
call back
Outcome of calls
Evaluation of
assessment
outcomes
Evaluation of
assessment
outcomes
The person I spoke to was really helpful and kind
Huge delays – people with immediate need often reach an answering service
The Crisis Team made my sense of crisis worse!
I found it difficult having them in my home – 3 people you do not know
Not recognised that people with mental
illness and drug / alcohol problem are
at serious risk - GPs / Psychiatrists
seem to think the person is at fault
Being ‘sectioned’ should not be a
humiliating experience and it often is
The MHA assessment – which is
intimidating – can cause symptoms
to escalateRoot cause
analysis – no. of
cases where a
social intervention
could have
prevented crisis
Lead time
VA time
Waiting time
No of
professionals
involved
Lead time
VA time
Waiting time
No of
professionals
involved
Where do GPs
go for help with
MH crisis?
How does one get help from
Crisis in a ‘crisis’? They tend
to hand off people like me
Crisis House –
‘Box 1’ or Box 2’?
Lead time
VA time
Waiting time
No of
professionals
involved
Lead time
VA time
Waiting time
No of
professionals
involved
GP data re people
suffering from depression,
on medication and / or
referred for psychological
assessment
When called, police explained
they could not resolve ‘crisis’
Police need to give assurance
to person – even if they are
cuffing them
Volume / source
of demand
involving MH
crisis, profiled by
day / time etc
It is often frightening to call the
police. They made me feel stupid
as if I was wasting their time
Pre-conceived opinions affected
Police handover – long wait in
A&E
Breakdown of
social factors
leading to
crisis in
Primary Care
and onwards
Volume / source
of demand
involving MH
crisis, profiled by
day / time etc
It is frightening to be in a
Police cell for very long
Conveyance post
assessment – who is
doing it and volume of
activity
Proportion of
demand involving
alcohol / drugs
Conveyance post
assessment – who is
doing it and volume of
activity
Volume / source of
demand
Outcomes

Page 22 of 26
The person leaves
the emergency
pathway in a
controlled way
with a plan
supervised by a
competent
professional
Psychiatric Liaison
Physical health
assessment /
triage
Mental health
matrix
(ED staff)
Hospital Emergency Department
Matrix output?
Refer to
psychiatric
liaison / CRHT
Refer to
psychiatric
liaison / wait in
Obs unit / ED
Discharge /
signpost support /
notify GP
Psychosocial
assessment / full
history
Red
Green
Amber /
Yellow
Detain S5(2)
waiting for MH
assessment
Informal
admission to
bed / psych bed
MHA assessment
Transport to bed
Care plan: care
coordinator /
signposting / rainy
day plan
Assessment
output?
ReferralSignpost to other
services
Co-ordinate S12
doctor / AMHP for
assessment
Complete MHA
assessment
Complete MHA
assessment
Detain? Find available bed
Crisis Resolution & Home Treatment Team
Community Mental Health Team
Primary Health – S12 doctor
Approved Mental Health Professional
Yes
No
Ambulance
Hospital Medical Wards
Refer to
psychiatric
liaison / CRHT
Referral
Gather and
evaluate
information
Recovery plan
Very kindly care offered at Torbay
ED after episode of self harm. Also
excellent nursing care that led to
psychiatric assessment
Clinicians not accessing previous MH history /
notes; not acknowledging extent of previous
self harm; transfer to inappropriate physical
ward
Medical staff on all wards to know
what Psychiatric Liaison does and how
to access it – it should not be the
responsibility of the person to ask
Lead time
VA time
Waiting time
No of
professionals
involved
Volume / source
of demand
involving MH
crisis, profiled by
day / time etc
Proportion of
demand involving
alcohol / drugs
Evaluation of
assessment
outcomes
Lead time
VA time
Waiting time
No of
professionals
involved
Root cause
analysis – no. of
cases where a
social intervention
could have
prevented crisis
Conveyance post
assessment – who is
doing it and volume of
activity
Chaotic spaces – no appropriate, calm
place to talk to Psychiatric Liaison
No appropriate place to talk to
Psychiatric Liaison – have been seen
in staff room where interrupted or at
bedside where there is no privacy
Time spent in A&E should be kept to a minimum –
especially when being watched by Police Officers
Lack of information sharing between
services leads to stigma
Lead time
VA time
Waiting time
No of
professionals
involved
Lead time
VA time
Waiting time
No of
professionals
involved

Page 23 of 26
Appendix 2 – ‘To Be’ VSM pre scenario testing
Consult Police
data
Speak to a MH
nurse / specialist
Assess physical
and mental health
needs
Encounter in
public place
Devon / Plymouth MH Crisis
High Level ‘To Be’ VSM draft
v0.3 03/07/15
Mental health
needs?
Yes
Yes
Physical health
needs?
Yes
Yes
Mental health
needs?
Yes
No
Physical health
emergency?
Output?
No
Yes Arrange
appropriate
conveyance to ED
Physical risk to
self or others?Yes
Call Police
Physical health
emergency?
Control room
receives call
Single, Unique Point of Contact Crisis Service
Primary Health
Prescribe / refer
for treatment
Police
Arrange
appropriate
conveyance to ED
Attend / Assess
situation
Ambulance
Warm transfers of call to
appropriate services i.e.
with relevant background
info and systems access
No
Intoxication Support Unit
Convey person to
ISU
Keep safe until fit
for assessment
Complete F2F
assessment Output?
Output?
Structured conversation:
- physical health?
- mental health?
- affected by alcohol; drugs;
other substances?
- in a safe, appropriate
place?
- wider social needs?
- known to MH services
(now and / or in the past)?
Output?
Conversation
meets need
Refer / signpost to
other services e.g.
Crisis House?
Refer to Crisis
service
Refer to ISU
Arrange
conveyance
Request MHA
assessment
Update systems
Advise GP / others
No further action
Refer / signpost to
other services e.g.
Crisis House?
Request MHA
assessment
Refer to Home
Treatment /
Inpatient services
Devon geography;
response times
Alignment with
concept of Street
Triage?
Skills, knowledge
required
Access to
information
systems
Capacity, capability,
confidence in assessing
moderate MH needs
Refer to CMHT
Co-ordinate S12
doctor / AMHP for
assessment
Complete MHA
assessment
Complete MHA
assessment
Output?
Find available bed
Primary Health – S12 doctor
Approved Mental Health Professional
Detain
Refer to other
services
Need for behaviour change if
demand on Police resources
is to reduce sustainably
Provision of appropriate
conveyance
No further action
Provide advice /
guidance
Convey person to
ISU
Convey person to
HB PoS
Convey person to
ED
Arrest / Detain
s136 etc
No further action
Provide advice /
guidance
Convey person to
ISU
Convey person to
HB PoS
Health Based Places of
Safety – officers having to
make several calls to
ascertain status / access
Physical &
Mental health
needs?
Advise Psychiatric
Liaison if person
being conveyed to
ED
Assess situation
Mental health
needs?
Physical health
needs?
Physical &
Mental health
needs?
Offence
committed?
Physical risk to
self or others?
Yes
Attend?
Yes
Physical health
needs?
Physical health
emergency?
Yes
Yes
Yes
Yes
Call paramedics
Physical &
Mental health
needs?Yes
Convey person to
ED
Yes
Sources of contact:
People experiencing / anticipating
MH crisis
Family members / carers
Care organisations - residential;
domiciliary; general; specialist
Friends
Members of the public
3rd sector / community
organisations
Workplace colleagues / managers
Social services – children;
adolescents; adults; older people
Workplace colleagues / managers
Schools

Page 24 of 26
The person leaves
the emergency
pathway in a
controlled way
with a plan
supervised by a
competent
professional
Psychiatric Liaison
Physical health
assessment /
triage
Mental health
screening
(ED staff)
Hospital Emergency Department
Matrix output?
Refer to
psychiatric
liaison / CRHT
Refer to
psychiatric
liaison / wait in
Obs unit / ED
Discharge /
signpost support /
notify GP
Psychosocial
assessment / full
history
Red
Green
Amber /
Yellow
Detain S5(2)
waiting for MH
assessment
Informal
admission to
bed / psych bed
MHA assessment
Transport to bed
Care plan: care
coordinator /
signposting / rainy
day plan
Assessment
output?
Refer to CRHT
Discharge / refer
to community MH
services
Signpost to other
services
Co-ordinate S12
doctor / AMHP for
assessment
Complete MHA
assessment
Complete MHA
assessment
Detain? Find available bed
Crisis Resolution & Home Treatment Team
Community Mental Health Team
Primary Health – S12 doctor
Approved Mental Health Professional
Yes
No
Ambulance
Devon / Plymouth MH Crisis
High Level ‘To Be’ VSM draft
v0.3 03/07/15
Redesign to be addressed in
separate workshop

Page 25 of 26
Appendix 3 – updated ‘To Be’ VSM post scenario testing
Mental Health Act Assessment
Consult Police
data
Speak to a MH
nurse / specialist
Assess physical
and mental health
needs
Encounter in
public place
Devon / Plymouth MH Crisis
High Level ‘To Be’ VSM draft
v0.7 20/10/15
Mental health
needs?
Yes
Yes
Physical health
needs?
Yes
Yes
Mental health
needs?
Yes
No
Physical health
emergency?
Output?
No
Yes Arrange
appropriate
conveyance to ED
Physical risk to
self or others?Yes
Call Police
Physical health
emergency?
Control room
receives call
Single, Unique Point of Contact
Crisis Response
Primary Health
Prescribe / refer
for treatment
Police
Arrange
appropriate
conveyance to ED
Attend / Assess
situation
Ambulance
Need to define requirements
for communications systems
to enable and support ‘warm
transfers’ of calls to
appropriate services.
No
Intoxication Support
Output?
Structured conversation:
- age; gender etc
- physical health?
- mental health?
- affected by alcohol; drugs;
other substances?
- in a safe, appropriate
place?
- wider social needs?
- known to MH services
(now and / or in the past)?
- evaluate need
- decide appropriate
response
Output?
Conversation
meets need
Refer / signpost to
other services
Initiate Crisis
Response
Arrange
conveyance
Request MHA
assessment
Update systems
Advise GP / others
Data requirements to baseline current demand categories / volumes /
profiles
Need to design range of
protocols for dealing with
wide range of demand.
Need to define content
and tone of
conversations.
Need to define range of
‘appropriate responses’.
Need to define range of
skills, knowledge and
experience required – job
design.
Need to define
requirements for access to
information systems.
Need to support development of
competence and confidence of
GPs in assessing MH needs.
Refer to CMHT
Co-ordinate S12
doctor / AMHP for
assessment
Complete MHA
assessment
Complete MHA
assessment
Output?
Find available bed
Primary Health – S12 doctor
Approved Mental Health Professional
Detain
Refer to other
services
Need to support and enable
sustained reduction in
inappropriate use of S136Need to define policy and
protocols relating to provision
and use of ‘appropriate
conveyance’.
No further action
Provide advice /
guidance
Convey person to
HB PoS
Convey person to
ED
Arrest / Detain
s136 etc
No further action
Provide advice /
guidance
Convey person to
ED / HB PoS etc
HB PoS – need to provide
officers with information on
status / capacity
Physical &
Mental health
needs?
Advise ED /
Psychiatric Liaison
if person being
conveyed to ED
Assess situation
Mental health
needs?
Physical health
needs?
Physical &
Mental health
needs?
Offence
committed?
Physical risk to
self or others?
Yes
Attend?
Yes
Physical health
needs?
Physical health
emergency?
Yes
Yes
Yes
Call paramedics
Physical &
Mental health
needs?Yes
Convey person to
appropriate place
(including ED)
Yes
People experiencing / anticipating
MH crisis
Family members / carers / friends
Care organisations
Members of the public 3rd sector / community
organisations
Workplace colleagues / managers
Social services – children;
adolescents; adults; older people
Schools / Colleges / Universities
PDCA
Plan
Do
Check
Act
Evaluate effectiveness of support
and guidance to GPs etc
PDCA
Plan
Do
Check
Act
Evaluate effectiveness of
assessment and output
PDCA
Plan
Do
Check
Act
PDCA
Plan
Do
Check
Act
Evaluate effectiveness of
assessment, appropriate
response and decision
making
Refer to CAMHS
Yes
PDCA
Plan
Do
Check
Act
Evaluate opportunity to
migrate demand to most
appropriate point of contact
Need for
conveyance?
Yes
Evaluate effectiveness of
assessment and output
Need to define policy and
protocols relating to provision
and use of ‘appropriate
conveyance’.
Speak to a ‘call
handler’Need to evaluate need and impact of
having ‘call handlers’ to address needs
for information / non-MH Crisis cals.
Need to support development of
competence and confidence of
paramedics in assessing MH
needs.
Need to align / integrate
purpose and function of
SUPOC with:
- DPT single point of contact
- CAMHS referral hubs /
single point of contact
Need to consider alignment /
integration of purpose and
function of SUPOC with:
- Emergency Duty Teams
- Street Triage
- MASH
Need to support development of
competence and confidence of
Police officers in assessing MH
needs.
See Scenario Testing outputs re failure modes.
Need to collect and analyse data relating to demand requiring ‘Crisis Response’: Sources of demand Profile of demand Points at which demand arises Range of responses required
Feed in to design of policy and capacity planning around ‘Crisis Response’ at appropriate points in the ‘To Be’ MH ACP VSM.
See Scenario Testing outputs re failure modes.
Need to collect and analyse data relating to intoxication and MH Crisis.
Need to review policy and define options for providing ‘Intoxication Support’ at appropriate points in the ‘To Be’ MH ACP VSM including who is responsible for making decision re fitness for MH assessment.

Page 26 of 26
Mental Health Act Assessment
The person leaves
the Crisis element
of the ACP in a
controlled way
with a plan
supervised by a
competent
professional
Psychiatric Liaison
Physical health
assessment /
triage
Mental health
screening
(ED staff)
Hospital Emergency Department
Matrix output?
Refer to
psychiatric
liaison / CRHT
Refer to
psychiatric liaison
Discharge /
signpost support /
notify GP
Psychosocial
assessment / full
history
Red
Green
Amber /
Yellow
Detain S5(2)
waiting for MH
assessment
Informal
admission to
bed / psych bed
MHA assessment
Transport to bed
Care plan: care
coordinator /
signposting / rainy
day plan
Assessment
output?Refer to CRHT
Discharge / refer
to community MH
services
Signpost to other
services
Co-ordinate S12
doctor / AMHP for
assessment
Complete MHA
assessment
Complete MHA
assessment
Detain? Find available bed
Crisis Resolution & Home Treatment Team
Community Mental Health Team
Primary Health – S12 doctor
Approved Mental Health Professional
Yes
No
Ambulance
Provision of appropriate
conveyance
Immediate
response?
Yes
NoMove to a safe
place in / near ED
Need to review protocols / processes
to enable Police officers / Paramedics
to provide ED with information relating
to MH needs ahead of arrival.
Need to review protocols / processes
to enable ED staff to provide ‘Crisis
Response’ to MH needs
PDCA
Plan
Do
Check
Act
Continuous Improvement:
Need to establish a series of feedback
loops - from ‘Box 3’ - that enable
ongoing evaluation of system
effectiveness and adjustment to policy /
process.
PDCA
Plan
Do
Check
ActEvaluate effectiveness of
assessment and output
PDCA
Plan
Do
Check
Act
Evaluate effectiveness of
assessment and output
Devon / Plymouth MH Crisis
High Level ‘To Be’ VSM draft
v0.7 20/10/15
Data requirements to baseline current demand categories / volumes /
profiles
Crisis Response
Intoxication Support
See Scenario Testing outputs re failure modes.
Need to collect and analyse data relating to demand requiring ‘Crisis Response’: Sources of demand Profile of demand Points at which demand arises Range of responses required
Feed in to design of policy and capacity planning around ‘Crisis Response’ at appropriate points in the ‘To Be’ MH ACP VSM.
See Scenario Testing outputs re failure modes.
Need to collect and analyse data relating to intoxication and MH Crisis.
Need to review policy and define options for providing ‘Intoxication Support’ at appropriate points in the ‘To Be’ MH ACP VSM including who is responsible for making decision re fitness for MH assessment.
Recommended