JOURNALOF
PSYCHIATRIC
Journal of Psychiatric Research 38 (2004) 577–582RESEARCH
www.elsevier.com/locate/jpsychires
Derivation of a definition of remission on theMontgomery–Asberg depression rating scale corresponding to
the definition of remission on the Hamilton rating scale for depression
Mark Zimmerman*, Michael A. Posternak, Iwona Chelminski
Department of Psychiatry and Human Behavior, Brown University School of Medicine, Rhode Island Hospital, 235 Plain Street,
Suite 501, Providence RI 02905, USA
Received 14 November 2003; received in revised form 5 March 2004; accepted 15 March 2004
Abstract
During the past decade the Montgomery–Asberg Depression Rating Scale (MADRS) has been used with increasing frequency to
measure outcome in antidepressant efficacy trials (AETs). In characterizing treatment outcome in AETs it is common to define
treatment remission as a score below a predetermined cutoff score on the scale. Various cutoffs have been used to define remission on
the MADRS. The goal of the present paper is to determine the cutoff on the MADRS that most closely corresponds to the cutoff
most frequently used on the Hamilton Rating Scale for Depression to define remission. Three hundred and three psychiatric
outpatients who were being treated for a DSM-IV major depressive episode were rated on the HRSD and the MADRS. A linear
regression equation was computed to estimate MADRS scores from HRSD scores. After deriving the regression equation, we
computed the MADRS score corresponding to an HRSD score of 7. We also examined the sensitivity, specificity and overall
classification rate of the MADRS for identifying remission on the HRSD. Based on the equation from a linear regression analysis
for the entire sample, a MADRS score of 611 would correspond to a score of 67 on the HRSD. We repeated the analysis after
excluding the more severely depressed patients who currently met criteria for MDD, and based on the equation from this regression
analysis a MADRS score of 610 would correspond to a score of 67 on the HRSD. In a complementary analysis, we examined the
sensitivity, specificity and overall classification rate of the MADRS at different cutoff points for identifying remission, and found
that a cutoff of 610 maximized the level of agreement with the HRSD definition of remission. In conclusion, the regression equation
relating HRSD and MADRS scores is dependent, in part, on the range and severity of scores in the sample. To facilitate com-
parisons of studies using the HRSD and MADRS our results suggest that a cutoff of 10 on the MADRS is equivalent to the HRSD
cutoff of 7.
� 2004 Elsevier Ltd. All rights reserved.
Keywords: Depression; Remission; Hamilton depression scale; Montgomery–Asberg depression rating scale
1. Introduction
In antidepressant efficacy trials (AETs) outcome istypically measured on standardized instruments, the two
most common being the Hamilton Rating Scale for
Depression (HRSD) (Hamilton, 1960) and the Mont-
gomery–Asberg Depression Rating Scale (MADRS)
* Corresponding author. Tel.: +1-401-277-0724; fax: +1-401-277-
0726.
E-mail address: [email protected] (M. Zimmerman).
0022-3956/$ - see front matter � 2004 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jpsychires.2004.03.007
(Montgomery and Asberg, 1979). For the past thirty
years the HRSD has been the most widely used outcome
measure in AETs (Prien et al., 1991), though during thepast decade the MADRS has been used with increasing
frequency (Khan et al., 2002). The HRSD was intended
as a measure of the severity of depressive symptoms,
whereas the MADRS was designed to be particularly
sensitive to change in patients treated with antidepres-
sant medication.
In describing treatment outcome in AETs it is com-
mon to define treatment response as a 50% or moreimprovement in scores on the HRSD or MADRS, and

Table
1
StudiesoftheassociationbetweentheMontgomery–Asbergdepressionratingscale
(MADRS)andtheHamiltonratingscale
fordepression(H
RSD)
Author
Patients
#Item
son
HRSD
MADRSmean
(SD)
HRSD
mean
(SD)
Correlation
coeffi
cient
Comment
Davidsonet
al.
44Inpatients
a32.2
(8.4)
27.0
(6.8)
0.46
Differentraters
completedHRSD
andMADRS
Dratcuet
al.
40Patients
–pre-treatm
ent(18inpatients,5
daypatients,17outpatients)
17
38.5
(8.1)
31.2
(6.1)
0.89
10Depressed
patients
after
4weeksoftreatm
ent
12.9
(16.1)
12.0
(12.9)
0.99
Hawleyet
al.
81In-andoutpatients
17
21.8
(12.8)
15.9
(9.1)
0.92
Correlationbasedon107pairsofratingsbecause
26patients
assessedtw
iceatleast
2weeksapart
Korner
etal.
40Inpatients
17
aa
0.82
Maieret
al.
130Inpatients
17
22.9
(11.5)
22.0
(7.3)
[17-item]
0.85
21
25.8
(7.9)
[21-item]
0.83
Mittm
annet
al.
77Outpatients
–pre-treatm
ent
17
29.7
(5.4)
23.9
(4.9)
0.66
49Outpatients
–after
4weeksoftreatm
ent
12.6
(9.5)
10.8
(6.6)
0.93
Mulder
etal.
195Outpatients
after
6weeksoftreatm
ent
17
13.0
(10.4)
8.0
(6.4)
0.92
Muller
etal.(2000)
40Inpatients
17
32.6
(5.0)
24.6
(4.3)
0.70
Muller
etal.(2003)
85Inpatients
17
23.4
(13.2)
18.4
(10.2)
0.94
Senra
52Outpatients
–pre-treatm
ent
17
26.5
(4.4)
20.8
(2.1)
0.68
45Outpatients
–after
24weeksoftreatm
ent
9.8
(6.6)
7.1
(6.1)
0.88
a
578 M. Zimmerman et al. / Journal of Psychiatric Research 38 (2004) 577–582
treatment remission as a score below a predetermined
cutoff score on the scale. Through the years many cutoff
scores have been used on the HRSD to define remission
(Zimmerman et al., 1985); however, since the publica-
tion of the recommendations of Frank et al. (1991) aconsensus has emerged to define remission on the
HRSD as a score of 7 or less.
No such consensus has yet emerged in defining re-
mission on the MADRS. Montgomery (1994) suggested
that a cutoff of 11 on the MADRS was comparable to
the HRSD cutoff of 7; however, investigators have used
cutoffs ranging from 6 to 12 to define remission on the
MADRS, a twofold difference (Forlenza et al., 2001;Guelfi et al., 2001; Kyle et al., 1998; Levine et al., 1989;
Nierenberg et al., 1994; Schweitzer et al., 2001). The lack
of convention in defining remission on the MADRS
makes it difficult to combine and contrast findings with
studies relying on the HRSD to assess remission.
Ten studies have examined the association between
the MADRS and HRSD (Table 1). In all studies, the
two measures were significantly correlated. The onlystudy finding a correlation below 0.65 used separate
interviewers to rate the two scales on different occasions
the same day (Davidson et al., 1986). All three studies
that examined the correlation before and after antide-
pressant treatment found higher correlations after
treatment initiation (Dratcu et al., 1987; Mittmann
et al., 1997; Senra, 1996). This is not surprising because
the size of the correlation between any two measures ofdepression severity will be influenced by the range and
variability of scores of patients included in the analysis.
The data in Table 1 shows that in each of the three
studies with pre- and post-treatment assessments, the
standard deviations of both the MADRS and HRSD
scores were higher in the post-treatment evaluations. In
these three studies, the average correlation between
post-treatment scores was 0.93. Thus, in treatmentstudies of depression, the MADRS and HRSD are
highly correlated, particularly when administered at
follow-up visits.
Three of the 10 studies used regression analyses to
develop formulas to derive MADRS scores from HRSD
scores. Mittmann et al. (1997) collected 262 MADRS-
HRSD pairs of ratings in 77 depressed outpatients, and
derived the following formula (MADRS¼ 1.23�HRSD) 0.30). Based on this formula they suggested
that a MADRS cutoff of 6 8 was equivalent to the
HRSD remission definition of 6 7. However, as the
authors noted, patients contributed multiple data points
to the regression analysis, thus most of the rating
couplets were not statistically independent.
Hawley et al. (1998) collected 107 MADRS-HRSD
pairs of ratings in 81 depressed in- and outpatients, andderived the following conversion formula (MADRS¼1.30�HRSD+0.7). Although they did not suggest a
cutoff for remission on the MADRS, based on this
Inform
ationnotprovided
inarticle.

M. Zimmerman et al. / Journal of Psychiatric Research 38 (2004) 577–582 579
formula a MADRS cutoff of 610 would be equivalent
to a HRSD cutoff of 67.
Muller et al. (2000) rated 40 moderate-severely de-
pressed inpatients on the MADRS and HRSD, and
derived the following conversion formula (MADRS¼0.81�HRSD+12.6). The goal of this study was to de-
termine a MADRS cutoff to distinguish moderate from
severe depression. When their formula is used to derive a
cutoff for remission, then a score of 6 18 on the
MADRS would correspond to the HRSD remission
threshold.
These three studies computed different regression
equations extrapolating MADRS scores from HRSDvalues, resulting in different cutoffs on the MADRS
corresponding to the cutoff of 7 on the HRSD. The
formulas in the two studies that included outpatients
who were rated after treatment initiation were roughly
comparable, and both differed from the formula de-
rived in the study of moderate-severely depressed in-
patients. This suggests that patient severity might
influence the derivation of the regression equation, andraises the question of how to select patients in studies
trying to extrapolate scores on one measure from an-
other. The inclusion of patients who currently meet
criteria for major depression might not be appropriate
for a study attempting to derive a cutoff for remission
on the MADRS that is equivalent to the HRSD cutoff
of 67.
In the present report from the Rhode Island Meth-ods to Improve Diagnostic Assessment and Services
(MIDAS) project, we determined the cutoff on the
MADRS that most closely corresponds to the HRSD
definition of remission in two ways. First, similar to
other research groups, we conducted a regression
analysis to derive an equation relating MADRS and
HRSD scores. We first conducted this analysis with the
entire sample, which includes patients who met fullcriteria for major depression as well as patients who
were in partial and full remission. Second, we repeated
the analysis after excluding patients who met criteria for
MDD. In this way, we were able to examine whether
inclusion of more severely depressed patients impacted
upon the regression equation used to derive a MADRS
equivalent for the HRSD definition of remission. The
second method of determining the MADRS equivalentto the HRSD cutoff of 6 7 used receiver operating
curve analysis.
2. Methods
Participants were 303 psychiatric outpatients who
were being treated for a DSM-IV major depressive ep-isode in the Rhode Island Hospital Department of
Psychiatry outpatient practice. This private practice
group predominantly treats individuals with medical
insurance on a fee-for-service basis, and it is distinct
from the hospital’s outpatient residency training clinic
that predominantly serves lower income, uninsured, and
medical assistance patients. The sample included 114
(37.6%) men and 189 (62.4%) women who ranged in agefrom 18 to 79 years (M ¼ 42:9, SD¼ 12.7). Almost half
of the subjects were married (47.9%, n ¼ 145); the re-
mainder were single (23.4%, n ¼ 71), divorced (19.8%,
n ¼ 60), separated (5.6%, n ¼ 17), widowed (2.0%,
n ¼ 6), or living with someone as if in a marital rela-
tionship (1.3%, n ¼ 4). The racial composition of the
sample was 86.8% (n ¼ 263) white, 2.6% ðn ¼ 8Þ black,4.3% ðn ¼ 13Þ Hispanic, 0.7% ðn ¼ 2Þ Asian, and 5.6%ðn ¼ 17Þ other. The Rhode Island Hospital institutional
review committee approved the research protocol, and
all patients provided informed, written consent.
Diagnoses were based on the Structured Clinical In-
terview for DSM-IV (First et al., 1995). The patients
were rated by the first two authors on the MADRS and
the 17-item HRSD. Inter-rater reliability on the
MADRS and HRSD was obtained in 16 patients, withone of the authors interviewing the patient while the
other observed and made independent ratings. For the
MADRS and HRSD the intraclass correlation
coefficients of reliability were 0.96 and 0.97, respectively.
At the time of the HRSD and MADRS assessments,
the patients were also rated on a 6-point rating scale
reflecting remission status according to DSM-IV. This
rating was based on the number of DSM-IV criteria fora major depressive episode and the level of psychosocial
impairment present during the past week. Slightly more
than one-third of the sample met MDD criteria at the
time of the evaluation ðn ¼ 114Þ, slightly less than one-
third were in partial remission ðn ¼ 87Þ, and one-third
were in remission ðn ¼ 102Þ.A linear regression equation was computed to esti-
mate MADRS scores from HRSD scores. This was doneseparately for the entire sample, and for patients who
were in partial or full remission. After deriving the re-
gression equation, we computed the MADRS score
corresponding to an HRSD score of 7.
We also examined the ability of the MADRS to
identify patients who were in remission according to the
HRSD across the range of MADRS cutoff scores by
conducting receiver operating curve (ROC) analyses(Hsiao et al., 1989). An ROC curve is a plot of a
measure’s sensitivity versus one minus specificity at each
cut-off score. The area under the curve (AUC) is the
evaluative measure, which can range from 0.5 (random
performance) to 1.0 (perfect performance).
3. Results
The mean score on the MADRS for the entire sample
was 17.2 (SD¼ 12.7). The mean score for the HRSD

580 M. Zimmerman et al. / Journal of Psychiatric Research 38 (2004) 577–582
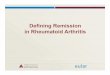
was 11.4 (SD¼ 8.4). The scattergram plot indicates
there was a linear relationship between the two measures
(Fig. 1). The Pearson correlation between the MADRS
and HRSD was 0.94 for the entire sample.
The linear regression analysis for the entire samplewith the MADRS as the dependent variable resulted in
the following equation: MADRS¼ 1.43�HRSD+
0.87. Based on this equation a MADRS score of 11
would correspond to a score of 7 on the HRSD. We
HRSD score403020100
MA
DR
S sc
ore
60
50
40
30
20
10
0
Fig. 1. Scatterplot of individual subjects’ pairwise co-ordinates be-
tween the Hamilton rating scale for depression (HRSD) and the
Montgomery–Asberg depression rating scale (MADRS).
1.00.75.50.250.00
1.00
.75
.50
.25
0.00
1 – Specificity (False Positive Rate)
Sensitivity (True Positive Rate)
Fig. 2. Receiver operating characteristic (ROC) curve of the Mont-
gomery–Asberg depression scale in depressed psychiatric outpatients
using the cutoff of 7 on the Hamilton depression scale to define
remission.
repeated the analysis after excluding the more severely
depressed patients who currently met criteria for MDD
and derived the following equation: MADRS¼ 1.36�HRSD+0.33. Based on this equation a MADRS score
of 10 would correspond to a score of 7 on the HRSD.In the Receiver Operating Curve analysis, the area
under the curve was significant (AUC¼ 0.98, p < 0:001)(Fig. 2). The sensitivity, specificity and overall classifi-
cation rate of the MADRS for identifying remission
according to the HRSD threshold of 67 is presented in
Table 2. A cutoff of 610 on the MADRS maximized the
level of agreement with the HRSD definition of
remission.
4. Discussion
The MADRS and HRSD are the two most frequently
used clinician-rated depression symptom severity scales.
Despite some differences in content and scaling of items,
the two scales are highly correlated. As seen in thesummary of studies in Table 1, MADRS scores tend to
be higher than HRSD scores; thus, the cutoffs to define
remission on the two scales would not be expected to be
equivalent.
In the absence of studies calibrating the MADRS
relative to the HRSD, investigators have had to estimate
the MADRS cutoff that would correspond to the HRSD
threshold. Two studies reporting remission rates usingboth the MADRS and HRSD found higher rates of
remission on the MADRS when a cutoff of 12 was used.
Guelfi et al. (2001) reported the results of an 8-week
study comparing venlafaxine and mirtazepine in severely
depressed inpatients. Remission was defined as a score
67 on the HRSD and 612 on the MADRS. From
figure 3 in their paper it appears that the remission rate
is about 10–15% lower in the two treatment groups ac-cording to the HRSD results. In contrast, the response
rate, defined as a 50% improvement in scores, was
similar according to both scales. Nierenberg et al. (1994)
reported response and remission rates according the
MADRS and 21-item HRSD in 70 patients treated with
venlafaxine. Remission was defined as a score 68 on the
HRSD and 612 on the MADRS. Response was defined
as a 50% decrease in scores along with final scores abovethe threshold used to define remission. At each time
point the remission rate was higher on the MADRS and
the response rate was higher on the HRSD. The higher
remission rates on the MADRS in these two studies are
not surprising in the context of the present study which
suggested that a cutoff of 10 on the MADRS most
closely approximates the HRSD cutoff of 7 to define
remission.Our results suggest that the regression equation
relating HRSD and MADRS scores is dependent, in
part, on the range and severity of scores in the sample.

Table 2
Sensitivity and specificity of the Montgomery–Asberg depression rating scale (MADRS) for identifying remission according to the Hamilton rating
scale for depression (HRSD) threshold of 6 7 in 303 depressed outpatients a
MADRS cutoff Cumulative N Sensitivity % Specificity % Overall % correct rate Kappa
0 23 19.5 100.0 68.6 0.23
61 34 28.8 100.0 72.3 0.33
62 52 44.1 100.0 78.2 0.49
63 60 50.8 100.0 80.9 0.56
64 68 57.6 100.0 83.5 0.62
65 78 66.1 100.0 86.8 0.70
66 88 73.7 99.5 89.4 0.77
67 96 79.7 98.9 91.4 0.81
68 99 81.4 98.4 91.7 0.82
69 102 83.9 98.4 92.7 0.84
610 106 87.3 98.4 94.0 0.87
611 116 89.8 94.6 92.7 0.85
612 121 89.8 91.9 91.1 0.81
613 126 90.7 89.7 90.1 0.79
614 135 95.8 88.1 91.1 0.82
615 146 98.3 83.8 89.4 0.79
616 148 98.3 82.7 88.8 0.77
617 155 98.3 78.9 86.5 0.73
618 164 100.0 75.1 84.8 0.70
619 176 100.0 68.5 80.8 0.63
620 178 100.0 67.6 80.2 0.62aResults are shown up to a MADRS cutoff score of 20. Beyond a score of 20, the sensitivity remains 100% and the specificity and overall level of
agreement continue to decline.
M. Zimmerman et al. / Journal of Psychiatric Research 38 (2004) 577–582 581
The mean HRSD and MADRS scores in the present
study are closest to those of Hawley et al. (1998), and
the regression equations in the two studies were sim-
ilar. To approximate the analysis by Muller and col-
leagues, we repeated the regression analysis in patients
who met MDD criteria. The equation computed for
these patients (MADRS¼ 1.04�HRSD+10.13), and
the MADRS score corresponding to an HRSD cutoffof 7 (i.e., 617), replicated Muller et al.’s findings. The
variability in results as a function of who is included
in the analyses suggests that the ROC approach,
which directly examines which MADRS score most
accurately corresponds to the HRSD definition of re-
mission, is a more valid method of addressing this
issue.
While the HRSD cutoff of 67 has been widelyadopted, there is little data supporting this threshold.
Rather it has been used for many years (DUAG, 1986;
Reisby et al., 1977), and was the recommended thresh-
old of a consensus conference to operationalize the
concepts of remission, relapse, and recovery-terms that
had acquired diverse definitions across studies. Addi-
tional recommendations from this panel were to em-
pirically validate the suggested operational definitions.Because the HRSD cutoff has gained widespread ac-
ceptance, it is important to determine the comparable
score on the MADRS, the second most frequently used
depression symptom severity outcome measure. The
findings of the present study do not, however, address
the question of which cutoff on the MADRS is the most
valid threshold for defining remission.
References
Davidson J, Turnbull CD, Strickland R, Miller R, Graves K. The
Montgomery–Asberg depression scale: reliability and validity. Acta
Psychiatrica Scandinavica 1986;73:544–8.
Dratcu L, da Costa Ribeiro L, Calil HM. Depression assessment in
Brazil. The first application of the Montgomery–Asberg depression
rating scale. British Journal of Psychiatry 1987;150:797–800.
Danish University Antidepressant Group (DUAG). Citalopram:
clinical effect profile in comparison with clomipramine. A
controlled multicenter study. Psychopharmacology 1986;90:131–
138.
First MB, Spitzer RL, Gibbon M, Williams JBW. Structured clinical
interview for DSM-IV axis I disorders – Patient edition (SCID-I/P,
version 2.0). New York: Biometrics Research Department, New
York State Psychiatric Institute; 1995.
Forlenza OV, Almeida OP, Stoppe Jr A, Hirata ES, Ferreira RCR.
Antidepressant efficacy and safety of low-dose sertraline and
standard-dose imipramine for the treatment of depression in older
adults: results from a double-blind, randomized, controlled clinical
trial. International Psychogeriatrics 2001;13:75–84.
Frank E, Prien RF, Jarrett RB, Keller MB, Kupfer DJ, Lavori PW,
et al. Conceptualization and rationale for consensus definitions of
terms in major depressive disorder. Archives of General Psychiatry
1991;48:851–5.
Guelfi JD, Ansseau M, Timmerman L, Korsgaard S, Group M-VS.
Mirtazapine versus venlafaxine in hospitalized severely depressed
patients with melancholic features. Journal of Clinical Psycho-
pharmacology 2001;21:425–431.
Hamilton M. A rating scale for depression. Journal of Neurology
Neurosurgery and Psychiatry 1960;23:56–62.
Hawley CJ, Gale TM, Smith V, Sen P. Depression rating scales can be
related to each other by simple equations. International Journal of
Psychiatry in Clinical Practice 1998;2:215–9.
Hsiao JK, Bartko JJ, Potter WZ. Diagnosing diagnoses: receiver
operating characteristic methods and psychiatry. Archives of
General Psychiatry 1989;46:664–7.

582 M. Zimmerman et al. / Journal of Psychiatric Research 38 (2004) 577–582
Khan A, Khan SR, Shankles EB, Polissar NL. Relative sensitivity of
the Montgomery–Asberg depression rating scale, the Hamilton
depression rating scale and the clinical global impressions rating
scale in antidepressant clinical trials. International Clinical Psy-
chopharmacology 2002;17:281–5.
Kyle CJ, Petersen HEH, Overo KF. Comparison of the tolerability
and efficacy of citalopram and amitriptyline in elderly depressed
patients treated in general practice. Depression and Anxiety
1998;8:147–53.
Levine S, Deo R, Mahadevan K. A comparative trial of a new
antidepressant, fluoxetine. International Clinical Psychopharma-
cology 1989;4:41–5.
Mittmann N, Mitter S, Borden EK, Herrmann N, Naranjo CA, Shear
NH. Montgomery–Asberg severity gradations. American Journal
of Psychiatry 1997;154:1320–1.
Montgomery S. Clinically relevant effect sizes in depression. European
Neuropsychopharmacology 1994;4:283–4.
Montgomery SA, Asberg M. A new depression scale designed to be
sensitive to change. British Journal of Psychiatry 1979;134:382–9.
Muller MJ, Himmerich H, Kienzle B, Szegedi A. Differentiating
moderate and severe depression using the Montgomery–Asberg
depression rating scale (MADRS). Journal of Affective Disorders
2003;77:255–60.
Muller MJ, Szegedi A, Wetzel H, Benkert O. Moderate and severe
depression gradations for the Montgomery–Asberg depression
rating scale. Journal of Affective Disorders 2000;60:137–
40.
Nierenberg AA, Feighner JP, Rudolph R, Cole JO, Sullivan J.
Venlafaxine for treatment-resistant unipolar depression. Journal of
Clinical Psychopharmacology 1994;14:419–23.
Prien RF, Carpenter LL, Kupfer DJ. The definition and operational
criteria for treatment outcome of major depressive disorder.
Archives of General Psychiatry 1991;48:796–800.
Reisby N, Gram L, Bech P, Nagy A, Petersen G, Ortmann J, et al.
Imipramine: clinical effects and pharmacokinetic variability. Psy-
chopharmacology 1977;54:263–72.
Schweitzer I, Burrows G, Tuckwell V, Polonowitz A, Flynn P, George
T, et al. Sustained response to open-label venlafaxine in drug-
resistant major depression. Journal of Clinical Psychopharmacol-
ogy 2001;21:185–9.
Senra C. Evaluation and monitoring of symptom severity and change
in depressed outpatients. Journal of Clinical Psychology
1996;52:317–24.
Zimmerman M, Coryell W, Pfohl B. The treatment validity of
DSM-III melancholic subtyping. Psychiatry Research 1985;
16:37–43.
Recommended
![Psychometric considerations of depression symptom rating ... · the Hamilton Rating Scale for Depression (HAM-D) [11] are multidimensional scales as they measure depression and anxiety](https://img.pdfslide.us/doc/110x75/60610d6e1e5829070461b7e5/psychometric-considerations-of-depression-symptom-rating-the-hamilton-rating.jpg)