MiniReview
Development of Clinical Pharmacology as a Medical Speciality inEurope – The Roles of WHO, IUPHAR and EACPT
Folke Sj€oqvist
Division of Clinical Pharmacology, Department of Laboratory Medicine, Karolinska Hospital, Huddinge, Stockholm, Sweden
(Received 23 May 2014; Accepted 26 May 2014)
Abstract: This MiniReview shows that both WHO and IUPHAR very early recognized that there is a gap between the availabil-ity of academic expert knowledge in pharmacology and its utilization in health care. Many initiatives have been taken to bridgethis gap, but still 12 European countries do not recognize clinical pharmacology as a medical speciality because the professionhas failed to develop defined functions in patient care. A first priority for EACPT therefore ought to be to promote clinical phar-macology as a medical speciality recognized by the European Union. The pharmacological services listed in Table 7 that focuson drug problems agree well with those that were recently prioritized in the IUPHAR/WHO/CIOMS manifesto to correct a majorweakness in the health care of today in order to promote rational use of drugs.
Clinical pharmacology has now existed as a teaching andresearch discipline for nearly 50 years, but with notable excep-tions, it is not yet established in many countries as a medicalspeciality. This MiniReview describes the attempts of IU-PHAR, WHO and EACPT to involve clinical pharmacologyin the global efforts to improve the use of medicines towardsincreased efficacy and safety. The MiniReview emphasizes thesituation in Europe.
The Role of WHO
Farsighted pharmacologists realized that clinical pharmacologyhad to reach out to the bedside in order to develop and there-fore initiated discussions with WHO on this matter. In Decem-ber 1969, WHO brought together a group of experts to outlinea report on the scope, organization and training of clinicalpharmacology [1]. The group was led by the late Sir DerrickDunlop (UK), and with the late professors Louis Lasagna(USA), Franz Gross (Germany) and Leon Goldberg (USA) asmembers. Participants who are still alive include L. Dettli,Switzerland, C.T. Dollery, UK and F. Sj€oqvist, Sweden.WHO was represented by professor Hans Friebel, Dr. H. Hal-bach, Dr. T.L. Chrusciel and the temporary adviser professorDesmond Laurence, London. The report concluded that thefunctions of clinical pharmacology should be:
to improve patient care by promoting the safer and moreeffective use of drugs;
to increase knowledge through research;to pass on knowledge through teaching and,to provide services, such as drug information, drug analy-sis, the monitoring of drug abuse and advice on the experi-mental design of clinical drug studies.
It was said that all these functions should in fact serve toenhance benefit–cost ratios of drugs. The first function is aprelude to the WHO priority of today ‘Rational Use of Medi-cines (RUM)’.Another important step in the development of clinical phar-
macology took place in Oslo the same year where a WHODrug Consumption Group was formed [2]. The methodologyfor international comparisons of the use of drugs was discussedand the WHO Drug Utilization Research Group (DURG) wasborn. A common drug classification and a common unit formeasuring drug consumption (the defined daily dose, DDD)was introduced permitting valid comparisons of prescribinghabits within and between countries [3,4]. The transit fromclassical clinical pharmacological studies such as drug trialsand pharmacokinetics to pharmacoepidemiology had then beentaken, and it is eloquently described in the WHO publicationDrug Utilization Studies edited by Graham Dukes [5].In 1977, WHO published its first list of essential drugs [6].
For many years, pioneers in clinical pharmacology were thedriving forces in the expert committees making these selec-tions, Daniel Azarnoff, Per Knut Lunde, Iwan Darmansjah,D.R. Laurence, Marcus Reidenberg and Gianni Tognoni tomention a few. It is clear, not the least from a review by Tog-noni and Lunde [7], that the idea had its origin from academicpharmacology. As an example, national drug lists based onclinical pharmacological evaluations of the therapeutic arma-mentarium were introduced in Scandinavia already in the mid
Author for correspondence: Folke Sj€oqvist, Division of Clinical Phar-macology, Department of Laboratory Medicine, Karolinska Hospital atHuddinge, S-141 86 Stockholm, Sweden (e-mail [email protected]).This is an invited MiniReview in recognition that Folke Sj€oqvist hasbeen awarded the 2013 BCPT Nordic Prize in Basic & Clinical Phar-macology & Toxicology.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
Basic & Clinical Pharmacology & Toxicology, 2014, 115, 172–178 Doi: 10.1111/bcpt.12278

1960s. Provided that such are well communicated, they mayhave a major impact on prescribers with up to 90% adherenceto the recommendations issued [8,9]. This series of WHOtechnical reports has now published the 17th Model list ofEssential Medicines and still clinical pharmacologists play animportant role in the selection process.During the next decades, clinical pharmacology developed
because of the medical need to establish in scientific terms thebenefits of drug therapy relative to its risks. A WHO WorkingGroup on Clinical Pharmacology in Europe was formed in1983 and its recommendations were summarized in threepapers in Eur. J. Clinical Pharmacology during 1988 [10–12].Clinical pharmacology was described as an indispensable partof the health service and considered to be important both inhospitals and primary health care. Services included patientcare directly in general medicine (drug problem-oriented con-sultations) or more indirectly through pharmacotherapeuticrounds and sessions. The roles in drug information and in for-mulary committees, clinical trials, drug utilization surveys andmonitoring of adverse drug reactions were underlined as wellas therapeutic drug monitoring.In 1990, WHO headquarter in Geneva (Drs V. Fattorusso
and J. Dunne) organized an informal meeting to discuss therole of clinical pharmacology in public health. The meetingtook place 20 years after the initial WHO study group met inGeneva and 5 years after the Nairobi conference on theRational Use of Drugs. It was agreed that clinical pharmacol-ogy had developed from being product-oriented to becomepatient-orientated and society-orientated. The discrepancybetween the need for and the availability of clinical pharma-cologists in health care had increased. It was underlined thatthe roles of clinical pharmacology and the new discipline clin-ical pharmacy were complementary and that collaborationbetween the two should be encouraged. Clinical pharmacolo-gists should be involved in the teaching about rational druguse at all levels. The proceedings of this meeting were notpublished.In 1991, WHO Europe in Copenhagen put together a book-
let with the three papers mentioned above dealing with theroles of clinical pharmacology in teaching, research and healthcare [13]. The WHO team consisted of Graham Dukes, LeoOfferhaus and Inga Lunde. The potential usefulness of the dis-cipline for the rational use of medicines (RUM) in primaryhealth care was emphasized. The booklet contains reports from21 European countries. A few countries reported that clinical
pharmacology now was established as an academic disciplineat all medical schools (Denmark, Finland, France, Germany,Norway, Sweden, Switzerland and UK), while most countriesconsidered that services in clinical pharmacology in healthcare were poorly developed or lacking.There are other examples from this time of mutually fruitful
collaboration between European clinical pharmacology andWHO such as the international cooperation in drug surveil-lance summarized in a CIOMS conference 1993 [14] and thebooklet Introduction to Drug Utilization Research 2003 [15].During the coming years, attempts were made to convince
WHO about the need to update the recommendations from1970. Finally, these efforts resulted in a joint publication fromWHO, CIOMS and IUPHAR in 2013 [16], which was a modi-fication of an IUPHAR paper from the previous year [17]. Adriving force within WHO in this important development wasProfessor Lembit R€ago.Recently, WHO (Richard Laing) and European drug experts
(on the initiative of Lars Gustafsson, Sweden) met to discussthe interface management of pharmacotherapy, particularly thecollaboration between hospitals and primary health care [8].The roles of WHO in the development of clinical pharma-
cology are summarized in Table 1.
The Role of IUPHAR
The International Union of Pharmacology (IUPHAR) wasfounded in 1965 after a decision in IUPS (International Unionof Physiological Sciences) to approve that its Section on Phar-macology formed an independent union [18]. In the forthcom-ing world congresses in pharmacology, due attention was paidto the developments in clinical pharmacology.An important step towards the formation of a Section of
Clinical Pharmacology within IUPHAR was taken in May1973. In a proposal to Arnold Burgen, president of IUPHAR,three clinical pharmacologists (Colin Dollery, UK, Dan Azar-noff, USA and Folke Sj€oqvist, Sweden) suggested that aninterim commission on clinical pharmacology should beformed. It was supposed to map out training sources for clini-cal pharmacologists in different countries, survey drug usageand response in different parts of the world, the latter includ-ing genetic and environmental differences in drug response. Itshould also evaluate the effectiveness of clinical pharmacologyin relation to healthcare delivery and the provision of druginformation by means of bias-free education of prescribing
Table 1.The role of WHO in developing clinical pharmacology.
Year Important event
1969 WHO study group on Clinical Pharmacology Scope, Organization, Training [1] meets in Gen�eva1969 WHO Drug Consumption group formed in Oslo [2]1977 The first list of essential drugs published by WHO [6]1983 The WHO Working Group on Clinical Pharmacology in Europe formed [9]1990 Informal consultation in clinical pharmacology and its relevance to public health held in Geneva1991 Clinical Pharmacology. The European Challenge was published [12]1993 Drug Utilization studies, Methods and Uses published by WHO [5]2013 Clinical Pharmacology in health care, teaching and research. WHO/IUPHAR/CIOMS joint publication [16]
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
MiniReview CLINICAL PHARMACOLOGY IN EUROPE 173

doctors. Already this early proposal emphasized the role ofclinical pharmacology in health care.The following year, IUPHAR decided to form a Section of
Clinical Pharmacology, which was formally established at theSixth World Conference in Pharmacology in Helsinki 1975.Colin Dollery became its first chairman. About 300 clinicalpharmacologists attended this meeting, bylaws were acceptedand an advisory board appointed with members from Ger-many, Hungary, India, Sweden, UK and USA.Important meetings with the executive board aiming to
strengthen the Section were held in Deer Lodge, Montana,1977, and in London 1978. The suggestion to organize thefirst World Conference in Clinical Pharmacology and Thera-peutics was made in 1977 and received with hesitation amongbasic pharmacologists but finally held in London in 1980. Themajor aim was to promote contacts between clinical pharma-cologists throughout the world.A visionary meeting for that purpose was held at the Royal
Society of Medicine in London on 6 August 1980. Briefreviews of the status of clinical pharmacology were given by20 experts from Africa, Asia, Australia, Europe and NorthAmerica and common goals of the discipline were outlined.Many of these pioneers left typed or handwritten notes of theircomments in my hands (as organizer of the meeting). My ownmentor Lou Lasagna stressed the importance of certification ofthe clinical pharmacologist and that teaching of clinical phar-macology must be obligatory at all medical schools, condi-tions that still are not fulfilled in USA. Similarly to his NorthAmerican colleague, Dick Ogilvie, Canada, reported about thedifficulties to recruit clinical pharmacologists in the absence ofcareer posts in the health service.Optimistic reports about the academic developments in Eur-
ope were presented by Denis McDevitt, UK and Per KnutLunde, Norway, regions where clinical pharmacology now iswell established as a medical speciality. In retrospect, it isinteresting to note the pessimistic predictions of AndrewSchaepdryver, Belgium, Harry Wesseling, the Netherlands, C.Sirtori, Italy, and Pierre Simon, France, countries where clini-cal pharmacology still has difficulties to reach out in thehealthcare system. Developing countries were well representedwith reports from India (R.C. Saxena), Africa (K. Adjepon-Yamoah, Ghana) and Barbados (H. Fraser).At this meeting, it was emphasized that the training of other
medical specialists in clinical pharmacology may be equally asimportant as recruiting clinical pharmacologists in the effortsto rationalize drug treatment. As an example, a great numberof internists, psychiatrists and paediatricians have beeninvolved in clinical pharmacological research and now act asambassadors of the discipline.One session of the meeting was devoted to drug problems
in developing countries (drug evaluation, drug promotion) andintroduced by Dr. Halfdan Mahler, director general of WHO.Three years experience of the WHO essential drug conceptwas discussed by P.K. Lunde, Norway, Gianni Tognoni, Italy,and N.D.V. Lionel, Sri Lanka.In 1983, the first two secretaries of the Section of Clinical
Pharmacology, Dan Azarnoff and Per Knut Lunde, put together
the first global list of persons active in the discipline. Contactpersons were identified in 60 countries and many on that listlater became national leaders in clinical pharmacology.Subsequent world conferences in clinical pharmacology were
held in Washington (1983), Stockholm (1986), Heidelberg-Mannheim (1989), Yokohama (1992), Buenos Aires (1996),Florence (2000), Brisbane (2004) and Quebec City (2008).The section of clinical pharmacology continuously increased
its activities and was promoted to a Division within IUPHARin 1996 with Folke Sj€oqvist as the first chairman and threerepresentatives in the executive committee of IUPHAR.In 2003, a proposal from the Clinical Division to broaden
the name of IUPHAR to the International Union of Basic andClinical Pharmacology was accepted after rather lengthy dis-cussions, but the idea was supported by some renowned phar-macologists including two former presidents of IUPHAR,B€orje Uvn€as, Sweden, and Colin Dollery, UK, and two NobelLaureates, Sir John Vane and Sir James Black. The decisionwas ratified at the IUPHAR congress in Beijing 2006. As aresult, it was decided to ask Kim Brøsen to arrange the firstjoint world congress in basic and clinical pharmacology inCopenhagen in 2010.The development of clinical pharmacology as a scientific
discipline during the first 75 years was reviewed by ColinDollery in 2006 [19]. He pointed out that European clinicalpharmacology had originated either from internal medicine orbasic pharmacology but that the two schools now had reachedconsiderable convergence.At the congress in Copenhagen, IUPHAR had composed a
50-year anniversary issue of its journal Pharmacology Interna-tional, where the CP division summarized its efforts toimprove the use of drugs worldwide [20]. It was mentionedthat between 1977 and 1983, several board members had par-ticipated and in some cases chaired the early expert commit-tees on the selection of essential drugs. Moreover, CPT worldconferences from the beginning of 1980 had devoted sessionsto the rational use of medicines. In this issue, the clinical divi-sion also presented its activities towards better use of medi-cines in children [21].During 2010, IUPHAR published its position paper entitled
‘Clinical Pharmacology in Research, Teaching and HealthCare’ [15]. It emphasized that research in clinical pharmacol-ogy often is a multidisciplinary effort involving collaborationwith other academic disciplines such as biochemistry, genetics,statistics, epidemiology and other pharmaceutical sciences.However, in clinical services aimed to improve the use ofdrugs in patients, the clinical pharmacologist has to stand onhis/her own feet relying on a full-fledged medical training.The position paper outlines the research domains in clinical
pharmacology and the fundamentals in teaching of the disci-pline. A model core curriculum is included for clinical phar-macology, therapeutics and prescribing for medical studentsbuilding on the experiences in Scotland by Simon Maxwell[22]. The near relationship between pharmacological knowl-edge and drug prescription is emphasized. Some years previ-ously, an embryo for a global curriculum was developed[23,24].
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
174 FOLKE SJ€OQVIST MiniReview

In another addendum, a model curriculum for medical spe-cialization in clinical pharmacology is outlined with referencesto curricula in European and non-European countries. Trainingto reach competence in the clinical pharmacology serviceslisted in Table 2 is emphasized.Key clinical pharmacological services suggested by
IUPHAR are listed in Table 2, but not in any particular orderas their importance may vary between countries. The listshows the limitless possibilities for the medical specialityclinical pharmacology to play an important role in patientcare.The major IUPHAR decisions about clinical pharmacology
are summarized in Table 3.
Joint Efforts of WHO, CIOMS and IUPHAR
The position paper from IUPHAR regarding clinical pharma-cology [17] was well received internationally and evoked theinterest of both WHO and CIOMS (The Council for Interna-tional Organizations of Medical Sciences). Both organizationsdecided to reedit the document to a joint publication withIUPHAR emphasizing the roles of the discipline in health careeven more [16]. This manifesto clearly distinguishes betweenits roles as an interdisciplinary science and as a medicalspeciality with responsibility to improve the utilization ofmedicines in health care. Leading pharmacological journalshave supported the manifest [25,26].
For the first time, the discipline has an internationallyagreed dynamic definition as follows:
Clinical pharmacology is the scientific discipline thatinvolves all aspects of the relationship between drugs andhuman beings. Its breadth includes the development ofnew drugs, the application of drugs as therapeutic agents,the beneficial and adverse effects of drugs in individualsand society and the deliberate misuse of drugs. Clinicalpharmacology is a science that may be of significant inter-est to a variety of professions including physicians, phar-macists, nurses and scientists in many different disciplines.The term ‘clinical pharmacologist’ is also used in a profes-sional sense to refer to those physicians who are specialistsin clinical pharmacology. They have usually undertakenseveral years of postgraduate training focusing on impor-tant aspects of clinical pharmacology including clinical tri-als theory, drug evaluations, pharmacoepidemiology,pharmacoeconomics, pharmacogenetics, pharmacovigilanceand clinical drug toxicology. Such clinical pharmacologistshave as their primary goals that of improving patient care,directly or indirectly, by promoting the safer and moreeffective use of drugs.
The Role of EACPT
The growth of clinical pharmacology in Europe was stimu-lated by an initiative taken by Pierre Bechtel, Besancon, which
Table 2.Service functions for clinical pharmacologists in health care (from 16).
Critical drug evaluation of new and old drugsParticipation in Drug and Therapeutics Committees (DTC:s)Pharmacoepidemiological services from providing statistics on drug utilization to pharmacoepidemiological surveysDrug information services aimed to evaluate drug problems in individual or groups of patientsServices in pharmacovigilance, responsibility for ADR reportingContinuing medical educationTherapeutic drug monitoring (TDM) and pharmacogenetic services (phenotyping and genotyping of drug metabolizing enzymes, transportproteins and receptors)
Measurement of drug concentrations for the diagnosis and prevention of drug abuseOther toxicological servicesDirect patient services for the evaluation of drug-related problems such as therapeutic failures, ADR:s, drug interactions and inappropriatepolypharmacy
Electronic Pharmacological (e-Pharmacological) services such as evidence-based databases for rational drug prescribing
Table 3.Development of clinical pharmacology in IUPHAR.
Year Important decisions
1965 The International Union of Pharmacology (IUPHAR) is founded1973 Decision to form a Section of Clinical Pharmacology within IUPHAR1975 Section of Clinical Pharmacology established at the IUPHAR congress in Helsinki1977 Suggestion to organize the First World Congress in Clinical Pharmacology1980 First World Congress in Clinical Pharmacology in London (chaired by prof. Collin Dollery)1983 First global list of clinical pharmacological societies, sections and contact persons1996 Division of Clinical Pharmacology formed in IUPHAR2003 Proposal to change the name of IUPHAR to International Union of Basic and Clinical Pharmacology2006 The proposal above is ratified in Beijing2010 First joint World Conference in Basic and Clinical Pharmacology in Copenhagen (prof. Kim Brøsen)2010 Position paper ‘Clinical Pharmacology in Research, Teaching and Health Care’ published [15]
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
MiniReview CLINICAL PHARMACOLOGY IN EUROPE 175

led to a European collaboration to define criteria for thechoice and definition of healthy volunteers and patients instudies on drug development. This included the exploration ofgenetic and environmental factors explaining interindividualdifferences in drug disposition [27]. The project was acceptedas a COST concerted action in late 1985, and in 1989 [27], 11countries were involved (Denmark, Finland, France, FederalRepublic of Germany, Ireland, Norway, Spain, Sweden,Switzerland and the United Kingdom). In 1998, Bechtel andGunnar Alvan summarized the 12 years of fruitful collabora-tion [28].The WHO Regional Publication from 1991 [13] revealed
several shortcomings in the development of clinical pharma-cology in Europe with surprising differences between coun-tries. The report led to the insight that there was a need for aEurope-wide organization whose primary aim should be topromote the overall development of the discipline in theregion. The idea was enhanced by the political developmentsin Europe with colleagues in East and West Europe comingcloser to each other.The proposal to create a European association was first dis-
cussed in Frankfurt and Paris 1991 and further developed atthe IUPHAR congress in Yokohama in July 1992 where repre-sentatives from France, Germany, Italy, Norway, Spain, Swe-den and UK participated. At the follow-up meeting in Paristhe same year, organized by George Cheymol, the aims of theassociation were outlined. EACPT was then founded in Vero-na in March 1993. At this meeting organized by GiampaoloVelo, statues and aims of EACPT were agreed upon and latergiven legal credibility in European law through legal officersin Germany [29]. Other pioneers at these early meetingsincluded P. Bechtel and P. Jaillon (France), H. Dengler, J. Ku-hlmann and N. Rietbrock (Germany), J.R. Laporte (Spain),P.K.M. Lunde (Norway), M. Orme (UK) and F. Sj€oqvist(Sweden). The history of EACPT during the first 10 years hasbeen documented by Jochen Kuhlmann, Wuppertal, in anunpublished booklet ‘10 years EACPT 1993–2003’. Sincethen, the policy of EACPT has been to recruit colleagues fromall European countries to joint efforts aiming to improve theuse of drugs in health care. The chairpersons have been cho-sen from different countries, in chronological order Sweden(F. Sj€oqvist), Italy (G. Velo), UK (M. Orme), Germany, (I.Cascorbi) and now Spain (G. Calvo-Rojas). The intention is toincrease the input from Eastern European countries.In the early 1990s, IUPHAR had already taken initiatives to
improve the contacts between Eastern and Western Europeanclinical pharmacologists. An exchange programme between UKand Sweden with three Eastern European countries, Bulgaria,Hungary and Estonia, was financed and organized in April1993. This programme has had great importance for the recruit-ment of Eastern European clinical pharmacologists to EACPT.A fundamental idea with the founding of EACPT was to
make the discipline much more visible in health care. This isevident from several of the aims in the statutes:
promoting the utilization of clinical pharmacological ser-vices in healthcare delivery.
improving and harmonizing the teaching of the rational useof drugs at both undergraduate levels.contributing with clinical pharmacological expertise to pol-icy decisions regarding drug regulation in Europe.arranging scientific meetings, workshops and courses inclinical pharmacology and therapeutics in Europe.utilizing the skills of clinical pharmacology and therapeu-tics in counteracting misuse of prescription drugs and otherchemical substances.promoting problem-oriented and patient-oriented druginformation for physicians and other health professionals.increasing the input of clinical pharmacological skills inthe clinical evaluation of drugs.promoting high professional standards in drug prescribing.promoting high ethical standards in clinical drug research.enabling individual countries to benefit from the diversifi-cation of clinical pharmacology and therapeutics in Europe.encouraging collaboration with other agencies interestedin clinical pharmacology and therapeutics (e.g. WHO,IUPHAR, EEC).
The first European Congress in clinical pharmacology washeld in Paris in 1995 with George Cheymol as president. Sub-sequent congresses have been arranged every second year. Acombined IUPHAR/EACPT congress was organized byGiampaolo Velo in Florence in 2000 (Table 4). This idea tohave joint congresses in basic and clinical pharmacology aroseanew in 2010.EACPT initiated a new inventory of the discipline in 1999
by publishing A Guide to Training in Clinical Pharmacologyin Europe edited by Kim Brøsen, Odense [30]. About 100training programmes in 28 countries were described. A mapof the academic units of clinical pharmacology in each countrywas presented together with a brief review of the status of thediscipline. A much more positive pattern of the progress ofclinical pharmacology emerged compared to 1991. The overallimpression was that clinical pharmacology had reached out tomost medical schools in Europe fulfilling its obligations inteaching and research, while the roles in health care still werevaguely defined in some countries.The most recent attempt to compare the developments of
clinical pharmacology in different European countries wasmade in 2011–2012 by Orme and Sj€oqvist [31]. A question-naire was sent to the senior delegate of each of the 31 membercountries on the Council of EACPT containing key questionsabout the present standing of the discipline. Based on the resultsof the completed survey forms (100% response rate), clinicalpharmacology is recognized as an academic discipline in teach-ing and research in 28 of the 31 countries but as a medical spe-ciality in only 22 countries. In 50% of the countries whereclinical pharmacology is recognized as a medical speciality, thisrecognition has occurred more than 30 years ago. The trainingof clinical pharmacologists in terms of years after internshipvaries between the countries. In 8 countries, the training is pre-dominantly in internal medicine with shorter periods in pharma-cology. In 11 countries, the training is predominantly in clinicalpharmacology, and in 6, there is dual training [31].
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
176 FOLKE SJ€OQVIST MiniReview
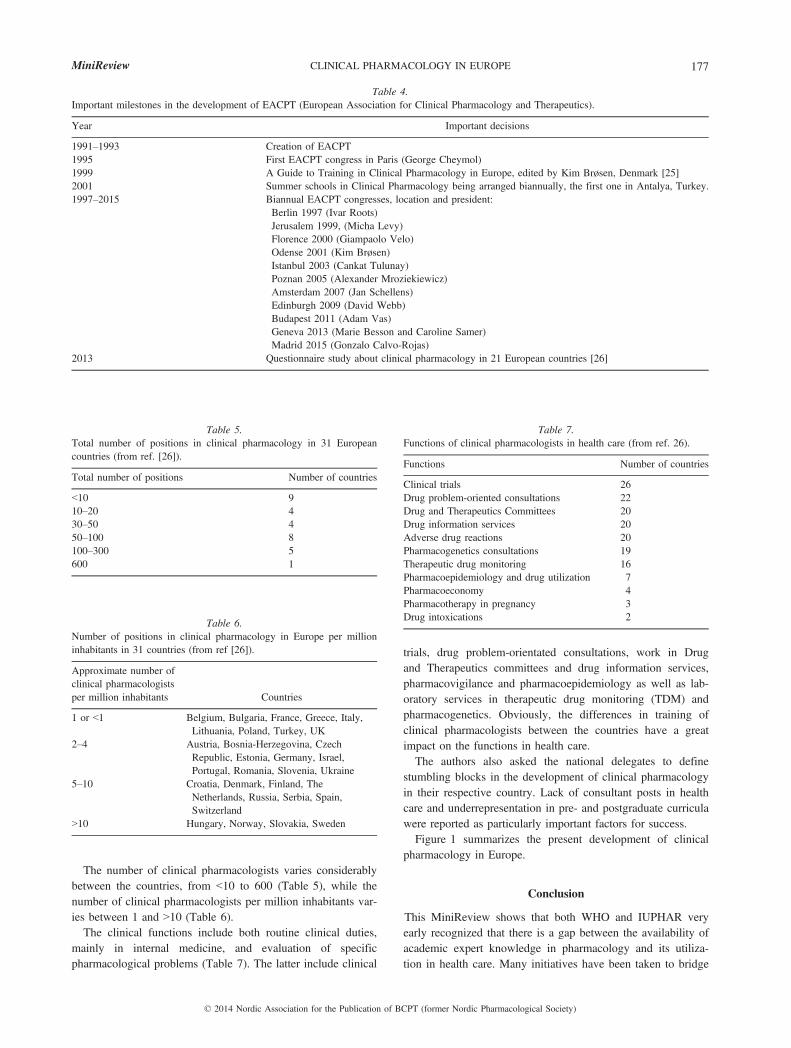
The number of clinical pharmacologists varies considerablybetween the countries, from <10 to 600 (Table 5), while thenumber of clinical pharmacologists per million inhabitants var-ies between 1 and >10 (Table 6).The clinical functions include both routine clinical duties,
mainly in internal medicine, and evaluation of specificpharmacological problems (Table 7). The latter include clinical
trials, drug problem-orientated consultations, work in Drugand Therapeutics committees and drug information services,pharmacovigilance and pharmacoepidemiology as well as lab-oratory services in therapeutic drug monitoring (TDM) andpharmacogenetics. Obviously, the differences in training ofclinical pharmacologists between the countries have a greatimpact on the functions in health care.The authors also asked the national delegates to define
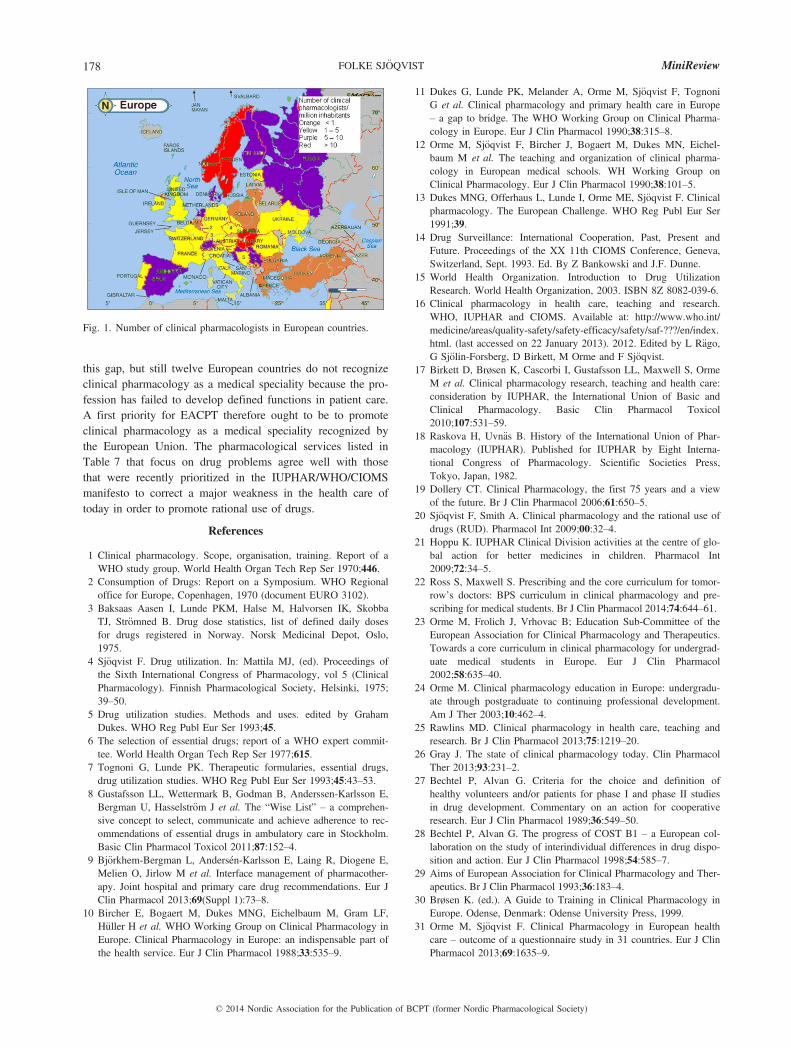
stumbling blocks in the development of clinical pharmacologyin their respective country. Lack of consultant posts in healthcare and underrepresentation in pre- and postgraduate curriculawere reported as particularly important factors for success.Figure 1 summarizes the present development of clinical
pharmacology in Europe.
Conclusion
This MiniReview shows that both WHO and IUPHAR veryearly recognized that there is a gap between the availability ofacademic expert knowledge in pharmacology and its utiliza-tion in health care. Many initiatives have been taken to bridge
Table 4.Important milestones in the development of EACPT (European Association for Clinical Pharmacology and Therapeutics).
Year Important decisions
1991–1993 Creation of EACPT1995 First EACPT congress in Paris (George Cheymol)1999 A Guide to Training in Clinical Pharmacology in Europe, edited by Kim Brøsen, Denmark [25]2001 Summer schools in Clinical Pharmacology being arranged biannually, the first one in Antalya, Turkey.1997–2015 Biannual EACPT congresses, location and president:
Berlin 1997 (Ivar Roots)Jerusalem 1999, (Micha Levy)Florence 2000 (Giampaolo Velo)Odense 2001 (Kim Brøsen)Istanbul 2003 (Cankat Tulunay)Poznan 2005 (Alexander Mroziekiewicz)Amsterdam 2007 (Jan Schellens)Edinburgh 2009 (David Webb)Budapest 2011 (Adam Vas)Geneva 2013 (Marie Besson and Caroline Samer)Madrid 2015 (Gonzalo Calvo-Rojas)
2013 Questionnaire study about clinical pharmacology in 21 European countries [26]
Table 5.Total number of positions in clinical pharmacology in 31 Europeancountries (from ref. [26]).
Total number of positions Number of countries
<10 910–20 430–50 450–100 8100–300 5600 1
Table 6.Number of positions in clinical pharmacology in Europe per millioninhabitants in 31 countries (from ref [26]).
Approximate number ofclinical pharmacologistsper million inhabitants Countries
1 or <1 Belgium, Bulgaria, France, Greece, Italy,Lithuania, Poland, Turkey, UK
2–4 Austria, Bosnia-Herzegovina, CzechRepublic, Estonia, Germany, Israel,Portugal, Romania, Slovenia, Ukraine
5–10 Croatia, Denmark, Finland, TheNetherlands, Russia, Serbia, Spain,Switzerland
>10 Hungary, Norway, Slovakia, Sweden
Table 7.Functions of clinical pharmacologists in health care (from ref. 26).
Functions Number of countries
Clinical trials 26Drug problem-oriented consultations 22Drug and Therapeutics Committees 20Drug information services 20Adverse drug reactions 20Pharmacogenetics consultations 19Therapeutic drug monitoring 16Pharmacoepidemiology and drug utilization 7Pharmacoeconomy 4Pharmacotherapy in pregnancy 3Drug intoxications 2
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
MiniReview CLINICAL PHARMACOLOGY IN EUROPE 177
this gap, but still twelve European countries do not recognizeclinical pharmacology as a medical speciality because the pro-fession has failed to develop defined functions in patient care.A first priority for EACPT therefore ought to be to promoteclinical pharmacology as a medical speciality recognized bythe European Union. The pharmacological services listed inTable 7 that focus on drug problems agree well with thosethat were recently prioritized in the IUPHAR/WHO/CIOMSmanifesto to correct a major weakness in the health care oftoday in order to promote rational use of drugs.
References
1 Clinical pharmacology. Scope, organisation, training. Report of aWHO study group. World Health Organ Tech Rep Ser 1970;446.
2 Consumption of Drugs: Report on a Symposium. WHO Regionaloffice for Europe, Copenhagen, 1970 (document EURO 3102).
3 Baksaas Aasen I, Lunde PKM, Halse M, Halvorsen IK, SkobbaTJ, Str€omned B. Drug dose statistics, list of defined daily dosesfor drugs registered in Norway. Norsk Medicinal Depot, Oslo,1975.
4 Sj€oqvist F. Drug utilization. In: Mattila MJ, (ed). Proceedings ofthe Sixth International Congress of Pharmacology, vol 5 (ClinicalPharmacology). Finnish Pharmacological Society, Helsinki, 1975;39–50.
5 Drug utilization studies. Methods and uses. edited by GrahamDukes. WHO Reg Publ Eur Ser 1993;45.
6 The selection of essential drugs; report of a WHO expert commit-tee. World Health Organ Tech Rep Ser 1977;615.
7 Tognoni G, Lunde PK. Therapeutic formularies, essential drugs,drug utilization studies. WHO Reg Publ Eur Ser 1993;45:43–53.
8 Gustafsson LL, Wettermark B, Godman B, Anderssen-Karlsson E,Bergman U, Hasselstr€om J et al. The “Wise List” – a comprehen-sive concept to select, communicate and achieve adherence to rec-ommendations of essential drugs in ambulatory care in Stockholm.Basic Clin Pharmacol Toxicol 2011;87:152–4.
9 Bj€orkhem-Bergman L, Anders�en-Karlsson E, Laing R, Diogene E,Melien O, Jirlow M et al. Interface management of pharmacother-apy. Joint hospital and primary care drug recommendations. Eur JClin Pharmacol 2013;69(Suppl 1):73–8.
10 Bircher E, Bogaert M, Dukes MNG, Eichelbaum M, Gram LF,H€uller H et al. WHO Working Group on Clinical Pharmacology inEurope. Clinical Pharmacology in Europe: an indispensable part ofthe health service. Eur J Clin Pharmacol 1988;33:535–9.
11 Dukes G, Lunde PK, Melander A, Orme M, Sj€oqvist F, TognoniG et al. Clinical pharmacology and primary health care in Europe– a gap to bridge. The WHO Working Group on Clinical Pharma-cology in Europe. Eur J Clin Pharmacol 1990;38:315–8.
12 Orme M, Sj€oqvist F, Bircher J, Bogaert M, Dukes MN, Eichel-baum M et al. The teaching and organization of clinical pharma-cology in European medical schools. WH Working Group onClinical Pharmacology. Eur J Clin Pharmacol 1990;38:101–5.
13 Dukes MNG, Offerhaus L, Lunde I, Orme ME, Sj€oqvist F. Clinicalpharmacology. The European Challenge. WHO Reg Publ Eur Ser1991;39.
14 Drug Surveillance: International Cooperation, Past, Present andFuture. Proceedings of the XX 11th CIOMS Conference, Geneva,Switzerland, Sept. 1993. Ed. By Z Bankowski and J.F. Dunne.
15 World Health Organization. Introduction to Drug UtilizationResearch. World Health Organization, 2003. ISBN 8Z 8082-039-6.
16 Clinical pharmacology in health care, teaching and research.WHO, IUPHAR and CIOMS. Available at: http://www.who.int/medicine/areas/quality-safety/safety-efficacy/safety/saf-???/en/index.html. (last accessed on 22 January 2013). 2012. Edited by L R€ago,G Sj€olin-Forsberg, D Birkett, M Orme and F Sj€oqvist.
17 Birkett D, Brøsen K, Cascorbi I, Gustafsson LL, Maxwell S, OrmeM et al. Clinical pharmacology research, teaching and health care:consideration by IUPHAR, the International Union of Basic andClinical Pharmacology. Basic Clin Pharmacol Toxicol2010;107:531–59.
18 Raskova H, Uvn€as B. History of the International Union of Phar-macology (IUPHAR). Published for IUPHAR by Eight Interna-tional Congress of Pharmacology. Scientific Societies Press,Tokyo, Japan, 1982.
19 Dollery CT. Clinical Pharmacology, the first 75 years and a viewof the future. Br J Clin Pharmacol 2006;61:650–5.
20 Sj€oqvist F, Smith A. Clinical pharmacology and the rational use ofdrugs (RUD). Pharmacol Int 2009;00:32–4.
21 Hoppu K. IUPHAR Clinical Division activities at the centre of glo-bal action for better medicines in children. Pharmacol Int2009;72:34–5.
22 Ross S, Maxwell S. Prescribing and the core curriculum for tomor-row’s doctors: BPS curriculum in clinical pharmacology and pre-scribing for medical students. Br J Clin Pharmacol 2014;74:644–61.
23 Orme M, Frolich J, Vrhovac B; Education Sub-Committee of theEuropean Association for Clinical Pharmacology and Therapeutics.Towards a core curriculum in clinical pharmacology for undergrad-uate medical students in Europe. Eur J Clin Pharmacol2002;58:635–40.
24 Orme M. Clinical pharmacology education in Europe: undergradu-ate through postgraduate to continuing professional development.Am J Ther 2003;10:462–4.
25 Rawlins MD. Clinical pharmacology in health care, teaching andresearch. Br J Clin Pharmacol 2013;75:1219–20.
26 Gray J. The state of clinical pharmacology today. Clin PharmacolTher 2013;93:231–2.
27 Bechtel P, Alvan G. Criteria for the choice and definition ofhealthy volunteers and/or patients for phase I and phase II studiesin drug development. Commentary on an action for cooperativeresearch. Eur J Clin Pharmacol 1989;36:549–50.
28 Bechtel P, Alvan G. The progress of COST B1 – a European col-laboration on the study of interindividual differences in drug dispo-sition and action. Eur J Clin Pharmacol 1998;54:585–7.
29 Aims of European Association for Clinical Pharmacology and Ther-apeutics. Br J Clin Pharmacol 1993;36:183–4.
30 Brøsen K. (ed.). A Guide to Training in Clinical Pharmacology inEurope. Odense, Denmark: Odense University Press, 1999.
31 Orme M, Sj€oqvist F. Clinical Pharmacology in European healthcare – outcome of a questionnaire study in 31 countries. Eur J ClinPharmacol 2013;69:1635–9.
Fig. 1. Number of clinical pharmacologists in European countries.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
178 FOLKE SJ€OQVIST MiniReview
Recommended

















