CyPass® Micro-Stent2017 Coding and Billing Guide
CyPass® Micro-Stent Description and IndicationThe CyPass® Micro-Stent received FDA approval on July 29, 2016. The CyPass® System is indicated for use in conjunction with cataract surgery for the reduction of intraocular pressure (IOP) in adult patients with mild to moderate primary open-angle glaucoma (POAG).1
Procedure and Device Coding
The CyPass® Micro-Stent should be reported using Current Procedural Terminology (CPT®2) Code 0474T; insertion of anterior segment aqueous drainage device, with creation of intraocular reservoir, internal approach, into the supraciliary space. The applicable cataract procedure code should also be reported.
Facility claims require a Healthcare Common Procedure Coding System (HCPCS) code to identify the implant. The most common HCPCS codes used to report the CyPass® Micro-Stent implant are C1783, ocular implant, aqueous drainage assist device, or L8612, aqueous shunt. Failure to include the HCPCS code that describes the CyPass® device may result in inaccurate payment.
Common Coding for Physicians and Facilities
Physician Ambulatory Surgery Center, Freestanding Hospital Outpatient Department
1. 0474T; insertion of anterior segment aqueous drainage device, with creation of intraocular reservoir, internal approach, into the supraciliary space
2. Applicable cataract procedure code*
Note: This is not an inclusive list of codes. An example of a physician services claim form is available on page 3.
1. 0474T; insertion of anterior segment aqueous drainage device, with creation of intraocular reservoir, internal approach, into the supraciliary space
2. Applicable cataract procedure code*
3. Either C1783, ocular implant, aqueous drainage assist device, or L8612, aqueous shunt
4. Applicable IOL Implant Code
Note: This is not an inclusive list of codes. An example of a freestanding ambulatory surgery center claim form is available on page 4.
1. 0474T; insertion of anterior segment aqueous drainage device, with creation of intraocular reservoir, internal approach, into the supraciliary space and associated revenue code
2. Applicable cataract procedure code* and associated revenue code
3. Either C1783, ocular implant, aqueous drainage assist device, or L8612, aqueous shunt with revenue code 0278, other implants
4. Applicable Intraocular Lens Implant Code and associated revenue code, 0276 IOL Implants
Note: This is not an inclusive list of codes. An example of a hospital outpatient claim form is available on page 5.
1. See the back page for Important Safety Information. 2. CPT® is a registered trademark of the American Medical Association.
* The most common cataract CPT code is 66984; Extracapsular cataract removal with insertion of intraocular lens prosthesis (one stage procedure), manual or mechanical technique (e.g. irrigation and aspiration or phacoemulsification), however other codes may apply.
1

Diagnosis Coding
Diagnosis coding is determined by the patient’s condition. The ICD-10-CM codes listed below are commonly associated with patients receiving the CyPass® Micro-Stent. The list below is not intended to provide an exhaustive list of all possible diagnosis codes. Note that in all cases, it is ultimately the responsibility of the provider to report the ICD-10-CM diagnosis code that most accurately describes the patient’s condition.
The CyPass® Micro-Stent is indicated for use in conjunction with cataract surgery for the reduction of intraocular pressure (IOP) in adult patients with mild to moderate primary open-angle glaucoma (POAG).
Common diagnosis codes include:
ICD-10-CM Description
H40.1111 Primary open-angle glaucoma, right eye, mild stage
H40.1112 Primary open-angle glaucoma, right eye, moderate stage
H40.1121 Primary open-angle glaucoma, left eye, mild stage
H40.1122 Primary open-angle glaucoma, left eye, moderate stage
H40.1131 Primary open-angle glaucoma, bilateral, mild stage
H40.1132 Primary open-angle glaucoma, bilateral, moderate stage
Coverage
Some payers have established positive coverage decisions for the implantation of the CyPass® Micro-Stent device. Alcon continues to work with payers to obtain positive coverage and specific guidance for the placement of the CyPass® Micro-Stent.
Payers may require a prior authorization or pre determination and in some cases additional documentation to support the claim.
Contact Alcon Reimbursement Services at (866) 457- 0277 or at: [email protected] with questions about specific coverage policies.
This information is provided for informational purposes only. It does not constitute legal or reimbursement advice or recommendations regarding clinical practice. Alcon makes no guarantee that use of this information will result in coverage or payment or prevent disagreement by payers with regard to billing, coverage or amount of payment. Alcon encourages providers to submit accurate and appropriate claims for services. It is always the provider’s responsibility to determine medical necessity, the proper site for delivery of any services and to submit accurate information, codes, charges, and modifiers for services that are rendered. Coding, coverage and payment policies are complex and are frequently updated. Alcon recommends that you consult with your legal counsel, applicable payers’ policies or reimbursement specialists regarding coding, coverage and reimbursement. 2

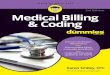
Physician Services 2017 Example CMS-1500
Alcon Reimbursement Services (866) 457- 0277
Insertion of aqueous drainage device into the supraciliary space
H25.1X
07 01 17 07 01 17 0474T
66984
LT or RT
LT or RT X,XXX XX
X,XXX XX
07 01 17 07 01 17
H40.11X1
Box 19: Insert the description of 0474T; “Insertion of aqueous drainage device into the supraciliary space.”
Box 21: DIAGNOSISEnter applicable diagnosis codes.
Common Place of Service Codes are:19: Off Campus-Outpatient Hospital22: On Campus-Outpatient Hospital24: Ambulatory Surgical Center, Freestanding
B
A
This information is provided for informational purposes only. It does not constitute legal or reimbursement advice or recommendations regarding clinical practice. Alcon makes no guarantee that use of this information will result in coverage or payment or prevent disagreement by payers with regard to billing, coverage or amount of payment. Alcon encourages providers to submit accurate and appropriate claims for services. It is always the provider’s responsibility to determine medical necessity, the proper site for delivery of any services and to submit accurate information, codes, charges, and modifiers for services that are rendered. Coding, coverage and payment policies are complex and are frequently updated. Alcon recommends that you consult with your legal counsel, applicable payers’ policies or reimbursement specialists regarding coding, coverage and reimbursement.
Example Physician Services Claim Form for the CyPass® Micro-Stent
3

(When using a UB-04, refer to the Hospital Outpatient Claim Form Example)
Insertion of aqueous drainage device into the supraciliary space
H25.1X
07 01 17 07 01 17 24 0474T B
A
B
66984
C1783OR
L8612
X,XXX XX
X,XXX XX
X,XXX.XX
X,XXX XX
07 01 17 07 01 17 24
07 01 17 07 01 17 24
H40.11X1
(LT or RT)
Alcon Reimbursement Services (866) 457- 0277
Box 24D: Report the CyPass® device with C1783, ocular implant, aqueous drainage assist device, or L8612, aqueous shunt.Failure to report the device may result in inaccurate payment.
Box 21: DIAGNOSISEnter applicable diagnosis codes.
Box 19: Insert the description of 0474T; “Insertion of an anterior segment aqueous drainage device, into the supraciliary space.”
(LT or RT)
Freestanding Ambulatory Surgery Center 2017 Example CMS-1500
This information is provided for informational purposes only. It does not constitute legal or reimbursement advice or recommendations regarding clinical practice. Alcon makes no guarantee that use of this information will result in coverage or payment or prevent disagreement by payers with regard to billing, coverage or amount of payment. Alcon encourages providers to submit accurate and appropriate claims for services. It is always the provider’s responsibility to determine medical necessity, the proper site for delivery of any services and to submit accurate information, codes, charges, and modifiers for services that are rendered. Coding, coverage and payment policies are complex and are frequently updated. Alcon recommends that you consult with your legal counsel, applicable payers’ policies or reimbursement specialists regarding coding, coverage and reimbursement.
Example Freestanding ASC Claim Form for the CyPass® Micro-Stent
4

1 2 4 TYPEOF BILL
FROM THROUGH5 FED. TAX NO.
a
b
c
d
DX
ECI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
A
B
C
A B C D E F G HI J K L M N O P Q
a b c a b c
a
b c d
ADMISSION CONDITION CODESDATE
OCCURRENCE OCCURRENCE OCCURRENCE OCCURRENCE SPAN OCCURRENCE SPANCODE DATE CODE CODE CODE DATE CODE THROUGH
VALUE CODES VALUE CODES VALUE CODESCODE AMOUNT CODE AMOUNT CODE AMOUNT
TOTALS
PRINCIPAL PROCEDURE a. OTHER PROCEDURE b. OTHER PROCEDURE NPICODE DATE CODE DATE CODE DATE
FIRST
c. d. e. OTHER PROCEDURE NPICODE DATE DATE
FIRST
NPI
b LAST FIRST
c NPI
d LAST FIRST
UB-04 CMS-1450
7
10 BIRTHDATE 11 SEX 12 13 HR 14 TYPE 15 SRC
DATE
16 DHR 18 19 20
FROM
21 2522 26 2823 27
CODE FROMDATE
OTHER
PRV ID
THE CERTIFICATIONS ON THE REVERSE APPLY TO THIS BILL AND ARE MADE A PART HEREOF.
b
.INFO BEN.
CODEOTHER PROCEDURE
THROUGH
29 ACDT 30
3231 33 34 35 36 37
38 39 40 41
42 REV. CD. 43 DESCRIPTION 45 SERV. DATE 46 SERV. UNITS 47 TOTAL CHARGES 48 NON-COVERED CHARGES 49
52 REL51 HEALTH PLAN ID
53 ASG.54 PRIOR PAYMENTS 55 EST. AMOUNT DUE 56 NPI
57
58 INSURED’S NAME 59 P.REL 60 INSURED’S UNIQUE ID 61 GROUP NAME 62 INSURANCE GROUP NO.
64 DOCUMENT CONTROL NUMBER 65 EMPLOYER NAME
66 67 68
69 ADMIT 70 PATIENT 72 73
74 75 76 ATTENDING
80 REMARKS
OTHER PROCEDURE
a
77 OPERATING
78 OTHER
79 OTHER
81CC
CREATION DATE
3a PAT.CNTL #
24
b. MED.REC. #
44 HCPCS / RATE / HIPPS CODE
PAGE OF
APPROVED OMB NO. 0938-0997
e
a8 PATIENT NAME
50 PAYER NAME
63 TREATMENT AUTHORIZATION CODES
6 STATEMENT COVERS PERIOD
9 PATIENT ADDRESS
17 STAT STATE
DX REASON DX71 PPS
CODE
QUAL
LAST
LAST
National UniformBilling Committee
™
OCCURRENCE
QUAL
QUAL
QUAL
CODE DATE
A
B
C
A
B
C
A
B
C
A
B
C
A
B
C
a
b
a
b
0360 Operating Room Services 0474T (LT or RT) 07-01-17 1 X,XXX XX
H25.1X H40.11X1
0360 Operating Room Services 66984 (LT or RT) 07-01-17 1 X,XXX XX0276 IOL Implants V2632 07-01-17 1 X,XXX XX027X Supplies XXX 07-01-17 1 XXX XXXXXX Pharmacy XXX 07-01-17 1 XXX XX0278 Other Implants C1783 or L8612 07-01-17 1 X,XXX XX
Line 3: Insertion of a posterior chamber intraocular lensLine 6: Insertion of aqueous drainage device
X,XXX XX
Alcon Reimbursement Services (866) 457- 0277
Box 42: REVENUE CODEUse revenue code 0278, other implants, for the CyPass® device.
Box 44: HCPCS CODE Report the CyPass® device with C1783, ocular implant, aqueous drainage assist device, or L8612, aqueous shunt. Failure to report the device may result in inaccurate payment.
Box 66: DIAGNOSISEnter applicable diagnosis codes.
Box 80: REMARKSInsert the description of the HCPCS Code for the aqueous drainage device.Example: Line 6: Insertion of an anterior segment aqueous drainage device into the supraciliary space (C1783 or L8612).
Box 80: REMARKS Insert the description of the HCPCS Code for the intraocular lens. Example: Line 3: Insertion of a posterior chamber intraocular lens (V2632).
Hospital Outpatient2017 Example UB-04
This information is provided for informational purposes only. It does not constitute legal or reimbursement advice or recommendations regarding clinical practice. Alcon makes no guarantee that use of this information will result in coverage or payment or prevent disagreement by payers with regard to billing, coverage or amount of payment. Alcon encourages providers to submit accurate and appropriate claims for services. It is always the provider’s responsibility to determine medical necessity, the proper site for delivery of any services and to submit accurate information, codes, charges, and modifiers for services that are rendered. Coding, coverage and payment policies are complex and are frequently updated. Alcon recommends that you consult with your legal counsel, applicable payers’ policies or reimbursement specialists regarding coding, coverage and reimbursement.
Example Hospital Outpatient Claim Form for the CyPass® Micro-Stent
5

(866) 457-0277 | [email protected]://ars.alcon.com © 2017 Novartis 06/17 US-CYP-16-E-3513
CyPass® Micro-Stent Important Product Information
Caution: Federal (USA) law restricts this device to sale by or on the order of a physician.
Indication: The CyPass® Micro-Stent is indicated for use in conjunction with cataract surgery for the reduction of intraocular pressure (IOP) in adult patients with mild to moderate primary open-angle glaucoma (POAG).
Contraindications: Use of the CyPass® Micro-Stent is contraindicated in the following circumstances or conditions: (1) in eyes with angle closure glaucoma; and (2) in eyes with traumatic, malignant, uveitic or neovascular glaucoma or discernible congenital anomalies of the anterior chamber angle.
MRI Information: The CyPass® Micro-Stent is magnetic resonance (MR) Safe: the implant is constructed of polyimide material, a non-conducting, non-metallic, non-magnetic polymer that poses no known hazards in all magnetic resonance imaging environments.
Warnings: Gonioscopy should be performed prior to surgery to exclude peripheral anterior synechiae (PAS), rubeosis, and other angle abnormalities or conditions that would prohibit adequate visualization of the angle that could lead to improper placement of the stent and pose a hazard.
Precautions: The surgeon should monitor the patient postoperatively for proper maintenance of intraocular pressure. The safety and effectiveness of the CyPass® Micro-Stent has not been established as an alternative to the primary treatment of glaucoma with medications, in patients 21 years or younger, in eyes with significant prior trauma, chronic inflammation, eyes with an abnormal anterior segment, eyes with chronic inflammation, eyes with glaucoma associated with vascular disorders, pseudophakic eyes with glaucoma, eyes with uveitic glaucoma, eyes with
pseudoexfoliative or pigmentary glaucoma, eyes with other secondary open angle glaucomas, eyes that have undergone prior incisional glaucoma surgery or cilioablative procedures, eyes with laser trabeculoplasty performed ≤ 3 months prior to the surgical screening visit, eyes with unmedicated IOP less than 21 mmHg or greater than 33 mmHg, eyes with medicated IOP greater than 25 mmHg, in the setting of complicated cataract surgery with iatrogenic injury to the anterior or posterior segment, and when implantation is without concomitant cataract surgery with IOL implantation for visually significant cataract. The safety and effectiveness of use of more than a single CyPass® Micro-Stent has not been established.
Adverse Events: In a randomized, multicenter clinical trial comparing cataract surgery with CyPass® to cataract surgery alone, the most common post-operative adverse events included: BCVA loss of 10 or more letters at 3 months after surgery (8.8% for CyPass vs. 15.3% for cataract surgery only); anterior chamber cell and flare requiring steroid treatment 30 or more days after surgery (8.6% vs. 3.8%); worsening of visual field mean deviation by 2.5 or more decibels (6.7% vs. 9.9%); IOP increase of 10 or more mmHg 30 or more days after surgery (4.3% vs. 2.3%); and corneal edema 30 or more days after surgery, or severe in nature (3.5% vs. 1.5%).
Attention: Please refer to the Product Instructions for a complete list of contraindications, warnings, precautions and adverse events.
Recommended